hemodynamic goal directed therapy 20110926
TRANSCRIPT
Perioperative hemodynamic goal-directed therapy
Flow-directed hemodynamic optimization
宋俊松

Goal-directed hemodynamic therapy
Hemodynamic treatment based on titration of fluid and inotropic agents infused to physiologic flow-related end points
(tissue oxygenation)
Perioperative goal-directed hemodynamic management
Rationale for fluid therapy
Perioperative fluid management (1)
• Previous concept of assumed perioperative fluid management: insensible perspiration + third space loss + NPO (fasting and operative period) fluid loss
• Assumptions & myths:– The preoperatively fasted patient is hypovolemic (ongoing
perspiration and urinary output)– The insensible perspiration increases dramatically when the
operation begins
– An unpredictable fluid shift toward the third space requires generous substitution
– Hypervolemia is harmless because the kidneys regulate the overload
Perioperative fluid management (2)
• Consequence of liberal fluid management: positive fluid balance and weight gain increased incidence of complications
• Truth:– Blood volume after fasting is normal– Fluid-consuming third space has never been reliably
shown– Crystalloids physiologically load the interstitial space– Colloids deteriorates a vital part of the vascular barrier– Undifferentiated fluid handling increases the shift
toward the interstitial space
Perioperative fluid management (3)
• Perioperative fluid therapy:– Lack of standardization
– Liberal (18-20 ml/kg/h) vs. restrictive ( 10 ml/kg/h) regimen
– Target:• Outcome
• Type of surgery: high-risk vs. low-risk surgery
• Demographs of patients
• Cardiac preload
• Volume (fluid) responsiveness
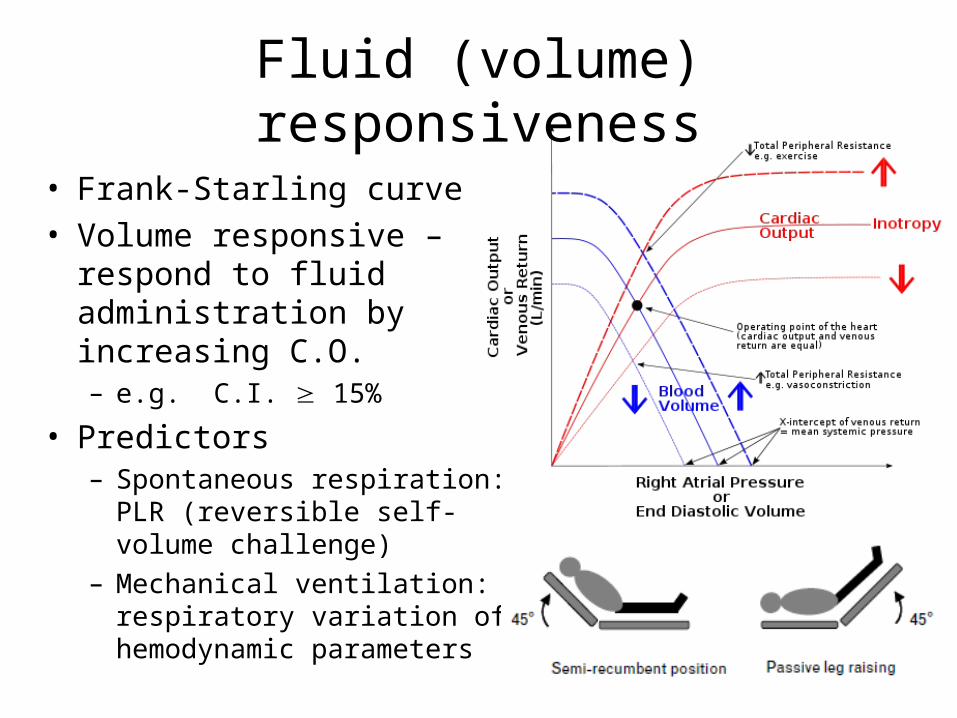
Fluid (volume) responsiveness
• Frank-Starling curve
• Volume responsive – respond to fluid administration by increasing C.O.– e.g. C.I. 15%
• Predictors– Spontaneous respiration: PLR
(reversible self-volume challenge)
– Mechanical ventilation: respiratory variation of hemodynamic parameters
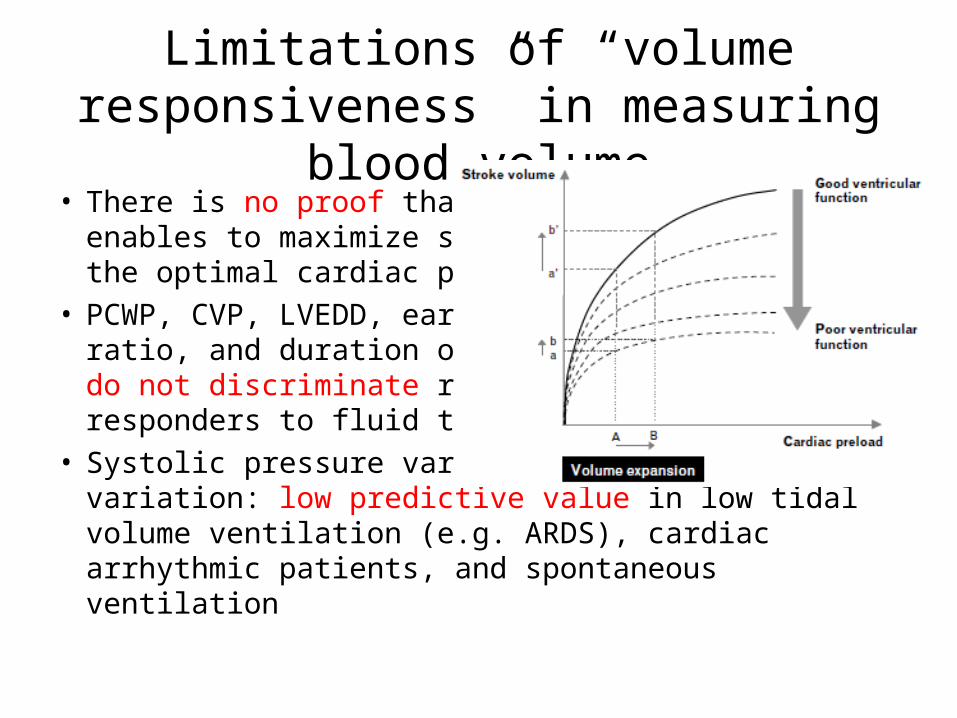
Limitations of “volume responsiveness” in measuring blood volume
• There is no proof that volume responsiveness enables to maximize stroke volume to achieve the optimal cardiac preload
• PCWP, CVP, LVEDD, early/late diastolic wave ratio, and duration of LV ejection time all do not discriminate responders and non-responders to fluid therapy
• Systolic pressure variation and pulse pressure variation: low predictive value in low tidal volume ventilation (e.g. ARDS), cardiac arrhythmic patients, and spontaneous ventilation

CVP and PCWP are not appropriate predictor of volume responsiveness
• Volume resuscitation targets on severe sepsis & septic shock– CVP 8-12 mmHg: Surviving Sepsis Campaign guidelines (Dellinger et
al., Crit Care Med 2004)
