heart failure - homepage |...
TRANSCRIPT

Heart Failure
Improving Evidence-Based Care for Heart Failure inOutpatient Cardiology Practices
Primary Results of the Registry to Improve the Use of Evidence-BasedHeart Failure Therapies in the Outpatient Setting (IMPROVE HF)
Gregg C. Fonarow, MD; Nancy M. Albert, PhD, RN; Anne B. Curtis, MD; Wendy Gattis Stough, PharmD;Mihai Gheorghiade, MD; J. Thomas Heywood, MD; Mark L. McBride, PhD; Patches Johnson Inge, PhD;
Mandeep R. Mehra, MD; Christopher M. O’Connor, MD; Dwight Reynolds, MD;Mary Norine Walsh, MD; Clyde W. Yancy, MD
Background—A treatment gap exists between heart failure (HF) guidelines and the clinical care of patients. The Registryto Improve the Use of Evidence-Based Heart Failure Therapies in the Outpatient Setting (IMPROVE HF) prospectivelytested a multidimensional practice-specific performance improvement intervention on the use of guideline-recommended therapies for HF in outpatient cardiology practices.
Methods and Results—Performance data were collected in a random sample of HF patients from 167 US outpatientcardiology practices at baseline, longitudinally after intervention at 12 and 24 months, and in single-point-in-time patientcohorts at 6 and 18 months. Participants included 34 810 patients with reduced left ventricular ejection fraction (�35%)and chronic HF or previous myocardial infarction. To quantify guideline adherence, 7 quality measures were assessed.Interventions included clinical decision support tools, structured improvement strategies, and chart audits with feedback.The performance improvement intervention resulted in significant improvements in 5 of 7 quality measures at the24-month assessment compared with baseline: �-blocker (92.2% versus 86.0%, �6.2%), aldosterone antagonist (60.3%versus 34.5%, �25.1%), cardiac resynchronization therapy (66.3% versus 37.2%, �29.9%), implantable cardioverter-defibrillator (77.5% versus 50.1%, �27.4%), and HF education (72.1% versus 59.5%, �12.6%) (each P�0.001). Therewere no statistically significant improvements in angiotensin-converting enzyme inhibitor/angiotensin receptor blockeruse or anticoagulation for atrial fibrillation. Sensitivity analyses at the patient level and limited to patients with bothbaseline and 24-month quality measure data yielded similar results. Improvements in the single-point-in-time cohortswere smaller, and there were no concurrent control practices.
Conclusions—The Registry to Improve the Use of Evidence-Based Heart Failure Therapies in the Outpatient Setting, a definedand scalable practice-specific performance improvement intervention, was associated with substantial improvements in theuse of guideline-recommended therapies in eligible patients with HF in outpatient cardiology practices.
Clinical Trial Registration—URL: http://www.clinicaltrials.gov. Unique identifier: NCT00303979.(Circulation. 2010;122:585-596.)
Key Words: guidelines � heart failure � outpatients � quality of health care
Heart failure (HF) is a chronic progressive disease thatresults in substantial morbidity, mortality, and expendi-
ture of healthcare resources.1,2 Clinical trials have establishedthat a number of therapies may improve clinical outcomes for
patients with HF and reduced left ventricular ejection fraction(LVEF).2 Despite extensive clinical trial evidence and rec-ommendations in national guidelines, prior studies havedemonstrated that treatment guidelines are adopted slowly,
Received December 23, 2009; accepted June 1, 2010.From the Department of Medicine, Ahmanson–UCLA Cardiomyopathy Center, UCLA Medical Center, Los Angeles, Calif (G.C.F.); Nursing Institute
and George M. and Linda H. Kaufman Center for Heart Failure, Cleveland Clinic Foundation, Cleveland, Ohio (N.M.A.); Division of Cardiology,University of South Florida College of Medicine, Tampa (A.B.C.); Department of Clinical Research, Campbell University School of Pharmacy, ResearchTriangle Park, and Department of Medicine, Duke University Medical Center, Durham, NC (W.G.S.); Division of Cardiology, Northwestern University,Center for Cardiovascular Quality and Outcomes, Chicago, Ill (M.G.); Division of Cardiology, Scripps Clinic, La Jolla, Calif (J.T.H.); Outcome SciencesInc, Cambridge, Mass (M.L.M., P.J.I.); Division of Cardiology, University of Maryland, Baltimore (M.R.M.); Division of Cardiology, Duke UniversityMedical Center, Durham, NC (C.M.O.); Cardiovascular Section, University of Oklahoma Health Sciences Center, Oklahoma City (D.R.); The Care GroupLLC, Indianapolis, Ind (M.N.W.); and Baylor Heart and Vascular Institute, Baylor University Medical Center, Dallas, Tex (C.W.Y.).
The online-only Data Supplement is available with this article at http://circ.ahajournals.org/cgi/content/full/CIRCULATIONAHA.109.934471/DC1.Correspondence to Gregg C. Fonarow, MD, Ahmanson–UCLA Cardiomyopathy Center, Ronald Reagan UCLA Medical Center, 10833 LeConte Ave,
Room A2–237 CHS, Los Angeles, CA 90095-1679. E-mail [email protected]© 2010 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.109.934471
585
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

are applied inconsistently, and thus often fail to lead toimprovements in patient care quality and outcomes.3–9 Forhospitalized HF patients and outpatients, gaps, variations,and disparities between evidence-based guideline recom-mendations and actual treatments provided have beendocumented.3–9 New, more effective approaches to improvethe use of evidence-based, guideline-recommended therapiesfor HF are needed for each healthcare setting in which thesepatients are encountered.
Editorial see p 561Clinical Perspective on p 596
Various strategies have been recommended to facilitateimplementation of practice guidelines, including the use ofperformance measures based on practice guidelines, chartaudits with feedback of results, reminder systems (includingpathways and tools), and educational outreach visits.2 Al-though certain hospital-based performance improvement pro-grams deploying these strategies have been successful inimproving the quality of care,10,11 improvement in the deliv-ery of evidence-based care in the outpatient practice settingthrough the use of a targeted and scalable performanceimprovement initiative has not been tested.12 Building onfeatures of previous hospital-based programs, the aim of theRegistry to Improve the Use of Evidence-Based Heart FailureTherapies in the Outpatient Setting (IMPROVE HF) was tofacilitate more consistent delivery of evidenced-based,guideline-recommended care to eligible patients with HF andreduced LVEF or previous myocardial infarction (MI) andreduced LVEF in the outpatient cardiology practice setting byproviding performance data feedback and a practice-specificperformance improvement intervention.12
MethodsIMPROVE HF is a prospective study designed to evaluate theeffectiveness of a practice-specific performance improvement inter-vention on the use of guideline-recommended therapies for patientswith diagnosed HF and reduced LVEF or prior MI and reducedLVEF in outpatient cardiology practices. The methods and overallstudy objectives have been described in detail elsewhere.12
Community and academic cardiology or multispecialty outpatientpractices from all regions of the country were invited to participateas previously described.12 Patients eligible for enrollment in theIMPROVE HF cohort included those with a clinical diagnosis of HF
or prior MI documented by a cardiologist on at least 2 separate visits.Left ventricular systolic dysfunction was required to be demonstratedquantitatively by a LVEF �35% or qualitatively by findings ofmoderate to severe left ventricular systolic dysfunction on the mostrecent echocardiogram, nuclear multiple gated acquisition scan,contrast ventriculogram, or magnetic resonance imaging scan. Pa-tients with a noncardiovascular medical condition associated with anestimated survival of �1 year and those who had undergone cardiactransplantation were excluded.
A baseline assessment of utilization rates for guideline-recommended therapies was completed at all participating practices.After completion of the baseline data collection, a practice-specificperformance improvement intervention was implemented, and carewas reassessed at prespecified time points during a 24-month period.Baseline and follow-up data were collected by medical chart review.Patient data included demographic and clinical characteristics, med-ical history, previous treatments, New York Heart Association(NYHA) functional status, QRS duration, laboratory results, diag-nostic tests and results, treatments, and patient education. Contrain-dications and other reasons for not administering evidence-basedtherapies were also collected from patient records if documented.Other reasons included patient noncompliance, patient refusal, andmedical, economic, social, and religious reasons for withholdingrecommended therapies.
A representative sample of medical records from patients with aclinical diagnosis of HF and LVEF �35% or prior MI and LVEF�35% at each cardiology practice was screened and selected atrandom to yield an average of 90 eligible patients for each practiceat each assessment period (baseline, 6 months, and 18 months) usingthe methodology described in the trial design (Figure 1).12 Theprimary end point and secondary analyses were prespecified in thestudy protocol and statistical analysis plan. The study design in-cluded rigorous measures to ensure data quality and accuracy. Theseincluded the use of 34 trained, centralized chart review specialistswho received ongoing training and testing to maintain the accuracyof data abstraction. Oversight of the data abstraction training wasprovided by members of the IMPROVE HF steering committee.Average interrater reliability between chart reviewers was 0.82 (�statistic). Additional efforts to ensure the completeness and accuracyof collected data included monthly data quality reports and inclusionof an average of 1.7 automated data quality checks for each data fieldto ensure that values met prespecified ranges, formats, and units. Anaudit of all patient data compared with source documentation wasconducted for 20% of the entire patient sample for a 10% randomsample of participating sites. Mean data concordance rate was 94.5%(range, 92.3% to 96.3%). Practices were required to obtain institu-tional review board approval or waivers to participate in IMPROVEHF. Outcome Sciences Inc (Cambridge, Mass) served as the registrycoordinating center for the trial.
Process Improvement Intervention
n = 165 sites
Longitudinal Cohort
Baseline Chart Review
(Cohort A) n = 15,177 patients
n = 167 sites
12 Month Chart Review
(Cohort A) n = 9386 patients
n = 155 sites
24 Month Chart Review
(Cohort A) n = 7605 patients
n = 155 sites
6 Month Chart Review
(Cohort B) n = 9992 patients
n = 154 sites
18 Month Chart Review
(Cohort C) n = 9641 patients
n = 151 sites
Single Time Points
Total Sites: 167
Patients Enrolled: 34,810
Total Chart Reviews: 63,143
Total # of Site Visits*: 782
* For chart reviews
Figure 1. IMPROVE HF study designand patient flow chart. Longitudinalcohort evaluates changes in qualitymeasures at patient level relative tobaseline. Single-time-point cohorts fur-ther characterize practice treatment pat-terns in unique patients.
586 Circulation August 10, 2010
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

Guideline-Recommended Quality MeasuresSeven quality measures were prospectively selected by the IMPROVE HFsteering committee12: use of (1) angiotensin-converting enzymeinhibitor (ACEI) or angiotensin receptor blocker (ARB), (2)�-blocker, (3) aldosterone antagonist, (4) anticoagulant therapy foratrial fibrillation or flutter, (5) cardiac resynchronization therapy(CRT) (CRT with a defibrillator/CRT with a pacemaker), (6)implantable cardioverter-defibrillator (ICD) (ICD or CRT with adefibrillator), and (7) HF education for eligible patients. The ratio-nale for the selection of each metric was based on its potential toimprove patient outcomes, the precision of its definition, its constructand content validity, and its feasibility.12 It is important to note thatalthough 4 of the 7 quality measures selected for IMPROVE HF (useof ACEI or ARB, �-blocker, HF education, and anticoagulation foratrial fibrillation or flutter) are American College of Cardiology/American Heart Association outpatient HF performance measuresand are endorsed by the National Quality Forum, 3 (use of aldoste-rone antagonist, ICD, and CRT) are not.13 Patients eligible forinclusion in an individual quality measure calculation were thosewho met the criteria for each specific therapy and for whom therewere no contraindications, intolerance, or other documented reasonsto explain why the indicated therapy should not be provided.12 Thedetailed quality measure specifications have previously been pub-lished,12 and eligibility, inclusion, and specific exclusion criteria foreach measure are detailed in Table I in the online-only DataSupplement. HF education was based on medical record documen-tation that written and/or verbal HF education had been provided.Documentation of NYHA functional class is required to be consid-ered eligible for an ICD, CRT, or aldosterone antagonist, andanalyses of these quality measures included only patients withquantitative or qualitative documentation of NYHA functional classat a level consistent with the measure specifications.12 Two summary(composite) measures were also calculated: a total composite score(defined as the percentage of the total indicated quality measuresprovided) and an all-or-none care measure (defined as the proportionof patients who received each quality measure for which they meteligibility criteria).12,14
Performance Improvement InterventionThe IMPROVE HF performance improvement intervention focused onhelping cardiology practices improve systems for treating patients withHF and has been previously described in detail.12 The interventionincluded a guideline-based clinical decision support tool kit, educationalmaterials, practice-specific data reports, benchmarked quality-of-carereports, and structured educational and collaborative opportunities.12 Aspart of an enhanced treatment plan, IMPROVE HF provided evidence-based best-practices algorithms, clinical pathways, standardizedencounter forms, checklists, pocket cards, chart stickers, andpatient education and other materials to facilitate improvedmanagement of outpatients with HF. Examples of IMPROVE HFtools are provided in the study design 12 and are included in theonline-only Data Supplement (A through L). These materials canalso be downloaded from www.improvehf.com. The IMPROVE HFSteering Committee followed a structured, rigorous, evidenced-based, guideline-driven process to develop these pathways and tools.Use of the tools at participating practices was encouraged but notmandatory, and practices could adopt or modify tools at theirdiscretion. A Web-based system provided quality-of-care reports foreach practice that included benchmark comparisons with regionaland national cardiology practices. The investigators and practicesupport personnel attended a 1-day workshop after completion ofbaseline data collection. During the workshop, study goals, guidelinerecommendations, the IMPROVE HF tool kit, performance improve-ment methodology, incentives to promote change in clinical practice,tips on how to serve as champions and engage colleagues in theperformance intervention, and strategies to use the collected dataeffectively to provide practice-specific performance feedback weredescribed and discussed. Clinicians at participating practices wereencouraged to participate in bimonthly educational and collaborativeWeb-based seminars and to continually evaluate, refine, and reassesscare delivery throughout the intervention phase of the study.
Assessment of Guideline-Recommended CareFive chart reviews using representative samples of patients wereconducted at each practice. These occurred at baseline (beforeimplementation of any practice improvement intervention activity)and at 6, 12, 18, and 24 months after initiation of the performanceimprovement intervention (Figure 1). The medical records of pa-tients enrolled in the longitudinal cohort were reviewed at baselineand subsequently at 12 and 24 months after the start of the practiceperformance intervention. These records provided data on temporalchanges in patient-specific quality measures. Two additional single-point-in-time chart reviews were conducted at 6 and 18 months.These chart reviews involved separate and unique patient cohortsfrom the baseline cohort, providing additional data to examinepractice-specific changes in care. Patients entered in the 6- and18-month single-point-in-time cohorts included patients not selectedfor the longitudinal cohort at baseline and those more recentlyreferred to the practice. All 167 practices completed the baselineassessment, and 154, 155, 151, and 155 practices completed the 6-,12-, 18-, and 24-month follow-up assessments, respectively.
The prespecified primary objective of IMPROVE HF was toachieve a relative 20% or greater improvement in at least 2 of the 7quality measures at 24 months compared with baseline for theaggregate of IMPROVE HF practice sites.12 Secondary predefinedobjectives included changes in the 2 summary care measures,changes in care evaluated at the individual practice level for each ofthe 7 quality measures and the 2 summary measures, changes in careconfined to patients with both baseline and 24-month qualitymeasure data (excluding patients who were lost to follow-up, died, ordid not have a follow-up visit in the specified time frame), andevaluation of changes in quality measures in the single-time-pointcohorts at 6 and 18 months compared with baseline.
Statistical MethodsAll statistical analyses were performed by independent biostatisti-cians contracted by Outcome Sciences. Descriptive statistics forbaseline patient and practice characteristics were calculated andreported. Large-sample tests on proportions and large-sample testsfor differences in means were used to evaluate statistical associationsfor ordinal and continuous data, respectively. Each quality measurewas evaluated separately. For each quality measure, the proportion ofpatients receiving therapy among those eligible for that therapy wascalculated for each practice and across all practices. The compositescore and all-or-none care measure were also calculated for eachpractice. To determine the total composite score, the numerators ofall individual quality measures were summed to produce a compositenumerator, and the denominators of all individual quality measureswere summed to produce a composite denominator. The finalcomposite score was produced by dividing the composite numeratorby the composite denominator. The all-or-none care measure wascalculated as the percentage of patients who received all eligiblemeasures (ie, patients who received all the care for which they weredocumented to be eligible). The rates of care for each individualpractice over time (practice-level analyses) at 24 months werecompared with baseline rates. The mean values for each measureacross all practices and care limited to patients with both baselineand 24-month quality measure data were also compared. In addition,utilization rates for each therapy in the single-point-in-time evalua-tion cohorts at baseline, 6 months, and 18 months were compared toevaluate changes in quality measures for unique patients over time.Finally, general estimating equation logistic regression models weredeveloped to quantify how each quality measure changed afterperformance improvement intervention, after adjustment for patientclinical characteristics and practice characteristics and taking intoaccount the correlation of data within patients and practices. Thelogistic regression models included all practice and patient charac-teristics shown in Tables 1 and 2 as possible predictors in the modelif P�0.10 in univariate analyses. Analyses were completed withSAS statistical software, version 9.1 (SAS Institute, Cary, NC). Allstatistical inference testing was 2 sided with results consideredstatistically significant at P�0.05. The authors had full access to and
Fonarow et al Performance Improvement for Heart Failure 587
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

