hcv highlights from aasld 2012 - chronic liver disease foundation
TRANSCRIPT

Boceprevir (BOC) Combined with Peginterferon alfa-
2b/Ribavirin (P/RBV) in Treatment-Naïve Chronic HCV
Genotype 1 Patients with Compensated Cirrhosis: Sustained
Virologic Response (SVR) and Safety Subanalyses from the
Anemia Management Study
Lawitz E, Zeuzem S, Nyberg LM, Nelson DR, Rossaro L,
Balart LA, K. Reddy R, Morgan T, Deng W, Koury KJ,
Alves K, Dutko F, Wahl J, Pedicone L, Poordad F
Abstract 50, AASLD 2012
HCV Highlights from AASLD 2012
November 9 - 13, 2012 Boston, MA

Boceprevir/PegIFN/ RBV in Treatment-Naïve Chronic
HCV Genotype 1 Patients with Compensated Cirrhosis:
Anemia Management
Objective
• To evaluate SVR rates and tolerability of two
anemia management strategies (RBV dose
reduction [DR] or erythropoietin [EPO] use) in
cirrhotics vs. non-cirrhotics treated with
BOC/PegIFN/RBV
Lawitz E et al. Hepatology 2012; 56(Suppl S1):216A

Boceprevir/PegIFN/ RBV in Treatment-Naïve Chronic
HCV Genotype 1 Patients with Compensated Cirrhosis:
Anemia Management
Lawitz E et al. Hepatology 2012; 56(Suppl S1):216A
After 4-week lead-in
with P/RBV, all
patients initiated
boceprevir.
Hb at wk 0, 2, 4, 6,
8, 10, 12, 24,
28, 34, 40, 48.
Randomized if
Hb ~10 g/dl
EPO
(n=251)
RBV DR
(n=249)
If Hb≤8.5 g/dL,
secondary
intervention
(RBV DR arm
could use EPO;
EPO arm could
use RBV DR)
If Hb>10 g/dL, patients
treated but not randomized
(n=187)
Study Design

Boceprevir/PegIFN/ RBV in Treatment-Naïve Chronic
HCV Genotype 1 Patients with Compensated Cirrhosis:
Anemia Management
Lawitz E et al. Hepatology 2012; 56(Suppl S1):216A
Initial dosing • PegIFN α-2b administered subcutaneously at 1.5 g/kg
once weekly, plus RBV using weight-based dosing of
600-1400 mg/day in a divided daily dose
Interventions for anemia • RBV DR by increments of 200 mg at the discretion of the
investigator (first increment of 400 mg if initial dose was
1,400 mg/day)
• EPO was started at 40,000 units/wk and could be
modified at the investigator’s discretion to doses of
20,000 to 60,000 units/wk
• If Hb≤7.5 g/dL, all study drugs were discontinued

Boceprevir/PegIFN/ RBV in Treatment-Naïve Chronic
HCV Genotype 1 Patients with Compensated Cirrhosis:
Anemia Management
Lawitz E et al. Hepatology 2012; 56(Suppl S1):216A
10%
71%
82%
10%
71%
82%
0
20
40
60
80
100
EOT SVR Relapse
% of Patients
RBV DR
EPO
Primary Efficacy Results
203/
249
205/
251
178/
249
178/
251 19/ 196
19/ 197

Boceprevir/PegIFN/ RBV in Treatment-Naïve Chronic
HCV Genotype 1 Patients with Compensated Cirrhosis:
Anemia Management
Lawitz E et al. Hepatology 2012; 56(Suppl S1):216A
18%
55%
68%
11%
64%
76%
0
20
40
60
80
100
EOT SVR Relapse
% of Patients
Cirrhotics
Non-Cirrhotics
Efficacy Results: Cirrhotics and Non-Cirrhotics
41/
60
460/
604
33/
60
387/
604 7/ 40
47/ 433

Boceprevir/PegIFN/ RBV in Treatment-Naïve Chronic
HCV Genotype 1 Patients with Compensated Cirrhosis:
Anemia Management
Lawitz E et al. Hepatology 2012; 56(Suppl S1):216A
73%
57%
72%64%
0
20
40
60
80
100
Cirrhotics Non-Cirrhotics
% of Patients
SVRs Were Similar with RBV Dose Reduction
or EPO
13/
23
16/
25
162/
221
157/
217
RBV DR RBV DR EPO EPO

Boceprevir/PegIFN/ RBV in Treatment-Naïve Chronic
HCV Genotype 1 Patients with Compensated Cirrhosis:
Anemia Management
Category
Number (%) of Patients
Cirrhotics
(N=60)
Non-cirrhotics
(N=604)*
Treatment-emergent AEs 60 (100) 597 (99)
Serious AEs 12 (20) 72 (12)
Death 0 (0) 1 (<1)ǂ
Life-threatening treatment-
emergent AEs
2 (3) 13 (2)
Study drug discontinuation due
to AE
10 (17) 94 (16)
*Includes all treated patients (RBV DR, EPO, treated and not randomized) Excludes 23 patients with inadequate portal tracts/missing for cirrhosis
ǂEvent assessed by investigator as unlikely related to study medication
Lawitz E et al. Hepatology 2012; 56(Suppl S1):216A
Summary of Adverse Events

Boceprevir/PegIFN/ RBV in Treatment-Naïve Chronic
HCV Genotype 1 Patients with Compensated Cirrhosis:
Anemia Management
Hematologic Variables Cirrhotics
n/m* (%)
Non-cirrhotics
n/m (%)
Hemoglobin concentration
6.5 g/dL to 8.0 g/dL
<6.5 g/dL
4/59 (7)
0/59 (0)
31/601 (5)
0/601 (0)
Neutrophil counts
500 to <750/mm3
<500/mm3
14/59 (24)
12/59 (20)
160/601 (27)
72/601 (12)
Platelet counts
25,000 to <50,000/mm3
<25,000/mm3
13/59 (22)
1/59 (2)
12/601 (2)
1/601 (<1)
Packed red blood cell transfusion 2/60 (3) 14/604 (2)
*n/m = number of patients with characteristic / subtotal
Lawitz E et al. Hepatology 2012; 56(Suppl S1):216A
Hematologic parameters

Boceprevir/PegIFN/ RBV in Treatment-Naïve Chronic
HCV Genotype 1 Patients with Compensated Cirrhosis:
Anemia Management
Lawitz E et al. Hepatology 2012; 56(Suppl S1):216A
Conclusions
• SVRs are comparable in cirrhotic patients when
anemia is managed by RBV dose reduction or
EPO
• Rates of anemia and transfusions similar in
cirrhotics and non-cirrhotics; higher rates of
neutropenia and thrombocytopenia in cirrhotics
• Ribavirin dose reduction should be considered
as the initial management strategy for anemia

