healthy aging: factors that predict preservation of
TRANSCRIPT

Loma Linda UniversityTheScholarsRepository@LLU: Digital Archive of Research,Scholarship & Creative Works
Loma Linda University Electronic Theses, Dissertations & Projects
8-2018
Healthy Aging: Factors that Predict Preservation ofCognitive Functioning in Older AdultsImari-Ashley F. Palma
Follow this and additional works at: http://scholarsrepository.llu.edu/etd
Part of the Medicine and Health Sciences Commons, and the Psychology Commons
This Dissertation is brought to you for free and open access by TheScholarsRepository@LLU: Digital Archive of Research, Scholarship & CreativeWorks. It has been accepted for inclusion in Loma Linda University Electronic Theses, Dissertations & Projects by an authorized administrator ofTheScholarsRepository@LLU: Digital Archive of Research, Scholarship & Creative Works. For more information, please [email protected].
Recommended CitationPalma, Imari-Ashley F., "Healthy Aging: Factors that Predict Preservation of Cognitive Functioning in Older Adults" (2018). LomaLinda University Electronic Theses, Dissertations & Projects. 518.http://scholarsrepository.llu.edu/etd/518

LOMA LINDA UNIERSITY
School of Behavioral Health
in conjunction with the
Faculty of Graduate Studies
____________________
Healthy Aging: Factors that Predict Preservation of Cognitive Functioning
in Older Adults
by
Imari-Ashley F. Palma
____________________
A Dissertation submitted in partial satisfaction of
the requirements for the degree
Doctor of Philosophy in Psychology
____________________
August 2018

© 2018
Imari-Ashley F. Palma
All Rights Reserved

iii
Each person whose signature appears below certifies that this dissertation in his/her opinion
is adequate, in scope and quality, as a dissertation for the degree Doctor of Philosophy.
, Chairperson
Adam L. Aréchiga, Associate Professor of Psychology
Rebecca E. Ballinger, Licensed Clinical Psychologist
Grace J. Lee, Assistant Professor of Psychology
David A. Vermeersch, Professor of Psychology

iv
ACKNOWLEDGEMENTS
I would like to thank Dr. Aréchiga who has consistently supported me throughout
my graduate studies and from start to finish with my dissertation. Your mentorship,
patience, and kindness have influenced me greatly and I will forever be grateful for your
leadership and friendship.
I would also like to thank each member of my committee: Dr.’s Lee, Vermeersch,
and Ballinger. I cannot express my deepest gratitude for the help each of you have
offered me throughout this journey. I want to especially thank Dr. Lee for her dedicated
assistance with the editing and revision process. I would not have been able to
successfully complete this milestone without you.
To the most important people in my life: my friends and family, I would like to
thank them for their unconditional support, love, and encouragement for the past six
years. Finally, I would like to thank my Heavenly Father for His always present hand in
my life; carefully leading me in directions that have ultimately placed me where I am
today.

v
CONTENT
Approval Page .................................................................................................................... iii
Acknowledgements ............................................................................................................ iv
List of Figures ................................................................................................................... vii
List of Tables ................................................................................................................... viii
List of Abbreviations ......................................................................................................... ix
Abstract .............................................................................................................................. xi
Chapter
1. Introduction ............................................................................................................. 1
Exploration of a Healthy Aging Profile: Factors that Predict
Preservation of Cognitive Functioning in Older Adults ................................... 1
Age and Cognitive Functioning .................................................................. 4
The Role of Mental Health ......................................................................... 5
The Role of Physical Health ....................................................................... 7
The Role of Life Purpose ............................................................................ 9
Other Factors to Consider ......................................................................... 10
Understanding the Relationships and Current Study ................................ 11
2. Method .................................................................................................................. 14
Participants ...................................................................................................... 14
Materials ......................................................................................................... 15
Demographic Variables ............................................................................ 15
Mental Health............................................................................................ 16
Physical Health ......................................................................................... 16
Life Purpose .............................................................................................. 17
Memory ..................................................................................................... 17
Executive Functioning .............................................................................. 18
Processing Speed ...................................................................................... 19
Statistical Analysis .......................................................................................... 20
3. Results ................................................................................................................... 24

vi
4. Discussion ............................................................................................................. 29
Non-Significant Relationships ........................................................................ 31
Limitations ...................................................................................................... 32
Future Directions and Implications ................................................................. 33
Conclusion ...................................................................................................... 35
References ......................................................................................................................... 38
Appendices
A. Spiritual Index of Well-Being Scale ................................................................. 51
B. 12-Item Short Form Health Survey ................................................................... 52

vii
FIGURES
Figures Page
1. Example of standard z-score bell-curve ................................................................ 21
2. Graphical representation of moderation effect between mental health and
life purpose on processing speed .......................................................................... 27

viii
TABLES
Tables Page
1. Correlations among mental health, physical health, and cognitive domains ........ 25
2. Summary of final regression models for variables predicting cognitive
functioning. ........................................................................................................... 28

ix
ABBREVIATIONS
ARCD Age-Related Cognitive Decline
MCI Mild Cognitive Impairment
AD Alzheimer’s Disease
ADL- Activities of Daily Living
NIH National Institutes of Health
BMI Body Mass Index
MMSE Mini Mental Status Exam
MCS Mental Health Composite Score
SF-12 12-Item Short Form Health Survey
SF-36 36-Item Health Survey
M Mean
SD Standard Deviation
PCS Physical Health Composite Score
SIWB Spiritual Index of Well-Being
RAVLT Rey Auditory Verbal Learning Test
TMT A Trails Making Test Trail A
TMT B Trails Making Test Trial B
SDMT Symbol Digit Modalities Test
DV Dependent Variable
IV Independent Variable
MLR Multiple Linear Regression
MH Mental Health

x
PH Physical Health
LP Life Purpose

xi
ABSTRACT OF THE DISSERTATION
Healthy Aging: Factors that Predict Preservation of Cognitive Functioning
in Older Adults
by
Imari-Ashley F. Palma
Doctor of Philosophy, Graduate Program in Psychology
Loma Linda University, August 2018
Dr. Adam Aréchiga, Chairperson
As the human race continues to defy chronological aging in due part to medical
advancements, an overarching goal for the older adult population and researchers is to
determine how to promote aging well. Cognitive functioning is a heavily researched area
due to the exponentially increasing number of older adults experiencing cognitive
decline. Preservation of cognitive functioning is one aspect of aging well. Three domains
of cognition that have shown to be particularly sensitive to the effects of aging are
memory, executive functioning, and processing speed. The aims of this current study are:
(i) to provide supporting evidence for research that has shown a significant relationship
between mental and physical health and cognitive functioning, (ii) to provide preliminary
evidence that shows a relationship between mental and physical health and life purpose,
and (iii) to examine the relationship between life purpose and cognitive functioning.
Participants were 220 community-dwelling healthy older adults. Results showed that life
purpose moderates the relationship between mental health and cognitive functioning,
such that those who endorsed more mental health issues performed better on tasks of
processing speed when they endorsed a higher sense of life purpose versus those who
endorsed more mental health issues and a lower sense of life purpose (p < .05). There

xii
were no other significant predictors for memory, executive functioning, or processing
speed. Future research should continue to evaluate the value life purpose has on cognitive
functioning and aging well, along with what other factors predict preservation of
cognitive functioning in order to promote living well in late life.

1
CHAPTER ONE
INTRODUCTION
Exploration of a Healthy Aging Profile: Factors that Predict Preservation of
Cognitive Functioning in Older Adults
Healthy aging can be defined in multiple ways. As the human race continues to
defy chronological aging in due part to medical advancements (Olshansky, Beard, and
Börsch-Supan, 2012), the side effects of aging also continue to increase. An overarching
goal for the older adult population and researchers is to determine how to promote aging
well. Preservation of cognitive functioning is one aspect of aging well. Cognitive
functioning is a heavily researched area due to the exponentially increasing number of
older adults experiencing cognitive decline in some facet (age-related cognitive decline,
ARCD; pre-clinical dementia; mild cognitive impairment, MCI; dementia; Alzheimer’s
Disease, AD). Functional and cognitive declines in aging are normal, and it is often
difficult to fully distinguish between preclinical dementia and normal declines due to
aging (Atkinson, and Berish, 2003; Hänninen, et al., 1996; Salthouse; Smith, 2016).
Although ARCD does not always lead to dementia, researchers have shown that early
cognitive decline places one at a significant higher risk for developing dementia (Ferri et
al., 2005; Smith, 2016).
AD is one type of dementia that continues to grow in the amount of research
devoted to better understanding the risk factors, development, prevention, and treatment
(Alzheimer’s Association, 2015). There is an estimated 5 million individuals who have
AD in America (Smith, 2016). Hebert, Weuve, Scherr, and Evans (2013) stated that those
affected by AD will likely triple by 2050 (Division of Population Health, National Center

2
for Chronic Disease Prevention and Health Promotion, 2015). Being over 65 years old
automatically places one at a greater risk for developing AD (Alzheimer’s Association,
2015), and up to 25%-50% of individuals will have developed, or will have shown signs
of, AD by age 85 years (Hebert, Scherr, Bienias, Bennett, and Evans, 2003). Heron
(2012) reported on the leading causes of death in 2009 and AD was seen to decrease by
4.2%, overall, which potentially revealed promising advancements in decreasing its
prevalence. Unfortunately, rates continue to increase, which is why researchers continue
to study the underlying mechanisms between aging and cognitive decline. While it is
important to further identify factors that lead to cognitive decline, and overall decline in
functioning due to aging, it is equally important to assess factors that can buffer against
early declines.
Researchers tend to operationalize successful aging as being free from physical
and mental illness/disability, maintenance of cognitive functioning, and or ability to stay
physically active (Atkinson et al, 2007; Balboa-Castillo, León-Muñoz, Graciana,
Rodríguez-Artalejo, and Gullar-Castillón, 2011; Barnes, Yaffe, Satariano, and Tager,
2003; Baumgart et al., 2015; Buchman et al., 2012; Cotman and Berchtold, 2002;
Daviglus et al., 2010; Ferreira, Owen, Mohan, Corbett, and Ballard, 2015; Scherder et al.,
2010). Reichstady, Sengupta, Depp, Palinkas, and Jeste (2010) conducted a qualitative
study that assessed how older adults operationalized successful aging and answered an
important question was answered: what do those, who are currently experiencing old age,
have to say about “successful aging?” These researchers found that, for these older
adults, self-acceptance and self-contentedness were the two major themes that were
associated with “successful aging.” These themes encompass ideas, such as, having a

3
sense of life purpose, connectedness with oneself and their environment, having a sense
of life satisfaction, and being content with who one’s life direction. There is not a lot of
research that has investigated the influence of these themes on aging, cognitive decline,
or cognitive preservation. There are some researchers who have assessed these themes in
terms of life meaning/purpose and how this influences mortality in aging (Boyle,
Buchman, Barnes, and Bennett, 2010; Reichstady, Sengupta, Depp, Palinkas, and Jeste,
2010; Krause, 2009), but it would be meaningful to investigate how this construct plays a
role in aging, and possibly cognitive functioning in late life.
As cognitive preservation is the outcome variable of interest in this study, it is
important to assess constructs that have been shown to reliably predict, or have
association with, cognitive decline and functioning across the lifespan. Physical health
and mental health functioning are two of these constructs. Researchers have consistently
shown that maintenance of better physical health is associated with better cognitive
functioning (Buchman et al., 2012; Erickson, Gildengers, and Butters, 2013; Scherder et
al., 2010). They have also shown support for significant mental health issues negatively
influencing cognitive functioning, and vice versa (Geeerlings et al., 2000; Jorm, 2000;
Steffens et al., 2006). How then do researchers interested in the promotion of aging well
integrate established research on the influence of physical health and mental health on
cognitive functioning and the hypothesis that aging well can be defined by having a sense
of life purpose? McKnight and Kashdan (2009) described the importance of fitting life
purpose into a coherent model on what it means to sustain health and well-being. They
described life purpose as, “a cognitive process that defines life goals and provides
personal meaning…that may help explain disparate empirical social science findings” (p.
4
242). Again, while there is more research devoted to assessment of how optimization of
mental health and physical health functioning predicts a decreased likelihood of cognitive
decline and impairment later in life, it would be meaningful to also assess how life
purpose later in life contributes to this growing body of research, as researchers have
shown its important role in aging well for older adults. Before doing so, it is important to
reiterate the relationships between the variables of interest (cognitive functioning, mental
health, physical health, and life purpose).
Age and Cognitive Functioning
Three domains of cognition that have shown to be particularly sensitive to the
effects of aging are memory, executive functioning, and processing speed. There are
various forms of memory, such as, working memory, short-term memory, and long-term
memory. Various brain regions work together to ensure proper memory functioning
including the hippocampus, amygdala, cingulate gyrus, thalamus, hypothalamus,
epithalamus, and mammillary body. All of these regions make up the limbic system,
which is in the medial temporal lobe of the brain (Erickson, Gildengers, and Butters,
2013; Mastin, 2010). Executive functioning encompasses multiple processes such as
regulatory control, working memory, reasoning, problem solving, and planning
(Salthouse, Atkinson, and Berish, 2003). It is typically associated with the prefrontal
cortex (PFC) in the frontal lobe region of the brain (Stuss and Alexander, 2000).
Cognitive processing speed is a term used to describe how efficiently one is able to
examine and complete a simple cognitive task (Deary, Johnson, and Starr, 2010).
Salthouse (1996) theorized that processing speed is the underlying, and entirely separate,