Table 1. IMPROVE HF Baseline Patient Characteristics
CharacteristicLongitudinal Cohort
(n�15 177)6-Month Cohort
(n�9992)18-Month Cohort
(n�9641)Baseline Paired Cohort*
(n�7605)24-Month Paired Cohort*
(n�7605)
Age, y
Mean (SD) 68.7 (13.2) 68.3 (13.2) 68.2 (13.6) 67.6 (12.7) 69.6 (12.7)
Median 70.0 70.0 70.0 69.0 71.0
Male, n (%) 10 787 (71.1) 7069 (70.7) 6814 (70.7) 5422 (71.3) 5422 (71.3)
Race, n (%)
White 6430 (42.4) 5257 (52.6) 5394 (55.9) 3238 (42.6) 3238 (42.6)
Black 1401 (9.2) 1150 (11.5) 1104 (11.5) 686 (9.0) 686 (9.0)
Not documented/missing 7081 (46.7) 3359 (33.6) 2985 (31.0) 3537 (46.5) 3537 (46.5)
Insurance type, n (%)
Medicare 9150 (60.3) 6120 (61.2) 5701 (59.1) 4425 (58.2) 5052 (66.4)
Medicaid 542 (3.6) 342 (3.4) 339 (3.5) 266 (3.5) 242 (3.2)
Private 3758 (24.8) 2725 (27.3) 2485 (25.8) 2091 (27.5) 1820 (23.9)
Other 532 (3.5) 252 (2.5) 212 (2.2) 259 (3.3) 128 (1.7)
Not documented 955 (6.3) 415 (4.2) 728 (7.6) 454 (6.0) 281 (3.7)
None 189 (1.2) 134 (1.3) 176 (1.8) 84 (1.1) 79 (1.0)
Heart failure origin, ischemic, n (%) 9930 (65.4) 6725 (67.3) 6353 (65.9) 4953 (65.1) 5095 (67.0)
Prior MI, n (%) 6072 (40.0) 4017 (40.2) 4014 (41.6) 3140 (41.3) 3929 (51.7)
History of coronary artery bypass graft, n (%) 4728 (31.2) 3142 (31.4) 3010 (31.2) 2344 (30.8) 2590 (34.1)
History of percutaneous coronaryintervention, n (%)
3881 (25.6) 2766 (27.7) 2810 (29.1) 1999 (26.3) 2279 (30.0)
History of atrial fibrillation/flutter, n (%) 4664 (30.7) 3234 (32.4) 3275 (34.0) 2240 (29.5) 3132 (41.2)
History of peripheral vascular disease, n (%) 1743 (11.5) 1155 (11.6) 1189 (12.3) 720 (9.5) 1215 (16.0)
History of diabetes mellitus, n (%) 5173 (34.1) 3467 (34.7) 3433 (35.6) 2401 (31.6) 2874 (37.8)
History of hypertension, n (%) 9437 (62.2) 6610 (66.2) 6715 (69.7) 4670 (61.4) 5714 (75.1)
History of chronic obstructive pulmonarydisease, n (%)
2528 (16.7) 1756 (17.6) 1740 (18.0) 1094 (14.4) 1657 (21.8)
History of depression, n (%) 1366 (9.0) 980 (9.8) 1031 (10.7) 637 (8.4) 1197 (15.7)
NYHA quantified/qualified, n (%) 14 343 (94.5) 9600 (96.0) 9588 (99.5) 7458 (98.1) 7553 (99.3)
NYHA class, n (%)
I 5262 (34.7) 3021 (30.2) 3081 (32.0) 3009 (39.6) 2891 (38.0)
II 5548 (36.6) 4282 (42.9) 4323 (44.8) 2946 (38.8) 3307 (43.5)
III 3144 (20.7) 2127 (21.3) 2034 (21.1) 1386 (18.2) 1245 (16.4)
IV 389 (2.6) 170 (1.7) 150 (1.6) 117 (1.5) 110 (1.4)
Not documented/missing 834 (5.5) 392 (3.9) 53 (0.5) 147 (1.9) 52 (0.7)
LVEF, %
Mean (SD) 25.4 (7.0) 25.7 (6.8) 25.8 (6.9) 25.7 (6.9) 32.3 (12.4)
Median 25.0 25.0 25.0 25.0 30.0
Systolic blood pressure, median, mm Hg 120 120 120 120 120
25th, 75th percentiles 108, 130 110, 132 110, 132 110, 131 110, 130
Diastolic blood pressure, median, mm Hg 70 70 70 70 70
25th, 75th percentiles 60, 80 62, 80 62, 80 62, 80 62, 78
Resting heart rate, median, bpm 71 72 72 70 70
25th, 75th percentiles 64, 80 64, 80 64, 80 64, 78 64, 78
Sodium, median, mEq/L 139 139 139 140 139
25th, 75th percentiles 137, 141 137, 141 137, 141 138, 142 137, 141
Blood urea nitrogen, median, mg/dL 22 22 21 21 22
25th, 75th percentiles 16, 30 16, 30 16, 29 16, 28 16, 32
(Continued)
588 Circulation August 10, 2010
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

take full responsibility for the integrity of the data. All authors haveread and agree to the manuscript as written.
ResultsClinical and Practice CharacteristicsThe medical records of 34 810 patients at 167 outpatientcardiology practices in the United States were included in this
analysis (Figure 1). There were 15 177 patients in thelongitudinal cohort evaluated at baseline, 12 months, and 24months. A median of 90 patients (25th to 75th percentile, 58to 107 patients) per practice were entered. There were 9992unique patients in the 6-month and 9641 unique patients inthe 18-month single-time-point cohorts. At 24 months, 7605(50.1%) of the 15 177 patients in the longitudinal cohort atbaseline were living and had a 24-month follow-up visit,1446 (9.5%) were living but did not have a 24-monthfollow-up visit, 2569 (16.9%) were dead, 2508 (16.5%) werelost to follow-up, and 1049 (6.9%) were from practices thatdid not complete a 24-month visit.
Baseline patient characteristics are shown in Table 1. Themean and median patient ages were 68.7 and 70.0 years, and71.1% of the patients were male. Mean LVEF was 25.4%,and an ischemic origin of HF was identified in 65.4% ofpatients. A history of hypertension (62.2%) and diabetesmellitus (34.1%) was common, and other important condi-tions, including atrial fibrillation (30.7%) and chronic ob-structive pulmonary disease (16.7%), were frequently identi-fied. The median initial blood pressure of registry patientswas 120/70 mm Hg. The median creatinine level was 1.2mg/dL. Among IMPROVE HF outpatient cardiology prac-tices, NYHA functional class was quantitatively documentedin 34.2% and qualitatively documented by symptoms andfunctional limitations in an additional 60.3% of medicalrecords (94.5% total). Characteristics of participating prac-tices at baseline are shown in Table 2. Most of the practiceswere not associated with an academic or university center,and fewer than half reported having a dedicated HF clinic. Ofparticipating practices, 96.0% reported on survey adoption of�1 performance improvement strategies, 85.2% reported useof the benchmarked quality reports, and 60.4% reported useof �1 IMPROVE HF tools.
The frequency of use of guideline-recommended qualitymeasures at baseline in eligible patients is shown in Tables 3and 4 and Figure 2. For aggregate practices at baseline, anACEI/ARB was prescribed for 11 165 (79.8%) of 13 987eligible patients; a �-blocker, for 11 868 (86.2%) of 13 772eligible patients; and an aldosterone antagonist, for 987(34.4%) of 2870 eligible patients. Anticoagulant therapy wasprescribed for 2910 (68.6%) of 4244 eligible patients withpermanent, persistent, or paroxysmal atrial fibrillation or
Table 1. Continued
CharacteristicLongitudinal Cohort
(n�15 177)6-Month Cohort
(n�9992)18-Month Cohort
(n�9641)Baseline Paired Cohort*
(n�7605)24-Month Paired Cohort*
(n�7605)
Creatinine, median, mg/dL 1.2 1.2 1.2 1.2 1.2
25th, 75th percentiles 1.0, 1.6 1.0, 1.5 1.0, 1.5 1.0, 1.5 1.0, 1.6
BNP, median, pg/mL 387 380 373 299 314
25th, 75th percentiles 160, 887 161, 882 158, 892 128, 659 125, 765
QRS duration, median, ms 124 124 122 124 132
25th, 75th percentiles 100, 156 100, 156 100, 154 100, 156 106, 160
n 10 225 7321 7511 5188 3788
QRS duration �120 ms, n (%) 5375 (52.6) 3771 (51.5) 3805 (50.7) 2710 (52.2) 2218 (58.6)
BNP indicates B-type natriuretic peptide.*Baseline and 24-month patient characteristics for patients with data at both time points.
Table 2. IMPROVE HF Baseline Practice Characteristics
CharacteristicPractice Sites
(n�167*)
Census region, n (%)
South 65 (38.9)
Northeast 54 (32.3)
Central 26 (15.6)
West 20 (12.0)
Missing 2 (1.2)
Practice setting, n (%)
University practice setting 13 (7.8)†
Nonuniversity, teaching setting 36 (21.6)†
Nonuniversity, nonteaching setting 108 (64.7)†
Multispecialty, n (%) 40 (24.0)
Hospital-based, n (%) 46 (27.5)
Transplant center, n (%) 16 (9.6)
Suburban/rural, n (%) 119 (71.3)
HF clinic in practice, n (%) 69 (41.3)‡
HF nurse in the practice (�1 FTE APN), n (%) 58 (34.7)
Device clinic in practice, n (%) 131 (78.4)
No. of physicians in practice, n (%)
1–10 81 (48.5)
11–20 46 (27.5)
�20 30 (18.0)
Electrophysiologist in practice, mean (SD)/median 1.5 (1.66)/1.0
Interventionalist in practice, n (%) 146 (87.4)
Average annual No. of patients managed by practice
Mean (SD) 3213.5 (3971.86)
Median 1837.5
FTE indicates full-time equivalent; APN, advanced practice nurse.*Two sites did not provide any survey data.†n�157; ‡n�163.
Fonarow et al Performance Improvement for Heart Failure 589
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

