heat illness in sports
DESCRIPTION
Heat illness in Athletes. Treatment, heat illness classification.TRANSCRIPT

J
R
Aps
TT
1d
ournal of Science and Medicine in Sport (2007) 10, 11—26
EVIEW
systematic review of guidelines for therevention of heat illness in community-basedports participants and officials
. Larsena, S. Kumara, K. Grimmera,∗, A. Potterb,
. Farquharsonb, P. Sharpeb
a The Centre for Allied Health Evidence, University of South Australia, City East Campus, North Tce,Adelaide 5000, Australiab Sports Medicine Australia, SA, Australia
KEYWORDSSystematic review;Guidelines;Sports participants;Sports officials;Heat injury
Summary This paper presents the findings of a systematic review of guide-lines on preventing heat illness in sports participants and officials. Universitylibrary databases and Internet sources were searched for guidelines pertainingto community-based sports, and occupational health and safety, using a compre-hensive list of search terms. Guidelines were included if they met the criteriaof English language, full text and fully referenced, and dealt specifically with,or could be extrapolated to, prevention of heat illness in sports participants andofficials. Guideline inclusion was evaluated by two independent reviewers, whoalso independently assessed guideline quality using the AGREE instrument. Com-mon guideline themes were identified by synthesis and recommendations for eachtheme were extracted. A synthesis of recommendations for common themes wasthen undertaken. Thirteen eligible guidelines were included. Thirty-two guidelineswere excluded, as they did not provide sufficient information on construction orreferences. The methodological quality of the included guidelines was variable. Theevidence-base of the guidelines varied, reflecting primary and secondary research.While five common heat-illness prevention themes were identified (fluid intake,heat limits, clothing, acclimatisation, precautionary interventions), variable rec-ommendations were made pertaining to these themes. This potentially reflectedthe variable underpinning evidence of the guidelines. This review highlighted theneed for better quality guideline construction related to defensible and transparentevidence sources regarding sports participation in hot weather. The synthesised rec-
ommendations cautiously provide a framework of current best evidence upon whichsporting organisations internationally can base strategies for safe participation inthe heat.© 2006 Sports Medicine Australia. Published by Elsevier Ltd. All rights reserved.∗ Corresponding author. Tel.: +61 8 83 022 769; fax: +61 8 83 022 766.E-mail address: [email protected] (K. Grimmer).
440-2440/$ — see front matter © 2006 Sports Medicine Australia. Published by Elsevier Ltd. All rights reserved.oi:10.1016/j.jsams.2006.07.008

12 T. Larsen et al.
Contents
Background .................................................................................................. 12Method....................................................................................................... 12
Data sources............................................................................................. 13Inclusion and exclusion criteria .......................................................................... 13Guideline quality assessment ............................................................................ 13Synthesised recommendations ........................................................................... 14
Results ....................................................................................................... 14Included evidence and its quality........................................................................ 14Common themes......................................................................................... 14
Common theme 1: fluid intake .................................................................... 14Common theme 2: heat limits ..................................................................... 15Common theme 3: clothing........................................................................ 15Common theme 4: acclimatisation ................................................................ 15Common theme 5: precautionary interventions.................................................... 15
Our synthesised evidence recommendations ............................................................. 16Discussion.................................................................................................... 17Conclusion ................................................................................................... 20Practical implications ........................................................................................ 20
References ................................................................................................... 20occupational guidelines shaded) ....................... 22ss i
from which a synthesis of evidence-based recom-mendations for safe sports practice was developed.These recommendations could form the basis forcommunity sporting organisations to develop spe-
cs
M
Toiovptuemhicitdg
c
n sports participants and officials .................. 25
ific strategies to protect the health of recreationalports participants and officials.
ethod
he research team conducted a systematic reviewf eligible guidelines related to preventing heatllness during sports participation. The objectivesf the systematic review were to identify rele-ant secondary evidence (guidelines) regarding therevention of injury related to sports participa-ion and sports management in the heat, to eval-ate the methodological quality of the availablevidence, and to synthesise the guideline recom-endations into a framework of advice. A stake-
older reference group assisted the research teamn defining search terms, inclusion and exclusionriteria for the review, and in reviewing and approv-ng decisions regarding the guidelines included inhe review and synthesis of guideline recommen-ations. Key members of the stakeholder referenceroup are authors on this publication.
The search strategy terms and their definitionsomprised:
Heat: Heat measured either in Fahrenheit (F) orCelsius (C). A form of energy that is transferred
Appendix A. Guidelines not included in the review (Appendix B. Recommendations to prevent heat illne
Background
Physical activity for reasons of occupation or recre-ational exercise in hot and humid environmentscan lead to serious harm from dehydration, heatexhaustion and heat stroke1—3. The maintenance ofoptimal physical output requires that body temper-ature be regulated within relatively narrow limits1.Work or sports participation in the heat for longperiods can lead to progressive heat illness, whichis associated with impaired physical and mentalperformance4.
Guidelines are therefore required that are basedon currently available best evidence5, which pro-vide a framework for community-based sports par-ticipants and officials to assess risks associated withhot weather activities, and to establish safe prac-tices. Occupational health and safety legislationaround the world seeks to provide standards toprotect the health of workers in hot environmentsand climates. There have been numerous attemptsto produce such guidelines for sports participants;however there has not been a review to date of thequality of these guidelines or the recommendationsthat they provide.