Safety and Efficacy of Telaprevir or Boceprevir in Combination with
Peginterferon alfa/Ribavirin, in 455 Cirrhotic Non Responders.
Week 16 Analysis of the French Early Access Program
(ANRS CO20-CUPIC) in Real-Life Setting
Hezode C, Dorival C, Zoulim F, Larrey DG, Pol S, Cacoub P, Canva V, Poynard T,
Samuel D, Bourliere M, Alric L, Raabe J-J, Zarski J-PH, Riachi G, Bernard P-H,
de Ledinghen V, Loustaud-Ratti V, Metivier S, Causse X, Marcellin P, Barthe Y,
Fontaine H, Carrat F, Bronowicki J-P
Abstract 51, AASLD 2012
HCV Highlights from AASLD 2012
November 9 - 13, 2012 Boston, MA

Safety and Efficacy of Telaprevir or Boceprevir in
Combination with PegIFN/RBV in Cirrhotic Non
Responder Chronic Hepatitis C Patients
Objective
• Week 16 analysis of safety and efficacy of
telaprevir (TVR) or boceprevir (BOC) in
combination with PegIFN/RBV in cirrhotic non
responder hepatitis C patients in a real-life
setting
Hezode C et al. Hepatology 2012; 56(Suppl S1):217A

Safety and Efficacy of Telaprevir or Boceprevir in
Combination with PegIFN/RBV in Cirrhotic Non
Responder Chronic Hepatitis C Patients
Methods
• Study involved treatment experienced (relapse, partial
response) HCV patients enrolled in a French Early
Access Program
• 674 genotype 1 patients with compensated cirrhosis
(Child A) were prospectively included
• Received 12W TVR/PegIFN-2a/RBV + 36W
PegIFN/RBV or 4W PegIFN-2b/RBV + 44W
BOC/PegIFN/RBV
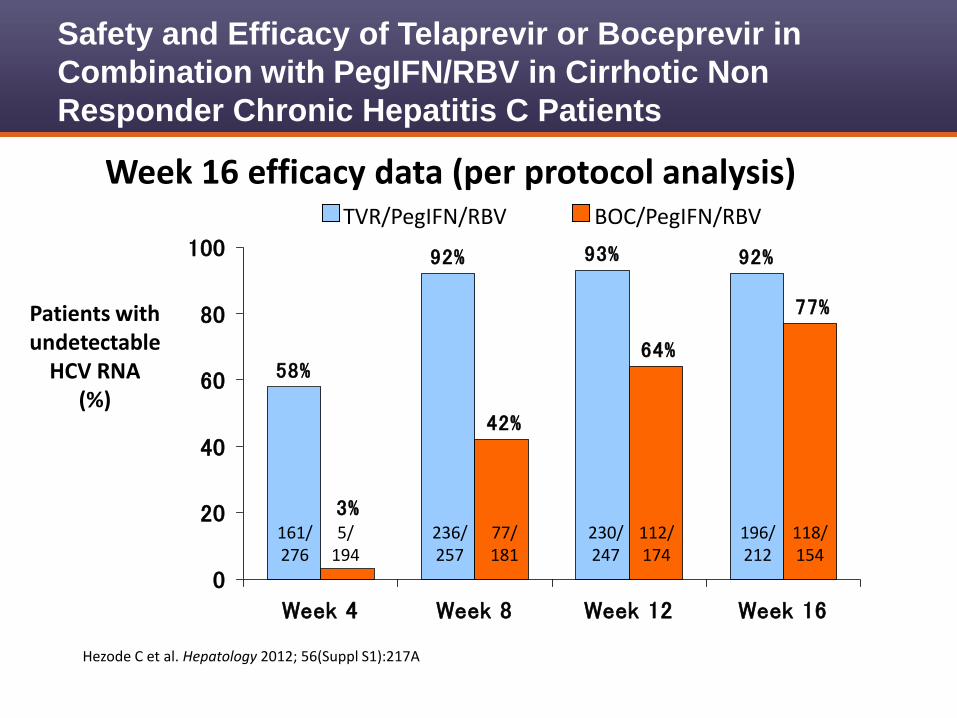
• Present analysis limited to 497 patients reaching W16 of
therapy
Hezode C et al. Hepatology 2012; 56(Suppl S1):217A
Safety and Efficacy of Telaprevir or Boceprevir in
Combination with PegIFN/RBV in Cirrhotic Non
Responder Chronic Hepatitis C Patients
Hezode C et al. Hepatology 2012; 56(Suppl S1):217A
92%93%92%
58%
77%
64%
42%
3%
0
20
40
60
80
100
Week 4 Week 8 Week 12 Week 16
Patients with undetectable
HCV RNA (%)
Week 16 efficacy data (per protocol analysis) TVR/PegIFN/RBV BOC/PegIFN/RBV
161/ 276
236/ 257
230/ 247
196/ 212
5/ 194
77/ 181
112/ 174
118/ 154

