hepatitis b: state of the art and open challenges · hepatitis b: state of the art and open...
TRANSCRIPT

Hepatitis B: State of the Art and open challenges
Berlin, October 20,2012Berlin, October 20,2012
Jorg PetersenLiver UnitIFI Institute for Interdisciplinary Medicine Asklepios Klinik St. Georg University of Hamburg
email: [email protected]

Baruch Blumberg * 28.07.1925 ‐
†
05.04.2011
Nobel laureate for Medicine 1976 für the isolation of Hepatitis B Virus (JAMA 1965)

mod. from S Urban and J Petersen; J Hepatology 2010
Once HBV –
always HBV ?!
1.
Immunological control of the virus but noeradication
2. No new drugs in phase III
3. HBsAg quantification in EASL CPG 2012

The main differences between HIV, HBV and HCV
HH
HBV
Host cell
cccDNAHost DNA
Integrated DNA
Nucleus
HH
HIV
Host cell
Host DNA
Proviral DNA
Nucleus
HH
HCV
Host cell
Host DNA
Nucleus
HCV RNA
Lifelong suppression of viral replication
Viral clearanceand SVR
Longterm suppression of viral replication
Kieffer et al. J Antimicrob Chemother 2010; Sorriano et al. J Antimicrob Chemother 2009; Clavel et al. New Engl J Med 2004; Zoulim &Locarnini Gastroenterology 2009; Sarrazin & Zeuzem Gastroenterology 2010

www.easl.eu
„HBsAg loss and viral suppression are the main goals of treatment“

HBsAg clearance improves survival
No HBsAg clearance
20
40
60
80
100
Surv
ival
(%)
With HBsAg clearance
P<0.001
Retrospective study of 309 cirrhotic patients over mean follow-up of 5.7 years
Fattovich et al. Am J Gastroenterol 1998
Time (years)0
2 4
6
8 10 12 14

