heparin induced thrombocytopenia (hit-type 2) by: tom pizzoferrato, pharmd
TRANSCRIPT
Heparin Induced Heparin Induced Thrombocytopenia Thrombocytopenia
(HIT-Type 2)(HIT-Type 2)
by: by: Tom Pizzoferrato, PharmDTom Pizzoferrato, PharmD
Heparin-Induced Thrombocytopenia Heparin-Induced Thrombocytopenia Learning Objectives Learning Objectives
Understand the etiology and pathogenesis of Heparin-Induced Thrombocytopenia Understand the etiology and pathogenesis of Heparin-Induced Thrombocytopenia
Be able to differentiate the two types of HIT; Type I and Type II. Be able to differentiate the two types of HIT; Type I and Type II.
Recognize the signs and symptoms of Heparin-Induced Thrombocytopenia and institute appropriate treatment Recognize the signs and symptoms of Heparin-Induced Thrombocytopenia and institute appropriate treatment
Gain the knowledge and skills necessary to assist physicians and nurses in starting Argatroban for a patient Gain the knowledge and skills necessary to assist physicians and nurses in starting Argatroban for a patient suspected for having HIT Type 2suspected for having HIT Type 2
Effectively monitor a patient on the IV Argatroban Protocol to achieve optimal outcomesEffectively monitor a patient on the IV Argatroban Protocol to achieve optimal outcomes
Assist providers in transitioning to warfarinAssist providers in transitioning to warfarin
Many OTHER Causes of Thrombocytopenia Many OTHER Causes of Thrombocytopenia PseudothrombocytopeniaPseudothrombocytopenia- plt. clumping- plt. clumping Decreased Platelet (plt) ProductionDecreased Platelet (plt) Production
- viral infections, HIV, congenital or acquired bone marrow aplasia or- viral infections, HIV, congenital or acquired bone marrow aplasia or
hypoplasiahypoplasia
- Etoh toxicity- Etoh toxicity
- B12/ Folate deficiency- B12/ Folate deficiency
* * InIncreased Plt. Destruction creased Plt. Destruction
- ITP- ITP
- Drugs- - Drugs- heparin, quinine, quinidine, and valproic acid heparin, quinine, quinidine, and valproic acid
- DIC, Sepsis- common in ICU patients- DIC, Sepsis- common in ICU patients
- TTP- TTP - HELLP syndrome - HELLP syndrome (hemolytic anemia, elevated liver function tests, and low platelet count) in pregnant women (hemolytic anemia, elevated liver function tests, and low platelet count) in pregnant women
- Mono, CMV- Mono, CMV• Dilutional –Common w Blood products, IVF’s –Common w Blood products, IVF’s • Spenic SequestrationSpenic Sequestration
Types of HITTypes of HIT
Type 1 HIT Type 1 HIT
