health insurance plan design and chronic disease management
TRANSCRIPT

The University of Maine The University of Maine
DigitalCommons@UMaine DigitalCommons@UMaine
Electronic Theses and Dissertations Fogler Library
Summer 8-21-2020
Health Insurance Plan Design and Chronic Disease Management Health Insurance Plan Design and Chronic Disease Management
Daniel E. Feldman University of Maine, [email protected]
Follow this and additional works at: https://digitalcommons.library.umaine.edu/etd
Part of the Cardiology Commons, Cardiovascular Diseases Commons, Endocrine System Diseases
Commons, Health and Medical Administration Commons, Health Economics Commons, Insurance
Commons, and the Pharmacy Administration, Policy and Regulation Commons
Recommended Citation Recommended Citation Feldman, Daniel E., "Health Insurance Plan Design and Chronic Disease Management" (2020). Electronic Theses and Dissertations. 3201. https://digitalcommons.library.umaine.edu/etd/3201
This Open-Access Thesis is brought to you for free and open access by DigitalCommons@UMaine. It has been accepted for inclusion in Electronic Theses and Dissertations by an authorized administrator of DigitalCommons@UMaine. For more information, please contact [email protected].

HEALTH INSURANCE PLAN DESIGN AND CHRONIC DISEASE MANAGEMENT
By
Daniel Feldman
B.A., Oberlin College, 1999
M.S., Physical Therapy, MGH Institute of Health Professions, 2001
A THESIS
Submitted in Partial Fulfillment of the
Requirements for the Degree of
Master of Science
(in Economics)
The Graduate School
The University of Maine
August 2020
Advisory Committee:
Angela Daley, Assistant Professor of Economics, Advisor
Keith Evans, Associate Professor of Economics
Caroline Noblet, Associate Professor of Economics

ii
Copyright 2020 Daniel Feldman

HEALTH INSURANCE PLAN DESIGN AND CHRONIC DISEASE MANAGEMENT
By Daniel Feldman
Thesis Advisor: Dr. Angela Daley
An Abstract of the Thesis Presented
in Partial Fulfillment of the Requirements for the
Degree of Master of Science
(in Economics)
August 2020
Each year, Americans spend more money on health care than any other industrialized nation,
despite comparable health outcomes. The reasons for this lack of health care value in the US are
numerous and complex – including market distortions like supplier-inflated pricing and
regulatory structures that enable consumers to utilize ubiquitous, high-cost medical technologies
that yield uncertain benefits. Health insurance, once thought to be an insignificant contributor to
rising health spending, has changed considerably in the past few decades in ways that make it
more accessible and more generous in coverage. Health insurance design thus continues to be of
considerable interest in health policy research.
Consumer responses to health insurance design changes can be difficult to predict from a
theoretical standpoint. This is due to ways in which some consumers misperceive health benefits
relative to costs or have difficulty accounting for complexities within health insurance contracts

when making consumption decisions. Empirical evidence, therefore, has the potential to
meaningfully influence health value-oriented policymaking. This paper explores the manner in
which consumers with one of three heart disease risk factors: high blood pressure, high
cholesterol, or type-II diabetes mellitus, modify their consumption of office visits and drugs to
treat these conditions in response to an increase in the price of other health care.
In Chapter 2, we find that a small absolute increase in cost-sharing for a broad range of medical
services is associated with a reduction in the rate of spending on drugs that treat heart disease
risk factors. For consumers with high blood pressure or high cholesterol, this comes without any
change to rates of drug utilization – a result that suggests an increase in health value. Consumers
with type-II diabetes lower rates of spending and utilization, a result we view as lowering health
value. Overall, consumers show little to no change in consumption rates of medical office visits,
a result consistent with prior literature, indicating that cost-sharing increases for office visits
mainly function to shift financial burden to consumers, rather than to improve health value.
Because we were unable to acquire data for a separate control group, we cannot infer causality
from these results. Consequently, in Chapter 3, we further explore potential mechanisms
whereby consumers with high blood pressure or high cholesterol lowered rates of spending on
drugs without modifying rates of utilization. We consider three such mechanisms: (1) the
purchase of drugs in higher quantities per prescription; (2) switching from brand-name drugs to
generics; and (3) price changes in the marketplace. We are unable to conclude that any one
mechanism contributed to our Chapter 2 results, but we do see evidence of distortions in how
health benefits are perceived, which may have contributed to changes in spending. Our results

have potential implications for health value resulting from insurance design. Cost-sharing
increases are unlikely to affect the insured population uniformly and may impact consumers with
heart disease risk factors in ways that both enhance and erode health value.

iii
DEDICATION
To April and Emilia

iv
ACKNOWLEDGEMENTS
I would like to extend profound gratitude to my advisor, Dr. Angela Daley, for her world-class
teaching, encouragement, moral support, patience, pragmatism, and intellectual guidance into the
production of this work. Thank you also to Drs. Keith Evans and Caroline Noblet for invaluable
guidance and support.
I also give a sincere thank you to S.F. for data access and troubleshooting and to Lynden
McGriff for pharmaceutical expertise.
Finally, I thank my wife, April, and daughter, Emilia for all of their patience and support
throughout the lengthy production of this work, which involved lots of time inside thinking and
staring at a screen and not as much time as I would have liked being a husband and father. But
it’s over, now, everyone! Let’s go camping!

v
TABLE OF CONTENTS
DEDICATION ............................................................................................................................... iii
ACKNOWLEDGEMENTS ........................................................................................................... iv
LIST OF TABLES ....................................................................................................................... viii
LIST OF FIGURES ....................................................................................................................... ix
LIST OF ACRONYMS .................................................................................................................. x
1. HEALTH INSURANCE PLAN DESIGN AND CONSUMER BEHAVIOR ........................... 1
1.1. Introduction .......................................................................................................................... 1
1.2. Health Care Supply and Expenditure Growth ..................................................................... 3
1.3. Health Care Demand and Expenditure Growth ................................................................... 5
1.4. The US Health Delivery System .......................................................................................... 9
1.5. Health Insurance Design .................................................................................................... 10
1.5.1. First and Second-Best Health Insurance ..................................................................... 10
1.5.2. Moral Hazard .............................................................................................................. 12
1.5.3. Behavioral Hazard ...................................................................................................... 14
1.5.4. Complex Information .................................................................................................. 19
1.6. Conclusion ......................................................................................................................... 24
2. THE EFFECT OF A CHANGE IN MEDICAL PRICES ON THE CONSUMPTION
OF HIGH-VALUE DRUGS AND OFFICE VISITS ....................................................... 26
2.1. Introduction ........................................................................................................................ 26
2.2. Background ........................................................................................................................ 28

vi
2.2.1. Defining High-Value Care .......................................................................................... 28
2.2.2. Own-Price Effects ....................................................................................................... 30
2.2.3. Spillover Effects.......................................................................................................... 33
2.3. Methods.............................................................................................................................. 37
2.3.1. Data ............................................................................................................................. 37
2.3.2. Study Inclusion ........................................................................................................... 39
2.3.3. Health Plan and Policy Change................................................................................... 42
2.3.4. Study Design ............................................................................................................... 44
2.3.5. Estimation ................................................................................................................... 45
2.3.6. Robustness Checks...................................................................................................... 50
2.4. Results ................................................................................................................................ 51
2.4.1. Characteristics of Chronic Disease Groups ................................................................ 51
2.4.2. Summary of Consumption Trends .............................................................................. 53
2.4.3. Regression Results ...................................................................................................... 58
2.4.4. Robustness Checks...................................................................................................... 65
2.5. Discussion and Conclusion ................................................................................................ 67
3. AN EXPLORATION OF CONSUMER PHARMACEUTICAL COST-SAVING
METHODS ....................................................................................................................... 72
3.1. Introduction ........................................................................................................................ 72
3.2. Background ........................................................................................................................ 72
3.2.1. Larger Per-Prescription Quantity ................................................................................ 72
3.2.2. Generic Substitution.................................................................................................... 73

vii
3.2.3. Lower Prices ............................................................................................................... 74
3.3. Methods.............................................................................................................................. 75
3.3.1 Data .............................................................................................................................. 75
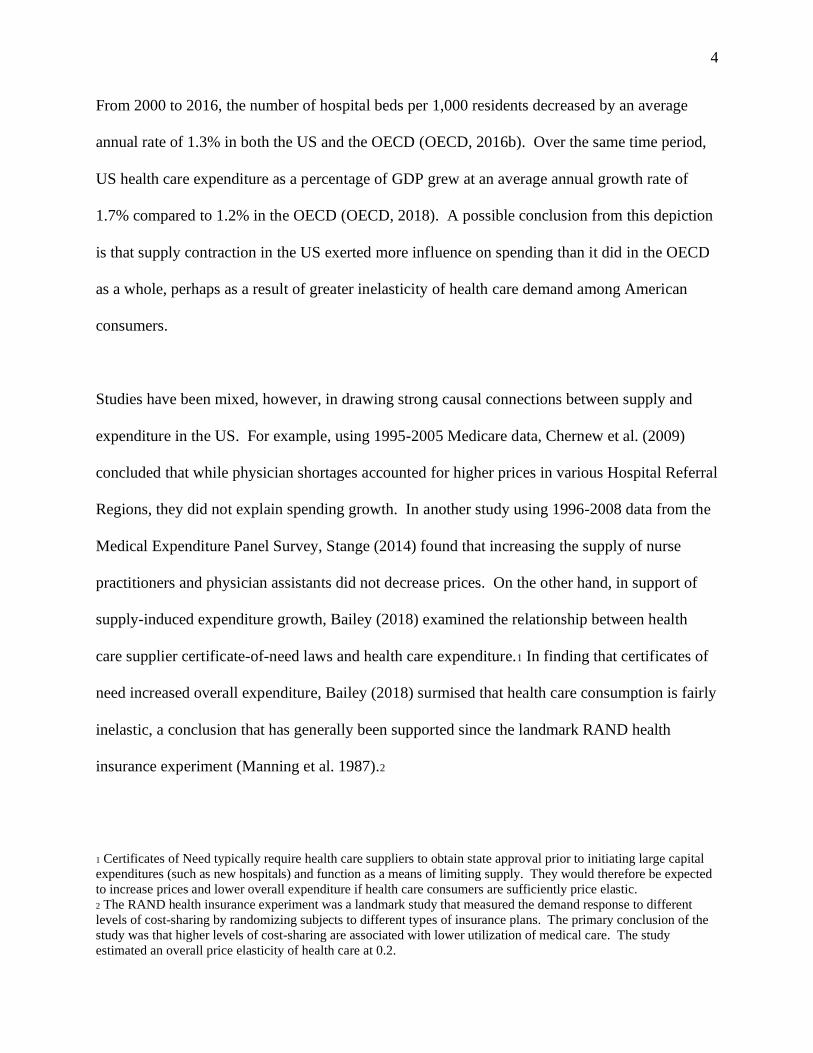
3.3.2 Pharmacy Plan ............................................................................................................. 76
3.3.3. Study Design and Estimation ...................................................................................... 77
3.4. Results ................................................................................................................................ 79
3.4.1. Per-Prescription Day Supply....................................................................................... 79
3.4.2. Per-Prescription Copayment ....................................................................................... 80
3.4.3 Generic Drug Cost ....................................................................................................... 84
3.4.4. Robustness Check ....................................................................................................... 86
3.5. Discussion and Conclusion ................................................................................................ 87
4. CONCLUSIONS....................................................................................................................... 91
REFERENCES ............................................................................................................................. 95
APPENDIX ................................................................................................................................. 101
BIOGRAPHY OF THE AUTHOR ............................................................................................. 109

viii
LIST OF TABLES
Table 2. 1. Selected Plan Features and Benefit Provisions, by Fiscal Year ................................. 43
Table 2. 2. Characteristics of the HTN, LIP and DM Groups in the First Half of Fiscal
Year 2015 .......................................................................................................................... 52
Table 2. 3. Changes in Dependent Variables during the Baseline and Intervention
Periods, Means and Percentages ....................................................................................... 54
Table 2. 4. Regression Results: Normalized Spending and Utilization for the HTN Cohort ....... 60
Table 2. 5. Regression Results: Normalized Spending and Utilization for the LIP Cohort ......... 62
Table 2. 6. Regression Results: Normalized Spending and Utilization for the DM Cohort ......... 64
Table 2. 7. Regression Results, Robustness Checks ..................................................................... 66
Table 3. 1. In-Network Pharmacy Plan, Copayment Structure..................................................... 77
Table 3. 2. Mean Cohort Change, Per-Prescription Day Supply, Numerical Example ................ 77
Table 3. 3. Number of Prescriptions Filled, Brand-Name Drugs Exceeding 0.50%
Spending, HTN Cohort ..................................................................................................... 83

ix
LIST OF FIGURES
Figure 1. 1. Health Care Spending as a Percent of GDP, US versus OECD, 2000-2018 ............... 1
Figure 1. 2. Average Annual Growth, Hospital Beds and Health Spending, 2000-2016 ............... 3
Figure 1. 3. Health Insurance Coverage in the US, Total Population, 1987-2018 ......................... 8
Figure 1. 4. Moral Hazard in Health Insurance ............................................................................ 13
Figure 1.5. Health Care Consumption with Negative Behavioral Hazard .................................... 16
Figure 1. 6. Health Care Consumption with Positive Behavioral Hazard .................................... 18
Figure 1. 7. Price per Dollar of Anticipated Health Care Spending, $500 versus $600
Deductible ......................................................................................................................... 22
Figure 2. 1. Sample Selection Process .......................................................................................... 40
Figure 2. 2. Study Design ............................................................................................................. 45
Figure 2. 3. Consumption Trends for the HTN Group ................................................................. 56
Figure 2. 4. Consumption Trends for the LIP Group .................................................................... 57
Figure 2. 5. Consumption Trends for the DM Group ................................................................... 58
Figure 3. 1. Mean Change, Per-Prescription Day Supply, HTN and LIP Cohorts ....................... 80
Figure 3. 2. Per-Prescription Drug Copayment, HTN and LIP Cohorts ....................................... 81
Figure 3. 3. Mean Cost of Generic Drugs, All Fill Sizes, HTN Cohort ....................................... 84
Figure 3. 4. Mean Cost of Generic Drugs, All Fill Sizes, LIP Cohort .......................................... 85
Figure 3. 5. Per-Prescription Drug Copayment, HTN Cohort, Robustness Check ....................... 87

x
LIST OF ACRONYMS
US: United States…………………………………………………………………… 1
CMS: Centers for Medicare & Medicaid Services…………………………………. 1
OECD: Organization for Economic Co-operation and Development……………… 1
GDP: gross domestic product……………………………………………………..... 1
RAND: Research and Development Corporation………………………………….. 4
ACA: Patient Protection and Affordable Care Act of 2010………………………... 6
CDC: Centers for Disease Control and Prevention………………………………… 7
AWP: average wholesale price……………………………………………………... 20
POS: point of service……………………………………………………………….. 20
HDHP: high-deductible health plan………………………………………………… 22
CalPERS: California Public Employees Retirement System ……………………… 34
ICD: International Classification of Diseases………………………………………. 37
CPT: common procedural terminology…………………………………………….. 37
ZCTA: zip code tabulation area……………………………………………………. 38
COBRA: Consolidated Omnibus Budget Reconciliation Act……………………… 39
HTN: primary hypertension (high blood pressure)……………………………….... 39
LIP: hyperlipidemia (high blood cholesterol)………………………………………. 39
DM: type-II diabetes mellitus………………………………………………………. 39
PCP: primary care physician……………………………………………………….. 42
FY: fiscal year………………………………………………………………………. 43
OOP: out-of-pocket………………………………………………………………… 43
COB: coordination of benefit………………………………………………………. 48

xi
GLS: generalized least squares……………………………………………………... 49
OLS: ordinary least squares………………………………………………………… 50
FE: fixed effects…………………………………………………………………….. 59
RE: random effects…………………………………………………………………. 59

1
CHAPTER 1
1. HEALTH INSURANCE PLAN DESIGN AND CONSUMER BEHAVIOR
1.1. Introduction
The US spends more per capita on health care than any other industrialized nation. In 2018, the
US spent $11,172 per capita on health care, which amounted to 17.7% of its gross domestic
product (CMS, 2018). Figure 1.1 displays health care spending in the US compared to the
average of the 35 nations comprising the Organisation for Economic Co-operation and
Development (OECD). Although spending growth has stabilized over the past decade and even
fallen over the past two years, it has remained substantially higher than the OECD average since
at least 2000.
Figure 1. 1. Health Care Spending as a Percent of GDP, US versus OECD, 2000-2018
Source: OECD (2018)

2
In 2018, US health care spending as a percentage of GDP was 38.5% more than the second
highest spender, Switzerland, and 57.9% more than its neighbor, Canada (OECD, 2018).
Despite this level of spending, health outcomes in the US are comparable to other OECD nations
and even worse in some areas. For example, US life expectancy at birth was 78.6 years in 2017,
below the OECD average of 80.6 years (OECD, 2017a). Additionally, in recent years, US
ischemic heart disease and diabetes mortality rates were 109.6 and 24.5 per 100,000,
respectively, compared to OECD averages of 110.5 and 21.3 (OECD, 2016a; OECD, 2015). The
US also had the third highest share of adults with diabetes in 2015, 10.8% compared to the
OECD average of 7.0% (OECD, 2017b). For nearly 50 years, a goal of US policy makers,
insurers, and employers has been to lower the cost of health care while maintaining or improving
health outcomes.
The remainder of this chapter explores the challenges to meeting this goal, beginning with an
overview of the role of supply and demand in health care expenditure growth. Next, after briefly
reviewing the US health care delivery system, the chapter will summarize health insurance
design theory and show how theoretical conclusions lead insurers to influence demand through
implementation of different cost-sharing features in the health insurance contract. This is
followed by a discussion of how consumer behavioral and informational challenges can modify
the assumptions underlying the response to these features. The chapter concludes with a
presentation of the experimental question to be explored in chapter two.

3
1.2. Health Care Supply and Expenditure Growth
The drivers of high health care spending in the US are multi-faceted and complex. One area of
research interest has been the relationship between health care supply and expenditure growth.
Classical economic theory predicts that by lowering supply, health care providers can command
a higher equilibrium price and total health care expenditure will grow if consumers are
sufficiently price inelastic. Figure 1.2 depicts long-run change in health care supply, measured
via hospital beds, and health care spending in the US and OECD nations.
Figure 1. 2. Average Annual Growth, Hospital Beds and Health Spending, 2000-2016
Sources: OECD (2016b, 2018)
4
From 2000 to 2016, the number of hospital beds per 1,000 residents decreased by an average
annual rate of 1.3% in both the US and the OECD (OECD, 2016b). Over the same time period,
US health care expenditure as a percentage of GDP grew at an average annual growth rate of
1.7% compared to 1.2% in the OECD (OECD, 2018). A possible conclusion from this depiction
is that supply contraction in the US exerted more influence on spending than it did in the OECD
as a whole, perhaps as a result of greater inelasticity of health care demand among American
consumers.
Studies have been mixed, however, in drawing strong causal connections between supply and
expenditure in the US. For example, using 1995-2005 Medicare data, Chernew et al. (2009)
concluded that while physician shortages accounted for higher prices in various Hospital Referral
Regions, they did not explain spending growth. In another study using 1996-2008 data from the
Medical Expenditure Panel Survey, Stange (2014) found that increasing the supply of nurse
practitioners and physician assistants did not decrease prices. On the other hand, in support of
supply-induced expenditure growth, Bailey (2018) examined the relationship between health
care supplier certificate-of-need laws and health care expenditure.1 In finding that certificates of
need increased overall expenditure, Bailey (2018) surmised that health care consumption is fairly
inelastic, a conclusion that has generally been supported since the landmark RAND health
insurance experiment (Manning et al. 1987).2
1 Certificates of Need typically require health care suppliers to obtain state approval prior to initiating large capital
expenditures (such as new hospitals) and function as a means of limiting supply. They would therefore be expected
to increase prices and lower overall expenditure if health care consumers are sufficiently price elastic.
2 The RAND health insurance experiment was a landmark study that measured the demand response to different
levels of cost-sharing by randomizing subjects to different types of insurance plans. The primary conclusion of the
study was that higher levels of cost-sharing are associated with lower utilization of medical care. The study
estimated an overall price elasticity of health care at 0.2.

5
More recently, public policymakers have taken aim at prices since supplier-inflated prices, rather
than consumption demand, is widely thought to be the key driver of US health care expenditure
growth (Frakt and Chernew, 2018; Anderson et al. 2003). For example, the Medicare Payment
Advisory Commission’s March 2020 report to Congress noted that, from 2008 to 2018, private
health insurance enrollee spending grew at nearly twice the rate as Medicare’s, despite declines
in utilization. The report attributed the private market’s rate of spending increase to rising
hospital and physician practice consolidation, resulting in better leverage over insurers to
negotiate higher rates. The report also concluded that Medicare, with greater monopsony control
over prices, nonetheless continues to function in a fee-for-service environment, where its overall
expenditure on health services is strongly tied to prices and utilization. Furthermore, Medicare
does not set prices on drugs, which have been a rising component of overall Medicare
expenditure (Medicare Payment Advisory Commission, 2020). In this context, some states have
successfully passed legislation aimed at lowering drug prices (Miller, 2019).
1.3. Health Care Demand and Expenditure Growth
There is also considerable interest in whether lowering health care expenditure can be
accomplished through demand. Rising consumer demand for health care can raise overall
expenditure if the supply response is sufficiently inelastic, perhaps due to limited infrastructure
or constrictions in the health care labor force. Indeed, both rising chronic disease and obesity
rates in the US have been linked to increased health care spending in the literature (Thorpe et al.
2015). Increases in demand induced by technological change may also contribute to rising
healthcare expenditure. One of the lesser-known conclusions of the RAND health insurance

6
experiment was that technological change might be responsible for some of the seven-fold
increase in health care spending observed between the post-WWII era and 1984. Manning et al.
(1987) noted that the 20th century brought about new technologies for treating chronic diseases
that were previously untreatable. In partial support of this conclusion, the authors pointed to
their experimental finding that the overall price elasticity of health care (-0.2) was too low to
explain the seven-fold rise in expenditure simply as a result of the subsidized demand created by
insurance. They did not, however, draw conclusions about what might have induced
technological change, only to note that some combination of insurance pricing and rising
incomes may have played a role (Manning et al. 1987). Expanding on this conclusion, Chandra
and Skinner (2012) argued that rapid diffusion of low productivity technology and technology
with unknown benefit relative to cost has been a key driver of US health care expenditures.
They suggested that such diffusion was in part due to payment systems failing to recognize and
financially reward value, due of the nature of the legal system where payors have difficulty
denying benefits for technologies that have no proven benefits and doctors, not insurers,
ultimately determine what constitutes ‘medically necessary’, and thus reimbursable health care.
Although Manning et al. (1987) suggested that demand growth due to insurance was unlikely to
be the primary driver of expenditure growth in the mid-late 20th century, a large body of modern
public health and economics research has nonetheless been devoted to studying the influence of
health insurance design on consumer demand for health care. This may be because health
insurance has changed in several key ways since the RAND experiment. Arguably, the most
notable way in which health insurance has changed has been through regulatory changes that
benefit consumers. For example, the Health Insurance Portability and Accountability Act of

7
1996 allowed employees to be enrolled in continuous coverage between jobs and be
automatically eligible for new coverage upon starting a new job, regardless of any pre-existing
condition or health status. In the same year, the Mental Health Parity Act required certain health
plans to offer mental health benefits at the same level as medical benefits and the Newborns’ and
Mothers’ Health Protection Act set minimum covered length-of-stay levels for mothers and
newborns. More recently, the Patient Protection and Affordable Care Act of 2010 (ACA)
regulated the individual health insurance market by requiring plans to accept all applicants and
charge the same rates, regardless of prior health history. The ACA also established a set of
“essential health benefits” that were required to be offered in all newly sold health insurance
plans. Where once health insurance provided only medical and surgical benefits, ACA-
compliant plans now provide substantial preventive health care coverage, including smoking
cessation, obesity treatment, well-child checks, and birth control. The collective outcome of
these laws is that health insurance has become not only more comprehensive, but also more
pervasive. Indeed, the percentage of persons of all ages without health insurance fell from
16.0% in 2010 to 9.1% in 2015 (Ward et al. 2016) and health insurance coverage as a percent of
the total population rose above 90% for the first time in 2015, remaining at this level through
2018 (US Census Bureau, 1987-2018, Figure 1.3).

