hemodynamics disorders tutorial activities. clinical case a 25-year-old iv drug abuser presents with...
TRANSCRIPT
Hemodynamics Disorders
Tutorial activities
Clinical Case
• A 25-year-old IV drug abuser presents with high fever, chills, and rigors. On examination, he is found to have a murmur in the tricuspid valve area. His face and extremities look flushed, and his blood pressure is 90/60.
• Laboratory evaluation reveals an elevated leukocyte count with polymorphonuclear leukocytosis. Blood cultures grow gram-negative bacteria.
• He is treated with intravenous antibiotics. His blood pressure continues to fall, and urinary output declines to 100 mL/24 hr. Terminally, he develops a bleeding diathesis from vein puncture sites and mucosal surfaces.
• He dies 3 days later.
Clinical Case
• 1.What do the fever and leukocytosis indicate? • 2. What may be the reason for the tricuspid
murmur? • 3. What is the basis of thrombus formation
(vegetations) on the endocardial surface? What complications may arise from such vegetations?
• 4. What is the pathophysiology of the low blood pressure, oliguria, and renal failure in this case?
• 5. What are some of the mechanisms involved in the pathogenesis of septic shock?
• 6. What is the pathophysiology of his bleeding?

Gross Heart, view of the tricuspid valve from the right atrial
What might be the consequences of infective endocarditis with formation of vegetations on the right side of the heart?
Embolism to the lung, causing infarction. Because the vegetations are infected, the necrotic areas can be infected, leading to formation of abscesses. Spread to the bloodstream may cause septicemia

Gross outer & cut
sufaces Kidney, renal tubular necrosis due to shock
Why did this patient develop shock?
This patient had infective endocarditis with gram-negative septicemia. The shock resulted from release from the bacteria of endotoxins that triggered the release of inflammatory mediators such as IL-1 and tumor necrosis factor (TNF)

How did this patient develop shock?
TNF plays an important role in the development of septic shock by promoting the release of IL-1, IL-6, IL-8, and nitric oxide, thus initiating a cytokine cascade. These mediators, in low to moderate quantities, may lead to local inflammation and systemic effects, such as fever. When present in higher quantities, however, they promote the development of shock by causing systemic vasodilation, impaired myocardial contractility, and widespread endothelial injury, which may lead to DIC.

High power Kidney acute
tubular necrosis due to shock

What are the major morphologic changes in multiple organ failure in a patient who dies of shock?
• Kidneys: Acute tubular necrosis. • Brain: Laminar cortical necrosis. • Lungs: Shock lung (diffuse alveolar damage)
with hyaline membranes (seen mainly in septic shock).
• Heart: Foci of necrosis, hemorrhage, contraction band necrosis.
• GI: Hemorrhages. • Liver: Central hemorrhagic necrosis, fatty
change.

What is the pathophysiology of acute renal failure in septic shock?
• Distributive effect: Systemic vasodilation leads to peripheral pooling of blood and consequent reduction in visceral blood flow, including renal perfusion.

Gross coronal section Brain,
cortical laminar
necrosis
How does this picture differ from a thrombotic/embolic infarct?
• A thrombotic/embolic infarct in the brain is a localized lesion present in the area supplied by the occluded vessel. In contrast, laminar cortical necrosis is due to global hypoxic change as in shock, and hence affects a large part of the cortical ribbon.

Gross Heart, aortic
valve, infective
endocarditis

What might happen if the infected vegetation breaks loose from the valve and lodges in a distant organ?
• Infarction and abscess formation through the systemic circulation

Medium powerHeart, mitral valve,infective endocarditis

Could this person develop a cerebral infarct? What would be the appearance of such an infarct of the brain?
This patient could develop a cerebral infarct from embolization. The infarct would be an area of liquefactive necrosis along with an acute inflammatory response to the bacteria in the
embolus, resulting in brain abscess formation.

How is fibrin formed? What are the categories of coagulant proteins?
• Fibrin is derived from its precursor, fibrinogen, a proenzyme. This is one of three types of coagulant proteins. The other two are enzymes (eg, active coagulation factors) and cofactors (eg, factors V and VIII and tissue factor). The latter are also called reaction accelerators.