– – common form of thrombocytopeniacommon form of thrombocytopenia
- no clinical consequence - no clinical consequence
- slight fall in platelet count within the first two days after heparin - slight fall in platelet count within the first two days after heparin (plt. >100,000)(plt. >100,000)
- returns to normal with continued heparin administration - returns to normal with continued heparin administration
- nonimmune - nonimmune
• Type 2 HIT Type 2 HIT = heparin associated thrombocytopenia= heparin associated thrombocytopenia
- less common- less common
- serious consequences- thrombosis and white clot ( arterial)- serious consequences- thrombosis and white clot ( arterial)
- large fall in platelet count within 1-7 days after heparin - large fall in platelet count within 1-7 days after heparin (Plt < 100,000)(Plt < 100,000)
- platelets rise in 6-8 days after all heparin/lmwh is dc’d- platelets rise in 6-8 days after all heparin/lmwh is dc’d
- immune-mediated with Antibodies vs Plt-F4- immune-mediated with Antibodies vs Plt-F4
HIT –Type 2HIT –Type 2
Antibody-mediated, adverse effect of heparin•Affects 1-4% of patients receiving heparin for at least 7 days–Higher rate for UFH–Lower for LMWH
•Strong association with venous and arterial thrombosis(30-75% risk in untreated patients)
Clinical featuresClinical featuresThrombocytopenia occurring after 5-7 days Thrombocytopenia occurring after 5-7 days of heparin therapy, can occur sooner on re-of heparin therapy, can occur sooner on re-exposureexposurePlatelet count nadir is between 20,000 and Platelet count nadir is between 20,000 and 150,000/ul, median 50,000/ul150,000/ul, median 50,000/ulBleeding is rareBleeding is rare
HIT- type 2HIT- type 2
Mechanisms of Type 2 HITMechanisms of Type 2 HIT Heparin-PF4 complex binds to activated platelet surface and forms Heparin-PF4 complex binds to activated platelet surface and forms
heparin-PF4-AB complex on the platelet surface [32,42]. heparin-PF4-AB complex on the platelet surface [32,42]. The Fc portion of this bound IgG further activates other platelets The Fc portion of this bound IgG further activates other platelets
and leads to more platelet activation with further release of PF4and leads to more platelet activation with further release of PF4 Activated PLT-Hep-PF4-AB complex undergoes aggregation and Activated PLT-Hep-PF4-AB complex undergoes aggregation and
are removed prematurely from the circulation leading to are removed prematurely from the circulation leading to thrombocytopenia (HIT)thrombocytopenia (HIT)
