hematology - imed 2017 | a continuing medical education...
TRANSCRIPT

Hematology:Challenging Cases with
Your ParticipationReed E. Drews, MD
Beth Israel Deaconess Medical CenterHarvard Medical School
Boston, MA
COPYRIG
HT

Question 1COPYRIG
HT

Question 1
• 64-year-old man is evaluated during routine exam
• He takes aspirin and acetaminophen for osteoarthritis
• On exam, pallor is absent. BP = 116/72 with no orthostatic changes; P = 68.COP
YRIGHT
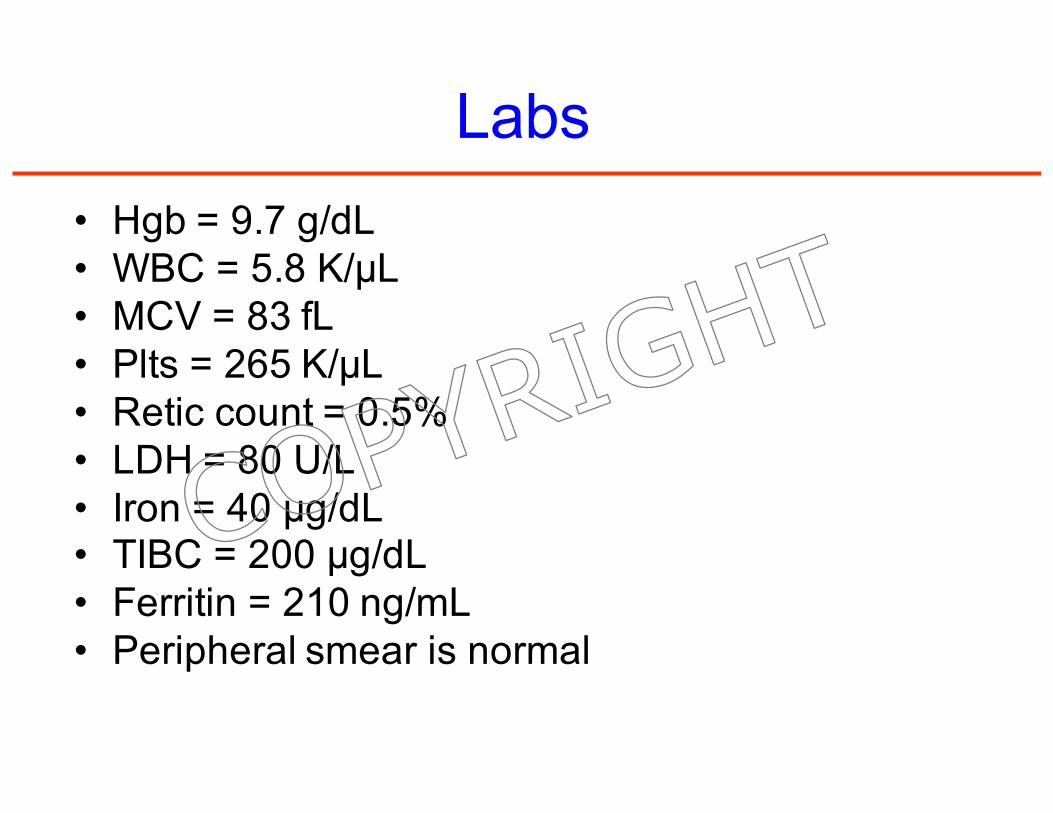
Labs
• Hgb = 9.7 g/dL• WBC = 5.8 K/μL• MCV = 83 fL• Plts = 265 K/μL• Retic count = 0.5%• LDH = 80 U/L• Iron = 40 μg/dL• TIBC = 200 μg/dL• Ferritin = 210 ng/mL• Peripheral smear is normal
COPYRIG
HT

Which of the following is the most likely diagnosis?
A. Inflammatory anemia
B. Hemoglobin C disease
C. Iron deficiency
D. Thalassemia
COPYRIG
HT