5
domain of cognitive functioning that experiences initial decline, which therefore
adversely influences other cognitive domains such as executive functioning and memory.
Processing speed has been shown to be associated with white matter of the left middle
frontal gyrus, bilateral parietal lobes, and bilateral temporal lobes. White matter fiber
tracts have been hypothesized to play an integral role in the transmission of information
and control signaling, which are necessary for efficiency in overall cognitive performance
tasks (Turken et al., 2008). While many research studies have assessed the relationship
between specific types of variables (e.g., physiological, structural, social, environmental,
psychological) and cognition, it is important to understand a person wholly and how an
individual’s different domains contribute to healthy aging and cognitive preservation.
The Role of Mental Health
The construct of mental health encompasses a variety of factors. Psychological
pathology is one aspect of poor mental health that has been continuously been linked to
acute and chronic cognitive decline and impairment in the literature (Geerlings et al.,
2000; Jorm, 2000; Starkstein, Mayberg, Leiguarda, Preziosi, and Robinson, 1992;
Steffems et al., 2006; Wilson et al., 2002). Psychological pathology can be described as
having symptoms that met criteria for any of the Diagnostic Statistical Manual, Fifth
Edition (2013) disorders. Mental health has also been interchangeably described as well-
being, quality of life, and general happiness. These terms pertaining to mental health are
operationalized in various ways in the literature. Engagement in social activities and
socialization with others is one operationalization of mental health. Researchers, in
general, have shown that regular engagement in social activity and connectedness with

6
others is associated with greater health benefits and decreased likelihood of cognitive
decline in older age (Bassuk, Glass, and Berkman, 1999; Béland, Zunzunegui, Alvarado,
Otero, and del Ser, 2005; Cracchiolo et al., 2007; Dickinson, Potter, Hybels, McQuoid,
and Steffens, 2011; Everard, Lach, Fisher, and Baum, 2000; Holahan and Holahan, 1987;
James, Wilson, Barnes, and Bennett, 2011; Kawachi and Berkman, 2001; Leung, Orrell,
and Orgeta, 2015; Yeh and Liu, 2003; Zunzunegui, Alvarado, Del Ser, and Otero, 2003).
Decreases in social engagement has been shown to be associated with worse cognitive
performance over time, which supports the notion that an enriched environment of being
surrounded by others can strengthen cognition (Small, Dixon, McArdelle, and Grimm,
2012).
Mental health has also been operationalized as subjective well-being. Research in
the area of chronic illness and palliative care has shown that higher levels of subjective
well-being is associated with higher levels of general contentedness of life and more of a
positive outlook, which does not necessarily slow down the progression of the chronic
illness or mortality, but can ameliorate the impact of the pain and or dying process
(Boyle, Buchman, Barnes, and Bennett, 2010; Krause, 2009; Reichstady, Sengupta,
Depp, Palinkas, and Jeste, 2010; Wong, 2007). The absence of chronic sadness, or having
more frequent feelings of happiness, is another definition of good mental health. Again,
research continues to provide supporting evidence for greater feelings of happiness being
linked to a myriad of positive health benefits and longevity (Crivelli, Della Bella, and
Lucchini, 2016; Post, 2005; Røysamb, Tambs, Reichborn-Kjennerud, Neale, and Harris,
2003). It is evident that good mental health later in life can benefit an individual in
multiple ways; therefore, it would be important to continue to assess how to strengthen

7
the benefits of good mental health in order to increase its efficacy on preservation of
cognitive functioning in late life.
The Role of Physical Health
Another aspect of health includes physical health. While physical health
experiences natural decline during aging, researchers continues to consistently support a
significant positive association between physical health and cognitive functioning
(Atkinson et al., 2007; Barnes, Yaffe, Satariano, and Tager, 2003; Cotman and Berchtold,
2002; Grigsby et al., 1998; Hultsch, Hammer, and Small, 1993; Hultsch, Hertzog, Small,
and Dixon, 1999). Physical health is operationalized in various ways across research
studies. Grigsby, Kaye, Baxter, Shatterly, and Hamman (1998) researched the importance
of executive functioning ability in aging individuals on activities of daily living (ADLs),
ADLs being a measure of physical health. They concluded that aging adults who had
higher performance on measures of executive functioning also scored higher on measures
of ADLs. Hultsch, Hertzog, Small, and Dixon (1999) also showed that active engagement
in various forms of ADLs buffered against cognitive decline through consistent
intellectual stimulation.
Researchers have also used self-report measures of health and level of activity to
assess the relationship between physical health and cognitive functioning. One study
found that self-reports of health and activity level were predictive of measures of
cognitive functioning in older adults, and particularly for processing speed ability
(Hultsch, Hammer, and Small, 1993). The presence or absence of physical illness is
another way physical health has been operationalized. Tilvis et al. (2004) sought out to

8
assess the predictive value of various physical health risk factors of cognitive decline.
Their results showed that “general ill health” was significantly correlated with cognitive
declines in individuals 75 years and older. Taken together, this evidence suggests that
despite the way physical health is defined, there appears to be consistent research that
supports a significant direct association with cognitive functioning in older adults.
Physical health has also been operationalized as level of fitness, or engagement in
physical activity. Engagement in leisure activities falls under a wide spectrum (e.g., low
to high levels of physical activity). As is evident, operationalizing leisure activities is
highly subjective, but studies continue to support that higher endorsed levels are
associated with higher levels of cognitive preservation (Ferreira, Owen, Mohan, Corbett,
and Ballard, 2015; Fritsch, McClendon, Smyth, Lerner, Friedland, and Larsen, 2007;
Scatmeas and Stern, 2003). Physical health can also be defined by level of fitness in older
adults such as cardiorespiratory fitness. Barnes, Yaffe, Satarino, and Tager (2003)
assessed the predictive value of baseline health on cognitive functioning in older adults.
They found that higher baseline cardiorespiratory fitness predicted maintenance of
cognitive functioning. Other researchers have more specifically defined physical health in
older adults as the efficiency of mobility. Atkinson et al. (2007) investigated the
multifaceted relationships between cognitive functioning, gait speed, and other factors of
mental health (e.g., depression). Their results showed support for cognitive decline being
predictive of a decline in gait speed. This association was reduced by depression, which
indicated a need to further understand the mechanisms and underlying relationships
between physical health and cognitive functioning in older adults.

9
The Role of Life Purpose
The role of life purpose throughout the lifespan has gained more attention in the
literature, including its effects on cognitive functioning in older adults (Lavretsky, 2010).
Life purpose has been defined and measured in various ways. Spirituality, or belief in a
higher power and structuring one’s life goals around service to, or promotion of, this
higher power is one way “life purpose” has been defined (Daaleman and Frey, 2004).
Life purpose has also been measured as an individual’s internalized belief that he or she
has the ability and resources to effectively carry out the necessary steps to obtain certain
goals (Bandura, 1993). The two aforementioned definitions of life purpose are similar. It
is helpful to look at the later as having more of an intrinsic mechanism and the former as
having more of an influence from a transcendent source. Negative perceptions about
aging, and the notion that life purpose decreases as age increases, have been shown to
have a significantly negative influence on cognitive functioning in older adults
(Robertson, King-Killimanis, and Kenny, 2016). Researchers have also shown that
increased life purpose in older adults is associated with maintenance of physical health
and decrease in mental health concerns (Holahan and Holahan, 1987; Mendes de Leon,
1996; Seeman, Unger, McAvy, and Mendes de Leon, 1999). More specific research on
cognitive functioning in older adults has shown a significant direct association between
life purpose and cognitive functioning as well (Seeman, McAvay, Merrill, Albert, and
Rodin, 1996). In addition, researchers have shown that increased levels of life purpose
may also slow down progression of cognitive decline in those developing AD (Coin et
al., 2010; Kaufman, Anaki, Binns, and Freedman, 2007).

10
It is important to continue to add to this body of research in order to better
understand the influence of life purpose. Some researchers have assessed the importance
of a positive sense of self in aging and that this helps explain better functional health in
older adults (Levy, Slade, and Kasi, 2002). Increased perceived self-efficacy and positive
attitude about aging in general can influence how one interacts with his or her
environment, which may also lower the risk of functional health decline. The
mechanisms by which these relationships operate are likely numerous; therefore, it is
important to further investigate how these factors relate to cognitive functioning, and
overall aging.
Other Factors to Consider
Research on cognitive functioning in older adults is vast and continuously
growing. The general goal for researchers is to better understand the mechanisms
underlying cognitive decline and cognitive preservation in order to better inform
interventions that help make the aging process less burdensome. The variables
aforementioned only contribute to a fraction of better understanding the mechanisms that
may help explain, or support, preservation of cognitive functioning in older adults. Other
important factors to consider when investigating cognitive functioning include level of
education and age. Researchers have found maintenance of cognitive functioning in older
adults can be predicted through age and having a higher level of education (Liévre, Alley,
and Crimmins, 2008; Yaffe et al., 2009). Increasing age, within itself, decreases an
individual’s likelihood to maintain baseline cognitive functioning later in life
(Alzheimer’s Association, 2015). Early education promotes strengthening of cognitive

11
resources during a key developmental period, which contributes to lessening the
influence of ARCD (Zahodne, Stern, and Manly, 2015). A higher level of education has
also been shown to contribute to increased cognitive reserve (León, García-García, and
Roldán-Tapia, 2016; Stern, 2002; Stern, 2003; Stern, 2009; Tucker and Stern, 2011;
Whalley, Deary, Appleton, and Starr, 2004). Cognitive reserve is related to resiliency.
The theory of cognitive reserve originated from the observation that there was a
discrepancy between brain pathology and cognitive performance in older adults (León,
García-García, and Roldán-Tapia, 2016; Stern, 2002; Stern, 2003; Stern, 2009; Tucker
and Stern, 2011; Whalley, Deary, Appleton, and Starr, 2004). There is on-going research
on further understanding what factors contribute to cognitive reserve, how to best
measure it, if it can be strengthened over time, and or if there is a pivotal time when it is
established. Cognitive reserve is made up of various factors, such as, baseline
intelligence, years of education, occupation, engagement in leisure activities (physically
and intellectually stimulating), and social involvement (Ferreira, Owen, Mohan, Corbett,
and Ballard, 2015; Scatmeas and Stern, 2003; Stern, Albert, Tang, and Tsai, 1942; León,
García-García, and Roldán-Tapia, 2016; Richards and Sacker, 2010; Zahodne, Stern, and
Manly, 2015). In other words, all of the variables of interest in this study are included
under the umbrella of cognitive reserve.
Understanding the Relationships and Current Study
The National Institute of Health (NIH) (2010) has recognized the increasing rates
of dementia and ARCD in older adults as a serious issue that needs further research to
investigate ways to help prevent or attenuate declines. Cognitive functioning is complex;

12
it encompasses attention, learning, memory, language, visuospatial skills, and executive
functioning (Daviglus et al., 2010). The 2010 NIH report on AD and ARCD synthesized
that researchers continues to show that: (1) poor health (e.g., high blood pressure,
diabetes) has been linked to cognitive decline but more well-designed studies need to be
conducted to assess other medical and health related factors; (2) there is limited and
inconsistent research findings on the associations between higher levels of social and
cognitive engagement (i.e., strengthening of mental health) in later life on cognitive
decline; and (3) the benefits of physical fitness on cognition is still in the preliminary
stages (Daviglus et al., 2010). The importance of continued investigation in this area of
research is to “bridge the gap” between research and practice, and to add another
dimension to the current research on these variables and cognition, life purpose. Small
(2016) mentioned the importance of translating what it is known about cognitive
functioning into clinical practice of detection and prevention. He emphasized the
importance of educating the community about factors that can help to buffer against
decline and ways to recognize early signs. The aims of this current study are: (i) to
provide supporting evidence for research that has shown a significant relationship
between mental and physical health and cognitive functioning, (ii) to provide preliminary
evidence that shows a relationship between mental and physical health and life purpose,
and (iii) to examine the relationship between life purpose and cognitive functioning. In
terms of directionality, it is hypothesized that:
1. Mental health and life purpose are directly correlated.
2. Physical health and life purpose are directly correlated.
3. Mental health and cognitive functioning are directly correlated.

