healthcare workers and ppe: lessons from sars/media/files/activity files... · healthcare workers...
TRANSCRIPT
Healthcare Workers and PPE: Lessons from SARS
Healthcare Workers and PPE: Lessons from SARS
Allison McGeer, MSc, MD, FRCPCMount Sinai HospitalUniversity of Toronto
Allison McGeer, MSc, MD, FRCPCMount Sinai HospitalUniversity of Toronto
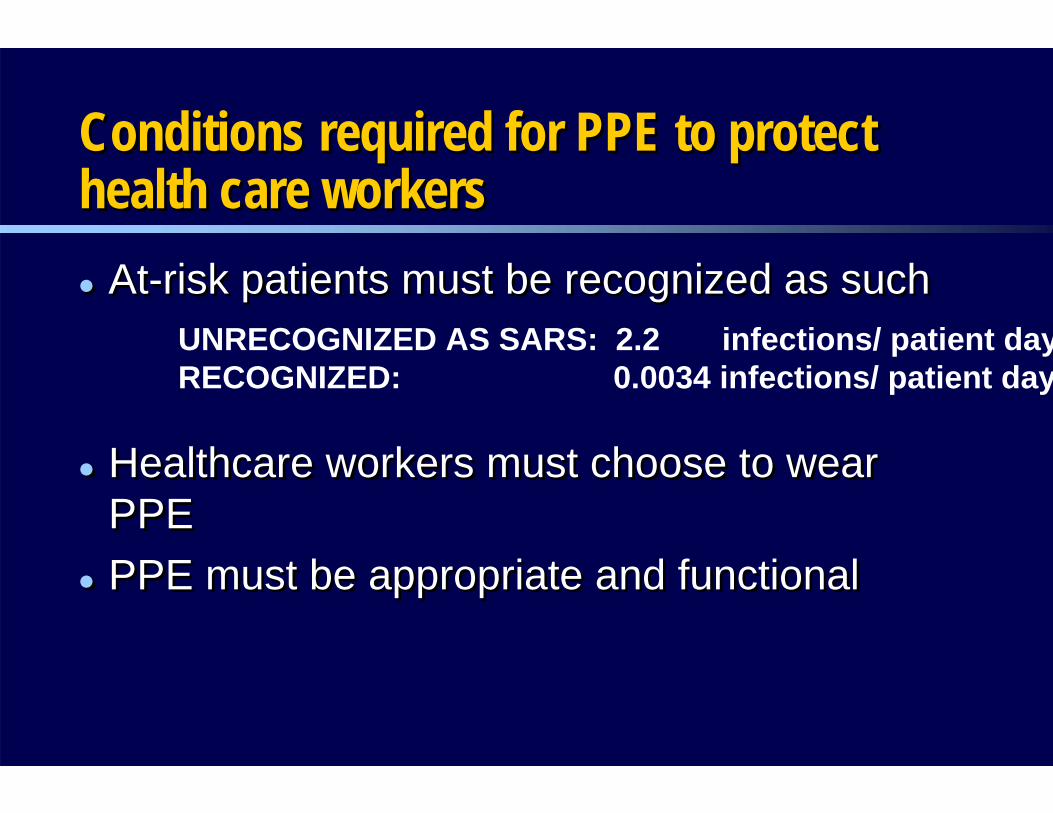
Conditions required for PPE to protect health care workersConditions required for PPE to protect Conditions required for PPE to protect health care workershealth care workers
At-risk patients must be recognized as such
Healthcare workers must choose to wear PPEPPE must be appropriate and functional
At-risk patients must be recognized as such
Healthcare workers must choose to wear PPEPPE must be appropriate and functional
UNRECOGNIZED AS SARS: 2.2 infections/ patient dayRECOGNIZED: 0.0034 infections/ patient day
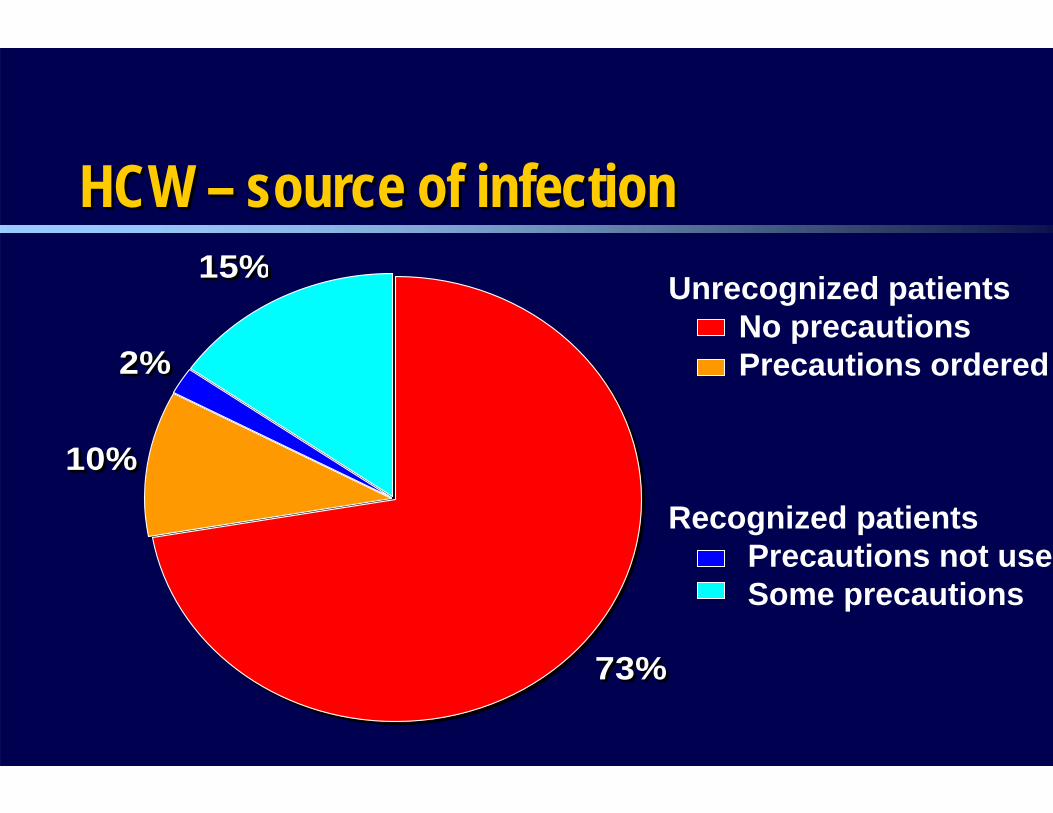
HCW – source of infectionHCW HCW –– source of infectionsource of infection
10%
2%
15%
73%
10%
2%
15%
73%
Unrecognized patientsNo precautionsPrecautions ordered
Recognized patientsPrecautions not useSome precautions

ProblemsProblemsProblems
If you ask HCWs to use inconvenient preventive practice when they think it is unnecessary–THEY WON’T DO IT
Barrier precautions are associated with highly significant rates of PATIENT adverse effects– Half as many HCW visits, 33% less contact time, increased rates of
