hepatitis c and corrections megan mahoney, md correctional medicine consultation network department...
TRANSCRIPT
Hepatitis C and Hepatitis C and CorrectionsCorrections
Megan Mahoney, MDCorrectional Medicine Consultation NetworkCorrectional Medicine Consultation NetworkDepartment of Family and Community MedicineUniversity of California, San Francisco

Image Courtesy of Ray Chavez and CA Prison Health Care Receivership

Objectives
Incarceration in the U.S. and California
Hepatitis C Epidemic among Incarcerated
Challenges to Hepatitis C Treatment in CDCR
Future Directions

Image Courtesy of Ray Chavez and CA Prison Health Care Receivership

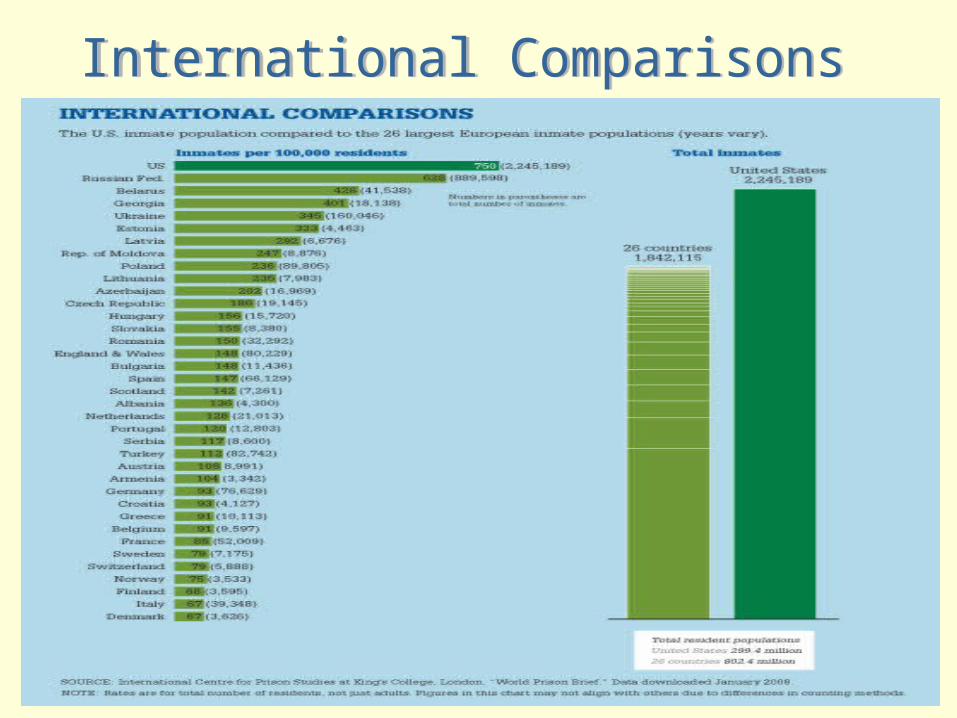
Incarceration in the U.S.
2.3 million people in prisons and jails1
Highest per capita incarceration rate in the world 750/100k2
More than one in every 100 adults is now incarcerated3
1 in 37 adults have been incarcerated4
1-3. Bureau of Justice Statistics 2003: www.ojp.usdoj.gov/bjs
4. Pew Report 2008: www.ncjrs.gov/App/Publications/abstract.aspx?ID=243732
Lifetime chance of incarceration
Black males 1 in 3
Latino males 1 in 6
White males 1 in 17
Incarceration in the U.S.
Image Courtesy of Ray Chavez and CA Prison Health Care Receivership Bureau of Justice Statistics 2003: www.ojp.usdoj.gov/bjs
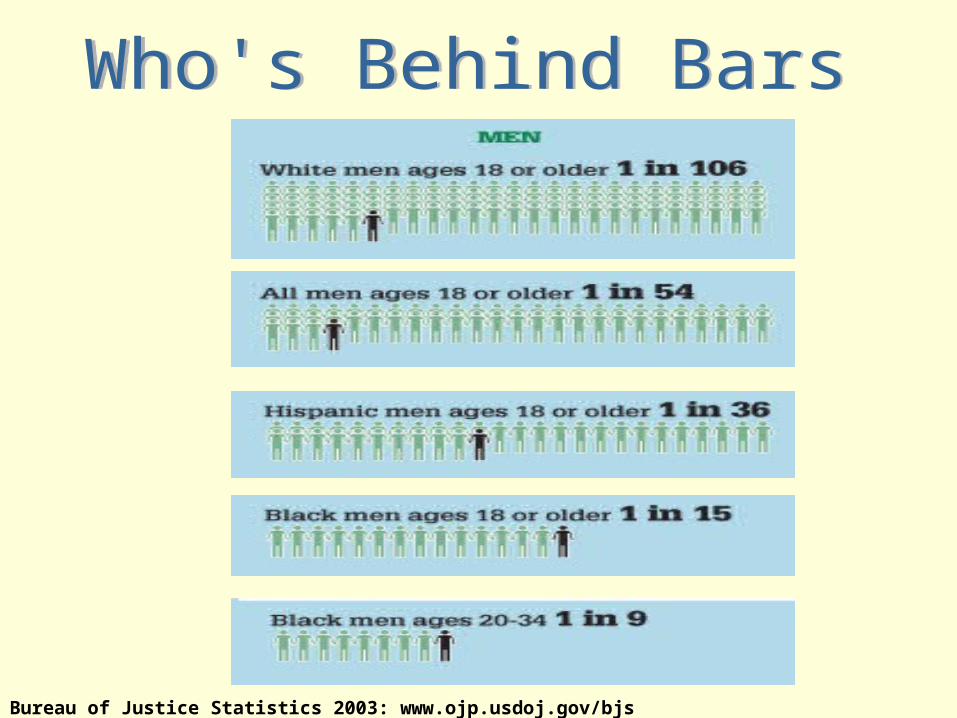
Bureau of Justice Statistics 2003: www.ojp.usdoj.gov/bjs