Answer = A
COPYRIG
HT
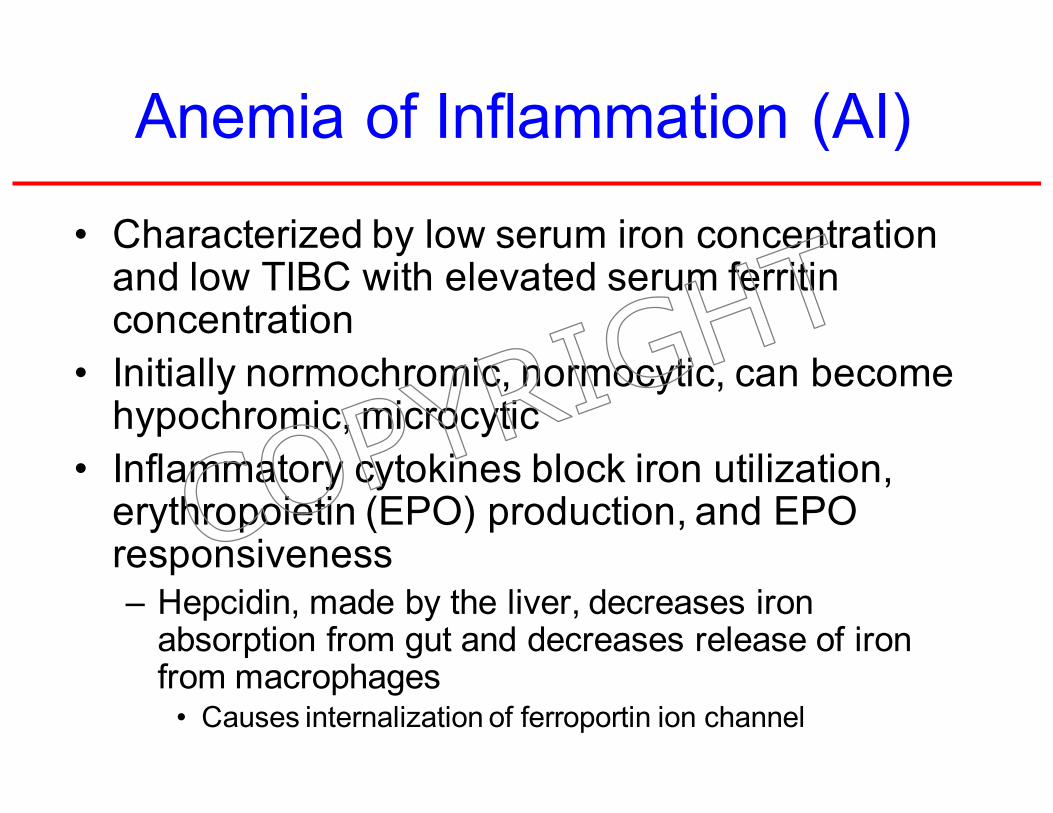
Anemia of Inflammation (AI)
• Characterized by low serum iron concentration and low TIBC with elevated serum ferritin concentration
• Initially normochromic, normocytic, can become hypochromic, microcytic
• Inflammatory cytokines block iron utilization, erythropoietin (EPO) production, and EPO responsiveness– Hepcidin, made by the liver, decreases iron
absorption from gut and decreases release of iron from macrophages
• Causes internalization of ferroportin ion channel
COPYRIG
HT

Hemoglobin C Disease
• Mild hemolytic anemia in persons of African ancestry
• Serum iron chemistries are typically normal
• Prominent targeting in addition to microcytosis on peripheral blood smearCOP
YRIGHT

Hgb CC
COPYRIG
HT

Iron Deficiency Anemia (IDA)
• Characterized by low serum iron concentration, elevated TIBC, and decreased serum ferritin
COPYRIG
HT

IDA
COPYRIG
HT

Thalassemia
• Hypochromic, microcytic anemia
• Evidence of hemolysis
• Targets, tear drops, and prominent basophilic stippling
COPYRIG
HT

Factors Distinguishing the 3 Most
Common Causes of Microcytosis
• Iron deficiency anemia (IDA)– Low serum ferritin
– Increased total iron binding capacity
– Low serum iron concentration
• Anemia of inflammation (AI)– Low serum iron
– Low total iron binding capacity
– Normal to increased serum ferritin
• Alpha or beta thalassemia minor– Patients may not be “anemic”
– Target cells, tear-drop forms, and basophilic stippling
IDA
b-thalassemia minor
COPYRIG
HT

Laboratory Characteristics ofAI, IDA, and IDA + Inflammation
From MKSAP®15
Parameter AI IDA IDA+AIMCV 72-100 fL <85 fL <100 fL
MCHC <36 g/dL <32 g/dL <32 g/dL
Serum iron <60 μg/dL <60 μg/dL <60 μg/dL
TIBC <250 μg/dL >400 μg/dL <400 μg/dL
TIBC saturation 2%-20%<15%
(usually <10%)<15%
Ferritin >35 ng/mL < 15 ng/mL <100 ng/mL
Bone marrow iron Present Absent Absent
COPYRIG
HT