Safety and Efficacy of Telaprevir or Boceprevir in
Combination with PegIFN/RBV in Cirrhotic Non
Responder Chronic Hepatitis C Patients
*SCAR: Severe cutaneous adverse reaction
Hezode C et al. Hepatology 2012; 56(Suppl S1):217A
Week 16 safety findings
Patients, n (% patients with at least one event) Telaprevir
n=292
Boceprevir
(n=205)
Serious adverse events (SAEs) 132 (45.2%) 67 (32.7%)
Premature discontinuation
Due to SAEs
66 (22.6%)
43 (14.7%)
54 (26.3%)
15 (7.3%)
Death 5 (2.6%) 1 (0.5%)
Infection (Grade 3/4) 19 (6.5%) 5 (2.4%)
Hepatic decompensation ( Grade 3/4) 6 (2.0%) 6 (2.9%)
Astnenia (Grade 3/4) 16 (5.5%) 12 (5.8%)
Rash (Grade 3/SCAR*) 14 (4.8%) 0
Renal failure 5 (1.7%) 0
Safety and Efficacy of Telaprevir or Boceprevir in
Combination with PegIFN/RBV in Cirrhotic Non
Responder Chronic Hepatitis C Patients
Hezode C et al. Hepatology 2012; 56(Suppl S1):217A
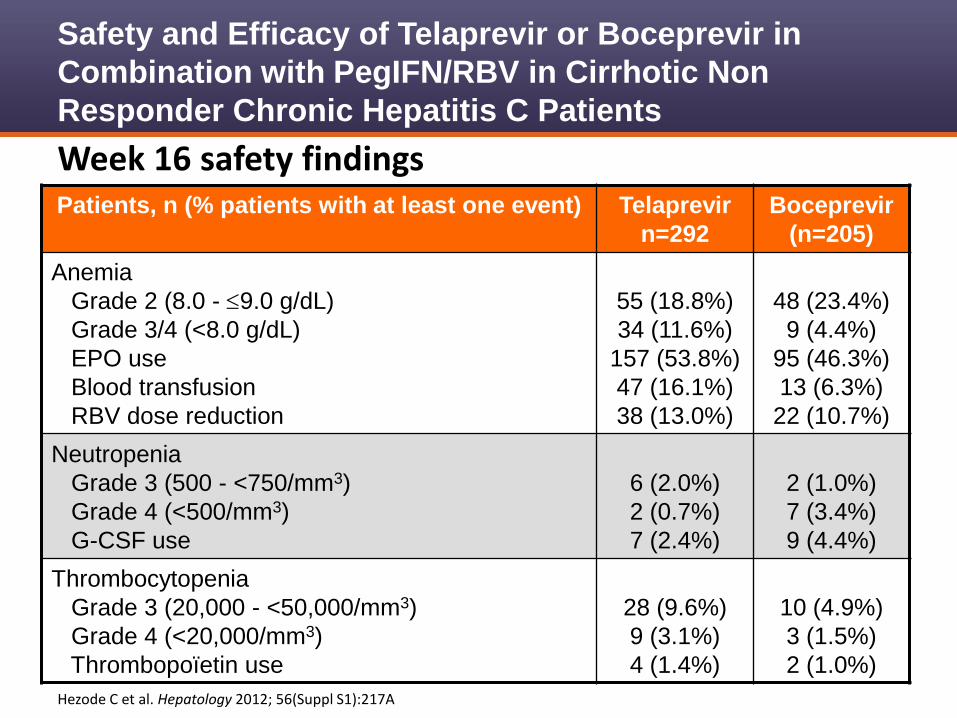
Week 16 safety findings Patients, n (% patients with at least one event) Telaprevir
n=292
Boceprevir
(n=205)
Anemia
Grade 2 (8.0 - 9.0 g/dL)
Grade 3/4 (<8.0 g/dL)
EPO use
Blood transfusion
RBV dose reduction
55 (18.8%)
34 (11.6%)
157 (53.8%)
47 (16.1%)
38 (13.0%)
48 (23.4%)
9 (4.4%)
95 (46.3%)
13 (6.3%)
22 (10.7%)
Neutropenia
Grade 3 (500 - <750/mm3)
Grade 4 (<500/mm3)
G-CSF use
6 (2.0%)
2 (0.7%)
7 (2.4%)
2 (1.0%)
7 (3.4%)
9 (4.4%)
Thrombocytopenia
Grade 3 (20,000 - <50,000/mm3)
Grade 4 (<20,000/mm3)
Thrombopoïetin use
28 (9.6%)
9 (3.1%)
4 (1.4%)
10 (4.9%)
3 (1.5%)
2 (1.0%)
Safety and Efficacy of Telaprevir or Boceprevir in
Combination with PegIFN/RBV in Cirrhotic Non
Responder Chronic Hepatitis C Patients
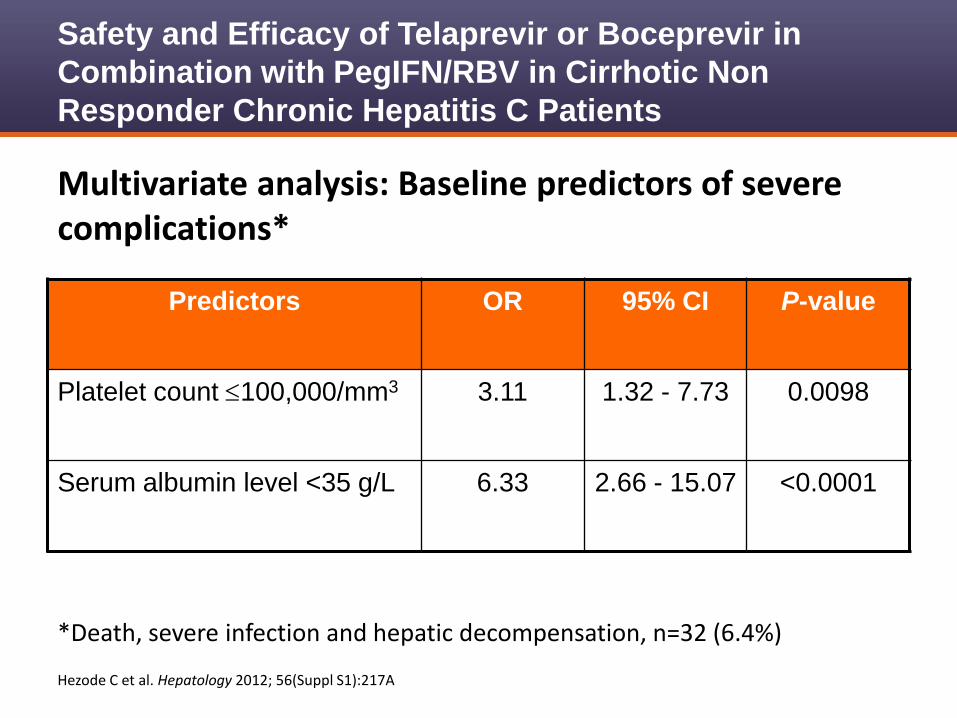
*Death, severe infection and hepatic decompensation, n=32 (6.4%)
Hezode C et al. Hepatology 2012; 56(Suppl S1):217A
Multivariate analysis: Baseline predictors of severe complications*
Predictors OR 95% CI P-value
Platelet count 100,000/mm3 3.11 1.32 - 7.73 0.0098
Serum albumin level <35 g/L 6.33 2.66 - 15.07 <0.0001