Generation of procoagulant platelet-derived microparticles, Generation of procoagulant platelet-derived microparticles, frequently resulting in thrombin generation and thrombosis (HITT) frequently resulting in thrombin generation and thrombosis (HITT)
The AB complex also activates microvascular endothelial cells, The AB complex also activates microvascular endothelial cells, resulting in release of IL-6- von Willebrand factor can injure resulting in release of IL-6- von Willebrand factor can injure endothelium which promotes thrombosis [endothelium which promotes thrombosis [
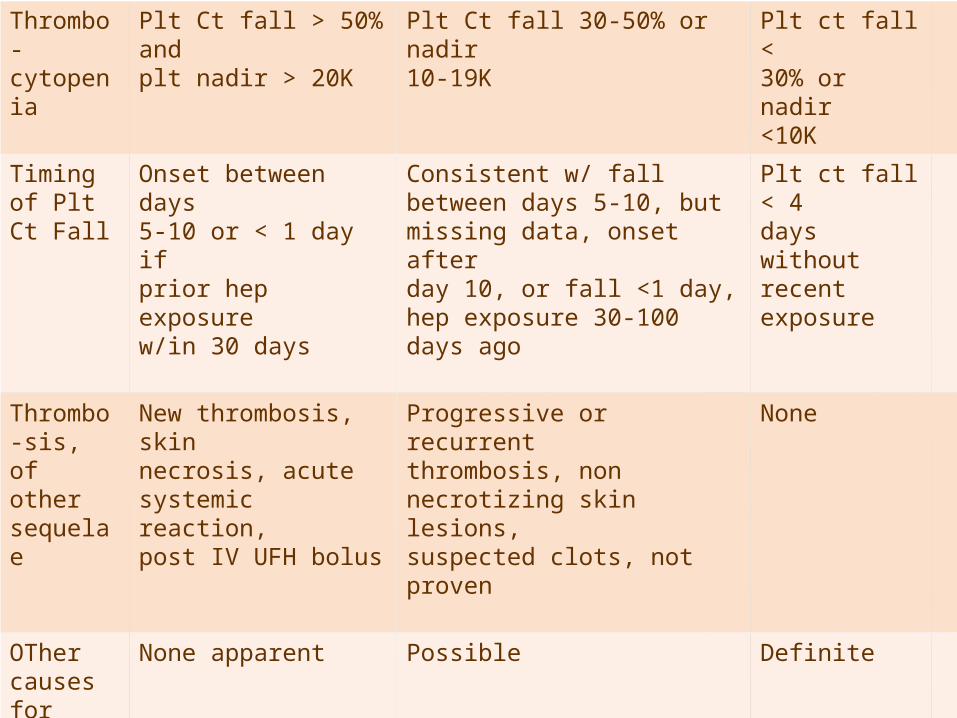
T Score System
2 points 1 point 0 point
Thrombo-cytopenia
Plt Ct fall > 50% andplt nadir > 20K
Plt Ct fall 30-50% or nadir10-19K
Plt ct fall <30% or nadir<10K
Timing of Plt Ct Fall
Onset between days5-10 or < 1 day ifprior hep exposurew/in 30 days
Consistent w/ fallbetween days 5-10, butmissing data, onset afterday 10, or fall <1 day,hep exposure 30-100days ago
Plt ct fall < 4days withoutrecentexposure
Thrombo-sis, of othersequelae
New thrombosis, skinnecrosis, acutesystemic reaction,post IV UFH bolus
Progressive or recurrentthrombosis, nonnecrotizing skin lesions,suspected clots, notproven
None
OTher causes forThrombo-cytopeniaT Score: Probability
None apparent
6-8 pts- HIT Likely
Possible
4-5- HIT Possible
Definite
0-3- HIT Unlikely
Possible sequela from HIT Possible sequela from HIT ((Heparin/LMWH ExposureHeparin/LMWH Exposure))
These may be indication of Developing HIT Type 2These may be indication of Developing HIT Type 2
Erythematous PlaquesErythematous Plaques
Heparin-Induced Skin NecrosisHeparin-Induced Skin Necrosis
Venous Gangrene (extremities)Venous Gangrene (extremities)
Warkentin TE. Heparin Induced Thrombocytopenia, 2nd Ed. Marcel Dekker, Warkentin TE. Heparin Induced Thrombocytopenia, 2nd Ed. Marcel Dekker, Inc; New York 2001Inc; New York 2001
HIT – DiagnosisHIT – Diagnosis
HIT should be considered a clinico-HIT should be considered a clinico-pathologic syndromepathologic syndrome
••Diagnosis requires both a compatible clinical history and Diagnosis requires both a compatible clinical history and demonstration of HIT antibody seroconversiondemonstration of HIT antibody seroconversion
••Demonstration of a heparin dependent platelet antibody Demonstration of a heparin dependent platelet antibody alone is insufficientalone is insufficient
* Use T score to help screen* Use T score to help screen* The HIT tests should NOT be used for screening of * The HIT tests should NOT be used for screening of