8
Figure 1. 3. Health Insurance Coverage in the US, Total Population, 1987-2018
The dotted line indicates passage of the ACA. Source: US Census Bureau (1987-2018)
Another way in which health insurance has changed since the late 1970s and 1980s is that plans
are now more complex. In 1988, the dominant form of employer-sponsored health insurance,
accounting for more than 70% of the employer-sponsored market share, was the conventional
indemnity plan where subscribers were reimbursed a portion of their health expenses and could
choose any health provider they wished. In 2018, indemnity plans made up less than 1% of
employer-sponsored plans (Claxton et al. 2018). Today’s plans are mostly a mix of health
maintenance organizations, preferred provider organizations, and point-of-service plans, all of
which have different networking and cost-sharing features.

9
As a final note on the evolution of health insurance from the days of the RAND experiment,
claims processing has largely become automated from the point of view of the consumer. Where
consumers once had to submit paper claims as they did in the RAND experiment, the claims-
handling process is now largely a function of insurers and providers. Greater consumer access
and coverage, complexity of plan design, and more convenient claims processing means that the
muted influence of health insurance plan design on expenditures (made by the RAND
experiment) does not necessarily hold.
1.4. The US Health Delivery System
Health insurance is the primary means through which health care services are paid for in the US;
only an estimated 9.4% of persons living in the US were uninsured in 2018 (Cohen et al. 2019).
Health insurance is delivered both by public and private institutions. In terms of the former,
Medicaid is state-and federally-sponsored health insurance for low-income families, qualified
children and pregnant women, and people with disabilities. Medicaid coverage is often provided
free of charge, although states have the option to charge limited premiums, copayments, and
enrollment fees in certain circumstances. Medicare is health insurance for persons over the age
of 64 and certain younger persons with disabilities. It is federally-sponsored, but administered
through a public and private partnership. Medicare is comprised of a premium-free base benefit,
part A, which covers hospital care and is wholly paid for through payroll taxes. Parts B and D
cover a portion of physician care and pharmaceuticals, respectively, and require payment of a
premium. Part C is a bundled private insurance option, known as Medicare Advantage, that
includes coverage for parts A, B, and often D. It also pays for health care services not covered by
parts A and B.

10
Private health insurance is predominantly available through employers, but can also be
individually purchased or provided through TRICARE.3 In 2018, among persons under the age
of 65, 161.4 million people were covered by employer-based coverage, compared to 27.1 million
with individually-purchased coverage and 5.8 million with TRICARE (U.S. Census Bureau,
2018). The size of the private health insurance market may be why health insurance design is
considered to be an important area in studying the demand for health care.
1.5. Health Insurance Design
1.5.1. First and Second-Best Health Insurance
The purpose of health insurance is to provide sufficient protection to a consumer’s wealth in the
event of an unexpected adverse health event. Modern health insurance accomplishes this by
spreading risk and allowing the consumer, in exchange for a premium, to utilize the health care
system at subsidized prices. Typically, basic health insurance plans consist of both cost-sharing
and stop-loss features. Cost sharing requires the consumer to pay for a portion of health care
services either before or simultaneously with the insurer and can act as a disincentive for
overconsuming health care. Stop losses protect the consumer from large losses due to large,
negative, and exogenous changes in health status. Although cost-sharing and stop-loss
provisions are tools designed to balance risk protection with disincentives for wasteful
consumption, as will be shown in this chapter, they are actually the key features of a second-best
insurance design.
3 TRICARE is health insurance for individuals and families with a military affiliation.

11
Zeckhauser (1970) and Pauly (2000) have summarized the features of a first-best health
insurance plan. In exchange for a risk-adjusted premium, first-best health insurance pays the
total cost of health care in the event of sickness without cost-sharing. First-best insurance
achieves this because of a key underlying assumption: complete information about consumer
health. In other words, the insurer has complete knowledge about the nature and severity of the
health condition of each insured. Moreover, the insurer can completely monitor and ensure that
insureds take socially optimal levels of health precaution (e.g. exercise, diet, risky behaviors).
Under the first-best design, insureds do not retain private information about their health.
Because the insurer has complete, accurate information about the health of the population, it can
pay the full cost of care and there is no incentive for the rational consumer to consume excess or
wasteful health care. This first-best design is infeasible in all practical terms because gaining
this level of information would require untenable discovery costs and privacy intrusions on the
part of the insurer.
Therefore, the reality of health insurance in the US is a second-best design, where consumers
have private information about their health and insurers, who lack this information, offer plans
that tradeoff between the value to consumers (in terms of risk reduction) and providing
incentives to consume health care responsibly. To get a sense of these tradeoffs, consider a
simple example of two insurers, A and B, who function in a second-best state of the world.
Ignoring premium pricing, insurer A provides 100% coverage of health expenditures, insurer B
provides 1% coverage, and consumers are able to access health care services as they see fit.
Under these hypotheticals, insurer A offers substantial consumer value and risk protection, but
will likely have to pay for a large amount of preventable or wasteful health spending as there is

12
no incentive for the insured to consume health care responsibly or reduce risky health behaviors.
Insurer B, on the other hand, will pay for far less wasteful consumption, but may be of little
value to the typically risk-averse consumer, and may thus have difficulty attracting subscribers.
In the second-best state of the world, insurers seek to design plans that strike a balance between
value and risk protection provided to the consumer, while limiting incentives for wasteful and
unnecessary consumption (moral hazard).
1.5.2. Moral Hazard
Moral hazard has a unique meaning in health insurance. As summarized in Einav and
Finkelstein (2018), moral hazard has traditionally been defined as risky behavior on the part of
the insured when they are not required to cover the full cost of any resulting damage. An
example of this “ex ante” moral hazard would be failing to install smoke and carbon monoxide
detectors in a home covered by homeowner’s insurance, or driving carelessly when covered by
auto insurance. While insureds can certainly engage in risky health behaviors, health insurers are
more concerned with “ex post” moral hazard, where insureds consume health care that costs
more (to the insurer and society) than the benefit it provides. The consumer does so because
insurance allows the consumer to purchase health care at prices that are discounted relative to
marginal social cost. Since the consumer will purchase health care when private marginal
benefits exceed private marginal costs, there will exist a quantity of health care services that are
viewed as efficient consumption by the consumer, but not by society. Figure 1.4 demonstrates
this concept graphically. In the figure, Q* represents the point where social cost meets marginal
benefit, the socially optimal level of health care consumption. Actual consumption occurs
instead at QM because this is the point where subsidized private marginal cost meets marginal

13
benefit. In this sense, moral hazard is a deadweight loss resulting from overconsumption.4 The
authors of the RAND experiment were skeptical of subsidized prices being the key factor driving
expenditures in the 1970s and 1980s. Their depiction of moral hazard would have certainly
featured a more vertical (price inelastic) marginal benefit curve and thus much smaller
deadweight loss.
There exists a class of health care that the consumer would like to consume, but insurers would
prefer not to pay for. If insurers attempt to disincentivize moral hazard by pricing health care
services close to marginal social cost, consumers will lose value. If prices are too steeply
subsidized, consumers will consume excess wasteful health care. This is the essence of the
tradeoff when designing health insurance plans.
4 “Moral”, in this case, is actually a misnomer since consumers who consume health care when private marginal
benefits exceed private marginal cost are acting rationally.
Moral Hazard
Marginal Social Cost
P
Marginal Private Cost
Q*
Marginal Benefit
Q
Figure 1. 4. Moral Hazard in Health Insurance

14
To control moral hazard, modern health insurance designs use a combination of co-insurance,
co-payments, deductibles, and stop-losses to manage the value-waste tradeoff. The generic
health insurance plan has a three-arm structure that resets on an annual basis. In the first arm, the
consumer pays the full marginal cost of care up to a certain amount, the deductible, for a broad
range of health care services. Once the deductible limit is reached, insurance will begin to pay
benefits as a percentage of the cost of care. In this second, coinsurance arm, the consumer
typically pays a small percentage of the cost of care, perhaps 10% or 20%. The third arm, the
stop-loss, is reached once the consumer has paid up to a maximum dollar amount for health care
out-of-pocket. Above the stop-loss, the insurer pays the full cost of care. This basic three-arm
design both disincentivizes moral hazard consumption through full cost-sharing for initial
spending, and also provides sufficient income protection in the case of a more catastrophic health
event.
1.5.3. Behavioral Hazard
A moral hazard construct assumes both that consumers are able to accurately compare their own
private costs to the true marginal benefit of care, and that any changes to consumption due to
cost-sharing primarily take place at the margin. For example, a moral hazard construct assumes
that if consumers pay $0.25 for every dollar of health care and this price is subsequently raised to
$0.30, then consumers who were indifferent between paying $0.25 and receiving no healthcare
would no longer consume healthcare. Other consumers, for whom $0.25 represents value above
private cost would continue to purchase healthcare. This, however, is not a realistic picture of
consumer behavior. A different type of hazard, behavioral hazard, can cause some consumers to
misperceive the true marginal benefit of health care consumption and their relationship to the

15
margin. Because changes to cost-sharing can potentially cause shifts in spending by consumers
above (or below) the margin due to behavioral hazard, efforts to control moral hazard spending
through cost-sharing changes can potentially have ambiguous effects.
Behavioral hazard is described in depth by Baicker et al. (2015), who argue that, without
behavioral hazard, the benefit that a person receives from medical treatment is strictly a function
of the extent to which the treatment alleviates sickness. In this moral-hazard only view,
incremental treatment yields incremental benefit and there is no benefit from no treatment.
Behavioral hazard then enters as additive or subtractive to actual health benefit. Symptom
salience and present bias are two types of subtractive (negative) behavioral hazard, where
consumers perceive the health benefit to be smaller or closer to the margin than the actual health
benefit. Symptom salient consumers undervalue the benefit of health care that does not have an
immediate relief of symptoms, but has a highly beneficial health impact. For example, a
symptom salient consumer may be reluctant to begin a course of physical therapy, with
continuing discomfort and a home exercise program as the short-term result of a program
intended to provide long-term relief. Another type of subtractive (negative) behavioral hazard is
present bias, which is the idea that future utility flows are subject to time-inconsistent
(hyperbolic) discounting. A present-biased health care consumer facing a rise in cost-sharing
may opt to curtail consumption of care that provides considerable health benefits well into the
future, but whose immediate health benefits are comparatively small. Examples of such care
includes cholesterol screening or medications to control blood pressure. Figure 1.5 depicts
negative behavioral hazard. In this figure, misperception of marginal benefit causes the marginal
benefit curve to shift inward, reflecting an under-consumption of health care. Rather than the

16
socially optimal level of consumption, Q*, consumers now choose to consume QH-. The result is
that the moral hazard overconsumption depicted in Figure 1.4 is eliminated, but in its place there
is deadweight loss resulting from consuming less than the socially optimal amounts of health
care.
The welfare implication of negative behavioral hazard depends on the size of the eliminated
wasteful moral hazard consumption relative to the added deadweight loss due to under-
consumption of socially beneficial care. Consider the act of raising a co-payment for a blood
pressure medication. A moral hazard-only approach would consider only the change in demand
at the margin and subsequently decompose this change in spending to a decrease in the value of
health benefit and a decrease in wasteful spending to marginal consumers. Such an analysis may
conclude that increasing the co-pay is welfare-enhancing if the reduction in wasteful moral
Figure 1.5. Health Care Consumption with Negative Behavioral Hazard
Negative Behavioral Hazard
Marginal Social Cost
Marginal Private Cost
Perceived Marginal Benefit QH-
P
Actual Marginal Benefit
Q* QM

17
hazard spending exceeds the reduction in the value of health benefits. If, however, the
population consists of individuals who exhibit a high degree of negative behavioral bias (Figure
1.5), the effect of raising a co-pay could be to create underutilization from individuals who are
above the margin. The health implications of using less blood pressure medication could be
profoundly negative and exceed the welfare gains predicted by a moral-hazard only analysis.
In contrast to negative behavioral hazard, false beliefs are a type of additive (positive) behavioral
hazard. False beliefs can be ascribed to consumers who derive significant utility from health
care or other products and services that have dubious actual health effect. False beliefs might
motivate health care consumers to purchase care where actual health benefits are below both
societal and private marginal cost. Controlling moral hazard consumption through the usual
method of raising a cost-sharing provision might prove quite difficult in a population
characterized by a high incidence of consumers with false beliefs. Symptom salience, described
earlier as a form of negative behavioral hazard, can also be a form of positive behavioral hazard.
Massage, for example, may provide effective temporary pain relief, but do very little to eliminate
the health problem causing the pain. A symptom salient consumer may therefore be willing to
over-pay for this service if this consumer believes that the massage has curative effects. Positive
behavioral hazard is depicted in Figure 1.6 where the demand curve is shifted outward, reflecting
a tendency to overconsume health care. This effect is to magnify the original moral hazard
problem. Rather than consuming Q* or QM, consumers now consume QH+.

18
Insurers can manage behavioral hazard consumption by layering additional cost-sharing features
and exemptions onto the basic three-arm design. For example, insurers might provide full
coverage for preventive health care, excluding these services from the deductible (and in effect
making them free to the consumer). Insurers may also introduce co-payments. Co-payments are
a specified dollar amount, typically separate from the deductible, that must be paid for each
instance of utilization. Suppose a generic medication is equivalent to a brand name medication
in terms of the benefit it provides, but is less costly. Insurers might subject the brand name
medication to a higher co-pay, since positive behavioral hazard may motivate consumers to
prefer a brand name to a generic. This kind of pricing scheme, known as tiering, is a common
feature in modern health insurance contracts. Interestingly, Figure 1.6 suggests that even if an
insurer prices the brand name medication at marginal social cost, some over-consumption will
still occur, indicating that the insurer may need to price the brand name medication above
marginal social cost if it wishes to eliminate wasteful consumption of brand name medications.
Positive Behavioral Hazard
Marginal Social Cost P
Marginal Private Cost
Perceived Marginal Benefit
Q* QM QH+
Actual Marginal Benefit
Figure 1. 6. Health Care Consumption with Positive Behavioral Hazard

19
In a theoretically optimal second-best plan, an insurer would be fully informed about the
behavioral tendencies of its enrollees and design a plan in which cost-sharing features are
tailored to these tendencies. For instance, such a plan might have tiering of pharmaceuticals, a
general deductible to reduce moral hazard, an additional surcharge for certain types of care that
are subject to positive behavioral hazard, and an exemption from the deductible for types of care
that are subject to negative behavioral hazard. This kind of complex plan is only optimal in a
theoretical sense. In reality, the insurer faces another kind of tradeoff, between plan specificity
and the limits of consumer engagement. Considering the plan just described, if the average
consumer is unable or unwilling to weigh various cost-sharing features before consuming health
care, they fail to work as intended. For example, there is evidence that a particular form of cost-
sharing, the deductible, misleads some consumers who not only cut back on care that is subject
to the deductible, but also on certain forms of free or preventive care that are not subject to the
deductible. It is for this reason that the deductible is sometimes referred to as a “blunt
instrument” (Reed et al. 2009; Brot-Goldberg et al. 2017). The next section takes a closer look at
the ways in which consumers adapt to the complex informational challenges that are present in
health insurance contracts.
1.5.4. Complex Information
“As to prescription drug expenses, the recognized charge for each service or supply is the lesser
of:
• What the provider bills or submits for that service or supply; and
• 110% of the Average Wholesale Price (AWP) or other similar resource. Average
Wholesale Price (AWP) is the current average wholesale price of a prescription drug

20
listed in the Medi-Span weekly price updates (or any other similar publication chosen
by Aetna).”
-Aetna Choice POS II Medical Plan (2017)
In addition to behavioral hazard, consumers may fail to act predictably in response to a change in
cost-sharing because of the complex nature of health insurance contracts. In an attempt to
simplify the interlinking structures of deductibles, copayments, coinsurance, and out-of-pocket
maximum, along with difficult-to-read contract language, the consumer may adopt a heuristic, a
simplified mental representation of the contract, and update this heuristic upon receipt of the bill.
Liebman and Zeckhauser (2004) describe such a heuristic, which they refer to generally as
‘schmeduling’. ‘Schmedulers’ can employ two kinds of heuristics: ironing and spotlighting. A
consumer who irons reduces multiple price schedules to a single average price or a price level
that is more easily understood. Health insurance contracts have multiple price schedules that
often layer various incentives to steer the consumer towards beneficial health care (and away
from wasteful health care). For example, certain forms of preventive care might be free, while
an emergency room co-payment may be quite large relative to a standard office visit copayment.
Sometimes, there are small (5-10%) differences between copayments for different types of health
services. Such incentive-layering may be lost on the consumer who, when faced with a health
care need that might incur search costs to uncover the nuances of the benefit provision, will
choose to iron the contract instead.
Spotlighting is a form of present bias under a non-linear payment schedule, where present
consumption impacts the price paid for future consumption. A spotlighting consumer will be

21
overly concerned with the spot, or current price, and will either heavily discount or be generally
unaware of its impact on future price. In health insurance, spotlighting consumers may be
overly sensitive to the deductible, a provision that specifies that the consumer must pay health
care expenditures up to a certain amount, after which the insurer begins to pay benefits. The
deductible represents a non-linear contract where the effective price paid for health care falls
with additional consumption beyond the deductible. As outlined in Aron-Dine et al. (2015), a
rational, non-liquidity constrained, forward-thinking consumer would react to an increase in the
deductible by considering their own health needs and anticipated spending levels (subtracting
any health care that is exempt from the deductible) for the year, and then determine whether and
how to modify expenditure. Should anticipated expenditure be past the new deductible, this
consumer should be indifferent to the spot prices faced while under the deductible, since the
overall price paid for health care in the benefit year will include a considerable amount of free or
discounted care. As an example, consider a consumer enrolled in a simple health insurance plan
with a $500 deductible, 10% coinsurance, and a $2,000 stop loss. The following year, this
consumer’s deductible increases to $600. If the consumer anticipates a high level of medical
spending, he or she should be indifferent to the deductible increase and make little change to
health care spending, since the actual price per dollar of expenditure under the new plan will be
equivalent to the old plan or too small to be of consequence (Figure 1.7)

22
Figure 1. 7. Price per Dollar of Anticipated Health Care Spending, $500 versus $600 Deductible
There is evidence that consumers who switch to high deductible health plans (HDHPs) spotlight,
and this finding extends to consumers with both high and low expected health care needs. For
example, Brot-Goldberg et al. (2017) found that 25% of the reduction in health care consumption
among those who swtiched from a free care plan to a HDHP came from the quartile of
consumers with the highest health care needs while still under the deductible.
There are a few reasons why consumers may exhibit ironing and spotlighting behavior. Other
than a few general categories of health care, such as elective surgeries and child birth, consumers
may have difficulty projecting their future health care expenditure since, by their nature, adverse
health events are unexpected. As a result, consumers may take a short-term outlook on health
care and respond only to the most recent bill, adopting this as a representative price for health
care. Consumer are not completely myopic, however, and do show adaptability to some of the

23
dynamic incentives offered in plans. For example, consumers who join plans with a deductible
mid-year have a probability of incurring any initial health care spending that falls as the month of
joining gets closer to December, whereas mid-year joiners who are not in a plan with a
deductible show no such pattern (Aron-Dine et al. 2015). Information limitations can also result
in spotlighting and ironing. Consumers may not understand how deductibles, co-payments or
co-insurance are linked together (Reed et al. 2009; Lieu et al. 2009). Additionally, the
complexity of modern health insurance contracts can entail considerable health benefit search
costs, even to consumers who know how to access publicly-posted hospital price
‘chargemasters’. Chargemaster prices are typically three times the amount actually charged to
insurers, and hospitals might post prices in this manner as a bargaining tactic (Batty and Ippolito,
2017). Ultimately, because insurers confidentially negotiate their own prices and have different
ways of applying cost-sharing to their consumers, chargemasters do not provide an easy-to-
interpret signal to the consumer about the final price to be paid.
The direction of the demand response to a price change under complex information is
theoretically ambiguous. If consumers perceive a heuristic price that is higher than their true
expected price, they may exhibit larger price elasticities than they would with less complex
information. On the other hand, if consumers exhibit a degree of unawareness or willful
ignorance of price changes, a term referred to as ‘ostriching’ by Liebman and Zeckhauser (2004),
they may be less price responsive than they would otherwise be.

