head injury fm brett md frcpath. at the end of this lecture you should be able to: 1.know basic...
TRANSCRIPT

Head injury
FM Brett MD FRCPath
At the end of this lecture you should be able to:
1. Know basic facts about the incidence of head injury
2. Know the difference between focal and diffuse injury
3. Know the difference between missile and non-missile head injury
4. Be able to classify ICH
5. Know the difference between traumatic and spontaneous SAH
6. Be able to list the complications of Raised ICP

Head Injury - Facts
• Whether accidental, criminal or suicidalleading cause of death < 45• Accounts 1% of all deaths, 30% traumaticdeaths and 50% of RTA deaths• Severity assessed by GCS
GCS
1. Best eye response - (max 4)2. Best verbal response - (max 5)3. Best motor response - (max 6)
GCS- 13+ mild H I9-12- moderate H I8 or less – severe H I

HI
• May result in LOC• Longer unconscious and deeper coma >likelihood that pt has suffered severe HI• 60% good recovery• Based on US, UK and Netherland figuresfor every 100 HI, 5 VS, 15 severely disabled, 20 minor problems, 60 full recovery

Nature of lesions in HI
• Non - missile- RTA• Missile
Distribution of lesions• Focal• Diffuse
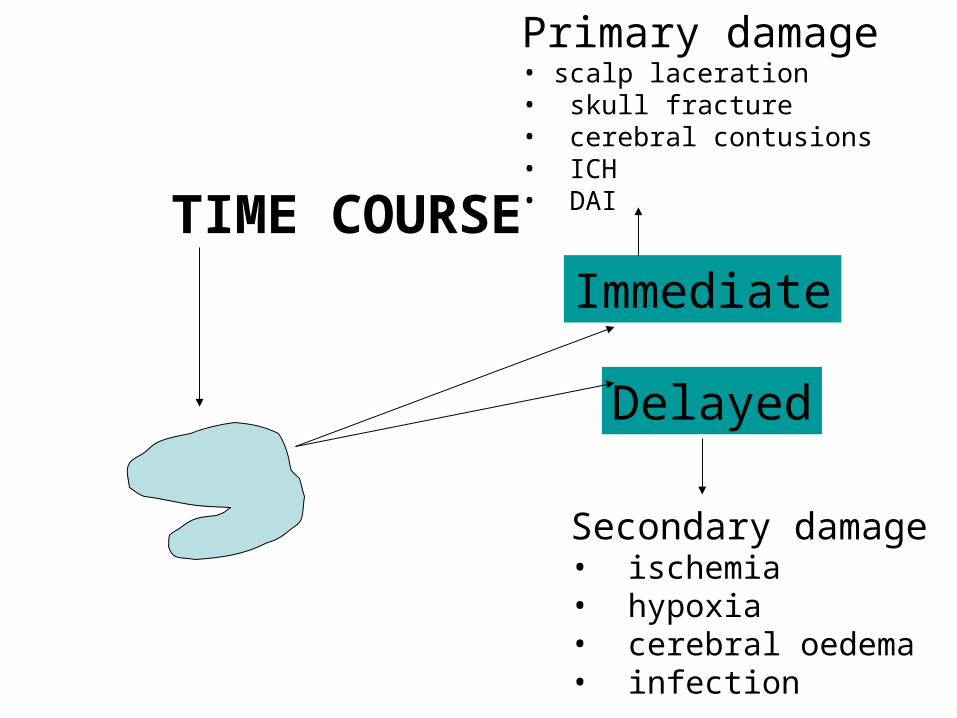
TIME COURSE
Immediate
Delayed
Primary damage• scalp laceration• skull fracture• cerebral contusions• ICH• DAI
Secondary damage• ischemia• hypoxia• cerebral oedema• infection

Pattern of damage in non -missile HIPattern of damage in non -missile HI
FocalFocalScalp- contusion, lacerationSkull - fractureMeninges - haemorrhage, infectionBrain - contusions, laceration, infection
Diffuse damageDiffuse damageBrain, DAI, DVI, HIE, Cerebral oedema