Yang NEJM 2002
12
10
8
6
4
2
0
Perc
ent c
umul
ativ
e in
cide
nce
0 1 2 3 4 5 6 7 8 9 10Time (years)
HBsAg+, HBeAg+
HBsAg–, HBeAg–
No eradication of HBV but HBsAg clearance reduces the risk of HCC
29.11.2012
8
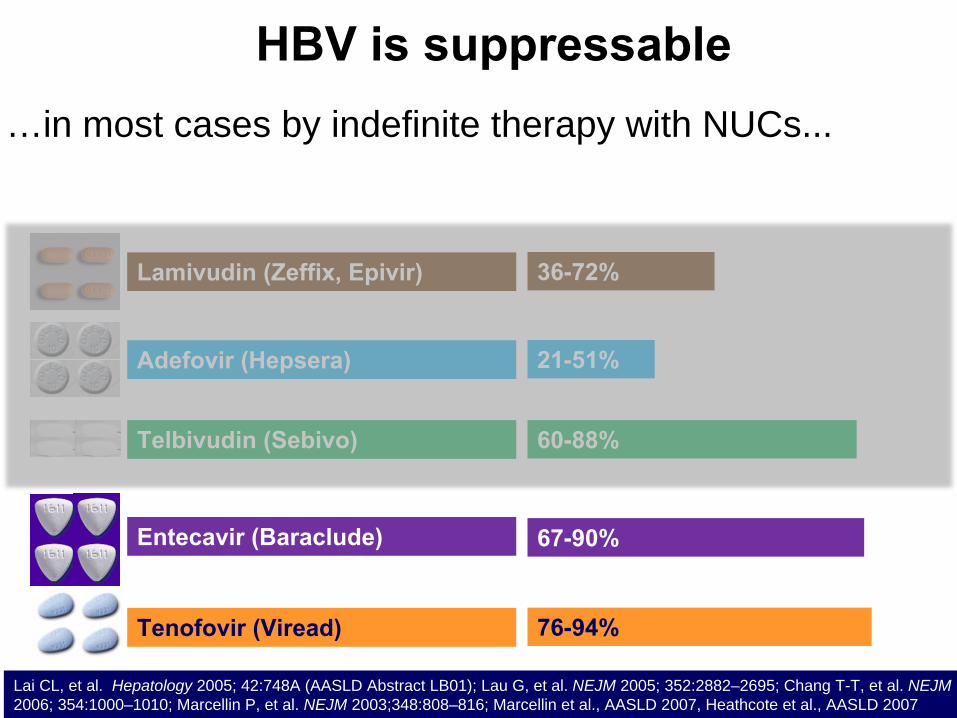
Lamivudin (Zeffix, Epivir)
Adefovir (Hepsera)
Entecavir (Baraclude)
Telbivudin (Sebivo)
Tenofovir (Viread)
36-72%
21-51%
67-90%
60-88%
76-94%
Lai CL, et al. Hepatology 2005; 42:748A (AASLD Abstract LB01); Lau G, et al. NEJM 2005; 352:2882–2695; Chang T-T, et al. NEJM 2006; 354:1000–1010; Marcellin P, et al. NEJM 2003;348:808–816; Marcellin et al., AASLD 2007, Heathcote et al., AASLD 2007
…in most cases by indefinite therapy with NUCs...
HBV is suppressable
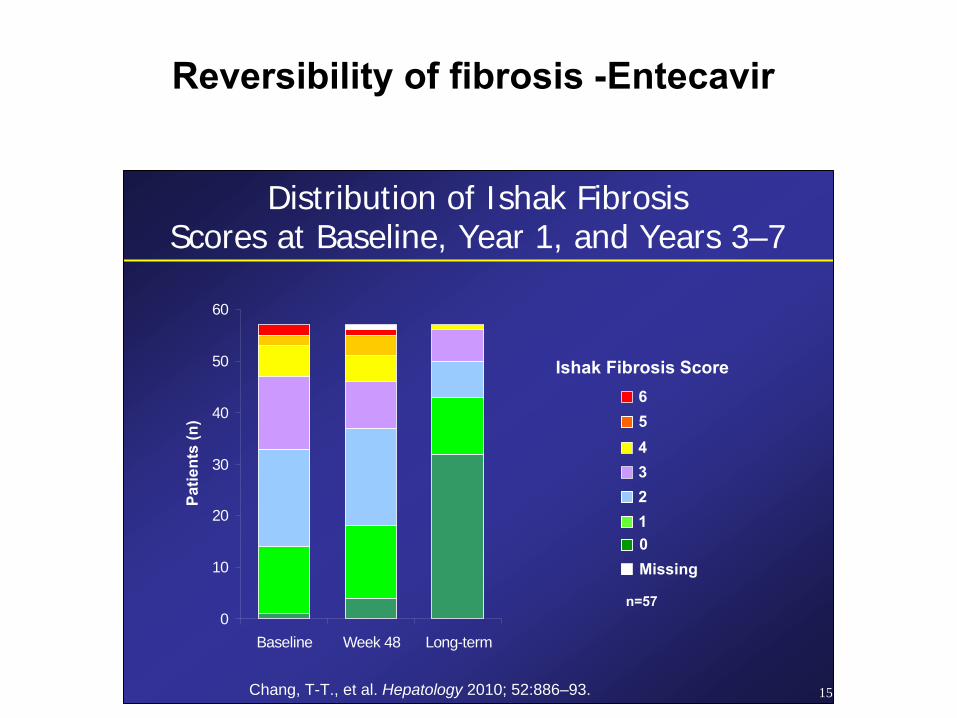
15
Ishak Fibrosis Score
1234
Distribution of Ishak FibrosisScores at Baseline, Year 1, and Years 3–7
56
Missing0
n=570
10
20
30
40
50
60
Baseline Week 48 Long-term
Patie
nts
(n)
Reversibility of fibrosis -Entecavir
Chang, T-T., et al. Hepatology 2010; 52:886–93.

5 yrs of tenofovir therapy: Sufficient HBV DNA suppression and significant regression of fibrosis
P. Marcellin, AASLD November 2011, San Francisco
But: HCC risk remains despite regression
of fibrosis – HBV patients need no be
included into long-term HCC surveillance
programs

Mathematic modeling of treatment duration with potent NUCs to reach HBsAg loss
Chevaliez/Pawlotsky: > 30 years
Zoutendiik, Janssen: median 36 years
Posters 374 und 381, AASLD 2010
Chang, T-T., et al. Hepatology 2010; 52:886–93.