– PCWP 12-15 mmHg: the American College of Critical Care Medicine (Hollenberg et al., Crit Care Med 2004)
• Osman et al. (Crit Care Med 2007)– 96 severe septic or septic shock patients monitored with PA catheter
and mechanically ventilated in MICU
– 150 volume challenges (500 ml of 6% hydroxyethyl starch infusion for 20 min)
– Fluid responsiveness: increase in C.I. induced by the volume challenge of 15% as responder
– In septic patients receiving mechanical ventilation, cardiac filling pressures (PCWP & CVP) afford a poor prediction of fluid responsiveness
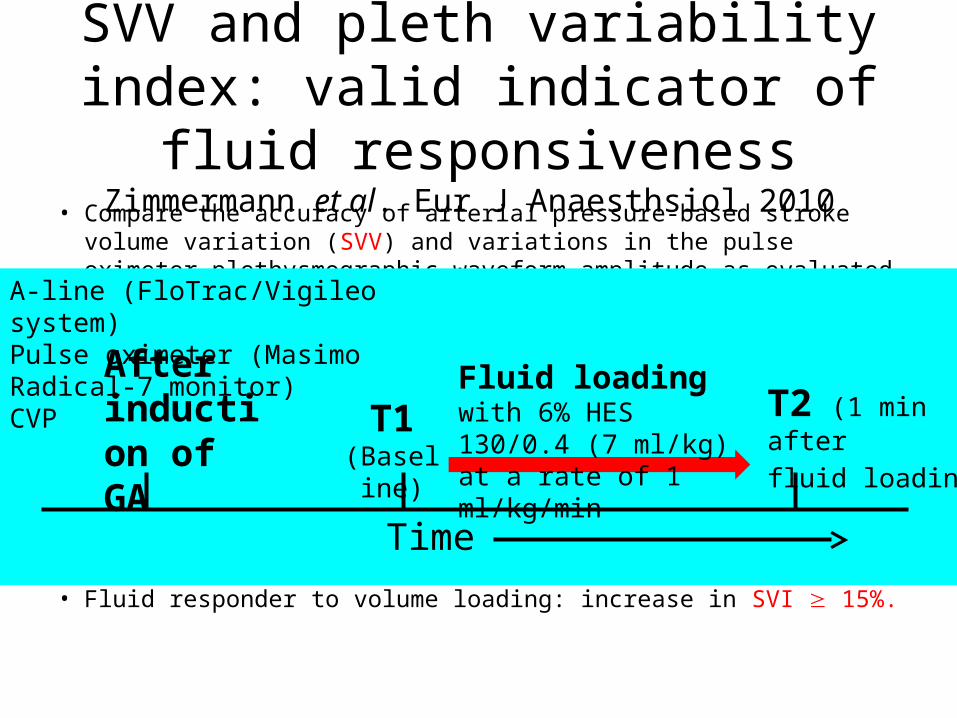
SVV and pleth variability index: valid indicator of fluid responsiveness
Zimmermann et al. Eur J Anaesthsiol 2010
• Compare the accuracy of arterial pressure-based stroke volume variation (SVV) and variations in the pulse oximeter plethysmographic waveform amplitude as evaluated with the noninvasive calculated pleth variability index (PVI) with CVP to predict the response of stroke volume index (SVI) to volume replacement in patients undergoing major surgery.
• 20 patients (M/F = 13/7) scheduled for elective major abdominal surgery
• After induction of anesthesia, all haemodynamic variables were recorded immediately before (T1) and subsequent to volume replacement (T2) by infusion of 6% hydroxy-ethyl starch (HES) 130/0.4 (7 ml/kg) at a rate of 1ml/kg/min
• Fluid responder to volume loading: increase in SVI 15%.