ICH is a complication of 66% of cases of non-missile head injury

HaemorrhageHaemorrhage
May be
EXTRADURAL
INTRADURAL - subdural, subarachnoid intracerebral

EDH
• Found in 2% HI
• Usually associated with skull fracture • Peak 10-30 yrs
• Rare < 2 and >60
• Arterial bleed - usually meningeal vessels
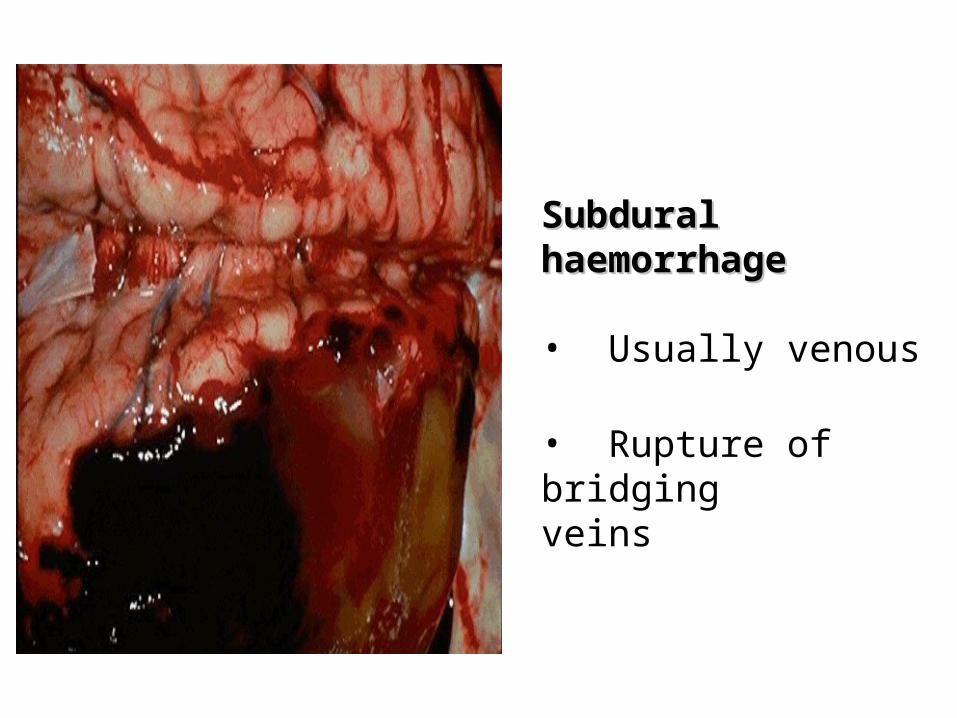
Subdural haemorrhageSubdural haemorrhage
• Usually venous
• Rupture of bridgingveins
Subdural haematoma: classification
48-72 hours – acute composed of clotted blood
3-20 dys – subacute – mixture of clotted and fluid blood
3 weeks + - chronic encapsulated haematoma

SAH
• Berry aneurysm• Traumatic• Infectious• Fusiform aneurysm• AVM• CAA
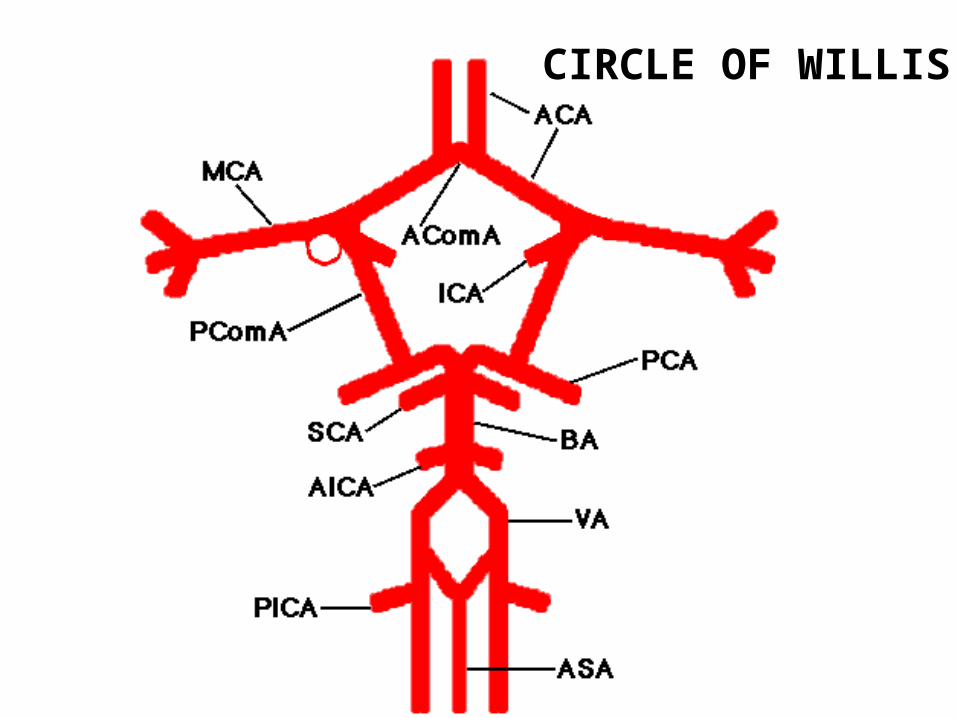
CIRCLE OF WILLIS