This paper presents a systematic review ofguidelines for safe practices in hot weather bycommunity-based sports participants and officials,
by a difference in temperature.6
Temperature: The degree of hotness or coldnessof a body or environment (corresponding to itsmolecular activity).6

P ts pa
D
SlbnmwEAS(2lSDerrllww
I
Feows
emtitpNauFcwbataTsir
G
TuaiidiCtdftsoSPgtStiittPf5cT
revention of heat illness in community-based spor
Wet bulb globe temperature (WBGT): The wetbulb temperature is the temperature at which nomore evaporation will occur, and thus no furtherdecrease in the temperature. The air will con-tinue to cool until the air can evaporate no moremoisture. The temperature, when the cooling con-tinues until the evaporation stops and the airbecomes saturated, is the wet bulb temperature.7
Dry (bulb) globe temperature (DBGT): Air temper-ature as indicated by an ordinary thermometer.8
Evidence-based: Information based on sound anddefensible science.5
Policy: A plan of action adopted by an individualor social group.6—8
Advice: A proposal for an appropriate course ofaction.6—8
Humidity: The moisture content of air. Relativehumidity is the ratio of the amount of water vaporactually present in the air to the greatest amountpossible at the same temperature.9
Guidelines: Evidence syntheses to underpin thedevelopment of policies and standards.5,10
Criteria: Standards, rules, or tests on which ajudgment or decision may be based.5,11
ata sources
earching involved all databases held in theibrary of University of South Australia androad spectrum Internet search engines, witho date restrictions on the search in order toaximise the search potential. The databases usedere extensive and included Academic Searchlite (1985—end 2004), AMED (1985—end 2004),usHealth (1966—end 2004), AUSPORT—–Australianports Database (start—end 2004), CINAHL1982—end 2004), Cochrane Library (start—end004), Current Content (1993—end 2004), Med-ine (1966—end 2004), PubMed (1966—end 2004),cience Direct (1997—end 2004), and Sportsiscus (1949—end 2004). The Internet searchngines were those that had been found by theesearch team in previous reviews of non-peereviewed (grey) literature to identify a compositeisting and broad spectrum of web-based guide-ines: www.dogpile.com, www.eurekster.com,ww.google.com, www.vivisimo.com, andww.yahoo.com.
nclusion and exclusion criteria
ull text (complete), English language secondary
vidence with listed cited references which focusedn sports participation in the community in hoteather, or to hot weather occupational expo-ures, was included. The guidelines could relate to
ttos
rticipants and officials 13
ither gender, any sport and all age groups. Infor-ation on occupations that could be extrapolated
o non-player activities (umpires, officials etc) wasncluded. Guidelines that were not available in fullext, or in English, or which did not provide a com-lete reference list of resources were excluded.o primary studies were included in this review,lthough note was made of the sources of evidencepon which the included guidelines were based.ull text guidelines were required in order to haveonfidence that the guideline recommendationsere based on sound methodology (i.e. minimumias in evidence collation and interpretation),5 andfull list of references was sought to determine
he level of bias in the underpinning evidence5
nd to enable validation of recommendations.16—18
wo independent reviewers determined the inclu-ion and exclusion status of each of the guidelinesdentified in the search, and disagreements wereesolved by discussion.
uideline quality assessment
he Appraisal of Guidelines for Research and Eval-ation instrument (AGREE)12,13 was used to evalu-te the internal and external methodological qual-ty of the guidelines included in this review. Thisnstrument is a commonly used, internationally vali-ated, critical appraisal tool to determine the qual-ty of guideline development and construction.14,15
ritical appraisal using AGREE was undertaken bywo independent reviewers, and the individualomain scores reported in this paper were derivedrom the standardised scoring system described inhe AGREE documentation.12 The AGREE instrumentcores six domains of quality using a four levelrdinal scale ranging from Strongly Agree (4) totrongly Disagree (1). The domain of Scope andurpose (Domain 1) reflects the overall aim of theuideline, the specific clinical questions and thearget patient population, while the domain oftakeholder Involvement (Domain 2) is the extento which the guideline reflects the views of itsntended users. Domain 3, Rigor of Development,s the quality of the process used to gather and syn-hesise the evidence, and the methods to formulatehe recommendations and update them. Clarity andresentation (Domain 4) assesses the language andormat of the guidelines, and Applicability (Domain) reflects the likely behavioral, organisational andost implications of implementing the guidelines.he sixth domain, Editorial Independence, reflects
he independence of the guideline recommenda-ions, and acknowledgement of conflict of interestf guideline developers. A high quality guidelinehould score close to 100% on all domains. No guide-
10 to occupation). The excluded guidelines arelisted in Appendix A with the reasons for exclusion,the most common being unavailability of full textguidelines and/ or the lack of cited references.
