healthcare associated infection control and prevention ... · healthcare associated infection...
TRANSCRIPT

Healthcare Associated Infection Control and Prevention Report to NHS Lanarkshire Board 27th April 2011.
Aim The purpose of this paper is to update Board members of current status of Healthcare Associated Infections (HAI) and infection control measures, with particular reference to performance against HEAT targets and cleanliness monitoring Key issues will include
• Staph Aureus Bacteraemias • Clostridium difficile • Hand hygiene compliance • Cleanliness Monitoring • Education • Outbreaks
Other HAI activity such as surgical site surveillance and antimicrobial prescribing will also feature. Background There is a national mandatory requirement for a Healthcare Associated Infection Control report to be presented to the Board on a bi -monthly basis utilising the template below. The HAI report will continue to be submitted to the board on a monthly basis as previously.
Summary This report highlights NHS Lanarkshire performance in relation to infection prevention and control. Site specific Information features in graph format at the end of the report
Recommendation
The Board is asked to note this report.
For further information or clarification of any issues in this paper please contact: Dr Alison Graham, Medical Director, 14 Beckford Street, Hamilton, 01698 206385.
Section 1 – Board Wide Issues Key Healthcare Associated Infection Headlines for February 2011 • NHSL have for the second year achieved the Scottish Government HEAT target related
to the reduction of Staphylococcus aureus bacteraemias.
• The Healthcare Environment Inspection (HEI) team undertook an unannounced inspection at Hairmyres Hospital on Wednesday 13th April. A draft of the report will be sent to the Chief Executive on the 4th May to check for accuracies prior to return to the HEI by the 12th May, with the final report published on the HEI website on 23rd May. Whilst there was some noted improvement since the announced visit in September 2010 , there are still some environmental issues in some areas that need to be addressed and the HEI indicated they would be returning to inspect these areas in the near future.
• The joint ECDC Europe wide point prevalence survey of HAI and antimicrobial
prescribing is planned for Sept/October 2011.The aim is to measure the prevalence of all HAI types and identify priority areas for interventions and surveillance at local and national level. From the antimicrobial perspective, the survey will measure antimicrobial prescribing and compliance with antimicrobial indicators such as the local empirical prescribing policy and surgical prophylaxis policy.
Data will be collected from 100% of acute hospitals and a 25% sample of non- acute hospitals and will be a joint collaboration between the infection control team and the antimicrobial management team. Training for data collectors will be provided by Health Protection Scotland. • NHSL participated in the SAB HEAT Support Initiative held on the 31st March.
The partnership event with HPS, QIS/SPSP and NES was facilitated by Ros Moore, CNO using video-conferencing .NHSL were commended by SPSP leads for the current work being undertaken to review the management of CVC lines out-with critical care areas.

Staphylococcus aureus (including MRSA)
Current HEAT Status Staphylococcus aureus (including MRSA)
The NHS Lanarkshire HEAT target is 142 SABs for the 12 months up to the end of March 2011. During this time there were a total of 137 SABs, demonstrating that NHS Lanarkshire achieved its target. The target for 2011-2013 is for all Boards to reduce their rate of Staphylococcus aureus bacteraemias down to 0.26 or less cases per 1000 acute occupied bed days by year ending March 2013. Should Boards achieve a rolling year rate lower than 0.26 before year ending March 2013 they should aim to maintain that lower rate. However, Boards will be held to account against the 0.26 rate. The rate of 0.26 cases or less per 1000 acute occupied bed days was the “best in class” rate achieved by a single board in year ending March 2010; and is a rate that is considered to be achievable by all Boards. In the most recent quarter reported by HPS, (October 2010 – December 2010), there was a SAB rate of 0.376 episodes / 1000 AOBDs (compared with 0.368 for NHS Scotland as a whole). However the annual reported rate for the period October 2009 – September 2010 was 0.282 SABs / 1000 AOBDs (compared with 0.355 for NHS Scotland as a whole) Initiatives to Reduce Staphylococcus aureus bacteraemia • The 6 month high impact improvement plan remained on target to further reducing
SABs and assisted NHSL in meeting the SAB HEAT target 2010/11. A further long-term plan is currently being developed for the HEAT target 2011/13. Progress will continue to be overseen by the SAB/CDI Improvement Group.
• Work to test processes aimed at the provision of optimum insertion and maintenance of CVCs out with critical care areas in a targeted manner at all 3 acute sites continues.