asymptomatic patients prior to or during heparin asymptomatic patients prior to or during heparin exposureexposure
-Warkentin, 2005-Warkentin, 2005
Heparin Antibody AssaysHeparin Antibody Assays
• Platelet Aggregation- not usefulPlatelet Aggregation- not useful
• 14C-Serotonin Release Assay 14C-Serotonin Release Assay (SRA)(SRA)
For confirmationFor confirmation
• Heparin-Induced Platelet Heparin-Induced Platelet Agglutination (HIPA)Agglutination (HIPA)
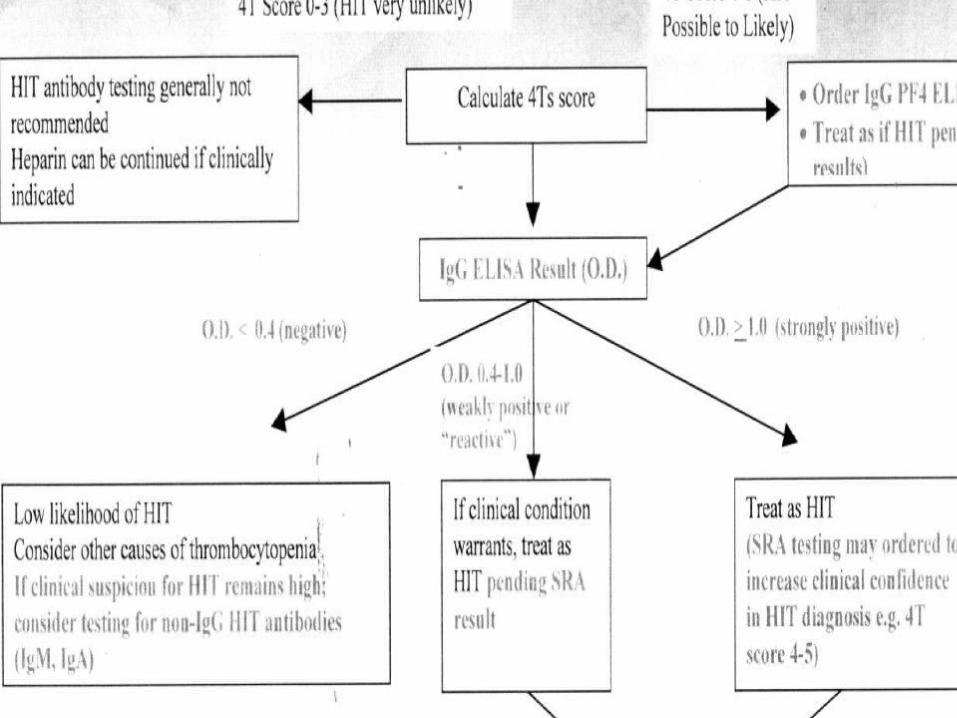
• Heparin/PF4 ELISA- Initial screenHeparin/PF4 ELISA- Initial screen
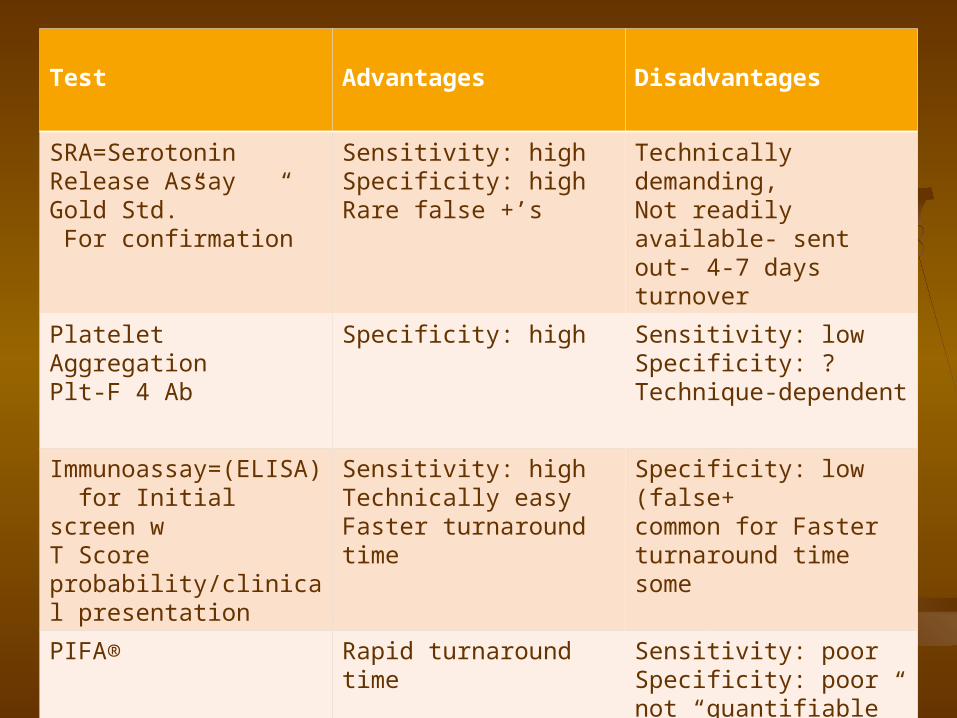
Test Advantages Disadvantages
SRA=Serotonin Release Assay “ Gold Std.” For confirmation
Sensitivity: highSpecificity: highRare false +’s
Technically demanding,Not readily available- sent out- 4-7 days turnover
Platelet AggregationPlt-F 4 Ab
Specificity: high Sensitivity: lowSpecificity: ?Technique-dependent
Immunoassay=(ELISA) for Initial screen w T Score probability/clinical presentation
Sensitivity: highTechnically easyFaster turnaround time
Specificity: low (false+common for Faster turnaround time some
PIFA® Rapid turnaround time Sensitivity: poorSpecificity: poornot “quantifiable”

HITHIT The incidence of HIT is likely to increase as an aging patient The incidence of HIT is likely to increase as an aging patient
population develops diseases and undergoes more complex population develops diseases and undergoes more complex procedures requiring heparin anticoagulation.procedures requiring heparin anticoagulation.
Early recognition, thorough risk assessment and platelet count Early recognition, thorough risk assessment and platelet count monitoring, and appropriate treatment of HIT are critical in reducing monitoring, and appropriate treatment of HIT are critical in reducing morbidity and mortality.morbidity and mortality.
The essence of appropriate treatment is:The essence of appropriate treatment is:
- - Immediate discontinuation of all sources of heparin,(IV, subq, Immediate discontinuation of all sources of heparin,(IV, subq, Heparin coated catheters & flushes and LMWH’s) and warfarin Heparin coated catheters & flushes and LMWH’s) and warfarin..
- Initiation of alternative anticoagulant (even if no clinical- Initiation of alternative anticoagulant (even if no clinical
thrombosis)thrombosis)
- Do not delay treatment pending confirmation by laboratory tests.- Do not delay treatment pending confirmation by laboratory tests.