Table 1 Included guidelines, access reference andcontent
Reference Content
19 [A] 6 peer reviewed published primaryresearch references
20 [B] 22 refs (21 peer reviewed publishedprimary research references)
21 [C] 92 peer reviewed published primaryresearch references
22 [D] 46 peer reviewed published references23 [E] 16 peer reviewed published primary
research references24 [F] Multiple weblinks and related
guidelines/ policies25 [G] 14 related weblinks, published
guidelines/ standards26 [H] 42 related weblinks, published
guidelines/ standards27 [I] 6 published guidelines/ standards28 [J] 4 published guidelines/ standards29 [K] 4 published guidelines/ standards30 [L] 6 published guidelines/ standards31 [M] 12 references (5 published guidelines/
standards, 1 peer-reviewed primaryresearch publication)
Alphabets appearing in brackets refer to the alphabeticreference listing of Appendix B.
sdbtladslPTpci(icarp(hgca
C
FtmgwfTi
CEtth
tgtttsg
flase
T. Larsen et al.
The individual guideline AGREE domain qualitycores, and the average domain scores (and stan-ard deviations) are listed in Table 2. The alpha-etic letter reference for the guidelines relateso Table 1, and also to the paper’s referenceist. The quality of the included guidelines variedcross and between domains, and no one guidelineemonstrated consistently good quality across allix domains. The highest average scores (and simi-ar variability) were found for Domain 1 (Scope andurpose) and Domain 4 (Clarity and Presentation).his suggests that most guidelines addressed theirurpose and target population, and were presentedlearly. Moderate average quality scores (and sim-lar variability) were observed for Domains 2 and 3Stakeholder Involvement, Rigor of Development),ndicating variability across guidelines regardingoncerns of users, and variable processes to gathernd synthesise evidence, and formulate and updateecommendations). The domains with consistentlyoor quality across guidelines were ApplicabilityDomain 5) and Editorial independence (Domain 6),ighlighting the limited information provided in theuidelines on likely behavioral, organisational orost implications of implementing the guidelines,nd independence of recommendations.
ommon themes
ive themes were reported across the guidelines,hese being fluid intake, heat limits, clothing, accli-atisation and precautionary interventions. Not all
uidelines addressed all themes. No other themesere identified. The recommendations synthesised
rom this review are presented for each theme inables 3—7 (the occupational guidelines are in ital-cs).
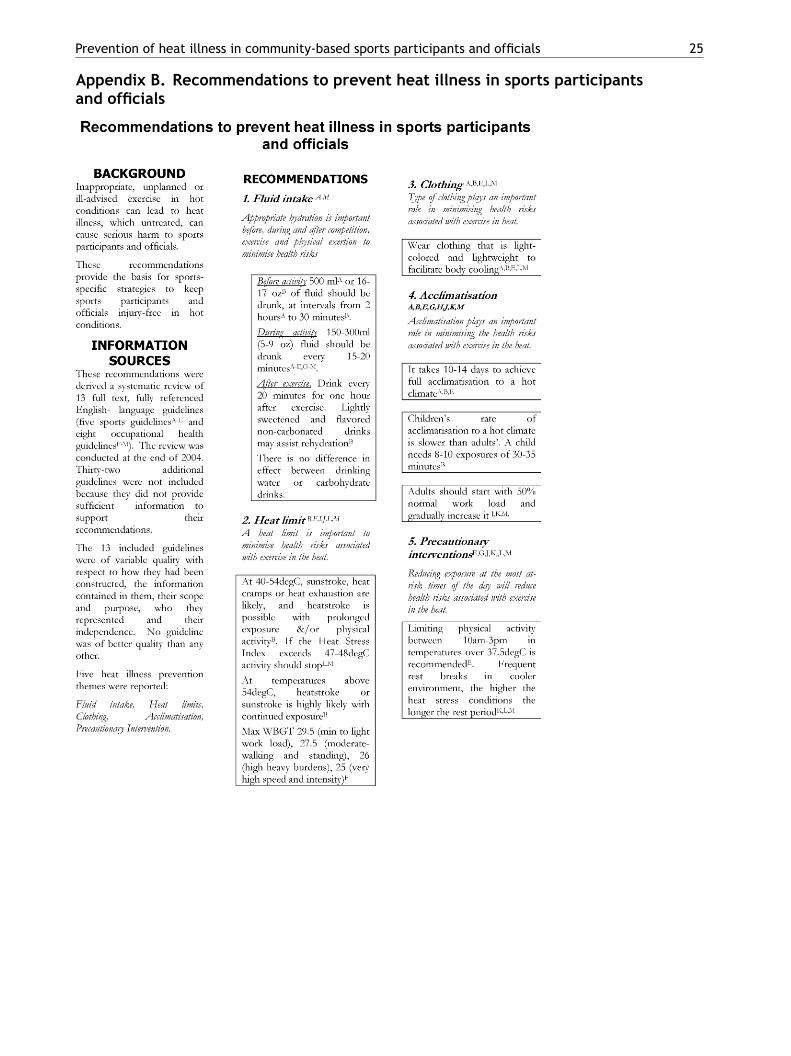
ommon theme 1: fluid intakevidence Synthesis Statement: Appropriate hydra-ion is important before, during and after compe-ition, exercise and physical exertion to minimiseealth risks.
All included guidelines19—31 contained informa-ion relevant to this theme (see Table 3). Theseuidelines reflected wide international interest inhis issue, was albeit with little consistency inhe recommendations. The evidence underpinninghese guidelines consisted of primary research5 andecondary evidence (policy documents and otheruidelines).
Before activity, drinking 500 ml (16—17 oz) of
14
line was excluded from the review if it was ofpoor quality i.e. all guidelines were included in thisreview irrespective of AGREE quality scoring.