depression, anxiety, anger, – 12% risk of preventable adverse events per one week admission
If you ask HCWs to use inconvenient preventive practice when they think it is unnecessary–THEY WON’T DO IT
Barrier precautions are associated with highly significant rates of PATIENT adverse effects– Half as many HCW visits, 33% less contact time, increased rates of
depression, anxiety, anger, – 12% risk of preventable adverse events per one week admission
To assess adherence to barrier precautions among staff who cared for critically ill SARS
patients during the Toronto SARS outbreak
ObjectiveObjectiveObjective
Design –Retrospective cohort analysisCohort – HCWs providing care for SARS patients immediately (<24h) before and during intubation during the Toronto outbreak (March-June, 2003)Cohort identification - HCWs identified from charts, staffing assignment forms, managers, and colleagues Data collection - Face-to-face interview using structured questionnaire, with chart available
Design –Retrospective cohort analysisCohort – HCWs providing care for SARS patients immediately (<24h) before and during intubation during the Toronto outbreak (March-June, 2003)Cohort identification - HCWs identified from charts, staffing assignment forms, managers, and colleagues Data collection - Face-to-face interview using structured questionnaire, with chart available
MethodsMethodsMethods
Outcome: – Consistent adherence to PPE
eye protection, mask, gloves, and gown“always wore”
Secondary: Removal practices
Outcome: – Consistent adherence to PPE
eye protection, mask, gloves, and gown“always wore”
Secondary: Removal practices
MethodsOutcome measuresMethodsMethodsOutcome measuresOutcome measures
PPE removalPPE removalPPE removalSafest– Gloves removed first– Consistent hand disinfection BEFORE hands touch face– Hand disinfection as terminal event
Some risk– Gloves removed first– Hand disinfection at least once
At risk– Gloves NOT removed first– No hand disinfection described
Safest– Gloves removed first– Consistent hand disinfection BEFORE hands touch face– Hand disinfection as terminal event
Some risk– Gloves removed first– Hand disinfection at least once
At risk– Gloves NOT removed first– No hand disinfection described
• Patient-related: –Patient’s diagnosis, Severity of illness (APACHE II
score), Precautions orderedHCW-related:
–Age, gender, occupation–Hospital, type of ward (SARS unit, ICU, ED, other)–Time spent in patient’s room–Number of room entries– Involvement in patient care activities (N=34)– Infection control training
• Patient-related: –Patient’s diagnosis, Severity of illness (APACHE II
score), Precautions orderedHCW-related:
–Age, gender, occupation–Hospital, type of ward (SARS unit, ICU, ED, other)–Time spent in patient’s room–Number of room entries– Involvement in patient care activities (N=34)– Infection control training