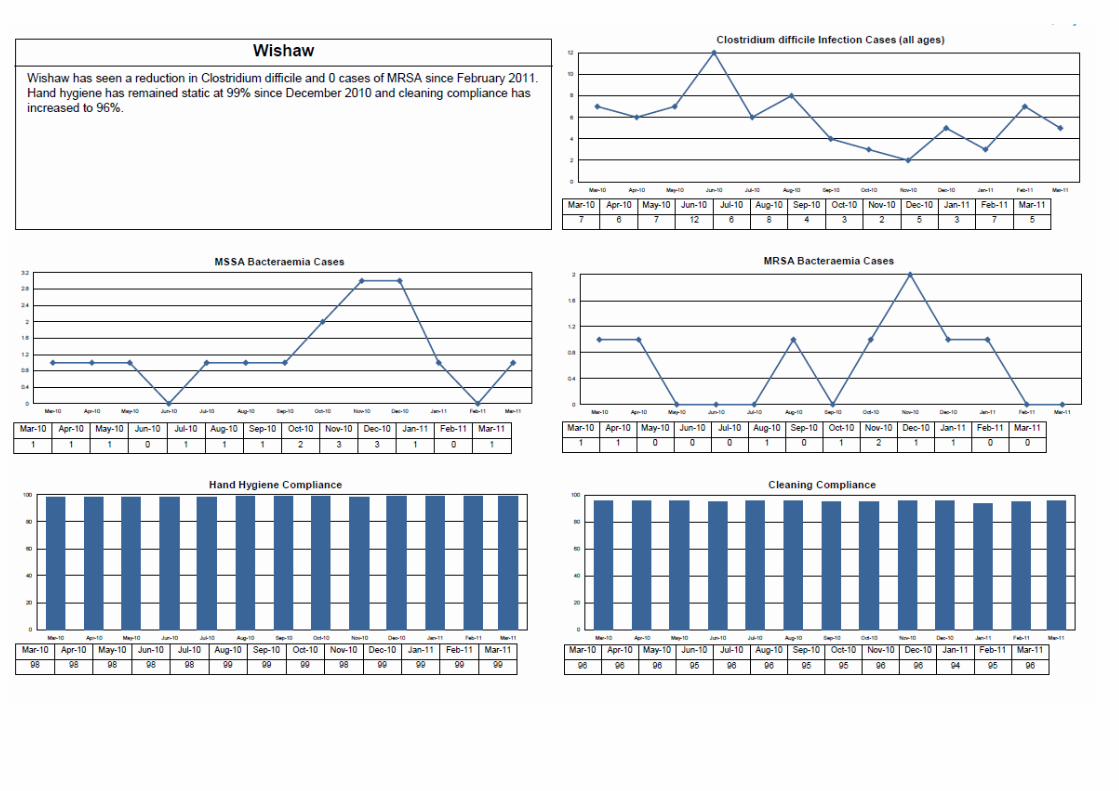
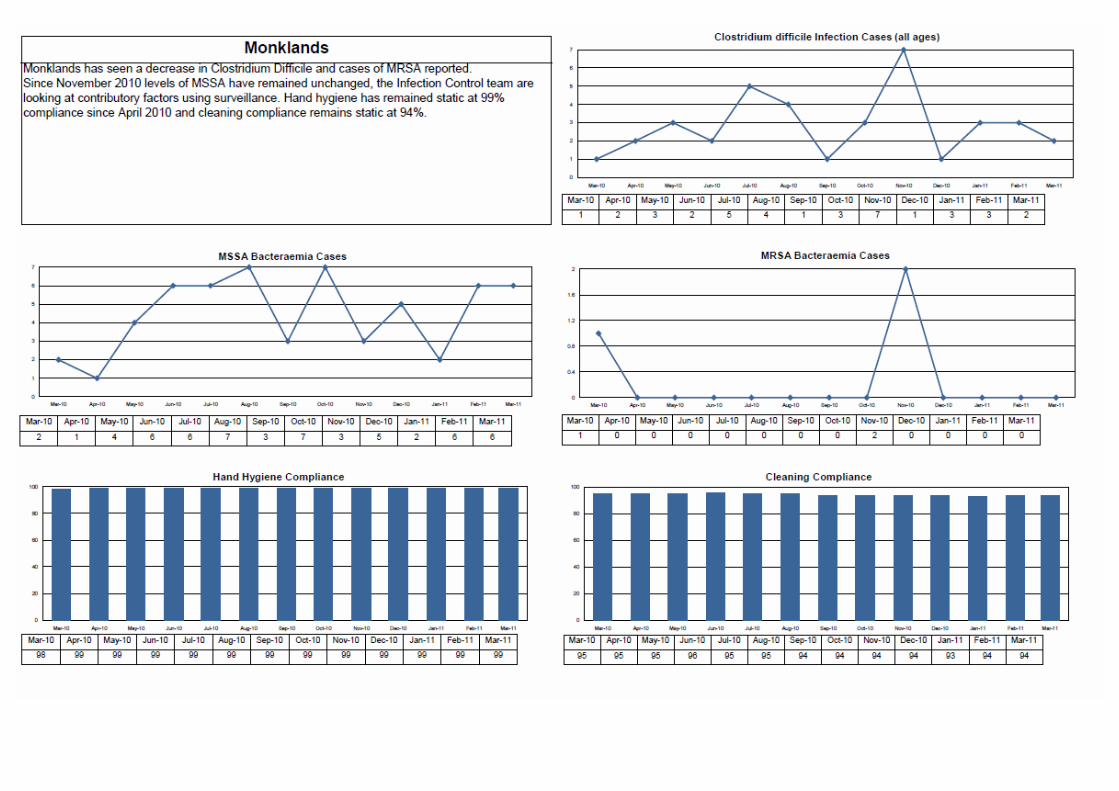
Staphylococcus aureus is an organism which is responsible for a large number of healthcare associated infections, although it can also cause infections in people who have not had any recent contact with the healthcare system. The most common form of this is Meticillin Sensitive Staphylococcus Aureus (MSSA), but the more well known is MRSA (Meticillin Resistant Staphylococcus Aureus), which is a specific type of the organism which is resistant to certain antibiotics and is therefore more difficult to treat. More information on these organisms can be found at:
http://www.nhs24.com/content/default.asp?page=s5_4&articleID=346
MRSA: http://www.nhs24.com/content/default.asp?page=s5_4&articleID=252
NHS Boards carry out surveillance of Staphylococcus aureus blood stream infections, known as bacteraemias. These are a serious form of infection and there is a national target to reduce them. The number of patients with MSSA and MRSA bacteraemias for the Board can be found at the end of section 1 and for each hospital in section 2. Information on the national surveillance programme for Staphylococcus aureus bacteraemias can be found at:

The SPSP Facilitators are driving this forward with input where required by Dr Sanjiv Chohan, Consultant Anaesthetist/SPSP Fellow. Clinician engagement at A&E, Wishaw General has also been secured.