Safety and Efficacy of Telaprevir or Boceprevir in
Combination with PegIFN/RBV in Cirrhotic Non
Responder Chronic Hepatitis C Patients
Hezode C et al. Hepatology 2012; 56(Suppl S1):217A
Multivariate analysis: Baseline predictors of anemia <8g/dL or blood transfusion (n=71/497, 14.3%)
Predictors OR 95% CI P-value
Gender: Female 2.19 1.11 - 4.33 0.023
No lead-in phase 2.25 1.15 - 4.39 0.018
Age 65 years 3.04 1.54 - 6.02 0.0014
Hemoglobin level
12 g/dL for female
13 g/dL for male
5.30 2.49 - 11.25 <0.0001

Safety and Efficacy of Telaprevir or Boceprevir in
Combination with PegIFN/RBV in Cirrhotic Non
Responder Chronic Hepatitis C Patients
Hezode C et al. Hepatology 2012; 56(Suppl S1):217A
Conclusions
• Treatment of compensated cirrhotic patients with TVR or BOC
in combination with PegIFN/RBV resulted in high rates on on-
treatment virologic response
• Treatment was associated with increased rates of SAEs and
more difficult management of anemia compared to phase III
trials
• Cirrhotic patients with platelet count 100,000/mm3 or serum
albumin level <35 g/L should be treated on a case by case
basis due increased risk for severe complications
• Cirrhotic patients without predictors of severe complications
should be treated cautiously and carefully monitored

Telaprevir in Combination with Peginterferon Alfa-
2a/Ribavirin in HCV/HIV Co-infected Patients: SVR24
Final Study Results
Sulkowski MS, Sherman KE, Soriano V, Rockstroh J, Dieterich DT, Girard PM,
Bsharat M, Henshaw J, Rubin RA, Garg V, Adda N
Abstract 54, AASLD 2012
HCV Highlights from AASLD 2012
November 9 - 13, 2012 Boston, MA

Telaprevir/PegIFN/RBV in HCV/HIV Co-Infected Patients
Primary Objectives
• Safety and tolerability of telaprevir (TVR) in combination
with PegIFN/RBV in HCV/HIV co-infected patients
• Proportion of patients who are HCV RNA undetectable
after 12 weeks of TVR/PegIFN/RBV
Secondary Objectives
• Efficacy of TVR/PegIFN/RBV at post-treatment week 12
(SVR12) and 24 (SVR 24); HCV RNA <LLOQ
• Pharmacokinetics of TVR, PegIFN, RBV, and pre-
specified antiretroviral therapy (ART)
Sulkowski M et al. Hepatology 2012; 56(Suppl S1):219A

Telaprevir/PegIFN/RBV in HCV/HIV Co-Infected Patients
TVR=telaprevir; P=pegylated interferon; R=ribavirin; EFV=efavirenz; TDF=tenofovir disoproxil
fumarate; FTC=emtricitabine; ATR/r=ritonavir-boosted atazanavir; 3TC=lamivudine
Sulkowski M et al. Hepatology 2012; 56(Suppl S1):219A
Part A: No ART
TVR + PR PR
Pbo + PR PR
Part B: ART (EFV/TDF/FTC or ATV/r+TDF+FTC or 3TC)
TVR + PR PR
Pbo + PR PR
T/PR
1:1
PR48
(control)
T/PR
2:1
PR48
(control)
Weeks 0 12 24 36 48 60 72
SVR12
SVR12
SVR12
SVR12
SVR24
SVR24
SVR24
SVR24
Study Design: Randomized, Double-Blind, Placebo Controlled Trial

Telaprevir/PegIFN/RBV in HCV/HIV Co-Infected Patients
Sulkowski M et al. Hepatology 2012; 56(Suppl S1):219A
Methods
• PegIFN α-2a dosed at 180 g/week SC + RBV with TVR
or placebo for 12 weeks
– RBV dosed at 800 mg/day (n=33); 5 patients received weight-
based RBV per country-specific protocol in France and Germany
– TVR dosed at 750 mg q8h with atazanavir and 1125 mg q8h with
efavirenz
• HCV RNA assessed at days 1, 2, and 4; weeks 1, 2, 3,
4, 8, 12, 16, 20, 24, 28, 36, and 48; and post-treatment
follow-up visits
– Roche COBAS TaqMan HCV test v 2.9, LLOQ of 25 IU/mL

Telaprevir/PegIFN/RBV in HCV/HIV Co-Infected Patients
Sulkowski M et al. Hepatology 2012; 56(Suppl S1):219A
Methods (cont)
• Futility rules
– Discontinue TVR if HCV RNA >100 IU/mL at week 4 or 8
– Discontinue all HCV drugs if
• HCV RNA >1000 IU/mL or <2 log10 decrease from baseline at
week 12
• Detectable HCV RNA at week 24 or 36
• Viral breakthrough
– Defined as HCV RNA >100 IU/mL after not detected or a >1 log10
increase from adir
– Stop all HCV drugs

Telaprevir/PegIFN/RBV in HCV/HIV Co-Infected Patients
TVR=telaprevir; PegIFN=pegylated interferon; RBV=ribavirin; EFV=efavirenz; TDF=tenofovir disoproxil fumarate; FTC=emtricitabine; ATR/r=ritonavir-boosted atazanavir; 3TC=lamivudine Sulkowski M et al. Hepatology 2012; 56(Suppl S1):219A
Efficacy: SVR24
33%
71%
50%
69%
50%
80%
45%
74%
0
20
40
60
80
100
TVR/PegIFN/RBV PegIFN/RBV
SVR24
(%)
No ART EFV/TDF/FTC ATV/r/TDF/FTC Total
5/7 11/16 12/15 28/38 2/6 4/8 4/8 10/22

Telaprevir/PegIFN/RBV in HCV/HIV Co-Infected Patients
Sulkowski M et al. Hepatology 2012; 56(Suppl S1):219A
Virologic Outcome, n/N (%) TVR/PegIFN/RBV PegIFN/RBV
SVR 28/38 (74) 10/22 (45)
No SVR
Stopping rule
Viral relapse post-treatment
LLOQ at EOT
Lost to follow-up
10/38 (26)
2/38 (5)
1/32 (5)
3/38 (8)
4/38 (11)
12/22 (55)
8/22 (36)
2/13 (15)
2/22 (9)
0/222 (0)
HCV Treatment Outcome