13
4. Physical health and cognitive functioning are directly correlated.
5. Life purpose and cognitive functioning are directly correlated.
6. Less endorsement of mental health issues predicts average to high average
cognitive functioning.
7. Less endorsement of physical health issues predicts average to high average
cognitive functioning.
8. Higher levels of perceived life purpose predict average to high average cognitive
functioning.
9. Life purpose moderates the relationship between mental/physical health and
cognitive functioning, such that better perceived mental/physical health had a
much stronger effect on cognitive functioning when an individual had greater
perceived life purpose.

14
CHAPTER TWO
METHOD
Participants
Participants were 365 community-dwelling older adults who were recruited for a larger
randomized, single blind, dual center, controlled study under the direction of the Loma
Linda University Department of Nutrition. The larger study’s aim was to collect baseline
data in order to assess what impact daily ingestion of walnuts, over a two year time period,
would have on ARCD and macular degeneration in a healthy aging population. In brief,
walnuts contain long n-3 fatty-acids (LC n-3 PUFA), which have been postulated to be
integral during brain development and prevention, or slowing, of ARCD and age-related
macular degeneration (AMD). The primary aim was to investigate factors that prevent or
slow down ARCD and AMD in healthy aging adults (Sabaté and Rajaram, 2011). For the
current study, baseline data from the Loma Linda University site was used. Participants
were recruited via flyers and posters posted in geriatric clinics, site hospitals, local
churches, and community centers. Exclusion criteria included:
Illiteracy or inability to understand the protocol or undergo neuropsychological
tests.
Morbid obesity (BMI 40 kg/m2).
Uncontrolled diabetes (HbA1c >8%).
Uncontrolled hypertension (on-treatment blood pressure ≥150/100 mm Hg).
Prior cerebrovascular accident.
Any relevant psychiatric illness, including major depression.
Advanced cognitive deterioration, dementia.

15
Other neurodegenerative diseases (i.e., Parkinson’s disease).
Any chronic illness expected to shorten survival (heart failure, chronic liver disease,
kidney failure, blood disease, cancer).
Bereavement in the first year of loss.
Bad dentures unless fixable dental prostheses are used.
Allergy to walnuts.
Customary use of fish oil or flaxseed oil supplements.
Eye-related exclusion criteria.
Participants were informed about the study protocol at an initial meeting in where informed
consent was obtained, clinical history was taken, a physical examination was done, and the
Mini Mental State Examination (MMSE) was administered to screen for potential cognitive
impairment. Participants who had a MMSE score < 24 were referred to a physician and
were not eligible for participation (Sabaté and Rajaram, 2011). At baseline, there were a
total of 365 participants who met inclusion criteria, were recruited and completed all
baseline measurements and testing.
Materials
Demographic Variables
Participants completed a clinical history questionnaire at the outset of the study,
which included age (M = 69, SD = 3.17), gender (67.1% female), ethnicity (77.2%
White, 10.3% Hispanic, 6.9% Black, 4.2% Asian, 1.4% Other) and level of education in
years (M = 15.96, SD = 2.50).

16
Mental Health
The Mental Health Composite Score (MCS) subscale on the 12-Item Short Form
Health Survey (Ware, Kosinski, and Keller, 1996; SF-12) was used to measure mental
health. The SF-12 is an abbreviated version of the SF-36. Its main purpose is it to
measure multiple health dimensions (Utah Department of Health, 2001, p. 3). It has been
shown to be a reliable and valid measure of general health when assessing a large sample
(American Thoracic Society, 2007). For this study, higher scores indicate better mental
health. It has been reported that sample norms for older adults between ages 65 year –
75+ years range from 55.0 – 56.5 (Utah Department of Health, 1996). Studies have
shown that average scores on the SF-12 subscales change overtime with age and type of
population being assessed (e.g., healthy versus sick individuals, young adults versus older
adults). MCS scores have been shown to generally increase overtime (Ware, Kosinski,
and Keller, 1996; Utah Department of Health, 2001). Therefore, it is important to obtain
an overall mean for the sample under investigation in order to generate a meaningful
interpretation. Gandek et al. (1998) reported the test-retest reliability of the MCS to be
0.76 in a sample assessed in the United States. The majority of the sample for this study
was within the average ranges on the MCS (M = 56.26, SD = 5.74).
Physical Health
The Physical Composite Scores (PCS) subscale on the 12-Item Short Form Health
Survey (Ware, Kosinski, and Keller, 1996; SF-12) was used to measure physical health.
Higher scores indicate better physical health. It has been reported that sample norms for
older adults between ages 65 year – 75+ years range from 42.7 – 44.6 (Utah Department

17
of Health, 1996). PCS scores tend to decrease overtime (Ware, Kosinski, and Keller,
1996; Utah Department of Health, 2001); therefore, it is important to obtain an overall
mean for the sample under investigation in order to generate a meaningful interpretation.
Gandek et al. (1998) reported the test-retest reliability of the PCS to be 0.89 in a sample
assessed in the United States. The majority of the sample for this study was fell within
above average ranges on the PCS (M = 50.37, SD = 8.04).
Life Purpose
The Life Scheme subscale on the 12-item Spiritual Index of Well Being
(Daaleman, Cobb, and Frey, 2001; SIWB) was used to measure life purpose (see
Appendix A) It is divided into two sub-scales: self-efficacy and life-scheme. A Likert
scale ranging from one (“Strongly Agree”) to five (“Strongly Disagree”) is utilized on the
SIWB. Higher overall scores indicate higher perceived life purpose. Daaleman, Frey,
Wallance, and Studenski (2002) reported the 12-item SIWB to have a reliability of 0.80
on Life Scheme subscale. For this sample, the minimum score for Life Purpose was 16,
while the maximum score was 35 (M = 31.92, SD = 4.12).
Memory
The Rey Auditory Verbal Learning Test (RAVLT; Rey, 1941) was used to assess
memory. In this measure, a list of 15 unrelated words are repeated five times (List A).
Between each trial, the participant is asked to repeat as many words as he or she can
recall. An additional list of 15 unrelated words are read after the multiple repetition of the
original list, and the participant is asked to repeat as many words as he or she can recall

18
from this new list (List B). The participant is then asked to recall as many of the words
from the original list as he or she can without repetition from the administrator. After a
30-minute interval, the participant is asked to verbally repeat, and visually recognize, as
many words as he or she can recall from the original list once more. Psychometrically,
the RAVLT has been shown to have good validity and reliability with a Cronbach’s
Alpha coefficient of 0.80 (de Sousa Magalhães, Fernandes Malloy-Diniz, and Cavalheiro
Hamdan, 2012). The RAVLT has also been shown to be effective in early identification
of AD in individuals with subjective memory complaints, and in differentiation between
preclinical phase AD patients, MCI individuals, and normal aging individuals (Estévez-
González et al., 2003). In a healthy population between the ages of 24-81 years,
performance on the RAVLT was shown to decrease with age, but females and
participants with a higher education tended to perform better compared to males and
participants with lower education, across all age ranges (Van der Elst, van Boxtel, van
Breukelen, & Jolles, 2005). For the current study, the total scores for Trials 1-5 (M = 49,
SD = 10.10) were converted to standard z-scores using the sample mean. The Delayed
Recall scores (M = 9.87, SD = 3.35) were also converted to standard z-scores using the
sample mean. The two standard z-scores were then added and averaged to obtain the final
score used for memory (M = 0.00, SD = 1.43).
Executive Functioning
The Trails Making Test, Trail B (TMT B) and the Stroop Color Word Test
(Stroop, 1935) were combined to measure executive functioning. The TMT is a widely
used neuropsychological test of visual attention and task switching. TMT B is used as a
19
measure of executive functioning, as participants are required to organize information
efficiently and rapidly in order to complete the task successfully (Tombaugh, 2004).
Psychometrically, the TMT B has been shown to have good retest reliability for TMT B
(0.86-0.94) (Wagner, Helmreich, Dahmen, Lieb, and Tadic, 2011). The TMT has also
been shown to be negatively correlated with age and level of education (Tombaugh,
2004). The Stroop Color Word Test is a well-known and heavily used
neuropsychological test that measures cognitive interference (Scarpina and Tagini, 2017).
The construct can also measure executive functioning, as it requires the examinee to read
aloud the color a word is printed in, and inhibit themselves from reading the actual name
of the color printed (e.g., if the word “RED” is printed in the color blue, the examinee
must say, “blue”). The Stroop Color Word Test has been shown to have good test-retest
reliability at 0.86 (Siegrist, 1997). For the current study, the scores in seconds for TMT B
(M = 95.59, SD = 47.91) were converted to standard z-scores using the sample mean and
negative/positive signs were reversed via multiplication by -1 to increase meaningful and
standard interpretation. The Stroop Color Word scores, in number of correctly stated
color names (M = 34.52, SD = 8.56), were also converted to standard z-scores using the
sample mean. The two standard z-scores were then added and averaged to obtain the final
score used for executive functioning (M = 0.00, SD = 1.25).
Processing Speed
The Symbol Digit Modalities Test (SDMT; Smith, 1968; Smith 1982) and the
Trails Making Test, Trail A (TMT-A) were combined to measure cognitive processing
speed. The SDMT was developed to assess for neurological impairment. It is also widely

20
used to assess attention, visual scanning, and motor speed (Sheridan et al., 2006). The
participants are instructed that they will have 90 seconds to pair specific numbers with
given symbols (a key of which numbers match to any given symbol is listed at the top of
the page). Sheridan et al. (2006) reported this single score measure to have a test/retest
reliability and correlation with the Wechsler Digit Symbol Test, a similar measure, of .80
in a normal sample. Benedict et al. (2012) also reported the SDMT to have a test/retest
reliability of .80. The TMT is a widely used neuropsychological test of visual attention
and task switching. TMT-A can measure processing speed as it requires the examinee to
connect scattered numbers on a paper using a pencil, in consecutive order, as fast as
possible. The TMT-A has been shown to have good test-retest reliability between 0.76-
0.82 (Wanger, Helmreich, Dahmen, Lieb, and Tadíc, 2011). For the current study, the
scores in seconds for TMT-A (M = 34.09, SD = 11.77) were converted to standard z-
scores using the sample mean and negative/positive signs were reversed via
multiplication by -1 to increase meaningful and standard interpretation. The SDMT
scores, in number of correctly paired symbols to numbers (M = 47.97, SD = 9.08), were
also converted to standard z-scores using the sample mean. The two standard z-scores
were then added and averaged to obtain the final score used for processing speed (M =
0.01, SD = 1.31).
Statistical Analysis
SPSS 20.0 was used to perform all statistical analyses. The outcome variables, or
dependent variables (DVs), were combined as described above, by converting each score
in a standard z-score and taking the average of the two scores for each DV. Higher z-