Bureau of Justice Statistics 2003: www.ojp.usdoj.gov/bjs

Incarceration in California
173,000 current; 302,000 total per year
Commitment rate: 456/100,000
32,400 life sentence, 660 condemned
Offenses: 50% persons, 21% drugs, 21% property
Avg. sentence: 4.5 years, 2 years served
Reading level: 7th gradeCDCR 2007: www.cdcr.ca.gov/Reports_Research/Offender_Information_Services_Branch/Projections/F07pub.pdf

Demographics of Incarceration in California
93 % male, 7% female 29 % African American
7 % of general population 37 % Latino
36 % of general population 29 % white
77 % of general population Average age= 36
CDCR 2007: www.cdcr.ca.gov/Reports_Research/Offender_Information_Services_Branch/Projections/F07pub.pdf

Incarceration In The US
1974-2001: number incarcerated for the first time tripled
Bureau of Justice Statistics 2003: www.ojp.usdoj.gov/bjs

1880
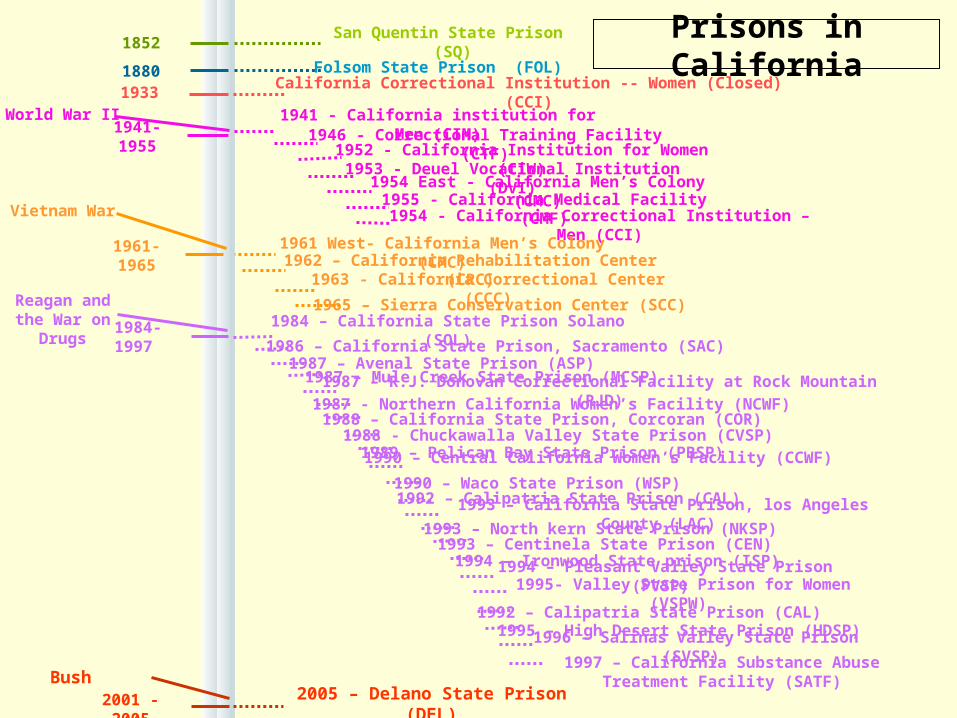
1852 Prisons in CaliforniaSan Quentin State Prison (SQ)
Folsom State Prison (FOL)