flutter. Of patients eligible for CRT, 580 (37.7%) of 1540patients received therapy; ICD therapy was provided to 4799(48.8%) of 9830 eligible patients. The baseline assessmentshowed that 9373 (61.8%) of 15 177 patients received docu-mented HF education.
Primary Analyses of Quality MeasuresA significant improvement was demonstrated in 5 of the 7quality measures at the practice level at 24 months afterimplementation of the performance improvement interven-tion (P�0.001; Table 3). By 24 months, adherence toevidence-based, guideline-recommended care among prac-tices increased in absolute terms by �25.1% for aldosteroneantagonist use, �29.9% for CRT use, and �27.4% for ICDuse compared with baseline results (P�0.001; Table 3). Useof �-blocker (�6.2%) and HF education (�12.6%) alsoshowed significant improvement (P�0.001; Table 3). Incontrast, use of anticoagulation in eligible patients withpermanent, persistent, or paroxysmal atrial fibrillation orflutter did not improve over time (�0.1%). Use of ACEI/ARB at the practice level increased (�6.8%), but this was nota statistically significant improvement at the practice level(P�0.063). Measures with the lowest level of baselineutilization showed the greatest relative and absolute rates ofimprovement. A modified intention-to-treat analysis of the
relative improvements at 12 and 24 months at the practicelevel showed statistically significant improvements for 6 of 7quality measures for the longitudinal cohort alive and withcomplete follow-up (P�0.001; Table II in the online-onlyData Supplement). There were 123 individual practices(79.4%) with �20% relative improvement in �2 measuresfrom baseline to 24 months. Analysis of quality measureimprovement in practices with and without electronic healthrecord systems is shown in Table III in the online-only DataSupplement.
When the quality measures were analyzed at the aggregatepatient level, there were significant improvements in 6 of 7measures (Figure 2 and Table 4). The absolute magnitude ofimprovement at the patient level in these 6 measures rangedfrom �6.7% (ACEI/ARB) to �30.9% (CRT), and the rela-tive improvement ranged from 8.4% to 81.9% (Table 4).Because 3 of the 7 quality measures improved by �20% at 24months relative to baseline, the prespecified primary endpoint for the study was met. Significant improvements in the6 quality measures that increased from baseline were ob-served by 12 months with further improvement by 24 months(Figure 2). General estimating equation univariate and mul-tivariate analyses, which adjusted for patient and practicecharacteristics, as well as the correlation of data withinpractices showed significant improvement at 24 months
Table 4. Use of Guideline-Recommended Therapies at Baseline, 12 Months, and 24 Months in the Longitudinal Cohort: Patient-Level
Quality MeasureBaseline (95% CI)
(n�15 177), %At 12 mo (95% CI)
(n�9386), %At 24 mo (95% CI)
(n�7605), %
Absolute Improvement,Baseline to 24 mo
(95% CI), %
Relative Improvement,Baseline to 24 mo
(95% CI), % P*
ACEI/ARB 79.8, 11 165/13 987 (79.2–80.5) 84.4, 6728/7968 (83.6–85.2) 86.5, 5348/6183 (85.6–87.3) �6.7 (5.6–7.8) �8.4 (7.0–9.7) �0.001
�-blocker 86.2, 11 868/13 772 (85.6–86.8) 92.5, 7651/8274 (91.9–93.0) 93.6, 6185/6608 (93.0–94.2) �7.4 (6.6–8.2) �8.6 (7.7–9.6) �0.001
Aldosteroneantagonist
34.4, 987/2870 (32.7–36.1) 50.9, 843/1656 (48.5–53.3) 61.8, 798/1291 (59.2–64.5) �27.4 (24.3–30.6) �79.7 (70.5–89.0) �0.001
Anticoagulationfor AF
68.6, 2910/4244 (67.2–70.0) 68.9, 2217/3219 (67.3–70.5) 69.3, 1883/2719 (67.5–71.0) �0.7 (�1.5–2.9) �1.0 (�2.2–4.2) 0.546
CRT-P/CRT-D 37.7, 580/1540 (35.2–40.1) 58.4, 685/1173 (55.6–61.2) 68.5, 751/1096 (65.8–71.3) �30.9 (27.2–34.5) �81.9 (72.2–91.7) �0.001
ICD/CRT-D 48.8, 4799/9830 (47.8–49.8) 70.8, 4654/6575 (69.7–71.9) 79.1, 4218/5331 (78.0–80.2) �30.3 (28.8–31.8) �62.1 (59.1–65.1) �0.001
HF education 61.8, 9373/15 177 (61.0–62.5) 69.0, 6477/9386 (68.1–69.9) 70.8, 5388/7605 (69.8–71.9) �9.1 (7.8–10.4) �14.7 (12.6–16.8) �0.001
Abbreviations as in Table 3.*P value is for relative improvement comparison.
Table 3. Use of Guideline-Recommended Therapies at Baseline, 12 Months, and 24 Months in the Longitudinal Cohort: Practice Level
Quality MeasureBaseline (95% CI)
(n�167), %At 12 mo (95% CI)
(n�155), %At 24 mo (95% CI)
(n�155), %Absolute Improvement, Baseline
to 24 mo (95% CI), %Relative Improvement, Baseline
to 24 mo (95% CI), % P*
ACEI/ARB 78.3 (76.5–80.2) 81.7 (79.7–83.6) 85.1 (83.4–86.8) �6.8 (4.8–8.8) �19.4 (�1.1–39.8) 0.063
�-blocker 86.0 (84.3–87.7) 90.8 (89.5–92.1) 92.2 (90.6–93.8) �6.2 (4.8–7.6) �7.6 (5.1–10.2) �0.001
Aldosteroneantagonist
34.5 (31.5–37.4) 48.1 (44.1–52.1) 60.3 (56.1–64.4) �25.1 (20.7–29.6) �86.5 (67.1–105.9) �0.001
Anticoagulationfor AF
68.0 (65.5–70.5) 68.3 (65.7–70.9) 67.8 (65.0–70.7) �0.1 (�3.0–2.8) �1.0 (�3.6–5.5) 0.673
CRT-P/CRT-D 37.2 (32.2–42.2) 56.4 (51.7–61.2) 66.3 (61.6–71.1) �29.9 (23.6–36.2) �124.5 (85.5–163.5) �0.001
ICD/CRT-D 50.1 (47.3–52.8) 69.7 (67.1–72.3) 77.5 (74.8–80.1) �27.4 (24.6–30.2) �70.9 (61.0–80.8) �0.001
HF education 59.5 (55.7–63.2) 69.4 (65.9–73.0) 72.1 (68.3–75.9) �12.6 (8.2–17.0) �50.6 (27.1–74.2) �0.001
All-or-none care 23.5 (21.6–25.3) 55.3 (53.0–57.6) 68.7 (66.7–70.8) �45.2 (42.8–47.7) �345.5 (246.2–444.9) �0.001
Composite care 67.1 (65.7–68.5) 75.2 (73.7–76.7) 79.0 (77.5–80.5) �11.9 (10.4–13.4) �19.2 (16.3–22.0) �0.001
AF indicates atrial fibrillation; CRT-D, CRT with defibrillator; CRT-P, CRT with pacemaker. Values are site mean percent of patients receiving indicated therapy.*P value is for relative improvement comparison for 24 months and baseline at practice level.
590 Circulation August 10, 2010
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

compared with baseline for 5 of 7 measures in the longitudi-nal cohort (Table IV in the online-only Data Supplement).Use of guideline-recommended therapies at baseline in pa-tients alive with 24-month follow-up and patients who died orwere lost to follow-up at the patient level is provided in TableV in the online-only Data Supplement. When the qualitymeasure results were stratified by patient age, improvementswere seen for each age group for 6 of 7 measures withoutevidence of heterogeneity except for the ICD measure (Ta-bles VI and VII in the online-only Data Supplement).
A modified intention-to-treat patient-level analysis con-fined to only patients alive and with complete follow-up at 24months showed that these patients had similar relative andabsolute improvement in the 6 quality measures at 12 and 24months (Table 5). This paired patient cohort had baselinecharacteristics similar to those of the primary analysis popu-lation (Table 1). The portion of patients with newly docu-mented contraindications or intolerance at the 24-monthassessment that were not documented at baseline and the
portion of patients newly treated are shown in Table 6. Theimprovements in the ICD, CRT, and HF education measureswere predominantly the result of more eligible patients beingtreated. For the ACEI/ARB, �-blocker, and aldosteroneantagonist measures, both improved treatment and betterdocumentation of contraindications or intolerance wereoperative.
Composite Score and All-or-None Care MeasuresAt baseline, the mean total composite score was 68.4%, andthe all-or-none care measure was met in 24.3% of patients(95% confidence interval [CI], 23.6–25.0). At 24 monthsafter intervention, the mean total composite score increased to80.1% (�11.6% absolute improvement and 17.0% relativeimprovement; P�0.001). For the all-or-none care measure,the percentage increased to 43.9% (95% CI, 42.8–45.0;�19.6% absolute improvement, 80.6% relative improvement;P�0.001).
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
ACEI/ARB Beta-Blockers Aldosterone Antagonist
Anticoagulant Therapy
CRT/ (CRT-P/CRT-D)
ICD/CRT-D HF Education
Baseline (n= 15177)
12 months (n = 9386)
24 months (n =7605)
* *
‡
†
§
†
†
†
* *
*
* *
* *
*
* *
Elig
ible
Pat
ient
s Tr
eate
d
Figure 2. Use of guideline-recommended therapies at baseline, 12 months, and 24 months in the longitudinal cohort. CRT-P indicatesCRT with pacemaker; CRT-D, CRT with defibrillator. *P�0.001, 12 and 24 months vs baseline. †P�0.001, 12 vs 24 months. ‡P�0.007,12 vs 24 months. §P�0.009, 12 vs 24 months.
Table 5. Use of Guideline-Recommended Therapies in the Longitudinal Cohort With Complete Follow-Up at 24 Months: Patient Level
Quality MeasureBaseline (95% CI)
(n�7605), %At 12 mo (95% CI)
(n�7605), %At 24 mo (95%CI)
(n�7605), %
Absolute Improvement,Baseline to 24 mo
(95% CI), %
Relative Improvement,Baseline to 24 mo
(95% CI), % P *
ACEI/ARB 83.0, 5921/7138 (82.1–83.8) 86.0, 5268/6125 (85.1–86.9) 86.5, 5348/6183 (85.6–87.3) �3.5 (2.3–4.8) �4.3 (2.8–5.7) �0.001
�-blocker 88.5, 6109/6905 (87.7–89.2) 92.8, 5863/6231 (92.1–93.4) 93.6, 6185/6608 (93.0–94.2) �5.1 (4.2–6.1) �5.8 (4.7–6.9) �0.001
Aldosteroneantagonist
35.4, 453/1278 (32.8–38.1) 51.6, 615/1192 (48.8–54.4) 61.8, 798/1291 (59.2–64.5) �26.4 (22.6–30.1) �74.4 (63.9–84.9) �0.001
Anticoagulationfor AF
72.2, 1488/2061 (70.3–74.1) 71.0, 1718/2420 (69.2–72.8) 69.3, 1883/2719 (67.5–71.0) �2.9 (�5.5–�0.3) �4.1 (�7.7–�0.5) 0.026
CRT-P/CRT-D 41.2, 277/673 (37.4–44.9) 60.3, 499/828 (56.9–63.6) 68.5, 751/1096 (65.8–71.3) �27.4 (22.7–32.0) �66.5 (55.2–77.7) �0.001
ICD/CRT-D 54.4, 2736/5028 (53.0–55.8) 73.2, 3653/4992 (71.9–74.4) 79.1, 4218/5331 (78.0–80.2) �24.7 (23.0–26.5) �45.4 (42.4–48.6) �0.001
HF education 59.7, 4539/7605 (58.6–60.8) 68.8, 4905/7134 (67.7–69.8) 70.8, 5388/7605 (69.8–71.9) �11.2 (9.7–12.7) �18.7 (16.2–21.2) �0.001
Abbreviations as in Table 3. Values are percent, n/N (95% CI) when appropriate.*P value is for relative improvement comparison.
Fonarow et al Performance Improvement for Heart Failure 591
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

Single-Point-in-Time CohortsThe 6- and 18-month single-point-in-time cohorts of uniquepatients had characteristics similar to those of the baselinecohort (Table 1). Improvement at the patient level wasdemonstrated at 6 and 18 months for each quality measureexcept anticoagulation for atrial fibrillation or flutter. Themagnitude of absolute and relative improvement in use ofguideline-recommended therapies was smaller (�1.5% to�14.1% and 1.9% to 22.8%, respectively) in the single-point-in-time cohorts (Table 7) compared with the longitudinalcohort. When analyzed at the practice level, 5 of 7 measuresshowed modest but statistically significant improvement inthe 18-month cohort compared with the baseline cohort(Table VIII in the online-only Data Supplement). Generalestimating equation multivariate analysis showed improve-ment in 4 of 7 measures in the 18-month cohort comparedwith the baseline cohort (Table IX in the online-only DataSupplement).
DiscussionDespite compelling scientific evidence and readily accessiblenational guidelines, beneficial therapies for HF remain under-used in many care settings.3–9 IMPROVE HF is the firstlarge-scale outpatient performance improvement initiativedesigned to assess the effects of a practice-specific, process-of-care improvement intervention on HF patient care. Byvirtue of its design, combining cardiology practice–basedstructured data collection and feedback with guideline-basedperformance improvement tools, IMPROVE HF has contrib-uted to the current description of care patterns for patientswith HF with reduced LVEF or prior MI with reduced LVEF.These results provide a model to enhance clinical manage-ment of these patients in the outpatient setting. IMPROVEHF has shown that use of evidence-based, guideline-recommended HF therapies can be enhanced by the use ofdecision support tools, patient data collection, and perfor-mance feedback, concentrating on the specific therapiesproven to improve outcomes. However, the determination ofeligibility for treatment by medical record review is complex,and this study highlights many of the challenges faced intrying to assess and improve care in outpatient cardiologypractices.
Gaps in the use of evidence-based therapies may reflectdifferences in training, familiarity with guidelines, patientcase mix, and lack of systems to ensure that recommendedcare is provided. Successful strategies to improve the imple-mentation of national practice guidelines include clinicaldecision support, provider education, patient education datacollection, and performance feedback.2 A number of large,national, US hospital-based programs have sought to monitorand improve the care of patients hospitalized with HF byencouraging the use of process improvement systems andevidence-based, guideline-recommended HF therapies, in-cluding the Acute Decompensated Heart Failure NationalRegistry (ADHERE), Organized Program to Initiate Life-Saving Treatment in Hospitalized Patients With Heart Failure(OPTIMIZE-HF), and Get With the Guidelines–Heart Failure(GWTG-HF).7,10,11 These performance improvement regis-tries focused on HF care in the inpatient setting or the earlypostdischarge follow-up period. Certain HF disease manage-ment programs involving specialty care and multidisciplinaryteams have been shown to be effective in improving qualityof care and outcomes in the outpatient setting.15 Unfortu-nately, despite the potential benefits, these programs are notthe norm and are often offered to only a small number of HFpatients. Thus, there is a substantial need for strategies to bebroadly implemented to improve the quality of outpatient HFcare.
Although there are many major obstacles to overcome toimprove care in the outpatient setting, cardiology practicesparticipating in IMPROVE HF were able to improve perfor-mance on 5 of 7 quality measures. At the time of the24-month assessment, 80.1% of the opportunities to provideevidence-based, guideline-recommended care to patients doc-umented to be eligible were fulfilled compared with 68.4% atbaseline. Importantly, all-or-none care demonstrated an80.6% relative improvement from baseline to 24-monthassessment. The relative and absolute rates of improvement inguideline-recommended use of CRT, ICD, and aldosteroneantagonist therapies in eligible patients were substantial.Other studies have suggested very little change in the use ofthese 3 therapies for HF from 2005 to 2008, making it lesslikely that the improvements observed were a result of seculartrends.6,7,16 Although the baseline rates of �-blocker use werereasonably high, there was still significant improvement at 24
Table 6. Newly Documented Contraindications/Intolerance and Newly Treated Patients at 24 Months in the LongitudinalCohort With Complete Follow-Up Who Were Eligible for Treatment at Baseline or Newly Eligible for Treatment by 24 Months
Quality Measure
Newly Documented Contraindications orIntolerance at 24 mo in Patients Initially
Eligible at Baseline (n�7605), %
Newly Treated at 24 moin Patients Initially Eligibleat Baseline (n�7605) %
Newly Treated at 24 mo in Patients NotInitially Eligible at Baseline but Eligible
by 24 mo %
ACEI/ARB 9.8 (699/7138) 7.6 (546/7138) 67.1 (49/73)
�-blocker 5.5 (381/6905) 6.3 (434/6905) 83.9 (208/248)
Aldosterone antagonist 16.4 (210/1278) 10.3 (132/1278) 54.2 (396/730)
Anticoagulation for AF 8.8 (181/2061) 6.9 (143/2061) 58.1 (493/848)
CRT-P/CRT-D 1.8 (12/673) 23.5 (158/673) 59.3 (377/636)
ICD/CRT-D 3.9 (198/5028) 15.3 (769/5028) 71.1 (857/1205)
HF education 0.0 (0/7605) 26.3 (2003/7605) 0.0 (0/0)
Abbreviations as in Table 3.
592 Circulation August 10, 2010
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