Time
A-line (FloTrac/Vigileo system)Pulse oximeter (Masimo Radical-7 monitor)CVP After
induction of GA
T1 (Baseline
)
T2 (1 min after
fluid loading)
Fluid loading with 6% HES 130/0.4 (7 ml/kg) at a rate of 1 ml/kg/min

SVV and pleth variability index: valid indicator of fluid responsiveness
Zimmermann et al. Eur J Anaesthsiol 2010
• Baseline SVV and PVI correlate significantly with ∆SVI whereas baseline CVP do not correlate with ∆SVI
• The best threshold value to predict fluid responsiveness:– SVV > 11%
– PVI > 9.5%
Current suggestion of perioperative fluid management
• The extracellular deficit after usual fasting is low
• The basal fluid loss via insensible perspiration is approximately 0.5-1 ml/kg/h during major abdominal surgery
• A primarily fluid-consuming third space does not exist
• Avoid over-hydration and keep an adequate fluid replacement improve outcome
Perioperative goal-directed hemodynamic management
Perfusion pressure
Perfusion pressure
• Cerebral perfusion pressure (CPP)–MAP – ICP (jugular venous pressure or CVP)
• Coronary perfusion pressure (CPP)– Right CPP = Aortic diastolic pressure – right atrial
diastolic pressure ( DABP – CVP)
– Left CPP = Aortic diastolic pressure – left atrial diastolic pressure ( DABP – PCWP)
• Abdominal perfusion pressure (APP)–MAP – IAP (intra-abdominal pressure)

Suggested optimal perfusion pressure
• Maintaining CPP (cerebral) 60-70