21
scores, more specifically z-scores equal to or greater than -0.5, indicate average to above
average memory (see Figure 1).
Figure 1. Example of standard z-score bell-curve (Neurofeedback Center of Rochester
(2018).
Hierarchical multiple linear regression (MLR) was used to analyze the hypothesized
predictive value of the above specified IVs on the DVs. Outliers were checked for using
the calculated D-Cooks, DFBETA and DFFITS values. If any participant exceeded the
standard cut off score of 1.0 (psych.unl.edu, 2018), that participant was deleted for the
given model. In addition, participants who did not complete baseline measures for any of
the variables of interest were excluded from the study. Many participants did not
complete the SF-12 questionnaire or SIWB. After checking for outliers and including

22
only participants that completed all baseline measure of interest in this study, there were
a total of 220 participants who were included. After conducting a Power Analysis for this
sample size, the analysis showed that there was very good statistical power (α = 0.80) to
detect an anticipated effect size of 0.80 (Soper, 2018). Multicollinearity was also
checked. Nonessential multicollinearity, or high correlations between main effects and
interaction terms, can change the regression coefficients’ magnitude and sign, standard
errors can become large, and interpretation of coefficients or significance tests can
become less accurate (Morrell, 2013).
Pearson’s r correlational analyses for each model were conducted to analyze the
hypothesized correlations between variables. Three separate hierarchical MLR analyses
were conducted to investigate the three cognitive domains (memory, executive
functioning, and processing speed). Before analysis, each continuous IV was centered to
increase meaningful interpretation of results. Centering predictor variables (𝑋𝑖– 𝑋¯
) helped
to remove nonessential multicollinearity and reduce correlations among predictors.
(Morrell, 2013). It also helped to create a more meaningful interpretation. For each
model, age and years of education were entered in step one of the hierarchical MLR to
control for the effects of these covariates. Mental health, physical health, and life purpose
were entered in the second step to test for main effects. All moderating relationships
(Mental health x Life purpose, Mental health x Physical health, and Life purpose x
Physical health) were entered in step three. The first hierarchical MLR model tested the
following equation:

23
Memory = B0 + B1(Mental health) + B2(Physical health) + B3(Life purpose) +
B4(Mental health x Life purpose) + B5(Mental health x Physical health) + B6(Life
purpose x Physical health).
The second MLR model tested the following equation:
Executive functioning = B0 + B1(Mental health) + B2(Physical health) + B3(Life
purpose) + B4(Mental health x Life purpose) + B5(Mental health x Physical
health) + B6(Life purpose x Physical health).
The third MLR model tested the following equation:
Processing speed = B0 + B1(Mental health) + B2(Physical health) + B3(Life
purpose) + B4(Mental health x Life purpose) + B5(Mental health x Physical
health) + B6(Life purpose x Physical health).
24
CHAPTER THREE
RESULTS
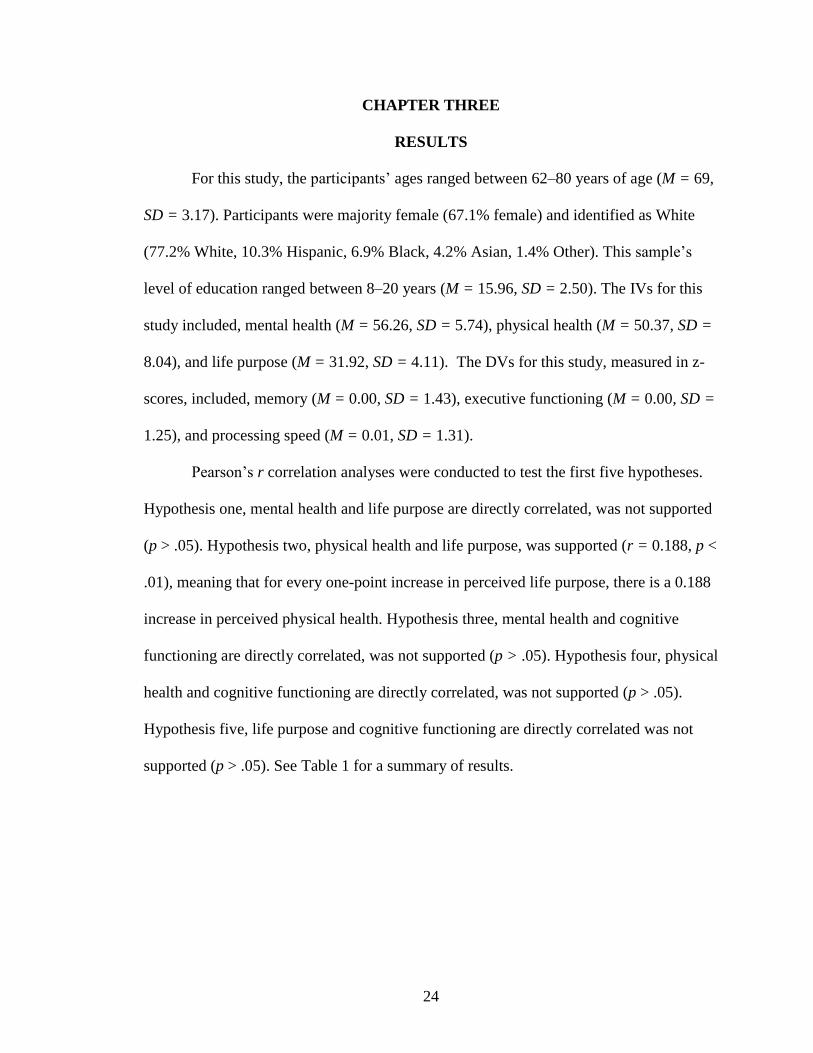
For this study, the participants’ ages ranged between 62–80 years of age (M = 69,
SD = 3.17). Participants were majority female (67.1% female) and identified as White
(77.2% White, 10.3% Hispanic, 6.9% Black, 4.2% Asian, 1.4% Other). This sample’s
level of education ranged between 8–20 years (M = 15.96, SD = 2.50). The IVs for this
study included, mental health (M = 56.26, SD = 5.74), physical health (M = 50.37, SD =
8.04), and life purpose (M = 31.92, SD = 4.11). The DVs for this study, measured in z-
scores, included, memory (M = 0.00, SD = 1.43), executive functioning (M = 0.00, SD =
1.25), and processing speed (M = 0.01, SD = 1.31).
Pearson’s r correlation analyses were conducted to test the first five hypotheses.
Hypothesis one, mental health and life purpose are directly correlated, was not supported
(p > .05). Hypothesis two, physical health and life purpose, was supported (r = 0.188, p <
.01), meaning that for every one-point increase in perceived life purpose, there is a 0.188
increase in perceived physical health. Hypothesis three, mental health and cognitive
functioning are directly correlated, was not supported (p > .05). Hypothesis four, physical
health and cognitive functioning are directly correlated, was not supported (p > .05).
Hypothesis five, life purpose and cognitive functioning are directly correlated was not
supported (p > .05). See Table 1 for a summary of results.

25
Table 1. Correlations among mental health, physical health, and cognitive domains.
1
2
3
4
5
6
M
SD
1.Memorya - .305** .281** -.019 .089 -.015 000 1.427
2. Executive functioningb - - .575** .021 .100 .082 .003 1.249
3. Processing speedc - - - .115 .021 .076 .006 1.306
4. Mental healthd
5. Physical healthe
6. Life purpose f
-
-
-
-
-
-
-
-
-
-
-
-
-.149*
-
-
-.040
.188**
-
56.26
50.37
31.92
5.742
8.043
4.106
N = 220. *p < .05. **p < .01. aMemory measured using the combined scores from the sum of trials 1-5 on the RAVLT
and RAVLT Delayed Recall. Z-score transformation was used to standardize the combined
score. bExecutive functioning measured using the combined scores from the TMT Trail B and
Digit Span on the WAIS-III. Z-score transformation was used to standardize the combined
score. cProcessing speed measured using the combined scores from the SDMT and sum of
the F, A, and S trials of the COWAT. Z-score transformation was used to standardize the
combined score. dMental health measured using the MCS subscale on the SF-12. For this study, higher
scores indicate less endorsed mental health concerns. ePhysical health measured using the PCS subscale on the SF-12. For this study, higher
scores indicate less endorsed physical health concerns. fLife purpose measured using the Life-scheme subscale on the Subjective Index of Well-
being questionnaire. For this study, higher scores indicate higher perceived life purpose.
Hierarchical MLR was used to assess hypotheses six, seven, eight, and nine: the
hypothesized main effects and moderating relationships between mental health, physical
health, and life purpose on the three domains of cognition (memory, executive
functioning, and processing speed). Hypothesis six, less endorsement of mental health
issues predicts average to high average cognitive functioning, was not supported for the
memory, executive functioning, or processing speed models (p > .05). Hypothesis seven,

26
less endorsement of physical health issues predicts average to high average cognitive
functioning, was not supported for the memory, executive functioning, or processing
speed models (p > .05). Hypothesis eight, higher levels of perceived life purpose predict
average to high average cognitive functioning, was not supported for the memory,
executive functioning, or processing speed models (p > .05). Hypothesis nine, life
purpose moderates the relationship between mental/physical health and cognitive
functioning, such that better perceived mental/physical health had a much stronger effect
on cognitive functioning when an individual had greater perceived life purpose, was
partially supported for the processing speed model. There was a significant interaction
effect between mental health and life purpose on processing speed (B = -0.011, t = -
3.069, p < .05, 95% CI [-0.018, -0.004]). The optimal linear combination of mental
health and life purpose uniquely accounted for 3.7% of the total variance in processing
speed performance (sr2 = 0.037). Processing speed performance was different at different
levels of mental health issue endorsement and perceived life purpose endorsement. In
other words, higher levels of perceived life purpose explained the relationship between
endorsement of more mental health issues and better performance on measures of
processing speed (see Figure 2).

27
Figure 2. Graphical representation of moderation effect between mental health and
life purpose on processing speed.
Hypothesis nine was not supported for the memory or executive functioning models (p >
.05). See Table 2 for a summary of all final regression models.
-15.
-10.
-5.
0.
5.
10.
15.
Less (-1 SD) More (+1 SD)
Pro
cess
ing
Sp
eed
Mental Health Issues
Less Life Purpose Endorsement (-1 SD)

28
Table 2. Summary of final regression models for variables predicting cognitive functioning.
95% Confidence
Interval for B
Model B SE B β sr2 pr2 Lower
Bound
Upper
Bound
Memorya
Mental health (MH) -.011 .017 -.044 .002 .002 -.045 .023
Physical health (PH) .014 .012 .079 .006 .005 -.011 .038
Life purpose (LP) -.018 .022 -.056 .003 .003 -.062 .026
MH x PH -.001 .002 -.046 .002 .002 -.004 .002
MH x LP .005 .004 .075 .005 .005 -.004 .013
PH x LP -.001 .002 -.049 .002 .002 -.006 .003
R2adjusted .036
F 2.036*
Executive functioningb
Mental health (MH) .004 .015 .018 ..000 .000 -,026 .033
Physical health (PH) .016 .011 .100 .009 .010 -.006 .037
Life purpose (LP) .008 .020 .029 .001 .001 -.030 .047
MH x PH -.003 .001 -.130 .015 .017 -.005 .000
MH x LP -.005 .004 -.085 .006 .007 -.012 .003
PH x LP -.001 .002 -.035 .001 .001 -.005 .003
R2adjusted
.084
F 3.512**
Processing speedc
Mental health (MH)
.027
.015
.122
.014
.016
-.002
.056
Physical health (PH) .002 .010 .013 .000 .000 -.019 .023
Life purpose (LP) .008 .019 .026 .000 .001 -.030 .045
MH x PH -.001 .001 -.035 .001 .001 -.003 .002
MH x LP -.011** .004 -.205 .037 .043 -.018 -.004
PH x LP -.003 .002 -.107 .010 .012 -.007 .001
R2adjusted .133
F 5.202***
Note. Unstandardized B values represent directionality of relationship. aMemory measured using the combined scores from the sum of trials 1-5 on the RAVLT and RAVLT
Delayed Recall. Z-score transformation was used to standardize the combined score. bExecutive functioning measured using the combined scores from the TMT Trail B and Digit Span on the
WAIS-III. Z-score transformation was used to standardize the combined score. cProcessing speed measured
using the combined scores from the SDMT and sum of the F, A, and S trials of the COWAT. Z-score
transformation was used to standardize the combined score.
*p < .05, ** p < .01; memory model (n = 205), executive functioning model (n = 207), processing speed
model (n = 207).