Telaprevir/PegIFN/RBV in HCV/HIV Co-Infected Patients
Sulkowski M et al. Hepatology 2012; 56(Suppl S1):219A
Most common adverse events in >15% patients: TVR treatment phase (weeks 1 - 12)
N (%) TVR/PegIFN/RBV N=38
PegIFN/RBV N=22
Fatigue Pruritus Headache Nausea Rash Diarrhea Dizziness Pyrexia Depression Anemia Vomiting Myalgia Chills Insomnia
15 (39) 13 (34) 13 (34) 12 (32) 11 (29) 8 (21) 8 (21) 7 (18) 6 (16) 5 (13) 6 (16) 5 (13) 5 (13) 5 (13)
9 (41) 1 (5)
5 (23) 4 (18) 4 (18) 3 (14) 2 (9) 2 (9) 2 (9)
4 (18) 2 (9)
5 (23) 4 (18) 4 (18)

Telaprevir/PegIFN/RBV in HCV/HIV Co-Infected Patients
Sulkowski M et al. Hepatology 2012; 56(Suppl S1):219A
Events of special interest: Overall treatment phase
Adverse events, n (%) TVR/PegIFN/RBV N=38
PegIFN/RBV N=22
Severe rash 0 (0) 0 (0)
Mild or moderate rash 13 (34) 5 (23)
Any anemia (hemoglobin <10 g/dL) 7 (18) 4 (18)
Severe anemia (hemoglobin 7.0-8.9 g/dL or from baseline 4.5 g/dL)
1 (3) 1 (5)
Erythropoietin stimulating agent 3 (8) 1 (5)
Blood transfusions 4 (11) 1 (5)
Discontinuation due to AE 3 (8) 0 (0)
• No HIV breakthrough • CD4 counts declined in TVR/PegIFN/RBV and PegIFN/RBV groups • CD4% unchanged

Telaprevir/PegIFN/RBV in HCV/HIV Co-Infected Patients
TVR concentrations similar among patients with and without antiretroviral therapy
Sulkowski M et al. Hepatology 2012; 56(Suppl S1):219A

Telaprevir/PegIFN/RBV in HCV/HIV Co-Infected Patients
Efavirenz and atazanavir concentrations similar with and without telaprevir
Sulkowski M et al. Hepatology 2012; 56(Suppl S1):219A

Telaprevir/PegIFN/RBV in HCV/HIV Co-Infected Patients
Sulkowski M et al. Hepatology 2012; 56(Suppl S1):219A
Conclusions • Higher SVR24 rates were observed in chronic genotype 1
HCV/HIV co-infected patients treated with TVR combination therapy
– TVR/PegIFN/RBV: 74%
– PegIFN/RBV: 45%
• Drug interactions with TVR and select ART were clinically meaningful
– Increased dose of TVR with efavirenz compensated for CYP3A induction
– Telaprevir did not substantiallly modify ART exposure
– No HIV breakthroughs in patients on ART
• Overall safety and tolerability profile of TVR/PegIFN/RBV was comparable to that previously observed in HCV mono-infected patients

Timing and Magnitude of Ribavirin Dose Reduction (RBV DR) Do
Not Impact Sustained Virologic Response (SVR) Rates with
Boceprevir (BOC) + Peginterferon alfa-2b / Ribavirin (P/RBV) in the
Anemia Management Study in Chronic HCV Genotype 1 Patients
Poordad F, Lawitz E, Reddy KR, Afdhal N, Hezode C, Zeuzem S, Lee SS,
Calleja JL, Brown RS, Craxi A, Wedemeyer H, Bacon BR, Flamm SL, Deng W,
Koury KJ, Pedicone L, Dutko F, Burroughs M, Alves K, Wahl J, Brass C,
Albrecht JK, Sulkowski MS
Abstract 154, AASLD 2012
HCV Highlights from AASLD 2012
November 9 - 13, 2012 Boston, MA

RBV Dose Reduction for Anemia Management and
Impact on SVR Rates with Boceprevir/PegIFN/RBV
Therapy in HCV Genotype 1 HCV Patients
Objective
• To assess the impact of timing and magnitude of
ribavirin dose reduction (RBV DR) on SVR rates
in chronic HCV genotype 1 patients treated with
Boceprevir/PegIFN/RBV who develop on-
therapy anemia
Poordad F et al. Hepatology 2012; 56(Suppl S1):269A-270A.

RBV Dose Reduction for Anemia Management and
Impact on SVR Rates with Boceprevir/PegIFN/RBV
Therapy in HCV Genotype 1 HCV Patients
After 4-week lead-in
with P/RBV, all
patients initiated
boceprevir.
Hb at wk 0, 2, 4, 6,
8, 10, 12, 24,
28, 34, 40, 48.
Randomized if
Hb ~10 g/dl
EPO
(n=251)
RBV DR
(n=249)
If Hb≤8.5 g/dL,
secondary
intervention
(RBV DR arm
could use EPO;
EPO arm could
use RBV DR)
If Hb>10 g/dL, patients
treated but not randomized
(n=187)
Study Design
Poordad F et al. Hepatology 2012; 56(Suppl S1):269A-270A.

RBV Dose Reduction for Anemia Management and
Impact on SVR Rates with Boceprevir/PegIFN/RBV
Therapy in HCV Genotype 1 HCV Patients
Poordad F et al. Hepatology 2012; 56(Suppl S1):269A-270A.
Initial dosing
• PegIFN α-2b administered subcutaneously at 1.5 g/kg
once weekly, plus RBV using weight-based dosing of
600-1400 mg/day in a divided daily dose
Interventions for anemia
• RBV DR by increments of 200 mg at the discretion of the
investigator (first increment of 400 mg if initial dose was
1,400 mg/day)
• EPO was started at 40,000 units/wk and could be
modified at the investigator’s discretion to doses of
20,000 to 60,000 units/wk
• If Hb≤7.5 g/dL, all study drugs were discontinued

RBV Dose Reduction for Anemia Management and
Impact on SVR Rates with Boceprevir/PegIFN/RBV
Therapy in HCV Genotype 1 HCV Patients
10%
71%
82%
10%
71%
82%
0
20
40
60
80
100
EOT SVR Relapse
% of Patients
RBV DR
EPO
Primary Efficacy Results
203/
249
205/
251
178/
249
178/
251 19/ 196
19/ 197
Poordad F et al. Hepatology 2012; 56(Suppl S1):269A-270A.

