hepatitis c
TRANSCRIPT
HEPATITIS CRajalekshmy.P.R
Dept of SwasthavrittaAmrita Schoolof Ayurveda

Clinical case…… A 45-year-old woman with a history of blood transfusion is seen in
the clinic for complaints of tiredness, fatigue, anorexia, and weakness. On Physical examination, nothing was remarkable. Laboratory values reported today include AST 150 IU/mL, ALT 250
IU/mL , SCr 0.9 mg/dL, Bilirubin: 2.0 mg/dL, albumin 2.5 g/dL. Serum Anti HCV : + HCV RNA level: 1, 220200 IU/mL A liver biopsy has revealed severe inflammation and fibrosis. What is the diagnosis ? What is the best course of action?

HEPATITIS C

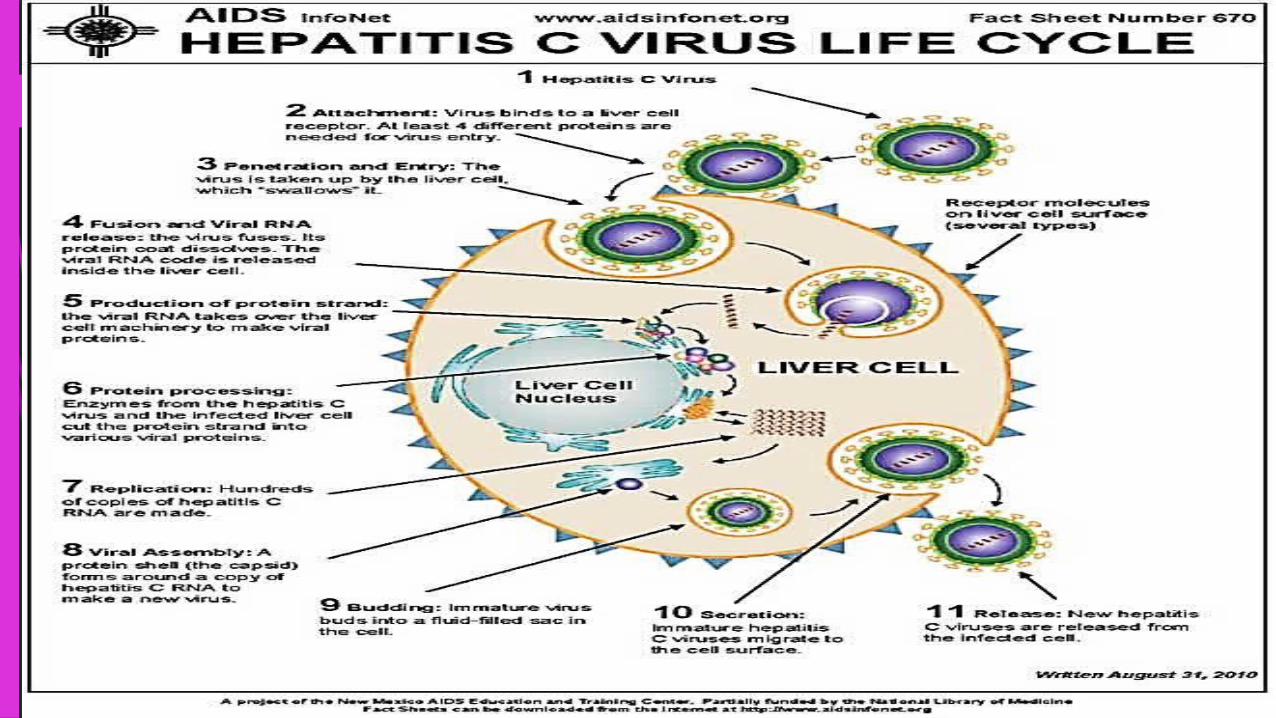
INTRODUCTION Hepatitis C is a contagious liver disease that results from
infection with HCV. It can range in severity from mild illness lasting a few
weeks to serious life long illness. Spread through transfusion of blood and blood products Transmitted sexually and perinatally also. No vaccine available to prevent hepatitis C.
HISTORY Identified in 1989. Blood test became available in 1992. Used to be known as “non-A, non-B” hepatitis (NANB) Also named as perinatally transmitted NA-NB Hepatitis
(PT-NANB).