24
1.6. Conclusion
Spending on health care in the US has far exceeded spending in other industrialized nations for
decades, despite comparable health outcomes. The reasons for high spending are varied –
including supplier-inflated pricing and the widespread accessibility of uncertain-benefit, high-
cost technology. This chapter focused on the ways in which health insurance design can
influence health care demand and subsequent expenditure. Early work by the authors of the
RAND experiment concluded that health care is an inelastic good, and consequently insurance-
subsidized prices were unlikely to be the primary drivers of high expenditure growth in the
1970s and early 1980s. However, health insurance in the US has changed considerably since the
RAND experiment, both in terms of the number of individuals covered and the scope of benefits
provided. Thus, health insurance design continues to be a productive area for health care policy
research.
Insurers face tradeoffs in plan design. A health insurance plan must offer enough value to
consumers so as to sufficiently protect against exogenous and costly adverse health events. On
the other hand, if a plan is too generous it will incentivize wasteful moral hazard consumption.
Insurers can balance this tradeoff by layering different consumer financial incentives, such as
free preventive care and higher pricing for brand name drugs. However, it is difficult to
anticipate how consumers will respond to these kinds of incentives because they may not
accurately perceive true health care benefit relative to their own private costs and, as a result,
could respond to incentives in a manner that is ultimately more harmful to health and costly to
the insurer. Consumers may also fail to fully account for nuanced or complex plan incentives,

25
especially since health care decisions can often be made when feeling unwell or under time
pressure.
The next chapter is an empirical examination of how consumers respond to plan design.
Specifically, we examine the effect of cost-sharing (price) changes on the consumption of high-
value drugs for consumers with three different risk factors for heart disease – high blood
pressure, high cholesterol, and type-II diabetes. 5 This is a population of individuals whom, by
nature of having such chronic diseases, are unlikely to be marginal health care consumers and
may be more demand-inelastic than consumers without chronic diseases. It might be expected,
therefore, that small price changes would result in little change in health care demand, but higher
costs for consumers. On the other hand, consumers with chronic diseases may be just as
susceptible to behavioral hazard and informational barriers as other consumers, making
theoretical predictions ambiguous. Chapter 2 attempts to quantify how a group of consumers
who take drugs to prevent or control risk factors for heart disease respond to a change in the
price of their medical care. Chapter 2 also discusses whether these responses are likely to have
improved overall health care value. Did the insurance plan succeed in effectively controlling
expenditure without sacrificing consumer health or did the plan simply shift more cost to
consumers?
5 High-value health care is identified by literature and guidelines published by panels of experts such as the
American Board of Internal Medicine Foundation’s Choosing Wisely initiative and the US Preventive Services Task
Force. We explore this definition as it relates to drugs in the next chapter.

26
CHAPTER 2
2. THE EFFECT OF A CHANGE IN MEDICAL PRICES ON THE CONSUMPTION OF
HIGH-VALUE DRUGS AND OFFICE VISITS
2.1. Introduction
Heart disease is the leading cause of mortality in the US (Kochanek et al. 2019). Together with
stroke, the average annual cost of cardiovascular disease was estimated at $351.2 billion in 2014-
2015, an amount consisting of $213.8 billion in direct costs and $137.4 billion in lost future
productivity (American Heart Association, 2019). While large, US heart disease mortality
figures are in-line with other industrialized nations. For example, US mortality rates for
ischemic heart disease were within one percentage point of the OECD average in 2016 (OECD,
2016a). On the other hand, in the same year, US total spending on health care was 17.1% of
GDP, far exceeding the OECD average of 8.8% (OECD, 2018). Although direct comparisons of
heart disease spending between the US and the rest of the OECD are not available, these
indicators suggest that the US has a health care value problem. Americans with heart disease are
no better off mortality-wise than the OECD average, despite much higher national spending on
health care.
Achieving better value for Americans with heart disease (or at significant risk for heart disease)
means either improving mortality while holding expenditure constant or lowering expenditure
while holding mortality constant. Of course, we could also aim to improve mortality and lower
expenditure. In any case, to improve health care value, it is necessary to have a clear

27
understanding of the response to health care price changes. 6 Any value-enhancing price change
should have the effect of steering consumers away from low-value care, towards high-value care,
or both.
Past studies have evaluated consumer response to changes in the price of drugs that treat three
common heart disease risk factors: high blood pressure, hyperlipidemia, and diabetes mellitus. 7
These drugs are widely considered to be a form of high-value care since their purpose is to
prevent costly and debilitating adverse events, such as heart attacks. In a recent systematic
review, Gourzoulidis et al. (2017) concluded that when faced with an increase in price,
consumers lower their adherence to these drugs (the size of the effect varies across the three risk
factor groups). Additionally, the authors found strong evidence that better adherence leads to
fewer adverse health outcomes and less utilization of other forms of health care, such as hospitals
and physician office visits. In this way, drugs and other health care can be thought of as
substitutes. However, unlike other forms of economic substitution characterized by intentional
choice, when consumers substitute between drugs and other health care, they largely do so
involuntarily as a result of an adverse health outcome. For example, a person who suffers a heart
attack, plausibly due to being non-adherent to cardiac drugs, has little choice but to go to a
hospital. Because of this uniqueness, we seek to determine whether the direction of substitution
also runs from other health care to drugs. That is, when the price of other health care rises, what
is the consumption response for drugs that treat high blood pressure, hyperlipidemia, and
diabetes mellitus? Do consumers continue to substitute, swapping less medical care for more
6 For the remainder of this chapter, ‘price’ refers to the amount faced by the consumer within a health insurance
plan. This is often different than the amount charged by the health care provider.
7 Hyperlipidemia is high blood cholesterol

28
drugs, or is a there a different kind of response? Does the response vary between risk factor
groups? Are their signs of behavioral hazard within this population?
Our contribution to the literature is to further explore the consumption relationship between
medical care and high-value drugs, utilizing three years of medical and pharmacy claims data
from a single large employer in the northeast US. Our objective is to inform health insurance
plan design by describing the extent to which the substitution effect between other health care
and high-value drugs holds when the price of medical care increases, but drug prices remain
constant. We also explore own-price effects by estimating how the consumption of office visits
changes under the same price increase. The results have the potential to better inform policy
decision-making to improve health care value.
2.2. Background
2.2.1. Defining High-Value Care
Simply put, high-value health care improves health by more than it costs to provide. Chandra
and Skinner (2012) elaborate on this definition, classifying high-value or ‘home run’ health care
technologies as those that either provide universal and substantial life-saving impact for a very
low cost, or are at minimal risk of overuse as a result of providing a well-defined health benefit
to a well-defined population. Drugs that target heart disease are an example of the latter.
Chandra and Skinner (2012) argue that such drugs would not normally be prescribed to
consumers who do not need them and have a significant health impact for those who do. This is
consistent with Ford et al. (2007), who studied the contribution of different forms of cardiac
intervention on heart disease mortality. They found that a group of drugs that act directly on the

29
cardiovascular system to prevent or treat heart disease had the largest impact on heart disease
mortality reduction of any medically-based intervention. Drugs in this group, which are
inexpensive to produce and widely accessible, directly target cardiac risk factors such as high
cholesterol and high blood pressure and are broadly categorized as secondary prevention.8 Other
studies support the high-value nature of these drugs by showing that higher rates of adherence
lead to lower rates of adverse cardiac events (Choudhry et al. 2011; Chowdhury et al. 2013;
Rasmussen et al. 2007; Ho et al. 2008). Full adherence to cardiovascular medications is also
associated with a 10% lower average annual cost of health care utilization (Simon-Tuval et al.
2016).
Drugs that treat diabetes mellitus can also lower risk for heart disease. In contrast to the drugs
studied by Ford et al. (2007) that directly act on the cardiovascular system to lower blood
pressure or cholesterol, drugs that target diabetes prevent heart disease indirectly by controlling
hyperglycemia (elevated blood sugar). Chronic hyperglycemia interacts with various biological
processes that contribute to heart disease risk factors like high blood pressure, high cholesterol,
and obesity (Leon and Maddox, 2015). Drugs that treat diabetes mellitus can be considered
high-value. Using a large dataset of Kaiser Permanente employees with diabetes, Ho et al.
(2006) found that non-adherence to antihypertensives, statins, and oral hypoglycemics was
associated with significantly higher risk of hospitalization and all-cause mortality. The study
concluded that a collection of health behaviors, including non-adherence, is correlated with
adverse health outcomes. Similarly, multiple literature reviews have concluded drugs that treat
8 Secondary prevention refers to interventions that lessen the impact of a disease, while primary interventions are
aimed at preventing the onset of disease.

30
diabetes are cost-effective or, in some cases, cost saving (Li et al. 2010; Tucker and Palmer,
2011). A review by Zheng et al. (2018) concluded that diabetes drugs lower cardiac mortality
risk, but this depends on the class of drug. Two classes of diabetes drugs, sodium-glucose
cotransporter 2 inhibitors and glucagon-like peptide 1 agonists, were both associated with lower
all-cause and cardiac mortality risk relative to controls. A third class of diabetes drugs,
dipeptidyl peptidase 4 inhibitors, was not associated with lower mortality risk.
If drugs that treat risk factors for heart disease, directly or indirectly, are together considered to
be high-value, how can insurers incentivize consumers to maintain or enhance adherence to these
drugs? Likewise, how can they ensure that consumers do not reduce quantities as an unintended
consequence of a price change? This is especially relevant in light of the fact that typical
adherence rates for these drugs are considered to be poor (Naderi et al. 2012; Bailey and Kodack,
2011). To better understand how consumers will respond to insurance changes, it is necessary to
understand how the demand for these drugs respond to own-price changes, as well as changes in
the price of other types of health care (i.e. spillover effects).
2.2.2. Own-Price Effects
The demand for drugs intended to treat risk factors for heart disease is similar to other goods;
when faced with a price increase, consumers curb demand. Evidence of this response comes
from studies that can be broadly classified as medication adherence or quantity response.
Research on medication adherence is primarily concerned with how copayment changes impact
the consistency by which consumers maintain enough drug supply to effectively treat their
chronic conditions. Past studies find that increasing a prescription drug co-payment results in
lower adherence to medications intended to treat risk factors for heart disease (Cole et al. 2006;

31
Maciejewski et al. 2010a; Gibson et al. 2006; Doshi et al. 2009). Furthermore, increasing co-
payments may have a more profound negative effect on adherence for consumers with a low
chronic disease burden, possibly leading to higher risk for adverse health consequences (Wang et
al. 2011). Similarly, consumers who switch (or are switched) to a high-deductible health plan
(HDHP) also experience lower adherence to drugs that treat risk factors for heart disease (Lewey
et al. 2018; Nair et al. 2009).
There is also evidence that lowering prescription drug co-payments improves adherence to
medications intended to treat risk factors for heart disease, although the consistency of this
response depends on the type of heart disease risk factor under study. For example, there is
fairly uniform evidence that decreasing copayments improves adherence to drugs that treat high
blood pressure and high cholesterol (Maciejewski et al. 2010b; Chernew et al. 2008; Gibson et
al. 2011, Choudhry et al. 2011; Frank et al. 2012). On the other hand, studies evaluating the
effect of copayment decreases on adherence to diabetes drugs are more mixed. Some conclude
that lowering copayments improves adherence (Maciejewski et al. 2010b; Chernew et al. 2008;
Zeng et al. 2010), while others find no effect (Gibson et al. 2011). There is also evidence that
adherence responses are sensitive to formulary design. For example, consumers with heart
disease risk factors who are switched to value-based formularies do not show significant changes
in medication adherence, despite overall cost savings (Yeung et al. 2018; Sullivan et al. 2015).9
9 A value-based formulary uses formal cost-effectiveness analysis to place drugs on different copayment tiers.
Consumers who are moved to these formularies are thus faced with a mix of price increases and decreases. This is
in contrast to most other studies, which typically only modify a single copayment for a single group or class of drugs
within an existing formulary framework.

32
In addition to studies on medication adherence, those on quantity response reach similar, but
more nuanced conclusions. Drugs used to treat risk factors for heart disease are generally
inelastic with estimates falling between -0.01 and -0.50; own-price elasticities depend on drug
type (Yeung et al. 2018; Chernew et al. 2008; Frank et al. 2012). For example, the demand
elasticity for cholesterol-lowering statins is -0.41, considerably more price elastic than high
blood pressure drugs, which have demand elasticities between -0.01 and -0.10. Likewise,
demand elasticities for biguanides and proton pump inhibitors (both of which are used to treat
diabetes) are -0.17 and -0.69, respectively (Yeung et al. 2018). Yeung et al. (2018) suspected
that the variation in demand elasticity between different classes of drugs was attributed to the
availability of substitutes within the same drug class or between different types of drugs. There
is also evidence that brand-name drugs are more demand elastic relative to generic drugs, and
that tiered pricing may be an effective means by which to extract value-based decisions from
consumers (Herr and Suppliet, 2017; Yeung et al. 2018).
Other studies on quantity response look at direct changes in demand. This approach is often
used when consumers are switched to HDHPs, where the effective annual price of a drug is
different between individuals depending on expected annual health consumption, thus making
price elasticity estimation impractical. Still, conclusions are consistent; consumers who are
switched to a HDHP reduce quantities of drugs that treat heart disease and diabetes (Brot-
Goldberg et al. 2017).10
10 In this study, consumers were switched from a so-called traditional plan to a HDHP, which has a different
payment structure. Therefore, it is difficult to separate the pure effects of the price change from the informational
challenges inherent in switching plans. This is evidenced by the finding that individuals also cut back on free care
(Brot-Goldberg et al., 2017).

33
2.2.3. Spillover Effects
If own-price changes to drugs intended to treat risk factors for heart disease affect quantity
consumed and adherence, how do drug price changes affect the consumption of other health
care? In other words, do these drugs act as complements or substitutes to other health care? The
direction of change is relevant for health policy. For example, if drugs and hospital care are
substitutes, raising a drug copayment would be associated with an increase in hospitalizations.
This could result in a loss of health care value since the decrease in expenditure on drugs could
be more than offset by an increase in hospital expenditures, while also worsening health status.
On the other hand, if drugs and hospital care are complements, raising a drug copayment would
be associated with a decrease in hospitalizations. This could result in an increase in health care
value if it results in the reduction of medically unnecessary care.
In the health economics literature, consumption responses stemming from relationships between
different types of health care are frequently referred to as spillover or offset effects. The two
terms are similar. ‘Spillover’ typically refers to changes in health care utilization, whereas
‘offset’ refers to the impact on spending. For example, if outpatient care and drugs are
complements, then raising the price of outpatient care would result in the spillover effect of
lowering drug consumption. For individuals with risk factors for heart disease, many of whom
need both outpatient care and drugs, a potential additional spillover effect would be greater
utilization of inpatient care. The savings associated with lower spending on outpatient care and
drugs may be offset by the increase in inpatient spending. Spillover effects can also occur when
the behavior of consumers in one health plan adversely impacts those in another type of health

34
plan. For example, Chandra et al. (2010) showed that an increase in consumer cost-sharing for
prescription drugs initiated by CalPERS, a Medicare supplemental insurance program in
California, resulted in lower utilization of drugs and a higher risk of hospitalization. These risks,
however, would not be borne by CalPERS, but by the Medicare program itself, which pays for
hospitalizations.
Studies that explore spillover effects between drugs that treat risk factors for heart disease and
hospital care are fairly uniform in their conclusion of a substitution relationship (Roebuck et al.
2011; Will et al. 2016; Gibson et al. 2006; Choudhry et al. 2012). Specifically, the consequence
of poor (good) adherence is to make consumers more (less) susceptible to an adverse health
event requiring hospitalization. Studies that estimate spillover effects between high-value drugs
and outpatient care also find a substitution relationship, although there is modest disagreement in
some areas. For example, using three years of longitudinal panel claims data, Gaynor et al.
(2006) concluded that an increase in prescription drug co-payments reduced spending on drugs,
but increased spending and utilization of outpatient care. Similarly, in a study of Pitney Bowes
employees, Choudhry et al. (2012) found that when copayments for statins were lowered for
employees with diabetes or heart disease, rates of physician visits, emergency department visits
and hospitalizations were significantly lower. In a similar study, Gibson et al. (2006)
distinguished between new and continuing users of high-value drugs. They concluded that a
reduction in the copayment for statins was associated with higher adherence, which was
associated with a lower likelihood of emergency department visits and hospitalizations for
continuing users (a substitution effect), but not for new users. Gibson et al. (2006) did not find a
significant association between adherence and physician visits for continuing users.

35
Furthermore, for new users, they found a complementary relationship between drugs and
physician visits.
The most intuitive explanation for a substitution spillover effect between high-value drugs and
other types of health care is that raising the cost of drugs results in lower adherence rates, which
worsens health and increases the likelihood of physician visits, emergency department visits
and/or hospitalizations. But does the same relationship hold in the opposite direction? That is,
for people with risk factors for heart disease, does raising the cost of other types of health care
increase the consumption of high-value drugs? In this study, we take advantage of a change in
the price in other health care to estimate the spillover effect on high-value drugs. To our
knowledge, we are the first study to examine spillover effects in this manner, and our results
have important implications for health insurance design. If our results are consistent with the
substitution effect, then a value-minded insurer could discourage certain forms of health care by
raising its price with the expectation of improving adherence to high-value drugs. On the other
hand, if we find a complementary effect, then raising the price of other types of health care could
lower adherence and potentially reduce health status, which may not be a value-enhancing
outcome.
There are reasons to believe that the effect of increasing medical care prices on high-value drug
consumption is ambiguous. The substitution relationship may persist if, when faced with an
increase in the price of medical care, consumers with risk factors for heart disease substitute
away from certain forms of health care, such as doctor’s visits and inpatient care, to buy more
high-value drugs. On the other hand, spillover effects may work in a complementary, rather than

36
substitute direction for this population. Evidence supporting a complementary response comes
from studies which show that the demand for medical care such as physician office visits (Cockx
and Brasseur, 2003; Jakobsson and Svensson, 2016; Ma et al. 2019) and hospital care (Ma et al.
2019) are inelastic. Although Ellis et al. (2017) concludes that price elasticity estimates for
hospital care tend to be unreliable due to low frequencies, the elasticity of emergency room visits
(which can lead to inpatient care) can be estimated more reliably at -0.04. Additionally, the
inelasticity of inpatient care can be inferred because large adverse health shocks are, by
definition, unpredictable. In this sense, an increase in the price of medical care may result in
little to no change to utilization of certain forms of medical care and, consequently, liquidity-
constrained consumers may instead choose to lower their utilization of high-value drugs.
Another reason to consider a complementary relationship is due to the consumer informational
barriers described in chapter one. Consumers may inappropriately group services that are both
affected and unaffected by the price change if they fail to differentiate between health care that
became more expensive and that which did not. For example, if an insurer increases the price of
medical care but leaves the price of drugs unchanged, consumers may nonetheless assume that
all care has become more expensive and reduce their consumption of both.

37
2.3. Methods
2.3.1. Data
We use de-identified health insurance enrollment and claims data from a large employer in the
Northeast US, covered by a national insurer.11 The data consist of continuously-enrolled in-state,
active employees, as well as their partners and dependents. The enrollment data contain basic
demographic information including age, sex, and residential zip code. The claims data are
subdivided into five commercially-enhanced files containing enrollee-level claims for: (1)
inpatient care; (2) prescription drugs; (3) professional services; (4) outpatient care (header); and
(5) outpatient care (detail claims). 12 13 Each medical claim includes up to four International
Classification of Diseases (ICD) codes, Common Procedural Terminology (CPT) codes, service
location information, and provider name.14 Each drug claim includes the tier, therapeutic group,
generic name, day supply, and National Drug Code. For both medical and drug claims, we
observe the total contractual obligation to the provider (the allowed amount), payment by the
insurer, enrollee cost-sharing amounts, and any coordination of benefit amounts that have been
paid by other insurers, such as Medicare. We also observe dates of service in six-month
intervals. Our data span three fiscal years: 2015 (July 2014 to June 2015), 2016 (July 2015 to
June 2016) and 2017 (July 2016 to June 2017). We divide the data into six-month intervals,
11 Due to confidentiality requirements of our data provider, we are unable to disclose the name or specific location
of the employer.
12 Claims are enhanced by a third party through the addition of claim descriptors. For example, drug claims are
enhanced with the addition of “therapeutic group” and “therapeutic class” variables that provide information about
the type of drug consumed. Medical claims are also enhanced with text descriptions of primary ICD-9 and ICD-10
codes.
13 A header claim is a summary of all services rendered during a single outpatient visit. For example, if an employee
has an outpatient surgery consisting of multiple procedures, the header claim would summarize the cost and nature
of the visit in a single observation. The detail claim lists each procedure separately.
14 Our study period spans the date of mandatory conversion from ICD-9 to ICD-10, so claims data are coded with
both descriptors. Claims coded in ICD-10 are cross-walked back to ICD-9. We use the latter.

38
beginning with the first half of fiscal year 2015 (July 2014 to December 2014) and ending with
the second half of fiscal year 2017 (January 2017 to June 2017).
We supplement the data with two proxy variables to describe physical access to healthcare:
travel time and hospital density. Travel time is defined as the driving time to the nearest acute
care hospital. To compute travel times, we first match the employee’s zip code to population-
weighted zip code tabulation area (ZCTA) centroids obtained from the Missouri Census Data
Center (MCDC, 2016). We then pair ZCTA centroids with the geolocation of all acute care
hospitals within the state and within 20 miles of the border in all neighboring states. Psychiatric
and specialty hospitals are excluded. We calculate travel time using the georoute Stata
command and retain the smallest value for each employee in each time period (Weber and
Péclat, 2016). Our second proxy of health care access is hospital density, calculated as the
number of acute care hospitals within a 20-mile straight line distance of the employee’s
population-weighted ZCTA centroid. Straight line distances are calculated using the geodist
Stata command with the miles and sphere options (Picard, 2010).15
As proxies for income and education, we match each employee’s zip code with the ZCTA
median household income and percentage of residents with a bachelor’s degree or higher. These
data, which come from the American Community Survey, were obtained from the Missouri
Census Data Center (MCDC, 2014-2017).
15 The geodist command with the sphere option calculates great circle straight line distances using the Haversine
formula.

39
2.3.2. Study Inclusion
Figure 2.1 shows the three stages of our sample selection process. In the study eligibility stage,
we retain active employees who, along with any enrolled partners and dependents, resided in the
same state as the employer and were enrolled for all three fiscal years. Additionally, employees
who had a dependent enter or exit the plan within the study time period are excluded. We also
exclude employees who were receiving disability benefits or worker’s compensation, as well as
those who were employed intermittently or receiving COBRA benefits. In this manner, we
define a balanced panel of employees who remained within the same plan tier throughout the
study.