RBV Dose Reduction for Anemia Management and
Impact on SVR Rates with Boceprevir/PegIFN/RBV
Therapy in HCV Genotype 1 HCV Patients
86% 86%
56% 56%
0
20
40
60
80
100
Undetectable Undetectable Detectable Detectable
RBV DR
EPO
SVRs Were Higher if Undetectable HCV RNA
at Start of Primary Anemia Management
111/
129
107/
124
67/
120 71/ 127
Poordad F et al. Hepatology 2012; 56(Suppl S1):269A-270A.
SVR (%)
HCV RNA at Start of Primary Anemia Management

RBV Dose Reduction for Anemia Management and
Impact on SVR Rates with Boceprevir/PegIFN/RBV
Therapy in HCV Genotype 1 HCV Patients
71%
82%79%
64%70% 71%
88%
70%68%71%
0
20
40
60
80
100
>4-8 wks >8-12 wks >12-16 wks >16 wks
SVR (%)
RBV DR
EPO Use
SVR rates did not vary with the start time of anemia management
38/
54
39/
55
58/
90
60/
88
Poordad F et al. Hepatology 2012; 56(Suppl S1):269A-270A.
17/
24
15/
21
15/
17
18/
22
47/
67
49/
62
Timing of the start of anemia management
4 wks

RBV Dose Reduction for Anemia Management and
Impact on SVR Rates with Boceprevir/PegIFN/RBV
Therapy in HCV Genotype 1 HCV Patients
83%
69%77%
64%
80%76%
67%
0
20
40
60
80
100
1 2 3 4 5 6 7
SVR (%)
SVR did not vary by number of steps* of RBV dose reduction
47/
70
44/
58
20/
25
*Step = decrease of 200 mg RBV/day for 3 days
Poordad F et al. Hepatology 2012; 56(Suppl S1):269A-270A.
10/
12
24/
35
23/
30
9/
14
Number of RBV DR Steps*
RBV DR arm only

RBV Dose Reduction for Anemia Management and
Impact on SVR Rates with Boceprevir/PegIFN/RBV
Therapy in HCV Genotype 1 HCV Patients
33%36%
67%
77%75%70%
60%
92%
0
20
40
60
80
100
0 200 400 600 800 1000 1200 1400
SVR
(%)
SVR rates by lowest RBV dose received
for 14 days
11/
12
3/
5
28/
40
Poordad F et al. Hepatology 2012; 56(Suppl S1):269A-270A.
1/
3
30/
45
43/
56
58/
77
Lowest RBV dose (mg/day) for 14 days
RBV DR arm only
4/
11

RBV Dose Reduction for Anemia Management and
Impact on SVR Rates with Boceprevir/PegIFN/RBV
Therapy in HCV Genotype 1 HCV Patients
92%89%
77%74%
18%
0
20
40
60
80
100
<50 50<60 60<70 70<80
SVR
(%)
SVR by Percent Total RBV Dose Received
Over the Treatment Period
10/
57
14/
19
Poordad F et al. Hepatology 2012; 56(Suppl S1):269A-270A.
34/
38
20/
26
Percent of total RBV dose received vs assigned RBV dose
for entire treatment period
RBV DR arm only
100/
109
80

RBV Dose Reduction for Anemia Management and
Impact on SVR Rates with Boceprevir/PegIFN/RBV
Therapy in HCV Genotype 1 HCV Patients
92%89%
83%75%
67%
0
20
40
60
80
100
<50 50<60 60<70 70<80
SVR
(%)
SVR by Percent Total RBV Dose Received in Patients
Who Received ≥80% of Treatment Duration
6/
9
9/
12
Poordad F et al. Hepatology 2012; 56(Suppl S1):269A-270A.
34/
38
20/
24
Percent of total RBV dose received vs assigned RBV dose
for entire treatment period
RBV DR arm only
100/
109
80

RBV Dose Reduction for Anemia Management and
Impact on SVR Rates with Boceprevir/PegIFN/RBV
Therapy in HCV Genotype 1 HCV Patients
Predictors of Anemia by Logistic Regression*
* Logistic Regression; Stepwise selected; All treated patients
† Normal ITPA activity = C at rs1127354 & A at rs7270101 for both haplotypes
Poordad F et al. Hepatology 2012; 56(Suppl S1):269A-270A.
Effect Odds Ratio 95% CI P-value
Baseline Hemoglobin
(continuous variable) 0.62 0.49 – 0.79 <0.0001
Normal ITPA Activity† 1.96 1.28 – 3.00 0.0019
Age (>40 vs ≤40) 1.98 1.19 – 3.28 0.0084
Baseline Fibrosis
(3/4 vs 0/1/2) 2.02 1.03 – 3.98 0.0421
RBV Dose Reduction for Anemia Management and
Impact on SVR Rates with Boceprevir/PegIFN/RBV
Therapy in HCV Genotype 1 HCV Patients
Poordad F et al. Hepatology 2012; 56(Suppl S1):269A-270A.
Conclusions
• SVR rates were similar with RBV dose reduction regardless
of: 1) The timing of the first RBV reduction, 2) The number of
steps of RBV dose reductions, or, 3) The lowest RBV dose
received to manage anemia
• Similar SVRs with RBV DR or EPO if HCV RNA was
detectable at time of anemia management; similar SVRs with
RBV DR or EPO if HCV RNA was undetectable at time of
anemia management
• SVR rates were lower if <50% of the intended total RBV dose
assigned per-protocol was administered
• RBV dose reduction is the preferred first strategy for anemia
management

OPTIMIZE Trial: Non-Inferiority of Twice-Daily
Telaprevir Versus Administration Every 8 Hours in
Treatment-Naïve, Genotype 1 HCV Infected Patients
Buti M, Agarwa K, Horsmans YJ, Sievert W, Janczewska E, Zeuzem S, Nyberg L,
Brown RS, Hezode C, Rizzetto M, Paraná R, De Meyer S, Luo D, Witek J
Abstract LB8, AASLD 2012
HCV Highlights from AASLD 2012
November 9 - 13, 2012 Boston, MA

Twice-daily Telaprevir vs. Administration Every 8 Hours
in Treatment-Naïve Genotype 1 HCV Patients
Objective
• To investigate the use of telaprevir (TVR) twice
daily (bid) vs. every 8 hours (q8h) in combination
with PegIFN/RBV in treatment-naïve patients
with chronic genotype 1 HCV infection
Buti M et al. Abstract LB-8. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012

Twice-daily Telaprevir vs. Administration Every 8 Hours
in Treatment-Naïve Genotype 1 HCV Patients
Buti M et al. Abstract LB-8. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012
TVR +
PegIFN +
RBV
Peg-IFN +
RBV
Peg-IFN + RBV
TVR +
PegIFN +
RBV
Peg-IFN +
RBV
Peg-IFN + RBV
T12 (750 mg q8h)/PR (N=371)
T12 (1125 mg bid)/PR (N=369)
RVR+
RVR-
RVR+
RVR-
Follow-up Follow-up
Follow-up Follow-up
Optimize Study Design
Follow-up
Follow-up
0 12 24 36 48 60 72 Time (weeks)