mmHg (in traumatic brain injury patients)
• Maintaining APP 60 mmHg

Goal-directed hemodynamic management
Beneficial effect of hemodynamic optimization
Decrease the postoperative infection• Systemic review and meta-analysis: 26 randomized, controlled
trials with a total of 4188 surgical patients (Dalfino et al., Crit Care 2011)
• Significant reduction in surgical site infection, pneumonia, urinary tract infection, and total infectious episodes
• Flow-directed hemodyanamic therapy to optimize O2 delivery protects surgical patients against postoperative hospital-acquired infections
• Strategies to prevent infection in surgical patients:– Strict asepsis
– Antibiotic prophylaxis
– Avoidance of glucose imbalance
– Normothermia
– Flow-directed hemodynamic therapy to optimize O2 delivery
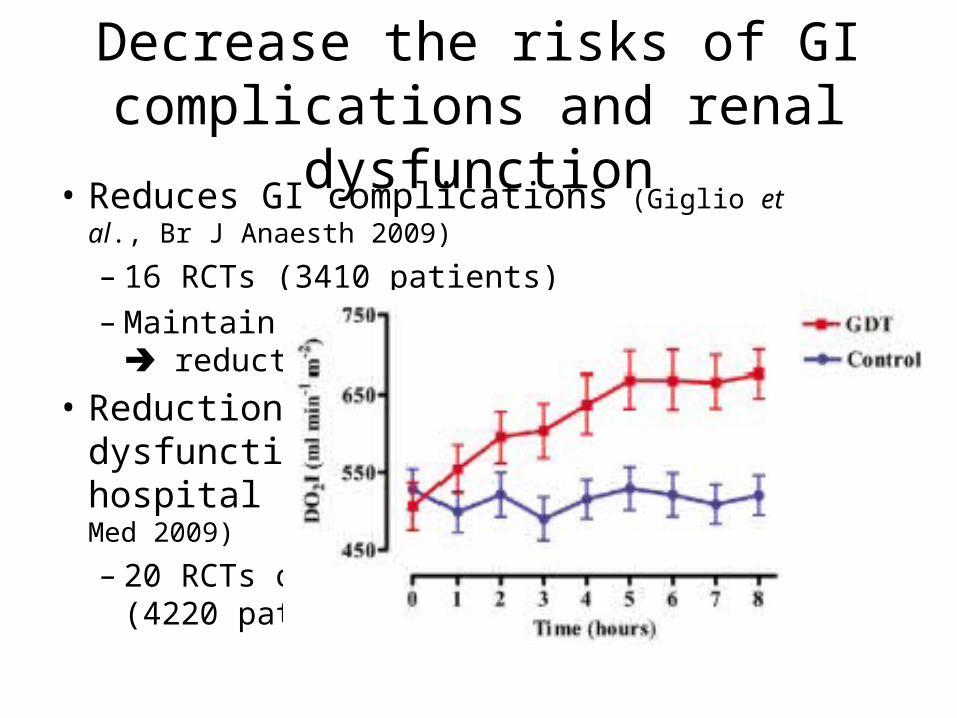
Decrease the risks of GI complications and renal dysfunction
• Reduces GI complications (Giglio et al., Br J Anaesth 2009)
– 16 RCTs (3410 patients)
– Maintain adequate tissue oxygenation reduction in GI complications
• Reduction in complicaitons, renal dysfunction and duration of hospital stay (Brienza et al., Crit Care Med 2009)
– 20 RCTs on goal-directed therapy (4220 patients)
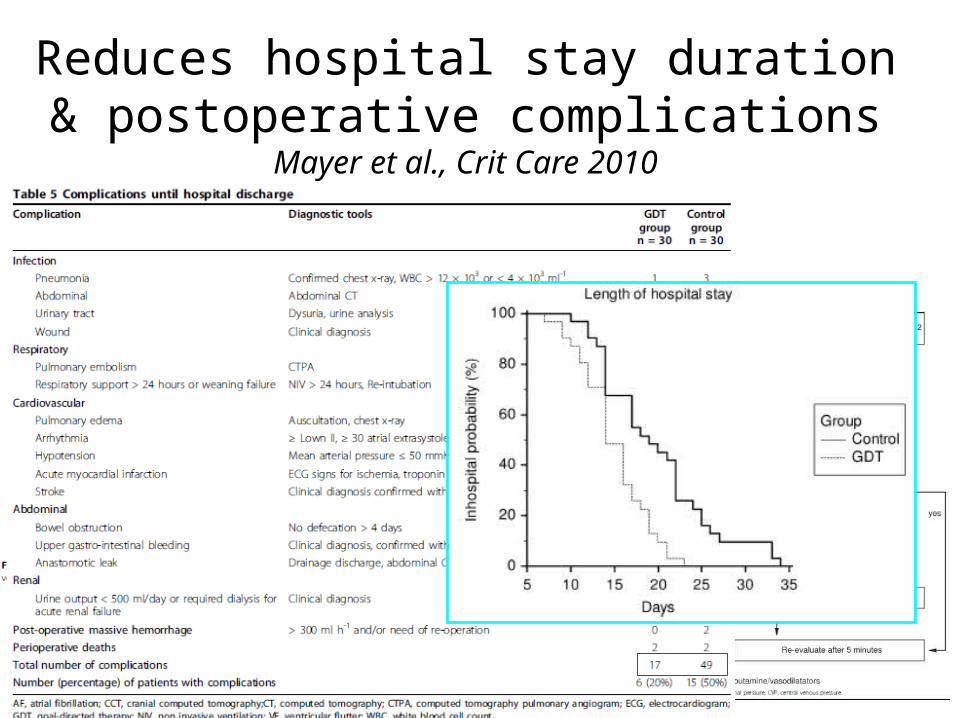
Reduces hospital stay duration & postoperative complications Mayer et al., Crit Care 2010
Goal-directed hemodynamic management
Some protocols