MethodsPredictor variablesMethodsMethodsPredictor variablesPredictor variables
ResultsResultsResults
56 patients intubated15 hospitals (4 teaching, 11 community) diagnosis at time of care– 49 SARS– 3 pneumonia (during outbreak)– 1 contact + airborne– 1 MRSA (gown, glove, mask)– 2 pneumonia (prior to outbreak recognition)
56 patients intubated15 hospitals (4 teaching, 11 community) diagnosis at time of care– 49 SARS– 3 pneumonia (during outbreak)– 1 contact + airborne– 1 MRSA (gown, glove, mask)– 2 pneumonia (prior to outbreak recognition)
795 HCWs (90% of 879 eligible) enrolled46% (368) nurses 14% (113) respiratory therapists 14% (113) physicians10% (82) X-ray technologists16% (125) Other (eg. paramedic, physiotherapists
Most HCWs cared for 1 patient (range 1-8) – 164 (20%) cared for more than one patient
5146 patient care activities/procedures assessed
795 HCWs (90% of 879 eligible) enrolled46% (368) nurses 14% (113) respiratory therapists 14% (113) physicians10% (82) X-ray technologists16% (125) Other (eg. paramedic, physiotherapists)
Most HCWs cared for 1 patient (range 1-8) – 164 (20%) cared for more than one patient
5146 patient care activities/procedures assessed
ResultsResultsResults
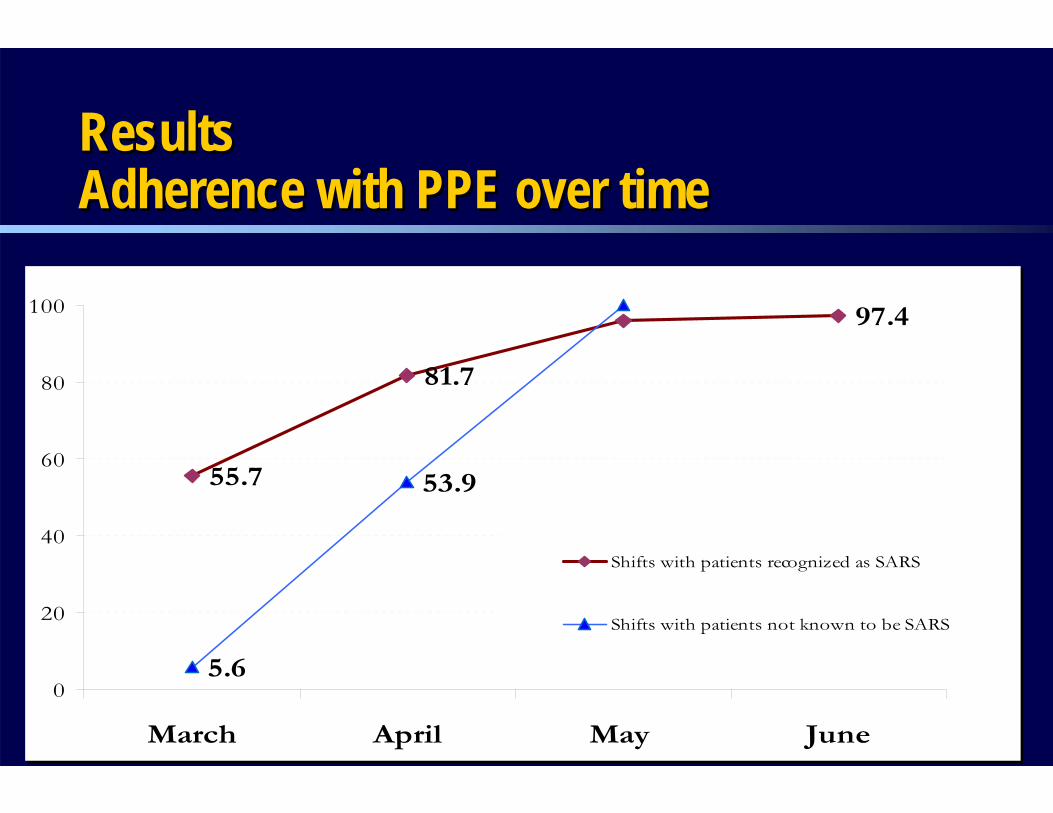
55.7
97.4
5.6
81.7
53.9
34.6
0
20
40
60
80
100
March April May June
Shifts with patients recognized as SARS
Shifts with patients not known to be SARS
55.7
97.4
