health financial systems
TRANSCRIPT

1
November 2, 20118:00 a.m. (Pacific Time)
1
Presented by
Health Financial Systems8109 Laguna Blvd
Elk Grove, CA 95758(888) 216-6041
[email protected]://peteharmon.hfssoft.net
2

2
Highlight major 2552-10 changes and News Review 2552-10, T.2, compared to T.1 Mention anticipated T3 Changes Inform attendees of software changes and
Improvements. Discuss compatibility issues between 2552-
96 system and the new 2552-10 software.
3
HFS Does NOT any expect changes to the extensions listed below.
Initial extension was only for 4/30/2011 FYE, and was 30 days (due 10/31/2011).
Current extensions approved by CMS:
4
3
All subsequent FYE due 5 months after the FYE.
CMS made extensions “official” through a TDL (Technical Direction Letter, not a JSM) to Contractors and Providers. HFS received advance TDL 7/27/2011and final on 9/2/2011. See copy posted onhttp://www.hfssoft.com/doc/ExtensionTDL.pdf
Home Office (287-05), NO extensions.
5
Short Period reports: Beginning on or after 5/1/2010 but ending
prior to 4/30/2011, must file and settle on the 2552-96.
These cost reports are due the latter of 30 days from the date of the TDL (10/2/2011), or 5 months after the FYE.
This includes hospitals with hospital based ESRD facilities and/or departments.
6

4
Hospital based ESRDs are subject to the same extension schedule as hospitals.
Hospital based ESRDs shall submit cost reports using the new 2552-10, with the existing I series worksheets.
Hospital based ESRD reports claiming bad debts will not be settled until revised 2552-10 Worksheet I series is released and contains the new bad debt calculation.
7
2552-10 Final published 12/30/2010. This was Transmittal #1.
T.2 DRAFT was received from CMS on 7/29/2011.
There are still open items. HFS commented 8/3/2011.
Final T.2 received 8/26/2011, included most of HFS’ comments.
Expect a T3 to incorporate more vendor comments…..
8

5
We received the T.2 CMS Test Case “A” on 8/30/2011.
We received a revised T.2 test case “B”, on 9/2/2011.
We received a revised T.2 test case “C”, on 9/9/2011.
We received a revised T.2 test case “D”, on 9/16/2011.
HFS submitted to CMS on 9/22/2011. CMS to approve by October 31, 2011.
9
CMS approves based on one test case Too many variables to test HFS has repeatedly requested leniency for
first wave of submissions – nothing in writing but verbal assurance
Providers should submit cost reports a few days early to qualify for grace period
Consider submitting your file to us to test -.mcrx, EC, PI and which Contractor it will be submitted to.
10
6
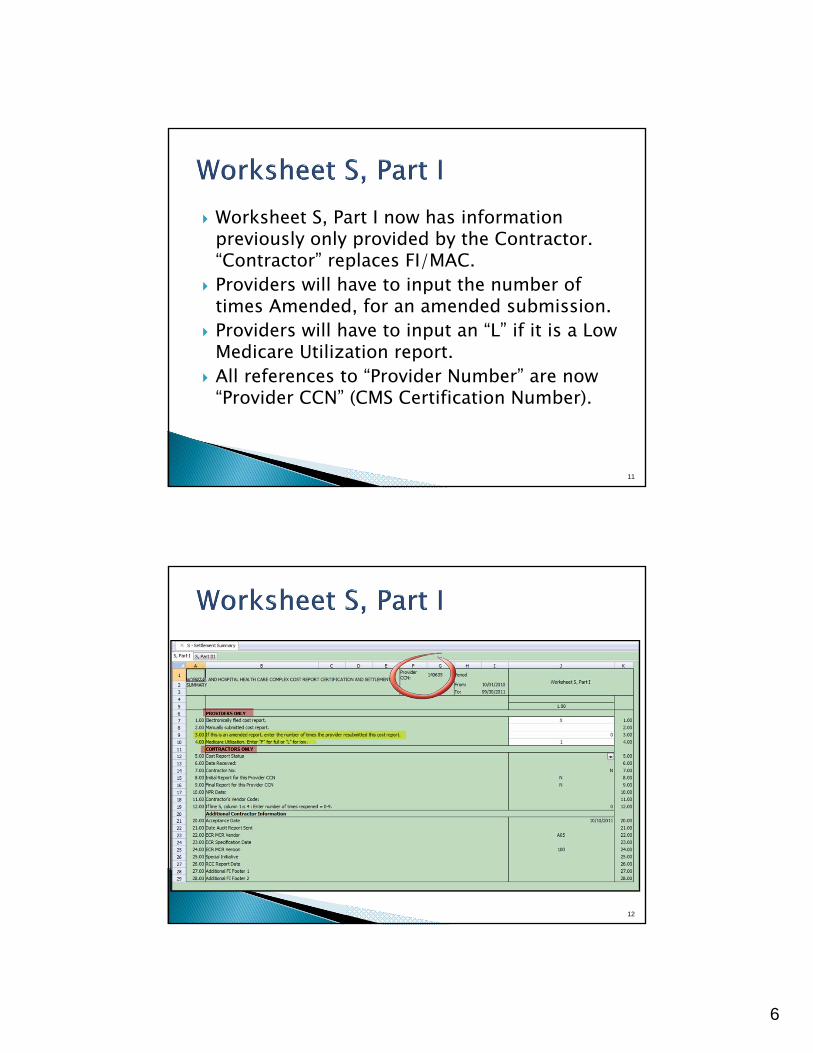
Worksheet S, Part I now has information previously only provided by the Contractor. “Contractor” replaces FI/MAC.
Providers will have to input the number of times Amended, for an amended submission.
Providers will have to input an “L” if it is a Low Medicare Utilization report.
All references to “Provider Number” are now “Provider CCN” (CMS Certification Number).
11
12