HBsAg quantification: substantial decreases in patients with clinically resolving acute hepatitis B
HBsAg change after 4 weeks
Clinically Cured (n) Persistent (n)
Decrease > 60% 337 2
Constant or < 60% 2 13
Increase 1 15
W Gerlich et al, Verh Dtsch Ges Inn Med 1977

qHBsAg changes during NUC therapy in patients with cHBV and undetectable HBV-DNA
HBsAg
HBV DNA
95 patients during NUC therapy, 67% HBeAg negative(HBV-DNA <100 IU/ml)
6,3% HBsAg loss after 6-107 months
Markova et al., AASLD 2011, Abstract 30

Why is finite therapy with PEG-IFN a goal for treatment?
Younger patients may find lifelong treatment
hard to accept
Women who want to become pregnant
Patients reluctant to start life long treatment
Working days lost to hospital visits
Cost savings to healthcare system
Long-term adherence issues
Side effects in (real) long-
term therapy

HBeAg negative CHB: PEG‐IFN Therapy Stopping Rule at Week 12
Any HBsAg decline
HBV DNA decline(cp/mL)
102*
patients
NO
N=54YES
N=48
<2 log
N=20≥2 log
N=34<2 log
N=20≥2 log
N=28
*Serum at week 12 was not available in 5/107 patients
Chance of
Response 0% 39%
Rijckborst et al. Hepatology 2010 & J Hep 2012
Validated in 2 separate, large studies (J Hepatol 2012)

Practical application of response-guided therapy using HBsAg levels
Week 12:
‐
HBeAg‐positive
No decline in HBsAg or HBsAg >20,000 IU/mL
‐
HBeAg‐negative
No decline in HBsAg + <2log decline HBV DNA
Identify non‐responders (NPV)Identify non‐responders (NPV)
e‐
e+
EASL CPG HBV 2012, J Hepatology 2012

Can we stop NUCs before HBsAg loss?
Petersen et al., AASLD 2011, Abstract 14175 German centers (Hamburg, Kiel, Düsseldorf, Leipzig, Hannover)
9 out of 33 patients without relapse (28%)
Patient Previous therapy
Duration of therapy(months)
qHBsAg at stopping point (IU/ml)
Last HBsAg level available (IU/ml) after stopping therapy
1 Lamivudine 74 930 726
2 Lamivudine 62 140 HBsAg seroconversion
3 Lamivudine 80 453 479
4 Adefovir 64 18 HBsAg loss (<0.05)
5 Adefovir 52 49 not available
6 Telbivudine 54 not available HBsAg loss (<0.05)
7 Entecavir 0.5 37 not available 357
8 Entecavir 0.5 42 432 280
9 Entecavir 1.0 48 121 HBsAg seroconversion
Hadzyannis et al – AASLD 2006 and Gastroenterology 2012
50% of HBeAg negative patients after 5 yrs of Adefovir treatment
with continuous HBV-DNA suppression during treatment remained
without relapse

Protection against HBV reactivation
All immunsuppressive therapies will raise the possibility for HBV to reactivate:
- Chemotherapies
- CD 20 antibodies (rituximab et al)
- TNF alpha antibodies (not only excluding tb)
- Chemoembolisation and HCC: Lamivudin is effective preemptively
- Steroids alone: not suficient data
Before starting immunsuppressive therapies: test for
HBsAg und anti HBc

Vertical transmission of HBV despite active and passive immunisation of newborns
• n=1068 children of HBeAg positive mothers
• 3% transmission with HBV DNA >106 cop/ml• 5,5 % transmission with HBV DNA >107 cop/ml• 9,6% transmission with HBV DNA >108 cop/ml
Han et al., J Hepatology 2011, Petersen J Hepatology 2011
Considering antiviral therapy starting 2./3. trimester with >200.000 IU/ml (106 cop/ml) HBV-DNA

Combination therapy only for a very few
patients that do show advanced liver
disease and that have failed mono
therapy mostly due to resistance to first
line NUCsPetersen et al J Hepatology 2012

?
Multiple drug
resistant mutants
with complex pattern
of mutations+ one mutation + one mutation
Drug A Drug B
Risk of selection of MDR mutants by sequential therapy‐ drugs sharing cross‐resistance characteristics‐ incomplete viral suppression‐ liver transplantation
The problem of sequential therapy with nucleoside analogues
Zoulim F, et al. J Hepatol.
2008;48:S2‐19.
Yim et al, Hepatology 2006; Villet et al Gastroenterology 2006 &
2009