• A draft national peripheral vascular cannula insertion checklist continues to be tested in
targeted areas at all 3 acute sites. This work is generated from a group developing national quality improvement tools and which Infection Control representation is integral.
• The Infection Control Nurse at Wishaw General presented an educational session to NHSL’s paramedics on 1st March 2011 in the care and maintenance of PVCs. This was well received and further HAI related sessions are being considered.
• The testing of Clinnel (Chlorexidine 2%) wipes is being carried out to minimise the acquisition of SABs outwith SAB hotspot and high peripheral venous cannulae areas.
• A revised ICP is being developed for use in level 1 Admission areas at all 3 acute sites
comprising peripheral and central venous cannulae care bundle elements to further minimise SABs.
• A draft national blood culture sampling checklist is currently being considered for testing
to identify practises leading to potential contamination. • SAB data at Monklands is now being feedback directly to the appropriate clinician to
better assist in facilitating clinician engagement resulting in improvements to clinical practice and resulting enhanced clinical outcomes.
• The Nurse Consultant, Infection Control, NHS QIS, has extended her Honorary Contract
in NHSL and will continue membership of the SAB/CDI improvement Group, bringing additional quality improvement approaches to reducing SABs/CDIs.
MRSA Screening Programme-Progress of Implementation The NHS Scotland MRSA Screening National Rollout Working Group Meeting was held on the 11th April 2011 and as yet Key performance indicators have still to be defined. HPS are preparing a new patient information leaflet and an information sheet for staff to explain the change to nasal and perineal swabbing. An action log is currently being drafted by the Programme Manager to outline introductory steps to the implementation of Clinical Risk assessment and subsequent nasal and perineal swabbing. Dialogue has also commenced with the Director of Nursing in order to progress implementation and alignment to better care. The current programme of nasal swabbing will continue until the clinical risk assessment (CRA) methodology is tested. Since the change to Trak care, Information Management have been experiencing difficulty with the daily downloads, and the MRSA team have been unable to provide electronic compliance data for this reporting period. There has been ongoing dialogue and testing of various downloads to resolve this matter
Clostridium difficile NHS Lanarkshire remain on trajectory to meet our HEAT target. The target for 2011-2013 is for all Boards to reduce from their current rate of Clostridium difficile infections down to 0.39 or less cases per 1000 total occupied bed days in patients aged 65 and over by year ending March 2013. Should Boards achieve a rate lower than 0.39 ahead of the March 2013 then they should aim to at least maintain that lower rate; however formal achievement of the target will still be measured against the 0.39 rate. Our exact figures for the most recent quarter October 2010 – December 2010 are 33 episodes (>65 years old) giving a rate of 0.27 cases > 65 years old / 1000 OCBDs for the quarter up to December 2010.
The annual figure reported continues to be only up to Dec 09 (0.60 cases > 65 years old / 1000 OCBDs). This compares with an original HEAT target of 1.00 cases > 65 years old / 1000 OCBDs or a revised target of 406 episodes (50% reduction) in the12 months up to March 2011.
Initiatives to reduce Clostridium difficile infection
• A national steer is still awaited on the development of a CDI Driver diagram and change package
• An NHSL draft CDI improvement plan has been developed to assist in meeting the
CDI HEAT Target 2011/13. Progress will be overseen by the SAB/CDI Improvement Group.
• A scoping exercise has been carried out to ensure that the critical elements of the
CDI Enhanced Surveillance continue resulting from the Post holder’s secondment period ending in March 2011. Data is now being collected by the Infection Control Surveillance Nurses, supported by the infection control teams locally
• The Enhanced surveillance data will undergo further analysed to determine
improvements that can be made to clinical practice and minimise the acquisition of CDI’s.