7
Lines 1-21 – General Provider/Component Information
Lines 22-25 – DSH and Medicaid Days Lines 26-27 – Geographic Reclassifications Lines 35-38 – SCH/MDH Designation Lines 45-48 – Capital PPS Lines 56-67 – Teaching Hospital Lines 70-71 – Inpatient Psychiatric Facility PPS Lines 75-76 Inpatient Rehabilitation Facility PPS Line 80 – Long Term Care Hospital Line 85-86 - TEFRA Providers
13
Lines 90-97 – Titles V and XIX Lines 105-109 - Rural Providers (CAH) Lines 115-121 - Miscellaneous Cost Reporting
Information Lines 125 – 134 - Transplant Center Information Lines 140-144 – Home Office Lines 144-149 – Other Lines 155-161 – LCC Exemption Lines 165-166 - Multi-campus Lines 176-169 - HIT
14

8
DSH Calculation◦ S-2, Part I, Lines 24-25 Medicaid Days for DSH
calculation ◦ Line 24 days are used to calculate the DSH
percentage on Worksheet E, Part A, line 31 ◦ If no days on S-2 Part I, line 24, no DSH calc. ◦ Line 25 days are used for the LIP calculation on
E-3, Part III, line 3. ◦ No days on S-2 Part I, line 25, no LIP calculation
for the Rehab.
15
S-2, Part I, Lines 24-25 Medicaid Days for DSH calculation (E, Part A), LIP Calculation(L, Part I)
16

9
Worksheet S-2 Part I, line 47 needs to be split as line 47 and 48, to record “new”, and then 100% PPS Capital election. Done in T.2.
S-2 line 47, for “new” hospital, was modified. This line is now Title specific, Title V, XVIII, and XIX, for “new” provider; and line 48 was added for “Elected 100% PPS Capital”.
Worksheet D-1 and Worksheet L calculations change if “new”, so lines 47 and 48 now allow us to consistently determine these calculations.
17
Worksheet S-2 Part I, line 55 eliminated in T.2, and line 56 reworded/revised.
Worksheet S-2 Part I, new line 61 added for IME/GME additional slots, under ACA section 5503. Effective 7/1/2011 FY Begin and after.
Worksheet S-2 Part I, line 62 changed in T.2, to line 60 (Nursing and Allied health).
18