months in this care measure. Documentation that HF educa-tion was provided also improved over the course of theprogram.
Those quality measures with lower baseline use showedgreater absolute and relative improvement over time. Thesefindings may reflect a greater effort to improve those mea-sures with the best opportunities to improve, a ceiling effecton measures with higher levels of conformity, or otherfactors. Despite being a focus of the process improvementintervention and despite significant improvements observedin all other quality measures, there was no increase in the useof anticoagulation in eligible patients with atrial fibrillation orflutter. Other quality improvement initiatives in the hospitalsetting have also failed to demonstrate improvement in theuse of this guideline-recommended therapy.10,17 The reasonsfor this are unclear but may be due in part to physicianperception that warfarin is not necessary for atrial fibrillationin certain patients with HF, reluctance to prescribe warfarinwhen indicated because of the inconvenience associated withmonitoring, undocumented concerns about risks, contraindi-cations that were present but not documented, undocumentedpatient refusal, or other factors. Further study is needed tounderstand the underlying causes of the anticoagulationtreatment gap and to develop more effective strategies toovercome these barriers.
Although performance improvements were evident for thelongitudinal and single-point-in-time (6- and 18-month) co-horts, the magnitudes of both relative and absolute improve-ments were not equivalent. This may be due to the fact thatpractice- and patient-level performance reports and the clin-ical decision support tools were provided for the longitudinalcohort but patient-level reports were not provided for thesingle-point-in-time patient cohorts. The patient-level reportsin the longitudinal cohort identified patients who were eligi-ble for specific therapies but were not being treated. Physi-cians and nurses could use this information to recall or flagpatients for initiation of the indicated therapy at a subsequentappointment. The greater magnitude of improvement overtime in the longitudinal cohort suggests that receipt ofpatient-level performance feedback that is actionable appearsto be a particularly important component of HF performanceimprovement efforts.
The improvements in certain quality measures in this studymay reflect improvements in the documentation of careprovided. For example, clinicians may have provided com-plete HF education at baseline but failed to document this inthe medical record, and over the course of IMPROVE HF,they started to include this documentation. Medication anddevice therapy treatment rates also could have improved as aresult of increased documentation of contraindications, intol-erances, and patient and physician reasons for not providingguideline-recommended therapies rather than an increase inthe number of eligible patients actually treated. However, thesensitivity analyses comparing patients who qualified fortreatment at both baseline and 24 months showed similarimprovements in the use of evidence-based therapies, whichsuggests that this finding is not solely attributed to changes indocumentation. Furthermore, there were only modest changesin the number of patients with documented contraindicationsor intolerance at 24 months compared with baseline for mostmeasures except aldosterone antagonists.
Although conformity with guideline recommendationssubstantially increased with the intervention, gaps in carepersisted at 24 months, as did opportunities for furtherimprovements in care. However, treatment rates that are�100% are not necessarily evidence of deficiencies of care.These data also may indicate that there is a need for betterdocumentation of decision making and patient exclusions forguideline-recommended therapies if they are present. Thedecision to proceed with device therapy requires in-depth andoften multiple discussions with patients, but these discussionsmay not always be documented in the medical record,especially when the decision is to forego use of an otherwiseindicated device.9 Use of an aldosterone antagonist requiresclose monitoring of patients’ potassium levels and renalfunction.2 As a result, patients may have appeared in themedical record to be eligible for treatment, but an appropriatedecision led to withholding that intervention. Conversely,because there was incomplete documentation of NYHAfunctional class and QRS duration, other patients who mighthave been eligible for treatment with improved documenta-tion were not included in the quality measures. Qualityimprovement efforts should also focus on better documenta-tion of patient eligibility for guideline-recommended thera-
Table 7. Use of Guideline-Recommended Therapies at Baseline, 6 Months, and 18 Months in the Single-Point-in-Time Cohorts:Patient Level
Quality MeasureBaseline (95% CI)
(n�15 177), %At 6 mo (95% CI)
(n�9992), %At 18 mo (95% CI)
(n�9641), %
Absolute Improvement,Baseline to 18 mo
(95% CI), %
Relative Improvement,Baseline to 18 mo
(95% CI), % P *
ACEI/ARB 79.8, 11 165/13 987 (79.2–80.5) 80.7, 7372/9130 (79.9–81.6) 81.3, 7061/8685 (80.5–82.1) �1.5 (0.4–2.5) �1.9 (0.5–3.2) 0.006
�-blocker 86.2, 11 868/13 772 (85.6–86.8) 90.3, 8065/8930 (89.7–90.9) 91.9, 7831/8519 (91.3–92.5) �5.7 (4.9–6.6) �6.7 (5.7–7.6) �0.001
Aldosteroneantagonist
34.4, 987/2870 (32.7–36.1) 36.9, 687/1862 (34.7–39.1) 38.0, 686/1804 (35.8–40.3) �3.6 (0.8–6.5) �10.6 (2.3–18.8) 0.012
Anticoagulationfor AF
68.6, 2910/4244 (67.2–70.0) 69.4, 2059/2967 (67.7–71.1) 69.9, 2062/2951 (68.2–71.5) �1.3 (�0.9–3.5) �1.9 (�1.3–5.1) 0.237
CRT-P/CRT-D 37.7, 580/1540 (35.2–40.1) 37.8, 398/1052 (34.9–40.8) 44.1, 456/1034 (41.1–47.1) �6.4 (2.6–10.3) �17.1 (6.8–27.4) 0.001
ICD/CRT-D 48.8, 4799/9830 (47.8–49.8) 54.1, 3736/6907 (52.9–55.3) 55.9, 3831/6859 (54.7–57.0) �7.0 (5.5–8.6) �14.4 (11.3–17.6) �0.001
HF education 61.8, 9373/15 177 (61.0–62.5) 67.5, 6748/9992 (66.6–68.5) 75.8, 7312/9641 (75.0–76.7) �14.1 (12.9–15.2) �22.8 (20.9–24.7) �0.001
Abbreviations as in Table 3. Values are percent, n/N (95% CI) when appropriate.*P value is for relative improvement comparison.
Fonarow et al Performance Improvement for Heart Failure 593
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

pies, patient exclusions if present, and clinical decisionmaking.
Cardiology practices participating in IMPROVE HF inaggregate were better able to translate the strongest clinicalevidence and national guideline-recommended therapies intoroutine clinical practice and/or to provide better documenta-tion of the therapies given after implementing the perfor-mance improvement initiative. Unlike other initiatives thatdepended on self-reported data, which may introduce thepotential for bias, data analyzed in this study were abstractedfrom patient medical records by independent operators. Rep-resentative samples of patients were generated, decreasing thelikelihood of selective case ascertainment. National guide-lines recommend the use of programs to identify appropriatepatients for therapy (Class I), to provide practitioners withuseful reminders based on the guidelines (Class IIa), and tocontinuously assess the success achieved in providing thesetherapies to patients who can benefit from them (Class IIa).2
The demonstration of substantial change in the use ofguideline-recommended therapies among practices participat-ing in IMPROVE HF provides direct evidence in support ofthese guideline recommendations. Because this program,except for practice-specific data collection, used existingpersonnel and resources within each practice, it may be morescalable and sustainable than alternative models to improveoutpatient care.
LimitationsCertain limitations are inherent in the design of IMPROVEHF and should be considered when interpreting these find-ings. Data were collected by medical chart review. Thus, thequality and validity of these data depend on the accuracy andcompleteness of the medical records and abstraction process.Importantly, determination of patient eligibility and utiliza-tion rates for each of the 7 quality measures was based on thisdocumentation. It is possible that the changes in treatmentrates found in this study may be attributable in part tovariations or inaccuracies in the medical record or dataabstraction process. A proportion of patients consideredeligible for treatment but not treated at each time point mayhave had contraindications or other reasons that preventedtreatment but were not documented. Documentation in themedical record of the provision of HF education may not bea reliable indication that the information was understood orsufficient to meet the educational needs of patients and theircaregivers. As expected in the clinical practice setting,follow-up was not available for all patients. However, im-provements in the quality measures were still observed whenthe analysis was confined to paired analyses of patients with24-month follow-up data and the 6- and 18-month single-point-in-time cohorts. Although this study assessed improve-ments in use of therapies at outpatient cardiology practicesexposed to a performance improvement initiative, the designdoes not support evaluation of the effect of the interventionon clinical outcomes. Additional studies are required toestablish that the improved use of guideline-recommendedtherapies actually results in improved clinical outcomes forHF patients in the real-world outpatient cardiology practicesetting. It is also not possible to determine whether the
intervention had unintended consequences such as increasingthe use of therapies not included in current guideline recom-mendations. Furthermore, individual intervention compo-nents that were more or less efficacious in facilitatingchanges in clinical practice cannot be determined. Althoughthe amount of missing data in the longitudinal cohort isgreater than that seen in clinical trials, there is no currentbenchmark for this kind of quality improvement data collec-tion in the outpatient practice setting, and given the variancesin patient mobility and access to care, the level of missingdata seen in IMPROVE HF may be within expectations.Although aldosterone antagonists, CRT, and ICD therapyhave been shown to reduce mortality and are Class I recom-mendations for eligible patients in the American College ofCardiology/American Heart Association guidelines, the out-patient performance measure sets do not include measures forthese therapies. Some experts question whether such mea-sures are appropriate for quality assessment and improve-ment.2,13 The practices participating in IMPROVE HF wereself-selected; thus, these findings may not apply to practicesthat differ in patient case mix, baseline care patterns, moti-vation, and resources from IMPROVE HF outpatient cardi-ology practices. In addition, all patients received care atoutpatient cardiology practices, whereas many HF patients inthe United States are treated in primary care settings. We donot know how this performance improvement interventionwould affect clinical practice in primary care settings. Pa-tients in IMPROVE HF were drawn from a representativesample from each practice, had documented left ventricularfunction, and had at least 2 office visits in the last 2 years.These factors may have introduced ascertainment bias, sothese patients may not be entirely representative of theoutpatient population of patients with HF in cardiologypractices.
IMPROVE HF was not a randomized clinical trial with aconcurrent control group of outpatient cardiology practicesnot exposed to the performance improvement intervention.Therefore, it is possible that the improvements in qualitymeasures may have been influenced by secular trends andfactors other than participation in this study. However,participation in IMPROVE HF was associated with substan-tial improvements in the use of HF therapies that were notpart of any other known concurrent local or regional perfor-mance improvement initiatives for HF, which makes it lesslikely that the observed improvements were due to externalfactors. Furthermore, quality-of-care improvement initiativesthat did include concurrent control groups such as theGuidelines Applied in Practice (GAP) Project resulted inchanges consistent with those found in IMPROVE HF.18
ConclusionsIMPROVE HF is the largest outpatient, cardiology practice–based performance improvement program dedicated to im-proving the use of guideline-recommended therapies in eli-gible patients with HF with reduced LVEF and previous MIwith reduced LVEF. Practices participating in IMPROVE HFdemonstrated a significant increase in the use of 5 of 7guideline-recommended therapies in eligible patients withoutcontraindications. The results of this study suggest a favor-
594 Circulation August 10, 2010
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

able impact of applying performance improvement tech-niques of clinical decision support, reminder systems,guideline-driven care improvement tools, educational out-reach, collaborative support, performance profiling, and feed-back in real-world cardiology practices. Implementation ofthis defined and scalable practice-specific intervention mayenhance the use of guideline-recommended HF therapiespreviously demonstrated to improve outcomes. These find-ings may also help to establish a model and framework forfuture performance-improvement programs administered inthe outpatient setting.
AcknowledgmentCommGeniX LLC provided technical copyediting support withfunding from Medtronic Inc.
Source of FundingThe IMPROVE HF registry and this study are sponsored byMedtronic Inc, Minneapolis, Minn.
DisclosuresDr Fonarow has received research grants from the National Institutesof Health; honoraria from Medtronic, GlaxoSmithKline, Pfizer, St.Jude Medical; and consultant frees from Medtronic, Novartis, and St.Jude Medical. Dr Albert has received consultant fees from Medtronicand speakers’ bureau fees from GlaxoSmithKline. Dr Curtis hasreceived research grants from Medtronic and St. Jude Medical;speakers’ bureau fees from Medtronic, St. Jude Medical, BostonScientific, Biotronik, and Sanofi-Aventis; honoraria from Medtronicand Sanofi-Aventis; consultant/advisory board fees from St. JudeMedical and Biosense Webster; and fellowship support fromMedtronic. Dr Gattis Stough has received consultant/advisory boardfees from GlaxoSmithKline, Gilead Sciences, Medtronic, and Scios.Dr Gheorghiade has received consultant fees from Abbott Labora-tories, Astellas, Astra Zeneca, Bayer Schering Pharma AG, CorTheraInc, Cytokinetics Inc, DebioPharm SA, Errekappa Terapeutici(Milan, Italy), GlaxoSmithKline, Johnson & Johnson, Medtronic,Merck, Novartis Pharma AG, Otsuka Pharmaceuticals, Pericor Ther-apeutics, Protein Design Laboratories, Sanofi-Aventis, Sigma Tau,and Solvay Pharmaceuticals. Dr Heywood has received researchgrants from Biosite, Medtronic, and St. Jude Medical; speakers’bureau fees/honoraria from GlaxoSmithKline, Medtronic, AstraZen-eca, Novartis, Actelion, St. Jude Medical, Otsuka, and BostonScientific; and consultant/advisory board fees from Emerge,Medtronic, and Actelion. Dr Mehra has received consultant feesfrom Medtronic, Orqis, Johnson & Johnson, Solvay, PeriCor, and St.Jude Medical and grants/research support from Maryland IndustrialPartnerships, Maryland Tobacco Fund, National Institutes of Health,and Orqis. Dr O’Connor has received consultant fees from Forest,Medtronic, Amgen, Medpace, Impulse Dynamics, Actelion, Cyto-kinetics, Roche, and Trevena. Dr Reynolds has received researchgrants from Medtronic and Biotronik; speakers’ bureau fees fromMedtronic and Sorin, and consultant fees from Medtronic. Dr Walshhas received consultant fees from ARCA, Boston Scientific,Medtronic, and United HealthCare. The other authors report noconflicts. Medtronic provided financial and material support for theIMPROVE HF registry. The sponsor had no role or input into theselection of endpoints or quality measures used in the study. Acontract research organization, Outcome Sciences Inc (Cambridge,Mass), independently performed the practice site chart abstractionsfor IMPROVE HF and is responsible for performing data checks,storing site-specific and aggregate data, and providing benchmarkedquality-of-care reports to practice sites. The contract research orga-nization receives funding from Medtronic. Individually identifiablepractice site data are not shared with either the steering committee orthe sponsor. The authors had complete control and authority over thestudy design, the manuscript preparation, and the decision to submit
this manuscript to Circulation for publication. The manuscript wassubmitted to Medtronic before submission for publication.
References1. Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB,
Flegal K, Ford E, Furie K, Go A, Greenlund K, Haase N, Hailpern S, HoM, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A,McDermott M, Meigs J, Mozaffarian D, Nichol G, O’Donnell C, RogerV, Rosamond W, Sacco R, Sorlie P, Stafford R, Steinberger J, Thom T,Wasserthiel-Smoller S, Wong N, Wylie-Rosett J, Hong Y. Heart diseaseand stroke statistics—2009 update: a report from the American HeartAssociation Statistics Committee and Stroke Statistics Subcommittee.Circulation. 2009;119:e21–e181.
2. Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, GaniatsTG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, RahkoPS, Silver MA, Stevenson LW, Yancy CW, Antman EM, Smith SC Jr,Adams CD, Anderson JL, Faxon DP, Fuster V, Halperin JL, Hiratzka LF,Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B. ACC/AHA 2005guideline update for the diagnosis and management of chronic heartfailure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (WritingCommittee to Update the 2001 Guidelines for the Evaluation andManagement of Heart Failure): developed in collaboration with theAmerican College of Chest Physicians and the International Societyfor Heart and Lung Transplantation: endorsed by the Heart RhythmSociety. Circulation. 2005;112:e154 – e235.
3. Williams SC, Schmaltz SP, Morton DJ, Koss RG, Loeb JM. Quality ofcare in U.S. hospitals as reflected by standardized measures, 2002–2004.N Engl J Med. 2005;353:255–264.
4. Lee DS, Tu JV, Juurlink DN, Alter DA, Ko DT, Austin PC, Chong A,Stukel TA, Levy D, Laupacis A. Risk-treatment mismatch in the phar-macotherapy of heart failure. JAMA. 2005;294:1240–1247.
5. Fonarow GC, Yancy CW, Heywood JT, for the ADHERE ScientificAdvisory Committee, Study Group, and Investigators. Adherence to heartfailure quality-of-care indicators in US hospitals: analysis of theADHERE Registry. Arch Intern Med. 2005;165:1469–1477.
6. Shah B, Hernandez AF, Liang L, Al-Khatib AM, Yancy CW, FonarowGC, Peterson ED, for the Get With the Guidelines Steering Committee.Hospital variation and characteristics of implantable cardioverter-defibrillator use in patients with heart failure: data from the GWTG-HF(Get With The Guidelines–Heart Failure) registry. J Am Coll Cardiol.2009;53:416–422.
7. Piccini JP, Hernandez AF, Dai D, Thomas KL, Lewis WR, Yancy CW,Peterson ED, Fonarow GC, for the Get With the Guidelines SteeringCommittee and Hospitals. Use of cardiac resynchronization therapy inpatients hospitalized with heart failure. Circulation. 2008;118:926–933.
8. Stafford RS, Radley DC. The underutilization of cardiac medications ofproven benefit, 1990 to 2002. J Am Coll Cardiol. 2003;41:56–61.
9. Fonarow GC, Yancy CW, Albert NM, Curtis AB, Gattis Stough W,Gheorghiade M, Heywood JT, McBride ML, Mehra MR, O’Connor CM,Reynolds D, Walsh MN. Heart failure care in the outpatient cardiologypractice setting: findings from IMPROVE HF. Circ Heart Fail. 2008;1:98–106.
10. Fonarow GC, Abraham WT, Albert NM, Gattis Stough W, GheorghiadeM, Greenberg BH, O’Connor CM, Pieper K, Sun JL, Yancy CW, YoungJB, for the OPTIMIZE-HF Investigators and Hospitals. Influence of aperformance-improvement initiative on quality of care for patients hos-pitalized with heart failure: results of the Organized Program to InitiateLifesaving Treatment in Hospitalized Patients With Heart Failure(OPTIMIZE-HF). Arch Intern Med. 2007;167:1493–1502.
11. Fonarow GC, Heywood JT, Heidenreich PA, Lopatin M, Yancy CW, forthe ADHERE Scientific Advisory Committee and Investigators.Temporal trends in clinical characteristics, treatments, and outcomes forheart failure hospitalizations, 2002 to 2004: findings from Acute Decom-pensated Heart Failure National Registry (ADHERE). Am Heart J. 2007;153:1021–1028.
12. Fonarow GC, Yancy CW, Albert NM, Curtis AB, Gattis Stough W,Gheorghiade M, Heywood JT, Mehra M, O’Connor CM, Reynolds D,Walsh MN. Improving the use of evidence-based heart failure therapies inthe outpatient setting: the IMPROVE HF performance improvementregistry. Am Heart J. 2007;154:12–38.
13. Bonow RO, Bennett SJ, Casey DE Jr, Ganiats TG, Hlatky MA, KonstamMA, Lambrew CT, Normand SLT, Pina IL, Radford MJ, Smith AL,Stevenson LW, Burke G, Eagle KA, Krumholz HM, Linderbaum J,
Fonarow et al Performance Improvement for Heart Failure 595
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