• The public Inquiry into the ‘’Outbreak of Clostridium difficile in Northern Trust
Hospitals - Northern Ireland" published in March 2011 will be scrutinised to identify
Clostridium difficile is an organism which is responsible for a large number of healthcare associated infections, although it can also cause infections in people who have not had any recent contact with the healthcare system. More information can be found at:
http://www.nhs.uk/conditions/Clostridium-difficile/Pages/Introduction.aspx
NHS Boards carry out surveillance of Clostridium difficile infections (CDI), and there is a national target to reduce these. The number of patients with CDI for the Board can be found at the end of section 1 and for each hospital in section 2. Information on the national surveillance programme for Clostridium difficile infections can be found at:
http://www.hps.scot.nhs.uk/haiic/sshaip/ssdetail.aspx?id=277

any additional actions requiring to be taken by NHSL to further inform the improvement plan for 2011/13.
• The Norovirus escalation plan developed in alignment with national guidance will be
presented at the next Acute Clinical &Governance Risk Management on the 06th May 2011, due to the previous meeting being cancelled on the 11th March 2011. The plan is still to be considered along with the review of the Boards Outbreak Plan.
Hand Hygiene
The previous Local Health Board Coordinator has taken up post as MRSA Project Manager. Ms Mary MacLean, has commenced as Local Health board Coordinator, and has worked as part of the Hand Hygiene Project since December 2008. National Audit National audit period for March/April 2011 is now complete. NHS Lanarkshire obtained an overall score of 87% (still to be validated by HPS).This figure will be sent to HPS for validation and published in the May National Audit Report. Compliance fell below the National target of 90%. Action Plans have been given to the areas with compliance below 90% with a return date of 2 weeks. The results were discussed at the local SPSP meeting on the 13th April 2011. A meeting has been scheduled between the Medical Director, HAI Manager, Divisional Director of Nursing and the Associate Directors of Nursing for each of the sites to discuss compliance issues. Scottish Patient Safety Programme (SPSP) The spread of SPSP ward self audit is nearing completion. Pioneering work has been carried out in both Primary Care and Acute Dental Services. Current Initiatives in Promoting Hand Hygiene • Hand Hygiene education sessions in partnership with Ecolab are ongoing on a monthly
basis and a plan is outlined for the coming year. • Further Education sessions being developed for key staff groups. • New awareness materials being developed for positioning at the front entrance of the
three acute sites.
Good hand hygiene by staff, patients and visitors is a key way to prevent the spread of infections. More information on the importance of good hand hygiene can be found at:
http://www.washyourhandsofthem.com/
NHS Boards monitor hand hygiene and ensure a zero tolerance approach to non compliance. The hand hygiene compliance score for the Board can be found at the end of section 1 and for each hospital in section 2. Information on national hand hygiene monitoring can be found at:
http://www.hps.scot.nhs.uk/haiic/ic/nationalhandhygienecampaign.aspx
• Primary Care Products Implementation programme complete, Cam glen and Rutherglen only areas to commence .Snagging nearing completion.
• Ecolab liaising with PSSD regarding progression of acute non clinical areas. Community Hospitals SPSP Hand Hygiene Monitoring is complete in all Acute Community Hospital Wards, 8 Primary Care / Community hospitals. The PDSA improvement methodology, education and peer support has been utilised to introduce this process Cleaning and the Healthcare Environment
• Following the HEI unannounced visit at Wishaw in December 2010, fortnightly service provider meetings are now in place with representation from PSSD, ISS & Serco. The group identified the requirement for standardising all domestic records across the sites. Some sites already operated a Daily/Weekly Cleaning Record Sheet that was signed off daily by domestic staff. The record sheet was redesigned to include sign off by nursing staff in all clinical areas. The new sheets were introduced across the three acute sites from the 14th February 2011.
• Domestic Supervisors/Managers are identifying on a daily basis, any areas that domestic staff have been unable to access for cleaning. An escalation process has been introduced to ensure all areas are cleaned promptly when the areas become available.
Keeping the healthcare environment clean is essential to prevent the spread of infections. NHS Boards monitor the cleanliness of hospitals and there is a national target to maintain compliance with standards above 90%. The cleaning compliance score for the Board can be found at the end of section 1 and for each hospital in section 2. Information on national cleanliness compliance monitoring can be found at:
http://www.hfs.scot.nhs.uk/online-services/publications/hai/
Healthcare environment standards are also independently inspected by the Healthcare Environment Inspectorate. More details can be found at:
Keeping the healthcare environment clean is essential to prevent the spread of infections. NHS Boards monitor the cleanliness of hospitals and there is a national target to maintain compliance with standards above 90%. The cleaning compliance score for the Board can be found at the end of section 1 and for each hospital in section 2. Information on national cleanliness compliance monitoring can be found at:
http://www.hfs.scot.nhs.uk/online-services/publications/hai/
Healthcare environment standards are also independently inspected by the Healthcare Environment Inspectorate. More details can be found at:
• Domestic Management are monitoring the level of calls being received through the helpdesk, relating to domestic issues. To date there has been no significant increase in calls being received
• Additional monitoring is being undertaken on all three acute sites with any issues
identified being resolved within 24 hours. • Steam Cleaners are now being used in sanitary areas at Monklands with improvement
noted in the overall appearance of shower walls, floors and sanitary fittings. • Problems continue to be experienced in relation to laundry bags not being labelled by
wards/departments prior to uplift and dispatch to the laundry. NHS Lanarkshire’s Control of Infection Manual Section D Management of Linen clearly identifies staff responsibilities to ensure traceability of improperly segregated & bagged linen. The laundry will continue to monitor non-compliance and this issue will be raised at all local HAI meetings.