10
Worksheet S-2, CMS added lines 62 and 62.01 to track number of FTEs in accordance with Health Resources and Services Administration’s (HRSA), or Primary Care Residency Expansion Program (PCRE).
Worksheet S-2 lines 63-67 added to report info for I&R training in non provider settings.
Worksheet S-2 Part I, new line 121 added for Implantable Devices (line 64 in 2552-96).
19
20

11
21
22

12
23
Hospital Reimbursement Questionnaire Exhibit 1 of CMS 339 required with 2552-96
24

13
◦ Added Cost Center Column that corresponds to Wkst A Line Numbers◦ LDR Days – same as 2552-96
25
Worksheet S-10 modified labels for lines 26 and 27, to clarify Bad Debt info is for the entire complex.
CAH must complete S-10. Overall Cost to Charge Ratio is coming from
Wkst C
26

14
Worksheet S-10, lines 8, 12, and 16, can be negative ( although the CMS ECR specifications do NOT allow negative amounts), and this can result in line 19 being negative. Thus, when line 31 is calculated for the Total unreimbursed and uncompensated cost, you could be adding negative unreimbursed cost from line 19, to unreimbursed bad debts (positive amount), for line 31, which is then meaningless. We suggested to CMS that S-10, lines 8, 12, and 16, if negative, have the sign flipped (multiply by -1), and then line 19 would always be positive, and line 31 be meaningful. If CMS does not make this instructional change before you file, you should do a workpapershowing the negative changed to a positive, and a manual calculation of S-10. 27
28
Days
Line 1 Excludes LDR Days
impute costs
Overall cost-to-charge ratio applied to program charges to impute costs

15
29
Part II – Wage Data Part III – Wage index Summary Part IV - Wage Related Costs (Previously on
339) Part V – Contract Labor and Benefit Costs
30

16
Wage Related Costs – like old 339 Exhibit 6. Line 24 of S-3, Part IV transfers to S-3, Part
II, line 17, but line 17 is NOT to include the excluded areas, and S-3 Part IV has no instruction or means to make these adjustments for excluded areas.
We suggested to CMS that they add two columns – column 2 for adjustments, and column 3 for the net (column 1 plus/minus column 2). Then column 3, line 24, would be the transfer to S-3 Part II, line 17.
31
If CMS does NOT make this change before you file, you should do a workpaperreflecting any adjustments for the excluded areas, and then show the net on S-3 Part IV, so that the transfer to S-3 Part II, line 17 is correct.
32
17
Worksheet S-4 – HHA Statistical Data Worksheet S-5 – Renal Dialysis Statistical Data◦ EPO/Aranesp Reporting
Worksheet S-6 – CMHC and Outer Outpatient Rehabilitation◦ No “fee only” Question◦ Only CMHC Completes J Series
Worksheet S-7 – SNF Statistical Data◦ All SNF Questions Consolidated on S-7◦ Line 202 – 207 Still Required
Worksheet S-8 – RHC/FQHC Statistical Date Worksheet S-9 – Hospice Statistical Data
33
Any user added lines (subscripts) you had in the 2552-96, are allowed in the 2552-10.
The 2552-10 will “grandfather” in all 2552-96 subscripts – no prior approval.
The 2552-10 did NOT change anything regarding user added lines (subscripts).
The 2552-10 eliminated all “standard” subscripts (i.e. pre-printed on CMS Form). T.2 changed this.
As long as the added cost center meets the definition of a cost center, and is approved by the Contractor (where applicable), it is allowed in the 2552-10.
34

18
Some subscripted lines/cost centers, are now “standard” (e.g. line 55.30 is line 72).
Some worksheets will now have no subscripted lines (e.g. Worksheet A).
Added lines which are not cost centers (e.g. Worksheet A-8), are the same as in the 2552-96.
Added lines are only limited by CMS ECR Specifications (i.e. 99 subscripts per line; and some lines not to be subscripted – e.g. A-8 lines 1-32).
35
36