Treatment Goals Based on Treatment Goals Based on Pathophysiology and Clinical StudiesPathophysiology and Clinical Studies
Interrupt the immune responseInterrupt the immune response
- - Discontinue heparin & flushes, LMWHDiscontinue heparin & flushes, LMWH
Inhibit thrombin generationInhibit thrombin generation
- - Treat active thrombosisTreat active thrombosis
Prevent new thrombosisPrevent new thrombosis Minimize complications of HITMinimize complications of HIT
- - Thromboses, limb amputation, deathThromboses, limb amputation, death
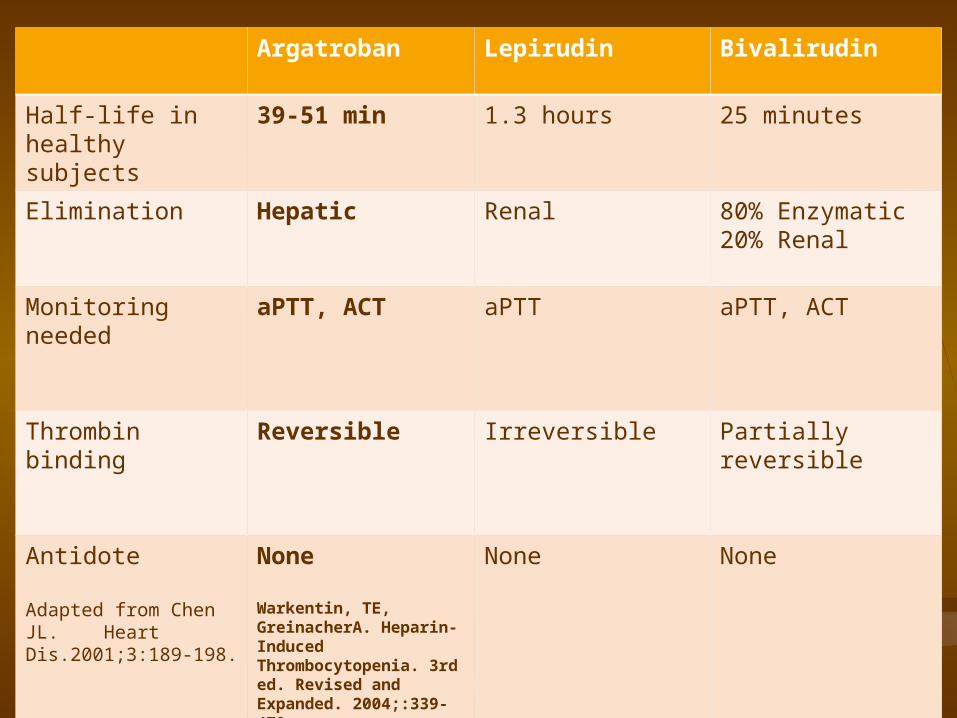
Argatroban Lepirudin Bivalirudin
Half-life in healthy subjects
39-51 min 1.3 hours 25 minutes
Elimination Hepatic Renal 80% Enzymatic20% Renal
Monitoring needed
aPTT, ACT aPTT aPTT, ACT
Thrombin binding Reversible Irreversible Partiallyreversible
Antidote
Adapted from Chen JL. Heart Dis.2001;3:189-198.
None
Warkentin, TE, GreinacherA. Heparin-Induced Thrombocytopenia. 3rd ed. Revised and Expanded. 2004;:339-479.