• The Monitoring Framework for NHS Scotland National Cleaning Services Specification
requires Public Peer Review (PPR) involvement once per year. However since April 2009 NHSL has carried out two PPR at each acute site. As a result of the HEI visit and the resulting action plan the frequency of PPR at Wishaw, was increased to weekly during the month of February. Due to the limited availability of Public Peer Reviewers it has not been possible to sustain this level of PPR for any period of time. It is therefore the intention to carry out PPR visits at each of the 3 acute sites in March and in April. Steps are underway to recruit additional Public Peer Reviewers utilising the volunteer network (meeting scheduled for 16/3/11 with Head of Patient Affairs). Thereafter the intention, subject to successful recruitment, is to carry out PPR visits at each of the 3 acute sites 6 times per year.
• Additional matting has been placed within the main entrances at Monklands to reduce
the risk of floors becoming’ slippy’ due to a build up of grit etc. • Interviews have been held for domestic assistant vacancies at Monklands & various
community posts. It should be noted, due to the time taken to obtain references and Disclosure Scotland checks, it is taking between 8-12 weeks before successful candidates are in post. This issue is being discussed at routine meetings with PSSD / HR.
• Cleaning performance scores across all NHSL premises during January – February 2011
produced an average score of 95.8%. For the three acute sites, 239 audits were undertaken, 12 audits failed, recording a score below 90%. Within the CHP sites 117
audits were undertaken, with no failures. Hotel Services Management ensured these were rectified within 24 hours. • All amber scores (below 90%) recorded in the NMF audits are discussed with service
users, Domestic Staff, Supervisors and, if appropriate, Control of Infection. Immediate actions are put in place by Domestic Managers to rectify the shortfall, identifying any on-going issues that are making cleaning difficult. Supervision is also increased and the area monitored closely.
• The Estates Monitoring Tool, introduced by Health Facilities Scotland, from April 10 has
been live with the results of the Estates Monitoring being submitted to Health Facilities Scotland on a monthly basis. Estates performance scores have not yet been published by Health Facilities Scotland (HFS).
• In relation to expenditure of the £496k SGHD budget allocation in terms of HEI works, all works have now been completed.
• Alert Monitoring Clocks are in situ in public toilets within the three acute sites which
demonstrate to the public, patients and staff the frequency of cleans being undertaken. Currently all these areas are checked every two hours and cleaned as required. It should be noted that at Monklands these clocks are subject to regular vandalism.
• Work is now complete to revise / update the HAI SCRIBE Register which reflects one
single register for all projects underway across NHSL. A protocol has been developed in conjunction with the Nurse Consultant HAI outlining the roles & responsibilities of all individuals associated with any refurbishment works being undertaken in areas/premises.
Outbreaks/ Incidents
• Increased incidence of surgical site infection in orthopaedic surgery. Following identification of 4 orthopaedic patients (2 elective and 2 emergency admissions) having developed SSIs following hip and hemi arthroplasty procedures in January and February 2011 in Wishaw, the HAI surveillance team conducted out a look back exercise .All of the patients fell within the mandatory elements of the SSI surveillance programme however 2 of the SSI’s detected on readmission were out with 30 day post operation surveillance period. No obvious common links were found in relation to microbiology, surgeons, theatre staff or wards. A further look back exercise was undertaken in Hairmyres following identification of an increased incidence of SSI in orthopaedics following 5 procedures (3 hip arthroplasties, 1 forearm fracture fixation and 1 patella tendon repair) carried out in February and March 2011. 1 patient fell within the mandatory elements of the SSI surveillance programme. Sensitivities of organisms as well as timing of hospitalisation of the patients did not indicate an outbreak. No obvious common links were found in relation to surgeons, theatre staff or wards.