19
Static throughout the report S-2 IPF = Line 4, IRF = Line 4 S-3 IPF = Line 16, IRF = Line 17 A IPF = 40, IRF = Line 41 Settlement Schedules
37
A-7 must be completed by all providers A-7 eliminated “old” capital, or Part I, and
renumbered new form as Parts I, II, and III – no Part IV. Old Part II is now Part I. Old Part IV is now Part II. Old Part III is new Part III.
A-7 Part I, line 7, new for HIT. – Report expenses prior to being a Meaningful Use User
38

20
Worksheet B-1 may allow additions to accumulated cost stats (previously, only reductions were allowed). ECR Spec change.
More B-1 “automatic stats” expected to be allowed in the ECR file (e.g. Gross Salary, Gross Charges, etc.). Currently, only accumulated cost is an “automatic stat”.
ECR may add “repeat stat” identifier (e.g. square feet).
We proposed all to CMS – no changes yet.
39
Worksheet C Part I, new lines 99-117 added for Special Purpose Cost centers (needed for Total Complex cost to charge ratio used on S-10).
Charges entered for these lines/cost centers are new, and only used for the purpose of calculating the entire complex RCC.
Worksheet C lines 88 and 89 (RHC & FQHC) added for Total cost and Charges.
40

21
Worksheet C Part I, line 200 (subtotal), columns 6, 7, and 8 charges, has a new instruction to NOT include line 61, PBP Clinical Lab Services-Program Only. It is assumed line 61 charges are already included in line 60, Lab.
Line 200 is sum of lines 30-60, and 62-199. Worksheet C Part I, line 92 (Observation
Beds), columns 6, 7, 8 charges, are NOT subtracted on line 201, for line 202, Total. Note that Observation Bed COST is subtracted in col 1 because it is included in Routine.
41
Originally, the new Worksheet C instructions DID NOT transfer “cost” from B Part I, lines 88 and 89 (RHC and FQHC), to column 1, yet columns 6-8 were “open” for the input of charges. This has now been changed for the test case but instructions still need changed.
Worksheet S-10 uses the Total Complex cost to charge ratio, so review Worksheet C cost/charges.
42

22
43
No more “splits” of payments on E Part A. No more IME “factor”. Worksheet E Part A line 7 changed to be MMA
section 422 IME cap reduction. Worksheet E Part A line 7.01 added for ACA section
5503 IME cap reduction adjustment. Worksheet E Part A line 8 changed to be
increase/decrease to IME FTE for allopathic and osteopathic affiliated programs.
Worksheet E Part A, lines 8.01 and 8.02 added for ACA Section 5503 and 5506, increased IME FTE Cap slots.
44

23
Worksheet E Part A, line 31 (DSH) calculation changed to use Medicaid days on S-2 Part I, line 24.
Now, in state, and out of state, paid and eligible days, as well as HMO days, are reported on S-2 Part I, line 24, and will be used to compute the DSH days to days percentage.
Include Observation Bed Days.
45
E Part A line 70 is the “Other” adjustments.1. Line 70.95 is designated for Recovery of
accelerated depreciation.2. Line 70.96 was designated for HCERA
payments (also shown on E-1 line 3.49), but T.25 for the 2552-96 rescinded this. T.2 did the same in the 2552-10.
3. Lines 70.97 to 70.99 have been designated for Low Volume Adjustment Payments. Should be moved to lines 70.96 – 70.98.
46

24
47
E Part B line 1.02 payments must be split for TOPS, if FY overlaps 12/31/2011.
Worksheet E Part B, TOPS extended to 12/31/2011.
Worksheet E Part B line 27, has an alternate calculation for CAH.
It currently includes Vaccine cost from D, Part V, line 73, column 7, as “cost not subject to deductibles and coinsurance”.
48