29
CHAPTER FOUR
DISCUSSION
Results of this study showed partial support for the outlined aims and hypotheses.
Hypothesis two, physical health and life purpose are directly correlated, was supported in
this study. There have been recent studies that have investigated the influence that an
increased sense of life purpose can have on physical health in older adults. These
researchers have highlighted the importance of assessing how psychological strengths can
act as possible aids in maintaining good physical health in late life, as opposed to
continuing to focus on how psychological distress and psychiatric disorders negatively
influence physical health in late life. These studies have shown that a higher sense of life
purpose has a relationship with improved physical functioning for older adults (Kim,
Kawachi, Chen, and Kubzansky, 2017; Ryff, 2017). These researchers have mentioned
that there may be other underlying mediating factors, such as the possibility that older
adults who have a greater sense of life purpose may have more motivation to be social,
engage in activities, and be health conscious. Still, these relationships need to be further
explored.
The hypothesis that life purpose moderates the relationship between
mental/physical health and cognitive functioning was partially supported. The moderating
effect of life purpose was only significant for the relationship between mental health and
cognitive processing speed, specifically. As stated prior, McKnight and Kashdan (2009)
endorsed the notion that life purpose is a cognitive process within itself that essentially
helps to exercise an individual’s mental toughness, ability to plan ahead, and ability to
goal set. It can be argued that regularly engaging in cognitive processes that involve

30
higher perceived life purpose can help maintain cognitive processing speed. This theory
would need to be further explored, but may help explain the significant relationship found
in this study. Boyle, Buchman, Barnes, and Bennett (2010) conducted a study to
investigate the role of life purpose on reduced risk for AD. In their longitudinal study,
they found that having a greater sense of life purpose was associated with a lower
incidence of developing AD in comparison to those individuals who developed AD, or
signs/symptoms of AD and did not have a sense of life purpose. While this association
does not necessarily indicate that life purpose will prevent the development of AD or
cognitive decline in general, it does exemplify a relationship between these two
constructs that should not be ignored. This study, conducted by
Boyle, Buchman, Barnes, and Bennett (2010), is one of the first of its kind to look at how
life purpose, a construct that is not biological, physiological, medical, or tangible, can
significantly influence something that is (i.e., cognitive decline in later life).
While all of the final models for memory performance, executive functioning
performance, and processing speed performance were significant, only about 3%, 8%,
and 13% of the variance was explained for each model. This suggests that the variables of
interest in this current study add a small percentage of meaningful predictive value to
what help preserve cognitive functioning in older age, but more research needs to be done
to investigate what other variables may contribute to preservation of cognitive
functioning in older adults. Results did show that life purpose was a significant moderator
for the relationship between mental health and life purpose for the processing speed
model, as explained above.

31
Non-Significant Relationships
As shown above, many of the hypothesized relationships were not supported. For
the majority, the literature does support the idea that better mental health and better
physical health are associated with less cognitive decline and better cognitive
performance (Baumgart et al., 2015; Buchman, Boyle, Yu, Shah, Wilson, and Bennett,
2012; Cracchiolo et al., 2007; Lautenschlager et al., 2008; Lee, 2000). It is important to
look at how mental health, physical health, and cognitive decline/performance are
defined in the literature assessing the relationships between these variables, as it can
change the interpretations and, therefore, the conceptualization of these relationships. In
terms of research in the area of mental health and cognitive functioning, there appears to
be more evidence that supports anxiety as more of a predictive factor for development of
cognitive impairment (Beaudreau and O’Hara, 2009; Mantella, 2007). In this study,
anxiety was not specifically measured. The DV, mental health, may have provided more
meaningful information if an anxiety measure was added.
Seeman, Lusignolo, Albert, and Berkman (2001) showed that, in their
longitudinal study, a high baseline of social support predicted better cognitive functioning
at the follow-up assessment. In this current study, social engagement was a small
component in how mental health was measured, but it was not particularly highlighted;
therefore, the specific influence of social engagement on cognitive performance could not
be teased apart. It could be that social support is a more meaningful variable to assess
when investigating how to preserve cognitive functioning in older adults.
For this study, how mental health and physical health were operationalized could
have been improved by utilizing more specific measures. For example, measures of

32
depression, anxiety, health-related anxiety, quality of life, ADLs, physiological
measurements that meet criteria for good health in older adults (e.g., cardiovascular
fitness, low blood pressure, healthy body mass index). Using the SF-12 may not have
been sensitive enough to detect meaningful significant relationships between health and
cognitive performance in the sample used. To reiterate, because this sample was healthier
than the general older adults population, more sensitive measures would have helped to
detect smaller but more valuable information.
Life purpose also may not have been measured in the best way possible for this
study. This study was somewhat exploratory in terms of investigating how the construct
of life purpose fits into the relationship between health and cognitive functioning in older
adults. It could be hypothesized that life purpose influences other constructs that fall
underneath the “mental health umbrella,” such as happiness, general quality of life, or
self-worth for example. Or, life purpose could be influencing other constructs, such as,
level of motivation, self-efficacy, and resiliency. In this study, a higher sense of life
purpose did explain better performance on processing speed when participants endorsed
more mental health issues, which means that the construct of life purpose could be a
meaningful variable to continue to assess in terms of how else it effects aging and
possible cognitive functioning.
Limitations
Establishing causal relationships was not possible in this study for multiple
reasons. Methodologically, cross-sectional data does not establish a pre-determined time
sequence of events, which would need to occur to confidently establish that x causes y
33
(Deary, Johnson, and Starr, 2010). Also, given the literature on mental health, psychical
health, life purpose, and cognitive functioning, including this current study, it cannot be
said that one construct causes the other, as these constricts are constantly changing for
individuals over time, across the lifespan; therefore, at any point in time, one construct
could be “causing” the other, but the reverse may be true given a different point in time.
This current study also intentionally assessed healthy older adults, which is meaningful,
but it also does not provide the opportunity to assess how these same relationships would
occur in older adults who may have had clinically significant mental health pathology,
poor physical health, and or below average cognitive functioning. Due to moderate
sample size of this study, there was a higher likelihood to detect significant effects, and
while there were more non-significant relationships, any significant relationship should
be interpreted with caution. Lastly, there may be a more comprehensive and meaningful
way to measure mental health, physical health, and life purpose. The investigator was
limited in using the measures that were used in the larger study where these variables
were collected.
Future Directions and Implications
While many of the results were shown to be non-significant, there is still
important information that can be gleaned from this study. Life purpose is a variable that
impacts cognitive functioning in older adults in some facet. While it is yet to be clear
how life purpose impacts cognitive functioning, it appears that the influence is positive,
which would mean there are meaningful possible clinical implications. For example,
therapy centered on development of life purpose could be a clinical intervention within

34
itself. This type of therapy would center on increasing self-efficacy, problem solving
ability, motivation, and short-term and long-term goal setting. It would be a strengths-
based approach to help increase life purpose and maintain mood stability. Future research
could assess the utility of this type of intervention for quality of life and cognitive
functioning in older adulthood by conducting a longitudinal controlled study. Clinical
providers who already have a part of an older adult’s care (e.g., physicians, nurses) could
also start to implement increasing the factors aforementioned that help to increase a sense
of life purpose.
Life purpose, as it relates to aging and cognitive performance in older adults, is
still not a heavily researched area. There is some promising research and theories that
suggest that an increased sense of having meaning later in life, and continuing to strive
towards goals, has the potential to increase overall quality of life and therefore the aging
process. The hope in this study was to show that an increased sense of life purpose could
also be directly and or indirectly related to actual measures of cognitive functioning in
older adults. As the results showed, there was some support for an indirect relationship.
An increased sense of life purpose appeared to help those participants who endorsed
more mental health issues perform somewhat better on measures of processing speed.
Because of the cross-sectional design of this study, the possible long-term effects
of having fairly healthy mental/physical health and higher levels of life purpose at
baseline on cognitive functioning could not be assessed. It could be hypothesized for
future studies that older adults with healthy levels of mental health, physical health, and
higher life purpose maintain their baseline cognitive performance scores, or even
improve.

35
It is also important to consider the bidirectional relationships between the DVs
within this study. In other words, without a more controlled longitudinal study design, it
is difficult to ascertain which variable is influencing the other. Because of the cross-
sectional design of this study, it is likely that mental health, physical health, and life
purpose influence each other. It would be expected that better physical health influences
better mental health, which would then influence better cognitive functioning, but based
on the literature and this study the relationships between these constructs are more
dynamic. How life purpose fits into this equation needs further investigation. It could be
hypothesized that having better mental health gives an individual enough motivation and
energy to continue to set goals in life and therefore feel a sense of life purpose, which
may influence cognitive functioning in that the mind is continuing to be cognitively
stimulated through goal setting, planning, problem solving, and new learning. As
explained prior, mental health can be defined in a variety of ways and can encompass
multiple constructs within it. While this study ensured that the variable of life purpose
was distinctly different from how mental health was measured, and results did show that
life purpose did explain the relationship between high mental health concerns and
cognitive processing speed, more research and controlled studies need to be conducted to
better understand this relationship.
Conclusion
The aims of this current study were to: (i) to provide supporting evidence for
research that has shown a significant relationship between mental and physical health and
cognitive functioning, (ii) to provide preliminary evidence that shows a relationship

36
between mental and physical health and life purpose, and (iii) to examine the relationship
between life purpose and cognitive functioning. These aims were partially reached in
that life purpose does appear to add a valuable contribution to how we understand aging
and cognition in late life. The natural decline of mental health and physical health in
older adults has been shown to impact cognition and decrease overall perceived quality of
life, which can then lead to multiple other issues that may indirectly impact overall
functioning in late life (Røysamb, Tambs, Reichborn-Kjennerud, Neale, and Harris,
2003; Strine, Chapman, Balluz, Moriart, Mokdad, 2008). As stated in the outset of this
study, the overarching goal is to increase knowledge of what it means to age well, and if
promotion of life purpose can add a positive influence on these relationships, it would be
important to then investigate how this can be applied for the older adult population.
Life purpose can be operationalized in a variety of ways, apart from how it was
defined this study. Emmons (2003) described how creating life meaning/purpose is
distinctly human characteristic, and highlighted the importance of understanding this
construct better in order to promote this throughout the lifespan in hopes of increasing
quality of life and aging well. Emmons stated that while the goal in life for many is to “be
happy,” researchers have shown that happiness is a by-product of engagement in
“worthwhile projects and activities” (p. 106) that help to create life purpose.
The aging process has historically been associated with a decline in overall
functioning, disease, and mortality. With advancements in medicine, people have been
living longer due to curing or controlling of disease for example. Unfortunately, living
longer chronological lives may include cognitive decline and a potential higher risk of
developing low perceived quality of life, as continued living in older age does not always

37
equate to living healthy or well. It is important to continue to assess what factors can help
to preserve cognitive functioning in older age. Researchers have shown that having
continued life purpose can create a domino effect of positive health and quality of life
outcomes in late life. This study also supported the potential that having a greater sense
of life purpose in late life can have on cognitive functioning and potentially overall
quality of life.