40
Figure 2. 1. Sample Selection Process
Study Eligibility
Continuous enrollment
Continuous in-state residency
Continuous active employment
N = 13,345
HTN Indexing
1st instance of HTN diagnosis or drug fill
HTN Confirmation
Keep confirmed HTN, any time period
N = 3,235
Keep indexed periods 1 and 2
N = 2,566
Keep if spending on both drugs and office visits
N = 2,351
LIP Indexing
1st instance of LIP diagnosis or drug fill
LIP Confirmation
Keep confirmed LIP, any time period
N = 4,128
Keep indexed periods 1 and 2
N = 3,013
Keep if spending on both drugs and office visits
N = 1,981
DM Indexing
1st instance of DM diagnosis or drug fill
DM Confirmation
Keep confirmed DM, any time period
N = 1,161
Keep indexed periods 1 and 2
N = 908
Keep if spending on both drugs and office visits
N = 736

41
In the indexing stage, using both medical and drug claims data, we identify employees who are
likely to have one of the following chronic conditions, all which are risk factors for heart disease:
primary hypertension (HTN), hyperlipidemia (LIP), and type II diabetes (DM). Employees may
be part of more than one study group if they have multiple chronic conditions. We retain all
employees who had a medical encounter with a relevant diagnosis code for the condition or at
least one filled prescription for a relevant drug (for DM, we also include supplies related to
insulin and glucose monitoring). For example, to the create the group of people with likely
HTN, we identify all employees who had a medical encounter with a 401.0 or 401.9 ICD code or
filled a prescription for an anti-hypertensive. We label the earliest time period in which either of
these conditions is met as the index date.
In the confirmation stage, we keep only those employees with a confirmed diagnosis. We do so
by dropping all employees retained from the indexing stage who do not have a medical
encounter with a relevant ICD code in any time period. Using this approach, we eliminate
employees who took drugs to treat the chronic condition of interest, but did not have the
condition. For example, in this stage we drop employees who took anti-hypertensives for reasons
other than primary HTN (e.g. secondary HTN, arrhythmias, preeclampsia). This approach also
allows us to create an accurate index date for employees with HTN who took anti-hypertensive
drugs, but may not have had frequent medical encounters. We keep only those who are indexed
to the first or second six-month intervals (fiscal year 2015) and have both office visits and drug
spending at any point during the study period. Refer to tables A.1-A.3 in the appendix for a full
listing of ICD codes and drug types considered in this study.

42
2.3.3. Health Plan and Policy Change
The health plan is a point-of-service plan administered by a national insurer, and is the only plan
offered to employees. In this way, we avoid enrollee adverse selection at the plan level, though
we are not able to address firm-level selection into plan offering. The plan distributes employee
cost-sharing using a combination of deductibles, co-payments, co-insurance, and out-of-pocket
maximums. Hospital, physician, and specialist care are broadly structured as a three-tiered
system with varying copayments or coinsurance levels for in-network preferred, in-network non-
preferred, and out-of-network providers. The plan generates considerable incentive to access in-
network providers. For example, as shown in Table 2.1, cost-sharing for primary care physician
(PCP) office visits in fiscal year 2015 was $0 for in-network preferred providers and $20 for in-
network non-preferred providers. Out-of-network providers were subject to a $500 deductible,
after which the plan paid a 60% coinsurance rate.
Also shown in Table 2.1, prescription drug benefits were offered in three copayment tiers:
generic, preferred brand-name, and non-preferred brand-name. In fiscal year 2015, the
copayment for a 30-day supply of a prescription drug was $10 for generics, $30 for preferred
brand name, and $45 for non-preferred brand name. State law required all prescriptions filled
under an insurance plan to be dispensed as generics. Brand name prescriptions could only be
filled if there was no generic equivalent or if the prescriber specifically indicated that the brand
name should be “dispensed as written.” Otherwise, any consumer requesting brand-name drug
with a generic equivalent was required to pay the full difference in cost between the generic and
brand-name drug.

43
Table 2. 1. Selected Plan Features and Benefit Provisions, by Fiscal Year
Plan Spending Limits FY 2015 FY 2016 FY 2017
In-Network Deductible (I/F) $500/$1,000 $500/$1,000 $600/$1,200
Non-Network Deductible (I/F) $2,500/$5,000 $2,500/$5,000 $3,000/$6,000
In-Network OOP Max (I/F) $2,000/$4,000 $2,000/$4,000 $2,000/$4,000
Non-Network OOP Max (I/F) $5,000/$10,000 $5,000/$10,000 $5,000/$10,000
Prescription Drug OOP Max (I/F) -- $4,200/$9,200 $4,200/$9,200
Plan Cost-Sharing Amounts
Preventive Care $0 $0 $0
PCP Office Visits, P $0 $0 $20
PCP Office Visits, NP $20 $20 $40
PCP Office Visits, NN 60% 60% 60%
Specialist Office Visits $25 $25 $30
Inpatient Physician Services, P 90% 90% 90%
Inpatient Physician Services, NP 80% 80% 80%
Inpatient Physician Services, NN 60% 60% 60%
Emergency Department $300 $300 $300
Complex Imaging $50 $50 $50
Prescription Drugs (30-day sup.) $10/$30/$45 $10/$30/$45 $10/$30/$45
Prescription Drugs (31to 90-day sup.) $15/$45/$70 $15/$45/$70 $15/$45/$70
I/F = individual/family coverage, PCP = primary care physician, OOP = out of pocket, P=In network, preferred.
NP = In network, non-preferred, NN = non-network. Percentage amounts indicate the coinsurance rate paid by
the plan once the deductible is met. Prescription drug amounts indicate copayments for generic/preferred brand-
name/non-preferred brand-name.

44
In fiscal year 2017, the employer increased copayments and deductibles affecting a broad range
of medical services (Table 2.1). Some increases were small in nominal terms, but quite large in
relative terms. For example, in-network preferred PCP office visits increased from $0 to $20 and
in-network non-preferred PCP office visits doubled from $20 to $40. Specialist office visits
increased by 20%, from $25 to $30. Additionally, the deductible increased from $500 to $600
for individuals. There were no changes to copayments for prescription drugs. The only
exception is the introduction of a new out-of-pocket maximum on prescription drugs in fiscal
year 2016, separate from the medical out-of-pocket maximum.
2.3.4. Study Design
We take advantage of a natural experiment where the price of medical care increased, but the
price of drugs remained unchanged. Specifically, we examine whether employees with HTN,
LIP, and DM modified their consumption of office visits and drugs used to treat these conditions
after medical care became more expensive. We do so by comparing the change in consumption
before the price increase to the change in consumption after the price increase. Figure 2.2
depicts our overall design. We define a baseline period as the change in consumption that took
place between the first two fiscal years of the study (FY ’15 & FY ’16) where there were no
changes to consumer cost-sharing levels. 16 We define an intervention period as the change in
consumption that took place between the second and third fiscal years of the study (FY ’16 & FY
’17) where the cost-sharing amounts for medical care increased. To account for seasonal trends,
we difference consumption on a same half-year basis. In this manner, our baseline period
16 As noted above, the insurer implemented a new out-of-pocket maximum for prescription drugs in fiscal year 2016.
For consumers with high out-of-pocket pharmaceutical spending, this may have impacted the consumption of drugs.
We consider this as a robustness check.

45
observations consist of seasonally-controlled changes in consumption from FY’ 15 to FY ’16.
Our intervention period observations consist of the seasonally-controlled changes in
consumption from FY ’16 to FY ’17.
This study did not receive outside funding and was exempted for review by the Internal Review
Board at the University of Maine because the claims data were de-identified. Correspondence to
this effect can be produced upon request.
2.3.5. Estimation
For each chronic condition group, we consider four dependent variables: the expenditure and
utilization of drugs used to treat these conditions, as well as the expenditure and utilization of
office visits. Our measure of expenditure is the allowed amount, or the total amount owed to the
health care provider, which equals the sum of the insurance plan payment and employee cost-
First Half of FY
2016 – First Half
of FY 2015
Second Half of
FY 2016 – Second
Half of FY 2015
First Half of FY
2017 – First Half
of FY 2016
Baseline Intervention
Second Half of
FY 2017 – Second
Half of FY 2016
Figure 2. 2. Study Design

46
sharing amount.17 Our measure of utilization for drugs is the number of days supplied in a single
prescription and our measure of utilization for office visits is the number of visits. 18 We
classify an office visit as a medical encounter tagged with one of ten possible CPT codes (table
A.4 in the appendix). We drop office visits that are highly likely to be miscoded based on setting
or service type. For example, we drop office visits reported to take place in an emergency room
or coded as an operating room service. As indicated previously, we difference each dependent
variable to account for trends in consumption.
The differencing equation is:
Δ𝑌𝑖ℎ𝑡 = 𝑌𝑖ℎ𝑡 − 𝑌𝑖ℎ𝑡−1
(2.1)
For each heart disease risk factor (HTN, DM, and LIP), the 𝑌𝑖ℎ𝑡 represents one of four dependent
variables for individual 𝑖 in half-year ℎ and fiscal year 𝑡. Additionally, because the absolute
level of spending may vary between the three heart disease risk factor groups, we normalize our
differenced dependent variables to enable comparison of changes across groups.
The normalizing equation is:
𝑍𝑖ℎ𝑡 =Δ𝑌𝑖ℎ𝑡
𝑌ℎ(𝑡−1)̅̅ ̅̅ ̅̅ ̅̅ ̅
𝑍𝑖ℎ𝑡, therefore, can be interpreted as a percentage change. It is the individual’s same-
season change in consumption across fiscal years relative to the same-season group
(2.2)
17 In practice, we only observe the cost-sharing responsibility of the employee, not whether the amount was actually
paid. This is a common barrier in studies using claims data.
18 In each six-month interval, for each employee, we add together the total number of office visits and days supplied
for all drugs.

47
mean level of consumption in the base fiscal year. For example, a consumer spends
$150 on drugs in the first half of FY ’15 and $200 on drugs in the first half of FY ’16.
The average level of group drug spending in the first half of FY ’15 was $100. For
this consumer, 𝑍𝑖ℎ𝑡 =$200−$150
$100= 0.50. The interpretation is that from FY ’15 to FY
’16, this consumer’s first half spending increased by 50% of the group mean level of
first half spending in FY ’15.
Our estimation equation is:
𝑍𝑖ℎ𝑡 = 𝛽0 + 𝛽1𝑃𝑜𝑠𝑡𝑖ℎ𝑡 + (𝑿𝒊𝒉𝒕 − 𝑿𝒊𝒉𝒕−𝟏)𝜶 + 𝑢𝑖 + 𝜖𝑖ℎ𝑡
(2.3)
𝛽0 is our intercept term and 𝛽1is our coefficient of interest. It pertains to 𝑃𝑜𝑠𝑡𝑖ℎ𝑡, which is a
dummy variable that takes a value of one if an observation occurs in the intervention period and
zero otherwise. A statistically significant, negative 𝛽1coefficient would suggest, in percentage
point terms, that the conditional mean change in consumption of the dependent variable during
the intervention period was lower than the conditional mean change during the baseline period.
This would indicate that the medical care price increase was associated with a lower rate of
consumption, ceteris paribus. The (𝑿𝒊𝒉𝒕 − 𝑿𝒊𝒉𝒕−𝟏)𝜶 term is a matrix of same-season
differenced covariates that pre-multiply a vector of coefficients. Our covariates include
observable socio-demographic, health status, payor, and market characteristics. The socio-
demographic covariates are: age group (under 19 years, 19-44 years (base group), 45-64 years,
and 65+ years), ZCTA % population with a bachelor’s degree or higher, ZCTA median
household income, travel time to the nearest acute care hospital, and the number of acute care

48
hospitals within a 20-mile radius.19 Because these covariates are differenced, they are non-zero
only if an employee moved to a new age group or residence in a different ZCTA.
We account for changes in health status by differencing each employee’s per-period number of
visits to the emergency department. Although an employee’s propensity to visit the emergency
department can involve attributes other than health, we assume that an employee’s non-health
related propensity to visit the emergency department remains constant over time.
In terms of payor characteristics, we include a dummy variable equaling one if we observe a
coordination of benefit (COB) amount and then difference this variable across periods. A
positive value for COB, therefore, would indicate that a new secondary payor assisted in
providing benefits during the time period (e.g. Medicare). The addition (or subtraction) of this
new payor could lead employees to spend differently than employees without a change in COB.
We also attempt to control for market factors that could have influenced health spending during
the study period. One such factor is the introduction of new drugs, which could impact
spending, especially if an inexpensive generic displaces market share from a brand name drug on
a large scale. To account for this, we include a dummy variable for certain drugs that were
released during the study period and purchased by an employee in our sample. This variable
takes a value of one for employees with pharmacy claims for the drug and zero otherwise, and is
differenced in the same manner as the other covariates. Specifically, for the HTN group, we
19 Age groupings are based on the CMS classification for reporting personal health care spending, with the 65-84
and 85+ age groups combined due to the low number of employees aged 85+ in our sample.

49
create dummy variables for generic versions of Azor, Benicar, Benicar HCT, and Exforge. There
were no other new drugs purchased by the HTN group during this period. For the LIP group,
we create dummy variables for generic versions of Crestor, Lescol XL, Vytorin, and Zetia. There
were no other new drugs purchased by the LIP group during this period. For the DM group, we
create dummy variables for Jardiance, Tresiba Flextouch U-200, Toujeo Solostar, and Trulicity.
We limited our selection of drugs in the DM group, all brand name, to any drug that exceeded
1% of market share in any time period. As a robustness check, we lower this threshold to 0.5%
and re-estimate with added drugs.20
There are two error terms in our estimation equation. 𝑢𝑖 denotes time-constant individual-level
effects and 𝜖𝑖ℎ𝑡 denotes the idiosyncratic error term. In practical terms, 𝑢𝑖 represents
characteristics related to an individual’s healthcare choices that are time-constant, but
unobservable. These factors may include the degree by which an individual trades off future
health benefits for current consumption or a prescriber’s propensity to recommend certain forms
of healthcare. Observable, time-constant factors are also a part of 𝑢𝑖 because they are
indistinguishable from unobservables from an estimation standpoint (e.g. sex, the individual’s
relationship to the plan employee). All other time-variant individual-level factors that we do not
observe, such as income and health shocks not proxied by our covariates, are part of the
idiosyncratic error term.
20 There was only one new generic DM drug that was introduced to the market during the study period, a generic
version of Glyset. We do not include generic Glyset in our estimations because there were only three prescriptions
filled in the entire dataset.

50
For each of the four dependent variables in each of the three chronic disease groups, we first
estimate equation 2.3 using a GLS random-effects model, and test it using the xtoverid Stata
command (Schaffer and Stillman, 2006) with a null rejection criteria set to p ≤ 0.10. This
command computes a Sargan-Hansen’s J-statistic and tests the null hypothesis that GLS random
effects and the same estimation with fixed effects are indistinguishable. Failure to reject this null
means that GLS random effects estimates are more efficient (and thus preferred) relative to fixed
effects, and we retain random effects as our main specification. If the null is rejected, we
estimate and retain a fixed effects model. A third possible outcome is that the test is unable to
compute a J-statistic due to zero variance in the 𝑢𝑖 term. In this case, random effects are
equivalent to pooled OLS, so we use the latter as our main specification.
If we retain GLS estimates, we conduct a Breuch-Pagan Lagrange multiplier test using the
xttest0 Stata command as a check on the significance of the variance of the 𝑢𝑖 term. Under the
null hypothesis, the variance of 𝑢𝑖 equals zero, which means that random effects estimation is
equivalent to pooled OLS, so we use the latter. If we reject the null hypothesis, we retain the
GLS results. In all cases, our standard errors are clustered at the household level. All statistical
computations are done in Stata 15.1.
2.3.6. Robustness Checks
We conduct three robustness checks. In the first, we consider whether our estimates of the effect
of the price change were impacted by the out-of-pocket maximum for prescription drugs, which
was introduced mid-study, in fiscal year 2016. This likely affected top drug spenders, who were
no longer able to include drug spending with other medical spending under a single out-of-
pocket limit. We examine the extent to which this affected our estimates by dropping employees

51
at or above the 95th percentile in out-of-pocket spending on drugs in fiscal year 2015, then re-
running the regressions. As a second check, for the HTN and LIP groups, we investigate
whether dual membership in the DM group influenced our results, since DM is associated with
increased costs of care for individuals with cardiovascular disease (Nichols & Brown, 2002).
Finally, we also consider whether the addition of two brand name drugs, Invokamet and
Humalog Kwikpen U-200, each accounting for between 0.5%-1.0% of market share in the DM
group, impacted our results.
2.4. Results
2.4.1. Characteristics of Chronic Disease Groups
Table 2.2 presents characteristics of the three chronic disease groups, as observed in the first
time period (first half of fiscal year 2015). In general, we do not observe substantial differences
between these groups in terms of the covariates or other descriptors. As might be expected of a
non-retired population with chronic disease, the majority of individuals are in the 45-64 age
group. At 1%, the DM group has a notably larger population under the age of 19 than the LIP or
HTN groups. On average, individuals live within 20 miles of two to three acute care hospitals
and are less than a 20-minute drive from the nearest acute care hospital.

52
Table 2. 2. Characteristics of the HTN, LIP and DM Groups in the First Half of Fiscal Year 2015
HTN LIP DM
Covariates
Age Category (percent, se)
<19 0.21 (0.10) 0.05 (0.05) 1.09 (0.38)
19-44 13.53 (0.71) 9.99 (0.67) 13.99 (1.28)
45-64 79.03 (0.84) 82.18 (0.86) 78.67 (1.51)
65+ 7.23 (0.53) 7.77 (0.60) 6.25 (0.89)
# Emergency Department Visits 0.13 (0.01) 0.13 (0.01) 0.16 (0.02)
Time to Nearest Hospital (min) 17.54 (0.22) 17.70 (0.23) 17.86 (0.40)
Hospital Density 2.33 (0.02) 2.34 (0.02) 2.29 (0.03)
ZCTA % Bachelors or Higher 28.14 (0.23) 28.00 (0.25) 27.60 (0.37)
ZCTA Median Household Income 52,538 (285) 52,349 (294) 51,904 (478)
Coordination of Benefits (percent, se) 0.43 (0.13) 0.15 (0.09) 0.41 (0.24)
Other Sample Characteristics
Female (percent, se) 45.25 (1.03) 41.85 (1.11) 45.38 (1.84)
Policy Tier (percent, se)
Employee Only 45.04 (1.03) 44.32 (1.12) 44.97 (1.83)
Employee + One 28.97 (0.94) 31.04 (1.04) 30.30 (1.70)
Employee + Dependent 6.93 (0.52) 6.36 (0.55) 7.20 (0.95)
Family 19.06 (0.81) 18.27 (0.87) 17.52 (1.40) Relation (percent, se)
Employee 77.37 (0.86) 76.73 (0.95) 75.14 (1.59)
Spouse 21.40 (0.85) 22.06 (0.93) 22.15 (1.53)
Dependent 1.23 (0.23) 1.21 (0.25) 2.72 (0.60)
# Individuals
2,351 1,981 736
Hospital density is the number of hospitals within 20 miles of the population-weighted ZCTA. Median
household income is in 2017$. Coordination of benefits is the percentage of the sample with an observed
coordination of benefits amount from the medical claims data.

53
We find that individuals receiving any COB are relatively rare. For example, individuals with a
COB represent 0.43% of the HTN group, and this was the largest share of any group. However,
the true COB level is likely understated since it is only observed when an individual consumes
health care. Additionally, COB will likely become more common over time as our sample ages
and individuals become Medicare-eligible. In the appendix, we provide a table of characteristics
of individuals with chronic diseases excluded from our analysis due to having zero spending on
either drugs or office visits (Table A.5). The zero-spending group appears to be younger, with a
larger proportion of women in the LIP and DM groups and a larger proportion of men in the
HTN group. Additionally, there are more members with family plans in the zero-spending
group, relative to the study group. The groups appear similar in the other covariates.
2.4.2. Summary of Consumption Trends
In table 2.3, we describe trends in the half-year expenditure and utilization levels of our
dependent variables, starting with the HTN group. We see that mean half-year spending on
drugs for people with HTN increases by $0.54 (0.62%) over the two fiscal years in the baseline
period. During the intervention period, we see a notable change in the trend, where half-year
drug spending falls by an average of $6.52 (-7.39%). Interestingly, we observe no such reversal
of trends in drug day supply between the baseline and intervention periods, where we observe
similar-sized increases in both periods. Taken together, this suggests that individuals with HTN
reversed their rate of drug spending while sustaining baseline drug quantity trends. We also see
a trend reversal for office visit spending, which grew by an average of $6.41 (1.96%) during the
baseline period, but fell by an average of $7.75 (-2.33%) during the intervention period.

54
Table 2. 3. Changes in Dependent Variables during the Baseline and Intervention Periods, Means
and Percentages
𝚫 Baseline %𝚫Baseline 𝚫Intervention %𝚫Intervention
HTN (N = 2,351)
Drug Spending 0.54 (1.67) 0.62 -6.52 (2.33) -7.39
Drug Day Supply 9.82 (1.61) 4.47 8.05 (1.56) 3.51
Office Visit Spending 6.41 (5.34) 1.96 -7.75 (5.37) -2.33
Office Visits 0.10 (0.04) 3.57 -0.04 (0.04) -1.38
LIP (N = 1,981)
Drug Spending -0.03 (4.74) -0.01 -73.31 (5.18) -33.67
Drug Day Supply 5.98 (1.25) 4.58 5.52 (1.22) 4.04
Office Visit Spending 7.21 (5.48) 2.28 -3.17 (5.82) -0.98
Office Visits 0.09 (0.04) 3.32 0.02 (0.05) 0.71
DM (N = 736)
Drug Spending 526.36 (50.11) 35.68 308.74 (44.61) 15.43
Drug Day Supply 33.83 (3.40) 14.81 16.70 (3.16) 6.37
Office Visit Spending -2.67 (10.47) -0.62 -0.70 (10.34) -0.16
Office Visits 0.09 (0.08) 2.56 0.08 (0.09) 2.22
Columns 1 and 3 describe the mean (se) change in the dependent variables during the baseline and intervention
periods, respectively. Columns 2 and 4 describe the mean change as a percentage of the mean level of spending
during the period. For example, individuals with HTN spent an average of $0.54 more on drugs in fiscal year 2015
compared to fiscal year 2016. Relative to the level of drug spending in fiscal year 2015, this amounts to an average
0.62% increase in half-year spending per individual. Mean levels of expenditure and utilization for each fiscal year
can be found in the appendix table A.6. Spending is in 2017$. Drug day supply and office visits are counts.