25
However, Vaccine is no longer the ONLY “cost not subject to deductibles and coinsurance”, thus, the calculation should include D Part V, line 200, column 7.
CMS has proposed to change this in Transmittal 3, so if you have to file before it is codified, prepare a work paper showing this calculation versus our programmed calculation which only includes line 73, and make an Other Adjustment on E Part B, line 39.
You should also be aware that CAH do NOT include Coinsurance on line 25 of E Part B, but instead, line 25 is Deductibles, and line 26 is Coinsurance.
49
New E-1 Part II for HIT (Health Information Technology) payments. Must be identified separately and paid out of the Stimulus Bill (HR 1), as these payments are NOT Part A or Part B, Medicare Trust Funds.
New Column on Wkst S for HIT Settlement Provider must be a “meaningful user” to
receive HIT payments. Penalties will be imposed in 2015 if not HIT
compliant.
50

26
S-2 lines 167 to 169 are new for HIT (Health Information Technology) or EHR (Electronic Health Records).
S-2 line 169 MUST have a factor for HIT calculation on Worksheet E-1 Part II.
CAH get 20% HIT bonus payment (Medicare share plus 20%, not to exceed 100%).
51
Worksheet E-1 Part II, the new HIT calculation worksheet, automatically subtracts 1149 discharges from the total on S-3 Part I, line 1, column 15.
S-10 line 20, column 3 is an integral Part of the HIT calculation (Total Charity Care).
Contractor Only? Hopefully not – Interim Payments should be input by provider
52

27
53
Worksheet E-4 is new in 2552-10, and consolidates old E-3 Part IV and E-3 Part VI.
Worksheet E-4 line 2 re-designated in T.2, to reflect unweighted FTE resident cap add-on for new programs, on or after 1/1/1995.
Worksheet E-4 line 3.01 added in T.2, for ACA section 5503 cap reduction.
Worksheet E-4 lines 4.01 and 4.02 added in T.2, for ACA Sections 5503 and 5506, increased IME FTE Cap.
Worksheet E-4 Line 4.02, for Section 5506 of the ACA. Closed teaching hospital GME FTEs.
54

28
55
Worksheet M-2 lines 7.01 and 7.02 added in T.2, for FQHC (only), for Medical Nutrition Therapist and Diabetes Self Management Training (FTE and Visits New stats must be maintained).
Worksheet M-3 line 16 subscripted to 16.01-16.05 for ACA section 4104, which eliminates coinsurance and deductibles for preventive services on or after 1/1/2011.
Lines 16.01-16,05 are to capture Total and Program charges and costs of the preventive programs. This is both RHC and FQHC.
New data collection required for Total Program charges; Total Program Preventive charges; Total Program Preventive costs; Total Program non-preventive costs; and Total Program Costs.
56

29
M-3 lines 18-20 modified to reflect addition of new lines 16.01-16.05, and line 19 as Coinsurance. Line 19 is for informational purposes only. Changed line 20 calculation.
Worksheet M-3 calculation for lines 16.04 and 16.05, CMS is to change this calculation to be (cost minus Deductibles) times 80%; instead of the current (cost times 80%) minus deductibles. This would then be the same as it was in the 2552-96.
Worksheet M-3 lines 18 and 19 instructions have the “caveat” for “this data is informational only”, on the wrong line. Currently this caveat is with the line 18 instructions, and it will be moved to the line 19 instructions, where it belongs.
57
58

30
59
Still separate I-4 for Renal Dialysis Department and Home Program Dialysis Program.
If you have more than one renal dialysis and/or home dialysis department, submit one Worksheet I-4 combining the renal dialysis departments and/or one Worksheet I-4 combining the home dialysis departments as only one average composite rate will apply to each modality. Enter on the combined Worksheet I-4 each provider’s satellite number if you are separately certified as a satellite facility.
60

31
Other issues we are awaiting CMS detailed instructions:
HCRIS (should be extract “all”) Threshold Acceptability Checklist CY to PY Comparison (Mgmt Reports) PDR (Professional Desk Review) PS&R Crosswalk Wage Index Verification
61
IRIS Reports STAR Modifications RCC Calculations (HFS Special Reports) Contractor internal Rate Calculations (need to
update for 2552-10 references) The Worksheet I series must be updated for
the 265-11 Draft changes (ESRD moving to PPS). This may be Transmittal 3?? The move to PPS is effective for Services on or after 1/1/2011.
62