5.6
81.7
53.9
34.6
0
20
40
60
80
100
March April May June
Shifts with patients recognized as SARS
Shifts with patients not known to be SARS
Pts with diagnosis of SARS
Pts not recognized as SARS
ResultsAdherence with PPE over timeResultsResultsAdherence with PPE over timeAdherence with PPE over time
64.372.274.5
84
59.780.9
86.5
57.176.4
88.2
6485.5
29.284.6
0 10 20 30 40 50 60 70 80 90 100
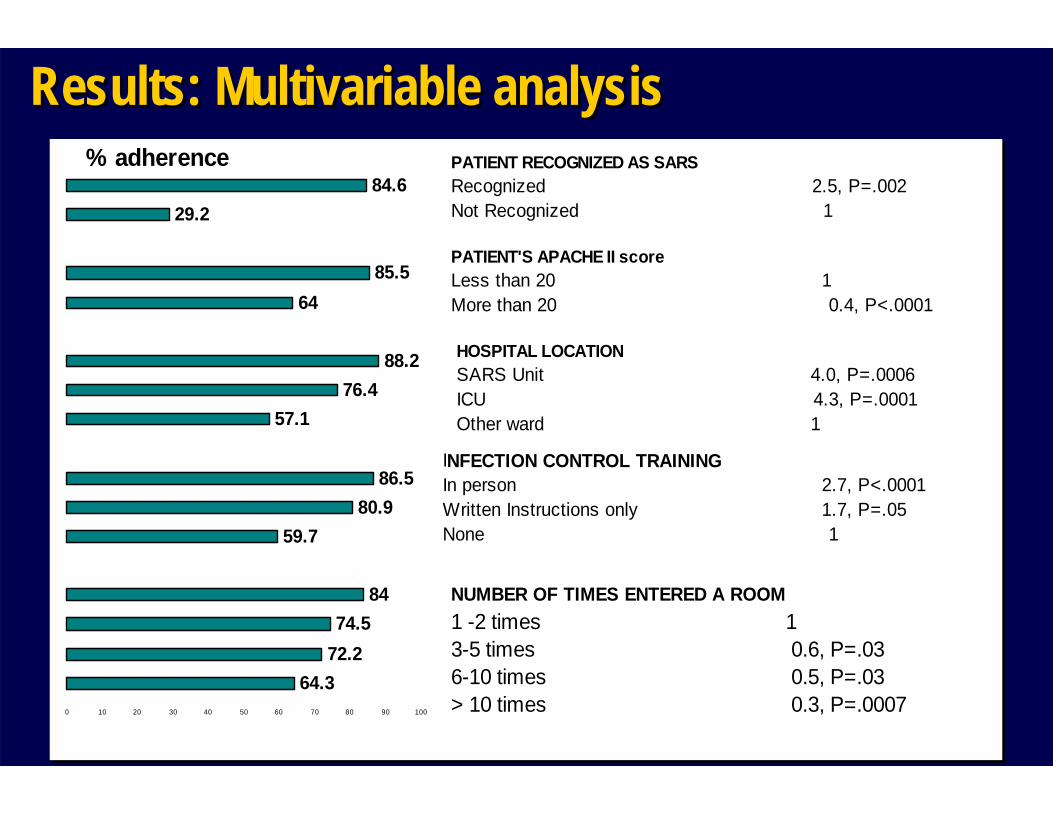
PATIENT RECOGNIZED AS SARS Recognized 2.5, P=.002Not Recognized 1
PATIENT'S APACHE II score Less than 20 1More than 20 0.4, P<.0001
HOSPITAL LOCATIONSARS Unit 4.0, P=.0006ICU 4.3, P=.0001Other ward 1
INFECTION CONTROL TRAINING In person 2.7, P<.0001Written Instructions only 1.7, P=.05None 1
NUMBER OF TIMES ENTERED A ROOM 1 -2 times 13-5 times 0.6, P=.036-10 times 0.5, P=.03> 10 times 0.3, P=.0007
% adherence
64.372.274.5
84
59.780.9
86.5
57.176.4
88.2
6485.5
29.284.6
0 10 20 30 40 50 60 70 80 90 100
PATIENT RECOGNIZED AS SARS Recognized 2.5, P=.002Not Recognized 1
PATIENT'S APACHE II score Less than 20 1More than 20 0.4, P<.0001
HOSPITAL LOCATIONSARS Unit 4.0, P=.0006ICU 4.3, P=.0001Other ward 1
INFECTION CONTROL TRAINING In person 2.7, P<.0001Written Instructions only 1.7, P=.05None 1
NUMBER OF TIMES ENTERED A ROOM 1 -2 times 13-5 times 0.6, P=.036-10 times 0.5, P=.03> 10 times 0.3, P=.0007
% adherence
Results: Multivariable analysisResults: Multivariable analysisResults: Multivariable analysis