38
REFERENCES
Aiken, L. S., & West, S. G. (1991). Multiple Regression: Testing and interpreting
interactions. Thousand Oaks: Sage.
Alzheimer’s Association. (2015). What is alzheimer’s? Retrieved from
http://www.alz.org/alzheimers_disease_what_is_alzheimers.asp.
American Thoracic Society. (2008). SF-12 health survey. American Thoracic Society
Quality of Life Resources. Retrieved from
http://qol.thoracic.org/sections/instruments/pt/pages/sf12.html.
Atkinson, H. H., Rosano, C. Simonsick, E. M., Williamson, J. D., Davis, C., Ambrosius,
W. T., Rapp, S. R., Cesari, M., Newman, A. B., Harris, T. B., Rubin, S. M.,
Yaffe, K., Satterfield, S., & Kritchevsky, S. B. (2007). Cognitive function, gait
speed decline, and comorbidities: The health, aging, and body composition study.
Journal of Gerontology: Medical Sciences, 62(8), 844 – 850.
Balboa-Castillo, T, León-Muñoz, L. M., Graciana, A., Rodríguez-Artalejo, F., & Gullar-
Castillón, P. (2011). Longitudinal association of physical activity and sedentary
behavior during leisure time with health-related quality of life in community-
dwelling older adults. Health and Quality of Life Outcomes, 9(47).
doi: 10.1186/1477-7525-9-47.
Bandura, A. (1993). Perceived self0efficacy in cognitive development and functioning.
Educational Psychologist, 28(2), 117 – 148. doi: 10.1207/s15326985ep2802_3.
Barnes, D. E., Yaffe, K., Satariano, W. A., & Tager, I. B. (2003). A longitudinal study of
cardiorespiratory fitness and cognitive function in healthy older adults. Journal of
the American Geriatric Society, 51(4), 459 – 465. doi: 10.1046/j.1532-
5415.2003.51153.x.
Baumgart, M., Snyder, H. M., Carrillo, M. C., Fazio, S., Kin, H., & Johns, H. (2015).
Summary of the evidence on modifiable risk factors for cognitive decline and
dementia: A population-based perspective. Alzheimer’s & Dementia: The Journal
of the Alzheimer’s Association, 11(6), 718-726. doi: 10.1016%2Fj.jalz.2015.
Baumeister, R. F. (1991). Meanings of life. New York: Guilford Press.
Bassuk, S. S., Glass, T. A., & Berkman, L. F. (1999). Social disengagement and
incident cognitive decline in community-dwelling elderly persons. Annals of
Internal Medicine, 131(3), 165 – 173. doi: 10.7326/0003-4819-131-3-199908030-
00002.
Bates, M. E. & Labouvie, E. (2008). FAS and CFL forms of verbal fluency differ in

39
difficulty: A meta-analytic study. Applied Neuropsychology, 15(2), 87-106, 97-
106. doi: 10.1080/09084280802083863.
Beaudreau, S. A. & O’Hara, R. (2009). The association of anxiety and depressive
symptoms with cognitive performance in community-dwelling older adults.
Psychology and Aging, 24(2), 507-512.
Béland, F., Zunzunegui, M., Alvarado, B., Otero, A., & del Ser, T. (2005). Trajectories of
cognitive decline and social relations. Journal of Gerontology: Psychological
Sciences, 60(6), P320 – P330. doi: 10.1093/geronb/60.6.P320.
Benedict, R. H., Smerbeck, A., Parikh, R., Rodgers, J., Cadavid, D., & Erlanger, D.
(2012). Reliability and equivalence of alternate forms for the symbol digit
modalities test: Implications for multiple sclerosis clinical trials. Multiple
Sclerosis, 18(9), 1320-1325. doi: 10.1177/1352458511435717.
Bittner, R. M. & Crowe, S. F. (2009). The relationship between working memory,
processing speed, verbal comprehension and FAS performance following
traumatic brain injury. Brain Injury, 21(7), 709-719.
doi: 1 0.1080/02699050701468917.
Boyle, P., Buchman, A. S., Barnes, L. L., & Bennett, D. A. (2010). Effect of a purpose in
life on risk of incident Alzheimer Disease and Mild Cognitive Impairment in
community-dwelling older persons. Arch Gen Psychiatry, 63(3), 304-310. doi:
10.1001/archgenpsychiatry.2009.208
Buchman, A. S., Boyle, P. A., Yu, L., Shah, R. C., Wilson, R. S., & Bennett, D. A.
(2012). Total daily physical activity and the risk of AD and cognitive decline in
older adults. Neurology, 78(17). Doi: 10.1212/WNL.0b013e3182535d35.
Cadar, D. Stephan, C. M., Jagger, C., Johansson, B., Hofer, S. M., Piccinin, A. M., &
Muniz-Terrera. (2016). The role of cognitive reserve on terminal decline: a cross-
cohort analysis from two European studies: OCTO-Twin, Sweden, and Newcastle
85+, UK. International Journal of Geriatric Psychiatry, 31, 601 – 610. doi:
10.1002/gps.4366.
Coin, A., Perissinotto, E., Girardi, A., Inelmen, E. M., Enzi, G., Manzato, E., & Sergi, G.
(2010). Does religiosity protect against cognitive and behavioral decline in
Alzheimer’s dementia? Current Alzheimer Research, 7(5), 445 – 452. doi:
10.2174/156720510791383886.
Cotman, C. W. & Berchtold, N. C. (2002). Exercise: a behavioral intervention to enhance
brain health and plasticity. Trends in Neuroscience, 25(6), 295 – 301. doi:
10.1016/S0166-2236(02)02143-4.
Cracchiolo, J. R. Mori, T., Nazian, S. T., Tan, J., Potter, H., & Arendash, G. W. (2007).

40
Enhanced cognitive activity—over and above social or physical activity—is
required to protect Alzheimer’s mice against cognitive impairment, reduce Aβ
deposition, and increase synaptic immunoreactivity. Neurobiology of Learning
and Memory, 88(3), 277 – 294. doi: 10.1016/j.nlm.2007.07.007.
Crivelli, L., Della Bella, S., Lucchini, M. (2016). Happiness and health. In: Bruni L,
Porta P-L (Eds.), Handbook of research methods and applications in happiness
and the quality of life. Elgar, Cheltenham (pp. 372–399).
Daaleman, T. P. & Frey, B. B. (2004). The Spirituality Index of Well-Being: A new
instrument for health-related quality of life research. Annals of Family Medicine,
2, 499-503. doi: 10.1370/afm.89.
Daaleman, T. P., Frey, B. B., Wallace, D. & Studenski, S. A. (2002). The Spirituality
Index of Well-Being: Development and testing of a new measure. Journal of
Family Medicine, 51(592), 499-503.
Daaleman, T. P., Cobb, A. K., & Frey, B. B. (2001). Spirituality and well-being: an
exploratory approach to the patient perspective. Soc Sci Med, 53, 119-27.
Daviglus, M. L., Bell, C. C., Berrettini, W., Bowen, P. E., Connolly, S. Jr., Cox, J. C.,
Dunbar-Jacob, J. M., Granieri, E. C., Hunt, G., McGarry, K., Patel, D., Potosky,
A. L., Sanders-Bush, E., Silberberg, D., & Trevisan, M. (2010). National institute
of health state-of-the-science conference statement: Preventing Alzheimer disease
and cognitive decline. Annals of Internal Medicine, 153(3), 176 -181. doi:
10.7326/0003-4819-153-3-201008030-00260.
Deary, I. J., Johnson, W., & Starr, J. M. (2010). Are processing speed tasks biomarkers of
cognitive aging? Psychology and Aging, 25(1), 219-228. doi: 10.1037/a0017750.
de Sousa Magalhães, S., Fernandes Malloy-Diniz, L., & Cavalheiro Hamdan, A. (2012).
Validity convergent and reliability test-retest of the rey auditory verbal learning
test. Clinical Neuropsychiatry, 9(3), 129.
Dickinson, W. J., Potter, G. G., Hybels, C. F., McQuoid, D. R., & Steffens, D. C. (2011).
Change in stress and social support as predictors of cognitive decline in older
adults with and without depression. International Journal of Geriatric Psychiatry,
26(12), 1267 – 1274. doi: 10.1002/gps.2676.
Division of Population Health, National Center for Chronic Disease Prevention and
Health Promotion. (2015, March 5). Alzheimer’s disease. Retrieved from
http://www.cdc.gov/aging/aginginfo/alzheimers.htm.
Emmons, R. A. (2003). Personal goals, life meaning, and virtue: Wellsprings of a

41
positive life. In C. L. M. Keyes, & J. Haidt (Eds.), Flourishing: Positive
psychology and the life well-lived (pp. 105-128). Washington DC: American
Psychological Association. http://dx.doi.org/10.1037/10594-005
Erickson, K. I., Gildengers, A. G., & Butters, M. A. (2013). Physical activity and brain
plasticity in late adulthood. Dialogues in Clinical Neuroscience, 15(1), 99–108.
Estévez-González, A., Kulisevsky, J., Boltes, A., Otermín, P., & García-Sánchez, C.
(2003). Rey verbal learning test is a useful tool for differential diagnosis in the
preclinical phase of Alzheimer’s disease: comparison with mild cognitive
impairment and normal aging. International Journal of Geriatric Psychiatry,
18(11), 1021-1028.
Everard, K. M., Lach, H. W., Fisher, E. B., & Baum, M. C. (2000). Relationship of
activity and social support to the functional health of older adults. Journal of
Gerontology: Social Sciences, 55(4), S208 – S212. doi:
10.1093/geronb/55.4.S208.
Ferreira, N., Owen, A., Mohan, A., Corbett, A., & Ballard, C. (2015). Associations
between cognitively stimulating leisure activities, cognitive function and age-
related cognitive decline. International Journal of Geriatric Psychiatry, 30, 422 –
430. doi: 10.1002/gps.4155.
Ferri, C. P., Prince, M., Brayne, C., Brodaty, H., Fratiglioni, L., Ganguli, M., Hall, K.,
Hasegawa, K., Hendrie, H., Huang, Y., Jorm, A., Mathers, C., Menezes, P. R.,
Rimmer, E., & Scazufca, M. (2005). Global prevalence of dementia: a Delphi
consensus study. Lancet, 366(9503), 2112-2117.
Fritsch, T., McClendon, M. J., Smyth, K. A., Lerner, A. J., Friedland, R. P., & Larsen, J.
D. (2007). Cognitive functioning in healthy aging: The role of reserve and
lifestyle factors early in life. The Gerontologist, 47(3), 307 – 322. doi:
10.1093/geront/47.3.307.
Gandek, B., Ware, J. E., Aaronson, N. K., Apolone, G., Bjomer, J. B., Brazier, J. E.,
Bullinger, M., Kaasa, S., Leplege, A., Prieto, L., & Sullivam, M. (1998). Cross-
validation of item selection and scoring for the SF-12 Health Survey in nine
countries: results from the IQOLA Project. International Quality of Life
Assessment. Journal of Clinical Epidemiology, 51(11), 1171 – 1178.
Geerlings, M. I., Bouter, L. M., Schoevers, R. A., Beekman, A. T. F., Jonker, C., Deeg,
D., J. H., Van Tilburg, W., Adér, H. J., & Schmand, B. (2000). Depression and
risk of cognitive decline and Alzheimer’s disease: Results of two prospective
community-bases studies in the Netherlands. The British Journal of Psychiatry,
176(6), 568-575. doi: 10.1192/bjp.176.6.568.
Grigsby, J., Kaye, K., Baxter, J., Shatterly, S. M., & Hamman, R. F. (1998). Executive

42
cognitive abilities and functional status among community dwelling older persons
in the San Luis Valley health and aging study. Journal of the American Geriatric
Society, 46(5), 590 – 596. doi: 10.1111/j.1532-5415.1998.tb01075.x.
Hänninen, T., Koivisto, K., Reinikainen, K. J., Helkala, E., Soininen, H., Mykkänen, L.,
Laakso, M., & Riekkinen, P. J. (1996). Prevelence of ageing-associated cognitive
decline in an elderly population. Age and Ageing, 25(3), 201 – 205. doi:
10.1093/ageing/25.3.201.
Hebert, L. E., Scherr, P. A., Bienias, J. L., Bennett, D. A., & Evans, D. A. (2003).
Alzheimer disease in the US population: prevalence estimates using the 2000
census. Archives of Neurology, 60(8), 1119-1122.
Heron, M. (2012). Deaths: Leading causes for 2009. National Vital Statistics Reports,
61(7), 1-95.
Hindle, J. V., Hurt, C. S., Burn, D. J., Brown, R. G., Samuel, M., Wilson, K. C., & Clare,
L. (2016). The effects of cognitive reserve and lifestyle on cognition and dementia
in Parkinson’s disease – a longitudinal cohort study. Geriatric Psychiatry, 31(1),
13 – 23. doi: 10.1002/gps.4284.
Holahan, C. K. & Holahan, C. J. (1987). Self-efficacy, social support, and depression in
aging: a longitudinal analysis. Journal of Gerontology, 42(1), 65 – 68.
doi: 10.1093/geronj/42.1.65.
Hultsch, D. F., Hammer, M., & Small, B. J. (1993). Age differences in cognitive
performance in later life: Relationships to self-reported health and activity life
style. Journal of Gerontology, 48(1), P1 – P11. doi: 10.1093/geronj/48.1.P1.
Hultsch, D. F., Hertzog, C., Small, B. J. & Dixon, R. A. (1999). Use it or lose it: Engaged
lifestyle as a buffer of cognitive decline in aging? Psychology and Aging, 14(2),
245-263. doi: 10.1037/0882-7974.14.2.245.
James, B. D., Wilson, R. S., Barnes, L. L., & Bennett, D. A. (2011). Late-life social
activity and cognitive decline in old age. Journal of the International
Neuropsychological Society, 17(6), 998-1005. doi: 10.1017/S1355617711000531.
Jorm, A. F. (2000). Is depression a risk factor for dementia or cognitive decline?
Gerontology, 46(4), 2190227. doi: 10.1159/000022163.
Kaufman, Y., Anaki, D., Binns, M., & Freedman, M. (2007). Cognitive decline in
Alzheimer disease: Impact of spirituality, religiosity, and QOL. Neurology,
68(18), 1509 – 1514. doi: 10.1212/01.wnl.0000260697.66617.59.
Kawachi, I. & Berkman, L. F. (2001). Social ties and mental health. Journal of Urban
Health, 78, 458. doi:10.1093/jurban/78.3.458.