• The ICT noticed an increase in patients with C. diff toxin positive results in Ward 9 Wishaw General Hospital over a 22 day period (ranging from 18/03/11 – 08/04/11). The HPS C. diff Trigger Tool (2009) was completed by the ICN on site to promptly identify any errors in the care of patients or in antimicrobial prescribing and thereby decrease the risk of patients becoming susceptible to CDI. . No obvious links relating to cross-infection were identified on the initial investigation. All four isolates were sent to Reference laboratory for typing. To date two isolates have been reported back which
This section should give details on any outbreaks that have taken place in the Board since the last report, or a brief note confirming that none have taken place. Where there has been an outbreak then for most organisms as a minimum this section should state when it was declared, number of patients affected, number of deaths (if any), actions being taken to bring the outbreak under control and whether this was reported to the Scottish Government. For outbreaks of norovirus a more general outline of the outbreak may be more appropriate.
have been identified as not of the same type. Typing on further two isolates is awaited.(both sent 12/04/11).
• A debriefing meeting has been held to consider lessons learned arising from the outbreak of H1N1 amongst haematology patients in January 2011 at Monklands Hospital. An action plan is in the process of being developed.
Norovirus
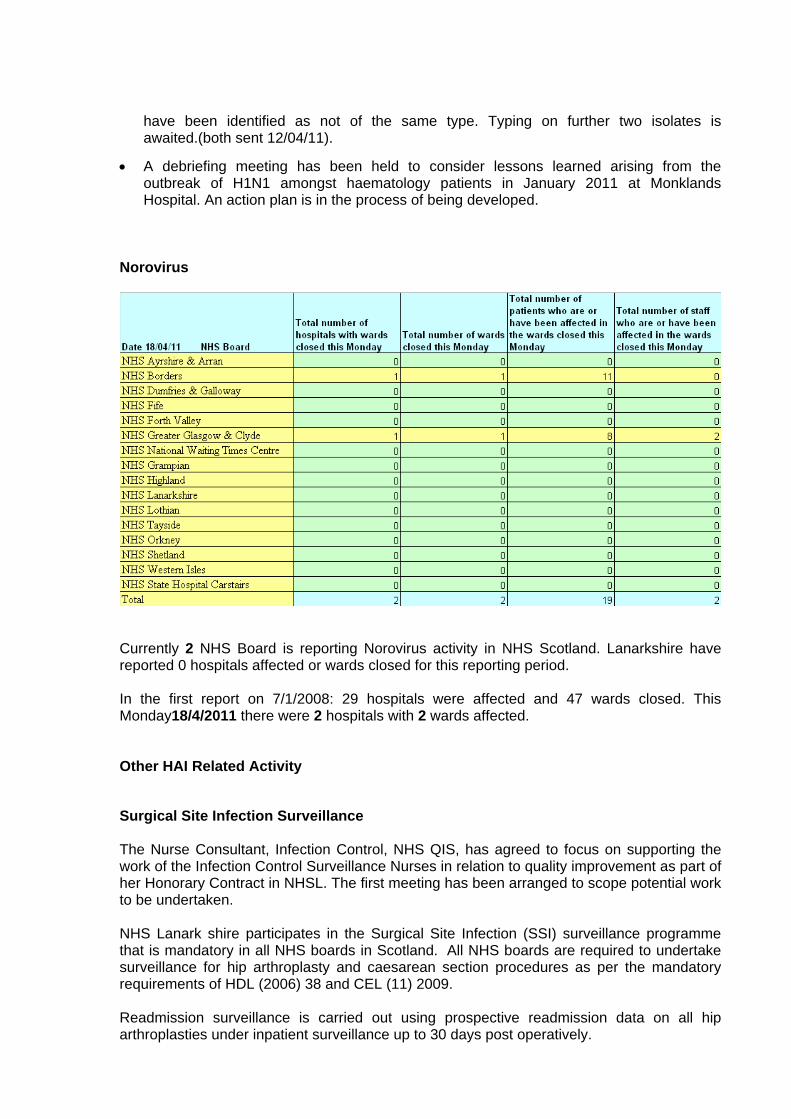
Currently 2 NHS Board is reporting Norovirus activity in NHS Scotland. Lanarkshire have reported 0 hospitals affected or wards closed for this reporting period. In the first report on 7/1/2008: 29 hospitals were affected and 47 wards closed. This Monday18/4/2011 there were 2 hospitals with 2 wards affected. Other HAI Related Activity Surgical Site Infection Surveillance The Nurse Consultant, Infection Control, NHS QIS, has agreed to focus on supporting the work of the Infection Control Surveillance Nurses in relation to quality improvement as part of her Honorary Contract in NHSL. The first meeting has been arranged to scope potential work to be undertaken. NHS Lanark shire participates in the Surgical Site Infection (SSI) surveillance programme that is mandatory in all NHS boards in Scotland. All NHS boards are required to undertake surveillance for hip arthroplasty and caesarean section procedures as per the mandatory requirements of HDL (2006) 38 and CEL (11) 2009. Readmission surveillance is carried out using prospective readmission data on all hip arthroplasties under inpatient surveillance up to 30 days post operatively.
Post discharge surveillance until day 10 post operation is also carried out for all caesarean sections performed. The aims of the Surgical Site Infection programme are:
• To collect surveillance data on surgical site infections to permit estimation of the magnitude of surgical site infection risk in hospitalised patients throughout Scotland.