Synthesised recommendations
The themes reported in each included guidelinewere collated, and common themes identified.The recommendations provided for the commonlyreported themes in the eligible guidelines were syn-thesised and reported in this review.
Results
Included evidence and its quality
Thirteen guidelines19—31 were included in thisreview (five related to sports and eight relatedto occupations) (see Table 1). This table providesthe publication details and the evidence sourceson which each guideline is based. A further 32guidelines were identified by the search, but wereexcluded from analysis (22 related to sports, and
uid was the most common recommendation,lthough guidelines regarding the timing of con-umption differed (from 30 min to 2 h prior). Duringxercise/physical activity there was general agree-

Prevention of heat illness in community-based sports participants and officials 15
Table 2 AGREE domain scores for included guidelines
Guideline reference(see Table 1)
Domain 1:Scope andpurpose
Domain 2:Stakeholderinvolvement
Domain 3:Rigour ofdevelopment
Domain 4:Clarity andpresentation
Domain 5:Applicability
Domain 6:Editorialindependence
A 75% 75% 67% 33% 25% 50%B 33% 16% 24% 83% 22% 0%C 66% 50% 14% 75% 0% 0%D 66% 16% 61% 33% 0% 50%E 77% 41% 24% 20% 11% 0%F 33% 4% 14% 75% 0% 0%G 88% 33% 5% 50% 0% 0%H 11% 8.30% 10% 40% 0% 0%I 22% 17% 10% 50% 0% 0%J 55% 17% 10% 92% 0% 0%K 67% 17% 10% 86% 0% 0%L 100% 25% 24% 74% 0% 0%M 56% 17% 14% 42% 33% 0%
Average 58% 26% 22% 58% 7% 8%Standard 26% 19% 20% 24% 12% 19%
s.
mSnrbp
CEie
gt
csgitaslilfw
CEpa
travwcur
CEpr
atinoga8w2ifhc
deviation (S.D.)
Italic guideline references indicate the occupational guideline
ent on 150—300 ml (5—9 oz) every 15—20 min.pecific reference to research evidence underpin-ing these values was lacking. There were no clearecommendations regarding the use of water or car-ohydrate drinks, and the amount or frequency ofost-exercise fluid replacement.
ommon theme 2: heat limitsvidence Synthesis Statement: A heat limit ismportant to minimise health risks associated withxercise in the heat.
One sports guideline20 and five occupationaluidelines guidelines24,27,28,30,31 provided informa-ion relevant to this theme (see Table 4).
Wet Bulb Globe Temperature (WBGT) was theommon heat limit reference in the Australianports recommendations, with the American sportsuidelines including air temperature, and humid-ty assessment measures in their recommenda-ions. For the occupational guidelines, DBGT, WBGTnd Humidex measures were reported. This con-trained establishing uniform recommended heatimits. Both WBGT and DBGT were used in report-ng ‘rest breaks’ and there was lack of consensus onength of the breaks, as well as temperature levelsor when the breaks should occur. The WBGT scaleas also used to reflect work intensity.24
ommon theme 3: clothingvidence Synthesis Statement: Type of clothinglays an important role in minimising health risksssociated with exercise in the heat.
CEs
Three sports guidelines19,20,23 and two occupa-ional guidelines30,31 were identified (see Table 5),elating to appropriate clothing for hot weatherctivities. There was consensus across all rele-ant guidelines on recommendations regarding hoteather clothing, with respect to light weight, lightolored and breathable clothing. Evidence sourcesnderpinning these guidelines reflected primaryesearch and secondary literature.
ommon theme 4: acclimatisationvidence Synthesis Statement: Acclimatisationlays an important role in minimising the healthisks associated with exercise in the heat.
There were three sport-related guidelines19,20,23
nd five occupational guidelines25—27,29,31 relevanto this theme (see Table 6). The guideline qual-ty varied across the AGREE domains. There waso common sports guidelines recommendationsn how to acclimatise, however the occupationaluidelines commonly recommended starting at 50%ctivity on the first day and progressing to 60%, then0% on the second and third days. For inexperiencedorkers, recommendations were to commence with0% maximum activity on the first day, with a dailyncrease of 20%. Ten to 14 days is the consensusor full acclimatisation for adults in a hot climate,owever there are conflicting recommendations forhildren.
ommon theme 5: precautionary interventionsvidence Synthesis Statement: Reducing expo-ure at the most at-risk times of the day will

16 T. Larsen et al.
Table 3 A summary of recommendation relating to fluid intake evidence
Guidelinereference(see Table 1)
AverageAGREEscore (S.D.)
N peerreviewedreferences
Recommendations
A 54% (22%) 6 Before: 500 ml 2 h before competition.During: 150—300 ml every 15—20 min during running or similaractivity (individual differences). Recent studies indicate 5%—8%CHO electrolyte sports drinks are well tolerated.After: High fluid volume replacement (150% of lost weight) andhigher sodium content
B 30% (28%) 21 Before: 12—16 oz (360—480 ml) of fluid approximately 30 minbefore playing.During: Every 20 min — 5 oz (150 ml) of fluid for a playerweighing 90 lbs (40.5 kg) or less, 9 oz (270 ml) for a playerweighing more than 90 lbs.After: Once the activity is over drinking every 20 min for 1 h.Lightly sweetened and flavored non-carbonated beverages arepreferred to facilitate rehydration.