32
Provision Dem “Super Committee” Recommendations President’s Plan for Economic Growth and Deficit
Reduction
Post‐acute provider payments One or two year market basket freeze (SNF, IRF, LTCH
and HHA)
Reduce payment rates 2014‐2021
HHA rebasing Rebase with 2014‐2015 phase in instead of ACA 4‐year
period
Increase SNF cost sharing Co‐pay of 5% on inpatient deductible per day for each of
the first 20 days of SNF care
Recoup FY11 SNF overpayment While CMS has proposed 11.1% reduction in SNF
payments to account for implementation of RUG‐IV, this
proposal would recover FY 2011 overpayments
New SNF value‐based
purchasing/readmissions program
Implements SNF VBP in non‐budget neutral manner Reduce SNF payments up to 3% for SNF facilities with high
percentage of preventable hospital readmissions
beginning in 2015.
HHA co‐pay 10% copayment for each episode $100 copayment for HHA services per episode (5 or more
visits) beginning in 2017
Rural hospital payment add‐ons Reduce or eliminate special payment provisions for
CAH/MDH/SCH
CAH reimbursement at 100% cost for CAHs more than 10
miles from nearest hospital
Bad debts Eliminate or phase down bad debt payments Reduce to 25% for all eligible providers over 3 years,
beginning in 2013
Graduate medical education Lower reimbursement for IME, lower or freeze DGME
payments for all hospitals or hospitals in high cost areas
Reduce IME by 10% beginning in 2013
Recoup overpayments from IPPS
documentation and coding
improvements
Require recoup of documentation and coding
overpayments from FY 2010‐2012
Equal payments for certain
conditions in IRF and SNF
Reduce some IRF payments to SNF levels
Encourage appropriate use of IRF Re‐establish 75% threshold for patients with designated
medical conditions that require rehabilitation
63
The HFS team has worked to get you the software and the features you need to file your Medicare Cost Report.
We appreciate all who have tested and given us feedback.
Please continue to let us know your issues and we will continue to work hard to make this transition as smooth as possible.
64

33
Over the past year we have been making internal improvements to gear up to ensure fast and accurate support and software◦ HFS has a new customer database that links to our
website ◦ We have installed a ticketing system to better track
your issues and get software fixes with documentation to you faster than ever.◦ Our updating process has been updated and
improved so that fixes are released faster to you.
◦ WE ARE READY!
65
66
System is included with the 2552-96 on the Downloads Page and can be installed.
Is also included in Check for Updates. Must Install with
Admin Rights – once. Still all one system
under Yellow HFS Icon
New File Type – 2552-10

34
File | Open will show both
The file structure has changed
.mcr = Indexed File
.mcrx = xml file
◦ No more Restore/Reorganize◦ About the same size as indexed file◦ No more .tmp file or .err* files◦ The HFS 2552-96 MCR (data) files can NOT be rolled
forward, renamed, and given new FY dates, and used as a 2552-10.
67
68

35
Imports from your 2552-96 Prior Year file(.mcr)◦ Wkst S-2 Facility Data◦ Cost Center Structure◦ B-1 Statistics Set Up and Square Feet◦ A-8 Adjustments – without amounts◦ A-8-1 Related Organizations – without
amounts◦ S-8 – RHC/FQHC Statistical Data◦ S-2, Part II Hosp Reimb Questionnaire(339
Exhibit I)◦ (You will need your prior year .xprq file)
69
70

36
You should avoid special characters in the Provider Name (S-2 Part I, line 3), as some have caused problems (e.g. &, %, etc.). We think we have this corrected, but better safe than sorry.
CTL X is a “hot key” to delete data (similar to “cut” in Excel). If you have trouble getting rid of a date, or any data cell, use CTL X to delete the data.
71
Worksheet S-2 FY Dates are now input on S-2 Part I, line 20 (second Tab), instead of on the initial screen. We do NOT display the calendar, but the F4 key, or a double mouse click on the cell, will bring up the calendar.
72