Twice-daily Telaprevir vs. Administration Every 8 Hours
in Treatment-Naïve Genotype 1 HCV Patients
Buti M et al. Abstract LB-8. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012
74%74%73%
0
20
40
60
80
100
T12(q8h)/PR T12(bid)/PR All patients
270/ 371
274/ 369
544/ 740
SVR12 (%)
Efficacy: SVR12

Twice-daily Telaprevir vs. Administration Every 8 Hours
in Treatment-Naïve Genotype 1 HCV Patients
Buti M et al. Abstract LB-8. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012
65%68%
87%
66%68%
92%
65%68%
90%
0
20
40
60
80
100
CC CT TT
92/ 106
141/ 208
37/ 57
SVR12 (%)
Efficacy: SVR12 by IL28B Genotype
97/ 105
189/ 211
139/ 206
280/ 414
38/ 58
75/ 115
IL28B Genotype
T12(q8h)/PR
T12(bid)/PR
All patients

Twice-daily Telaprevir vs. Administration Every 8 Hours
in Treatment-Naïve Genotype 1 HCV Patients
Buti M et al. Abstract LB-8. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012
59%
78%
58%
81%
59%
79%
0
20
40
60
80
100
F0-F2 F3-F4
209/ 268
61/ 103
SVR12 (%)
Efficacy: SVR12 by Liver Disease Status
213/ 264
422/ 532
61/ 105
122/ 208
Liver Disease Status
T12(q8h)/PR
T12(bid)/PR
All patients

Twice-daily Telaprevir vs. Administration Every 8 Hours
in Treatment-Naïve Genotype 1 HCV Patients
*SSC=Special search category: Grouped AE terms representing similar medical concepts
Buti M et al. Abstract LB-8. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012
Adverse event, n (%)
T12(q8h)/PR
(N=371)
T12(bid)/PR
(N=369)
All patients
(N=740)
Any adverse event 367 (99) 360 (98) 727 (98)
Serious adverse event
Death
35 (9)
1 (<1%)
28 (8)
0
63 (9)
1 (<1%)
Any Grade 3 adverse event
Grade 3 anemia SSC*
Grade 3 rash SSC*
139 (38)
70 (19)
22 (6)
156 (42)
95 (26)
18 (5)
295 (40)
165 (22)
40 (5)
Any Grade 4 adverse event 24 (7) 23 (6) 47 (6)
Any adverse event leading to
permanent discontinuation of TVR
69 (19) 57 (15) 126 (17)
Any treatment-related adverse event
considered possibly related to TVR
335 (90) 344 (93) 679 (92)
Adverse events during the TVR treatment phase

Twice-daily Telaprevir vs. Administration Every 8 Hours
in Treatment-Naïve Genotype 1 HCV Patients
*Adverse events occurring in >25% in all patients in any group SSC=Special search category: Grouped AE terms representing similar medical concepts
Buti M et al. Abstract LB-8. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012
Most frequent AEs, n (%)*
T12(q8h)/PR
(N=371)
T12(bid)/PR
(N=369)
All patients
(N=740)
Fatigue 177 (48) 173 (47) 350 (47)
Pruritus SSC 171 (46) 170 (46) 341 (46)
Anemia SSC 162 (44) 167 (45) 329 (45)
Nausea 142 (38) 128 (35) 270 (37)
Rash SSC 199 (54) 189 (51) 388 (52)
Headache 107 (29) 87 (24) 194 (26)
Adverse events during the TVR treatment phase

Twice-daily Telaprevir vs. Administration Every 8 Hours
in Treatment-Naïve Genotype 1 HCV Patients
Buti M et al. Abstract LB-8. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012
Conclusions
• SVR12 rates for TVR 1125 mg bid were noninferior to
TVR 750 mg q8h (74% vs. 73%, respectively)
• SVR 12 outcomes for T12(bid)/PR and T12(q8h)/PR
were similar regardless of liver fibrosis status and IL28B
genotype
• The safety and tolerability profile of T12(bid)/PR and
T12(q8h)/PR was similar between treatment groups
• Similar SVR and AE rates achieved with 1125 mg bid
TVR and 750 mg q8h TVR offers the potential of a
simplified dosing regimen for genotype 1 HCV patients

Treatment of Hepatitis C Genotype 1 Patients with
Severe Fibrosis or Compensated Cirrhosis: The
International Telaprevir Early Access Program
Colombo M, Fernández I, Abdurakhmanov D, Abrão Ferreira PR, Strasser SI,
Urbanek P, Moreno C, Streinu-Cercel A, Verheyen A, Iraqi W, DeMasi R, Hill A,
Läuffer JM, Lonjon-Domanec I, Wedemeyer H
Abstract LB-15, AASLD 2012
HCV Highlights from AASLD 2012
November 9 - 13, 2012 Boston, MA

Treatment of Hepatitis C Genotype 1 Patients with
Severe Fibrosis or Compensated Cirrhosis With
Telaprevir/PegIFN/RBV: Interim Analysis
Objective
• To assess efficacy and safety of telaprevir (TVR)
in combination with PegIFN/RBV in treatment
naïve and treatment experienced patients with
genotype 1 hepatitis C with severe fibrosis or
compensated cirrhosis
Colombo M et al. Abstract LB-15. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012

Treatment of Hepatitis C Genotype 1 Patients with
Severe Fibrosis or Compensated Cirrhosis With
Telaprevir/PegIFN/RBV: Interim Analysis
Methods
• Required at entry: Liver biopsy or noninvasive tests
showing severe fibrosis (Metavir F3 or Ishak 3-4) or
cirrhosis (Metavir F4 of Ishak 5-6) and platelet count
>90,000/mm3
• Inclusion criteria: Genotype 1, severe fibrosis (F3) or
compensated cirrhosis (F4)
• 1,900 patients recruited to date; first 609 patients with
data to week 16 included in interim analysis
Colombo M et al. Abstract LB-15. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012

Treatment of Hepatitis C Genotype 1 Patients with
Severe Fibrosis or Compensated Cirrhosis With
Telaprevir/PegIFN/RBV: Interim Analysis
Methods (cont)
• Patients were treated with telaprevir 750 mg every 8
hours (q8h) and PegIFN/RBV (dosed according to label)
for 12 weeks
– Treatment-naïve or prior treatment relapsers: After week 12,
PegIFN/RBV was given for an additional 12-36 weeks,
depending on the initial virological response observed
– Previously treated patients with prior partial or prior null
response: After week 12, PegIFN/RBV was given for an
additional 36 weeks
Colombo M et al. Abstract LB-15. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012