Masoudi FA, Ritchie JL, Rumsfeld JS, Spertus JA. ACC/AHA clinicalperformance measures for adults with chronic heart failure: a report of theAmerican College of Cardiology/American Heart Association Task Forceon Performance Measures (Writing Committee to Develop Heart FailureClinical Performance Measures): endorsed by the Heart Failure Society ofAmerica. J Am Coll Cardiol. 2005;46:1144–1178.
14. Nolan T, Berwick DM. All-or-none measurement raises the bar on per-formance. JAMA. 2006;295:1168–1170.
15. McAlister FA, Stewart S, Ferrua S, McMurray JJ. Multidisciplinarystrategies for the management of heart failure patients at high risk foradmission: a systematic review of randomized trials. J Am Coll Cardiol.2004;44:810–819.
16. Albert NM, Yancy CW, Liang L, Zhao X, Hernandez AF, Peterson ED,Cannon CP, Fonarow GC. Use of aldosterone antagonists in heart failure.JAMA. 2009;302:1658–1665.
17. Piccini JP, Hernandez AF, Zhao X, Patel MR, Lewis WR, PetersonED, Fonarow GC, for the Get With the Guidelines Steering Committeeand Hospitals. Quality of care for atrial fibrillation among patientshospitalized for heart failure. J Am Coll Cardiol. 2009;54:1280 –1289.
18. Eagle KA, Montoye CK, Riba AL, DeFranco AC, Parrish R, Skorcz S,Baker PL, Faul J, Jani SM, Chen B, Roychoudhury C, Elma MA,Mitchell KR, Mehta RH, for American College of Cardiology’sGuidelines Applied in Practice (GAP) Projects in Michigan andAmerican College of Cardiology Foundation’s Guidelines Applied inPractice Steering Committee. Guideline-based standardized care isassociated with substantially lower mortality in Medicare patients withacute myocardial infarction: the American College of Cardiology’sGuidelines Applied in Practice (GAP) projects in Michigan. J Am CollCardiol. 2005;46:1242–1248.
CLINICAL PERSPECTIVEHeart failure (HF) is a chronic progressive disease that results in substantial morbidity, mortality, and expenditure ofhealthcare resources. Despite compelling scientific evidence and professional society guidelines, beneficial therapies forHF remain underused and inconsistently applied in many care settings. New, more effective approaches to improve the useof guideline-recommended therapies for HF are needed. The Registry to Improve the Use of Evidence-Based Heart FailureTherapies in the Outpatient Setting (IMPROVE HF) prospectively tested a multidimensional practice-specific performanceimprovement intervention on the use of guideline-recommended therapies for HF in outpatient cardiology practices.Performance data were collected in a random sample of HF patients from 167 outpatient cardiology practices at baseline(pre-intervention), longitudinally following intervention at 12 and 24 months, and in unique patient cohorts at 6 and 18months. Participants included 34 810 patients with reduced left ventricular ejection fraction and chronic HF orpost–myocardial infarction. Interventions included clinical decision support tools, structured improvement strategies, andchart audits with performance feedback. The performance improvement intervention resulted in significant improvementsin 5 of 7 quality measures at the 24-month assessment compared to baseline. Improvements in the unique single-point-in-time cohorts were smaller. The results of this study suggest a favorable impact of applying performance improvementtechniques of clinical decision support, reminder systems, guideline-driven care improvement tools, educational outreach,collaborative support, performance profiling, and feedback in real-world cardiology practices. These findings may also helpto establish a model and framework for future performance-improvement programs administered in the outpatient setting.
596 Circulation August 10, 2010
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

Mehra, Christopher M. O'Connor, Dwight Reynolds, Mary Norine Walsh and Clyde W. YancyGheorghiade, J. Thomas Heywood, Mark L. McBride, Patches Johnson Inge, Mandeep R.
Gregg C. Fonarow, Nancy M. Albert, Anne B. Curtis, Wendy Gattis Stough, MihaiTherapies in the Outpatient Setting (IMPROVE HF)
Primary Results of the Registry to Improve the Use of Evidence-Based Heart Failure Improving Evidence-Based Care for Heart Failure in Outpatient Cardiology Practices:
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2010 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.109.9344712010;122:585-596; originally published online July 26, 2010;Circulation.
http://circ.ahajournals.org/content/122/6/585World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2010/07/22/CIRCULATIONAHA.109.934471.DC1Data Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

SUPPLEMENTAL MATERIALS
Appendix Table 1. IMPROVE HF Quality Measures
Use of ACEI and/or ARB: Prescription of ACEI or ARB for patients with LVSD in the outpatient setting
Use of angiotensin-converting enzyme inhibitor (ACEI) and/or angiotensin receptor blocker (ARB) in eligible patients with LVSD and without documented contraindications, intolerance, or other medical reason(s) (eg, allergy, symptomatic hypotension, hyperkalemia, pregnancy) for not prescribing; without patient reason(s) for not prescribing (eg, patient refusal); and without system reason(s) for not prescribing (eg, financial) for ACEI and ARB therapy.
Use of beta-blocker: Prescription of beta-blockers for patients with LVSD in the outpatient setting
Use of beta-blocker in eligible patients with LVSD and without documented contraindications, intolerance, or other medical reason(s) (eg, allergy, asthma, symptomatic hypotension, symptomatic bradycardia, 2nd- or 3rd-degree heart block without a pacemaker) for not prescribing; without patient reason(s) for not prescribing (eg, patient refusal); and without system reason(s) for not prescribing (eg, financial).
Use of aldosterone receptor antagonist: Prescription of aldosterone receptor antagonists for patients with HF and LVSD in the outpatient setting
Use of aldosterone receptor antagonist in eligible patients with LVSD and NYHA Functional Class III or IV HF and without documented contraindications, intolerance, or other medical reason(s) (eg, allergy, hyperkalemia, creatinine >2.5 mg/dL in men or >2.0 mg/dL in women) for not prescribing; without patient reason(s) for not prescribing (eg, patient refusal, compliance); and without system reason(s) for not prescribing (eg, financial, close monitoring could not be assured).
Use of anticoagulation therapy: Prescription of anticoagulation therapy for patients with chronic or paroxysmal atrial fibrillation and LVSD in the outpatient setting
Use of anticoagulation therapy in eligible patients with paroxysmal or chronic atrial fibrillation without documented contraindications, intolerance, or other medical reason(s) (eg, allergy, bleeding disorder, high risk of bleeding) for not prescribing; without patient reason(s) for not prescribing (eg, patient refusal, compliance); and without system reason(s) for not prescribing (eg, financial, close monitoring could not be assured).
Use of ICD or CRT defibrillator device (CRT-D): Prescription of ICD for patients with NYHA Class II or III HF and a quantitative LVEF ≤ 35% or prior MI or NYHA Class I HF and a quantitative LVEF ≤ 30% in the outpatient setting
Use of an implantable cardioverter defibrillator in eligible patients with 1) LVEF ≤ 35% and NYHA Class II or III HF or 2) LVEF ≤ 30% post myocardial infarction with NYHA Class I

HF without documented contraindications or other medical reason(s) (e.g. Class IV heart failure, contraindications to standard pacing such as infection or anatomy not suitable, medical condition which would limit one year survival) for not prescribing; without patient reason(s) for not prescribing (eg, patient refusal); and without system reason(s) for not prescribing (eg, financial).
Use of CRT: Prescription* of CRT for patients with NYHA class III or IV HF, QRS ≥ 120 milliseconds, and a quantitative LVEF ≤ 35% in the outpatient setting
Use of cardiac resynchronization therapy in eligible patients with LVEF ≤ 35%, QRS duration ≥ 120 ms, and NYHA Class III or ambulatory Class IV HF without documented contraindications or other medical reason(s) (eg, contraindications to standard pacing such as infection or anatomy not suitable) for not prescribing; without patient reason(s) for not prescribing (eg, patient refusal); and without system reason(s) for not prescribing (eg, financial).
Documentation of HF education provided to patients: Documentation of HF education provided to patients with HF in the outpatient setting
Documentation that written and/or verbal HF education on disease management (including one or more of the following: discussion of salt-restricted diet, monitoring of daily weight, warning signs of worsened heart failure with action plan, medication instructions including side effects, and activity recommendations) was provided to eligible patients on one or more visits within a 6-month period.
*Prescription of device therapy reflects device implantation. ACEI indicates angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CRT, cardiac resynchronization therapy; CRT-D, CRT defibrillator device; HF, heart failure; ICD, implantable cardioverter-defibrillator; LVEF, left ventricular ejection fraction; LVSD, left ventricular systolic dysfunction; MI, myocardial infarction; NYHA, New York Heart Association. For the detailed IMPROVE HF measure specifications, please see Fonarow GC, Yancy CW, Albert NM, Curtis AB, Gattis Stough W, Gheorghiade M, Heywood JT, Mehra M, O’Connor CM, Reynolds D, Walsh MN. Improving the use of evidence-based heart failure therapies in the outpatient setting: the IMPROVE HF performance improvement registry. Am Heart J. 2007;154:12-38.
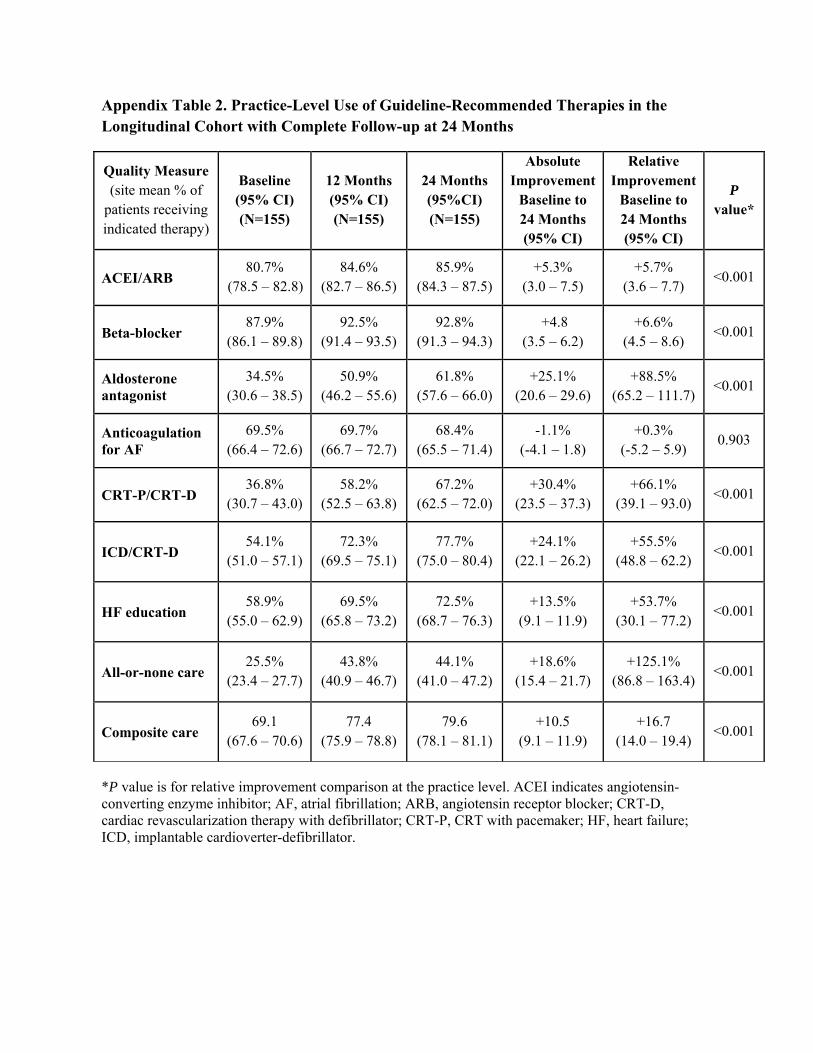
Appendix Table 2. Practice-Level Use of Guideline-Recommended Therapies in the Longitudinal Cohort with Complete Follow-up at 24 Months
Quality Measure (site mean % of
patients receiving indicated therapy)
Baseline (95% CI) (N=155)
12 Months (95% CI) (N=155)
24 Months (95%CI) (N=155)
Absolute Improvement
Baseline to 24 Months (95% CI)
Relative Improvement
Baseline to 24 Months (95% CI)
P value*
ACEI/ARB 80.7%
(78.5 – 82.8) 84.6%
(82.7 – 86.5) 85.9%
(84.3 – 87.5) +5.3%
(3.0 – 7.5) +5.7%
(3.6 – 7.7) <0.001
Beta-blocker 87.9%
(86.1 – 89.8) 92.5%
(91.4 – 93.5) 92.8%
(91.3 – 94.3) +4.8
(3.5 – 6.2) +6.6%
(4.5 – 8.6) <0.001
Aldosterone antagonist
34.5% (30.6 – 38.5)
50.9% (46.2 – 55.6)
61.8% (57.6 – 66.0)
+25.1% (20.6 – 29.6)
+88.5% (65.2 – 111.7)
<0.001
Anticoagulation for AF
69.5% (66.4 – 72.6)
69.7% (66.7 – 72.7)
68.4% (65.5 – 71.4)
-1.1% (-4.1 – 1.8)
+0.3% (-5.2 – 5.9)
0.903
CRT-P/CRT-D 36.8%
(30.7 – 43.0) 58.2%
(52.5 – 63.8) 67.2%
(62.5 – 72.0) +30.4%
(23.5 – 37.3) +66.1%
(39.1 – 93.0) <0.001
ICD/CRT-D 54.1%
(51.0 – 57.1) 72.3%
(69.5 – 75.1) 77.7%
(75.0 – 80.4) +24.1%
(22.1 – 26.2) +55.5%
(48.8 – 62.2) <0.001
HF education 58.9%
(55.0 – 62.9) 69.5%
(65.8 – 73.2) 72.5%
(68.7 – 76.3) +13.5%
(9.1 – 11.9) +53.7%
(30.1 – 77.2) <0.001
All-or-none care 25.5%
(23.4 – 27.7) 43.8%
(40.9 – 46.7) 44.1%
(41.0 – 47.2) +18.6%
(15.4 – 21.7) +125.1%
(86.8 – 163.4) <0.001
Composite care 69.1
(67.6 – 70.6) 77.4
(75.9 – 78.8) 79.6
(78.1 – 81.1) +10.5
(9.1 – 11.9) +16.7
(14.0 – 19.4) <0.001
*P value is for relative improvement comparison at the practice level. ACEI indicates angiotensin-converting enzyme inhibitor; AF, atrial fibrillation; ARB, angiotensin receptor blocker; CRT-D, cardiac revascularization therapy with defibrillator; CRT-P, CRT with pacemaker; HF, heart failure; ICD, implantable cardioverter-defibrillator.