20
30
40
50
60
70
80
90
100
Perform
edAss
isted
Observ
ed
Perform
edAss
isted
Observ
ed
Perform
edAss
isted
Observ
ed
Perform
edAss
isted
Observ
ed
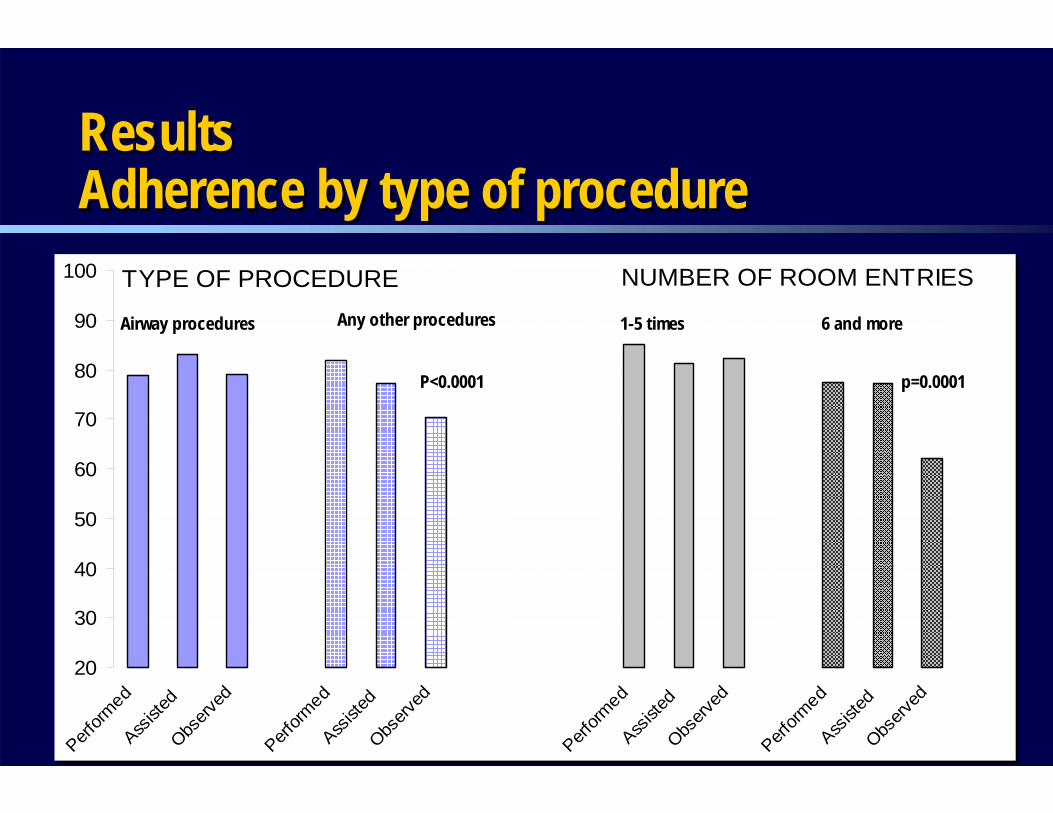
Airway procedures Any other procedures
P<0.0001
1-5 times 6 and more
p=0.0001
TYPE OF PROCEDURE NUMBER OF ROOM ENTRIES
20
30
40
50
60
70
80
90
100
Perform
edAss
isted
Observ
ed
Perform
edAss
isted
Observ
ed
Perform
edAss
isted
Observ
ed
Perform
edAss
isted
Observ
ed
Airway procedures Any other procedures
P<0.0001
1-5 times 6 and more
p=0.0001
TYPE OF PROCEDURE NUMBER OF ROOM ENTRIES
ResultsAdherence by type of procedureResultsResultsAdherence by type of procedureAdherence by type of procedure
Results Removal practicesResults Results Removal practicesRemoval practices
Safest – 15%Some risk – 62%At risk – 22%
Safest – 15%Some risk – 62%At risk – 22%
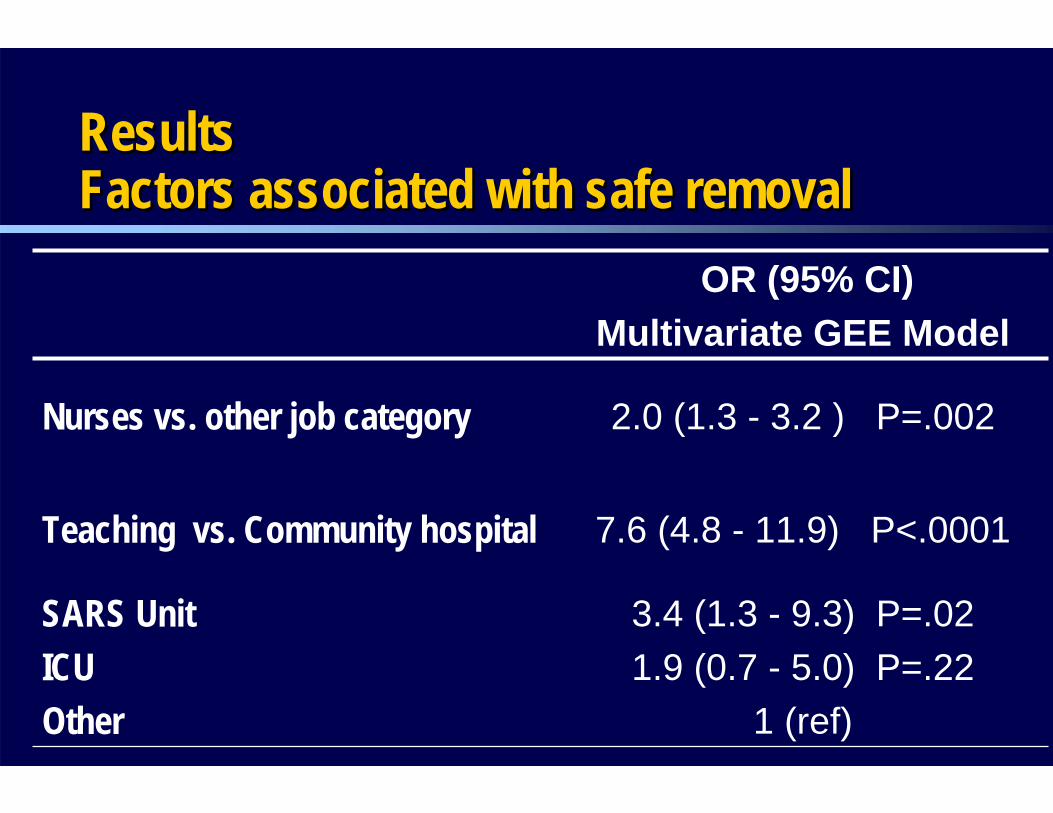
3.4 (1.3 - 9.3) P=.021.9 (0.7 - 5.0) P=.22
1 (ref)
SARS UnitICUOther
7.6 (4.8 - 11.9) P<.0001Teaching vs. Community hospital
2.0 (1.3 - 3.2 ) P=.002Nurses vs. other job category
OR (95% CI)Multivariate GEE Model
ResultsFactors associated with safe removalResultsResultsFactors associated with safe removalFactors associated with safe removal
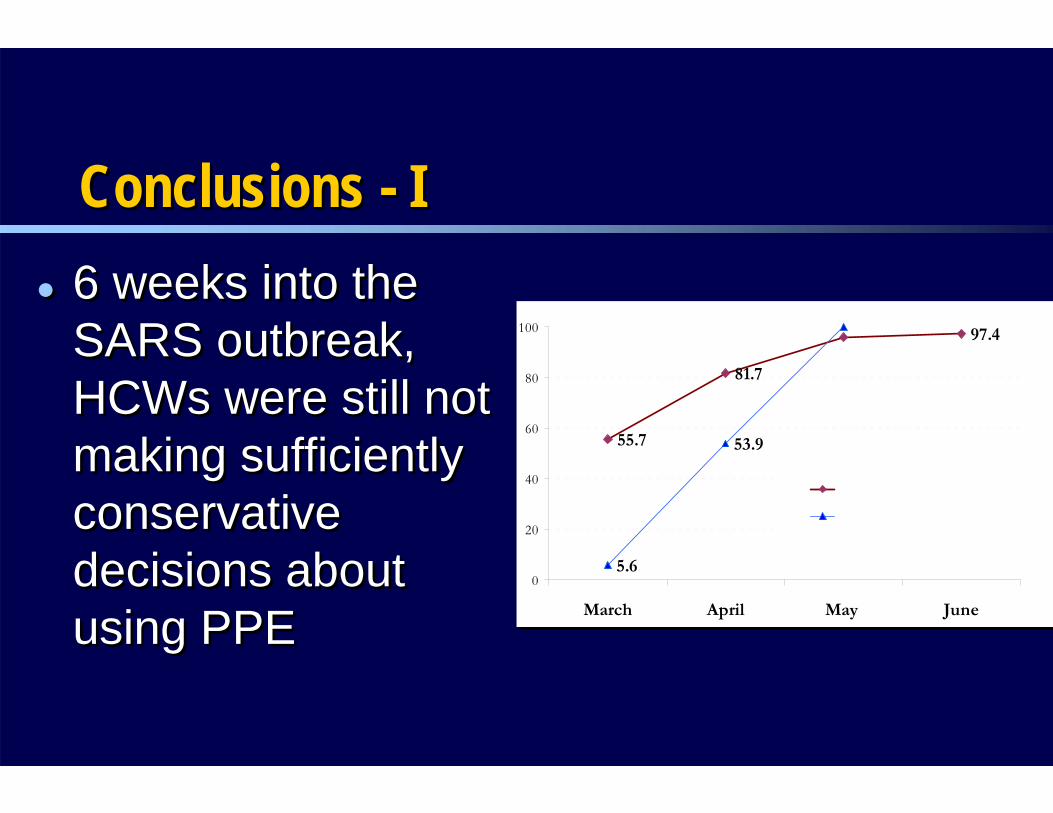
6 weeks into the SARS outbreak, HCWs were still not making sufficiently conservative decisions about using PPE
