headache dr nick pendleton march 2015. headache tension type headache cranial nerve examination...
TRANSCRIPT
HEADACHEDr Nick PendletonMarch 2015
Headache• Tension Type Headache• Cranial Nerve Examination• Migraine• Migraine Treatment• Medication Overuse Headache• Headache Red Flags• Sinusitis Headache• Raised ICP Headache• Acute Severe Headache
Small Group Work• Tension Type Headache• Cranial Nerve Examination• Migraine• Migraine Treatment• Medication Overuse Headache• Headache Red Flags• Sinusitis Headache• Raised ICP Headache• Acute Severe Headache
NICE GUIDELINE CG150
Diagnosis and Management of Headaches in Young People and Adults
https://www.nice.org.uk/guidance/cg150
DIAGNOSTIC CRITERIA FOR TTH
(A)At least 10 episodes fulfilling the criteria B-D:
(B) Headache lasting from 30 minutes to 7 days(C) Headache has at least two of the following characteristics:Bilateral locationPressing/tightening (non-pulsating) qualityMild or moderate intensityNot aggravated by routine physical activity such as walking or
climbing stairs(D) Both of the following:No nausea or vomiting (anorexia may occur)No more than one episode of photophobia or phonophobia(E) Not attributable to another disorder
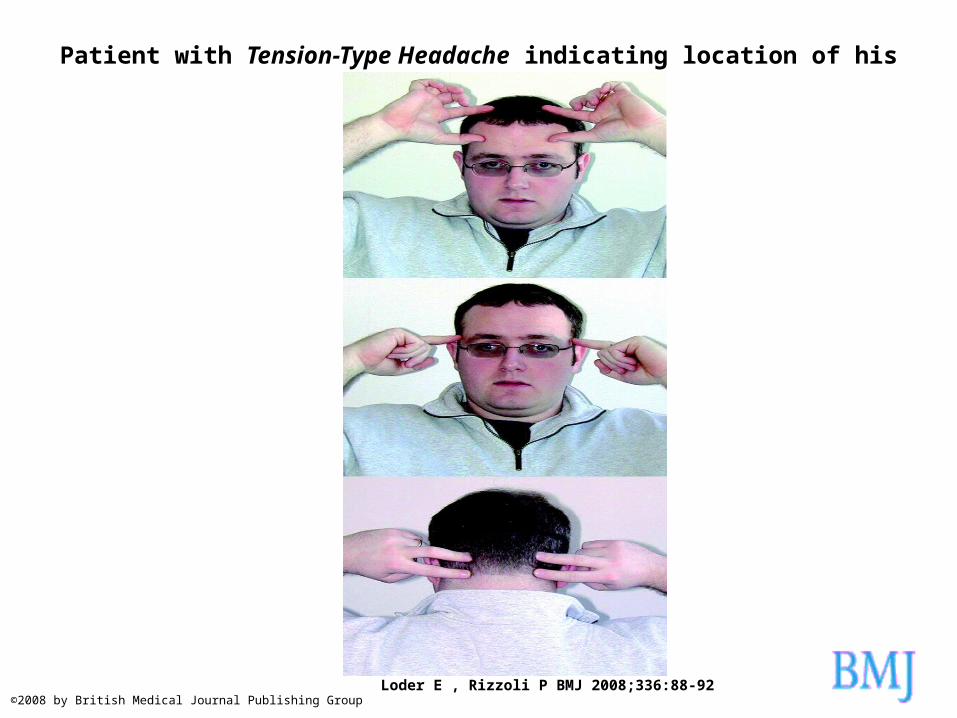
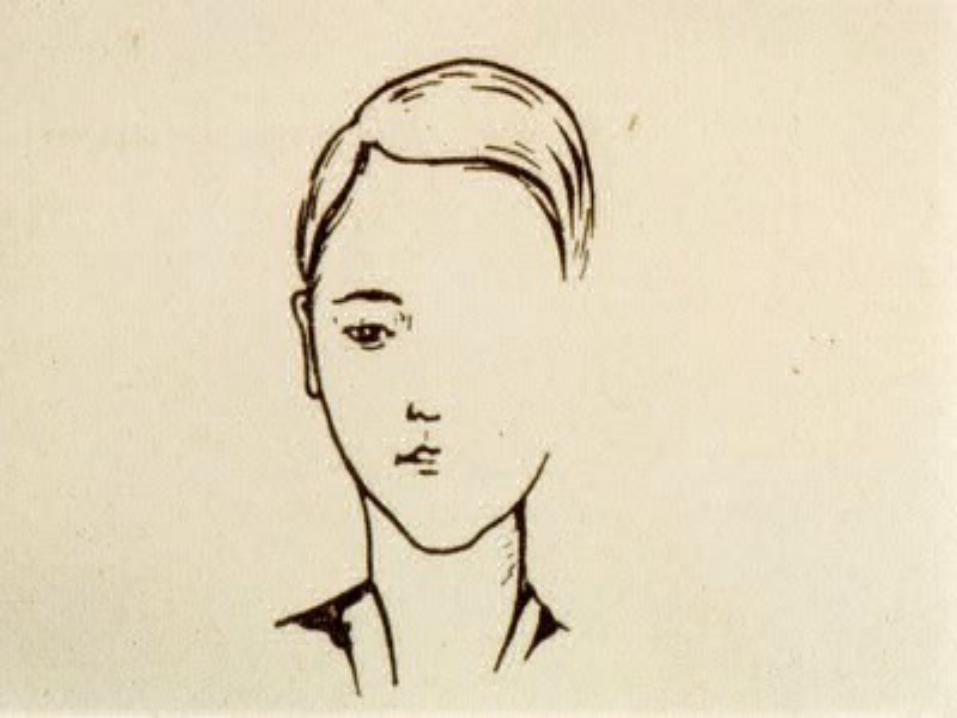
Patient with Tension-Type Headache indicating location of his headache pain.