Iron Deficiency Happens in Stages
• Iron deficiency without anemia
– Ferritin < 20 ng/mL; Fe/TIBC > 15%
• Iron deficiency with mild anemia
– Ferritin < 15 ng/mL; Fe/TIBC < 15%
• Severe iron deficiency with severe anemia
– Ferritin < 10 ng/mL; Fe/TIBC < 10%
• Bone marrow iron absent in all stages
COPYRIG
HT

Ferritin Levels in IDA
• Virtually all patients with serum ferritin levels <10 to 15 ng/mL are iron deficient– Sensitivity 59%, specificity 99%
• 25% of women with absent stainable bone marrow iron have ferritin levels >15 ng/mL
• Assuming no inflammation, higher ferritin cutoff limits provide improved diagnostic efficiency– 30 ng/mL: sensitivity 92%, specificity 98%
– 41 ng/mL: sensitivity 98%, specificity 98%
COPYRIG
HT

Anemia of Inflammation
• Inflammation decreases serum iron and plasma transferrin concentrations
– Transferrin saturations are in “iron deficiency range” in 20% of patients with anemia of inflammation
• 20 to 30% of patients with inflammatory anemia do not have underlying inflammatory condition
Guyatt GH et al. Am J Med 1990;88:205.
COPYRIG
HT

Ferritin Levels in Iron Deficiency AND Inflammatory States
• Inflammation increases ferritin levels by about 3-fold
• Iron deficiency should be suspected in patients with inflammatory states and ferritin levels <100 ng/mL
– In anemic patients with rheumatoid arthritis, ferritin levels < 60 ng/mL predicted response to oral iron therapy with 83% accuracy
(Hansen TM, Hansen NE. Ann Rheum Dis 1986;45:596)
COPYRIG
HT

Question 2COPYRIG
HT

Question 2
• 27-year-old woman undergoes follow-up evaluation 5 months after diagnosis of unprovoked PE for which she was prescribed a 6-month course of anticoagulant therapy
• Family history– Maternal grandmother took warfarin for many years
for unknown reason
– Older brother with DVT at age 32 years
• Meds: no contraceptives or other medications
• Labs: CBC normal; INR = 3.0
COPYRIG
HT

Which of the following is the most appropriate next step in the evaluation of this patient?
A. Immediate thrombophilic screening
B. JAK2 mutation analysis
C. No further evaluation needed
D. Thrombophilic screening at least 2 weeks after therapy cessationCOP
YRIGHT

Answer = D
COPYRIG
HT

Thrombophilia
• Unprovoked PE + family history of VTE = high likelihood of underlying thrombophilic condition
• Screening decisions– Strongly thrombophilic
• 1st unprovoked VTE before 50 yrs of age; or
• History of recurrent thromboses; or
• 1st-degree relative(s) with documented VTE before age 50 yrs
– Weakly thrombophilic• All others
• Do NOT screen during acute episode or during anticoagulant therapy when heparin or warfarin influence certain tests
• Risk of recurrent VTE cannot be estimated without screening for inherited thrombophilia
COPYRIG
HT

Thrombophilic Disorders with High Risk for Recurrence
• Antithrombin, protein C or protein S deficiency
• Homozygous factor V Leiden (FVL) or prothrombin gene mutation (PTM)
• Compound heterozygous FVL + PTM
• Patients with these disorders are candidates for long-term, if not lifelong, anticoagulation therapy
COPYRIG
HT

Thrombophilia due to Myeloproliferative Neoplasm
• PV and ET predispose to venous and arterial thromboses, particularly when RBC mass and platelet count are not controlled
• JAK2 mutation is found in nearly all pts with PV and ~50% of pts with ET
– Routine screening for this mutation is not recommended unless pts have Budd-Chiari syndrome of portal vein thrombosis
COPYRIG
HT

Target INR
• Target INR of 1.5 to 2 has efficacy in preventing recurrent VTE
• However, target INR of 2 to 3 is more efficacious
• Risk for major bleeding is similar for the two target INR ranges
(1) Ridker PM et al. Long-term, low-intensity warfarin therapy for the prevention of recurrent venous thromboembolism. N Engl J Med 2003; 348:1425-34.
(2) Kearon C et al. Comparison of low-intensity warfarin therapy with conventional-intensity warfarin therapy for long-term prevention of recurrent venous thromboembolism. N Engl J Med 2003; 349:631-9.
COPYRIG
HT