37
Early Beta users who used the Template feature may have inadvertently had lines 18.01 to 18.20, added on Worksheet S-2 , Part I. This was fixed, and all you need to do is change something on S-2 (e.g. change a Y to an N), then calculate. Then change the S-2 N back to a Y.
The CBSA code was S-2 line 21.03, column 5, in the 2552-96 (Hospital component only). It is now S-2 , Part I, column 3, lines 1-19 (all components). Under TOOLS, we have a “Look-Up” table for CBSA codes.
73
Auto Open Forms – we automatically open certain forms, based upon the Worksheet S-2 , Part I answers.
If line 3 is a PPS acute care hospital, we open E , Part A, if line 4 is a Psych, we open E-3 , Part II, etc.
Early in the Beta process, we inadvertently opened forms we should NOT have, so you need to Delete these.
Click on FORMS, Delete, and look for the little green triangle next to the form. This indicates all “open” forms
74

38
If you see a triangle next to E , Part A for the Other Subprovider, this is most likely an error and should be deleted.
Same for E-1 for the Other Subprovider. Also, E-3 , Part II for the Hospital (unless it
is a free standing Psych Hospital), and E-3 , Part III for the Hospital (unless it is a free standing Rehab Hospital).
Check all forms to make sure all “open” are correct.
75
Contact Information was in the 339
This data will be in EC file as “Extraneous Data” Type 5 records
Will not go to HCRIS database
Not Required by CMS
76

39
77
More Automated Statistics◦ Patient Days = P◦ Inpatient Charges = I◦ Outpatient Charges = O
Still have ◦ Gross Salaries = S
Total Charges = CAccumulated Cost – Only Use Negative statistic code - # has been retired.
78

40
79
Adding lines can be done on any worksheet. Click on EDIT, Add Lines, or Cost Center and
Statistics Setup. If applicable, there’s a Tab for the specific worksheet.
If on Worksheet S-2, S-3, C, etc., and EDIT, Add Lines is selected, the cost center add/delete drop down screen appears, as these are “cost center” driven worksheets. Any additions or deletions will then be reflected on Worksheet A, B, B-1, etc. (all cost center related worksheets).
If you want to add an HHA on S-3 line 22, you get the drop down screen and scroll down to line 101, HHA, and add line 101 to Worksheet A, which adds line 22.01 on S-3 and 12.01 on S-2.
80
41
81
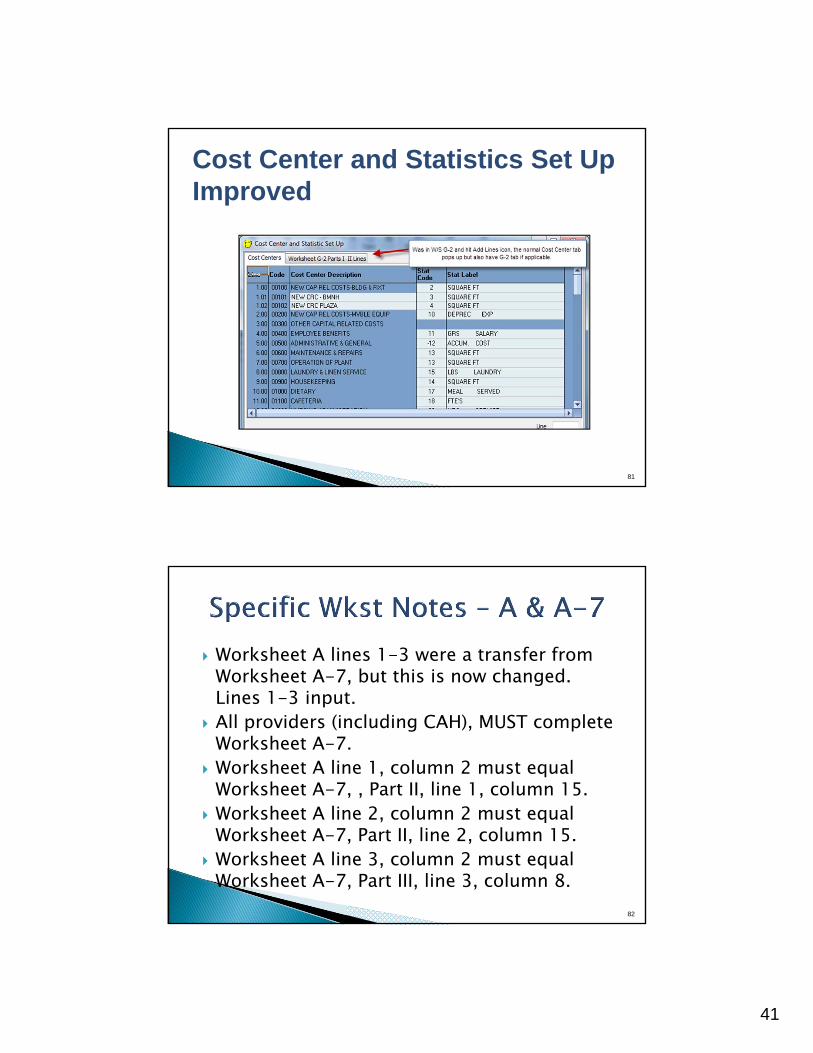
Cost Center and Statistics Set UpImproved
Worksheet A lines 1-3 were a transfer from Worksheet A-7, but this is now changed. Lines 1-3 input.
All providers (including CAH), MUST complete Worksheet A-7.
Worksheet A line 1, column 2 must equal Worksheet A-7, , Part II, line 1, column 15.
Worksheet A line 2, column 2 must equal Worksheet A-7, Part II, line 2, column 15.
Worksheet A line 3, column 2 must equal Worksheet A-7, Part III, line 3, column 8.
82