Loder E , Rizzoli P BMJ 2008;336:88-92©2008 by British Medical Journal Publishing Group
DIAGNOSTIC CRITERIA FOR TTH
Infrequent episodic tension-type headacheDiagnosed if headaches meeting the above criteria occur <1 day a month (<12 days a year) on average
Frequent episodic tension-type headacheDiagnosed if headaches occur >1 and <15 days a month (>12 and <180 days a year).
Chronic tension-type headacheDiagnosed if headaches occur ≥15 days a month (180 or more days a year).
RED FLAGS• Onset of new or different headache• Nausea or vomiting• Worst headache ever experienced• Progressive visual or neurological
changes• Paralysis• Weakness, ataxia or loss of co-
ordination• Drowsiness, confusion, memory
impairment or loss of consciousness• Onset of headache after age of 50 years
More RED FLAGS
• Symptoms/Signs of Papilloedema• Stiff neck• Onset of headache with exertion, sexual
activity or coughing• Systemic illness• Numbness• Asymmetry of pupillary response • Sensory loss• Signs of meningeal irritation

Link to Article about Red Flags
• http://www.gponline.com/red-flag-symptoms-headaches/neurology/headache-migraine/article/1332134


MIGRAINE

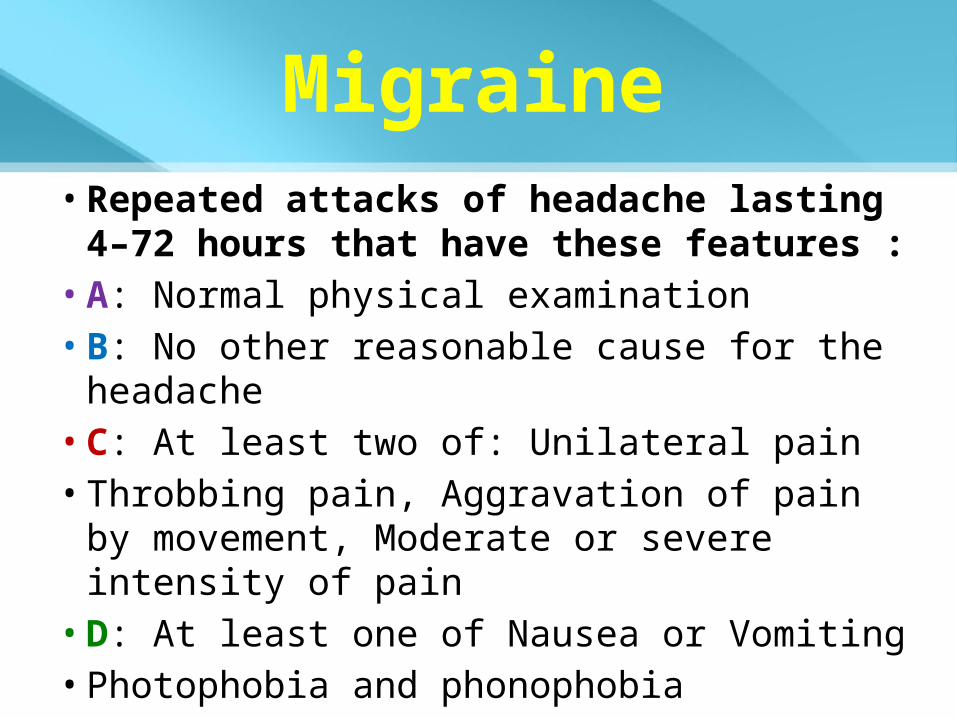
Migraine• Repeated attacks of headache lasting 4–72
hours that have these features :• A: Normal physical examination• B: No other reasonable cause for the headache• C: At least two of: Unilateral pain• Throbbing pain, Aggravation of pain by
movement, Moderate or severe intensity of pain
• D: At least one of Nausea or Vomiting• Photophobia and phonophobia
MIGRAINE WITH AURA
• 20–30% experience migraine with aura• Focal neurological phenomena that
precede the attack• Appear gradually over 5 to 20 minutes
and generally last fewer than 60 minutes• Headache phase usually begins within 60
minutes of the end of the aura phase.
