healthcare policy essentials for georgia...
TRANSCRIPT

HEALTHCARE POLICY ESSENTIALS FOR GEORGIA APRN’S
Laura Searcy MN, APRN, PPCNP-BC President, National Association of Pediatric Nurse Practitioners UAPRN State Conference September 24, 2016 Savannah, GA

Overview of Selected Federal Policy Issues

MACRA Provisions
Removed Medicare barrier for APRN ordering of Durable Medical Equipment (DME) • As a condition for payment, section 6407 of the Affordable
Care Act (ACA) requires that a physician, physician assistant, nurse practitioner, or clinical nurse specialist conduct a face-to-face examination with a Medicare beneficiary within the last six months before writing an order for certain types of DME
• Section 6407 also required that a physician co-sign this examination if it was performed by a non-physician.
• MACRA has eliminated this requirement for physician involvement
MACRA and DME
• MACRA statute did not address Medicaid (Just CHIP) • Federal Medicaid Statute- no language for APRN ordering of
DME • Feds defer to state Medicaid program • State policies driven by practice act and insurance policies • CMS not currently enforcing DME provisions • CMS often “harmonizes” Medicaid and Medicare policies, but
has not indicated if or when this will occur • Advocates at the federal level exploring options to resolve
Quality Payment Program (enacted through MACRA)
• Repeals the Sustainable Growth Rate (SGR) Formula
• Streamlines multiple quality reporting programs into the new Merit-based Incentive Payment System (MIPS)
• Provides incentive payments for participation in Advanced Alternative Payment Models (APMs)
• Providers will participate in either a MIPS or APM
• Most clinicians will fall under MIPS

Medicare Part B eligible Clinicians are affected by MIPS
• Years 1 and 2 • Physicians (MD/DO and DMD/DDS), • PAs • NPs, Clinical Nurse Specialists, Certified Registered Nurse Anesthetists
• Years 3+ • Secretary may broaden Eligible Clinicians group to include
others such as • Physical or occupational therapists, Speech-language pathologists,
Audiologists, Nurse midwives, Clinical social workers, Clinical psychologists, Dietitians / Nutritional professionals

MIPS Composite Performance Score Year 1 category
• Quality (50%) • Clinicians will be able to choose quality measures
• Resource Use (Cost 10%) • Comparison of similar care episodes and clinical condition groups across
practices (risk adjusted)
• Clinical practice improvement activities (15%) • Care coordination, shared decision making, safety checklists, expanding practice
access
• Advancing care information( 25%) • Weight of this may decrease as more users adopt HER • NPs and PAs not eligible under this category

VA Proposed Full Practice Authority Rule
• Department of Veterans Affairs Proposed Rule (This proposal [RIN: 2900-AP44 - Proposed Rule - Advanced Practice Registered Nurses (81 Fed. Reg. 33155, May 25, 2016)]
• Authorizes NPs to practice without physician supervision practice • exception of prescribing controlled drugs
• Over 60,000 comments, mostly positive, submitted

VA Proposed Full Practice Authority Rule
Next Steps: VA to review comments, draft and publish final rule • Strong Opposition from Anesthesiologists to exclude CRNAs
from final rule
• Advanced Practice Community strongly opposes this exclusion

VA Proposed Full Practice Authority Rule
Recent Action Friday September 16: HR 5985 introduced by House Veterans Affairs committee Chair Jeff Miller (R-FL) • Critical legislation extending expiring Veterans benefits • Provision to put off for one year any rule offering FPA for
CRNA’s specifically • Vote scheduled for October 20 • Provision was removed by leadership prior to vote

Overview of State Policy Issues

Nov-12 Oct-13 Oct-14 Oct-15 Sept -16
CRNA 1821 1828 1853 1870 1890
CNM 453 457 489 501 504
NP 5466 5646 6709 7650 8590
CNS/PMH 295 288 283 271 254
CNS 57 66 110 133 147
RN 120,989 112,759 120,135 125,339 127,004

Nurse Practitioner Schedule II Controlled Substance Prescriptive Authority
Legend
Yes: 44 states + DC
Limited to Hydrocodone Combination Products: 2 states
No: 4 states
Information provided for informational purposes only and does not constitute legal advice. Please contact your state Board of Nursing or an attorney for guidance on state laws. © American Association of Nurse Practitioners, 2016 Updated: 4.21.2016

Nurse Practitioner Authorization to Sign Death Certificates
DC
Legend
Yes: 28 states
In Limited Circumstances: 3 states
No: 19 states + DC
Information provided for informational purposes only and does not constitute legal advice. Please contact your state Board of Nursing or an attorney for guidance on state laws. © American Association of Nurse Practitioners, 2016 Updated: 4.21.2016

Percent of Physician Reimbursement in Medicaid for Nurse Practitioners
Legend
100%: 29 states + DC 90-92%: 9 states
85%: 4 states 75-80%: 8 states
Information provided for informational purposes only and does not constitute legal advice. Please contact your state Board of Nursing or an attorney for guidance on state laws. © American Association of Nurse Practitioners, 2016