Berry aneurysms
Congenital
Risk of bleeding inc;• Hypertension• AVM • systemic vascular disease• defects collagen• polcystic renal disease

Traumatic SAH
• may result from severe contusions• Fracture of skull can rupture vessels• IVH may enter SAS
• RULE OUT ANEURYSMRULE OUT ANEURYSM
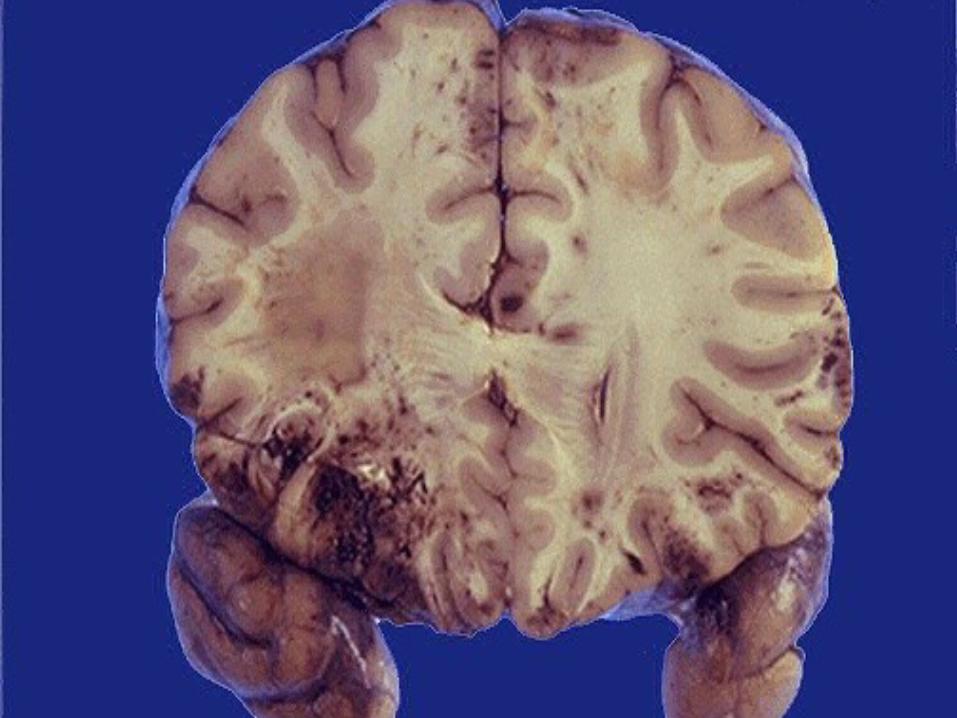
Cerebral contusionsCerebral contusions
• Superficial bruises of the brain
• Frequent but not inevitable afterhead injury

Various types of surface contusions and lacerations
~ Coup – at point of impact~ Contrecoup- diametrically opposite point
of impact~ Herniation – at point of impact between
hernia~ Fracture related to # of skull