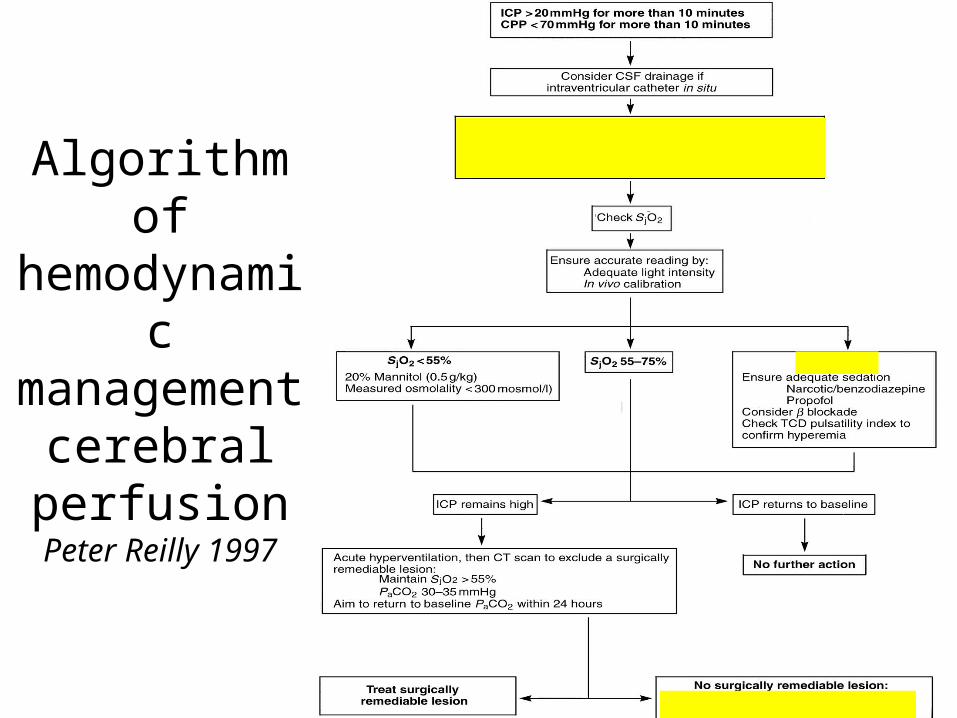
Algorithm of hemodynamic management
cerebral perfusion
Peter Reilly 1997
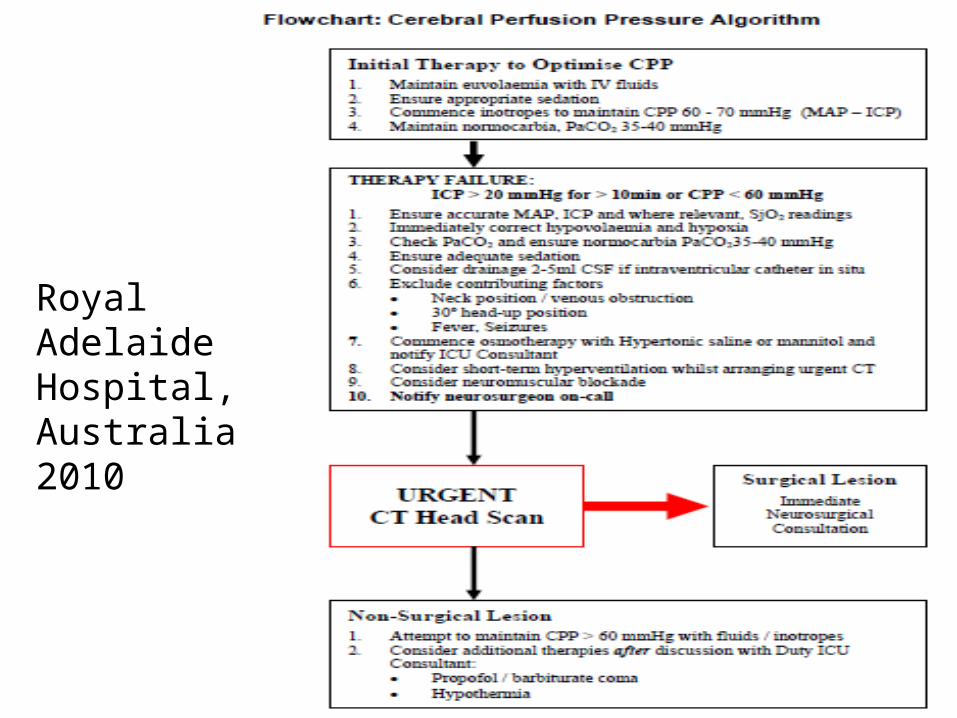
Royal Adelaide Hospital, Australia 2010
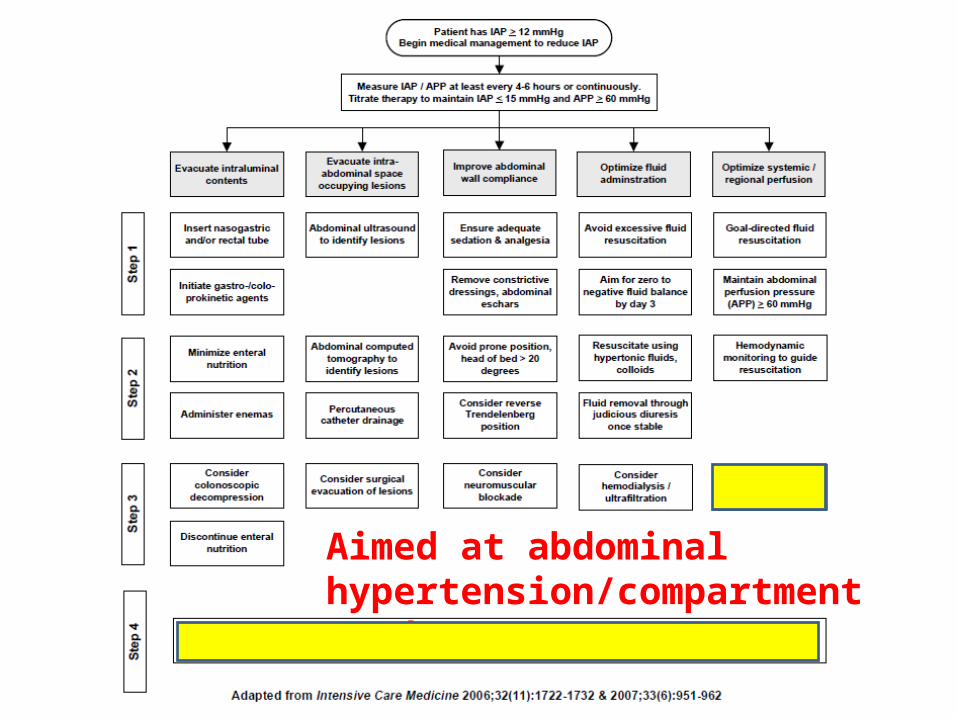
Aimed at abdominal hypertension/compartment syndrome
Summary
• Maintain adequate blood volume hemodynamic stability: avoid hypovolemia & hypoperfusion
• Improve tissue oxygenation: optimize oxidative killing ability of neutrophils, tissue repair, and wound healing
• Flow-directed hemodynamic therapy aims at optimizing perioperative tissue oxygenation
References• Chappell D, Jacob M, Hofmann-Kiefer K, Conzen P, Rehm M. A Rational
approach to perioperative fluid management. Anesthesiology 2008; 109(4):723-740.
• Monnet X, Teboul JL. Volume responsiveness. Curr Opin Crit Care 2007; 13(5):549-553.
• Zimmermann M, Feibicke T, Keyl C, Prasser C, Moritz S, Graf BM, Wiesenack C. accuracy of stroke volume variation compared with pleth variability index to predict fluid responsiveness in mechanically ventilated patients undergoing major surgery. Eur J Anaesthesiol 2010; 27(6):551-561.
• Cannesson M. Arterial pressure variation and goal-directed fluid therapy. J Cardiothorac Vasc Anesth 2010; 24(3):487-97.
• Osman D, Ridel C, Ray P, Monnet X, Anguel N, Richard C, Teboul JL. Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge. Crit Care Med 2007; 35(1):64-68.