43
Keyes, C. L. M. (1998). Social well-being. Social Psychology Quarterly, 61, 121–140.
Kim, E. S., Sun, J. K., & Peterson, C. (2013). Purpose in life and reduced incidence of
stroke in older adults: ‘The health and retirement study.’ Journal of
Psychosomatic Research, 74(5), 427-432.
doi: 10.1016/j.psychores.2013.01.013.
Kline, R. B. (1998). Principles and practices of structural equation modeling. New York,
NY: Guilford Press.
Krause, N. (2009). Meaning in life and mortality. The Journals of Gerontology, 64B(4),
517-527. doi: 10.1093/geronb/gbp047.
Lautenschlager, N. T., Cox, K. L., Flicker, L., Foster, J. K., van Bockxmeer, F. M., Xiao,
J., Greenop, K. R., & Almeida, O. P. (2008). Effect of physical activity on
cognitive function in older adults at risk for Alzheimer Disease. JAMA, 300(9),
1027-1037. doi: 10.1001/jama.300.9.1027.
Lavretsky, H. (2010). Spirituality and aging. Aging Health, 6(6), 749 – 769. doi:
10.2217/ahe.10.70.
Lee, Y. (2000). The predictive value of self assessed general, physical, and mental health
on functional decline and mortality in older adults. Journal of Epidemiology &
Community Health, 54, 123-129.
León, I., García-García, J., & Roldán-Tapia, L. (2014). Estimating cognitive reserve in
health adults using the cognitive reserve scale. PLoS One, 9(7), e102632. doi:
10.1371/journal.pone.0102632.
León, I., García-García, J., & Roldán-Tapia, L. (2016). Cognitive reserve and ageing.
Anales de Psicología, 32(1), 218 – 223. doi: 10.6018/analesps.32.1.182331.
Leung, P., Orrell, M., & Orgeta, V. (2015). Social support group interventions in people
with dementia and mild cognitive impairment: a systematic review of the
literature. International Journal of Geriatric Psychiatry, 30(1), 1 – 9. doi:
10.1002/gps.4166.
Levy, B., R., Slade, M. D., & Kasi, S. V. (2002). Longitudinal benefit of positive self-
perceptions of aging on functional health. Journal of Gerontology: Psychosocial
Sciences, 57(5), P409 – P417. doi: 10.1093/geronb/57.5.P409.
Liévre, A., Alley, D., & Crimmins, E. M. (2008). Educational differential in life
expectancy with cognitive impairment among the elderly in the United States.
Journal of Aging and Health, 20(4). doi: 10.1177/089826430831557.
Lockwood, K. A., Alexopoulos, G. S., van Gorp, W. (2002). Executive dysfunction in

44
geriatric depression. The American Journal of Psychiatry, 159(7), 1119-1126. doi:
10.1176.appi.ajp.159.7.1119.
Mantella, R. C., Butters, M. A., Dew, M. A., Mulsant, B. H., Begley, A. E., Tracey, B.,
Shear, M. K., Reynolds, C. F. III, & Lenze, E. J. (2007). Cognitive impairment in
late-life generalized anxiety disorder. Psychiatry, 15(8), 673-679. doi:
10.1097/JGP.0b013e31803111f2.
Mastin, L. (2010). Parts of the brain. The Human Memory. Retrieved from
http://www.human-memory.net/brain_parts.html.
McKnight, P. E. & Kashdan, T. B. (2009). Purpose in life a sa system that creates and
sustains health and well-being: An integrative, testable theory. American
Psychological Association, 13(3), 242-251. doi: 10.1037/a0017152.
Morrell, H. M. (2013). Path analysis. [PowerPoint slides]. Retrieved from
https://llu.instructure.com/.
Niolon, R. [Web article post]. (2005, August 24). Introduction to the WAIS-III.
Retrieved February 28, 2018 from
http://www.psychpage.com/learning/library/intell/wais_history.html.
Nucci, M., Mapelli, D., & Mondini, S. (2012). Cognitive Reserve Index questionnaire
(CRIq): a new instrument for measuring cognitive reserve. Aging Clinical and
Experimental Research, 24(3), 218 – 226. doi: 10.3275/7800.
Neurofeedback Center of Rochester. (2018). [Web article post]. What is z-score
training? Retrieved on March 5, 2018 from
http://neurofeedbackcenterofrochester.com/what-is-z-score-training/.
Nygren, B., Jonsén, L. A., Gustafson, Y., Norberg, A., & Lundman, B. (2010).
Resilience, sense of coherence, purpose in life and self-transcendence in relation
to perceived physical and mental health among the oldest old. Aging & Mental
Health, 9(4), 354-362. doi: 10.1080/1360500114415.
Olshansky, S. J., Beard, J., & Börsch-Supan, A. (2012). Pursuing health ageing: What
healthy ageing involves. The longevity dividend: Health as an investment. In J.
Beard, S. Biggs, D. Bloo,, L. Fried, P. Hogan, A. Kalache, & J. Olshansky (Eds.),
Global population ageing: Peril or promise? (pp. 57-60). Retrieved on March 5,
2018 from the Program on the Global Demography of Aging Working Paper No.
89 http://www.hsph.harvard.edu/pgda/working.htm.
Patterson, J. (2011). F-A-S Test. In: Kreutzer J.S., DeLuca J., Caplan B. (Eds)
Encyclopedia of Clinical Neuropsychology. Springer, New York, NY.
doi: 10.1007/978-0-387-79948-3_886.
Post, S. G. (2005). Alturism, happiness, and health: it’s good to be good.

45
International Journal of Behavioral Medicine, 12(2), 66-77. doi:
10.1207/s15327558ijbm12024.
Reichstady, J., Sengupta, G., Depp, C. A., Palinkas, L. A., & Jeste, D. V. (2010). Older
adults’perspectives on successful aging: Qualitative interview. The American
Journal of Geriatric Psychiatry, 18(7), 567-575.
doi: 10.1097/JGP.0b013e3181e040bb.
Richards, M. & Sacker, A. (2010). Lifetime antecedents of cognitive reserve. Journal or
Clinical and Experimental Neuropsychology, 25(5), 614 – 624.
doi: 10.1076/jcen.25.5.614.14581.
Robertson, D. A., King-Killimanis, B. L., & Kenny, R. A. (2016). Negative perceptions
of aging predict longitudinal decline in cognitive function. Psychology and Aging,
31(1), 71 – 81. doi: 10.1037/pag0000061.supp.
Rockefeller College University at Albany. [Web PDF post]. (2007, September 4). Outlier
and DFBETA. Retrieved February 29, 2018 from
https://www.albany.edu/faculty/kretheme/PAD705/SupportMat/DFBETA.pdf.
Ross, T. O., Calhoun, E., Cox, T., Wenner, C., Kono, W., & Pleasant, M. (2007). The
reliability and validity of qualitative scores for the Controlled Oral Word
Association Test. Archives of Clinical Neuropsychology, 22(4), 475-488.
doi: 10.1016/j.acn.2007.01.026.
Røysamb, E., Tambs, K., Reichborn-Kjennerud, T., Neale, M. C., & Harris, J. R. (2003).
Happiness and health: Environmental and genetic contributions to the relationship
between subjective well-being, perceived health, and somatic Illness. Journal of
Personality and Social Psychology, 85(6), 1136-1146.
doi: 10.1037/0022-3514.85.6.1136.
Ryff, C. D. (2017). The benefits of purposeful life engagement on later-life physical
function. JAMA Psychiatry, 74(10), 1046-1046.
doi: 10.1001/jamapsychiatry.2017.2136.
Sabaté, J., & Rajaram, S. (2011). Effects of daily ingestion of walnuts for 2 years on age-
related cognitive decline and macular degeneration in healthy elderly subjects: A
randomized, single blind, dual center, controlled trial (Unpublished research
grant proposal). Loma Linda University, Loma Linda, CA, USA.
Salthouse, T. A. (1996). The processing-speed theory of adult age differences in
cognition. Psychological Review, 103(3), 403-428. doi: 10.1037/0033-
295X.103.3.403
Salthouse, T. A., Atkinson, T. M., & Berish, D. E. (2003). Executive functioning as a

46
potential mediator of age-related cognitive decline in normal adults. Journal of
Experimental Psychology: General, Vol 132(4), 566-594. doi: 10.1037/0096-
3445.132.4.566.
Scarpina, F. & Tagini, S. (2017). The Stroop color and word test. Frontiers in
Psychology, 8, 557. Htto://doi.org/10.3389/fpsyg.2017.00557.
Scatmeas, N. & Stern, Y. (2003). Cognitive reserve and lifestyle. Journal of Clinical and
Experimental Neuropsychology, 25(5), 625 – 633.
doi: 10.1076/jcen.25.5.625.14576.
Scherder, E. J. A., Van Paasschen, J., Deijen, J.-B., Van Der Knokke, S., Orlebeke, J. F
K., Burgers, I., Devriese, P.-P., Swaab, D. F., & Sergeant, J. A. (2010). Physical
activity and executive functions in the elderly with mild cognitive impairment.
Aging & Mental Health, 9(3), 272-280. doi: 10.1080/13607860500089930.
Seeman, M. (1991). Alienation and anomie. In J. P. Robinson, & P. R. Shaver (Eds.),
Measures of personality and social psychological attitudes (pp. 291–371). San
Diego, CA: Academic Press.
Seeman, T., McAvay, G., Merrill, S., Albert, M., & Rodin, J. (1996). Self-efficacy beliefs
and change in cognitive performance: MacArthur studies on successful aging.
Psychology and Aging, 11(3), 538 – 551. doi: 10.1037/0882-7974.11.3.538.
Seeman, T. E., Unger, J. B., McAvy, G., & Mendes de Leon, C. F. (1999). Self-efficacy
beliefs and perceived declines in functional ability: MacArthur studies of
successful aging. Journal of Gerontology: Psychological Sciences, 54B(4),
P214 – P222. doi: 10.1093/geronb/54B.4.P214.
Sheridan, L. K., Fitzgerald, H. E., Adams, K. M., Nigg, J. T., Martel, M. M., Puttler, L.
I., Wong, M. M., & Zucker, R. A. (2006). Normative symbol digit modalities test
performance in a community-based sample. Archives of Clinical
Neuropsychology, 21(1), 23-28. doi: 10.1016/j.acn.2005.07.003.
Siegrist, M. (1995). Effects of taboo words on color-naming performance on a stroop test.
Perceptual and Motor Skills, 81(2 Pt 2), 1119-1122.
doi: 10.2466/pms.1995.81.3f.1119.
Singh-Manoux, A., Marmot, M. G., Glymour, M., Sabia, S., Kivimäki, M., Dugravot, A.
(2011). Does cognitive reserve shape cognitive decline? Annals of Neurology,
70(2), 296 – 304. doi: 10.1002/ana.22391.
Small, B. J., Dixon, R. A. McArdelle, J. J., & Grimm, K. J. (2012). Do changes in
lifestyle engagement moderate cognitive decline in normal aging? Evidence from
the Victoria Longitudinal Study. Neuropsychology, 26(2), 144 – 155. doi:
10.1037/a0026579.