18801933
1852 Prisons in CaliforniaSan Quentin State Prison (SQ)
Folsom State Prison (FOL)
California Correctional Institution -- Women (Closed) (CCI)

18801933
1852 Prisons in California
1941-1955World War II
San Quentin State Prison (SQ)
Folsom State Prison (FOL)
California Correctional Institution -- Women (Closed) (CCI)
1941 - California institution for Men (CIM)1946 - Correctional Training Facility (CTF)
1953 - Deuel Vocational Institution (DVI)1952 - California Institution for Women (CIW)
1955 - California Medical Facility (CMF)
1954 East - California Men’s Colony (CMC)
1954 - California Correctional Institution – Men (CCI)

1961-1965
18801933
1852 Prisons in California
1941-1955World War II
Vietnam War
San Quentin State Prison (SQ)
Folsom State Prison (FOL)
1941 - California institution for Men (CIM)1946 - Correctional Training Facility (CTF)
1953 - Deuel Vocational Institution (DVI)1952 - California Institution for Women (CIW)
1955 - California Medical Facility (CMF)1954 East - California Men’s Colony (CMC)
1961 West- California Men’s Colony (CMC)1962 – California Rehabilitation Center (CRC)
1963 - California Correctional Center (CCC)1965 – Sierra Conservation Center (SCC)
1954 - California Correctional Institution – Men (CCI)
California Correctional Institution -- Women (Closed) (CCI)