6
3
LVD ADV LdT ETV TDF
0
10
20
30
40
50
60
70
80
23
Prop
ortio
n of patients (%
)
46
55
71
80
0
11
18
29
5
25
0.2 0.51.2
0
1 2 3 4 5 1 2 3 4 5 1 2 1 2 3 4 5 1 2 3
0 0
Option to add
emtricitabine at
week 72*
*Patients confirmed to be viraemic at Week 72 or beyond could add emtricitabine to TDF at the discretion of the investigator.
Clinical data on the safety and efficacy of emtricitabine and TDF in CHB are pending
Barrier to resistance in NA‐naïve patients
4
0
High barrier to resistance
Gish, Jia, Locarnini & Zoulim, Lancet ID 2012
5
Prevention of ant
iviral drug resista
nce
> Antivirals with a
high barrier to re
sistance
> Achieve viral su
ppression
Antiviral drug res
istance became a manageab
le issue
Special attention
to patients with p
revious treatment
exposure and inco
mplete viral suppres
sion
Prevention of ant
iviral drug resista
nce
> Antivirals with a
high barrier to re
sistance
> Achieve viral su
ppression
Antiviral drug res
istance became a manageab
le issue
Special attention
to patients with p
revious treatment
exposure and inco
mplete viral suppres
sion

Is combination therapy bringing us closer to eradication of HBV ?
Role of cccDNA ?
Is combo better for higher rates of HBsAg loss?
Is switching possible too?

Once HBV ‐
always HBV ?!
mod. from S Urban, J Petersen; J Hepatol 2010
Is there a chance to eliminate or silence
cccDNA – dividing hepatocytes and cccDNA
stability
Is there a chance to eliminate or silence
cccDNA – dividing hepatocytes and cccDNA
stability

2‐3 week‐olduPA+/+/SCID
Generation of uPA/SCID mice harboring “humanized livers”
1 week
Ki67/Ki67/
CK18CK18
Human hepatocytesIsolation & cryo‐preservation
Hu‐CK18
48 weeks
Hepatology 2001; Nature Biotech. 2008; Gastroenterol. 2011, J. Hepatology 2011; Hepatology 2012
Hu‐CK18
4 weeks

Determination of intrahepatic cccDNA loads in proliferating hepatocytes in a mouse model (uPA/SCID mice)
2.5 cccDNA copies /PH before TxcccDNA copies after TX
Days after transplantation
0.01
10
0.1
1
0 10 20 40 80
Log cccD
NA cop
ies /PH
cccDNA decline per infected cell Intrahepatic cccDNA dilutionor loss?
Log cccD
NA / m
ouse liver
4
5
6
7
0 10 20 30 40 50 60 70 80
Days after transplantation
Lutgehetmann, Petersen, Dandri, Hepatology 2010
In vivo proliferat
ion of infected h
epatocytes induc
ed
continuous reduc
tion of cccDNA a
nd significant
cccDNA loss in in
fected livers in th
e absence of
antiviral drugs
In vivo proliferat
ion of infected h
epatocytes induc
ed
continuous reduc
tion of cccDNA a
nd significant
cccDNA loss in in
fected livers in th
e absence of
antiviral drugs
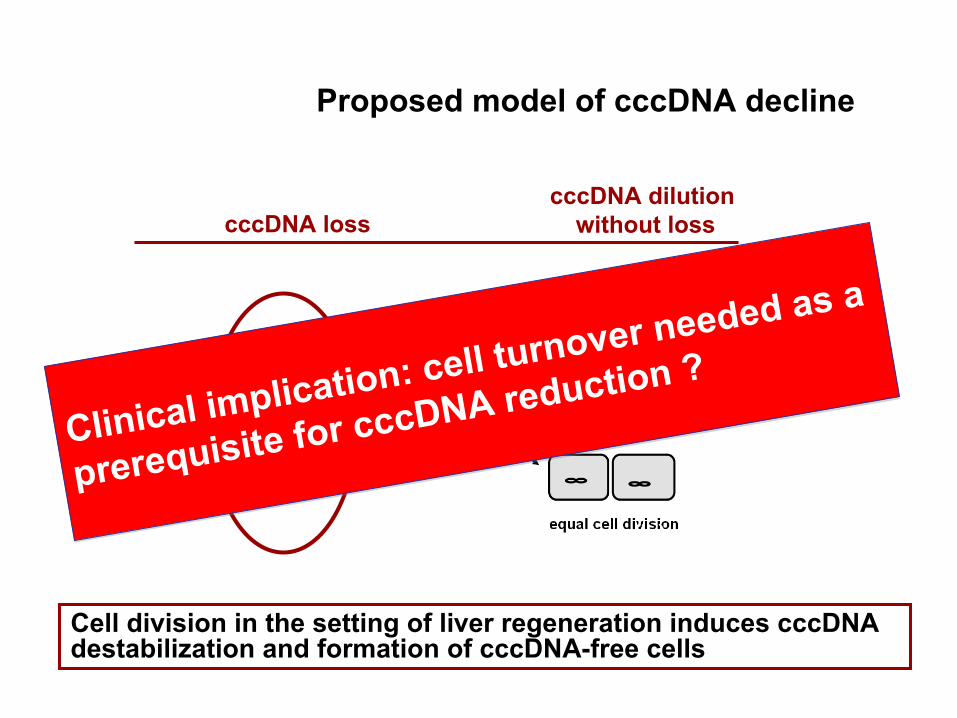
Proposed model of cccDNA decline
cccDNA dilution without losscccDNA loss
Cell division in the setting of liver regeneration induces cccDNA destabilization and formation of cccDNA-free cells
Clinical implication: cell turnover needed as a
prerequisite for cccDNA reduction ?Clinical implication: cell turnover needed as a
prerequisite for cccDNA reduction ?