Treatment of Hepatitis C Genotype 1 Patients with
Severe Fibrosis or Compensated Cirrhosis With
Telaprevir/PegIFN/RBV: Interim Analysis
Colombo M et al. Abstract LB-15. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012
Treatment-naïve or prior treatment relapsers
Telaprevir 750
mg q8h +
PegIFN/RBV
PegIFN/RBV Follow-up
PegIFN/RBV Follow-up
Previously treated with prior partial or prior null response
Telaprevir 750
mg q8h +
PegIFN/RBV
PegIFN/RBV
Follow-up
Study Design
0 12 24 48 72
Time (weeks)

Treatment of Hepatitis C Genotype 1 Patients with
Severe Fibrosis or Compensated Cirrhosis With
Telaprevir/PegIFN/RBV: Interim Analysis
Baseline characteristics
• Treatment-naïve: 20%
• Prior relapsers: 28%
• Prior partial responders: 15%
• Prior null responders: 29%
• Non-responders (unspecified): 3%
• Prior viral breakthrough: 5%
• HCV RNA levels 800,000 IU/mL: 66%
• Severe fibrosis: 45%
• Cirrhosis: 55%
• HCV genotype 1a: 28%
Colombo M et al. Abstract LB-15. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012

Treatment of Hepatitis C Genotype 1 Patients with
Severe Fibrosis or Compensated Cirrhosis With
Telaprevir/PegIFN/RBV: Interim Analysis
Colombo M et al. Abstract LB-15. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012
77%82%
68%
80%80%86%
54%
68%
41%
52%
63% 59%
0
20
40
60
80
100
Naive Relapser Partial
Responder
Null
Responder
Viral
Breakthrough
Overall
Week 4 Viral Response
Patients (%)
HCV RNA <25 IU/mL
HCV RNA not detected
(n=124) (n=171) (n=94) (n=176) (n=28) (n=609)

Treatment of Hepatitis C Genotype 1 Patients with
Severe Fibrosis or Compensated Cirrhosis With
Telaprevir/PegIFN/RBV: Interim Analysis
Colombo M et al. Abstract LB-15. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012
83%89%
76%
85%87%88%
79%
86%
68%
77%
85% 85%
0
20
40
60
80
100
Naive Relapser Partial
Responder
Null
Responder
Viral
Breakthrough
Overall
Week 12 Viral Response
Patients (%)
HCV RNA <25 IU/mL
HCV RNA not detected
(n=124) (n=171) (n=94) (n=176) (n=28) (n=609)

Treatment of Hepatitis C Genotype 1 Patients with
Severe Fibrosis or Compensated Cirrhosis With
Telaprevir/PegIFN/RBV: Interim Analysis
Anemia • Patients developing anemia up to week 16
– Grade 1-4 anemia (Hb <11 g/dL or >2.5 g/dL ): 359/609 (59%)
– Grad 3 or Grade 4 anemia (Hb <9 g/dL or >4.5 g/dL ): 189/609
(31%)
• Management of anemia
– Reduced RBV dose: 171/609 (28%)
– Received erythropoietin: 148/609 (24%)
– Received transfusions: 70/609 (11.5%)
– Discontinued TVR treatment due to anemia: 19/609 (3%)
Colombo M et al. Abstract LB-15. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012

Treatment of Hepatitis C Genotype 1 Patients with
Severe Fibrosis or Compensated Cirrhosis With
Telaprevir/PegIFN/RBV: Interim Analysis
*SSC=Special search category: Grouped AE terms representing similar medical concepts
Colombo M et al. Abstract LB-15. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012
Adverse event, n (%)
F3
(n=273)
F4
(n=335)
All
(n=609)
Subjects with one or more Grade
2 or higher treatment related AEs
171 (62.6) 247 (73.7) 418 (68.6)
Anemia SSC 101 (37.0) 172 (51.3) 273 (44.8)
Rash SSC 42 (15.4) 52 (15.5) 94 (15.4)
Thrombocytopenia 15 (5.5) 45 (13.4) 60 (9.9)
Pruritus SSC 19 (7.0) 32 (9.6) 51 (8.4)
Asthenia 23 (8.4) 27 (8.1) 50 (8.2)
Nausea 12 (4.4) 24 (7.2) 36 (5.9)
Anorectal SSC 14 (5.1) 21 (6.3) 35 (5.7)
Grade 2-4 drug-related AEs ( 5%) by fibrosis stage--until week 16

Treatment of Hepatitis C Genotype 1 Patients with
Severe Fibrosis or Compensated Cirrhosis With
Telaprevir/PegIFN/RBV: Interim Analysis
*SSC=Special search category: Grouped AE terms representing similar medical concepts
Colombo M et al. Abstract LB-15. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012
Adverse event, n (%)
F3
(n=273)
F4
(n=335)
All
(n=609)
Subjects with one or more AEs
leading to discontinuation
32 (11.7) 53 (15.8) 85 (14.0)
Rash SSC 15 (5.5) 15 (4.5) 30 (4.9)
Anemia SSC 3 (1.1) 16 (4.8) 19 (3.1)
Asthenia 3 (1.1) 4 (1.2) 7 (1.1)
Abdominal pain 1 (0.4) 5 (1.5) 6 (1.0)
Nausea 3 (1.1) 3 (0.9) 6 (1.0)
Pruritus SSC 1 (0.4) 5 (1.5) 6 (1.0)
Vomiting 4 (1.5) 2 (0.6) 6 (1.0)
Discontinuation of TVR due to AEs: Reported by 1% of patients-- until week 16

Treatment of Hepatitis C Genotype 1 Patients with
Severe Fibrosis or Compensated Cirrhosis With
Telaprevir/PegIFN/RBV: Interim Analysis
Colombo M et al. Abstract LB-15. Presented at The Liver Meeting 2012, Boston, MA, November 9-13, 2012
Conclusions
• A treatment week 16 interim analysis of 609
patients with severe fibrosis or compensated
cirrhosis treated with TVR/PegIFN/RBV found:
– 79% had undetectable HCV RNA by week 12
– HCV RNA responses at week 12 were lower for prior
null responders compared with treatment-naïve
patients, prior relapsers or prior partial responders
– Serious AEs occurred in 14% of patients and
discontinuation due to anemia or rash was similar to
Phase III registration trials