Major Risk Factors for Thrombosis: AcquiredFrom MKSAP®15
• Prior thrombosis
• Advancing age
• Obesity
• Immobilization
• Major surgery
• Estrogens (OCPs, HRT, SERMs)
• Malignancy
• Prolonged air travel
• Antiphospholipid antibody syndrome
• MPNs (PV, ET)
• PNH
• Hemoglobinuria
• HIT
• Inflammatory bowel disease
• Nephrotic syndrome
COPYRIG
HT

Major Risk Factors for Thrombosis: Inherited From MKSAP®15
• Antithrombin deficiency
• Protein C deficiency
• Protein S deficiency
• Factor V Leiden (FVL)
• Prothrombin G20210A
• Dysfibrinogenemias (rare)
COPYRIG
HT

Uncertain Risk Factors for Venous ThrombosisFrom MKSAP®15
• Hyperhomocysteinemia
• High levels of factor VIII
• APC-resistance in the absence of FVL
• High levels of factor IX
• High levels of factor XI
• High levels of TAFI
• Low levels of free TFPI
• Decreased fibrinolytic potential
TAFI = thrombin-activatable fibrinolysis inhibitor; TFPI = tissue factor pathway inhibitor.
COPYRIG
HT

Risks and Incidence of a First Episode of Venous Thrombosis
(From The Leiden Thrombophilia Study)
Relative Risk Incidence/y (%)Normal 1 0.008
Prothrombin G20210A mutation 2.8 0.02
Oral contraceptives 4 0.03
Factor V Leiden heterozygote 7 0.06
Oral contraceptives + factor V Leiden 35 0.29
Factor V Leiden homozygous 80 0.5 to 1.0
COPYRIG
HT

Site of Thrombosis According to Coagulation Defect
Abnormality Arterial VenousFactor V Leiden - +
Antithrombin III deficiency - +
Protein C deficiency - +
Protein S deficiency - +
Prothrombin gene mutation - +
Hyperhomocysteinemia + -
Lupus anticoagulant/APL + +
APL = antiphospholipid antibody syndrome.
COPYRIG
HT

Testing for Risk Factors
• In all patients– Cancer screening
• 20% of all patients with symptomatic VTE have cancer
– Unprovoked venous thrombosis and/or unexplained arterial thrombosis
• Antiphospholipid antibody syndrome (venous and/or arterial)
• Hyperhomocysteinemia (arterial)
• In patients younger than 50 years– AT, protein C, protein S
• Less than 5% over 50
• In patients older than 50 years– FVL, prothrombin G20210A
• 26% of men over 60 in the Physicians’ Health Study
COPYRIG
HT
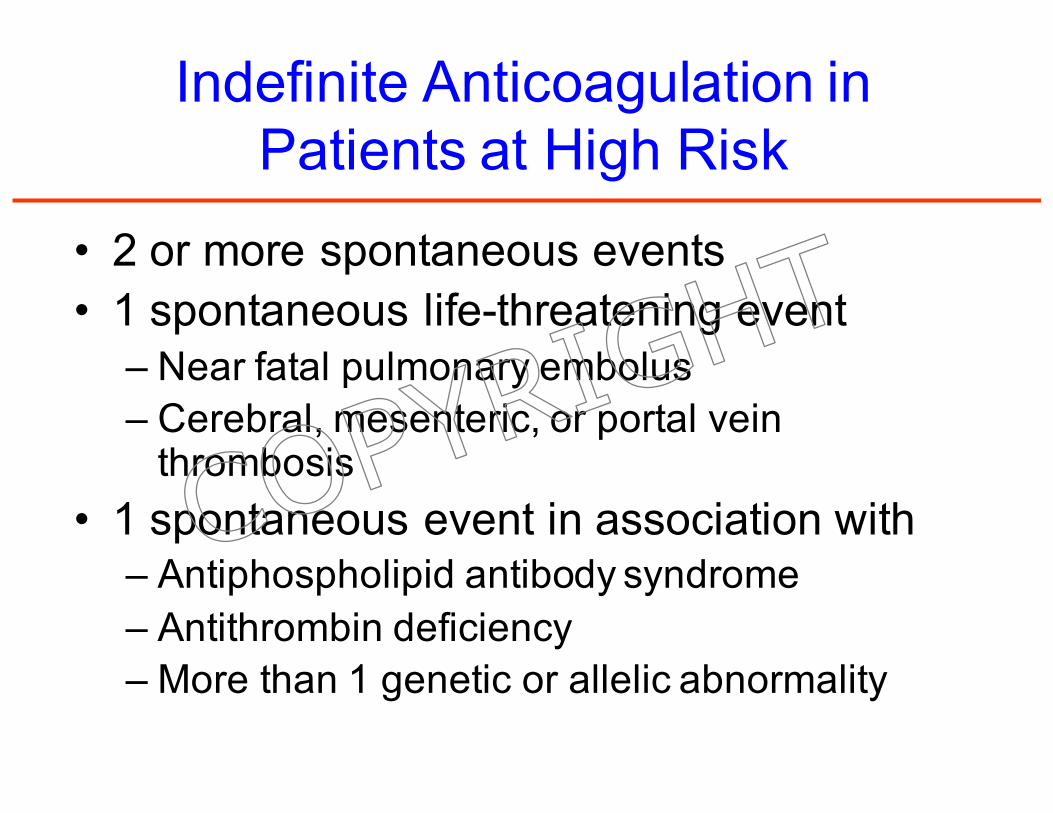
Indefinite Anticoagulation in Patients at High Risk
• 2 or more spontaneous events
• 1 spontaneous life-threatening event– Near fatal pulmonary embolus
– Cerebral, mesenteric, or portal vein thrombosis
• 1 spontaneous event in association with– Antiphospholipid antibody syndrome
– Antithrombin deficiency
– More than 1 genetic or allelic abnormality
COPYRIG
HT