None None
Direct Thrombin Inhibitors: FDA Direct Thrombin Inhibitors: FDA Indications and UsageIndications and Usage
ArgatrobanArgatroban - Preferred - Preferred
-Indicated as an anticoagulant for prophylaxis or -Indicated as an anticoagulant for prophylaxis or
treatment of thrombosis in patients with HIT Type 2treatment of thrombosis in patients with HIT Type 2
- Indicated as an anticoagulant in patients with or at - Indicated as an anticoagulant in patients with or at risk risk
for HIT undergoing PCI – bivalirudin is used @ JDHfor HIT undergoing PCI – bivalirudin is used @ JDH
**Lepirudin- not made, supplies to be exhausted in mid2013Lepirudin- not made, supplies to be exhausted in mid2013
- Indicated for anticoagulation in patients with HIT and - Indicated for anticoagulation in patients with HIT and
associated thromboembolic disease to prevent furtherassociated thromboembolic disease to prevent further
thromboembolic complicationsthromboembolic complications BivalirudinBivalirudin
- Indicated as an anticoagulant in patients undergoing- Indicated as an anticoagulant in patients undergoing
percutaneoustransluminalcoronary angioplasty (PTCApercutaneoustransluminalcoronary angioplasty (PTCA))


Argatroban Argatroban
Indication: Treatment of Heparin Induced thrombocytopenia Indication: Treatment of Heparin Induced thrombocytopenia Dosing: Infusion ConcentrationDosing: Infusion Concentration
250 mg/ 250 mls NS= 1mg/1 ml= 1000 mcg/ml250 mg/ 250 mls NS= 1mg/1 ml= 1000 mcg/ml
No initial bolus dose required.No initial bolus dose required. Criteria for Use: Criteria for Use:
- Patient at intermediate to high risk for HIT - Patient at intermediate to high risk for HIT • Have MD’s follow existing protocolHave MD’s follow existing protocol• If you receive a request to vary from protocolIf you receive a request to vary from protocol
1st. Discuss w provider that the Hem/Onc team has agreed to protocol and 1st. Discuss w provider that the Hem/Onc team has agreed to protocol and no literature demonstrates that varying the Goal PTT is of benefit. If still no literature demonstrates that varying the Goal PTT is of benefit. If still an issue then an issue then
2. Call Clinical Coordinator to have discussion w provider2. Call Clinical Coordinator to have discussion w provider
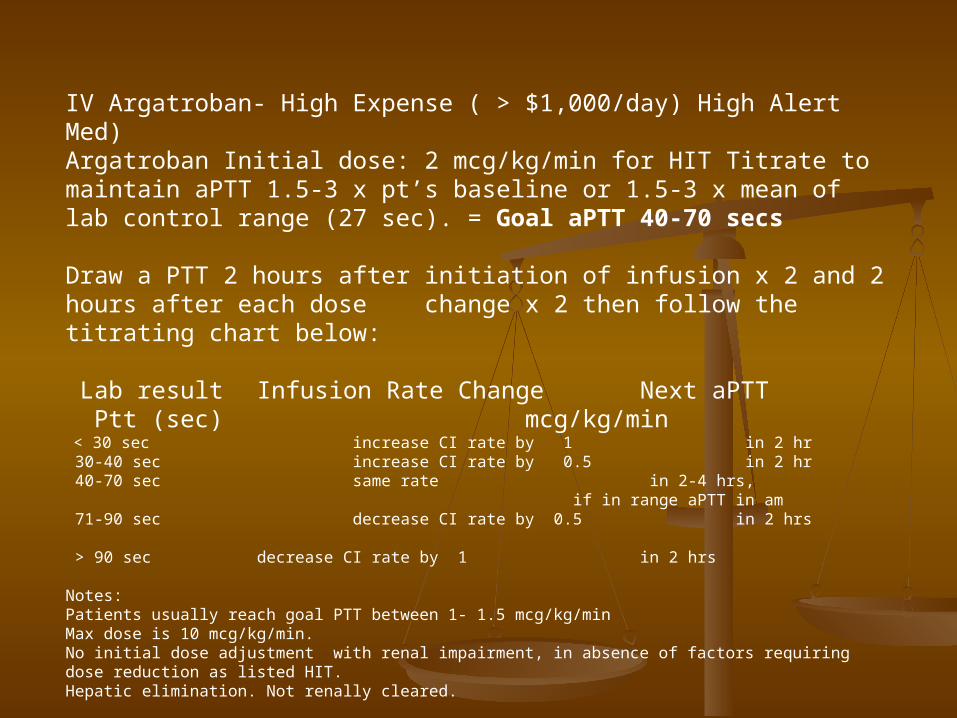
IV Argatroban- High Expense ( > $1,000/day) High Alert Med)Argatroban Initial dose: 2 mcg/kg/min for HIT Titrate to maintain aPTT 1.5-3 x pt’s baseline or 1.5-3 x mean of lab control range (27 sec). = Goal aPTT 40-70 secs
Draw a PTT 2 hours after initiation of infusion x 2 and 2 hours after each dose change x 2 then follow the titrating chart below:
Lab result Infusion Rate Change Next aPTT Ptt (sec) mcg/kg/min < 30 sec increase CI rate by 1 in 2 hr 30-40 sec increase CI rate by 0.5 in 2 hr 40-70 sec same rate in 2-4 hrs,
if in range aPTT in am 71-90 sec decrease CI rate by 0.5 in 2 hrs > 90 sec decrease CI rate by 1 in 2 hrs
Notes:Patients usually reach goal PTT between 1- 1.5 mcg/kg/minMax dose is 10 mcg/kg/min.No initial dose adjustment with renal impairment, in absence of factors requiring dose reduction as listed HIT. Hepatic elimination. Not renally cleared.