55
We also observe a trend reversal for office visits, which grew at an average of 0.10 visits
(3.57%) during the baseline period and fell by 0.04 visits (-1.38%) visits during the intervention
period.
Trends for the LIP group are similar in terms of direction, but some are larger in magnitude. The
average baseline change in half-year drug spending was -$0.03 (-0.01%). During the
intervention period, the average change in half-year drug spending was -$73.31 (-33.67%),
which is larger than the decline in drug spending for the HTN group. We do not see a trend
reversal in the number of office visits, but we do see a slower rate of increase in the intervention
period (0.02 visits, 0.71%) compared to the baseline (0.09 visits, 3.32%).
For the DM group, there was a $526.36 (35.68%) increase in drug spending during the baseline
period, followed by a smaller increase of $308.74 (15.43%) during the intervention period. This
was accompanied by an increase of drug day supply of 33.83 days (14.81%) in the baseline
period and 16.70 days (6.37%) during the intervention period. This differs from the HTN and
LIP groups, where changes in drug supply were similar during the baseline and intervention
periods. For the DM group, there are negligible changes in consumption patterns for office
visits.
We also depict consumption trends over time with a series of figures. Figure 2.3 depicts the per-
period mean consumption of each of the dependent variables for the HTN group. We observe a
sharp drop in drug expenditure during the latter two time periods that define FY’17, the
intervention period. In contrast, drug day supply appears to maintain a steady increase

56
throughout the study period. Spending and utilization of office visits show more of a seasonal
pattern of consumption with no clear disruption in trend.
Figure 2. 3. Consumption Trends for the HTN Group
Baseline and intervention periods are demarcated by the vertical dashed line through the first half of 2016, which
was the final half-year of the baseline period.
Figure 2.4 depicts the per-period mean consumption of each of the dependent variables for the
LIP group. Similar to the HTN group, we observe a sharp drop in drug expenditure during the
intervention period with a steady increase in drug utilization throughout the study period, albeit
there appears to be a pause in the trend during the second half of 2016. Spending and utilization
of office visits show a seasonal pattern of consumption with no clear disruption in trend.

57
Figure 2. 4. Consumption Trends for the LIP Group
Baseline and intervention periods are demarcated by the vertical dashed line through the first half of 2016, which
was the final half-year of the baseline period.
Figure 2.5 depicts the per-period mean consumption of each of the dependent variables for the
DM group. In contrast to the HTN and LIP groups, we do not observe a sharp drop in the level
of spending during the intervention period. Rather, we see that spending levels off during the
second half of 2016, followed by an increase in the first half of 2017 – a pattern seemingly
replicated in drug day supply. Spending on office visits shows an irregular seasonal pattern of
consumption, and visits seem to be more seasonal with what appears to be an underlying upward
trend.

58
Figure 2. 5. Consumption Trends for the DM Group
Baseline and intervention periods are demarcated by the vertical dashed line through the first half of 2016, which
was the final half-year of the baseline period.
2.4.3. Regression Results
For all four estimations in each chronic disease group, our dependent variable is the relative
(percentage) change in consumption as defined in equations 1.1 and 1.2. We include regressions
where the dependent variable is defined in dollar amounts in Appendix 2, tables A.7-A.9. Table
2.4 contains regression estimates for the HTN group. The table headers denote each of the four
dependent variables and the type of estimator used. The results indicate that an increase in the
price of medical care during the intervention period was associated with an 8 percentage-point
reduction in the rate of change in half-year spending on drugs to treat HTN. In other words, the
average change in per-person half-year spending in the intervention period was 8 percentage
points lower than it might have been, had the medical price increase not taken effect. This effect

59
was significant at the 5% level. The increase in the price of medical care did not affect the rate
of change in drug day supply. In terms of office visits, it had weakly significant and negative
effect on the change in spending and number of visits. The average change in the rate of half-
year spending and utilization of office visits during the intervention period was 5 percentage
points lower than the baseline period. Our key estimates are net of the effect of generic market
entry, which is accounted for in the regressions.

60
Table 2. 4. Regression Results: Normalized Spending and Utilization for the HTN Cohort
Drugs
Office Visits
Δ Spending
Δ Day Supply
Δ Spending
Δ Visits
Estimator OLS FE OLS OLS
Variable
Post -0.08** -0.01 -0.05* -0.05*
(0.04) (0.01) (0.03) (0.03)
Δ ED visits -0.02 0.02** 0.32*** 0.30***
(0.03) (0.01) (0.03) (0.03)
Δ Time to Nearest Hospital 0.02** 0.00 0.00 0.00
(0.01) (0.00) (0.01) (0.01)
Δ Hospital Density 0.26 0.03 0.13* 0.16**
(0.19) (0.06) (0.08) (0.08)
Δ ZCTA % Bachelor’s + 0.01 0.00 0.00 0.00
(0.01) (0.01) (0.01) (0.01)
Δ ZCTA Median HH Income 0.00** 0.00 0.00 0.00
(0.00) (0.00) (0.00) (0.00)
Aged 19 0.24 0.43 -0.82 -0.59
(0.24) (0.31) (0.77) (0.94)
Aged 45 0.09 0.02 0.11 0.09
(0.07) (0.06) (0.08) (0.08)
Aged 65 0.05 0.09** 0.07 0.06
(0.05) (0.04) (0.06) (0.06)
COB + 0.08 -0.11 0.24 -0.03
(0.11) (0.17) (0.26) (0.23)
COB - 0.10 -0.14 0.06 0.10
(0.13) (0.13) (0.28) (0.31)
Generic Azor -6.58*** 0.47*** -0.13 0.02
(0.34) (0.03) (0.51) (0.49)
Generic Benicar 2.13 -0.09 -0.39 -0.48
(2.21) (0.25) (0.41) (0.42)
Generic Benicar HCT -1.06 0.08** -0.79 -0.66
(1.39) (0.04) (0.50) (0.54)
Generic Exforge -12.36*** -0.01 -0.86*** -0.78***
(0.02) (0.01) (0.02) (0.02)
# Observations
9,404 9,404 9,404 9,404
# Individuals
2,351
2,351
2,351
2,351
All variables describe the year-over-year change in 6-month, same-period consumption or status. OLS = Ordinary
Least Squares; FE = Fixed Effects Estimation; COB+/- = Gained/Lost Coordination of Benefits. Travel time is in
minutes, density is # of hospitals within a 20-mile radius, median HH income is normalized to 100s of 2017$.
Effect of generic drugs is for new prescriptions. Cluster robust standard errors are reported in parentheses.
***p<0.01; **p<0.05; *p<0.10

61
Table 2.5 contains regression estimates for the LIP group. We find that an increase in the price
of medical care was associated with a 26 percentage-point decrease in the rate of change in half-
year drug spending. This effect is statistically significant at the one percent level. However, the
increase in the price of medical care had no (statistically significant) effect on the change in drug
day supply. Unlike the HTN group, the increase in the price of medical care did not affect the
change in office visit spending or utilization. This suggests a very low own-price elasticity of
demand for office visits. Our key estimates are net of the effect of generic market entry, which is
accounted for in the regressions.

62
Table 2. 5. Regression Results: Normalized Spending and Utilization for the LIP Cohort
Drugs
Office Visits
Δ Spending
Δ Day Supply
Δ Spending
Δ Visits
Estimator OLS OLS OLS OLS
Variable
Post -0.26*** -0.01 -0.03 -0.03
(0.04) (0.02) (0.03) (0.03)
Δ ED visits 0.02 0.01 0.30*** 0.28***
(0.02) (0.01) (0.03) (0.03)
Δ Time to Nearest Hospital -0.01 0.00 0.00 0.00
(0.01) (0.00) (0.01) (0.01)
Δ Hospital Density 0.02 0.03 0.07 0.12
(0.20) (0.05) (0.11) (0.11)
Δ ZCTA % Bachelor’s + 0.01 0.00 -0.01 -0.01
(0.01) (0.00) (0.01) (0.01)
Δ ZCTA Median HH Income 0.00 0.00 0.00 0.00
(0.00) (0.00) (0.00) (0.00)
Aged 19 0.26*** 0.29*** -0.71*** -0.29*** (0.03) (0.02) (0.04) (0.03)
Aged 45 0.09 0.02 -0.12 -0.11
(0.18) (0.05) (0.09) (0.08)
Aged 65 -0.07 -0.05 -0.10 -0.07
(0.10) (0.04) (0.07) (0.07)
COB + 0.13 0.03 0.07 -0.15
(0.09) (0.13) (0.51) (0.35)
COB - 0.22 0.03 0.27 0.46
(0.15) (0.20) (0.28) (0.33)
Generic Crestor -1.34*** 0.12*** -0.15*** -0.12**
(0.16) (0.03) (0.06) (0.06)
Generic Zetia 0.25 0.19 0.33 0.20
(0.58) (0.13) (0.27) (0.24)
Generic Vytorin -1.14** -0.03*** -1.04 -0.80
(0.49) (0.01) (1.42) (1.29)
Generic Lescol XL -1.03*** -0.08** -0.27 -0.20
(0.24) (0.04) (0.20) (0.16)
# Observations
7,924 7,924 7,924 7,924
# Individuals
1,981
1,981
1,981
1,981
All variables describe the year-over-year change in 6-month, same-period consumption or status. OLS = Ordinary
Least Squares; COB+/- = Gained/Lost Coordination of Benefits. Travel time is in minutes, density is # of
hospitals within a 20-mile radius, median HH income is normalized to 100s of 2017$. Effect of generic drugs is
for new prescriptions. Effects for losing prescriptions are omitted. Cluster robust standard errors are reported in
parentheses. ***p<0.01; **p<0.05; *p<0.10

63
Table 2.6 contains regression estimates for the DM group. The increase in the price of medical
care is associated with a 22 percentage-point reduction in the rate of change in half-year
spending on drugs. The price increase is also associated with a 9 percentage-point reduction in
the rate of change in half-year drug day supply. Both effects are statistically significant at the
one percent level. Similar to the LIP group, the increase in the price of medical care did not
affect the rate of change in spending or utilization for office visits. Our key estimates are net of
the effect of brand name market entry, which is accounted for in the regressions.

64
Table 2. 6. Regression Results: Normalized Spending and Utilization for the DM Cohort
Drugs
Office Visits
Δ Spending
Δ Day Supply
Δ Spending
Δ Visits
Estimator GLS, RE FE OLS OLS
Variable
Post -0.22*** -0.09*** -0.01 -0.01
(0.05) (0.02) (0.04) (0.04)
Δ ED visits -0.01 0.01 0.23*** 0.22***
(0.04) (0.02) (0.03) (0.04)
Δ Time to Nearest Hospital 0.00 0.00 0.01 0.01
(0.01) (0.01) (0.01) (0.01)
Δ Hospital Density 0.13 -0.01 -0.03 0.02
(0.09) (0.09) (0.18) (0.16)
Δ ZCTA % Bachelor’s + 0.02* 0.00 0.01 0.02
(0.01) (0.01) (0.01) (0.01)
Δ ZCTA Median HH Income 0.00 0.00* 0.00* 0.00*
(0.00) (0.00) (0.00) (0.00)
Aged 19 0.14 -0.22 -0.52 -0.18 (0.24) (0.15) (0.42) (0.22)
Aged 45 0.02 0.12 -0.06 -0.03
(0.11) (0.10) (0.12) (0.13)
Aged 65 0.11 0.03 0.20 0.16
(0.15) (0.07) (0.13) (0.12)
COB + -0.67*** -0.30 -0.13 -0.10
(0.22) (0.20) (0.27) (0.21)
COB - 0.32 0.54*** 0.68*** 0.84***
(0.47) (0.07) (0.16) (0.19)
Trulicity 1.21*** 0.26** 0.10 0.12
(0.17) 0.10 (0.13) (0.12)
Tresiba Flextouch 0.19 -0.08 -0.04 -0.05
(0.26) (0.17) (0.12) (0.15)
Toujeo Solostar 0.26 0.54** 0.08 0.16
(0.30) (0.26) (0.14) (0.20)
Jardiance 0.27 0.48*** 0.19 0.27**
(0.50) (0.11) (0.14) (0.11)
# Observations
2,944
2,944
2,944
2,944
# Individuals
736
736
736
736
All variables describe the year-over-year change in 6-month, same-period consumption or status. OLS = Ordinary
Least Squares; GLS, RE = Generalized Least Squares, Random Effects; FE = Fixed Effects Estimation; COB+/-
= Gained/Lost Coordination of Benefits. Travel time is in minutes, density is # of hospitals within a 20-mile
radius, median HH income is normalized to 100s of 2017$. Effect of generic drugs is for new prescriptions.
Effects for losing prescriptions are omitted. Cluster robust standard errors are reported in parentheses.
***p<0.01; **p<0.05; *p<0.10

65
2.4.4. Robustness Checks
Table 2.7 describes the results of our robustness checks. Dropping top spenders reduces (makes
less negative) the effect of the medical price change on drug spending for all three groups by
approximately 1-2 percentage points. We find no change to our results for drug day supply.
Likewise, we find no change to our results for office visits in the LIP and DM groups. We do,
however, find a 1 percentage-point larger (more negative) effect for spending and utilization of
office visits in the HTN group, which is significant at the 5% level. We find no effect having a
dual diagnosis of DM in either the HTN or LIP groups.21 Lastly, adding two additional brand
name drugs to the DM sample has no appreciable effect on our results. Taken together, we find
little evidence that our key estimates are driven by the new out-of-pocket maximum for
prescription drugs, dual diagnoses, or by including DM brand name drugs with lower market
share.
21 Our approach for the dual diagnosis robustness check was to add a non-differenced dummy variable to our LIP
and HTN main specifications, signifying membership in the DM group. Because our specification for drug day
supply for the HTN group was fixed effects, we could not use this approach due to multicollinearity. Based on our
results of the other checks, which were estimated with OLS and concluded no significant dual diagnosis effect, we
do not believe that omitting this check materially influenced our results. A more rigorous examination of dual
diagnosis effects is a subject for future study.

66
Table 2. 7. Regression Results, Robustness Checks
Drugs
Office Visits
Δ Spending
Δ Day Supply
Δ Spending
Δ Visits
HTN
Post -0.08** -0.01 -0.05* -0.05*
(0.04) (0.01) (0.03) (0.03)
Post, excluding high spend -0.07** -0.02 -0.05* -0.06**
(0.03) (0.01) (0.03) (0.03)
Post, dual diagnosis -0.08** n/a -0.05* -0.05*
(0.04) n/a (0.03) (0.03)
LIP
Post -0.26*** -0.01 -0.03 -0.03
(0.04) (0.02) (0.03) (0.03)
Post, excluding high spend -0.25*** -0.02 -0.03 -0.03
(0.04) (0.02) (0.03) (0.03)
Post, dual diagnosis -0.26*** -0.01 -0.03 -0.03
(0.04) (0.02) (0.03) (0.03)
DM
Post -0.22*** -0.09*** -0.01 -0.01
(0.05) (0.02) (0.04) (0.04)
Post, excluding high spend -0.20*** -0.09*** -0.03 -0.02
(0.05) (0.02) (0.04) (0.04)
Post, added drugs -0.21*** -0.09*** -0.01 -0.01
(0.05) (0.02) (0.04) (0.04)
This table compares the effect of the medical price change before and after removal of employees that were in the
top 95% of out-of-pocket drug spending in FY’15. It also compares the effect of adding two additional brand
name drugs with lower market share in the DM estimates.

67
2.5. Discussion and Conclusion
Our objective was to better understand the relationship between high-value drugs used to treat
risk factors for heart disease and other health care. Previous studies have generally defined them
as substitutes, where an increase in the price of drugs leads to an increase in the consumption of
other health care. We sought to determine whether they also function as substitutes when the
price of other health care increases, but the price of drugs remains the same. For all groups, we
found that a small, but broad increase in the price of medical care was associated with a
statistically significant decrease in the rate of change in half-year drug spending. The effect was
small and moderately significant (-8pp, p<0.05) for employees with primary hypertension, but
was large and strongly significant for those with hyperlipidemia (-26pp, p<0.01) and type-II
diabetes (-22pp, p<0.01). The effects were net of mid-study market entry of new drugs. For
employees with primary hypertension and hyperlipidemia, this was not accompanied by a change
in the rate of drugs consumed. We therefore conclude that medical care and high-value drugs
intended to treat risk factors for heart disease do not function as substitutes when the price of
medical care changes (unlike when the price of drugs is changed). In fact, for employees with
type-II diabetes, the two types of health care may be viewed as complements since the increase
in price of medical care was associated with a reduction in rate of change in half-year drug
utilization.
We also found, common across groups, a muted response to the increase in the price of medical
care on the spending and utilization of office visits. Specifically, we found that an increase in
the price of medical care was associated with a small and weakly negative (-5pp, p<0.10) impact
on the rate of office visit spending and utilization for employees with hypertension, and had no

68
statistically significant effect on the rate of spending and utilization of office visits for employees
with hyperlipidemia and type-II diabetes. These results suggest that office visits are highly price
inelastic, consistent with past findings (Cockx and Brasseur, 2003; Jakobsson and Svensson,
2016; Ma et al. 2019).
For employees with primary hypertension or hyperlipidemia, the results were especially
interesting. These employees did not modify their rate of drug utilization, but significantly
lowered their rate of drug expenditure. Three mechanisms could explain this finding. First,
employees could have substituted to lower-priced generics during the intervention period. This
would have allowed employees to maintain underlying quantity trends while reducing spending
trends, since generics provide the same therapeutic effect at a lower cost, both to the consumer
and the insurer. We view this mechanism as unlikely, however, due to “dispense as written”
provisions which required all drugs to be dispensed as generics unless the prescriber specifically
indicated otherwise. Thus, for this mechanism to be valid, there would need to be a considerable
number of employees who, together with their prescribers, overcame legal defaults and insurer
financial disincentives to receive brand name drugs instead of generic equivalents in the baseline
period. Such a population of individuals would be characterized as having a high level of
positive behavioral hazard. These employees would then have needed to modify their behavior
during the intervention period to consume generic equivalents.
Another type of generic substitution is more likely. Rather than switching to generic equivalents,
consumers may have switched from a brand-name drug to a generic drug the in same class, as
suggested by Yeung et al. (2018). Brand-name drugs that do not have generic equivalents may

69
nonetheless compete with other drugs that act in a physiologically similar manner, and are
available as lower cost generics. For example, statins are a class of drug that block a liver
enzyme from producing cholesterol. Although they act in a physiologically similar manner,
statins may differ from one another in chemical formulation. It is conceivable that, when faced
with a medical care price increase, some employees taking brand-name drugs with no generic
equivalent could have chosen to switch to a generic drug in the same class, thus saving on costs.
Such a response would avoid needing to overcome “dispense as written” defaults and would be a
rational response to the price change.
A second possibility is that employees purchased drugs in larger quantities per prescription
during the intervention period relative to the baseline period. In other words, they chose drugs
in a >30-day supply instead of a ≤ 30-day supply. As shown in table 2.1, drugs purchased in
higher quantities per prescription were discounted at a level that increased with the number of
days supplied. Specifically, a generic medication was priced at $10 for ≤30 days and $15 for 31
to 90 days. Thus, a 30-day supply of medication cost the consumer $10/30 days = $0.33 per day
and a 90-day supply cost the consumer $15/90 days = $0.17 per day. If enough consumers
switched to larger quantities per prescription, and higher quantities of drugs per prescription
were also less costly to the insurer, this could explain the result of lower expenditure and similar
quantity.
Finally, our results could be attributable to factors not controlled for in the study. A notable
limitation of this study is that we did not have a control group, and thus could not account for
time-varying factors that impacted changes in spending and utilization of drugs and office visits

70
For example, coinciding with the timing of our study, if there was a change in prescribing
practices that resulted in a propensity to prescribe lower cost drugs over higher cost drugs, this
could have contributed to the lower expenditure result. Similarly, if competition among generic
drug manufacturers resulted in a lower overall cost of generic drugs, this could also have
contributed to the lower expenditure result. While we are not aware of any large, region-wide
shifts in prescribing patterns or pricing during our study period, we cannot rule out these
possibilities. We attempted to account for other region-level disturbances and trends by
controlling for market entry of new drugs and defining our dependent variables as year-over-year
differences rather than levels, but we cannot account for all such disturbances.
Another limitation is that we examined a single employer in the Northeast region of the US. As
such, we cannot rule out firm-level adverse selection effects, which may have occurred if the
firm selected a health plan specific to the underlying characteristics of its employees. To address
these generalizability issues, we attempted to describe our sample in as much detail as possible
without revealing the name of the employer, which was prohibited under our data agreement.
Medical care and drugs that treat risk factors for heart disease do not appear to function as
substitutes. For consumers with primary hypertension and hyperlipidemia, an increase in the
price of medical care is not associated with a change in drug utilization, but we do find a
decrease in the rate of change in spending on drugs. This may be viewed as value-enhancing.
We also find that, for people with type-II diabetes, an increase in the price of medical care is
associated with a lower rate of change in spending and utilization of drugs. This would only be
value-enhancing if the lower rate of drug utilization was primarily due to a reduction in the use

71
of drugs whose cost exceeds health value. However, since we focus on high-value drugs, this
effect is value-reducing. Finally, office visits appear to be highly price inelastic for all
consumers with heart disease risk factors. Thus, increases to cost-sharing primarily shift the cost
burden to consumers, rather than lowering expenditure or increasing health value.
When weighing the costs and benefits of changes to insurance plans, insurers should consider
that price changes may have differential effects on consumers with and without heart disease risk
factors. Insurers who seek to control spending through a price increase for medical care might
consider exempting office visits for consumers with heart disease risk factors, since we show that
these consumers might not lower office visit utilization and will thus be faced with higher costs
of necessary care. Price changes may also have differential effects within heart disease risk
factor groups. Insurers who seek to control spending without raising health risk might couple an
increase in the price of medical care with a reduction in copayment for drugs that treat diabetes,
but not those that treat high blood pressure or high cholesterol.