Question 3COPYRIG
HT

Question 3
• A 68-year old woman has hypertension for which she takes HCTZ and low-dose aspirin daily. On routine blood testing, she is found to have a high total protein.
• On exam, she appears well without lymphadenopathy, hepatosplenomegaly or bony pain to palpation or percussion.
• Hgb = 12.9 g/dL; WBC = 6.2K/μL; platelets = 245K/μL.
• SPEP shows 1.2 g/dL monoclonal IgG-kappa. UPEP is negative for protein, including Bence Jones protein.
COPYRIG
HT
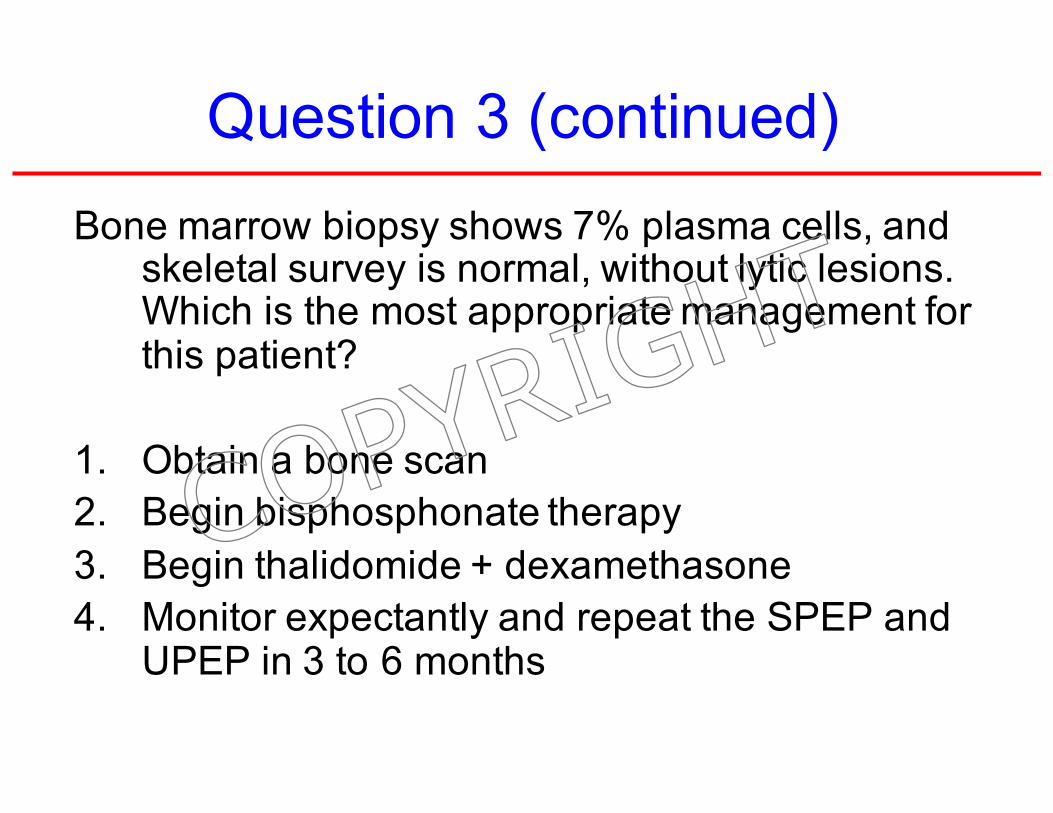
Question 3 (continued)
Bone marrow biopsy shows 7% plasma cells, and skeletal survey is normal, without lytic lesions. Which is the most appropriate management for this patient?
1. Obtain a bone scan
2. Begin bisphosphonate therapy
3. Begin thalidomide + dexamethasone
4. Monitor expectantly and repeat the SPEP and UPEP in 3 to 6 months
COPYRIG
HT
Answer = 4COPYRIG
HT