Triplet liver biopsies were obtained from 16 patients
Study design: Monocenter open label, HBeAg+ and HBeAg-
patients
Biopsy # 3(n=16)
Baseline Week 48 Week 144Week 96
Biopsy #2(n=23)
Biopsy #1 (n=26)
n=24 n=24 n=21n=26
PEG IFN α2b
ADVScreening
Wursthorn, Petersen Hepatology 2006Lütgehetmann, Petersen Antiviral Therapy 2008

Combination therapy with PEG-IFN
+ ADV induced strong intrahepatic HBV DNA reduction
• Reduction achieved after 1 yr IFN + ADVwas maintained in the following 2 yr of ADV monotherapy
• No further cccDNA decrease with ADV only
Lütgehetmann Antiviral Therapy 2008
Why?
PEG IFNα2b
ADV
p= 0,001
ALT (ULN)IFN

Inhibition of intrahepatic viral productivity by different antiviral regimens
Baseline (n=24)
1100
0
100
200
(503)
(735)
(861)
(1088)
300
W48(n=19)
W144(n=16)
-99%
-76%
p=0,001p=0,001
rcDNA/cccDNA
How about the more potent NUCsETV and TDF ?
Silencing of cccDNA?
Regulation of cccDNAtranscriptional activity?
PEG IFN α2bADV
ADV
Lütgehetmann Antiviral Therapy 2008

Histone acetylation/methylation affects the regulation of gene expression
Pollicino et al. Gastroenteroplogy 2006; Levrero et al. J Hepatol, 2009; Belloni, PNAS 2009
IFN
treatment
is
accompanied
by
a
decrease
in
the
acetylation
of
cccDNA
bound H4 histones in vitro
Transcription of the HBV cccDNA minichromosome can be regulated epigenetically
PCAF PCAFCBPp300
p300 CBP
Sirt1Ezh2YY1HDAC1
acetylated histonesdeacetylated histones
+ IFN
Levrero, Dandri, Raimondo, Petersen J Hepatol 2009; Belloni, Levrero, Petersen, Dandri, Raimondo J Clin Inv 2012
Beginning of understanding that cccDNA is
controlled epigenetically – silencing possible?
Beginning of understanding that cccDNA is
controlled epigenetically – silencing possible?
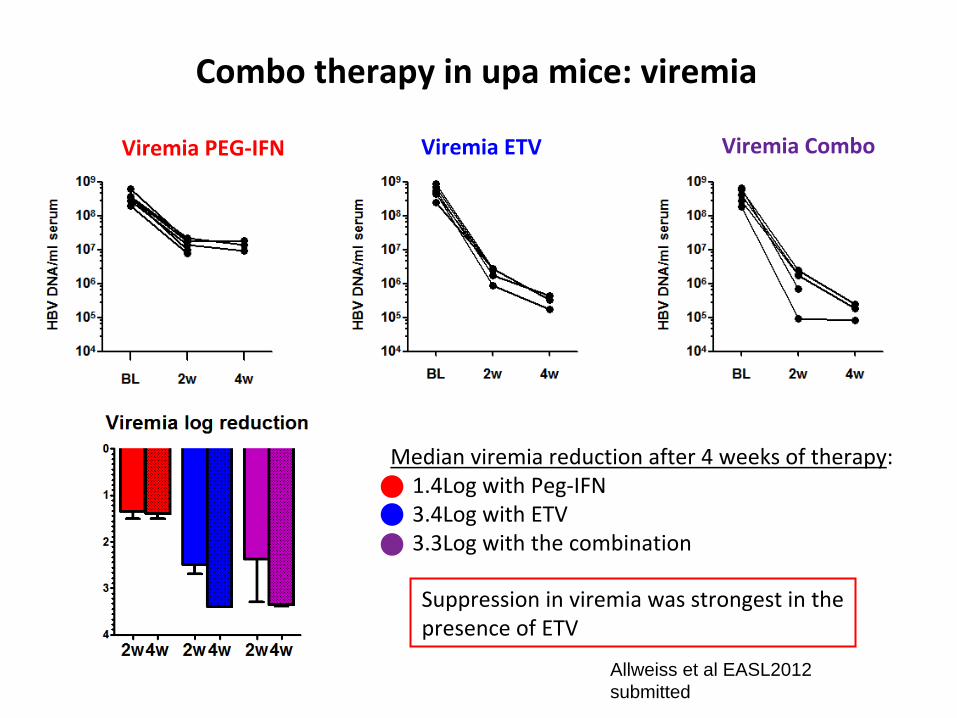
Combo therapy in upa mice: viremia
Viremia PEG‐IFN Viremia ETV Viremia Combo
Median viremia reduction after 4 weeks of therapy: 1.4Log with Peg‐IFN 3.4Log with ETV 3.3Log with the combination
Suppression in viremia was strongest in the
presence of ETV
Allweiss et al EASL2012submitted