42
83
Tools | CMS 339 Questionnaire Exhibit 1 (Old Exhibit 2) Exhibit 2 – Bad Debts(Old Exhibit 5)◦ Tab for Inpatient and Outpatient◦ Expanded for more entries
Data is stored in .xprq file Encrypted File
84

43
85
86

44
87
PI File format has changed from a text file to a .pdf so our viewer has been upgraded.
Preferences
88

45
89
PS&R is ready for use with the update that we released Friday?◦ Import – ready◦ Import 2552-96 provider crosswalk for conversion
to 2552-10 provider crosswalk◦ Import Prior Year statistics and convert to 2552-10◦ Assign – done◦ Difference Report – ready◦ Export to Cost Report – ready◦ Export to Auditor – probably next release
90

46
We have added the ability to bring in multiple provider based RHC and FQHC PS&R data from S-8 when consolidated.
We were hoping to make changes to the PS&R tool to import and assign provider based esrd reports. Unfortunately, this needs a complete overhaul of the PS&R to incorporate the condition codes. Right now the fields are unable to be carried. Still need to manually do esrd Report 720 assignments.
91
92

47
One change from the 2552-96 to the 2552-10 that will affect the PS&R reconciliation process is with provider based HHA settlements.
In the 2552-96, CMS shaded the H-6 visits by CBSA, however, with the 2552-10 H-3 does require the visits to be separated by CBSA.
This change will require verification that the CBSA codes on PS&R are included on S-4 prior to importing the PS&R csv file. See next slides.
93
94

48
95
Import Data – Ready Imports Crosswalk, or uses Assignment Rules
– Ready All functionality of the 2552-96 Exports to the Cost Report Produces Grouping Report
Working on minor bug fixes from our testersWorking on translation of rules and crosswalk from 2552-96 to 2552-10
96

49
Allows input of data specifications - ready All of the features of the 2552-96 feature –
ready Extracts data to chosen File format Batch Data Extractor – functional
Working on translation of .csdx files from 2552-96 to 2552-10
97
Just released Fully functional Kept same functionality of 2552-96 Working on translation of imported 2552-96 adjustments to 2552-10
98

50
Totally new Interface…….
99
Under Construction◦ The Interface is functional and you can check it out◦ We are still working on the reports ◦ And 2552-96 to 2552-10 Comparison
COMING SOON!
100

51
HFS User Manual 2552-10 CMS Instructions – Already, Wow!◦ Recent CMS Changes in Red◦ HFS Notes in Blue
***Did you know that if you push the F1 key the CMS instructions pop up?
101
Questions and comments.
102