Monoclonal gammopathy of undetermined significance
• No symptoms• No end organ damage related to plasma cell
dyscrasia or a related B cell lymphoproliferative disorder– No lymphadenopathy, organomegaly, hypercalcemia,
renal failure, anemia, bone abnormalities (skeletal survey)*
• Relatively low paraprotein level (<3 g/dL)• < 10% plasmacytosis in bone marrow• Phenomenon of aging
*No role for bone scans or PET scans
COPYRIG
HT

Prevalence of MGUS According to Age Group and Sex among Residents of Olmsted County, Minnesota
Age Men Women Totalpercent
50-59 yr 2.0 1.4 1.7
60-69 yr 3.7 2.3 3.0
70-79 yr 5.6 3.8 4.6
≥ 80 yr 8.3 6.0 6.6
Total 3.7 2.9 3.2
Kyle RA et al. Prevalence of monoclonal gammopathy of undetermined significance. N Engl J Med 2006; 354:1362-9.
COPYRIG
HT

Management of MGUS
• No role for anti-plasma cell therapy
• Monitor expectantly– Monitor for signs and symptoms of progression to
multiple myeloma• Follow CBCs, BUN/cre, albumin/calcium, SPEP, UPEP, and
free serum kappa & lambda light chains
• Assess risk for progression– Lowest with paraprotein levels ≤ 0.9 g/dL
– Highest with paraprotein levels ≥ 3 g/dL
– Serum free light chain assay (FLC)• Ratio of serum free kappa to serum free lambda
COPYRIG
HT

Risk of progression to myeloma or related disorder in 1148 pts with MGUS
Rajkumar SV et al. Blood 2005; 106:812-7
COPYRIG
HT

Risk of progression of MGUS in patients with abnormal FLC ratio
Rajkumar SV et al. Blood 2005; 106:812-7
COPYRIG
HT

Diagnostic criteria for myeloma
• Myeloma– Serum or urinary monoclonal protein
– Clonal plasma cell in bone marrow or plasmacytoma
– End organ damage related to plasma cell dyscrasia
• Aymptomatic (smoldering) myeloma– Serum monoclonal protein ≥ 3 g/dL and/or bone
marrow plasma cells ≥ 10 percent
– No end organ damage related to plasma cell dyscrasia
COPYRIG
HT

Treatment of Myeloma
• Alkylating agent and corticosteroid– Melphalan mainstay of myeloma therapy for more than 40 years– Now use cyclophosphamide + bortezomib +/- lenalidomide +/-
dexamethasone
• Thalidomide– Fetal malformations; VTE; somnolence; neuropathy
• Bortezomib– Neuropathy
• Carfilzomib– Less neuropathy; more heart failure
• Lenalidomide– Myelosuppression; VTE; less somnolence & neuropathy than
thalidomide
• Autologous stem cell transplantation with high-dose melphalan– Improves survival to a median of 4.5 to 5 years
• Bisphosphonate therapy once monthly (1-2 years)– Osteonecrosis of jaw; renal dysfunction
COPYRIG
HT

COPYRIG
HT

Other Findings of “Undetermined Significance”
Steensma DP et al. Blood 2015; 126:9.
COPYRIG
HT