Sites of cerebral contusionsSites of cerebral contusions
• Frontal poles• Orbital surfaces of the frontal poles• Temporal poles• lateral and inferior surfaces of occipital poles• cortex adjacent to sylvian fissure
Uncommon types of focal brain damageUncommon types of focal brain damage
• Ischaemic brain damage due to traumaticdissection and thrombosis of vertebral or carotidarteries by hyperextension of the neck• Infarction of pituitary - due to transection of pituitary stalk• pontomedullary rent

InfectionInfection
• complication of skull fracture• Open HI• Incidence is increased even after closedHI as devitalised tissue prone to infection
Diffuse brain injury – term coined by clinicans to describe head-injured patients who have global disruption of neurological function without a lesion on CT scan thatwould account for their clinical state
Implies widespread structural damage which neuropathologically is likely to be traumatic or hypoxic/ischaemic in origin
Diffuse damageDiffuse damage
• DAI - widespread damage to axons in theCNS due to acceleration/deceleration of the head• Pts usually unconscious from moment of impact• Lesser degrees compatible with recovery of consciousness
Pathogenesis of DAI
• Primary axotomy - almost immediate
• Large axolemmal tears- influx of CA++- activation of calcium activated proteases- severe cytoskeletal disruption- disconnection

Secondary axotomy
• Ca++ activated proteases focally damage thethe axonal BUTBUT immediate disconnection does not occur • Failure of cellular repair mechanisms or secondary neuronal damage results in axonaldisconnection• Axoplasmic transport continues and results in proximal axonal swelling
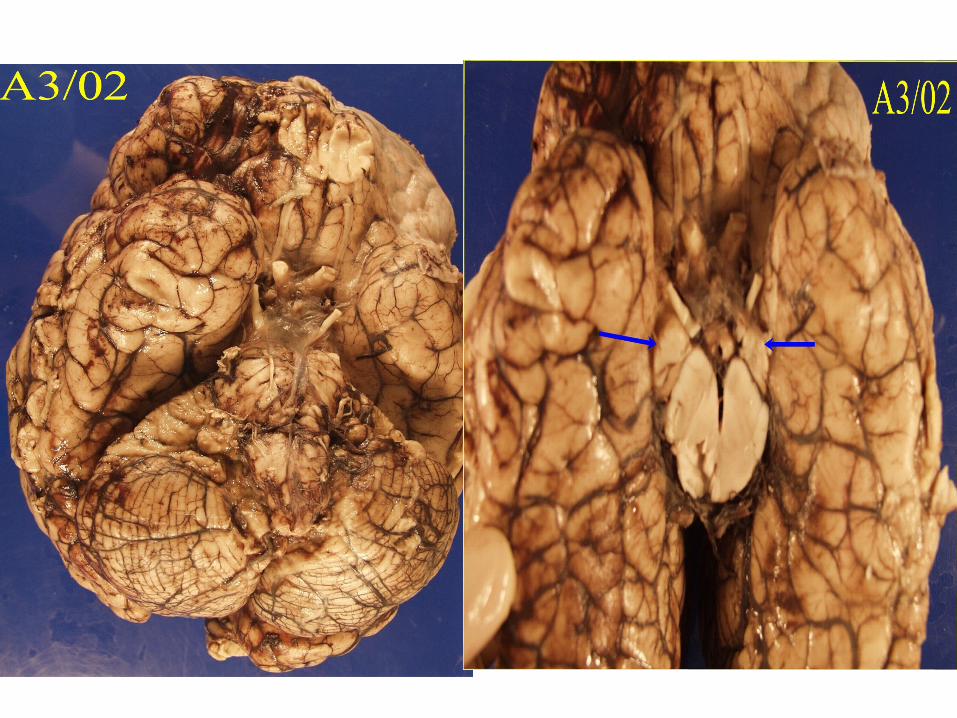
Diffuse vascular injuryDiffuse vascular injury
Multiple petechial haemorrhages inthe white matter of the frontal and temporal lobes
Probably results from traction and shearingof parenchymal BV
Brain swelling and raised ICPBrain swelling and raised ICP
Results from:• cerebral vasodilation - inc cerebral blood vol• damage to BV - escape of fluid through BBB• inc water content of neurones and glia- cytotoxiccerebral oedema
Three patterns of brain swelling in Three patterns of brain swelling in HIHI
• Swelling adjacent to contusions
• Diffuse swelling of one cerebral hemispheree.g evacuation of ASDH
• Diffuse swelling both hemispheres