6 weeks into the SARS outbreak, HCWs were still not making sufficiently conservative decisions about using PPE
55.7
97.4
5.6
81.7
53.9
34.6
0
20
40
60
80
100
March April May June
Shifts with patients recognized as SARS
Shifts with patients not known to be SARS
All shifts
55.7
97.4
5.6
81.7
53.9
34.6
0
20
40
60
80
100
March April May June
Shifts with patients recognized as SARS
Shifts with patients not known to be SARS
All shifts
Conclusions - IConclusions Conclusions -- II
Decreased adherence with increased APACHE score suggests that HCWs may make decisions based on patient safety despite risk to themselves
This cohort did not make PPE decisions based on the procedure they were about to undertake
Decreased adherence with increased APACHE score suggests that HCWs may make decisions based on patient safety despite risk to themselves
This cohort did not make PPE decisions based on the procedure they were about to undertake
Conclusions - IIConclusions Conclusions -- IIII
Education is critical– In person training>written materials>none– SARS units>other hospital areas– Teaching hospitals vs community for PPE
removalDespite education, most HCWs did not clearly understand self-contamination with PPE removal
Education is critical– In person training>written materials>none– SARS units>other hospital areas– Teaching hospitals vs community for PPE
removalDespite education, most HCWs did not clearly understand self-contamination with PPE removal