C 34% (34%) 92 Before: 500 ml about 2 h before.During: Every 15—20 min 150 ml—350 ml. Less than 1 h — water, iflonger 30—60 g carbohydrate loaded.Fluid to be flavored and or sweetened.
D 38% (26%) 46 During: Excessive drinking among marathon runners can lead tohyponatraemia severe enough to cause fatalities. Thus, a morereasonable approach is to urge these participants not to drink asmuch as possible but to drink no more than 400—800 ml/h.
E 29% (27%) 16 Before: Well hydrated.During: 150 ml every 20 min.
F 21% (21%) 0 The employer shall ensure an ample supply of drinking water atall places of work.
G 29% (35%) 0 Cool drinks every 20 min.H 11% (15%) 0 Cool (50—60 F) water or any cool liquid should be made available
to workers to encourage them to drink small amounts frequently(one cup every 20 min).
I 16% (19%) 0 Drink plenty before you get thirsty.J 29% (37%) 0 Fluid intake — 8oz every 20 min. The ideal temperature for
liquids should be 50—60 F.K 30% (37%) 0 Fluid intake — 8oz every 20 min. The ideal temperature for
liquids should be 50—60 F.L 37% (41%) 0 Drink small amount of fluid regularly.M 27% (20%) 1 Drinking a small cup of fluid every 20 min.
rdpawi
All included guidelines provided evidence on this theme.
reduce health risks associated with exercise in theheat.
There was one sports guideline23 and five occu-pational guidelines25,28—31 relating to this theme(see Table 7).
All relevant guidelines recommended length ofbreaks in accordance to the temperature, and
were generally unified in their recommendations.At 30 ◦C there should be a 10—15 min break andthe length of these breaks should increase as tem-perature rise. There was also consensus regardingO
Tc
ecommendations for limiting exposure to hot con-itions, with a common recommendation limitinghysical activity between 10 am and 2 pm (11 amnd 3 pm in non-daylight saving locations). Thereas no reference to specific months, or to support-
ng meteorological data.
ur synthesised evidence recommendations
he findings from this review were synthesised intoomposite recommendations that could underpin

Prevention of heat illness in community-based sports participants and officials 17
Table 4 A summary of recommendation relating to heat limits evidence
Guidelinereference(see Table 1)
AverageAGREEscore (S.D.)
N peerreviewedreferences
Recommendations
B 30% (28%) 21 130 F — heatstroke/sunstroke highly likely with continuedexposure, 105—130 F — sunstroke, heat cramps or heatexhaustion likely, and heatstroke possible with prolongedexposure and or physical activity.
F 21% (21%) 0 Max WBGT 29.5 (minimum to light work load), 27.5(moderate- walking and standing), 26 (high heavy burdens),25 (very high speed and intensity).
I 16% (19%) 0 Humidex — 35◦, airtemp > 30 stop work?J 29% (37%) 0 If the heat stress index exceeds 120 F or 118 F work should
stop.L 37% (41%) 0 INDOOR — optimum comfort is between 21—26 ◦C (below 30 ◦C
in sedentary work places). Extreme temperature cancel.OUTDOOR > 39 cease work.
M 27% (20%) 1 If the heat stress index exceeds 120 F or 118 F work shouldstop.
Four sports guidelines (A, C, D, E) and three occupational guidelines (G, H, K) did not provide evidence on this theme.
Table 5 A summary of recommendations relating to clothing evidence
Guidelinereference(see Table 1)
AverageAGREEscore (S.D.)
N peerreviewedreferences
Recommendations
A 54% (22%) 6 Fabrics that minimise heat storage and enhance sweat evaporationshould be selected. White or light color, cotton or other breathablefabrics and designs that maximise skin exposure are beneficial.
B 30% (28%) 21 Wear clothing that are light-colored and lightweight to facilitatebody cooling.
E 29% (27%) 16 Light color, light weight, and limited to one layer.L 37% (41%) 0 Appropriate clothing, broad brimmed hat, lightweight clothing,
and sunglasses.ose fi
did n
dsBbsttstc
D
Emsb
sbitfisootmtam
M 27% (20%) 1 Wear lo
Two sports guidelines (C, D) six occupational guidelines (F—K)
iscussions with sporting organisations to establishpecific heat participation strategies (see Appendix). The aim was that these recommendations coulde used in education and planning sessions withporting bodies in order to identify issues relevanto that sport, and to provide the organisations withhe best current evidence upon which to developtrategies to prevent heat illness for sports par-icipants and officials in local environments andonditions.
iscussion
xtreme heat conditions around the world are com-only associated with reports of heat illness in
ports participants and officials.2—4 In their pream-les, the guidelines considered in this review all
ptmh
tting, light colored porous clothing.
ot provide recommendations on this theme.
uggest that the likelihood for heat illness shoulde predictable, and that the illness is preventablef appropriate precautions are taken. This sys-ematic review of currently available full text,ully referenced guidelines for prevention of heatllness in sports participants and officials (usingports and occupational guidelines) provides anpportunity to collate and compare current rec-mmendations, and to consider them relative tohe quality of guidelines from which these recom-endations were extracted. The guidelines iden-
ified in the review reflect work from countriesround the world, indicating wide-spread prag-atic interest in protecting the health of sports
articipants and officials. The five themes iden-ified in the review reflect concerns relevant toost sports played in hot weather (fluid intake,eat limits, clothing, acclimatisation, precaution-

18 T. Larsen et al.
Table 6 A summary of recommendation relating to acclimatisation evidence
Guidelinereference(see Table 1)
AverageAGREEscore (S.D.)