Question 4
COPYRIG
HT

Question 4
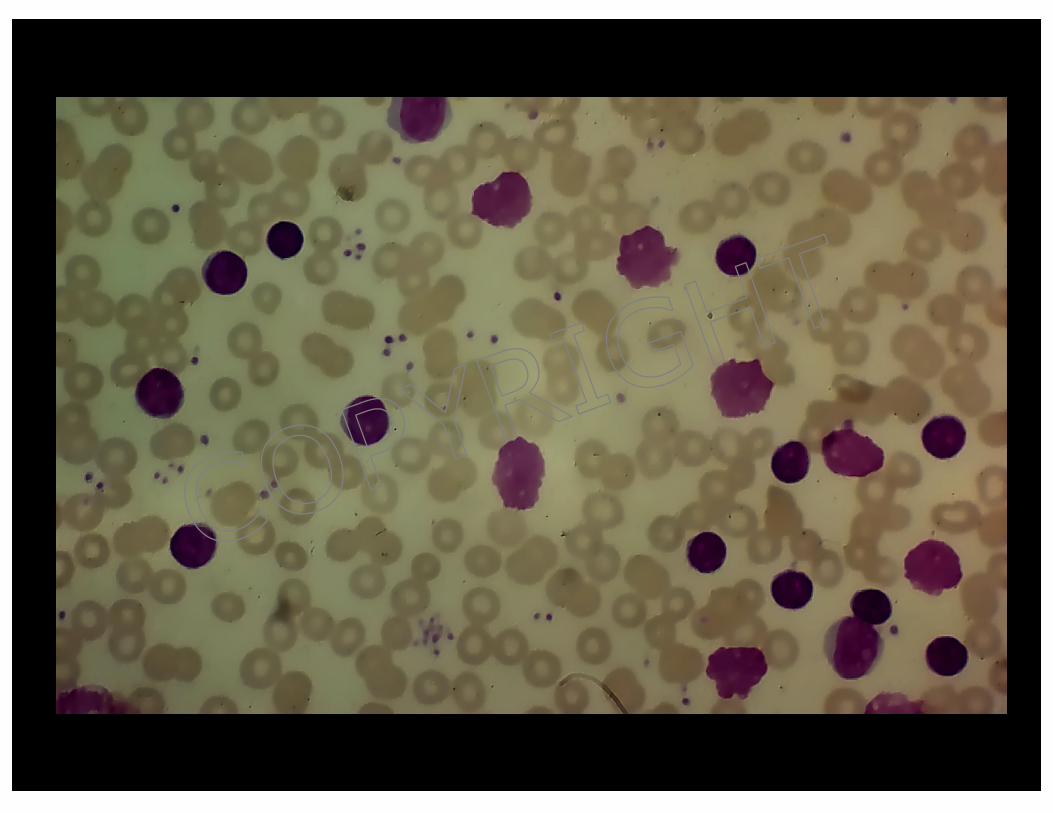
• A 65-year old presents with cervical adenopathy and splenomegaly.
• HCT = 37%; WBC = 34,000/µL with 2% polys and 98% lymphs; platelets = 177,000/µL.
• Peripheral blood smear review reveals mature appearing lymphocytes and “smudge cells” (see next slide).
COPYRIG
HT
COPYRIG
HT

Question 4 (continued)
Which of the following is true of this patient?
1. Patients in late childhood or young adulthood are as likely to have this disease as older patients
2. One should be alert for the “blast phase” of disease
3. The patient might present with autoimmune hemolytic anemia and/or immune thrombocytopenia
4. The evidence favors early treatment
COPYRIG
HT

Answer = 3COPYRIG
HT

HCL CLL PLL
COPYRIG
HT

Approximate Median Time to Treatment and Median Survival of Patients with Early-Stage Disease according to Prognostic Variables
Prognostic Variable Median Time to Treatment, y Median Survival, yResult of FISH
13q- (sole abnormality) 7.5 >11 to 15
Normal karyotype 4 >10 to 15
+12 3 10
11q- 1 6 to 9
17p- <1 2 to 4
IgVH gene mutation statusMutated ≥8 ≥20
Not mutated <4 7 to 10
ZAP-70Negative 9 to 10 ≥20
Positive 3 to 4 8 to 10
CD38Negative ≥5 ≥20
Positive <4 8 to 10
COPYRIG
HT

Question 5COPYRIG
HT

Question 5
• A 63-year old patient develops exertional dyspnea.
• On exam, sclerae are slightly icteric.
• HCT = 28% with MCV = 105; reticulocyte count = 9%; WBC and platelet counts are normal.
• The laboratory reports “bite” cells on peripheral blood smear (see next slide).
COPYRIG
HT

COPYRIG
HT

Question 5 (continued)
What is the most likely underlying mechanism of anemia in this patient?
1. Autoimmune hemolysis
2. Microangiopathic hemolytic anemia
3. Oxidant hemolysis
4. Paroxysmal nocturnal hemoglobinuria
COPYRIG
HT

Answer = 3COPYRIG
HT

Bite cells Heinz body prep
By Carola von Kapff, SH (ASCP) from UpToDateÒ
COPYRIG
HT

Drugs and chemicals in glucose-6-phosphate dehydrogenase deficiency
Unsafe for class I, II, and III variants
Acetanilid Phenylhydrazine
Dapsone Primaquine
Furazolidone Sulfacetamide
Methylene blue Sulfamethoxazole
Nalidixic acid Sulfanilamide
Naphthalene (mothballs, henna) Sulfapyridine
Niridazole Thiazosulfone
Nitrofurantoin Toluidine blue
Phenazopyridine Trinitrotoluene
Source: UpToDate®
COPYRIG
HT