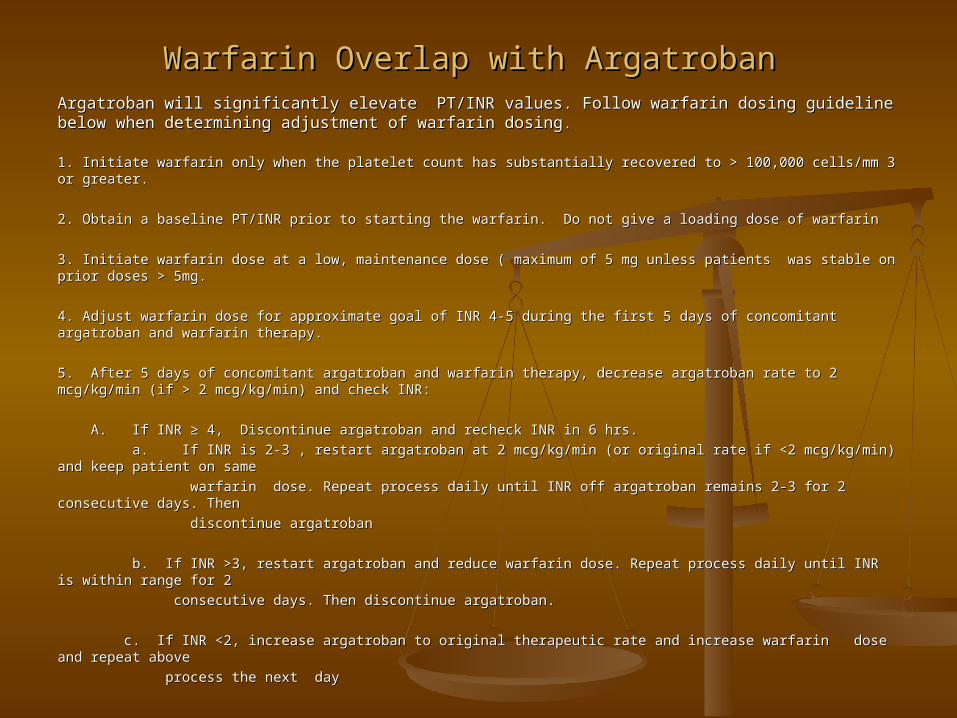
Warfarin Overlap with Argatroban Warfarin Overlap with Argatroban Argatroban will significantly elevate PT/INR values. Follow warfarin dosing guideline below when Argatroban will significantly elevate PT/INR values. Follow warfarin dosing guideline below when determining adjustment of warfarin dosingdetermining adjustment of warfarin dosing . .
1. Initiate warfarin only when the platelet count has substantially recovered to > 100,000 cells/mm 3 or greater. 1. Initiate warfarin only when the platelet count has substantially recovered to > 100,000 cells/mm 3 or greater.
2. Obtain a baseline PT/INR prior to starting the warfarin. Do not give a loading dose of warfarin 2. Obtain a baseline PT/INR prior to starting the warfarin. Do not give a loading dose of warfarin
3. Initiate warfarin dose at a low, maintenance dose ( maximum of 5 mg unless patients was stable on prior doses > 3. Initiate warfarin dose at a low, maintenance dose ( maximum of 5 mg unless patients was stable on prior doses > 5mg.5mg.
4. Adjust warfarin dose for approximate goal of INR 4-5 during the first 5 days of concomitant argatroban and warfarin 4. Adjust warfarin dose for approximate goal of INR 4-5 during the first 5 days of concomitant argatroban and warfarin therapy.therapy.