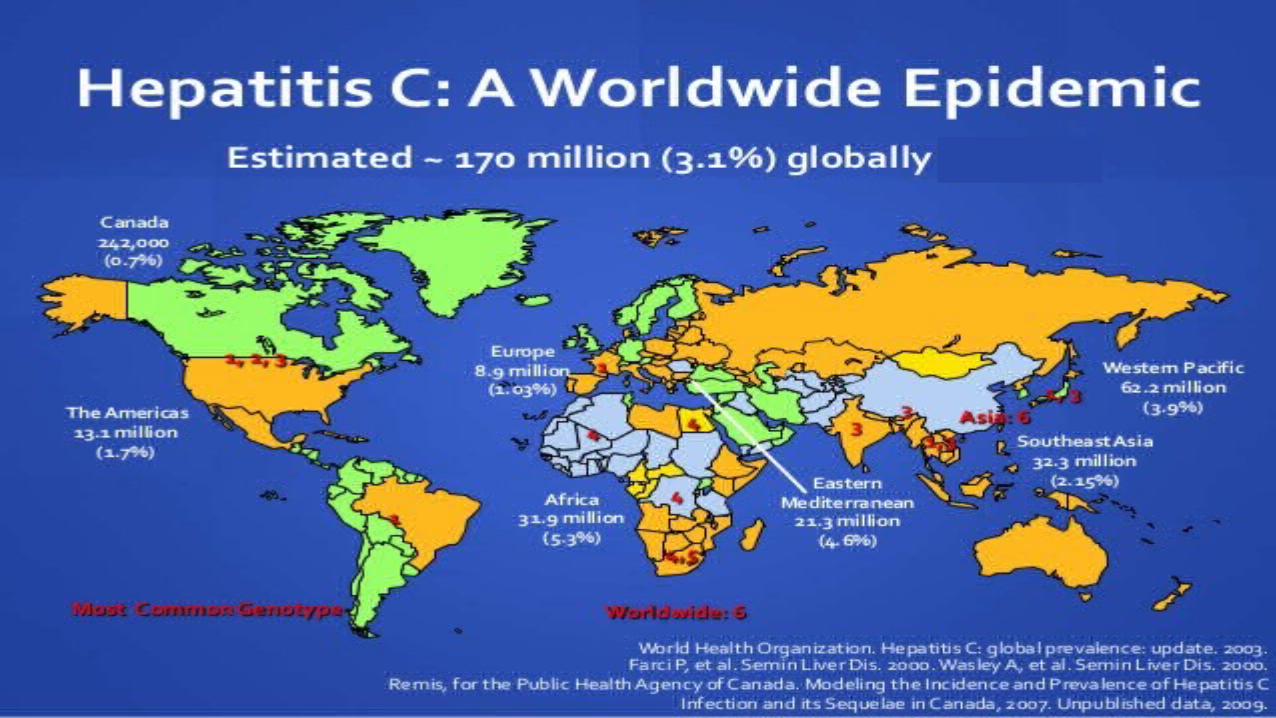
EPIDEMOLOGY Globally, an estimated 130–170 million persons (2%–3% of the
world's population) are living with hepatitis C virus (HCV) infection.
150 million are chronically infected and at risk of developing liver cirrhosis and liver cancer.
More than 350000 people die from hepatitis C related liver diseases every year.
The epidemiology and burden of HCV infection varies throughout the world, with country-specific prevalence ranging from <1% to >10%.

Developed countries
Transmission primarily through injection drug use
Australia and Western Europe - <2%Eastern Europe, Latin America, Africa, Middle East, South Asia, countries of
former Soviet Union - >3%Egypt with highest prevalence - >10%
Developing countries
Unsafe injections in health care settings resulting in 2 million new HCV infection
each year.China has highest estimated number of
HCV infected IDU in the world.In Mexico. Pakistan and Thailand, >80% of
IDU are anti-HCV positive.


EGYPT
• The reuse of syringes during a schistosomiasis eradication program in the 1960s and 1970s is the purported cause of the widespread introduction and spread of
HCV in that country.
• However, Egypt is experiencing continued HCV transmission associated with unsafe
injection practices, poor infection control in hospitals, and widespread use of unscreened
blood for transfusion.
• Up to 500 000 new infections are estimated to occur annually.
PAKISTAN
• Ongoing transmission in Pakistan, where HCV
infection is highly endemic, also is associated
with unsafe injections.
• At a mean of 13 injections per person annually,
Pakistan has the highest documented rate of
injections in the world.


HEPATITIS C VIRUS Family – Flaviviridae Genus – Hepacivirus 55-65 nm, enveloped positive sense single stranded RNA genome. 7 genotypes with several subtypes. Subtypes 1a and 1b are found world wide and cause 60% of all cases. Half life of the virus particles in the serum is around 3 hours and may
be as short as 45 minutes. In an infected person, about 1012 virus particles are produced each
day. Replication in hepatocytes and lymphocytes.

The hepatitis C virus is gradually inactivated outside the body of a host.
The presence of heat can greatly reduce the virus's lifespan outside the body.
The virus can remain infectious outside a host for about sixteen days at 25 °C and two days at 37 °C.
It can remain active for more than six weeks at temperatures less than or equal to 4 °C.
When heated to temperatures of 60 °C and 65 °C, the hepatitis C virus can be inactivated in eight and four minutes.