Appendix Table 3. Improvement in Quality Measures by Practice Use of Electronic Health Records Including Only Patients with Baseline and 24-Month Data
Quality Measure Paper (N= 61 Practices)
EHR (N = 78 Practices)
Paper at Baseline Switching to EHR
(N = 15 Practices)
P value*
Baseline (95% CI) (n = 2809)
24 Months (95% CI) (n = 2809)
Absolute Change From
Baseline
Baseline (95% CI) (n = 4056)
24 Months (95% CI)
(n = 4056)
Absolute Change From
Baseline
Baseline (95% CI) (n = 700)
24 Months (95% CI) (n = 700)
Absolute Change
from Baseline
Baseline EHR vs P P to E vs P
24 Months EHR vs P P to E vs P
Absolute Change
EHR vs P P to E vs P
ACEI/ARB 82.0% (80.6 - 83.5)
86.5% (85.1 – 87.9)
+4.4% (2.4 – 6.5)
83.7% (82.5 – 84.9)
86.5% (85.3 – 87.7)
+2.8% (1.1 - 4.4)
81.6% (78.6 – 84.6)
86.7% (83.9 – 89.6)
+5.2% (1.1 – 9.3)
0.085 0.775
0.968 0.890
0.221 0.749
Beta-blocker 90.0% (88.8 – 91.1)
93.3% (92.3 – 94.3)
+3.3% (1.8 – 4.8)
88.0% (86.9 – 89.0)
94.1% (93.3 – 94.9)
+6.1% (4.8 – 7.4)
85.2% (82.4 – 88.0)
91.9% (89.7 – 94.1)
+6.7% (3.1 – 10.2)
0.014 0.001
0.193 0.247
0.006 0.088
Aldosterone antagonist
34.3% (30.2 – 38.5)
58.0% (53.3 – 62.6)
+23.6% (17.4 – 29.8)
36.6% (33.1 – 40.2)
63.8% (60.3 – 67.2)
+27.1% (22.2 – 32.1)
32.1% (21.9 – 42.3)
63.0% (53.9 – 72.1)
+30.9% (17.2 – 44.5)
0.426 0.800
0.048 0.383
0.385 0.343
Anticoagulation for AF
69.8% (66.5 – 73.1)
66.2% (63.3 – 69.2)
-3.5% (-8.0 – 0.9)
73.9% (71.3 – 76.5)
70.8% (68.5 – 73.1)
-3.1% (-6.6 – 0.3)
73.3% (66.9 – 79.8)
73.3% (67.9 – 78.8)
0.0% (-8.4 – 8.4)
0.057 0.364
0.020 0.035
0.885 0.467
CRT-P/CRT-D 46.9% (40.9 – 52.8)
69.7% (65.2 – 74.1)
+22.8% (15.4 – 30.2)
37.9% (32.9 – 43.0)
66.2% (62.4 – 70.0)
+28.3% (22.0 – 34.6)
36.6% (21.8 – 51.3)
77.2% (68.6 -85.8)
+40.6% (23.5 – 57.6)
0.027 0.242
0.272 0.164
0.269 0.061
ICD/CRT-D 57.1% (54.9 – 59.3)
79.7% (78.0 – 81.5)
+22.6% (19.8 – 25.5)
52.0% (50.1 – 53.9)
78.7% (77.2 – 80.2)
+26.7% (24.3 – 29.1)
59.5% (54.9-64.2)
80.2% (76.7 – 83.8)
+20.7% (14.9 – 26.6)
<0.001 0.385
0.388 0.850
0.033 0.565
HF education 55.6% (53.7 – 57.4)
66.5% (64.8 – 68.3)
+11.0% (8.4 – 13.5)
64.6% (63.2 – 66.1)
75.8% (74.5 – 77.1)
+11.1% (9.2 – 13.1)
46.4% (42.7 – 50.1)
58.4% (54.8 – 62.1)
+12.0% (6.8 – 17.2)
<0.001 <0.001
<0.001 <0.001
0.913 0.726
*P value is based on large sample test of proportions and evaluates the difference in percent at baseline, 24 months, and absolute change from baseline to 24 months between practice types. ACEI indicates angiotensin-converting enzyme inhibitor; AF, atrial fibrillation; ARB, angiotensin receptor blocker; CRT-D, cardiac revascularization therapy with defibrillator; CRT-P, CRT with pacemaker; E, electronic; EHR, electronic health record; HF, heart failure; ICD, implantable cardioverter-defibrillator; P, paper.

Appendix Table 4. Odds Ratios for the Use of Guideline-Recommended Therapies in the Longitudinal Cohort with Complete Follow-up at 24 Months Relative to Baseline in GEE Models
Quality Measure Unadjusted
OR 95% CI P value
Adjusted OR
95% CI P value
ACEI/ARB 1.079 0.993-1.172 0.0715 1.108 0.985-1.247 0.0889
Beta-blocker 1.680 1.513-1.865 <0.0001 1.678 1.474-1.910 <0.0001
Aldosterone antagonist
1.836 1.538-2.192 <0.0001 2.102 1.610-2.744 <0.0001
Anticoagulation for AF
1.040 0.952-1.135 0.3873 1.053 0.949-1.168 0.3302
CRT-P/CRT-D 4.092 3.167-5.286 <0.0001 6.500 4.386-9.633 <0.0001
ICD/CRT-D 2.401 2.243-2.571 <0.0001 2.523 2.229-2.854 <0.0001
HF education 1.642 1.540-1.750 <0.0001 1.725 1.582-1.881 <0.0001
All-or-none care 2.182 2.049-2.324 <0.0001 2.360 2.152-2.587 <0.0001
Model controlled for within-patient and within-practice correlations. The multivariate model included all patient and practice characteristics that were significant at the P < 0.10 level in univariate analysis. ACEI indicates angiotensin-converting enzyme inhibitor; AF, atrial fibrillation; ARB, angiotensin receptor blocker; CI, confidence interval; CRT-D, cardiac resynchronization therapy with defibrillator; CRT-P, CRT with pacemaker; GEE, general estimating equation; HF, heart failure; ICD, implantable cardioverter-defibrillator; OR, odds ratio.
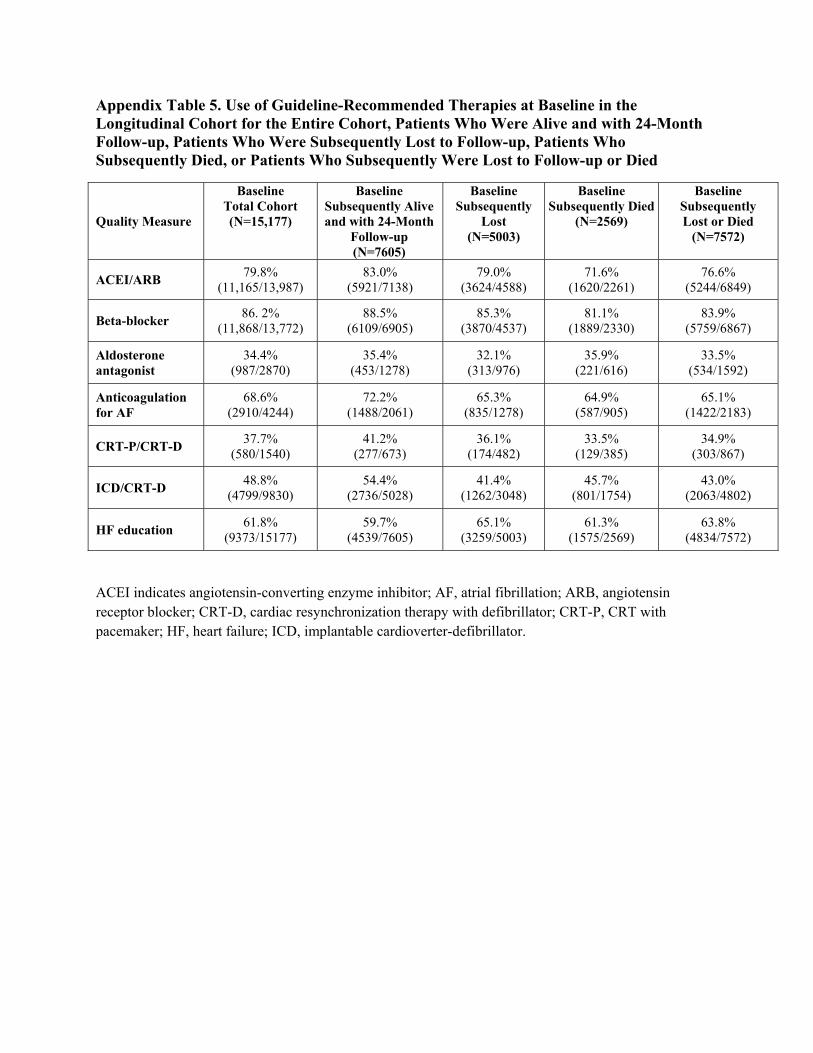
Appendix Table 5. Use of Guideline-Recommended Therapies at Baseline in the Longitudinal Cohort for the Entire Cohort, Patients Who Were Alive and with 24-Month Follow-up, Patients Who Were Subsequently Lost to Follow-up, Patients Who Subsequently Died, or Patients Who Subsequently Were Lost to Follow-up or Died
Quality Measure
Baseline Total Cohort (N=15,177)
Baseline Subsequently Alive and with 24-Month
Follow-up (N=7605)
Baseline Subsequently
Lost (N=5003)
Baseline Subsequently Died
(N=2569)
Baseline Subsequently Lost or Died
(N=7572)
ACEI/ARB 79.8% (11,165/13,987)
83.0% (5921/7138)
79.0% (3624/4588)
71.6% (1620/2261)
76.6% (5244/6849)
Beta-blocker 86. 2% (11,868/13,772)
88.5% (6109/6905)
85.3% (3870/4537)
81.1% (1889/2330)
83.9% (5759/6867)
Aldosterone antagonist
34.4% (987/2870)
35.4% (453/1278)
32.1% (313/976)
35.9% (221/616)
33.5% (534/1592)
Anticoagulation for AF
68.6% (2910/4244)
72.2% (1488/2061)
65.3% (835/1278)
64.9% (587/905)
65.1% (1422/2183)
CRT-P/CRT-D 37.7% (580/1540)
41.2% (277/673)
36.1% (174/482)
33.5% (129/385)
34.9% (303/867)
ICD/CRT-D 48.8% (4799/9830)
54.4% (2736/5028)
41.4% (1262/3048)
45.7% (801/1754)
43.0% (2063/4802)
HF education 61.8% (9373/15177)
59.7% (4539/7605)
65.1% (3259/5003)
61.3% (1575/2569)
63.8% (4834/7572)
ACEI indicates angiotensin-converting enzyme inhibitor; AF, atrial fibrillation; ARB, angiotensin receptor blocker; CRT-D, cardiac resynchronization therapy with defibrillator; CRT-P, CRT with pacemaker; HF, heart failure; ICD, implantable cardioverter-defibrillator.