Serological parameters: HBsAg changes
Median HBsAg reduction after 4 weeks of therapy: 0.21Log with Peg‐IFN 0.13Log with ETV 0.5Log with combination
Suppression of HBsAg was strongest in the presence of Peg‐IFN‐
Allweiss et al EASL2012submitted

Peg‐IFN Add‐On Strategy leads to more HBsAg reduction
HBeAg-positive (n=4)
HBeAg-negative (n=12)
Time, months
HB
sAg,
IU/m
L 6000
5000
4000
3000
2000
1000
0 Baseline 6 1 2 3 4 5
4802
841 1115 927 740 634
509
5588
2708
Extrapolated data
Lampertico P, et al. EASL 2012; Abstract 523
• Seroconversion to anti-HBe in 2 patients (months 4 and 7)• All patients remained HBV DNA negative• 8 (50%) patients discontinued PEG-IFN, including
5 (31%) for unchanged HBsAg levels at 24-week, and 3 for IFN-related side effects
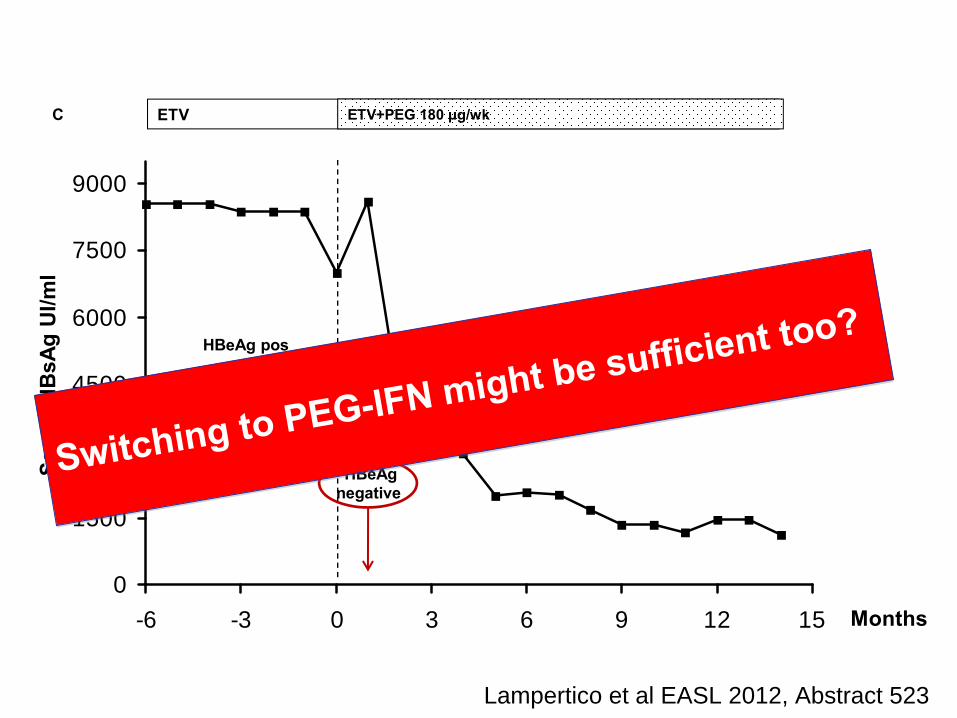