Nurse Practitioner Authorization to Provide Proof of Disability for Disabled Parking Placards
Information provided for informational purposes only and does not constitute legal advice. Please contact your state Board of Nursing or
an attorney for guidance on state laws. © American Association of Nurse Practitioners, 2015
Legend
Yes: 43 states
No: 6 states + DC

Recognition of Nurse Practitioners as Primary Care Providers in State Law
Information provided for informational purposes only and does not constitute legal advice. Please contact your state Board of Nursing or an
attorney for guidance on state laws. © American Association of Nurse Practitioners, 2015 Updated: 10.15.2015
Legend
Yes: 42 states (May include recognition in Medicaid
or in other insurance laws)
Not Explicitly Recognized: 8 states + DC

Nurse Practitioner Authorization to Sign
Providers Orders for Life-Sustaining Treatment (POLST)* Forms
Legend
Yes: 28 states (Hover over each state for more detail.)
No: 9 states (Hover over each state for more detail.)
POLST Program in Early Development: 7 states
No POLST Program: 6 states + DC
Information provided for informational purposes only and does not constitute legal advice. Please contact your state Board of Nursing or an
attorney for guidance on state laws. © American Association of Nurse Practitioners, 2016 Updated: 4.21.2016
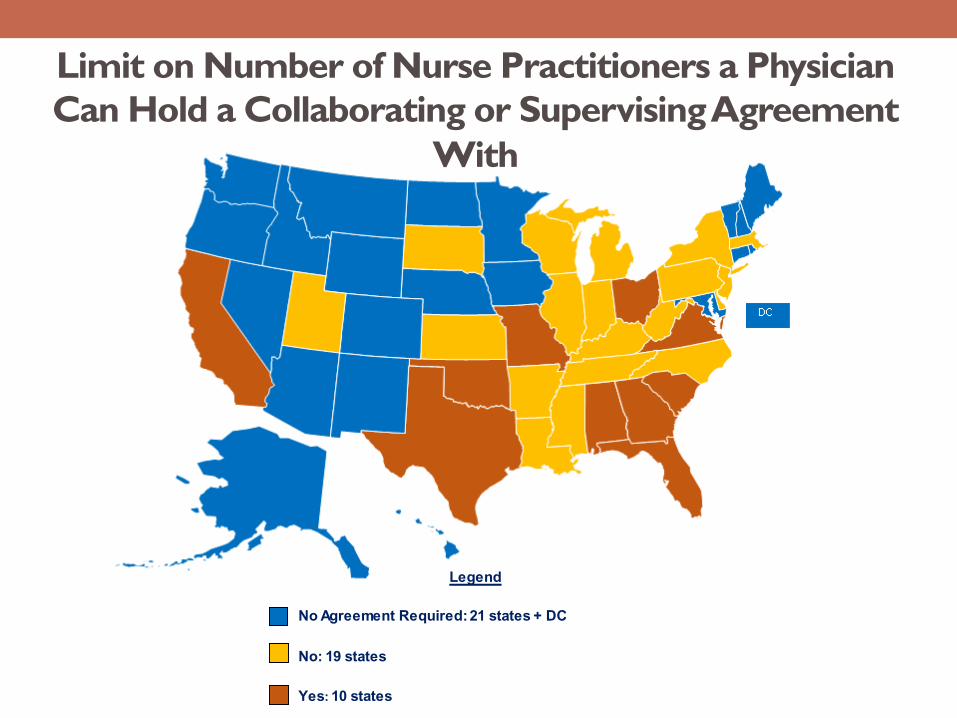
Limit on Number of Nurse Practitioners a Physician Can Hold a Collaborating or Supervising Agreement
With
Information provided for informational purposes only and does not constitute legal advice. Please contact your state Board of Nursing or an attorney for guidance on
state laws. © American Association of Nurse Practitioners, 2015 Updated: 3.24.16
Legend
No Agreement Required: 21 states + DC
No: 19 states Yes: 10 states

Advanced Nurse Practitioner's Loan Repayment Program
• Georgia Board of Physician Workforce proposed rule (Not Composite Medical Board) will administer the funds
• Budget item in the 2017 state budget($200,000 total for APRN’s and PA’s)
• Two separate proposed rules, one for APRN’s, one for PA’s http://gbpw.georgia.gov/notice-intent-amend-rules
• Written Comments accepted through September 30, 2016 • Public Hearing October 20, 2016 8:30 am Morehouse School of
Medicine • 720 Westview Drive SW Atlanta, GA 30310

State of Healthcare in Georgia Commonwealth Fund State Health System Scorecard
Georgia Ranking • Overall Performance: GA in Bottom quartile (13 states) • Access and Affordability: 41 • Prevention and Treatment: 46 • Avoidable Hospital Use 28 • Healthy Lives 39 • Equity 46