• To analyse and report surgical site infection (SSI) data and describe trends in SSI rates throughout Scotland.
The national figures are dependent on all health boards inputting their data in a timely manner therefore national SSI rates should be viewed with caution. In relation to orthopaedic procedures the denominators are small therefore the infection rates are higher in comparison to national figures.
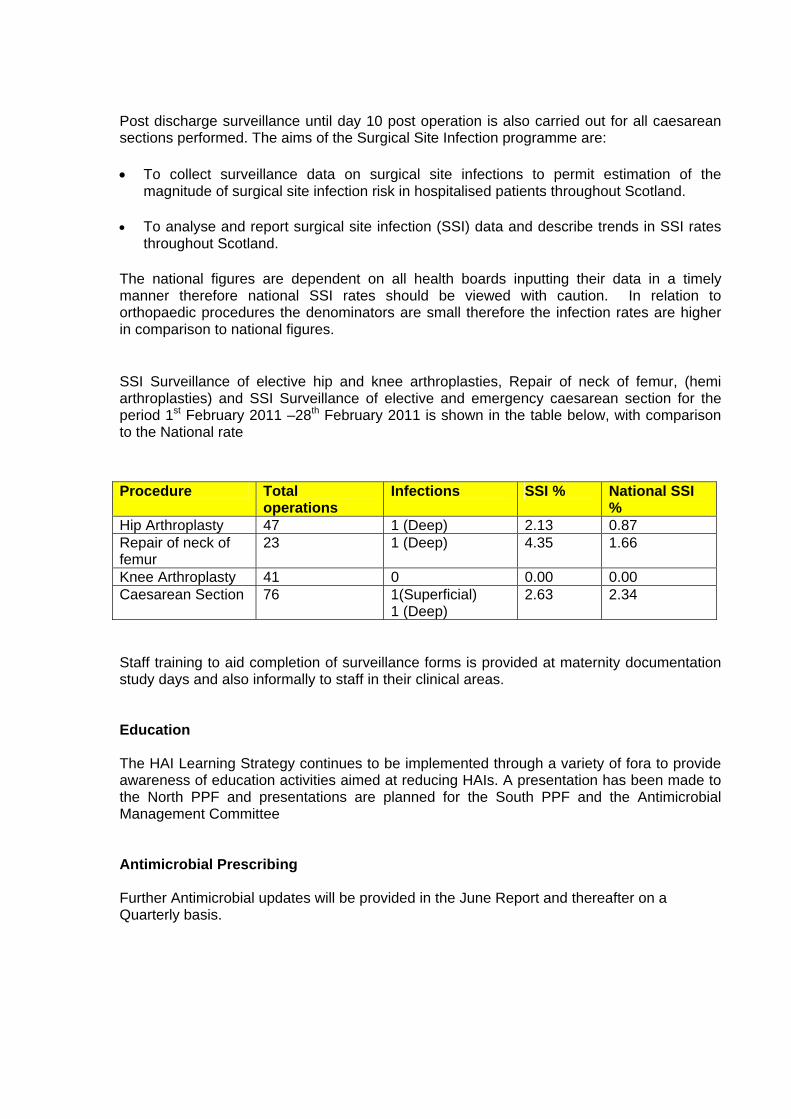
SSI Surveillance of elective hip and knee arthroplasties, Repair of neck of femur, (hemi arthroplasties) and SSI Surveillance of elective and emergency caesarean section for the period 1st February 2011 –28th February 2011 is shown in the table below, with comparison to the National rate
Staff training to aid completion of surveillance forms is provided at maternity documentation study days and also informally to staff in their clinical areas. Education The HAI Learning Strategy continues to be implemented through a variety of fora to provide awareness of education activities aimed at reducing HAIs. A presentation has been made to the North PPF and presentations are planned for the South PPF and the Antimicrobial Management Committee Antimicrobial Prescribing Further Antimicrobial updates will be provided in the June Report and thereafter on a Quarterly basis.