N peerreviewedreferences
Recommendations
A 54% (22%) 6 Acclimatisation typically requires 10—14 days in the warmerenvironment, but 75% of the adaptation is believed to occur within5 days. Initial exercise sessions should be shorter and lessintensive.
B 30% (28%) 21 The rate of acclimatisation is slower than that of adults. A childneeds as many as 8—10 exposures (30—35 min each).
E 29% (27%) 16 Should be allowed 10—14 days of acclimatization.
G 29% (35%) 29 Acclimatisation — two ways for experienced and not experienced:Experienced — 50% first day, 60% second day, 80% third day, then afull shift.Not experienced: 20% first day then increase by 20% each day ofwork.
H 11% (15%) 0 Acclimatisation — two ways for experienced and not experienced:Experienced — 50% first day, 60% second day, 80% third day, then afull shift.Not experienced: 20% first day then increase by 20% each day ofwork.
J 29% (37%) 0 Acclimatisation — takes a few days — start with 50% of normalwork loads and gradual increase.
K 30% (37%) 0 Acclimatisation — takes a few days — start with 50% of normalwork loads and gradual increase.
M 27% (20%) 1 Acclimatisation — 50% first day and gradually increase.
Two sports guidelines (C, D) and three occupational guidelines (F, I, L) did not provide evidence on this theme.
Table 7 A summary of recommendation relating to precautionary interventions evidence
Guidelinereferencefrom Table 1
AverageAGREEscore (S.D.)
N peerreviewedreferences
Recommendations
E 29% (27%) 16 The intensity of activities that last 15 min or more should be reducedwhenever relative humidity, solar radiation and air temperature areabove critical levels (WBGT 24—26).
G 29% (35%) 0 Increase air movement with fan.Increase frequency and length of rest.
J 29% (37%) 0 When the HEAT STRESS INDEX exceeds the extreme caution level of90 F precautions in Table 2 must be observed (HR, Fatigue, nausea,dizziness, lightheadedness). If Employees are wearing protectiveclothing precautions should be followed at a 88 F. If the heat stressindex exceeds 120 F or 118 F work should stop.
K 30% (37%) 0 When the HEAT STRESS INDEX exceeds the extreme caution level of90 F precautions in Table 2 must be observed (HR, Fatigue, nausea,dizziness, lightheadedness). If Employees are wearing protectiveclothing precautions should be followed at a 88 F. If the heat stressindex exceeds 120 F or 118 F work should stop.
L 37% (41%) 0 Breaks — 30 ◦C — 10 min/h breaks.>35 ◦C — 15—20 min/h.No direct sunlight between 1100—1500 h.Reschedule work to cool times of day.
M 27% (20%) 1 Frequent rest breaks in cooler environment, the higher the heat stressconditions the longer the rest periods.
Four sports guidelines (A—D) and three occupational guidelines (F, H, L) did not provide evidence on this theme.

P ts pa
atutssh
bwtsmtreslltrlagg1awbrvelpmria
bidotlmerosfpEbad
oiatqcbctijarfTsoogcw
tgadaotbnizoptElo(dlnliretttip
revention of heat illness in community-based spor
ry interventions). The synthesised recommenda-ions presented in this paper are currently beingsed in South Australia by Sports Medicine Australia,o underpin discussions and education sessions withporting organisations regarding establishment ofports- and environment-specific strategies to avoideat-illness in participants and officials.
The approach taken in this paper is advocatedy key guideline development teams around theorld5,16—18 when developing current best prac-
ice statements that are understandable, defen-ible and believable, and are readily imple-entable. The approach taken in this review
o explore sports and occupational guidelineseflected our purpose to consider all stakehold-rs in sporting activities (participants, officials,pectators, volunteers, etc.). This review high-ighted the difficulty of finding relevant guide-ines from standard readily accessed sources. Onlyhree included guidelines were published in peer-eviewed journals19,21,23 with the remainder pub-ished on Internet websites.20,22,24—31 The aver-ge overall quality score (AGREE) for the publisheduidelines was higher than that for the web-baseduidelines, but not significantly different ((39%(S.D.3%) compared with 27% (S.D. 8%)). This trend waslso observed across each of the AGREE domains,hen comparing the peer-reviewed and the web-ased guidelines. Publication of guidelines in peer-eviewed journals is in its infancy because of theolume of literature which should be included asvidence of validity of construction.5,17,18 The wordimits of many peer-reviewed journals precludeublication of guidelines which provide extensiveethodology and reference lists. Given the compa-
able AGREE scores, the location of the guidelinesncluded in this review thus should not be taken asn indication of quality of construction.