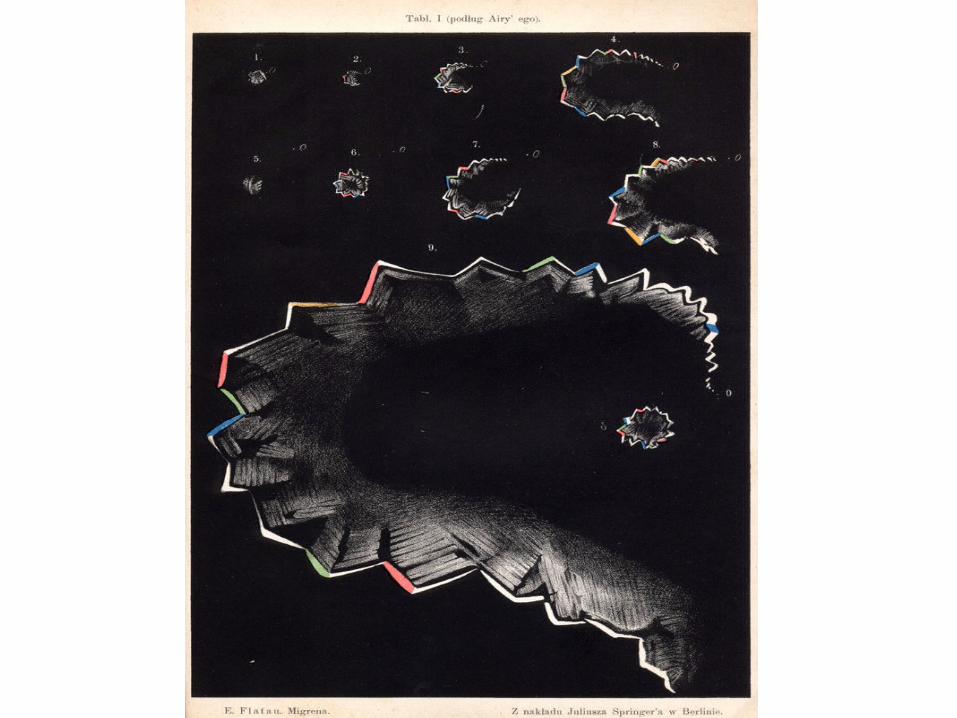
AURA
• Common aura symptoms include:• Visual disturbances (such as
flashing/flickering lights, zigzag lines and even temporary blindness)
• Numbness, tingling sensations and slurred speech.