5. After 5 days of concomitant argatroban and warfarin therapy, decrease argatroban rate to 2 mcg/kg/min (if > 2 5. After 5 days of concomitant argatroban and warfarin therapy, decrease argatroban rate to 2 mcg/kg/min (if > 2 mcg/kg/min) and check INR: mcg/kg/min) and check INR:
A. If INR ≥ 4, Discontinue argatroban and recheck INR in 6 hrs. A. If INR ≥ 4, Discontinue argatroban and recheck INR in 6 hrs.
a. If INR is 2-3 , restart argatroban at 2 mcg/kg/min (or original rate if <2 mcg/kg/min) and keep patient on same a. If INR is 2-3 , restart argatroban at 2 mcg/kg/min (or original rate if <2 mcg/kg/min) and keep patient on same
warfarin dose. Repeat process daily until INR off argatroban remains 2-3 for 2 consecutive days. Thenwarfarin dose. Repeat process daily until INR off argatroban remains 2-3 for 2 consecutive days. Then
discontinue argatroban discontinue argatroban
b. If INR >3, restart argatroban and reduce warfarin dose. Repeat process daily until INR is within range for 2 b. If INR >3, restart argatroban and reduce warfarin dose. Repeat process daily until INR is within range for 2
consecutive days. Then discontinue argatroban. consecutive days. Then discontinue argatroban.
c. If INR <2, increase argatroban to original therapeutic rate and increase warfarin dose and repeat abovec. If INR <2, increase argatroban to original therapeutic rate and increase warfarin dose and repeat above
process the next dayprocess the next day
Argatroban ProtocolArgatroban Protocol BB. If INR < 4, Return argatroban infusion to original therapeutic rate and increase . If INR < 4, Return argatroban infusion to original therapeutic rate and increase
warfarin dose. Check INR daily for 2 days. warfarin dose. Check INR daily for 2 days.
a. If after 2 days INR has not increased, increase warfarin dose and repeat process.a. If after 2 days INR has not increased, increase warfarin dose and repeat process.
b. If INR has increased but still < 4, repeat process at same warfarin dose untilb. If INR has increased but still < 4, repeat process at same warfarin dose until
INR ≥ 4, then follow as in a aboveINR ≥ 4, then follow as in a above
c. If new INR ≥ 4, follow as in a abovec. If new INR ≥ 4, follow as in a above
MD/LIP ResponsibilityMD/LIP Responsibility:: Order labs: Baseline: PT, PTT, CBC with platelet count, Stool for blood, urinalysis Order labs: Baseline: PT, PTT, CBC with platelet count, Stool for blood, urinalysis
Platelet count, Hematocrit q 2-3 daysPlatelet count, Hematocrit q 2-3 days
Nursing ResponsibilityNursing Responsibility::
Requires RN/LPN verification double check on MAR.Requires RN/LPN verification double check on MAR.
Infusion via Guardrails on Alaris Volumetric Infusion PumpInfusion via Guardrails on Alaris Volumetric Infusion Pump
Order f/u PTT’s and Monitor PTTOrder f/u PTT’s and Monitor PTT
Monitor bleeding symptoms, Monitor bleeding symptoms,
Pharmacist responsibilitiesPharmacist responsibilities::
- Upon initial Order validation provide Argatroban written protocol for RN, Review w them- Upon initial Order validation provide Argatroban written protocol for RN, Review w them
- Assure DC of all heparin/lmwh sources- Assure DC of all heparin/lmwh sources
- Double calc’s, monitor supplies and dispensing to minimize waste- Double calc’s, monitor supplies and dispensing to minimize waste
- Monitor daily & document in Siemans notes, PUP Com. sheet, shift report- Monitor daily & document in Siemans notes, PUP Com. sheet, shift report
- Warfarin dose validation- Warfarin dose validation
- Monitor for compliance with transition to warfarin - to references for transition to warfarin.- Monitor for compliance with transition to warfarin - to references for transition to warfarin.
Adjust dose for approximate goal of INR 4-5 during the first 5 days of concomitant argatroban andAdjust dose for approximate goal of INR 4-5 during the first 5 days of concomitant argatroban and
warfarin therapywarfarin therapy. .
ACCP Guidelines: HITACCP Guidelines: HIT
Do not use Vitamin K antagonists (\Do not use Vitamin K antagonists (\warfarin) until after the platelet count is > warfarin) until after the platelet count is > 150,000/ul150,000/ul
And only during overlap with alternative And only during overlap with alternative anticoagulationanticoagulation
Start VKA at lower dose (5-6 mg)Start VKA at lower dose (5-6 mg)
Alternative anticoagulants should not be Alternative anticoagulants should not be dc’d until platelet count has reached a dc’d until platelet count has reached a stable plateau and with at least the last 2 stable plateau and with at least the last 2 days of INR within target therapeutic rangedays of INR within target therapeutic range
The EndThe EndProceed to Post TestProceed to Post Test