Procedure Total operations
Infections SSI % National SSI %
Hip Arthroplasty 47 1 (Deep) 2.13 0.87 Repair of neck of femur
23 1 (Deep) 4.35 1.66
Knee Arthroplasty 41 0 0.00 0.00 Caesarean Section 76 1(Superficial)
1 (Deep) 2.63 2.34



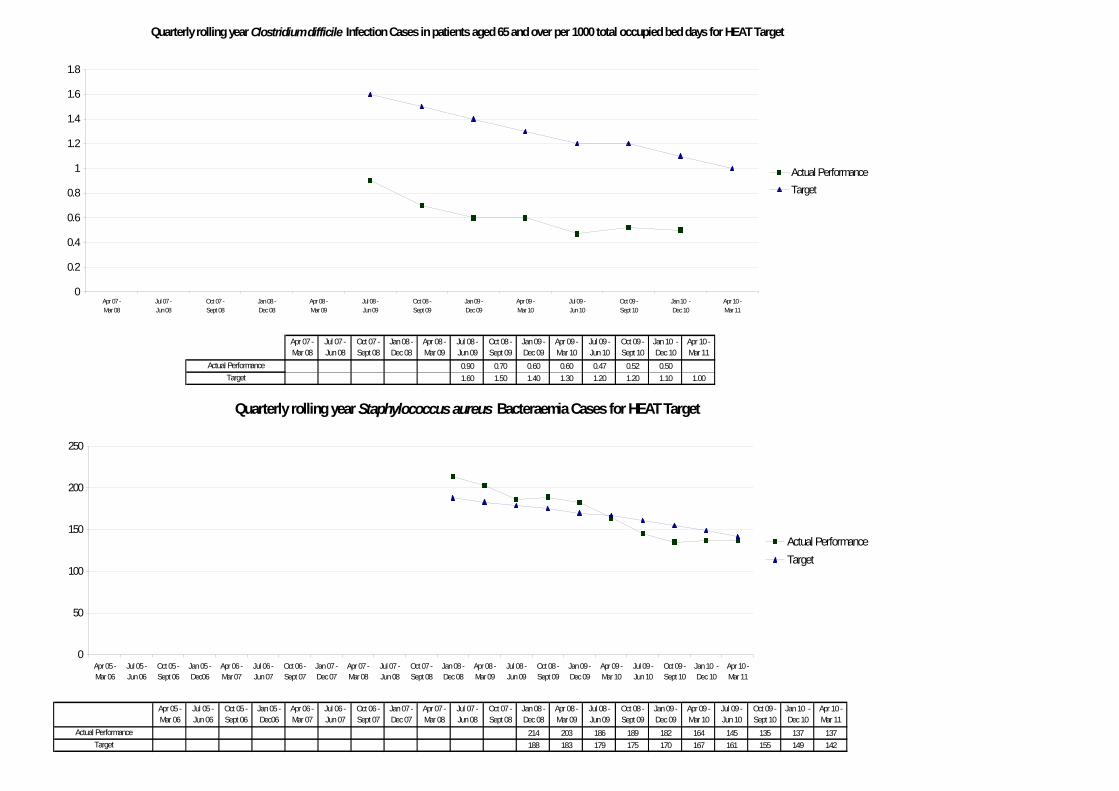
0.90 0.70 0.60 0.60 0.47 0.52 0.501.60 1.50 1.40 1.30 1.20 1.20 1.10 1.00
214 203 186 189 182 164 145 135 137 137188 183 179 175 170 167 161 155 149 142
Apr 08 -Mar 09
Jan 09 -Dec 09
Oct 08 -Sept 09
Jul 08 -Jun 09
Jan 10 -Dec 10
Oct 09 -Sept 10
Jul 09 -Jun 10
Apr 09 -Mar 10
Actual PerformanceTarget
Oct 09 -Sept 10
Jan 10 -Dec 10
Apr 06 -Mar 07
Jul 06 -Jun 07
Oct 06 -Sept 07
Jan 07 -Dec 07
Apr 07 -Mar 08
Jul 07 -Jun 08
Apr 10 -Mar 11
Oct 08 -Sept 09
Jan 09 -Dec 09
Apr 09 -Mar 10
Jul 09 -Jun 10
Apr 05 -Mar 06
Jul 05 -Jun 06
Oct 05 -Sept 06
Jan 05 -Dec06
Actual Performance
Quarterly rolling year Clostridium difficile Infection Cases in patients aged 65 and over per 1000 total occupied bed days for HEAT Target
Quarterly rolling year Staphylococcus aureus Bacteraemia Cases for HEAT Target
Jan 08 -Dec 08
Oct 07 -Sept 08
Jul 07 -Jun 08
Apr 07 -Mar 08
Target
Apr 10 -Mar 11
Oct 07 -Sept 08
Jan 08 -Dec 08
Apr 08 -Mar 09
Jul 08 -Jun 09
0
50
100
150
200
250
Apr 05 -Mar 06
Jul 05 -Jun 06
Oct 05 -Sept 06
Jan 05 -Dec06
Apr 06 -Mar 07
Jul 06 -Jun 07
Oct 06 -Sept 07
Jan 07 -Dec 07
Apr 07 -Mar 08
Jul 07 -Jun 08
Oct 07 -Sept 08
Jan 08 -Dec 08
Apr 08 -Mar 09
Jul 08 -Jun 09
Oct 08 -Sept 09
Jan 09 -Dec 09
Apr 09 -Mar 10
Jul 09 -Jun 10
Oct 09 -Sept 10
Jan 10 -Dec 10
Apr 10 -Mar 11
Actual PerformanceTarget
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
Apr 07 -Mar 08
Jul 07 -Jun 08
Oct 07 -Sept 08
Jan 08 -Dec 08
Apr 08 -Mar 09
Jul 08 -Jun 09
Oct 08 -Sept 09
Jan 09 -Dec 09
Apr 09 -Mar 10
Jul 09 -Jun 10
Oct 09 -Sept 10
Jan 10 -Dec 10
Apr 10 -Mar 11
Actual PerformanceTarget