Drugs and chemicals in glucose-6-phosphate dehydrogenase deficiency
Safe for class II and III variants*
Acetaminophen Phenacetin
Ascorbic acid (except in very high doses) Phenytoin
Aspirin Probenecid
Chloramphenicol Pyrimethamine
Chloroquine Quinine
Colchicine Streptomycin
Diphenhydramine Sulfisoxazole
Isoniazid Trimethoprim
L-DOPA Vitamin K
* Safety for class I variants is usually not known. Source: UpToDate®
COPYRIG
HT

Question 6COPYRIG
HT

Question 6
• A 24-year old patient develops dyspnea and is found to be anemic with HCT = 28%, MCV = 104 fL, and reticulocyte count = 6%.
• The laboratory reports 2+ spherocytes on peripheral blood smear (see next slide).COP
YRIGHT

COPYRIG
HT

Question 6 (continued)
Coombs testing is positive for IgG and negative for C3. What is the most appropriate management in this patient?
1. Transfuse packed red blood cells
2. Begin prednisone 1 mg/kg and folic acid 5 mg daily
3. Begin danazol
4. Administer rituximab
COPYRIG
HT

Answer = 2COPYRIG
HT

Macrophage
Ingesting an
IgG-Coated
RBC
Bessis M. Corpuscles. Atlas of
Red Cell Shape. Berlin, Springer-
Verlag, 1974
COPYRIG
HT

Etiologies of WAIHA
• Idiopathic• Viral infections (usually in children)• Autoimmune and connective tissue diseases
(particularly SLE)• Malignancies of the immune system
– NHL; CLL– Treatment with purine nucleoside analogs
• Immune deregulation
• Prior allogeneic blood transfusion or HSCT• Certain drugs
– Hydralazine, isoniazid, methyldopa, penicillin, procainamide, quinidine, quinine
COPYRIG
HT

Lab Findings in WAIHA• Combination of increased LDH and reduced
haptoglobin– 90% specific for diagnosing hemolysis
• Combination of normal LDH and haptoglobin > 25 mg/dL– 92% sensitive for ruling out hemolysis
• Reticulocytosis > 4-5% (median, 9%)– Lower than expected degree of reticulocytosis in 20-37%
• Lag in marrow responsiveness to hemolytic stress• Hemolysis of reticulocytes• Parvovirus B19 infection
• Spherocytosis with elevated MCHC– May not be obvious in milder cases
(1) Liesveld JL et al. Blood 1987; 69:820. (2) Marchand A et al. JAMA 1980;
243:1909. (3) Galen RS. Clin Lab Med 1982; 2:685. (4) Conley CL et al. JAMA
1980; 244:1688.
COPYRIG
HT

Treatment of WAIHA
• Can present as a medical emergency requiring immediate PRBC transfusion
– Contact Blood Bank personnel
• Stop any possible offending drug (e.g., penicillin)
• Treat underlying disease (e.g., SLE, CLL)
• Reduce autoantibody production
COPYRIG
HT

Reduction in Antibody Production
• Corticosteroids (Wendell Rosse & Stanley Schrier)– Prednisone 1 mg/kg per day– Maintain high dose for 1 week beyond goal Hgb level
(e.g., >10 g/dL)– Rapidly taper by 20 mg increments every 1 to 2 weeks
to 20 mg/day– Maintain 20 mg/day for 1 month– If remission persists
• Gradually reduce dose on alternate days to 10 mg/day and maintain for 1 month
• Omit the dose on alternate days• Reduce dose to 10 mg/day on alternate days
– Maintain this dose as long as remission persists and the DAT remains positive
• Danazol (may be steroid sparing)
COPYRIG
HT

Reduction in Antibody Production
• Immunosuppressive and cytotoxic agents– Azathioprine
• 100 to 150 mg/day
– Cyclophosphamide• 100 mg/day by mouth
• 500 to 700 mg IV every 3 to 4 weeks
• High-dose (as in aplastic anemia)
– 50 mg/kg per day IV for 4 days with Mesna and G-CSF
– Cyclosporine and mycophenolate mofetil
– Vincristine
– Rituximab
– Alemtuzumab
COPYRIG
HT

Reduction in Antibody Effectiveness
• Splenectomy
• IVIg
– Less effective than in management of ITP
COPYRIG
HT

The End
COPYRIG
HT