72
CHAPTER 3
3. AN EXPLORATION OF CONSUMER PHARMACEUTICAL COST-SAVING
METHODS
3.1. Introduction
In chapter two, we sought to determine whether consumers with primary hypertension (HTN),
hyperlipidemia (LIP), or type-2 diabetes mellitus (DM) modified their consumption of drugs to
treat these conditions when their medical care became more expensive, but the price of drugs
remained unchanged. Using a sample of employees from a large firm in the northeast US, we
found that employees with HTN significantly decreased their rate of drug spending by 8
percentage points, but did not change their rate of drug utilization. In other words, following the
increase in the price of medical services, these employees continued to fill drug prescriptions at
the same rate as before the price increase, but their rate of change in spending was lower.
Similarly, consumers with LIP significantly decreased their rate of drug spending by 26
percentage points, but did not change their rate of drug utilization. These results were net of
generic market entry. In this chapter, we explore three mechanisms by which consumers in the
HTN and LIP cohorts could have maintained the same rate of utilization growth, at a lower rate
of spending growth. The first two mechanism involve action on the part of the consumer, while
the third relies on changes in the drug market.
3.2. Background
3.2.1. Larger Per-Prescription Quantity
Consumers could have lowered their rate of spending on drugs by purchasing drugs in higher
quantities per prescription. This mechanism relies on two channels. The first is that consumers
have sufficient incentive to buy drugs in larger quantities per prescription. An example of such

73
an incentive might be a lower copayment for purchasing a 90-day prescription over a 30-day
prescription. There is evidence that consumers respond to copayment incentives by changing
their purchasing habits (Karter et al. 2015). The second channel involves the time savings
associated with purchasing larger quantities per prescription. Assuming that consumers have
incentives to purchase larger quantities, the reduction in spending associated with larger
prescription sizes operates through lower cost. For example, 90-day prescriptions are less costly
than 30-day prescriptions for consumers who take statins (for hyperlipidemia) or drugs to lower
blood pressure, even after accounting for greater waste with 90-day sizes (Taitel et al. 2012). 22
A net decrease in spending, however, may not be achieved if the two channels work against one
another. If lower copayments for larger prescription sizes induce consumers to buy more drugs
and this offsets the cost savings from buying in larger sizes, then net spending may actually
increase. This result may, in part, rely on the strength of incentives (Clark et al. 2009).
Nonetheless, our results in chapter 2 indicate that the rate of change in drug day supply did not
increase over the study period.23 Thus, if we find an increase in the rate of change in prescription
fill sizes during the intervention period, then we may be able to infer that this contributed to our
finding of a lower rate of change in drug spending.
3.2.2. Generic Substitution
Consumers may also lower their rate of drug spending by substituting brand-name drugs with
generic drugs, since treating or preventing chronic diseases like heart disease are less costly with
generic drugs compared to brand-name drugs (Shrank et al. 2011). As suggested in chapter two,
22 Cost in this context refers to the total price of the drug, which is the sum of the consumer’s copayment and the
benefit paid by the insurance plan.
23 Day supply is the quantity of medicine, usually pills, in a single prescription.

74
there are two ways by which consumers might choose to consume generic drugs over brand-
name drugs. The first is through switching from a brand-name drug to a generic equivalent.24
However, there were both regulatory and plan design features that provided strong disincentives
for consuming brand-name drugs with generic equivalents, so this was an unlikely mechanism
for the decreasing rate of drug spending in the intervention period. The second means by which
consumers could achieve higher utilization of generic drugs is by substituting away from brand-
name drugs with no generic equivalents to generic drugs within the same class. This mechanism
was suggested by Yeung et al. (2018), who found that among statins, brand-name drugs were
more price elastic than generics.
3.2.3. Lower Prices
Finally, we recognize that our findings in chapter two may be attributable to a lower price level
for generic prescription drugs (net of inflation adjustments), coinciding with the intervention
period. As we are not aware of substantial structural changes in the drug market or
macroeconomy coinciding with the intervention period, a likely mechanism for falling prices
may be an increase in competition among generic drug manufacturers. Generic prices fall when
the number of competitors in a market exceeds a monopoly or near monopoly, with one study
estimating that prices are 31.7% lower in quadropolies and 11.8% lower in duopolies (Dave et al.
2017).25
24 “Equivalent” means the same chemical formulation, route of administration, and dosage.
25 Prices in this case refers to the allowed amount, the total amount paid by the insurer and consumer.

75
3.3. Methods
3.3.1 Data
We utilize the same data as in chapter 2, focusing on the HTN and LIP cohorts. For an in-depth
description of the data, how the cohorts were constructed, and how we define the baseline and
intervention periods, refer to section 2.3. We make two key changes to the data in this chapter.
First, rather than aggregating pharmacy data to per-employee, per-period consumption, we use
disaggregated pharmacy claims data. At this level, we observe individual pharmacy claims – the
six-month time period, drug day supply, total cost, copayment, tier (generic or brand name),
brand name, and generic equivalent name. For those who did not fill a pharmacy claim in a
particular period, we impute a zero copayment and a zero day supply for that employee in that
period. We also drop claims for generic drugs that were controlled for in chapter 2, in addition to
claims for their brand-name equivalents. We drop the brand-name equivalents because we
assume that, when a generic drug enters the market, it replaces its equivalent brand-name drug.
The strength for this assumption comes from the so-called “dispense as written” provisions in
state regulations and the insurance plan’s design.
Under “dispense as written” state regulations, any outpatient prescription issued by an in-state
practitioner is required to be dispensed in generic form, unless the prescriber indicates that the
brand-name version of the drug is to be filled or if the person obtaining the prescription pays for
the full cost of the prescription out-of-pocket. The “dispense as written” insurance plan design is
a provision that, if an employee requests a brand-name drug for which a generic equivalent is
available (without indication from the prescriber that the brand-name drug should be dispensed),
the employee is responsible for the entire difference in cost between the brand-name and the

76
generic version of the drug, plus the applicable brand-name copayment.26 Together, “dispense as
written” state regulations and insurance design provide a legal default and financial disincentive
for consumption of brand-name drugs when a generic equivalent is available.
3.3.2 Pharmacy Plan
Table 3.1 describes the copayment structure of the employee in-network pharmacy plan, which
remained unchanged throughout the study period.27 Under this plan, an employee filling a
prescription was responsible for paying a fixed copayment, regardless of the cost of the drug.
There were three key exceptions whereby an employee could pay a different amount than the
copayment. First, as previously described, if the employee requested a brand-name drug with a
generic equivalent, but without a “dispense as written” exemption, the employee would be
responsible for the cost difference between the brand-name drug and the generic, plus the brand-
name copayment. Second, consumers who reached their out-of-pocket maximum would not owe
a copayment. Finally, where the full cost of the drug was below the copayment, the consumer
paid the cost instead of the copayment.
26 We cannot provide specific references regarding the drug plan or state regulations due to the confidentiality
agreement with our data provider.
27 We only consider the in-network pharmacy structure due to the wide-variety of drugs that treat primary
hypertension and hyperlipidemia, and the fact that the insurer had in-network pharmacies throughout the state.
Thus, there is little reason for employees to use out-of-network pharmacies. Nonetheless, the out-of-network
pharmacy benefit provided the same cost-structure for a 30-day supply at all tiers. It did not provide a 90-day drug
benefit.
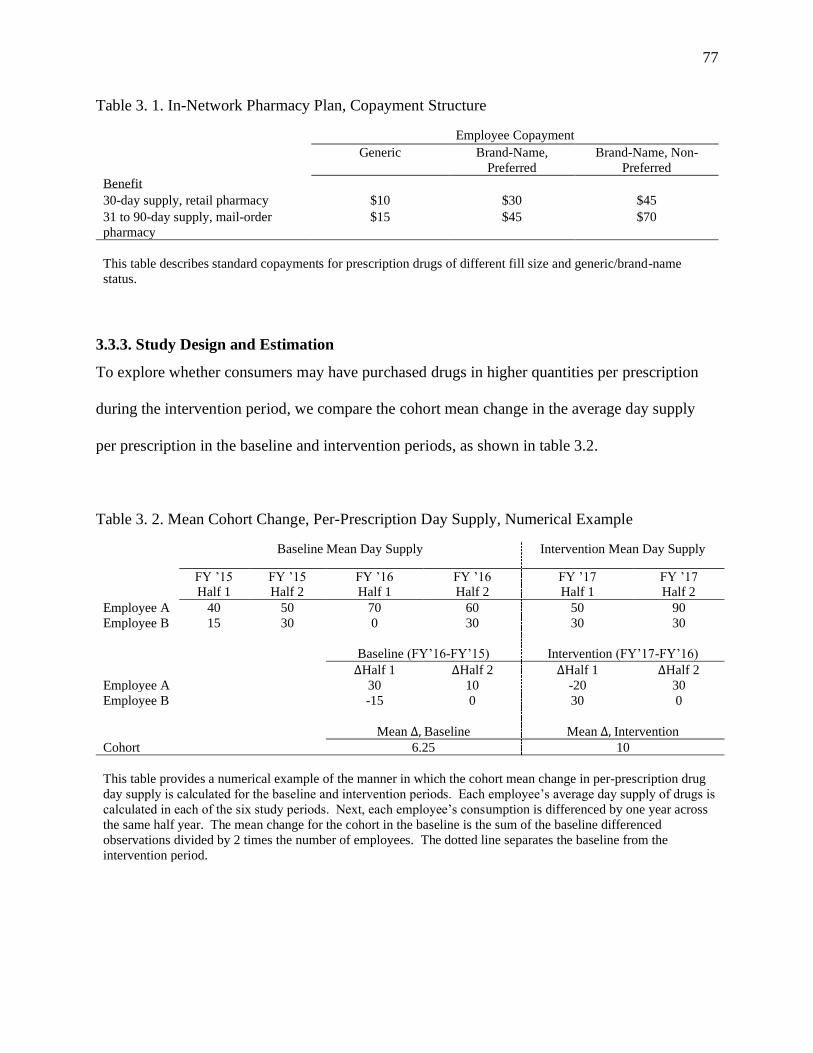
77
Table 3. 1. In-Network Pharmacy Plan, Copayment Structure
Employee Copayment
Generic Brand-Name,
Preferred
Brand-Name, Non-
Preferred
Benefit
30-day supply, retail pharmacy $10 $30 $45
31 to 90-day supply, mail-order
pharmacy
$15 $45 $70
This table describes standard copayments for prescription drugs of different fill size and generic/brand-name
status.
3.3.3. Study Design and Estimation
To explore whether consumers may have purchased drugs in higher quantities per prescription
during the intervention period, we compare the cohort mean change in the average day supply
per prescription in the baseline and intervention periods, as shown in table 3.2.
Table 3. 2. Mean Cohort Change, Per-Prescription Day Supply, Numerical Example
Baseline Mean Day Supply Intervention Mean Day Supply
FY ’15 Half 1
FY ’15 Half 2
FY ’16 Half 1
FY ’16 Half 2
FY ’17 Half 1
FY ’17 Half 2
Employee A 40 50 70 60 50 90
Employee B 15 30 0 30 30 30
Baseline (FY’16-FY’15) Intervention (FY’17-FY’16)
ΔHalf 1 ΔHalf 2 ΔHalf 1 ΔHalf 2
Employee A 30 10 -20 30
Employee B -15 0 30 0
Mean Δ, Baseline Mean Δ, Intervention
Cohort 6.25 10
This table provides a numerical example of the manner in which the cohort mean change in per-prescription drug
day supply is calculated for the baseline and intervention periods. Each employee’s average day supply of drugs is
calculated in each of the six study periods. Next, each employee’s consumption is differenced by one year across
the same half year. The mean change for the cohort in the baseline is the sum of the baseline differenced
observations divided by 2 times the number of employees. The dotted line separates the baseline from the
intervention period.

78
We compare means using a t-test with unequal variances. If employees are filling prescriptions
in a larger day supply per prescription, we would expect the mean change to be significantly
larger in the intervention period.
To explore whether consumers switched from brand-name drugs to generic drugs, we begin by
comparing the cohort average change in the copayment per prescription in the baseline and
intervention periods. We use the same method as we did to determine the cohort mean change in
the day supply per prescription except our variable of interest is the copayment instead of day
supply. If employees are switching from brand name drugs to generic drugs, we expect the mean
change in the copayment to be significantly smaller in the intervention period. There may be
multiple reasons for a decrease in the average change in the per-prescription copayment (smaller
day-supply per prescription, for example). Thus, if we find that the mean change in the
copayment is significantly smaller in the intervention period, we explore specific patterns of
consumption for brand-name drugs and their generic equivalents for all brand-name drugs
exceeding a 0.5% share of total drug expenditures in the study period. Our choice of 0.5% limits
the analysis to brand-name drugs consumed in significant enough quantities to have a
meaningful influence over spending. For drugs without generic equivalents, we explore patterns
of consumption for brand-name drugs and generics in the same drug class using the same 0.5%
cutoff.
To explore whether generic drugs were less costly during the intervention period, we compare
the average per-day cost in the baseline and intervention periods using a t-test with unequal
variances, for all non-zero observations. To determine average per-day cost in a period we take
the ratio of each prescription’s cost to its day supply, and then estimate the mean of this ratio for

79
all prescriptions.28 We also calculate the average per-day cost in each half-year time period and
plot these results. We do this to determine whether the difference in average cost per day
between the baseline and intervention periods was the result of a sharp, level change in cost
corresponding with the intervention period, or if it was the result of a large difference in cost in
any single half-year period. The former could help explain our results from chapter two. 29
3.4. Results
3.4.1. Per-Prescription Day Supply
Figure 3.1 displays the mean per-employee, per-prescription change in the quantity of drugs
supplied in the baseline and intervention periods for the HTN and LIP cohorts, respectively. On
average, during the two fiscal years comprising the baseline period, employees in the HTN group
increased their average fill by 1.65 days per prescription, 95% CI [0.81, 2.51]. During the
intervention period, these same employees increased their average fill by 0.59 days per
prescription, 95% CI [-0.21, 1.38]. This amounted to a weakly significant decline in the per-
prescription fill rate of 1.07 days (p<0.10). In contrast, during the baseline period, the LIP group
increased their average fill by 1.22 days per prescription, 95% CI [0.12, 2.33] and by 2.45 days
per prescription 95% CI [1.39, 3.52] during the intervention period. The difference in means of
1.23 (p = 0.11) was just above the significance cutoff at conventional levels for a bidirectional
null.
28 Alternatively, we could have chosen to sum drug costs in a period and divide by the total drug day supply. We
rejected this method because we wanted to weigh each prescription equally when considering average costs.
29 Available upon request, we separately evaluated generic price changes for 90-day fill sizes, which represented
77% of all generic HTN prescriptions and 83% of all generic LIP prescriptions.

80
Figure 3. 1. Mean Change, Per-Prescription Day Supply, HTN and LIP Cohorts
HTN (N = 2,351) LIP (N = 1,981)
This figure displays the mean per-employee change in the quantity of drugs supplied per prescription in the
baseline and intervention periods for the HTN and LIP cohorts. N is the cohort size. The bars indicate 95%
confidence intervals. The difference in means for the HTN group was -1.07 (p<0.10). The difference in means
for the LIP group was 1.23 (p = 0.11).
3.4.2. Per-Prescription Copayment
Figure 3.2 displays the mean per-employee, per-prescription change in the drug copayment in the
baseline and intervention periods for the HTN and LIP cohorts, respectively. The mean per-
employee change in the copayment for the HTN cohort during the baseline period was an
increase of $0.83 per prescription, 95% CI [0.30, 1.36]. During the intervention period, the mean
change was a decrease of $1.30 per prescription, 95% CI [-3.13, 0.54]. This amounted to a
moderately significant $2.13 (p < 0.05) decrease in the copayment rate of change during the
intervention period. The mean per-employee change in the copayment for the LIP cohort
during the baseline period was an increase of $0.28 per prescription, 95% CI [0.02, 0.53].
During the intervention period, the mean change was an increase of $0.41 per prescription, 95%
CI [0.20, 0.62]. The difference in means of 0.13 was not significant at conventional levels.

81
Figure 3. 2. Per-Prescription Drug Copayment, HTN and LIP Cohorts
HTN (N = 2,351) LIP (N = 1,981)
This table displays the mean drug copayment per-prescription in the baseline and intervention periods for the
HTN and LIP cohorts. The bars indicate 95% confidence intervals. N is the cohort size. The difference between
means was -$2.13 (p<0.05) for the HTN group and $0.13 (p>0.10) for the LIP group.
In the remainder of this section, we explore whether the change in the copayment among those in
the HTN cohort may have been the result of employees switching from brand-name drugs to
their generic equivalents, or employees switching from a brand name drug with no equivalent to
a generic in the same drug class. As we noted in the methods section, when preparing our
sample, we removed any drugs plus their generic or brand equivalents that were controlled for in
the Chapter 2 analysis. In the remaining sample, the number of prescriptions for brand-name
drugs in the HTN cohort is very small relative to the number of generic prescriptions. In total,
there were 41,838 prescriptions filled, of which 255 (0.06%) were for brand-name drugs. Of
these, five brand-name drugs exceeded our 0.5% expenditure cutoff.
Table 3.3 presents the distribution of these five drugs in each fiscal year of the sample. Three
brand name drugs, Inderal LA, Diovan, and Micardis, had generic equivalents available
throughout the study period. A prescription for Inderal LA was filled just seven times in our
sample yet, at 2.54%, accounted for the largest share of expenditures on brand name drugs with

82
generic equivalents. Inderal LA was an expensive drug, costing an average of $4,129.45 per
prescription. All seven prescriptions were filled by a single employee who paid between
$2,432.74 and $4,221.47 in copayments.30 In comparison, Inderal LA’s generic equivalent
(extended-release propranolol hydrochloride) was filled 219 times at an average cost of $142.42,
for which employees faced an average copayment of $13.79. Inderal LA was filled six times
during the baseline period and once during the intervention period. Because of its outsized effect
on cost and the asymmetry in prescription fills, we re-estimate the mean change in copayment
with Inderal LA removed from the sample as a robustness check. Diovan and Micardis
comprised 0.62% and 0.52% of sample expenditures, respectively. Diovan, which was filled 15
times in the first fiscal year with no fills in the second or third fiscal years, had a mean cost of
$476.89, for which employees paid between $10.00 and $70.00 in copayments.31 Diovan’s
generic equivalent (valsartan) was obtained 427 times at a mean cost of $211.76. Employees
filling a prescription for valsartan faced an average copayment of $14.33. Micardis was filled
11 times and similarly distributed across each fiscal year. The average cost for Micardis was
$535.36, for which employees had an average copayment of $70. The generic equivalent of
Micardis (telmisartan) was obtained 123 times at an average cost of $282.23, for which
employees faced an average copayment of $14.27.
30 This employee did not obtain a “dispense as written” exemption from the prescriber. As a result, because Inderal
LA’s generic equivalent was available, the employee was responsible for the cost difference between Inderal LA and
its generic equivalent.
31 Here, the $70 maximum copayment, which is the standard copayment for a >30 day supply for a brand-name
drug, suggests that all employees who sought a prescription for Diovan did so with a “dispense as written”
exemption. The $10 minimum copayment, which is the amount for a 30-day supply of a generic drug, may be
indicative of a particular pharmacy being out of generic Diovan. Thus, the consumer would have received brand-
name Diovan at the generic copayment.

83
Table 3. 3. Number of Prescriptions Filled, Brand-Name Drugs Exceeding 0.50% Spending,
HTN Cohort
Number of Prescriptions
Drug Name Generic Equivalent? FY ‘15 FY ‘16 FY ‘17
Inderal LA Yes 3 3 1
Diovan Yes 15 0 0
Micardis Yes 4 3 4
Bystolic No 55 40 41
Coreg CR No 8 7 4
This table describes the number of prescriptions filled for brand-name drugs exceeding 0.50% of total drug
expenditures. Fiscal years 15 and 16 make up the baseline period. Fiscal year 17 is the intervention period. The
total number of prescriptions filled for both generic and brand name drugs was 41,838.
Two drugs without generic equivalents, Bystolic and Coreg CR, exceeded 0.50% of drug
expenditures. Bystolic prescriptions accounted for 4.00% of expenditures and were filled 136
times at an average cost of $334.36. Employees faced copayments ranging from $30 to $45.
Bystolic is in a class of drugs called cardiac-selective beta blockers, which interact with a
specific type of cell receptor in the heart to regulate blood pressure. There are generic drugs that,
while not formulary equivalents of Bystolic, act in the same manner to lower blood pressure and
were available to the HTN cohort throughout the study period. Prescriptions for these drugs
were widely utilized, filled 7,860 times at an average cost of $28.41. Employees faced an
average copayment of $8.71. Coreg CR prescriptions accounted for 0.97% of expenditures and
were filled 19 times at an average cost of $583.08. Employees faced copayments ranging from
$30 to $70. Coreg CR is in a class of drugs called alpha-beta blockers, which act on the heart
and circulatory system to lower blood pressure. Although there were no formulary equivalents
to Coreg CR available during the study period, there were other generic drugs that were
considered to be alpha-beta blockers. Prescriptions for these drugs were filled 673 times at an
average cost of $34.05. Employees faced an average copayment of $12.25.

84
3.4.3 Generic Drug Cost
Figure 3.3 displays the results of our generic drug cost analysis for the HTN cohort. Starting with
the right frame, the average cost per day of a generic HTN prescription during the baseline
period was $0.33, 95% CI [$0.33, $0.34]. During the intervention period, the average cost per
day was $0.30, 95% CI [$0.29, $0.31]. This amounted to a highly significant decrease in the
average cost per day of $0.03 (p<0.01). In the left frame, the average cost is disaggregated into
six-month time intervals. In this depiction, average cost appears to drop sharply in the second
half of 2016 and the first half of 2017. Both time intervals comprise the intervention period.
Figure 3. 3. Mean Cost of Generic Drugs, All Fill Sizes, HTN Cohort
This figure displays the mean cost per day ($2017) for generic prescription drugs, all fill sizes, for the HTN cohort. The solid vertical bars are 95% confidence intervals. The dotted vertical line separates the four baseline
periods from the two intervention periods. Cohort size was 2,351. The difference in means between the baseline
and intervention periods in the right panel was -$0.03 (p<0.01).

85
Figure 3.4 displays the results of our generic drug cost analysis for the LIP cohort. Again,
starting with the right frame, the average cost per day of a generic LIP prescription was $0.68,
95% CI [$0.66, $0.70] during the baseline period. During the intervention period, the average
cost per day was $0.52, 95% CI [$0.49, $0.55]. This amounted to a highly significant decrease
in the average cost per day of $0.16 (p<0.01). In the left frame we see that, although there was a
reduction in prices during the two six-month periods comprising the intervention period, there
were steeper decreases in cost per day during the first two six-month periods of the baseline.
Figure 3. 4. Mean Cost of Generic Drugs, All Fill Sizes, LIP Cohort
This figure displays the mean cost per day ($2017) for generic prescription drugs, all fill sizes, for the LIP cohort.
The solid vertical bars are 95% confidence intervals. The dotted vertical line separates the four baseline periods
from the two intervention periods. Cohort size was 1,981. The difference in means between the baseline and
intervention periods in the right panel was -$0.16 (p<0.01).