Appendix Table 6. Use of Guideline-Recommended Therapies at Baseline and 24 Months in the Longitudinal Cohort with Complete Follow-up at 24 Months Stratified by Age Groups
Quality Measure Age Groups Baseline 24 Months HeterogeneityP value*
ACEI/ARB
<50 87.6% (588/671)
91.0% (565/621)
0.0683
50-59 86.9% (985/1134)
91.5% (921/1007)
60-69 85.5% (1603/1874)
88.1% (1461/1658)
70-79 80.9% (1770/2188)
85.4% (1567/1835)
>80 76.7% (971/1266)
78.6% (831/1057)
Beta-blocker
<50 94.0% (598/636)
95.5% (568/595)
0.1279
50-59 91.7% (1002/1093)
95.5% (1008/1056)
60-69 88.5% (1609/1819)
94.2% (1612/1711)
70-79 87.3% (1848/2117)
93.3% (1912/2049)
>80 84.8% (1047/1235)
90.8% (1082/1192)
Aldosterone Antagonist
<50 54.0% (74/137)
79.9% (135/169)
0.7148
50-59 44.0% (95/216)
72.8% (171/235)
60-69 36.8% (118/321)
62.6% (189/302)
70-79 29.4% (109/371)
56.2% (196/349)
>80 24.6% (57/232)
45.5% (107/235)
Anticoagulation for AF
<50 71.1% (64/90)
64.3% (90/140)
0.7318
50-59 72.2% (151/209)
69.3% (201/290)
60-69 73.8% (361/489)
70.9% (482/680)
70-79 75.0% (572/763)
73.2% (714/976)
>80 66.7% (340/510)
62.7 (396/632)
CRT-P/CRT-D
<50 53.7% (22/41)
59.5% (44/74)
0.1760 50-59 39.0% (32/82)
74.3% (101/136)
60-69 41.9% 72.7%

(72/172) (202/278) 70-79 43.5%
(100/230) 66.8%
(253/379) >80 34.5%
(51/148) 65.9%
(151/229)
ICD/CRT-D
<50 51.4% (235/457)
80.8% (367/454)
<0.0001
50-59 54.8% (439/801)
82.8% (670/809)
60-69 58.7% (776/1321)
82.1% (1167/1421)
70-79 56.8% (884/1555)
81.7% (1373/1681)
>80 45.1% (402/892)
66.3% (639/964)
HF education
<50 65.6% (458/698)
77.9% (544/698)
0.6188
50-59 63.4% (760/1199)
74.7% (896/1199)
60-69 61.4% (1216/1981)
70.9% (1404/1981)
70-79 57.4% (1344/2343)
69.3% (1624/2343)
>80 55.0% (758/1379)
66.4% (916/1379)
*P value is for heterogeneity for relative improvement comparison between baseline and 24 months among the age groups. ACEI indicates angiotensin-converting enzyme inhibitor; AF, atrial fibrillation; ARB, angiotensin receptor blocker; CRT-D, cardiac resynchronization therapy with defibrillator; CRT-P, CRT with pacemaker; HF, heart failure; ICD, implantable cardioverter-defibrillator.
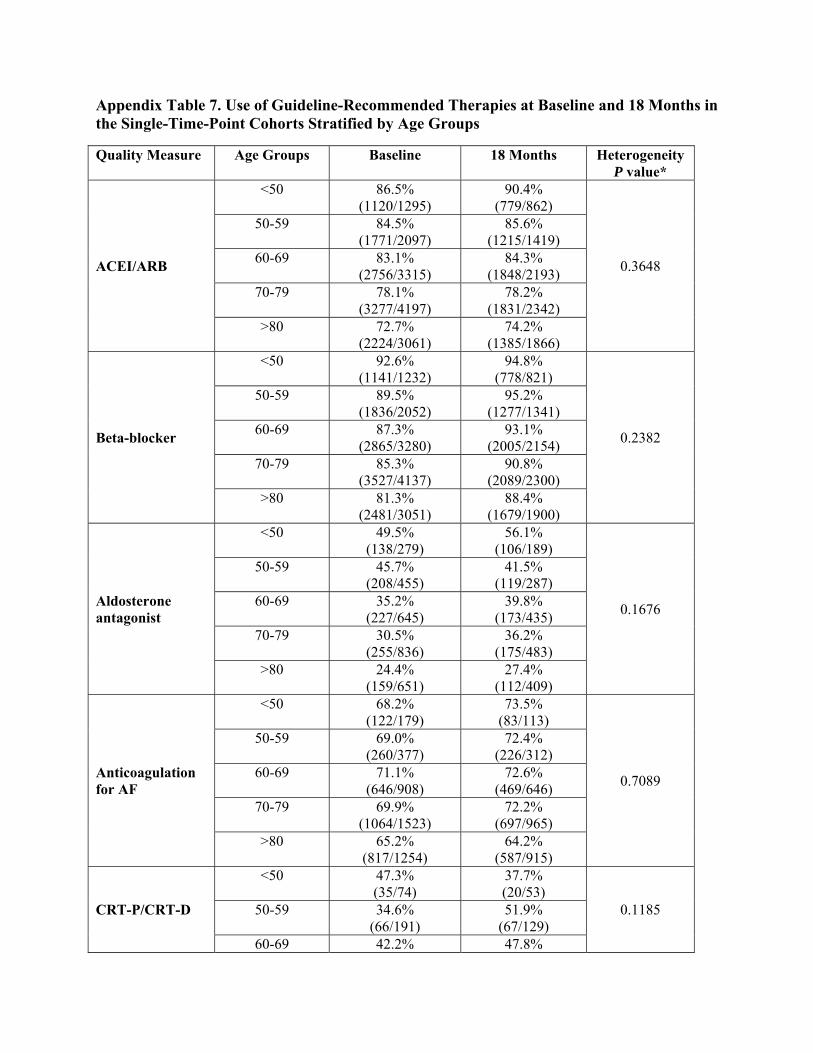
Appendix Table 7. Use of Guideline-Recommended Therapies at Baseline and 18 Months in the Single-Time-Point Cohorts Stratified by Age Groups
Quality Measure
Age Groups
Baseline
18 Months
Heterogeneity P value*
ACEI/ARB
<50 86.5% (1120/1295)
90.4% (779/862)
0.3648
50-59 84.5% (1771/2097)
85.6% (1215/1419)
60-69 83.1% (2756/3315)
84.3% (1848/2193)
70-79 78.1% (3277/4197)
78.2% (1831/2342)
>80 72.7% (2224/3061)
74.2% (1385/1866)
Beta-blocker
<50 92.6% (1141/1232)
94.8% (778/821)
0.2382
50-59 89.5% (1836/2052)
95.2% (1277/1341)
60-69 87.3% (2865/3280)
93.1% (2005/2154)
70-79 85.3% (3527/4137)
90.8% (2089/2300)
>80 81.3% (2481/3051)
88.4% (1679/1900)
Aldosterone antagonist
<50 49.5% (138/279)
56.1% (106/189)
0.1676
50-59 45.7% (208/455)
41.5% (119/287)
60-69 35.2% (227/645)
39.8% (173/435)
70-79 30.5% (255/836)
36.2% (175/483)
>80 24.4% (159/651)
27.4% (112/409)
Anticoagulation for AF
<50 68.2% (122/179)
73.5% (83/113)
0.7089
50-59 69.0% (260/377)
72.4% (226/312)
60-69 71.1% (646/908)
72.6% (469/646)
70-79 69.9% (1064/1523)
72.2% (697/965)
>80 65.2% (817/1254)
64.2% (587/915)
CRT-P/CRT-D
<50 47.3% (35/74)
37.7% (20/53)
0.1185 50-59 34.6% (66/191)
51.9% (67/129)
60-69 42.2% 47.8%

(138/327) (128/268) 70-79 40.8%
(216/530) 45.6%
(145/318) >80 29.9%
(124/415) 36.1%
(96/266)
ICD/CRT-D
<50 44.3% (371/838)
48.0% (289/602)
0.2419
50-59 50.7% (728/1436)
55.8% (584/1046)
60-69 54.6% (1276/2338)
60.7% (1044/1721)
70-79 52.9% (1577/2981)
62.3% (1194/1917)
>80 37.9% (845/2230)
45.7% (718/1570)
HF education
<50 69.5% (942/1355)
82.1% (759/925)
0.2775
50-59 65.1% (1458/2239)
80.4% (1211/1506)
60-69 63.4% (2272/3581)
76.8% (1831/2384)
70-79 60.0% (2749/4583)
74.4% (1959/2634)
>80 57.1% (1937/3391)
70.8% (1549/2189)
*P value is for heterogeneity for relative improvement comparison between baseline and 18 months among the age groups. ACEI indicates angiotensin-converting enzyme inhibitor; AF, atrial fibrillation; ARB, angiotensin receptor blocker; CRT-D, cardiac resynchronization therapy with defibrillator; CRT-P, CRT with pacemaker; HF, heart failure; ICD, implantable cardioverter-defibrillator.

Appendix Table 8. Practice-Level Use of Guideline-Recommended Therapies at Baseline, 6 Months, and 18 Months in the Single-Time-Point Cohorts
Quality Measure (site mean % of patients receiving indicated therapy)
Baseline (95% CI) (N=167)
6 Months (95% CI) (N=154)
18 Months (95% CI) (N=150)
Absolute Improvement
Baseline to 18 Months (95% CI)
Relative Improvement
Baseline to 18 months (95% CI)
P value*
ACEI/ARB 78.7%
(76.9 – 80.5) 80.2%
(78.5 – 81.9)80.3%
(78.4 – 82.3) +1.6%
(-0.6 – 3.8) +10.5%
(-5.3 – 26.3) 0.190
Beta-blocker 85.9%
(84.2 – 87.7) 90.0%
(88.8 – 91.1)91.8%
(90.7 – 92.9) +5.9%
(4.0 – 7.7)) +14.3%
(0.1 – 28.4) 0.048
Aldosterone antagonist
34.7% (31.6 – 37.7)
33.4% (30.0 – 36.9)
36.3% (32.5 – 40.1)
+1.8% (-2.7 – 6.3)
+14.9% (-0.2 – 30.0)
0.052
Anticoagulation for AF
67.9% (65.3 – 70.4)
68.9% (66.0 – 71.7)
69.6% (66.8 – 72.3)
+1.7% (-1.8 – 5.2)
+6.7% (0.5 – 13.0)
0.033
CRT-P/CRT-D 37.6%
(32.5 – 42.7) 34.9%
(30.1 – 39.6)43.5%
(38.3 – 48.7) +4.9%
(-1.8 – 11.5) +39.1%
(9.4 – 68.8) 0.010
ICD/CRT-D 49.9%
(47.2 – 52.7) 52.7%
(49.9 – 55.5)54.0%
(51.2 – 56.8) +4.1%
(1.2 – 7.0) +17.6%
(9.3 – 25.8) <0.001
HF education 59.4%
(55.6 – 63.2) 67.5%
(64.1 – 70.8)75.0%
(71.4 – 78.6) +15.6%
(11.2 – 20.0) +59.5%
(33.9 – 85.2) <0.001
All-or-none care 23.5%
(21.6 – 25.3) 27.6%
(25.6 – 29.6)32.3%
(30.0 – 34.5) +8.8%
(6.3 – 11.3) +96.5%
(52.1 – 141.0) <0.001
Composite care 67.1%
(65.7 – 68.5) 70.7%
(69.4 – 72.0)73.2%
(71.9 – 74.6) +6.1%
(4.5 – 7.6) +10.6%
(7.6 – 13.6) <0.001
*P value is for relative improvement comparison between baseline and 18 months at the practice level. ACEI indicates angiotensin-converting enzyme inhibitor; AF, atrial fibrillation; ARB, angiotensin receptor blocker; CRT-D, cardiac revascularization therapy with defibrillator; CRT-P, CRT with pacemaker; HF, heart failure; ICD, implantable cardioverter-defibrillator.

Appendix Table 9. Odds Ratios for Use of Guideline-Recommended Therapies in the 18-Month Single-Point-in-Time Cohort Relative to the Baseline Cohort in GEE Models*
Quality Measure Unadjusted
OR 95% CI P value
Adjusted OR
95% CI P value
ACEI/ARB 1.079 1.008-1.156 0.0284 1.036 0.941-1.140 0.4745
Beta-blocker 1.736 1.580-1.907 <0.0001 1.685 1.474-1.927 <0.0001
Aldosterone antagonist
1.107 0.975-1.257 0.1166 1.018 0.875-1.183 0.8194
Anticoagulation for AF
1.063 0.958-1.180 0.2489 1.025 0.894-1.174 0.7243
CRT-P/CRT-D 1.334 1.132-1.573 0.0006 1.361 1.136-1.629 0.0008
ICD/CRT-D 1.310 1.231-1.395 <0.0001 1.269 1.138-1.415 <0.0001
HF education 2.024 1.910-2.146 <0.0001 2.072 1.894-2.267 <0.0001
All-or-none care 1.552 1.464-1.645 <0.0001 1.684 1.568-1.810 <0.0001
*Models controlled for within-practice correlations. The multivariate model included all patient and practice characteristics that were significant at the P<0.10 level in univariate analysis. ACEI indicates angiotensin-converting enzyme inhibitor; AF, atrial fibrillation; ARB, angiotensin receptor blocker; CI, confidence interval; CRT-D, cardiac revascularization therapy with defibrillator; CRT-P, CRT with pacemaker; HF, heart failure; ICD, implantable cardioverter-defibrillator; OR, odds ratio.
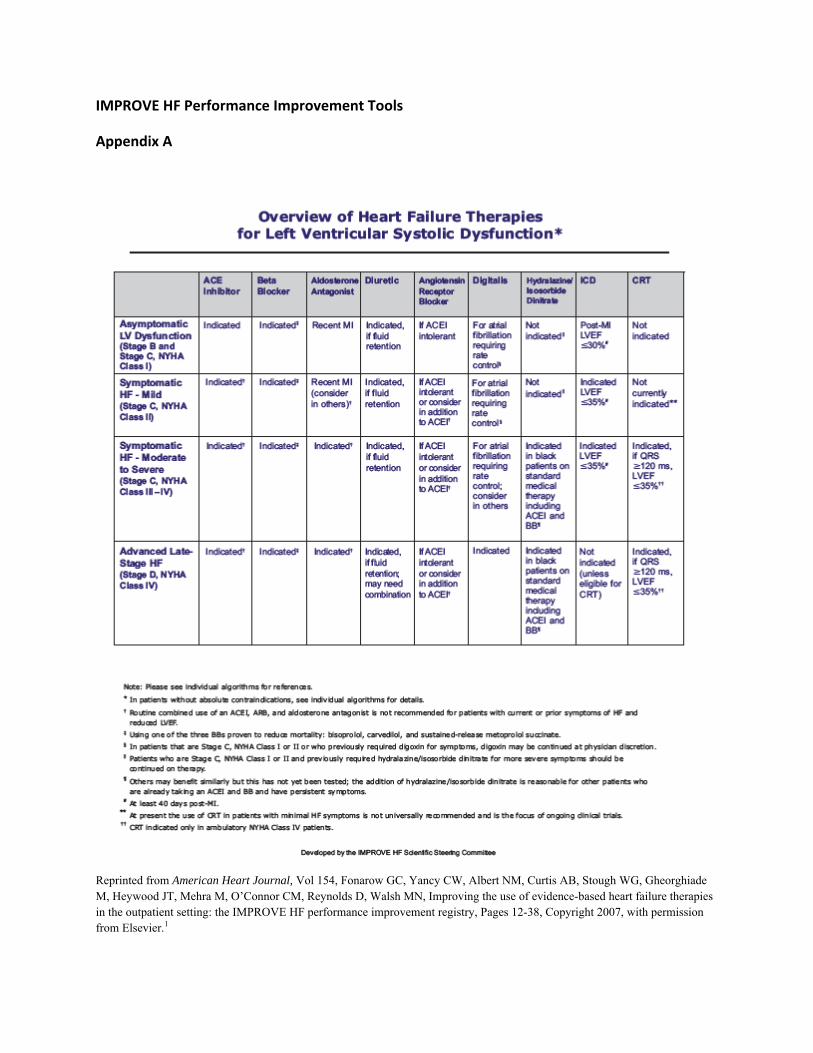
IMPROVE HF Performance Improvement Tools
Appendix A
Reprinted from American Heart Journal, Vol 154, Fonarow GC, Yancy CW, Albert NM, Curtis AB, Stough WG, Gheorghiade M, Heywood JT, Mehra M, O’Connor CM, Reynolds D, Walsh MN, Improving the use of evidence-based heart failure therapies in the outpatient setting: the IMPROVE HF performance improvement registry, Pages 12-38, Copyright 2007, with permission from Elsevier.1
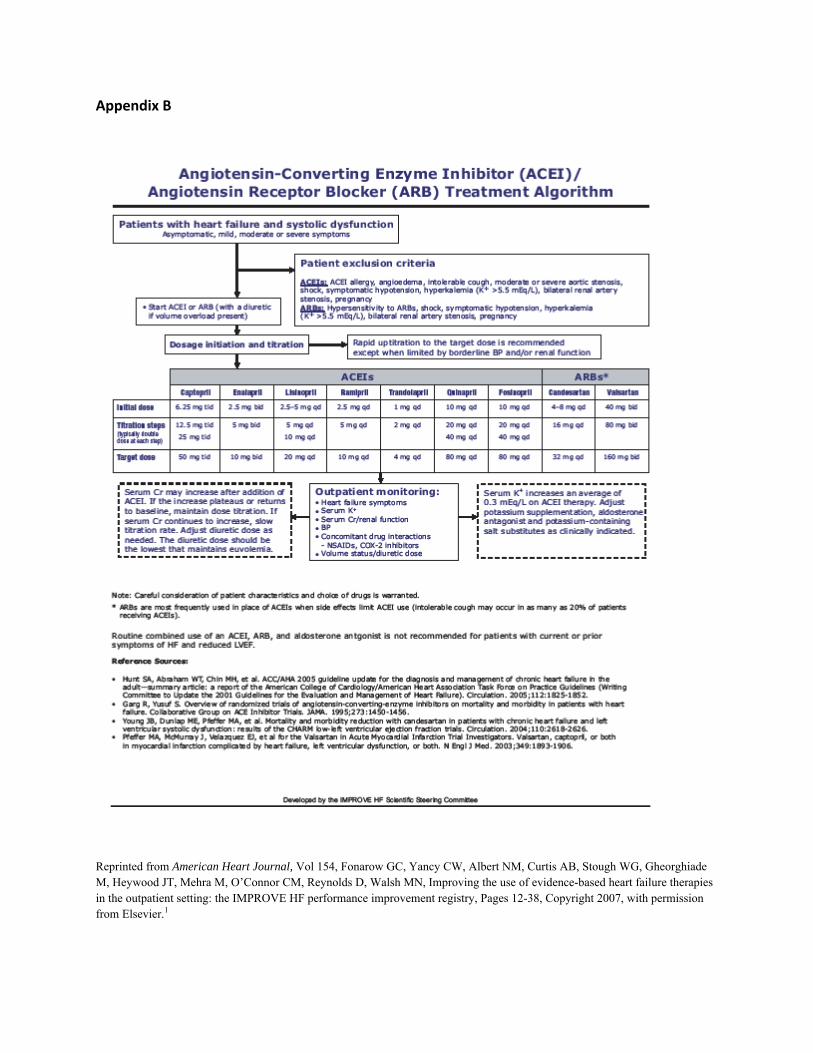
Appendix B
Reprinted from American Heart Journal, Vol 154, Fonarow GC, Yancy CW, Albert NM, Curtis AB, Stough WG, Gheorghiade M, Heywood JT, Mehra M, O’Connor CM, Reynolds D, Walsh MN, Improving the use of evidence-based heart failure therapies in the outpatient setting: the IMPROVE HF performance improvement registry, Pages 12-38, Copyright 2007, with permission from Elsevier.1