ICH Herniation
SubfalcineSubfalcineherniationherniation
Tentorial herniationTentorial herniation
Tonsillar herniationTonsillar herniation

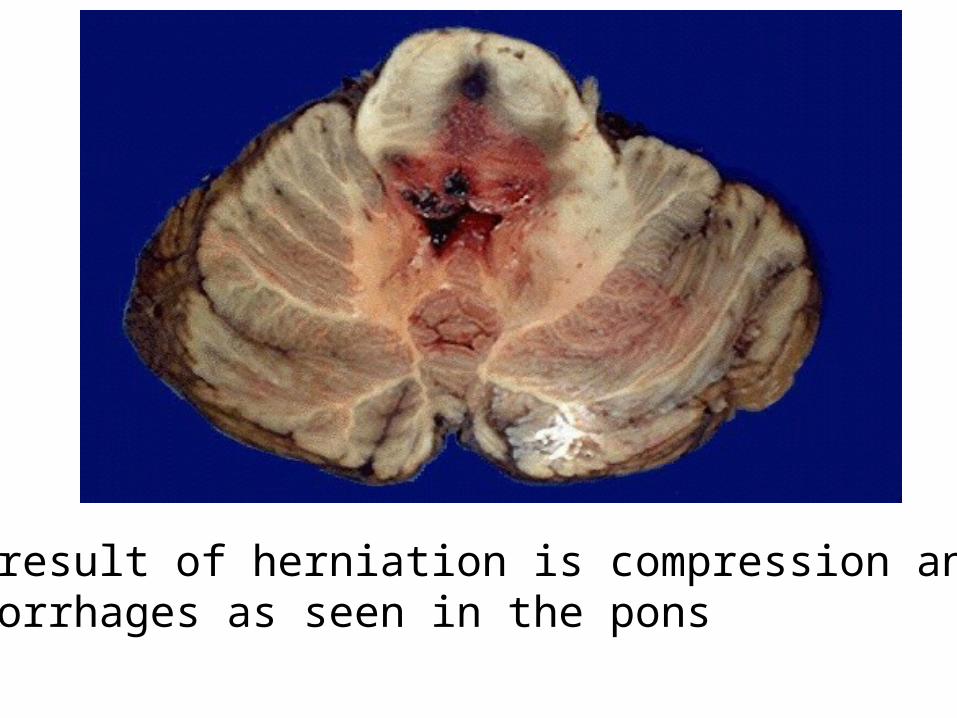
End result of herniation is compression and Duret haemorrhages as seen in the pons
Ischemic damage - likely if:Ischemic damage - likely if:
• clinically evident hypoxia• hypotension with systolic < 80mmHg for at least 15 mins • episodes of inc BP i.e > 30 mm Hg

MISSILE HEAD INJURYMISSILE HEAD INJURY
• Caused by objects propelled through air
Injury may be: • Depressed• Penetrating• Perforating

Traumatic spinal cord injuryTraumatic spinal cord injury
Nature of lesions - Indirect/direct
Distribution - 60-70% cervical, 25% thoracic, 6-15% lumbar.
Fractures C1/2, C4-7, T11-L2

Principal causes of spinal cord compression
~ Lesions in vertebral column- prolapsed disc, kyphoscoliosis, #, Metastatic tumour
~ Spinal extradural lesions – metastatic carcinoma, lymphoma, myeloma,abscess
~ Intradural extramedullary lesions – Meningioma, Schwannoma
~ Intramedullary lesions - Astrocytoma, ependymoma, cyst formation
CONCLUSIONS
~ HI – leading cause of death under age of 45
~ Can be missile or non-missile.
~ Distribution of lesions – focal or diffuse.
~ ICH may be extradural or intradural
~ SAH may be traumatic or spontaneous
~ Main complication of HI is raised ICP.