Conclusions - IIIConclusions Conclusions -- IIIIII
Research questionsResearch questionsResearch questionsWhy was education so important during SARS outbreak, when other research suggests that knowledge is not a particularly important factor in HCW PPE adherence?How to worker and patient safety interact? How do we balance priorities if they conflict?Is a continued focus on procedure-driven PPE feasible?
Why was education so important during SARS outbreak, when other research suggests that knowledge is not a particularly important factor in HCW PPE adherence?How to worker and patient safety interact? How do we balance priorities if they conflict?Is a continued focus on procedure-driven PPE feasible?
Toronto SARS Hospital Investigation Team:E. Bontovics, D. Gravelle, B. Henry, M. Loeb, C.
MacDonald, S. Paton, J.M. Raboud, D. Scales, S. Shen, A.E. Simor, M. Vearncombe, D. Zoutman
Patients with SARS, their families and friendsThe staff, visitors and patients of greater Toronto area hospitals and public health departments and their families
Toronto SARS Hospital Investigation Team:E. Bontovics, D. Gravelle, B. Henry, M. Loeb, C.
MacDonald, S. Paton, J.M. Raboud, D. Scales, S. Shen, A.E. Simor, M. Vearncombe, D. Zoutman
Patients with SARS, their families and friendsThe staff, visitors and patients of greater Toronto area hospitals and public health departments and their families
AcknowledgementsAcknowledgementsAcknowledgements