What complications may arise from this lesion, infective endocarditis?
• Infected vegetations on the mitral valve may embolize systemically and cause infarcts, abscesses, or septicemia. In addition, the mitral valve, chordae tendineae, or papillary muscles may rupture, causing ventricular failure.
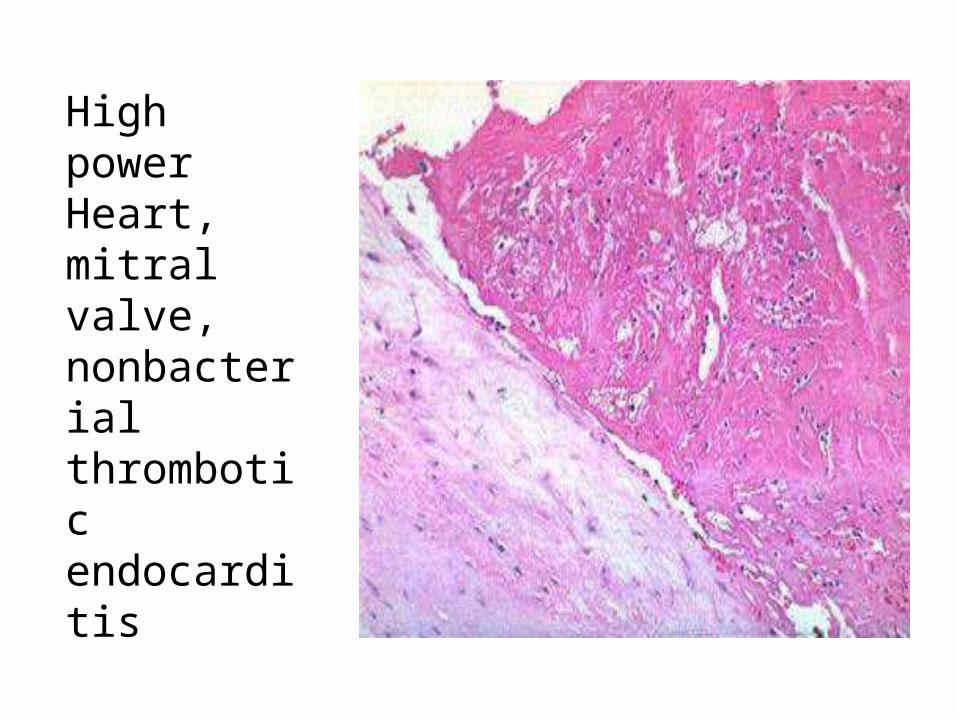
High power Heart, mitral valve, nonbacterial thrombotic endocarditis

Medium power Adrenal cortex, disseminated intravascular coagulation (DIC)

What are the most common causes of DIC?
The two most common causes are complications of pregnancy (50%) and widespread carcinomatosis (33%). The other major causes include sepsis and major trauma.

What is the spectrum of the clinical course of DIC?
• The clinical presentation and course of DIC can be quite variable, depending on the cause and the extent of individual organs involved. Acute DIC, dominated by a bleeding diathesis, is associated with obstetric complications, septic shock, or major trauma. Chronic DIC, dominated by thrombotic complications, is associated with carcinomatosis.

What are the common morphologic changes seen in DIC?
• Microthrombi in many organs - brain, heart, lungs, kidney; microinfarcts in kidney, brain, etc; hyaline membranes in lungs; adrenal hemorrhage in meningococcemia (Waterhouse-Friderichsen syndrome); necrosis of the pituitary gland (Sheehan syndrome); fragmented red cells and thrombocytopenia on the blood smear

Diagram Pathogenesis
of disseminated intravascular coagulation -

What are the two major triggers of DIC?
• Release of tissue factor and endothelial injury.

What are some of the common sources of tissue factor that can trigger DIC?
• Major trauma to tissues; the placenta in obstetric complications; mucus released by adenocarcinomas; granules of leukemic cells in acute promyelocytic leukemia; bacterial endotoxins stimulate release of tissue factor from monocytes; interleukin-1 and tumor necrosis factor stimulate expression of tissue factor on endothelial cell surfaces.

What are some of the common triggers of endothelial injury in DIC?
• Microorganisms (eg, meningococci, rickettsiae); temperature extremes (eg, heat stroke, burns); antigen-antibody complexes (eg, systemic lupus erythematosus)

What is the mechanism of DIC in sepsis?
• Bacterial endotoxins promote increased synthesis and release of tissue factor from monocytes. Activated monocytes also release IL-1 and TNF, which increase the expression of tissue factor on endothelial cells while decreasing the expression of thrombomodulin on endothelial cells. Increased tissue factor activates the clotting system. Lowered thrombomodulin levels decrease protein C activation. Thus, there is simultaneous activation of the clotting system and inhibition of coagulation control, leading to the formation of widespread microthrombi.

What is the pathophysiology of bleeding in DIC?
• Bleeding in DIC occurs as a result of the consumption of coagulation factors during the formation of widespread microthrombi. Widespread activation of the fibrinolytic system further aggravates bleeding. Plasmin cleaves not only fibrin, but also factors V and VIII. In addition, fibrinolysis leads to the formation of fibrin degradation products, which inhibit thrombin, platelet aggregation, and fibrin polymerization