47
Small, G. W. (2016). Detection and prevention of cognitive decline. American Journal of
Geriatric Psychiatry. Advance online publication.
doi: 10.1016/j.jagp.2016.08.013.
Smith, G. E. (2016). Healthy cognitive aging and dementia prevention. American
Psychologist, 71(4), 268 – 275. doi: 10.1037/a0040250.
Soper, D. (2018). A-priori sample size calculator for multiple regression. Retrieved from
https://www.danielsoper.com/statcalc/calculator.
Sumowski, J. F., Rocca, M. A., Leavitt, V. M., Dackovic, J., Mesaros, S., Drulovic, J.,
DeLuca, J., & Fillippi, M. (2014). Brain reserve and cognitive reserve protect
against cognitive decline over 4.5 years in MS. Neurology, 82(20), 1776 – 1783.
doi: 10.1212/WNL.0000000000000433.
Starkstein, S. E., Mayberg, H. S., Leiguarda, R., Preziosi, T. J., & Robinson, R. G.
(1992). A prospective longitudinal study of depression, cognitive decline, and
physical impairments in patients with Parkinson's disease. Journal of Neurology,
Neurosurgey & Psychiatry, 55, 377-382. doi: 10.1136/jnnp.55.5.377.
Steffens, D. C., Otey, E., Alexopoulos, G. S., Meryl A. Butters, M. A., Cuthbert, B.,
Ganguli, M., Geda, Y. E., Hendrie, H. C., Krishnan, R. R., Kumar, A., Lopez, O.
L., Lyketsos, C. G., Mast, B. T., Morris, J. C., Norton, M. C., Peavy, G. M.,
Petersen, R. C., Reynolds, C. F., Salloway, S., Welsh-Bohmer, K. A., &
Yesavage, J. (2006). Perspectives on depression, mild-cognitive impairment, and
cognitive decline. Archives of General Psychiatry, 63(2), 130-139.
doi: 10.1001/archpsyc.63.2.130.
Stern, Y. (2002). What is cognitive reserve? Theory and research application of the
reserve concept. Journal of the International Neuropsychological Society, 8(3),
448 – 460. doi: 10.1017/S1355617702813248.
Stern, Y. (2003). The concept of cognitive reserve: A catalyst for research. Journal of
Clinical and Experimental Neuropsychology, 25(5), 589 – 593. doi:
10.1076/jcen.25.5.589.14571.
Stern, Y. (2009). Cognitive reserve. Neuropsychologia, 47(10), 2015 – 2028.
doi:10.1016/j.neuropsychologia.2009.03.004.
Stern, Y., Albert, S., Tang, M., & Tsai, W. (1942). Rate of memory decline in AD is
related to education and occupation. Neurology, 53(9), 1526 – 632X. doi: 10.
1212/WNL.53.9.1942.
Strine, T. W., Chapman, D. P., Balluz, L. S., Moriart, D. G., & Mokdad, A. H. (2008).

48
The associations between life satisfaction and health-related quality of life,
chronic illness, and health behaviors among U.S. community-dwelling adults.
Journal of Community Health, 33(1), 40-50. doi: 10.1007/s10900-007-9066-4.
Stroop, J. R. (1935). Studies of interference in serial verbal reactions. Journal of
Experimental Psychology, 18, 643-662.
Stuss, D. T., & Alexander, M. P. (2000). Executive functions and the frontal lobes: a
conceptual view. Psychological Research, 63(3), 289-298.
doi: 10.1007/s004269900007.
Tilvis, R. S., Kähönen-Väre, M. H., Jolkkonen, J., Valvanne, J., Pitkala, K. H., &
Strandberg, T. E. (2004). Predictors of cognitive decline and mortality of aged
people over a 10-year period. Journal of Gerontology: Medical Sciences, 59(3),
M268 – M274. doi: 10.1093/gerona/59.3.M268.
Tombaugh, T.N.T.N. (2004). Trail Making test A and B: Normative data stratified by age
and education. Archives of Clinical Neuropsychology : The Official Journal of the
National Academy of Neuropsychologists, 19(2), 203–214. doi:10.1016/s0887-
6177(03)00039-8.
Tucker, A. M. & Stern, Y. (2011). Cognitive reserve in aging. Current Alzheimer
Research, 8(3), 1 – 7.
Turken, A. U., Whitfield-Gabrieli, S., Bammer, R., Baldo, J., Dronkers, N. F., &
Gabrieli, J. D. E. (2008). Cognitive processing speed and the structure of white
matter pathways: Convergent evidence from normal variation and lesion studies.
Neuroimage, 42(2), 1032-1044. doi: 10.1016/j.neuroimage.2008.03.057.
University of Nebraska Lincoln [Web PDF post]. (2007, July 24). Multiple regression
diagnostics. Retrieved February 28, 2018 from
http://psych.unl.edu/psycrs/statpage/regdiag_eg.pdf.
Utah Department of Health (2001). Interpreting the SF-12. Utah Health Status Survey.
Retrieved from
http://health.utah.gov/opha/publications/2001hss/sf12/SF12_Interpreting.pdf.
Van der Elst, W., van Boxtel, M. P., van Breukelen, G. J., & Jolles, J. (2005). Rey's
verbal learning test: normative data for 1855 healthy participants aged 24-81
years and the influence of age, sex, education, and mode of presentation. Journal
of the International Neuropsychological Society, 11(3), 290-302.
Wagner, S., Helmreich, I., Dahmen, N., Lieb, K., & Tadic, A. (2011). Reliability of three
alternative forms of the trail making tests a and b. Archives of Clinical
Neuropsychology: The Official Journal of the National Academy of
Neuropsychologists, 26)4), 314-321. doi: 10.1093/arclin/acr024.

49
Walker, L. A. S., Cheng, A., Beard, J., Berrigan, L. I., Rees, L. M., & Freedman, M. S.
(2012). Tests of information processing speed. International Journal of Multiple
Sclerosis Care, 14(2), 92-99. doi: 10.7224/1537-2073-14.2.92.
Ware, J. J., Kosinski, M., & Keller, S. D. (1996). A 12-Item Short-Form Health Survey:
construction of scales and preliminary tests of reliability and validity. Medical
Care, 34(3), 220 – 233.
Whalley, L. J., Deary, I. J., Appleton, C. L., & Starr, J. M. (2004). Cognitive reserve and
the neurobiology of cognitive aging. Ageing Research Reviews, 3(4), 369 – 382.
doi: 10.1016/j.arr.2004.05.001.
Wilson, R. S., Barnes, L. L., Mendes de Leon, C. F., Aggarwal, N. T., Schneider, J. S.,
Bach, J., Pilat, J., Beckett, L. A., Arnold, S. E., Evans, D. A., & Bennett, D. A.
(2002). Depressive symptoms, cognitive decline, and risk of AD in older persons.
Neurology, 59(3). doi: 10.1212/WNL.59.3.364.
Wong, P. T. P. (2007). [Web article post]. Meaning of life and meaning of death in
successful aging. Retrieved on March 5, 2018 from the International Network of
Personal Meaning at http://www.meaning.ca/archives/archive/art_successful-
aging_P_Wong.htm.
Wongpakaran, T., Wongpakaran, N., & Ruktrakul, R. (2011). Reliability and validity of
the multidimensional scale of perceived social support (MSPSS): Thai version.
Clinical Practice & Epidemiology in Mental Health, 12(7), 161 – 166.
doi: 10.2174/1745017901107010161.
Yaffe, K., Fiocco, A. J., Lindquist, K., Vittinghoff, E., Simonsick, M., Newman, A. B.,
Satterfield, S., Rosano, C., Rubin, S. M., Ayonayon, H. N., Harris, T. B., & For
the Health ABC Study. (2009). Predictors of maintaining cognitive function in
older adults. American Academy of Neurology, 72(23). Doi:
10.1212/WNL.0b013e3181a92c36.
Yeh, S. J. & Liu, Y. (2003). Influence of social support on cognitive function in the
elderly. BMC Health Services Research, 3(9), 1 – 9. doi: 10.1186/1472-6963-3-9.
Zahodne, L. B., Stern, Y., & Manly. (2015). Differing effects of education on cognitive
decline in diverse elders with low versus high educational attainment.
Neuropsychology, 29(4), 649 – 657. doi: 10.1037/neu0000141.
Zhu, J., Tulsky, D. S., Price, L., & Chen, H.-Y. (2001). WAIS-III reliability data for
clinical groups. Journal of the International Neuropsychological Society, 7,
8620866.
Zimet, G. D., Dahlem, N. W., Zimet, S. G. & Farley, G. K. (1988). The Multidimensional
Scale of Perceived Social Support. Journal of Personality Assessment, 52, 30-41.
50
Zunzunegui, M., Alvarado, B. E., Del Ser, T., & Otero, A. (2003). Social networks,
social integration, and social engagement determine cognitive decline in
community-dwelling Spanish older adults. Journal of Gerontology: Social
Sciences, 58(2), S93 – S100.
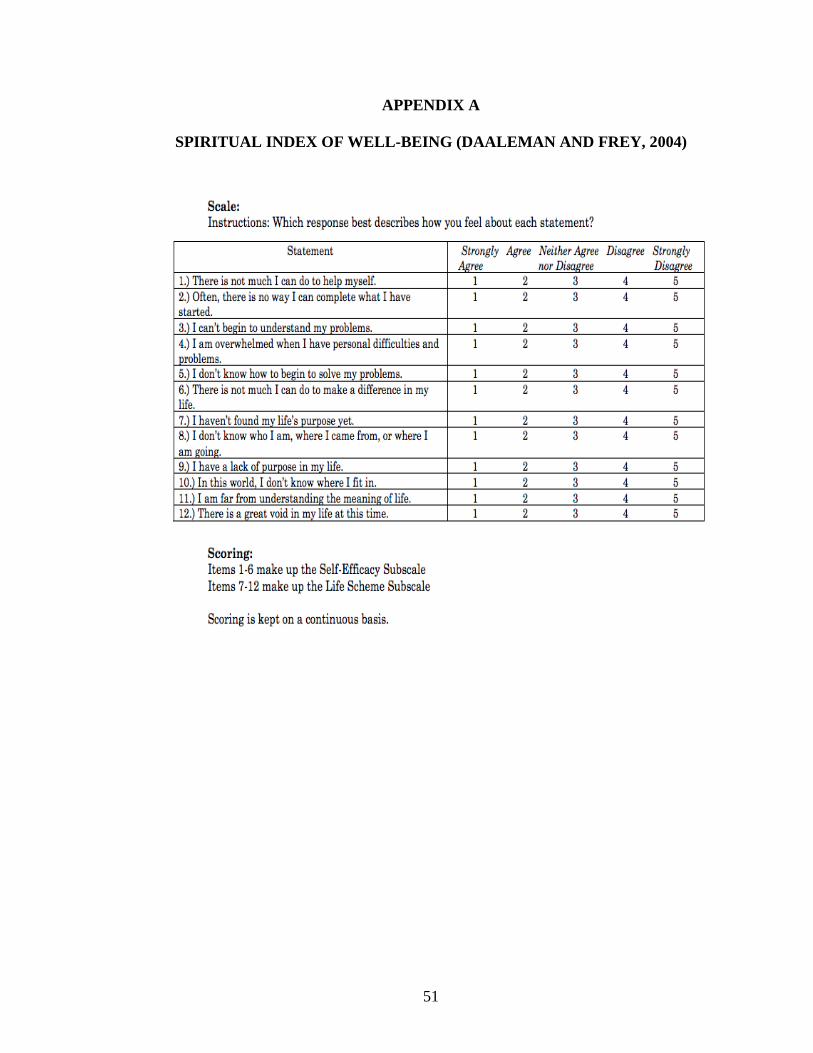
51
APPENDIX A
SPIRITUAL INDEX OF WELL-BEING (DAALEMAN AND FREY, 2004)

52
APPENDIX B
12-ITEM SHORT FORM HEALTH SURVEY (WARE, KOSINSKI, AND
KELLER, 1996; SF-12)