1961-1965
1984-1997
18801933
1852 Prisons in California
1941-1955World War II
Vietnam War
Reagan and the War on
Drugs
San Quentin State Prison (SQ)
Folsom State Prison (FOL)
California Correctional Institution -- Women (Closed) (CCI)
1954 - California Correctional Institution – Men (CCI)
1941 - California institution for Men (CIM)1946 - Correctional Training Facility (CTF)
1953 - Deuel Vocational Institution (DVI)1952 - California Institution for Women (CIW)
1955 - California Medical Facility (CMF)1954 East - California Men’s Colony (CMC)
1961 West- California Men’s Colony (CMC)1962 – California Rehabilitation Center (CRC)
1963 - California Correctional Center (CCC)1965 – Sierra Conservation Center (SCC)
1984 – California State Prison Solano (SOL)1986 – California State Prison, Sacramento (SAC)1987 – Avenal State Prison (ASP)
1987 – Mule Creek State Prison (MCSP)1987 – R.J. Donovan Correctional Facility at Rock Mountain (RJD)1987 - Northern California Women’s Facility (NCWF)
1988 – California State Prison, Corcoran (COR) 1988 - Chuckawalla Valley State Prison (CVSP)
1989 – Pelican Bay State Prison (PBSP) 1990 – Central California Women’s Facility (CCWF)
1990 – Waco State Prison (WSP) 1992 – Calipatria State Prison (CAL)
1993 – California State Prison, los Angeles County (LAC) 1993 – North kern State Prison (NKSP)
1993 – Centinela State Prison (CEN) 1994 – Ironwood State prison (ISP)
1994 – Pleasant Valley State Prison (PVSP) 1995- Valley State Prison for Women (VSPW) 1992 – Calipatria State Prison (CAL)
1995 – High Desert State Prison (HDSP)1996 – Salinas Valley State Prison (SVSP)
1997 – California Substance Abuse Treatment Facility (SATF)
1961-1965
1984-1997
2001 - 2005
18801933
1852 Prisons in California
1941-1955World War II
Vietnam War
Reagan and the War on
Drugs
San Quentin State Prison (SQ)
Folsom State Prison (FOL)
California Correctional Institution -- Women (Closed) (CCI)
1954 - California Correctional Institution – Men (CCI)
1941 - California institution for Men (CIM)1946 - Correctional Training Facility (CTF)
1953 - Deuel Vocational Institution (DVI)1952 - California Institution for Women (CIW)
1955 - California Medical Facility (CMF)1954 East - California Men’s Colony (CMC)
1961 West- California Men’s Colony (CMC)1962 – California Rehabilitation Center (CRC)
1963 - California Correctional Center (CCC)1965 – Sierra Conservation Center (SCC)
1984 – California State Prison Solano (SOL)1986 – California State Prison, Sacramento (SAC)1987 – Avenal State Prison (ASP)
1987 – Mule Creek State Prison (MCSP)1987 – R.J. Donovan Correctional Facility at Rock Mountain (RJD)1987 - Northern California Women’s Facility (NCWF)
1988 – California State Prison, Corcoran (COR) 1988 - Chuckawalla Valley State Prison (CVSP)
1989 – Pelican Bay State Prison (PBSP) 1990 – Central California Women’s Facility (CCWF)
1990 – Waco State Prison (WSP) 1992 – Calipatria State Prison (CAL)
1993 – California State Prison, los Angeles County (LAC) 1993 – North kern State Prison (NKSP)
1993 – Centinela State Prison (CEN) 1994 – Ironwood State prison (ISP)
1994 – Pleasant Valley State Prison (PVSP) 1995- Valley State Prison for Women (VSPW) 1992 – Calipatria State Prison (CAL)
1995 – High Desert State Prison (HDSP)1996 – Salinas Valley State Prison (SVSP)
1997 – California Substance Abuse Treatment Facility (SATF)Bush
2005 – Delano State Prison (DEL)

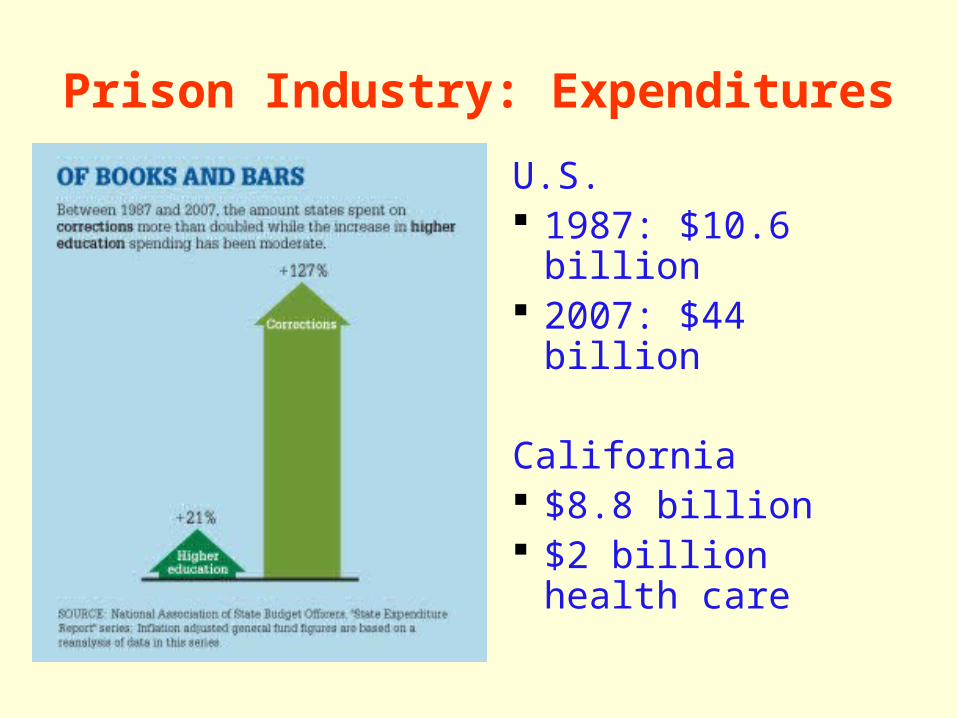
Prison Industry: Expenditures
U.S. 1987: $10.6 billion 2007: $44 billion
California $8.8 billion $2 billion health
care