The AGREE instrument12—15 provides a defensi-le approach for considering guideline quality. Its internationally referenced, and provides a stan-ard framework for assessing a range of elementsf guideline quality. It was particularly useful forhis review, as its domains highlighted the generalack of information in the included guidelines onethodology, e.g. how the underpinning refer-
nces were identified, information on excludedeferences, methodological quality, and relevancef research design to the guideline purpose andcope. This is reported as the average quality scoresor Domains 3 (Rigour of Development) and theoor scores for Domains 5 and 6 (Applicability and
ditorial Independence). Guidelines that are notased on defensible and repeatable methods (suchs structured search strategy, defined data sources,efined hierarchy of evidence, standard method-trcc
rticipants and officials 19
logical quality scores and valid approaches to datanclusion/exclusion (stated criteria, independencend reliability of decision-making)) therefore havehe potential to provide recommendations ofuestionable believability. We attempted to over-ome these concerns in this guideline synthesis,y addressing best practice guideline constructionriteria5,16—18 by using stated search strategy anderms, stated and extensive data sources, clearnclusion and exclusion criteria, information toustify our decisions, and stated independencend reliability of decision-making. Our search iseproducible and could be reapplied in the futureor new guidelines developed since this search.he result of our search was a synthesis of eligibleecondary evidence (which itself was a synthesisf primary and secondary evidence). Thus whileur search is defensible, the variable quality of theuidelines included in this review suggests that theomposite recommendations should be consideredith caution.Given international interest in heat illness,
here were surprisingly few sports and occupationaluidelines relevant to this review. Over four timess many sports and occupational guidelines wereeemed ineligible for review because they providedbsent or incomplete information about methodol-gy and the evidence-basis for their recommenda-ions. Also of concern was the variable evidencease underpinning the included guidelines. Theumber of peer reviewed primary research stud-es cited in the included guidelines ranged fromero to 92 (see Table 1). No guideline reportedn the hierarchy of this primary evidence,5,18 thusroviding no information on the nature (experimen-al/observational design) of the evidence-base.xperimental studies are considered to incur theeast amount of bias comparing all design typesf primary quantitative research.5 Seven guidelinesoccupational) were based solely on secondary evi-ence (policies, recommendation and other guide-ines). All of these references were web-based (i.e.ot peer reviewed). There was considerable over-ap between guideline literature sources, suggest-ng perhaps that many guidelines simply quoted theeferences from other guidelines without consid-ration of the value of the evidence upon whichhey were based, or the sensitivity of the evidenceo specific heat illness prevention recommenda-ions. Without reviewing the hierarchy and qual-ty of the primary and secondary evidence under-inning the included literature it is not possible
o determine the level of bias underpinning theecommendations.5,17,18 This is another reason foronsidering our composite recommendations withaution.
asttirsAshotdpt
R
20
Barriers to uptake of guideline recommendationsare believed to be the relevance of the informationto the individual, and the ease with which recom-mendations are able to be put into practice.16—18
The lack of consensus in the included guidelinesregarding specific instructions to deal with hotweather issues suggests that the recommendationssynthesised from this review need to be care-fully worded to be readily adopted by any sport.Thus, the synthesised recommendations (AppendixB) were constructed in a manner that can beadapted to the needs of different sports in a rangeof environments. This paper reports in an academicforum on the information developed for SportsMedicine Australia, South Australia (SMASA) froma consultancy to identify current best evidencein heat illness prevention for sports participantsand officials. This information has been dissemi-nated by SMASA to sporting organisations via theirwebsite, education sessions, brochures, discussionsand workshops. Sporting organisations have beenencouraged by SMASA to consider this informationand modify it to suit the individual requirementsof the sport within its local contexts and commu-nity. Evaluation of uptake of this evidence and itsrelevance to developing effective sports-specificstrategies will be reported elsewhere.
Concerns about the strength of the evidencebase of the included guidelines, and the qualityof guideline construction, suggests that the rec-ommendations in any individual guideline cited inthis review may not be defensible if challenged.Given the importance of protecting the healthof individuals around the world who are activein hot weather, this suggests the need to firstlyconstruct better quality comprehensive guidelinesbased on the hierarchy and quality of primaryresearch evidence for the five themes outlined inthis review, and secondly to undertake primaryresearch in areas where the guideline developmentprocess highlights its absence. This would improvethe sensitivity, robustness and applicability ofnew guidelines. In the interim, where primaryor secondary research is not currently availableto underpin the development of evidence-basedguidelines, structured and facilitated approachesare required to obtain consensus opinion on whatis currently accepted as best practice.
Conclusion
This review provides recommendations regardingprevention of heat illness in sports participantsand officials that are based on current best avail-
T. Larsen et al.
ble guideline evidence. Given the internationalources of underpinning the guidelines included inhis review, these recommendations are applicableo sports participants and officials in hot weathern any country around the world. The synthesisedecommendations from this review have been dis-eminated by Sports Medicine Australia in Southustralia to sports organisations to inform sports-pecific strategies aimed to reduce the likelihood ofeat illness. While the evidence-basis for the rec-mmendations proposed from this review is ques-ionable, these recommendations provide the mostefensible information at this point in time to sup-ort decisions regarding safe sports participation inhe heat.
Practical implications
• Current best evidence-based recommenda-tions regarding prevention of heat illness insports participants and officials.
• Provides a template for future guidelinereviews in this area.
• Outlines the quality domains of guideline con-struction for guideline users.
• Highlights the need to access well constructedand referenced guidelines through a range oflibrary databases and the Internet.
• Highlights the need to be way when interpret-ing recommendations based on best evidencesources because of variability in guideline con-struction and literature interpretation.
eferences
1. Bates G. What are the fluid replacement guideline for work-ers undertaking physically demanding tasks in the heat?Aust J Nutr Diet Suppl 1996;53:44—6.