86
3.4.4. Robustness Check
As a robustness check, we explore whether the brand-name drug Inderal LA disproportionately
influenced our results in the copayment analysis by removing these observations from the sample
and re-estimating the difference in the (change in) mean copayments between the baseline and
intervention periods. These results are presented in Figure 3.5. The left panel displays the
original results with the seven Inderal LA prescriptions in the sample. As we reported in section
3.4.2 of the results, employees increased their copayment by an average of $0.83 per
prescription, 95% CI [0.30, 1.36] during the baseline period and decreased their copayment by an
average of $1.29 per prescription, 95% CI [-3.13, 0.54] during the intervention period, resulting
in a moderately significant $2.12 (p < 0.05) decrease in the copayment rate of change. The right
panel displays the results with the Inderal LA prescriptions removed. Here, the mean per-
employee change in copayment during the baseline period was an increase of $0.46, 95% CI
[0.35, 0.57]. During the intervention period, the mean per-employee change in the copayment
was a decrease of $0.11, 95% CI [-0.22, -0.02]. The difference between these means was a
decrease of $0.57 (p < 0.01).

87
Figure 3. 5. Per-Prescription Drug Copayment, HTN Cohort, Robustness Check
With Inderal LA Without Inderal LA
This table displays the mean drug copayment per-prescription in each half-year time period for the HTN and LIP
cohorts. The bars indicate 95% confidence intervals. Cohort size was 2,351. The difference between means in
the left panel is -$2.12 (p<0.05). The difference between means in the right panel is -$0.57 (p<0.01)
3.5. Discussion and Conclusion
In chapter two, we found that an increase in the price of medical care was associated with a
reduction in the rate of spending on drugs but no change to the rate of drug utilization for
employees in the HTN and LIP cohorts. In this chapter, we looked more closely at two
mechanisms by which employees could have accomplished such a dual response: buying in
larger quantities per prescription and switching from brand name to generic drugs. We also
explored whether changes to the cost of generic drugs could have driven results.
For the HTN group, we found some evidence of changing behavior, but nothing that decidedly
explains our chapter two results. Specifically, we found that the rate of change in the number of
days per prescription fell from 1.65 during the baseline period to 0.65 in the intervention period.
This suggests that employees increased their average fill size in both periods, but did so at a
lower rate during the intervention period. As a result, larger fill size is an unlikely mechanism
for our chapter two results. On the other hand, we found that the rate of change in the

88
copayment not only fell during the intervention period relative to the baseline, but was negative.
This suggests that employees paid a lower copayment per prescription in the intervention period.
After removing seven prescriptions for Inderal LA (a very costly, high copayment brand-name
drug that was mostly consumed during the baseline period) our results continued to show a
reduction in the copayment rate of change: $0.46 per prescription in the baseline period
compared to -$0.11 in the intervention period. We were not able to detect whether employees
achieved this outcome through a large-scale shift from brand-name drugs to generic drugs
because, out of more than 40,000 filled prescriptions, only 0.06% were for brand-name drugs.
Nonetheless, we examined the consumption time path of selected brand name drugs with generic
equivalents, as well as brand-name drugs without generic equivalents. We found that a small
number of brand-name prescriptions could make a meaningful change in the group mean due to
outsized cost. Specifically, out of 41,838 prescriptions, a single employee’s purchase of seven
prescriptions for Inderal LA was enough to raise the mean change in copayment during the
baseline period from $0.46 to $1.26 and lower the mean change in copayment during the
intervention period from -$0.11 to -$1.29. It is also interesting to note that, despite state
regulations and insurer “dispense as written” provisions, the availability of a generic formulary
equivalent and the sizeable difference in price (less than $15 for the generic versus over $2,000
for the brand name), the employee nonetheless chose to purchase the brand-name drug.32
Finally, we found evidence that a $0.03 decrease in the per-day cost of generic drugs, which
coincided with the intervention period, could have influenced our results. In this case, our
chapter two findings of a lower rate of spending on drugs would be explained, at least in part, by
32 The data do not allow us to confirm whether this employee actually paid the high price out of his or her own
personal funds. Other mechanism for payment may have been applied, such as copayment assistance from an
outside party.

89
changes in the drug market. We are not able to conclude whether the reduction in cost was the
result of increased competition among generic manufacturers, changes to prescriber practices, or
another mechanism.
Turning to the LIP cohort, we find less explanatory evidence regarding our chapter two results
compared to the HTN cohort. Specifically, we found that this group increased their rate of
change in the number of days per prescription from 1.14 in the baseline period to 2.39 in the
intervention period, a difference of 1.25 days per prescription. With a p-value of 0.11, this result
was just outside conventional significance levels, but nonetheless suggests that these employees
may have increased fill size at a higher rate, which could help explain our results from chapter
two. On the other hand, we found no difference in the rate of change in the copayment between
the baseline and intervention periods. Copayments for this group increased slightly in both
periods. Moreover, we found a large, statistically significant reduction in the per-day average
cost of generic LIP drugs between the baseline and intervention periods. However, examining
the average cost of generic drugs in each period, we find that the difference may have been due
to high costs in the first and second six-month periods of the baseline, a sharp fall in costs during
the last two periods of the baseline, and a smaller reduction in costs during the intervention
period. In other words, we do not see strong evidence of a level trend in cost during the baseline
period, followed by a sharp drop in cost during the intervention period (as we see with the HTN
group). This means that our chapter two results, where the rate of change in LIP drug spending
was sharply lower in the intervention period compared to the baseline period, is unlikely due to
changes in drug cost.

90
This study was limited in the sense that not all avenues for cost savings were explored. For
example, we did not examine changes in cost exclusively for brand-name drugs because the
majority of prescriptions were for generics. Additionally, when constructing our sample, we
dropped generic drugs and their brand-name equivalents that were controlled for in our chapter
two analysis. We did this because our chapter two findings were net of the effects of new
generics entering the marketplace mid-study. Moreover, we assumed that new generics largely
displace their brand-name equivalents. The strength of our results, therefore, relies on the
strength of this assumption. This may be a reason why we failed to find considerable changes in
the LIP cohort, who experienced a 26 percentage-point decrease in their rate of spending during
the intervention period. Partway through the study period, generic Crestor (a statin) was
released to the market, displacing a popular brand-name high cholesterol drug. Although our
chapter two results control for this major market entry, it is possible that our control was not
adequate. Thus, it is possible that our results still reflect the effect of generic Crestor entering the
market, which likely would likely have reduced rates of change in spending. Thus, by dropping
Crestor and its generic in this analysis, we have failed to find significant changes in consumer
behavior.
In conclusion, we did not find strong evidence indicating that changes to employee behavior
around prescription drug consumption took place in a manner that sufficiently describes how
employees lowered their rate of spending on drugs despite making no change to their rate of drug
utilization. Lower generic drug prices may have explained a portion of our chapter 2 results for
the HTN group. Future work should include a more formal analysis of the ways in which
consumers alter their behavior within drug benefit plans in response to changes in the price of
medical care, using more rigorous experimental design and estimation techniques.

91
CHAPTER 4
4. CONCLUSIONS
The purpose of this work was to examine a long-standing attribute of the American health care
system: high expenditure for average outcomes. There are numerous consumer demand and
market-based factors that contribute to this problem, but health insurance design continues to be
a fruitful area of health policy research. This is perhaps owing to the ways in which insurance
has evolved over recent decades. Statutory changes to the health insurance market have required
plans to cover more services. They have also enabled access for more people, seemingly without
constraints placed on limiting the utilization of health care that is characterized as high-cost,
uncertain-benefit.
It is important, from a health value standpoint, to understand how consumers modify their use of
health care in response to change in insurance design. This is because consumer response is
difficult to predict theoretically. Consumers who receive health benefit in excess of societal cost,
such as those with certain chronic diseases, may nonetheless view themselves as marginal
consumers. Similarly, consumers who consume health care for which societal (and even private)
cost exceeds health benefit may nonetheless perceive health benefits to be outsized and of good
value. Consumers may also misinterpret or fail to consider complex insurance plan incentives,
especially when making consumption decisions under time pressure or adverse health conditions.
This work adds to the body of knowledge about health insurance design by examining whether
consumers with risk factors for heart disease modified their consumption of office visits and
drugs in response to a small increase in the price of other medical care. This price change made

92
office visits more expensive, but had no direct impact on drugs. Previous literature has generally
established an inelastic response to the price of office visits. It has also shown that drugs and
other health care are best described as substitutes. Specifically, when drugs become more
expensive, consumers are less adherent to them. However, because such drugs are intended to
prevent adverse health events, other forms of medical care are used more often when adherence
falls (e.g. hospitals, physician office visits). In this work, we sought to determine whether the
substitution effect holds in the other direction – when the price of other health care increases, but
the price of drugs remains unchanged.
Our main results suggest that, for consumers with risk factors for heart disease, the substitution
relationship does not hold when it is the price of medical care that changes. In association with a
small increase in the copayment and deductible affecting an array of medical services, consumers
with high blood pressure and high cholesterol did not change their rate of utilization of drugs,
despite lowering their rate of spending. These consumers increased their drug utilization in the
two years preceding the price increase, and continued to increase drug utilization at the same rate
in the intervention period. Consumers with type-II diabetes also utilized more drugs in the two
years before the price change, but did so at a lower rate after the price change. This suggests
that, for people with type-II diabetes, a complementary relationship might exist between drugs
and other health care when the price of other health care changes. We were also able to confirm
the finding from past studies that office visits are highly price inelastic; we found little change in
utilization rates that were attributable to an own-price increase.

93
Unfortunately, our experimental design did not permit causal inferences. This was part of the
motivation for chapter three, which explored ways in which consumers with high blood pressure
and high cholesterol might have kept rates of drug utilization unchanged while lowering rates of
spending. There was unconvincing evidence of large-scale changes in behavior that could
explain chapter two results. This may have been, in part, due to a reduction in prices coinciding
with the intervention period, but also to the very low utilization of brand-name drugs in our
sample. In some respect, the latter is evidence regarding the effectiveness of financial incentives
embedded in the insurance contract. These incentives placed a price penalty on the use of brand-
name drugs, which increased if brand-name drugs were chosen over available generic
equivalents without an explicit exemption from the prescriber (by hundreds or even thousands of
dollars). Nonetheless, we detected a perceptual distortion (a positive behavioral hazard, as
described theoretically in chapter one). A small number of consumers purchased brand-name
drugs where generic equivalents or generic similars were available, and were willing to accept
higher prices to consume them. Because these drugs were so costly, they distorted the average
expenditure of the group, despite the small quantities.
Altogether, this work shows that, to lower health care spending without sacrificing outcomes, a
society that is characterized by private health insurance markets and private providers should
consider that individuals with risk factors for heart disease may respond to price changes
differently than consumers without them. Further, individuals with high blood pressure and high
cholesterol respond differently than individuals with type II diabetes. For consumers with high
blood pressure or high cholesterol, raising the price of medical care could result in a reduction in
the rates of drug expenditure without sacrificing health– an outcome that could be considered

94
value-enhancing. On the other hand, individuals with diabetes might lower rates of both
expenditure and utilization. We view this as value-reducing since we assume that all drugs
intended to treat diabetes are high value. Ultimately, insurers must decide whether implementing
benefit changes for different groups of consumers (which would require increased administration
and discovery costs, as well as increased complexity for consumers) outweighs the cost savings
associated with utilization.
Insurance design has the capacity to improve health care value. By raising cost-sharing amounts
for medical care by small increments, insurers can disincentivize the use of wasteful care by
marginal consumers. However, as we show in this work, broad cost-sharing increases, though
small, may also impact consumers with heart disease risk factors. These consumers are above
the margin, but may nonetheless modify consumption in ways that can be value-enhancing or
value-reducing, depending on the risk factor. Insurers should consider these differential effects
when determining the overall impact of plan design.

95
REFERENCES
American Heart Association. (2019, March 5). Heart Disease and Stroke Statistics - 2019
Update: A report from the American Heart Association. Circulation, e56 - e528. doi:
10.1161/CIR.0000000000000659.
Anderson, G., Reinhardt, U., Hussey, P., & Petrosyan, V. (2003). It's the prices, stupid: Why the
United States is so different from other countries. Health Affairs, 22(3), 89-105.
Aron-Dine, A., Einav, L., Finkelstein, A., & Cullen, M. (2015, October). Moral hazard in health
insurance: Do dynamic incentives matter? The Review of Economics and Statistics, 97(4),
725-741.
Bailey, C., & Kodack, M. (2011, March). Patient adherence to medication requirements for
therapy of type 2 diabetes. International Journal of Clinical Practice, 65(3), 314-322,
doi: 10.1111/j.1742-1241.2010.02544.x.
Batty, M., & Ippolito, B. (2017, Apr). Mystery of the chargemaster: examining the role of
hospital list prices in what patients actually pay. Health Affairs, 36(4), 689-696.
Brot-Goldberg, Z., Chandra, A., Handel, B., & Kolstad, J. (2017). What does a deductible do?
The impact of cost-sharing on health care prices, quantities, and spending dynamics.
Quarterly Journal of Economics, 1261-1318.
Chandra, A., & Skinner, J. (2012, Sept). Technology growth and expenditure growth in health
care. Journal of Economic Literature, 50(3), 645-680.
Chernew, M., Shah, M., Wegh, A., Rosenberg, S., Juster, I., Rosen, A., . . . Fendrick, A. (2008).
Impact of decreasing copayments on medication adherence within a disease management
environment. Health Affairs, 27(1), 103-112.
Choudhry, N., Avorn, J., Glynn, R., Antman, E., Schneeweiss, S., Toscano, M., . . . Shrank, W.
(2011). Full coverage for preventive medications after myocaridal infarction. New
England Journal of Medicine, 365, 2088-2097.
Choudhry, N., Fischer, M., Avorn, J., Lee, J., Schneeweiss, S., Solomon, D., . . . Shrank, W.
(2012). The impact of reducing cardiovascular medication copayments on health
spending and resource utilization. Journal of the American College of Cardiology,
60(18), 1817-1824.
Chowdhury, R., Khan, H., Heydon, E., Shroufi, A., Fahimi, S., Moore, C., . . . Franco, O. (2013).
Adherence to cardiovascular therapy: a meta-analysis of prevalence and clinical
consequences. European Heart Journal, 34, 2940-2948.

96
Clark, B., Siracuse, M., & Garis, R. (2009). A comparison of mail-service and retail community
pharmacy claims in 5 prescription benefit plans. Research in Social and Administrative
Pharmacy, 5, 133-142.
Claxton, G., Rae, M., Long, M., Damico, A., & Whitmore, H. (2018). Health benefits in 2018:
modest growth in premiums, higher worker contributions at firms with more low-wage
workers. Health Affairs, 37(11), 1892-1900.
CMS. (2018). National Health Expenditure Data. Retrieved June 2020, from CMS.gov:
https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-
Reports/NationalHealthExpendData/NationalHealthAccountsHistorical
Cockx, B., & Brasseur, C. (2003). The demand for physician services: evidence from a natural
experiment. Journal of Health Economics, 22(881-913).
Cohen, R., Terlizzi, E., & Martinez, M. (2019, May). Health insurance coverage: early release of
estimates from the National Health Interview Survey, 2018. Available from:
https://www.cdc.gov/nchs/nhis/ releases.htm.
Cole, J., Norman, H., Weatherby, M., & Walker, A. (2006). Drug copayment and adherence in
chronic heart failure: effect on cost and outcomes. Pharmacotherapy, 26(8), 1157-1164.
Dave, C., Kesselheim, A., Fox, E., Qiu, P., & Hartzema, A. (2017). High generic drug prices and
market competition. Annals of Internal Medicine, 167(3), 145-151,
https://doi.org/10.7326/M16-1432.
Doshi, J., Zhu, J., Lee, B., Kimmel, S., & Volpp, K. (2009). Impact of a prescription copayment
increase on lipid-lowering medication adherence in veterans. Circulation, 119, 390-397.
Ford, E., Ajani, U., Croft, J., Critchley, J., Labarthe, D., Kottke, T., . . . Capewell, S. (2007).
Explaining the decrease in U.S. deaths from coronary disease, 1980-2000. New England
Journal of Medicine, 356, 2388-2398.
Frakt, A., & Chernew, M. (2018, February 6). The importance of relative prices in health care
spending. JAMA, 319(5), 441-442.
Frank, M., Fendrick, M., He, Y., Zbrozek, A., Holtz, N., Leung, S., & Chernew, M. (2012). The
effect of a large regional health plan's value-based insurance design program on statin
use. Medical Care, 50(11), 934-939.
Gaynor, M., Li, J., & Vogt, W. (2006, December). Is drug coverage a free lunch? Cross-price
elasticities and the design of prescription drug benefits. NBER Working Paper #12758,
http://www.nber.org/papers/w12758.
Gibson, T., Mark, T., Axelsen, K., Baser, O., Rublee, D., & McGuigan, K. (2006). Impact of
statin copayments on adherence and medical care utilization and expenditures. American
Journal of Managed Care, 12, SP11-SP19.

97
Gibson, T., Wang, S., Kelly, E., Brown, C., Turner, C., Frech-Tamas, F., . . . Mauceri, E. (2011).
A value-based insurance design program at a large company boosted medication
adherence for employees with chronic illnesses. Health Affairs, 30(1), 109-117.
Gourzoulidis, G., Kourlaba, G., Stafylas, P., Giamouzis, G., Parissis, J., & Maniadakis, N.
(2017). Association between copayment, medication adherence and outcomes in the
management of patients with diabetes and heart failure. Health Policy, 121, 363-377,
http://dx.doi.org/10.1016/j.healthpol.2017.02.008.
Herr, A., & Suppliet, M. (2017). Tiered co-payments, pricing, and demand in reference price
markets for pharmaceuticals. Journal of Health Economics, 56, 19-29.
Ho, P., Magid, D., Shetterly, S., Olson, K., Maddox, J., Peterson, P., . . . Rumsfeld, J. (2008).
Medication nonadherence is associated with a broad range of adverse outcomes in
patients with coronary artery disease. American Heart Journal, 155(4), 772-779.
Jakobsson, N., & Svensson, M. (2016). Copayments and physicians visits: a panel data study of
Swedish regions 2003-2012. Health Policy, 120, 1095-1099.
Karter, A., Parker, M., Duru, O., Schillinger, D., Adler, N., Moffet, H., . . . Schmittdiel, J.
(2015). Impact of a pharmacy benefit change on new use of mail order pharmacy among
diabetes patients: the diabetes study of Northern California (DISTANCE). Health
Services Research, 52(2), 537-559.
Kochanek, K., Murphy, S., Xu, J., & Arias, E. (2019). Deaths: Final data for 2017. National
Vital Statistics Reports; vol 68 no 9. Hyattsville, MD: National Center for Health
Statistics.
Leon, B., & Maddox, T. (2015, October 10). Diabetes and cardiovascular disease: Epidemiology,
biological mechanisms, treatment recommendations and future research. World Journal
of Diabetes, 6(13), pp. 1246-1258.
Lewey, J., Gagne, J., Franklin, J., Lauffenburger, J., Brill, G., & Choudhry, N. (2018,
November). Impact of high deductible health plans on cardiovascular medication
adherence and health disparities. Circulation: Cardiovascular Quality and Outcomes, 1-
12.
Li, R., Zhang, P., Barker, L., Chowdhury, F., & Zhang, X. (2010). Cost-effectiveness of
interventions to prevent and control diabetes mellitus: a systematic review. Diabetes
Care, 33, 1872-1894.
Lieu, T., Solomon, J., Sabin, J., Kullgren, J., Hinrichsen, V., & Galbraith, A. (2009). Consumer
awareness and strategies among families with high-deductible health plans. Journal of
General Internal Medicine, 25(3), 249-254.
Ma, Q., Sylwestrzak, G., Oza, M., Garneau, L., & DeVries, A. (2019). Evaluation of value-based
insurance design for primary care. American Journal of Managed Care, 25(5), 221-227.

98
Maciejewski, M., Bryson, C., Perkins, M., Blough, D., Cunningham, F., J.C., F., . . . Liu, C.-F.
(2010a). Increasing copayments and adherence to diabetes, hypertension, and
hyperlipidemic medications. American Journal of Managed Care, 16(1), 220-35.
Maciejewski, M., Farley, J., Parker, J., & Wansink, D. (2010b). Copayment reductions generate
greater medication adherence in targeted patients. Health Affairs, 29(11), 2002-2008.
Manning, W., Newhouse, J., Duan, N., Keeler, E., & Leibowitz, A. (1987). Health insurance and
the demand for medical care: evidence from a randomized experiment. American
Economic Review, 77(3), 251-277.
MCDC. (2014-2017). Dexter - Data Extracter. Retrieved February 2020, from MCDC Data
Applications: http://mcdc.missouri.edu/cgi-
bin/broker?_PROGRAM=utils.uex2dex.sas&path=/pub/data/georef&dset=zcta_master&
view=0
MCDC. (2016, September 10). Geocorr 2015: Geographic Correspondence Engine. Retrieved
February 2020, from MCDC Data Applications:
http://mcdc.missouri.edu/applications/geocorr2014.html
Medicare Payment Advisory Commission. (March 2020). Medicare Payment Policy: Report to
the Congress. Washington, DC: MEDPAC.
Miller, K. (2019, June 24). Gov. Mills signs 4 bills to reduce medication prices, including buying
from Canada. Retrieved September 2019, from Portland Press Herald:
https://www.pressherald.com/2019/06/24/mills-signs-bill-to-import-prescription-drugs-
from-canada/
Naderi, S., Bestwick, J., & Wald, D. (2012, September). Adherence to drugs that prevent
cardiovascular disease: meta-analysis on 376,162 patients. American Journal of
Medicine, 125(9), 882-887.e1, doi:10.1016/j.amjmed.2011.12.013.
Nair, K., Park, J., Wolfe, P., Saseen, J., Allen, R., & Ganguly, R. (2009). Consumer-driven
health plans: impact on utilization and expenditures for chronic disease sufferers. Journal
of Occupational and Environmental Medicine, 2009(51), 594-603.
Nichols, G., & Brown, J. (2002). The impact of cardiovascular disease on medical care costs in
subjects with and without type 2 diabetes. Diabetes Care, 25, 482-486.
OECD. (2015). Health Status: Causes of Mortality: Diabetes Mellitus: Deaths per 100,000
population (standardized rates). Retrieved February 2020, from OECD.Stat:
https://stats.oecd.org/index.aspx?queryid=30115
OECD. (2016a). Health Status: Causes of Mortality: Ischemic Heart Disease: Deaths per
100,000 population (standardized rates). Retrieved February 2020, from OECD.Stat:
https://stats.oecd.org/

99
OECD. (2016b). Health Care Resources: Hospital Beds. Retrieved June 2020, from OECD.Stat:
https://stats.oecd.org/index.aspx?queryid=24879#
OECD. (2017a). Health Status: Life Expectancy: Total Population at Birth. Retrieved February
2020, from OECD.Stat: https://stats.oecd.org/index.aspx?queryid=24879
OECD. (2017b). Health at a glance 2017: OECD indicators. Paris: OECD Publishing.
OECD. (2018). Health Expenditure and Financing: Current expenditure on health (all
functions): Share of Gross Domestic Product. Retrieved June 2020, from OECD.stat:
https://stats.oecd.org/index.aspx?queryid=24879#
Picard, R. (2010). GEODIST: Stata Module to compute geographical distances. Retrieved from
Statistical Software Components S457147, Boston College Department of Economics:
https://ideas.repec.org/c/boc/bocode/s457147.html
Rasmussen, J., Chong, A., & Alter, D. (2007). Relationship between adherence to evidence-
based pharmacotherapy and long-term mortality after acute myocardial infarction. JAMA,
297(2), 177-186.
Reed, M., Fung, V., Price, M., Brand, R., Benedetti, N., Derose, S., . . . Hsu, J. (2009). High-
deductible health insurance plans: efforts to sharpen a blunt instrument. Health Affairs,
28(4), 1145-1153.
Roebuck, M., Liberman, J., Gemill-Toyama, M., & Brennan, T. (2011). Medication adherence
leads to lower health care use and costs despite increased drug spending. Health Affairs,
30(1), 91-99.
Schaffer, M., & Stillman, S. (2006). XTOVERID: Stata module to calculate tests of
overidentifying restrictions after xtreg, xtivreg, xtivreg2, xthtaylor. Retrieved June 2020,
from Statistical Software Components S456779, Boston College Department of
Economics: https://ideas.repec.org/c/boc/bocode/s456779.html
Shrank, W., Choudhry, N., Liberman, J., & Brennan, T. (2011). The use of generic drugs in
prevention of chronic disease is far more effective than thought, and may save money.
Health Affairs, 30(7), 1351-1357.
Simon-Tuval, T., Triki, N., Chodick, G., & Greenberg, D. (2016). The association between
adherence to cardiovascular medications and healthcare utilization. European Journal of
Health Economics, 17, 603-610.
Sullivan, S., Yeung, K., Vogeler, C., Ramsey, S., Wong, E., Murphy, C., . . . Watkins, J. (2015).
Design, implementation, and first-year outcomes of a value-based drug formulary.
Journal of Managed Care & Specialty Pharmacy, 21(4), 269-275.
Taitel, M., Fensterheim, L., Kirkham, H., Sekula, R., & Duncan, I. (2012). Medication days'
supply, adherence, wastage, and cost among chronic patients in medicaid. Medicare &
Medicaid Research Review, 2(3), E1-E12.