Rural Health Care Crisis
Sept. 16, 2016 Saporta Report Rural Georgia, home to 17 percent of state’s residents, faces grueling hardships David Pendered reports that the once-behemoth Rural Georgia is slumping to its knees. The region that once controlled the governor’s office, state House and Senate, and the highway department is bleeding jobs as health care is becoming scarce, according to accounts in two recent reports. Georgia Trend Daily, 9/16/16

Rural Health Care Crisis
August, 2016, the Georgia Chamber of Commerce issued a white paper that portrays a grim case for rural health care. • Four rural hospitals have closed since 2013
• Rural hospitals are scaling back services; this sets the stage for a vicious cycle of health care shortage because physicians won’t move to places with limited hospital privileges
• Rural patients tend to utilize emergency rooms, where care is the most costly to provide

Rural Health Care Crisis
Rural Georgia is defined as the 124 counties that aren’t in metro Atlanta or the 13 hub cities scattered across the state. • Rural Georgia lost 6.9 percent of its jobs from 2007 to 2014.
• At same time rural population grew 12.7%
• Compare to: • loss of 0.3 percent in metro Atlanta • loss of 2.7 percent in hub cities

Georgia Health Related Legislative Study Committees
• Children's Mental Health
• Health, Education, and School Based Health Centers
• Senate Study Committee on Surprise Billing Practices (SR 974)
• Senate Study Committee on Premium Assistance (SR 1056)

Georgia Health Related Legislative Study Committees
• State Commission on Narcotics Treatment in Georgia (SB 402) • October 11 in Ringold Georgia at 9 am
• House Study Committee on Mental Illness Initiative (HR 1093) • September 29 from 9-12:30 in room 606 CLOB (Coverdale Legislative
Office Building (18 Capitol Sq. SW SW, Atlanta, GA )
• Senate Study Committee on Opioid Abuse (SR 1165) • September 30 In Gainesville • October 28 at the Capitol

Georgia Health Related Legislative Study Committees
• Senate Study Committee on Hearing Aids for Children (SR 1091)
• Senate Study Committee on Emergency Cardiac Centers (SR 1154)
• Senate Study Committee on State Sponsored Self-Insured Group Health Insurance Plan (SR 1166)

Many Georgians caught in the Coverage Gap
• 400,000 Georgians unable to obtain insurance coverage gap • Do not qualify for Medicaid • Not enough income to qualify for health insurance marketplace subsidies
WHY: Georgia did not expand Medicaid August, 2016: Georgia Chamber of Commerce Health and Wellness Committee • Proposed three policy alternatives to close the coverage gap
• Would require applying to the federal government for a waiver from full Medicaid expansion

To gain the support of an elected official for an APRN initiative, there must be a preexisting relationship of trust and an understanding of the role and skills of APRN’s FROM THEIR HOME DISTRICTS They care what their constituents think, not what the organization thinks
APRN Advocacy Basics

APRN Advocacy Basics
Nursing 101 Therapeutic relationship • Essential • Trust and Respect are key components. • Transfers to advocacy
Legislative successes are built one legislator at a time when there is a relationship based on trust, respect and an understanding of our roles and how we serve their constituents
Only YOU can accomplish this.
• Write a letter introducing your self as a health care expert in your field, your role and patients served and offer assistance in any health care related areas
• Invite elected officials to local meetings of fellow professionals
• Invite elected to your practice site
• Find out some of their main interests, and agree to work on some of their priority projects
Relationships require effort and outreach throughout the year (3-6 contacts a year )

Meet your legislators in person if at all possible
1. “Know your audience”. Learn as much as you can about them prior to the visit : http://www.legis.ga.gov/en-US/default.aspx
2. Share background and offer support on issues you share in common
3. Follow-up with a letter (e-mail is ok, but “snail mail” is noticed)
a) providing a brief description of the patient care you provide b) Include your contact information. c) Know (or ask) whether your legislators prefer phone calls. E-
mails, or fax communications.
APRN Advocacy Basics

} Interview them when they’re running for office, and find the candidate that supports nursing issues
} Tell all of your colleagues
} If supportive, you can also offer to help them with election efforts. If you help them, they’ll often help you
APRN Advocacy Basics

• When discussing legislation, know and provide the bill number,
and the sponsor’s name, if possible • Provide them with local stories and situations that
illustrate your stance on an issue • A picture relevant to your concerns or funding requests with a
few words about how your desired outcome would improve the lies of Georgians is more powerful than a 3 page letter or newsletter they don‘t have time to read
Be Specific and Concise in your
communications

• Be able to articulate your challenges in providing the best care to your patients . That these challenges exist in Georgia, but not other states, and how changes would improve ACCESS and QUALITY for your patients and REDUCE COSTS
• Now go TELL YOUR STORY to physicians, patients, leaders in your community, etc.
Success is within our reach !!

.
I am only one, but I am one. I cannot do everything, but I can do something. And because I cannot do everything, I will not refuse to do the something that I can do. Edward Everett Hale, a 19th century American author and historian

Thanks so much for all the “somethings” that you do each day.