0
1500
3000
4500
6000
7500
9000
-6 -3 0 3 6 9 12 15
Seru
m H
BsA
gU
I/ml
Months
ETV ETV+PEG 180 μg/wk
HBeAgnegative
HBeAg pos
genotype D
chronic hepatitis
IL28B TT
C
Lampertico et al EASL 2012, Abstract 523
Switching to PEG-IFN might be sufficient too?
Switching to PEG-IFN might be sufficient too?
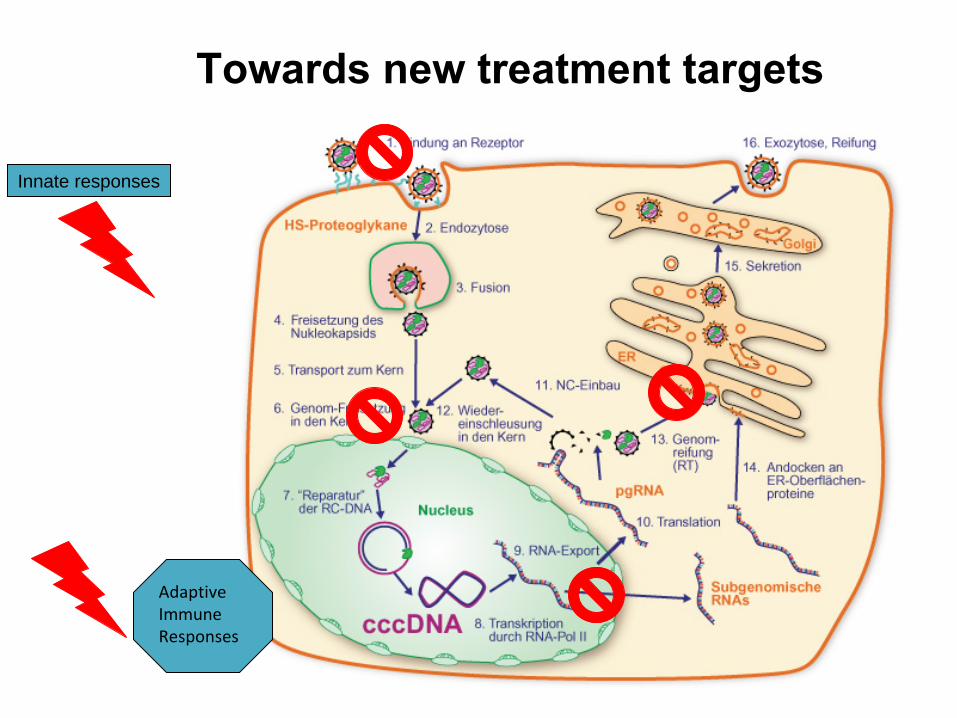
Towards new treatment targets
Innate responses
Adaptive
Immune
Responses
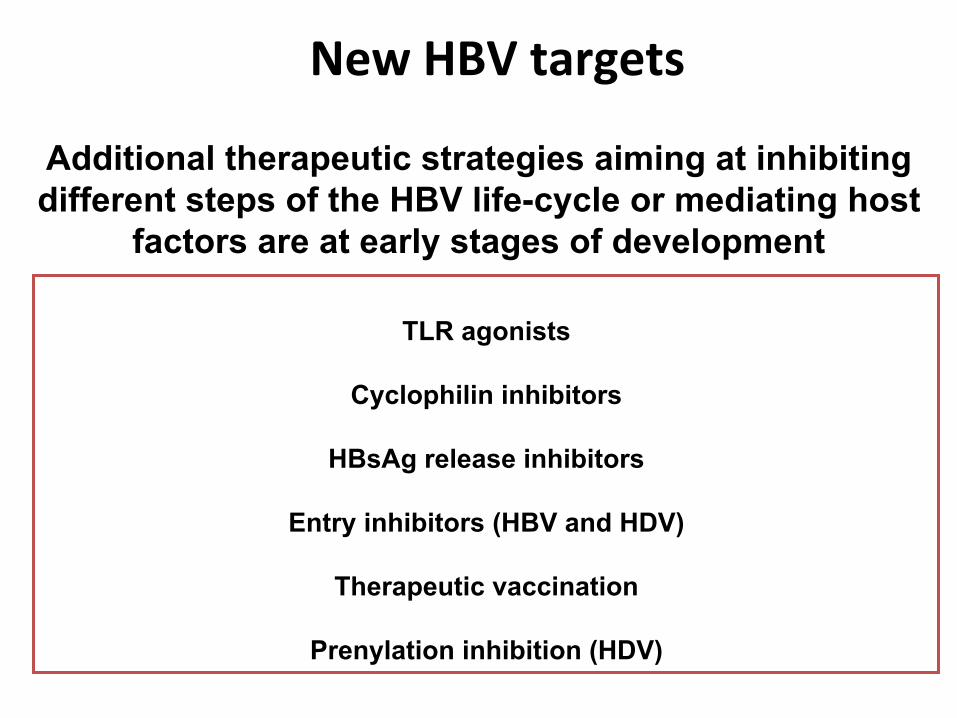
New HBV targets
TLR agonists
Cyclophilin inhibitors
HBsAg release inhibitors
Entry inhibitors (HBV and HDV)
Therapeutic vaccination
Prenylation inhibition (HDV)
Additional therapeutic strategies aiming at inhibiting different steps of the HBV life-cycle or mediating host
factors are at early stages of development