100
Thorpe, K., Allen, L., & Joski, P. (2015). The role of chronic disease, obesity, and improved
treatment and detection in accounting for the rise in healthcare spending between 1987
and 2011. Applied Health Economics and Health Policy, 13, 381-387.
Tucker, D., & Palmer, A. (2011). The cost-effectiveness of interventions in diabetes: a review of
published economic evaluations in the UK setting, with an eye on the future. Primary
Care Diabetes, 5, 9-17.
U.S. Census Bureau. (1987-2018). Health Insurance Data Tables (Tables HIC-4_ACS, HIA-1,
HI-1). Retrieved October 2019, from Census.gov:
https://www.census.gov/topics/health/health-insurance/data/tables.html
U.S. Census Bureau. (2018). Health Insurance Coverage Status by State and Age for All People:
2018 (Table HI05). Retrieved October 2019, from Census.gov:
https://www.census.gov/data/tables/time-series/demo/health-insurance/acs-hi.html
Wang, V., Liu, C.-F., Bryson, C., Sharp, N., & Maciejewski, M. (2011). Does medication
adherence following a copayment increase differ by disease burden? HSR: Health
Services Research, 46(6), 1963-1985.
Ward, B., Clarke, T., & Schiller, J. (2016). Early release of selected estimates based on data
from January-June 2016. CDC, National Center for Health Statistics, National Health
Interview Survey.
Weber, S., & Péclat, M. (2016). GEOROUTE: Stata module to calculate travel distance and
travel time between two addresses or two geographical points . Retrieved February 2020,
from Statistical Software Components S458264, Boston College Department of
Economics: https://ideas.repec.org/c/boc/bocode/s458264.html
Will, J., Zhang, Z., Ritchey, M., & Loustalot, F. (2016). Medication adherence and incident
preventable hospitalizations for hypertension. American Journal of Preventive Medicine,
50(4), 489-499.
Yeung, K., Basu, A., Hansen, R., & Sullivan, S. (2018). Price elasticities of pharmaceuticals in a
value-based formulary setting. Health Economics, 27, 1788-1804.
Zeng, F., An, J., Scully, R., Barrington, C., Patel, B., & Nichol, M. (2010). The impact of value-
based benefit design on adherence to diabetes medications: a propensity score-weighted
difference in difference evaluation. Value in Health, 13(6), 846-852.

101
APPENDIX
Table A. 1. ICD-9 Diagnosis Codes and Drug Therapeutic Groups for HTN
ICD-9 Codes Drug Therapeutic Groups
401.0 ACE Inhibitors
401.9 Calcium Channel Blockers
Beta Blockers
Angiotensin II Receptor Blockers
Diuretics
Peripheral Alpha-1 Receptor Blockers
Central Alpha-2 Receptor Agonists
Renin Inhibitors
We also include drugs that are combinations of these therapeutic groups or combine a drug from this list with a
drug used to treat other conditions. For example, we include drugs that combine an HMG CoA reductase
inhibitor (a statin) with a calcium channel blocker (for HTN).
Table A. 2. ICD-9 Diagnosis Codes and Drug Therapeutic Groups for LIP
ICD-Codes Drug Therapeutic Groups
272.0 Bile Acid Sequestrants
272.1 Fibric Acid Derivatives
272.2 HMG CoA Reductase Inhibitors (statins)
272.4 Nicotinic Acid Derivatives
272.9 Omega-3 Fatty Acids
Selective Cholesterol Absorption Inhibitors
Anti-PCSK9 Monoclonal Antibodies*
We also include drugs that are combinations of these therapeutic groups or combine a drug from this list with a
drug used to treat other conditions. For example, we include drugs that combine an HMG CoA reductase inhibitor
(a statin) with a calcium channel blocker (for HTN). *In our spending analysis, we omit spending on anti-PCSK9
monoclonal antibodies, since they are reported to be a low-value medication by accepted clinical practice
guidelines.

102
Table A. 3. ICD-9 Diagnosis Codes and Drug Therapeutic Groups for DM
ICD-9 Codes Drug Therapeutic Groups
250.00/250.02 Alpha-Glucosidase Inhibitors
250.10/250.12 Dopamine Receptor Agonists
250.20/250.22 Meglitinide Analogs
250.30/250.32 Sodium Glucose Cotransporter-2 (SGLT2) Inhibitors
250.40/250.42 Sulfonylurea Derivatives
250.50/250.52 Dipeptidyl Peptidase-4 (DPP-4) Inhibitors
250.60/250.62 Incretin Mimetic, GLP-1 Receptor Agonist Analog-Type Antihyperglyc.
250.70/250.72 Amylin Analog-Type Antihyperglycemics
250.80/250.82 Biguanides
250.90/250.92 Thiazolidinediones (PPAR-gamma agonists)
Human Insulins
Insulin Analogs
Hyperglycemics
Insulin Needles and Syringes*
Blood Glucose Testing Supplies*
Urine Ketone, Urine Glucose-Acetone Tests*
We include drugs that are combinations of these therapeutic groups or combine a drug from this list with a drug
used to treat other conditions. For example, we include drugs that combine an SGL-2 inhibitor with a biguanide.
*Excluded from the spending analysis
Table A. 4. Office Visit CPT Codes and Excluded Settings
CPT Codes Excluded Settings
99201 Home
99202 Emergency Room - Hospital
99203 Skilled Nursing Facility
99204 Nursing Facility
99205 Comprehensive Inpatient Rehabilitation Facility
99211 End-Stage Renal Disease Treatment Facility
99212 Non-Residential Substance Abuse Treatment Facility
99213 Inpatient Hospital
99214
99215 Excluded Service Types
Occupational Therapy
Emergency Room
Operating Room Services
Individual/Group/Family Therapy
Day/Night Treatment
The above CPT codes are used to identify office visits. Within this dataset, we identified settings and service types
that may have been inappropriately coded as an office visit.

103
Table A. 5. Baseline (First Time Period) Characteristics, Zero Spending Cohorts
HTN LIP DM
Covariates
Age Category (percent, se)
<19 1.40 (0.80) 0.58 (0.24) 2.33 (1.15)
19-44 25.12 (2.96) 21.51 (1.28) 12.79 (2.55)
45-64 67.44 (3.20) 74.22 (1.36) 75.58 (3.29)
65+ 6.05 (1.63) 3.68 (0.59) 9.30 (2.22)
# Emergency Department Visits 0.16 (0.04) 0.07 (0.01) 0.13 (0.04)
Time to Nearest Hospital (min) 17.34 (0.78) 17.82 (0.33) 16.25 (0.72)
Hospital Density 2.38 (0.07) 2.33 (0.03) 2.45 (0.07)
ZCTA % Above Bachelors 28.58 (0.78) 27.76 (0.34) 28.96 (0.84)
ZCTA Annual Household Income 51,400 (869) 52,556 (435) 53,859 (953)
Coordination of Benefits (percent, se) 0.47 (0.47) 0.48 (0.22) 1.74 (1.00)
Other Sample Characteristics
Sex, Female (percent, se) 40.93 (3.36) 49.81 (1.56) 54.65 (3.81)
# Comorbidities 2.10 (0.13) 2.07 (0.05) 2.68 (0.14)
Policy Tier (percent, se)
Employee Only 40.93 (3.36) 43.41 (1.54) 45.93 (3.81)
Employee + One 21.40 (2.80) 23.93 (1.33) 27.33 (3.41)
Employee + Dependent 8.83 (1.94) 8.04 (0.85) 5.23 (1.70)
Family 28.84 (3.10) 24.61 (1.34) 21.51 (3.14)
Relation (percent, se)
Employee 72.56 (3.05) 78.20 (1.29) 72.67 (3.41)
Spouse 23.26 (2.89) 19.57 (1.24) 22.09 (3.17)
Dependent 4.19 (1.37) 2.23 (0.46) 5.23 (1.70)
Sample Size
215 1,032 172
Hospital density is the number of hospitals within 20 miles of the population-weighted ZCTA. Median
household income is in 2017$. Coordination of benefits is the percentage of the sample with an observed
coordination of benefits amount from the medical claims data

104
Table A. 6. Mean Level of Dependent Variables by Fiscal Year, All Cohorts
FY ‘15 FY ‘16 FY ‘17
HTN (N = 2,351)
Drug Spending 87.73 (3.15) 88.26 (3.26) 81.74 (2.52)
Drug Day Supply 219.71 (2.20) 229.53 (2.19) 237.58 (2.31)
Office Visit Spending 326.46 (5.26) 332.87 (5.56) 325.12 (5.64)
Office Visits 2.80 (0.43) 2.90 (0.46) 2.86 (0.46)
LIP (N = 1,981)
Drug Spending 217.79 (7.15) 217.76 (7.90) 144.45 (5.59)
Drug Day Supply 130.65 (1.42) 136.63 (1.42) 142.14 (1.39)
Office Visit Spending 316.83 (5.86) 324.04 (5.88) 320.88 (6.21)
Office Visits 2.71 (0.05) 2.81 (0.05) 2.83 (0.05)
DM (N = 736)
Drug Spending 1,475.03 (60.37) 2,001.39 (78.87) 2,310.13 (81.67)
Drug Day Supply 228.45 (4.69) 262.29 (4.81) 278.99 (4.84)
Office Visit Spending 429.69 (10.85) 427.02 (10.68) 426.32 (11.24)
Office Visits 3.52 (0.08) 3.61 (0.09) 3.69 (0.10)
This table describes the mean (se) level of half-year consumption for each fiscal year. Spending is in
2017$. Visits and day supply are counts.

105
Table A. 7. Regression Results – Changes in Spending and Utilization for the HTN Cohort
Drugs
Office Visits
Δ Spending
Δ Day Supply
Δ Spending
Δ Visits
Estimator OLS FE OLS OLS
Post -6.79** -1.90 -14.74 -0.14*
(3.30) (2.65) (9.13) (0.07)
Δ Emergency Department Visits -2.19 5.47** 106.19*** 0.86***
(2.66) (2.51) (9.60) (0.08)
Δ Time to Nearest Hospital 1.65** 0.96 1.06 0.00
(0.79) (1.01) (2.03) (0.02)
Δ Hospital Density 23.05 7.62 43.92* 0.44*
(16.51) (12.50) (26.58) (0.23)
Δ ZCTA % Bachelors or Higher 0.46 0.46 -1.66 -0.01
(0.95) (1.27) (3.16) (0.02)
Δ ZCTA Median Household
Income -0.16** -0.09 -0.11 0.00
(0.08) (0.11) (0.26) (0.00)
Aged19 20.29 91.97 -274.39 -1.71
(20.80) (69.19) (247.93) (2.63)
Aged 45 7.80 5.21 35.12 0.24
(5.93) (14.15) (26.14) (0.22)
Aged 65 4.64 19.99** 23.19 0.17
(4.67) (9.33) (19.96) (0.17)
COB + 7.29 -23.69 86.15 -0.03
(10.06) (38.63) (86.94) (0.65)
COB - 8.56 -32.10 12.30 0.20
(11.50) (28.07) (90.84) (0.88)
Generic Azor -586.15*** 105.07** -40.32 0.07
(30.61) (6.99) (168.74) (1.40)
Generic Benicar 188.64 -19.89 -130.12 -1.41
(198.87) (8.63) (137.93) (1.25)
Generic Benicar HCT -96.43 19.17** -268.28 -1.98
(124.64) (8.63) (170.16) (1.60)
Generic Exforge -1,076.82*** -1.26 -266.27*** -2.09***
(1.93) (1.77) (5.52) (0.04)
# Observations
9,404 9,404 9,404 9,404
# Individuals
2,351
2,351
2,351
2,351
All variables describe the year-over-year change in 6-month, same-period consumption or status in $2017. OLS =
Ordinary Least Squares; FE = Fixed Effects Estimation; COB+/- = Gained/Lost Coordination of Benefits. Travel
time is in minutes, density is # of hospitals within a 20-mile radius, median HH income is normalized to 100s of
2017$. Effect of generic drugs is for new prescriptions. Cluster robust standard errors are reported in parentheses.
***p<0.01; **p<0.05; *p<0.10

106
Table A. 8. Spending and Utilization Regression Results for the LIP Cohort
Drugs
Office Visits
Δ Spending
Δ Day Supply
Δ Spending
Δ Visits
Estimator OLS OLS OLS OLS
Variable
Post -56.44*** -1.44 -9.91 -0.07
(8.51) (2.13) (9.43) (0.08)
Δ ED visits 4.59 1.13 97.29*** 0.76***
(5.20) (1.68) (10.44) (0.08)
Δ Time to Nearest Hospital -1.84 -0.42 0.94 0.01
(3.26) (0.52) (2.95) (0.03)
Δ Hospital Density 5.29 3.40 22.97 0.34
(45.20) (6.04) (36.60) (0.32)
Δ ZCTA % Bachelor’s + 2.31 -0.58 -3.46 -0.02
(2.45) (0.52) (3.54) (0.03)
Δ ZCTA Median HH Income 0.16 0.07 -0.13 0.00
(0.23) (0.05) (0.31) (0.00)
Aged 19 57.48*** 39.63*** -231.99*** -0.81***
(7.53) (2.19) (12.37) (0.10)
Aged 45 20.12 2.40 -37.37 -0.28
(39.97) (6.40) 28.03 (0.23)
Aged 65 -14.01 -5.97 -31.82 -0.21
(20.80) (5.97) (21.70) (0.20)
COB + 29.11 4.89 41.04 -0.27
(18.90) (16.89) (161.32) (0.93)
COB - 49.40* 2.97 81.78 1.18
(32.75) (27.08) (90.55) (0.91)
Generic Crestor -292.84*** 16.72*** -47.88*** -0.33**
(34.15) (3.74) (18.45) (0.16)
Generic Zetia 50.94 26.44 111.04 0.59
(128.41) (18.48) (91.34) (0.69)
Generic Vytorin -255.76** -3.96*** -346.34 -2.35
(109.75) (1.46) (472.85) (3.77)
Generic Lescol XL -214.62*** -11.02** -83.99 -0.54
(50.61) (5.61) (66.01) (0.45)
# Observations
7,924 7,924 7,924 7,924
# Individuals
1,981
1,981
1,981
1,981
All variables describe the year-over-year change in 6-month, same-period consumption or status in $2017. OLS =
Ordinary Least Squares; COB+/- = Gained/Lost Coordination of Benefits. Travel time is in minutes, density is #
of hospitals within a 20-mile radius, median HH income is normalized to 100s of 2017$. Effect of generic drugs
is for new prescriptions. Effects for losing prescriptions are omitted. Cluster robust standard errors are reported
in parentheses. ***p<0.01; **p<0.05; *p<0.10

107
Table A. 9. Spending and Utilization Regression Results for the DM Cohort
Drugs
Office Visits
Δ Spending
Δ Day Supply
Δ Spending
Δ Visits
Estimator FE FE OLS OLS
Variable
Post -243.88*** -18.01*** -2.15 -0.03
(84.57) (5.54) (17.94) (0.14)
Δ ED visits 11.39 2.84 98.36*** 0.77***
(67.22) (3.76) (14.74) (0.13)
Δ Time to Nearest Hospital -5.71 0.26 4.86 0.03
(19.19) (1.47) (6.17) (0.04)
Δ Hospital Density 486.01* -1.48 -16.04 0.09
(280.47) (20.74) (76.02) (0.57)
Δ ZCTA % Bachelor’s + 56.18*** 0.33 5.46 0.05
(19.59) (1.49) (5.04) (0.05)
Δ ZCTA Median HH Income 0.26 0.25* -0.72* -0.01*
(1.86) (0.14) (0.39) (0.00)
Aged 19 97.01 -48.41 -216.71 -0.57
(200.20) (37.49) (174.93) (0.73)
Aged 45 230.09 32.85 -25.16 -0.10
(206.39) (23.82) (52.15) (0.44)
Aged 65 495.40 5.68 84.00 0.53
(398.46) (17.60) (52.97) (0.41)
COB + -812.50*** -72.75 -54.14 -0.33
(164.07) (53.56) (114.27) (0.72)
COB - 1,797.88 121.42*** 287.15*** 2.92***
(1,387.36) (17.31) (72.69) (0.71)
Trulicity 1,906.64*** 70.51*** 45.29 0.42
(411.78) (25.27) (55.23) (0.44)
Tresiba Flextouch -109.57 -18.31 -17.13 -0.14
(435.50) (43.79) (52.07) (0.53)
Toujeo Solostar 574.29 135.02** 38.17 0.63
(867.73) (64.24) (60.17) (0.70)
Jaridance -218.50 116.28*** 80.03 0.98**
(1,517.18) (27.55) (59.83) (0.40)
# Observations
2,944
2,944
2,944
2,944
# Individuals
736
736
736
736
All variables describe the year-over-year change in 6-month, same-period consumption or status in $2017. OLS =
Ordinary Least Squares; GLS, RE = Generalized Least Squares, Random Effects; FE = Fixed Effects Estimation;
COB+/- = Gained/Lost Coordination of Benefits. Travel time is in minutes, density is # of hospitals within a 20-
mile radius, median HH income is normalized to 100s of 2017$. Effect of generic drugs is for new prescriptions.
Effects for losing prescriptions are omitted. Cluster robust standard errors are reported in parentheses.
***p<0.01; **p<0.05; *p<0.10

108
Table A. 10. Regression Results, Robustness Checks
Drugs
Office Visits
Δ Spending
Δ Day Supply
Δ Spending
Δ Visits
HTN
Post -6.79** -1.90 -14.74 -0.14*
(3.30) (2.65) (9.13) (0.07)
Post, excluding high spend -5.91** -3.28 -16.48* -0.16**
(2.30) (2.72) (9.11) (0.07)
LIP
Post -56.44*** -1.44 -9.91 -0.07
(8.51) (2.13) (9.43) (0.08)
Post, excluding high spend -54.04*** -1.72 -9.44 -0.07
(8.36) (2.18) (9.43) (0.08)
DM
Post -243.88*** -18.01*** -2.15 -0.03
(84.57) (5.54) (17.94) (0.14)
Post, excluding high spend -226.90*** -18.01*** -10.91 -0.06
(86.45) (5.57) (17.98) (0.14)
Post, added drugs -239.85*** -17.80*** -2.00 -0.03
(84.88) (5.55) (17.96) (0.14)
This table compares the effect of the medical price change before and after removal of employees that were in the
top 95% of out-of-pocket drug spending in FY’15. It also compares the effect of adding two additional brand
name drugs with lower market share in the DM estimates. Units are in $2017.

109
BIOGRAPHY OF THE AUTHOR
Dan Feldman was born in Brunswick, ME on April 10, 1977 and received his high school
diploma from Mt. Ararat High School in 1995. He subsequently attended Oberlin College in
Oberlin, OH where he double-majored in biology and neuroscience with a minor in African-
American studies, culminating in a bachelor of arts degree.
Following college, Dan attended the MGH Institute of Health Professions in Boston, MA (now
Charlestown). He earned a master of science in physical therapy degree in 2001 and, following a
year-long internship at National Rehabilitation Hospital in Washington, DC, began a full-time
career in pediatric physical therapy at Children’s National Medical Center in Washington, DC.
Dan spent four years at Children’s National before founding Brown Bear Home Therapies, an
agency dedicated to providing in-home physical therapy support for children with disabilities.
During this time, Dan earned board certification in pediatrics from the American Board of
Physical Therapy Specialties, a certification which he maintained through 2017. Dan sold
Brown Bear and moved back to Maine in 2010, where he joined Child Development Services as
a provider of preschool-based physical therapy and home-based parent and caregiver coaching.
He was later promoted to Early Intervention Program Manager, a position he held until his
departure in 2018 when he enrolled in the School of Economics at the University of Maine.
Dan currently lives in Bowdoinham, ME with his wife and 4-year-old daughter. He is author of
the book Long Distance Hiking (Stackpole Books) and enjoys all manner of outdoor recreation.
He is employed as a decision support analyst at MaineGeneral Health in Augusta, ME. Dan is a
candidate for the Master of Science degree from the University of Maine in August, 2020.