• Other aura symptoms include a stiff neck, weakness on one side, partial paralysis, confusion or fainting
Migraine, Stroke and the OCP
• Patients who have Migraine with Aura are at increased risk of ischaemic stroke
• Giving these patients an OCP increases this risk significantly
• + Hypertension• + Smoking• + age > 35
Some figures: • In Women under 35:
• those who do not have migraine and do not take the pill (i.e. the background risk): 1.3 per 100,000 women per year are at risk of stroke
• those who have migraine without aura but don’t take the pill: 4 per 100,000 women per year at risk of stroke
• those who have migraine with aura but don’t take the pill: 8 per 100,000 women per year are at risk of stroke
• those who don’t have migraine and take the pill: 5 per 100,000 women per year at risk of stroke
• those who have migraine with aura and take the pill: 28 per 100,000 women per year at risk of stroke
• those who have migraine without aura and take the pill: 14 per 100,000 women per year are a risk of stroke
http://www.migrainetrust.org/factsheet-stroke-and-migraine-10891
Treatments for Migraine• Triptans, selective 5-HT1B/1D receptor agonists –various
formulations & types• Ergot derivatives (older treatment, not commonly used)• Antiemetics & nsaids
Preventative : 2/3 will have 50% reduction• Many have significant side effects:• Pizotifen – weight gain, drowsiness• B- Blockers – tiredness• Tricyclics – drowsiness• Anticonvulsants – valproate, topiramate, gapapentin –
significant s/e. Botulinum Toxin type A http://www.nice.org.uk/guidance/ta260
• Candesartan : http://www.ncbi.nlm.nih.gov/pubmed/24335848
Medication Overuse Headache
• Headache present on at least 15 days per month
• Developed or markedly worsened during medication overuse
• Headache resolves or reverts to its previous pattern within two months on discontinuation
• Regular overuse for three months or more
Culprits
• Opiates, codeine +/- paracetamol• 10 days+ per month
• Triptans or NSAIDs• 15 days+ per month
Vicious Cycle
• Bad spell of headaches eg stress• Take more painkillers• Body gets used to medication• Rebound/withdrawal if stop for>1d• Think this is another usual
headache• Take more painkillers• Problem worsens
Blood Pressure and Headache
• Very High BP can cause Headache
• Patients will Expect to have BP checked when presenting with Headache
• Children with Headache – check BP
• 3rd Trimester Pregnancy and Headache ?Pre-eclampsia
SINUSITIS HEADACHE
Headache worse on lying downNasal congestionNasal discharge purulent +/- bloodCough, Fever, MalaiseTender at point of painCan be unilateralTreatment:
http://bjgp.org/content/63/616/611
RAISED ICP
• New increasing headache• Present on waking• Increased by stooping or straining• Changes in mental state• Vomiting• Papilloedema• Causes: sinister and benign, acute and
chronic
Idiopathic Intracranial Hypertension
• Link to Excellent summary:
• http://www.patient.co.uk/doctor/idiopathic-intracranial-hypertension-pro
SAH• Risk factors similar to stroke eg. Smoking,
hypertension• Family History in 5-20%• Incidence 6 cases per 100,000 patient yrs• 50% fatality, 1/3 remain dependent• Sudden explosive headache is the
cardinal feature.• If related to sexual intercourse ?SAH• CT scanning is mandatory in all, to be
followed by (delayed) lumbar puncture if CT is negative
SAH
• A period of unresponsiveness of >1 h occurs in almost half of patients
• Focal signs develop at the same time as the headache or soon afterwards in one third of patients
• Classically, the headache from aneurysmal rupture develops in seconds, but can be minutes
SAH
• Vomiting occurs in 70% of patients• Neck stiffness is a common sign in SAH of any
cause, but takes hours to develop and therefore cannot be used to exclude the diagnosis if a patient is seen soon after the sudden-onset headache
• If thunderclap headache is the only symptom then 10% only will have SAH, but all need investigation
JULIE JONES, 45TELEPHONE TRIAGE CONSULTATION (Dr A)• Headache: started 3 days ago gradual onset worse
last night• Started to feel nauseous with it yesterday• Analgesia does help• Global but more at front left• Slight dizziness with nausea no vomiting or visual
disturbance of gross neurological symptoms• Suggested comes in for examination but most likely
tension type headache
Fictional name and age for illustration
JULIE JONES, 45FY2 CONSULTATION IN SURGERY (same day)• 3/7 tension like headache, frontal. No
photophobia• Vomited 3x overnight• Very stressed with work• Had tension and migraines in the past• Helped when lying down• Not worse bending over• No visual symptoms
JULIE JONES, 45• Unlikely to be pregnant - partner has had
vasectomy. D/W Dr B• Ibuprofen and paracetamol helped marginally• o/e PEARL, no focal tenderness, appears
anxious• Discussed stress at work and sleep hygeine• Advised to return if problem persists or
deteriorates
JULIE JONES, 45• DISCHARGE LETTER Hosp to ITU (1 week later)• Collapsed that evening and had seizure• Intubated and ventilated• Platelet count 6• Discussed with Haematology• Diagnosis TTP• To Have Plasma Exchange in Liverpool
JULIE JONES, 45Edited Highlights:• Had 3 cardiac arrests, Had plasma exchange• Discharged after 3 weeks• Medication started: Phenytoin, Prednisolone,
Aspirin, Gliclazide• Haematology follow up, Platelet count
recovered• Steroids reduced, gliclazide stopped• Driving: notify DVLA. Cannot drive for 6
months
LEARNING POINTS?

UPCOMING SESSIONS
17th March – Women’s Health (Dr Helen Wall)
21st April – Genetics (Dr David Harniess)