Acylated HBV preS1‐derived peptides block HBV infection in vitro
– entry inhibitor
cccDNA
AAAAAA
Myrcludex B
Chemically synthesized lipopeptides derived
from the envelope of HBV block virus
infection in cell culture (HepaRG & PTH, PHH)

HBcAg
HBcAg
huCyt‐18
huCyt‐18
16 weeks after HBV infection
Petersen, Dandri et al. Nature Biotech. 2008
Administration of Myrcludex B prevents the establishment of de novo HBV infection in vivo; Phase I studies completed
3 6 9
Liver histology
‐1h 3d2d1d 5d
Subcoutanous peptide
application
12 15
Blood samples after infection
weeks
Inoculation

Abstracts # 455/440
Title
GS‐9620 INDUCES A PRESYSTEMIC
INNATE IMMUNE RESPONSE IN THE
ABSENCE OF SERUM INTERFERON OR
ADVERSE EFFECTS IN BOTH NON‐
CLINICAL SPECIES AND HUMANS
Speaker: Abigail Fosdick
Author: D. Tumas1, A. Fosdick1*, X. Zheng1, R.
Lanford2, J. Hesselgesser1, C. Frey1, W.
Grushenka1, R. Halcomb1, U. Lopatin1
Affiliation:
1Gilead Sciences Inc., Foster City, CA, 2Department of Virology and Immunology,
Texas Biomedical Research Institute, San
Antonio, TX, USA.

• GS 9620: Toll like receptor 7 agonist as oral immunmodulating substance
• Inducing antiviral Type 1 IFN Response (GALT-gut associated lymphoid tissue) without systemic IFN effect
• Phase I study in the US, Canada, Australia recruiting (finished mid 2013)

Mono therapy either with potent NUCs or PEG IFN is the therapy of choice for the great majority of chronically infected HBV patients in 2012
Fibrosis seems to be reversible
With adherent patients, resistance seems to be a minor and manageable problem using Entecavir or Tenofovir
The combo of ETV + TDF is only required in a very few clinical situations such as drug resistance (sequential therapy) and advanced liver disease
Combination therapy with NUCs and PEG IFN have shown to greaterreduce the amount of cccDNA and HBsAg
There might be room for combo therapies in the future for a higher chance of clinical cure (HBsAg loss) – immunological characterisation of patients responses urgently needed
New therapeutics are still only at very early stages of clinical development
Conclusions

UKE Hamburg:
M. Dandri
M. LütgehetmannT. Volz
M. Ben M’BarekT.BornscheuerL. AllweissL. ManckeT. Hellbig
A.W. LohseJ. M. Pollok
R. ReuschG. Apitzsch
Acknowledgments
Collaborations:
P. Lampertico, MilanS. Locarnini, Australia
H. Wedemeyer, HannoverS. Urban, Heidelberg
F. Zoulim, LyonM. Levrero, RomeM. Buti, Barcelona
H. Janssen, RotterdamT. Pollicino, Mesina

Thank you for your attention
Jorg PetersenLiver UnitIFI Institute for Interdisciplinary Medicine Asklepios Klinik St. Georg University of Hamburg
email: [email protected]