2. Blum LN, Bresolin LB, Williams MA. Heat-related illness dur-ing extreme weather emergencies. JAMA 1998;279:1514.
3. Kilbourne EM. Illness due to thermal extremes. PublicHealth Prevent Med 1992;13:491—501.
4. Sawka M. Physiological consequences of hypohydration:exercise performance and thermoregulation. Med Sci SportsExerc 1992;24:657—70.
5. Sackett D, Richardson W, Rosenberg W, Haynes R. Evidence-based medicine: how to practice and teach EBM. London:Churchill Livingstone; 2000.
6. http://www.cogsci.princeton.edu/cgi-bin/webwn,accessed 9 January 2006.
7. http://www.aws.com/aws 2001/homeland/gloss.html,
accessed 9 January 2006.8. http://www.hvac2000.com/definitionslist.htm, accessed 9January 2006.
9. http://www.sol.crest.org/renewables/SJ/glossary/H.html,accessed 9 January 2006.

P ts pa
,
G
revention of heat illness in community-based spor
10. http://www.safetyventures.com/safety terms glossary.aspaccessed 9 January 2006.
11. http://www.wetlandtraining.com/glossary.html, accessed9 January 2006.
12. AGREE Collaboration. Appraisal of Guidelines for Researchand Evaluation (AGREE) Instrument. Available at:http://www.agreecollaboration.org/. Accessed 9 January2006.
13. AGREE Collaboration. Development and validation of aninternational appraisal instrument for assessing the qual-ity of clinical practice guidelines: the AGREE project. QualSaf Health Care 2003;12:18—23.
14. MacDermid JC, Brooks D, Solway S, Switzer-McIntyre S,Brosseau L, Graham ID. Reliability and validity of theAGREE instrument used by physical therapists in assess-ment of clinical practice guidelines. BMC Health ServicesRes 2005;5:18.
15. Vlayen J, Aertgeerts B, Hannis K, Sermeus W, Ramaekers D.A systematic review of appraisal tools for clinical practiceguidelines: multiple similarities and one common deficit.Int J Qual Health Care 2005;17:235—42.
16. National Health and Medical Research Council. How to usethe evidence: assessment and application of scientific evi-dence. Canberra: Australian Government Publisher; 2000.
17. Thomson R, Lavender M, Madhok R. Fortnightly review:how to ensure that guidelines are effective. BMJ1995;311:237—42.
18. Margolis CZ. Clinical practice guidelines: methodologicalconsiderations. Int J Qual Health Care 1999;11:303—6.
uidelines included in the review
19. Sparling PB, Millard-Stafford M. Keeping sports participantssafe in hot weather. Phys Sports Med 1999;27(7):27—40.20. US Soccer Federation. Youth soccer heat stress guidelines.
http://www.ussoccer.com/templates/includes/news/USSoccer Guidelines.pdf, accessed 18.1.06.
rticipants and officials 21
21. ACSM Position Stand. Exercise and fluid replacement. MedSci Sports Exe 1996;28(1):i—viii.
22. IMMDA. Guidelines for fluid replacement during Marathonrunning. http://www.aims-association.org/guidelines forfluid replacement.htm, accessed 18.1.06.
23. Committee on Sports Medicine and Fitness. Climatic heatstress and the exercising child and adolescent. Pediatrics2000;106(1):158—9.
24. IFC Environmental Guideline for Occupational Health andSafety. Environmental and social guideline for occupationalhealth and safety. http://ifcln1.ifc.org/ifcext/enviro.nsf/Content/EnvironmentalGuidelines; 2003. Accessed18.1.06.
25. Ontario Ministry of Labour. Heat stress. http://www.labour.gov.on.ca/english/hs/guidelines/gl heat.html;2003. Accessed 18.1.06.
26. Interstate Products Inc. OSHA Technical Manual. Heat StressInformation. http://www.xpdnc.com/links/hsheatst.html,accessed 18.1.06.
27. OSHA Fact Sheet. Working outdoors. http://www.osha.gov/OshDoc/data General Facts/working-outdoors-factsheet.pdf; 2003. Accessed 18.1.06.
28. University of Texas-Pan American Department of Envi-ronmental Health and Safety. Heat stress policy. http://ehs.panam.edu/prog occupational/Heat Stress 2000.pdf;2000. Accessed 18.1.06.
29. University of Florida, Environmental Health and Safety.Heat stress policy. http://www.ehs.ufl.edu/General/heatstrs.pdf; 2001. Accessed 18.1.06.
30. University of Adelaide. Policy on safety while work-ing in temperature extremes. https://www.adelaide.edu.
au/hr/policies/ohs/tempextremes.html; 2004. Accessed18.1.06.31. OSEH. Occupational safety and environmental healthguideline. http://www.oseh.umich.edu/heat stress.pdf;1997. Accessed 18.1.06.

T. Larsen et al.
ional
22
Appendix A. Guidelines not included in the review (occupatguidelines shaded)

P ials 23
A
revention of heat illness in community-based sports participants and offic
ppendix A (Continued )

T. Larsen et al.
24Appendix A (Continued )
P ts pa 25
t ha
revention of heat illness in community-based spor
Appendix B. Recommendations to prevennd officials
rticipants and officials
eat illness in sports participants

T. Larsen et al.
26Appendix B (Continued )