Appendix C
Reprinted from American Heart Journal, Vol 154, Fonarow GC, Yancy CW, Albert NM, Curtis AB, Stough WG, Gheorghiade M, Heywood JT, Mehra M, O’Connor CM, Reynolds D, Walsh MN, Improving the use of evidence-based heart failure therapies in the outpatient setting: the IMPROVE HF performance improvement registry, Pages 12-38, Copyright 2007, with permission from Elsevier.1

Appendix D
Reprinted from American Heart Journal, Vol 154, Fonarow GC, Yancy CW, Albert NM, Curtis AB, Stough WG, Gheorghiade M, Heywood JT, Mehra M, O’Connor CM, Reynolds D, Walsh MN, Improving the use of evidence-based heart failure therapies in the outpatient setting: the IMPROVE HF performance improvement registry, Pages 12-38, Copyright 2007, with permission from Elsevier.1

Appendix E
Reprinted from American Heart Journal, Vol 154, Fonarow GC, Yancy CW, Albert NM, Curtis AB, Stough WG, Gheorghiade M, Heywood JT, Mehra M, O’Connor CM, Reynolds D, Walsh MN, Improving the use of evidence-based heart failure therapies in the outpatient setting: the IMPROVE HF performance improvement registry, Pages 12-38, Copyright 2007, with permission from Elsevier.1

Appendix F
Reprinted from American Heart Journal, Vol 154, Fonarow GC, Yancy CW, Albert NM, Curtis AB, Stough WG, Gheorghiade M, Heywood JT, Mehra M, O’Connor CM, Reynolds D, Walsh MN, Improving the use of evidence-based heart failure therapies in the outpatient setting: the IMPROVE HF performance improvement registry, Pages 12-38, Copyright 2007, with permission from Elsevier.1
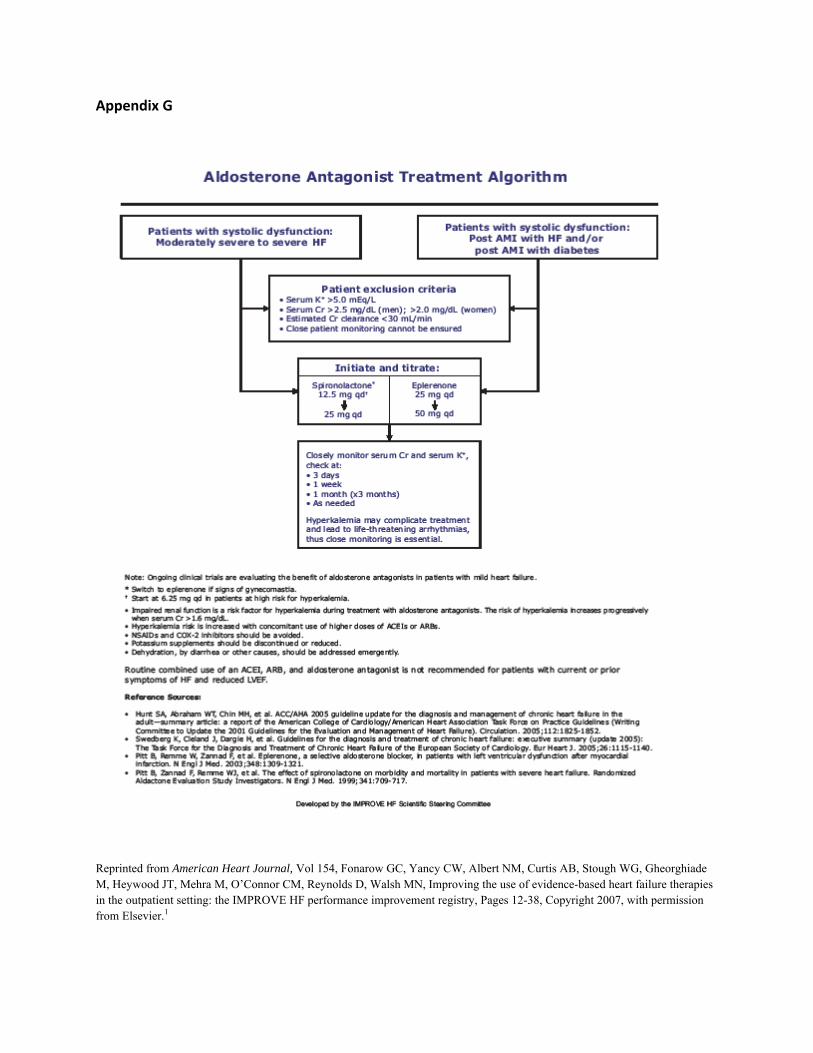
Appendix G
Reprinted from American Heart Journal, Vol 154, Fonarow GC, Yancy CW, Albert NM, Curtis AB, Stough WG, Gheorghiade M, Heywood JT, Mehra M, O’Connor CM, Reynolds D, Walsh MN, Improving the use of evidence-based heart failure therapies in the outpatient setting: the IMPROVE HF performance improvement registry, Pages 12-38, Copyright 2007, with permission from Elsevier.1

Appendix H
Reprinted from American Heart Journal, Vol 154, Fonarow GC, Yancy CW, Albert NM, Curtis AB, Stough WG, Gheorghiade M, Heywood JT, Mehra M, O’Connor CM, Reynolds D, Walsh MN, Improving the use of evidence-based heart failure therapies in the outpatient setting: the IMPROVE HF performance improvement registry, Pages 12-38, Copyright 2007, with permission from Elsevier.1

Appendix I. Initial Visit Patient Assessment
Age/date of birth: ____________________ Cardiologist: ________________________ Main complaint at visit: Gender: Male FemaleWeight: Heart rate:
Blood pressure:
Ejection fraction (LVEF):
Race/ethnicity: Caucasian Asian Hispanic
Black/African American Native Hawaiian/Other Pacific Islander American Indian/Alaska Native
Insurance coverage:
Medicare Medicaid Military HMO Private None
Prescription plan:
Yes No
Recent hospitalizations:
Describe reason(s):
Comorbidities/ additional risk factors:
Hypertension CAD
HF etiology: Ischemic Non ischemic
Diabetes Cerebrovascular accident Arthritis
Renal disease Sleep apnea/sleeping
disorder Allergies Asthma/reactive airway
disease Alcohol/drug abuse Smoking Anemia
COPD Gout Depression Peripherial vascular
disease Alzheimer’s
disease/dementia Valve dysfunction Other _______
Atrial fibrillation status:
Permanent
Paroxysmal in AFIB Paroxysmal in NSR
Never
QRS duration: NYHA class: Class I Class II Class III Class IV Device therapy: DDD pacer VVI pacer CRT CRT-D ICD Other _______
Current medications:
Please specify name, dosage, and frequency:

Appendix J. Final Visit Patient Assessment
Age/date of birth: Initial diagnosis:
EF: Date EF was obtained: ____ /____ /_________
Date of visit:
____ /____ /_____
____ /____ /_____
____ /____ /_____
____ /____ /_____
Clinical assessment
Recent hospitalizations:
Describe reason(s):
Describe reason(s): Describe reason(s):
Describe reason(s):
Weight:
_______________ lbs
_______________ lbs
___________________ lbs
_______________ lbs
Heart rate (resting):
_______________ bpm
_______________ bpm
___________________ bpm
_______________ bpm
Blood pressure:
_______________ mmHg
_______________ mmHg
__________________ mmHg
_______________ mmHg
QRS duration:
Atrial fibrillation status:
Permanent Paroxysmal in AFib Paroxysmal NSR Never
Permanent Paroxysmal in AFib Paroxysmal NSR Never
Permanent Paroxysmal in AFib Paroxysmal NSR Never
Permanent Paroxysmal in AFib Paroxysmal NSR Never
Tests performed (LVEF):
Echo MUGA
EF_________________
Echo MUGA
EF_________________
Echo MUGA
EF_________________
Echo MUGA
EF_________________
Symptoms of volume overload:
Dyspnea Fatigue Orthopnea Other
Dyspnea Fatigue Orthopnea Other
Dyspnea Fatigue Orthopnea Other
Dyspnea Fatigue Orthopnea Other
Assessment of clinical signs of volume overload:
Peripheral edema Rales Hepatomegaly Ascites Jugular venous pressure Other
Peripheral edema Rales Hepatomegaly Ascites Jugular venous pressure Other
Peripheral edema Rales Hepatomegaly Ascites Jugular venous pressure Other
Peripheral edema Rales Hepatomegaly Ascites Jugular venous pressure Other

Lab tests: Please specify results:
CBC __________ BUN __________ Glucose __________ Sodium __________ Potassium __________ Creatinine __________ TSH __________ BNP __________ LDL __________ Other __________
Please specify results:
CBC __________ BUN __________ Glucose __________ Sodium __________ Potassium __________ Creatinine __________ TSH __________ BNP __________ LDL __________ Other __________
Please specify results:
CBC __________ BUN __________ Glucose __________ Sodium __________ Potassium __________ Creatinine __________ TSH __________ BNP __________ LDL __________ Other __________
Please specify results:
CBC __________ BUN __________ Glucose __________ Sodium __________ Potassium __________ Creatinine __________ TSH __________ BNP __________ LDL __________ Other __________
NYHA Class: Class I Class II Class III Class IV
Class I Class II Class III Class IV
Class I Class II Class III Class IV
Class I Class II Class III Class IV
Recommended consults:
Please specify: Please specify: Please specify: Please specify:
__________________ Medical therapy (dose and frequency)
Beta blocker: Carvedilol ___________ Metoprolol
succinate ___________ Other ___________
Carvedilol ___________ Metoprolol
succinate ___________ Other ___________
Carvedilol ___________ Metoprolol
succinate ___________ Other ___________
Carvedilol ___________ Metoprolol
succinate ___________ Other ___________
ACE inhibitor: Specify medication ____________________
____________________
Specify medication ____________________
____________________
Specify medication ____________________
____________________
Specify medication ___________________
___________________
Angiotensin receptor blocker:
Candesartan _________ Valsartan _________ Other _________
Candesartan ________ Valsartan _________ Other _________
Candesartan ________ Valsartan _________ Other _________
Candesartan ________ Valsartan _________ Other _________
Aldosterone antagonist:
Spironolactone _______ Eplerenone ________
Spironolactone _______ Eplerenone _________
Spironolactone _______ Eplerenone ________
Spironolactone _______ Eplerenone ________
Hydralazine/Nitrate: ____________________ ____________________ ____________________ ____________________
Warfarin: Specify medication ____________________
____________________
Specify medication ____________________
____________________
Specify medication ____________________
____________________
Specify medication ____________________
____________________
Antiarrhythmic: Specify medication ____________________
____________________
Specify medication ____________________
____________________
Specify medication ____________________
____________________
Specify medication ____________________
____________________
Diuretic: Furosemide __________ Torsemide __________ Metolazone __________ HCTZ ___________ Other ___________
Furosemide __________ Torsemide __________ Metolazone __________ HCTZ ___________ Other ___________
Furosemide __________ Torsemide __________ Metolazone __________ HCTZ __________ Other __________
Furosemide __________ Torsemide __________ Metolazone __________ HCTZ __________ Other __________
Digoxin: ____________________ ____________________ ____________________ ____________________
Other: ____________________ ____________________ ____________________ ____________________

Drug intolerance(s):
Please specify:
Please specify: Please specify: Please specify:
Device therapy
Device therapy:
Please specify brand name:
CRT __________ CRT-D __________ ICD __________ DDD pacer __________ VVI pacer __________ Other __________
Please specify brand name:
CRT __________ CRT-D __________ ICD __________ DDD pacer __________ VVI pacer __________ Other __________
Please specify brand name:
CRT __________ CRT-D __________ ICD __________ DDD pacer __________ VVI pacer __________ Other __________
Please specify brand name:
CRT __________ CRT-D __________ ICD __________ DDD pacer __________ VVI pacer __________ Other __________
Date of implant:
____ /____ /_____
____ /____ /_____ ____ /____ /_____
____ /____ /_____
Notes:
Please specify:
Please specify:
Please specify:
Please specify:
ICD therapy administered:
ICD shock ATP
ICD shock ATP
ICD shock ATP
ICD shock ATP
ICD shock(s) documented:
All appropriate All inappropriate Mix
appropriate/inappropriate
All appropriate All inappropriate Mix
appropriate/inappropriate
All appropriate All inappropriate Mix
appropriate/inappropriate
All appropriate All inappropriate Mix
appropriate/inappropriate
Patient education
Patient education provided:
Diet Exercise Weight Disease process Fluid intake Smoking Medication compliance Device therapy Other ______________
Diet Exercise Weight Disease process Fluid intake Smoking Medication compliance Device therapy Other ______________
Diet Exercise Weight Disease process Fluid intake Smoking Medication compliance Device therapy Other ______________
Diet Exercise Weight Disease process Fluid intake Smoking Medication compliance Device therapy Other ______________

Appendix K. Patient Education Materials





















Appendix L. IMPROVE HF Clinical Pathway