STRUCTURE
• Core genetic material(RNA)
• Surrounded by protective shell of protein
• Encased in a lipid envelope of cellular origin
• 2 viral envelope glycoproteins E1 and E2 embedded in lipid envelope.
TRANSMISSIONExposure to infectious blood
• Receipt of contaminated blood transfusions, blood products and
organ transplants.• Injection given with contaminated
syringes and needle site injuries in health care settings.• Injection drug use
• Being born to hepatitis C infected mother


Dr.T.V.Rao MD
19
Before 1985 1999
Illegal Drug UseTransfusion
SexualOther
Unknown

20
Sexual 15%
Other* 5%Unknown 10%
Injecting drug use 60%
Transfusion 10%(before screening)
*Nosocomial; Health-care work; Perinatal
Source: Centers for Disease Control and Prevention

INCUBATION PERIOD
2 weeks to 6 months

PATHOLOGYVirus causes inflammation of Liver
Microscopically spotted parenchymal cell degeneration
Necrosis of Hepatocytes
Causes diffuse lobular inflammatory reaction
Disruption of liver cell cords
Accumulation of Macrophages near degenerating Hepatocytes.


ACUTE MANIFESTATIONS Fever Fatigue Decreased appetite Nausea Vomiting Abdominal pain Dark coloured urine Grey coloured faeces Joint pain Jaundice

Hepatitis C virusAcute infection
Recovery and clearance (15%) Persistent infection (85%)
Chronic hepatitis
Liver failure (6%) Cirrhosis (20%) Hepatocellular carcinoma (4%)

PROGRESS OF EVENTS IN HCV INFECTION

EXTRA HEPATIC MANIFESTATIONS
Arthralgia is a common symptom of hepatitis C that is characterized as joint pain.
Hepatitis C-related arthritis (HCVrA) is estimated to affect about 4% of the HCV population.
Cerebral Vasculitis is a disorder that is characterized by inflammation and cell death of arteries in the brain.
The cause of cerebral vasculitis is unknown, but it is thought to be caused by immune dysfunction.

Insulin Resistance (IR) is a condition caused by the inability of cells to absorb glucose. HCV can induce IR.
Cryoglobulinemia is a blood disorder caused by abnormal proteins in the blood called cryoglobulins that precipitate or clump together when blood is chilled and then dissolve when warmed.
These proteins can be deposited in the small and medium sized blood vessels, which restricts blood flow and can lead to further problems.

OCCULT INFECTION Persons who have been infected with hepatitis C may appear to clear the
virus but remain infected. The virus is not detectable with conventional testing but can be found with
ultra-sensitive tests. The original method of detection was by demonstrating the
viral genome within liver biopsies, but newer methods include an antibody test for the virus core protein and the detection of the viral genome after first concentrating the viral particles by ultracentrifugation.


DIAGNOSIS Presence of antibodies against HCV indicates that a person
is or has been infected. Diagnosis of chronic infection is made when antibodies to
HCV are present in the blood for more than 6 months. HCV Recombinant Immunoblot Assay(RIBA) and HCV
RNA testing confirms the diagnosis. Early diagnosis can prevent health problems that may
result from infection and prevent transmission to family members and close contacts.

Molecular methods in Diagnosis of hepatitis c infection
Qualitative reverse transcription- polymerase chain reaction (RT-PCR) assays for HCV RNA are simpler than quantitative tests and sufficient for confirmation of the diagnosis of HCV infection.

ALANINE AMINOTRANSFERASE
Serum ALT testing is inexpensive and noninvasive. Insensitive means of monitoring disease activity. A single determination gives limited information, and serial
measurements recommended. Resolution of ALT elevation with antiviral therapy appears to
indicate disease response.

Dr.T.V.Rao MD
34Serologic Pattern of Acute HCV Infection
with Recovery
Symptoms +/-
Time after Exposure
Tite
r
anti-HCV
ALT
Normal0 1 2 3 4 5 6 1 2 3 4
YearsMonths
HCV RNA

Dr.T.V.Rao MD
35Serologic Pattern of Acute HCV Infection
with Progression to Chronic Infection
Symptoms +/-
Time after Exposure
Tite
r
anti-HCV
ALT
Normal0 1 2 3 4 5 6 1 2 3 4
YearsMonths
HCV RNA

Who should be screened?
People who receive blood, blood products or organs Current or former injecting drug users People on long term haemodialysis Health care workers People living with HIV People with abnormal liver tests or liver disease Infants born to infected mothers

TREATMENT
Does not always require treatment. Combination antiviral therapy with interferon and ribavirin has been
the mainstay of HC Rx. Scientific advances have led to the development of new antiviral
drugs. 2 new therapeutic agents telaprevir and boceprevir have recently
been licensed in some countries.

Can we prevent hepatitis c infection
There is no vaccine for Hepatitis C.
The best way to prevent Hepatitis C is by avoiding behaviors that can spread the disease, especially injection drug use.

PREVENTION
Primary prevention
Risk of infection can be reduced by avoiding- Unnecessary and unsafe injections Unsafe blood products Unsafe sharp waste collection and disposal Use of illicit drugs and sharing of injection equipment Unprotected sex with HCV infected people. Sharing sharp personal items contaminated with infected blood Tattoos, piercing and acupuncture performed with contaminated
equipment
Secondary & tertiary prevention
• Education and counselling• Immunization with HA and HB vaccines to prevent
co-infection from these viruses to protect their liver.• Early and appropriate medical management including
antiviral therapy• Regular monitoring for early diagnosis of chronic
liver disease.