Burden of Disease:Mental Illness
700,000 people with severe mental illness are admitted to U.S. jails and prisons each year
NYC and LA county jails are the largest inpatient psych units in the country
Mentally ill inmates report longer criminal histories than other inmates
Bureau of Justice Statistics 2003: www.ojp.usdoj.gov/bjs

Incarceration and Mental Illness: US
1970
1999
500,000State Psychiatric
Hospital Beds
1,2000,000
Prison & Jails
100,000Prison & Jails
100,000State Psych Beds
Bureau of Justice Statistics 2003: www.ojp.usdoj.gov/bjs

Summary Summary Pew Center Public Safety Pew Center Public Safety Performance Project 2007Performance Project 2007
States in the U.S. are spending more and more on inmates who are less and less a threat to public safety
Image Courtesy of Ray Chavez and CA Prison Health Care Receivership
Hepatitis C Epidemic in Corrections in U.S.
• HCV prevalence high in prisons- 15%-40%1 1.8% prevalence in general population
• Intravenous drug use leading risk factor
• Women incarcerated for IDU-related criminal offenses2
1Boutwell, Allen, Rich. Opportunities to Address the Hep C Epidemic in the Correctional Setting. Clinical Infectious Diseases. 2005;40:S367-72.
2Harrison PM, Karberg JC. Prison and jail inmates at midyear 2002. National Criminal Justice document 198877. Washington, DC: Bureau of Justice Statistics, 2003.

Substance Abuse
Newly sentenced state prisoners convicted of drug offenses
1985 13% 1990 32%
65-80% of prisoners with history substance use and abuse
Only 25-33% with history of treatment for substance abuse
Bureau of Justice Statistics 2003: www.ojp.usdoj.gov/bjs

High Risk Behaviors and Exposures
Unprotected sexual activity IV drug use Tattooing Violence Sexual Assault

Image Courtesy of Ray Chavez and CA Prison Health Care Receivership

Historical Challenges to HCV Treatment in Prisons in U.S.
1) Psychiatric Illness 2) ALT Level 3) HIV Co-infection 4) Lack of Funding 5) Access to Subspecialty Care 6) Transition Care 7) Duration of Stay

Recent Evidence• 1) Psychiatric Illness and Substance Use: Not
a barrier if remote or adequately treated1
• 2) ALT Level: Pts w/normal ALT may deteriorate histologically and respond to tx2
• 3) HIV: Coinfection common (1.4% prevalence). Pts respond to treatment3
1 Paris JE. Potential legal pitfalls of HCV management in corrections and how to avoid them.
Infectious Diseases in Corrections Report. September 2007. Spotlight Article. 2 Pearlman B, Paris JE. Hot Topics in Hepatitis C. HEPP Report on Infectious Diseases in Corrections. 2004;7(6):1-4.
3Cengiz C, Park JS, Sarah N et al. HIV and Liver diseases: Recent clinical advances. Clinics in Liver Disease. 2005;9:647-66.
Hepatitis C Treatment Guidelines 2008
• CDCR had similar to barriers seen nationwide
• California Department of Corrections and Rehabilitation revising guidelines based on new evidence
• HIV/Hepatitis Advisory Committee, chaired by Dr. Joseph Bick
• Previous restrictions due to Hx of Substance Use, Normal ALT, and Age reexamined

Historical Challenges to HCV Treatment in Prisons
1) Psychiatric Illness 2) HIV Co-infection 3) ALT Level 4) Lack of Funding 5) Access to Subspecialty Care 6) Transition Care 7) Duration of Stay

Image Courtesy of Ray Chavez and CA Prison Health Care Receivership
[The] principles [behind the guarantee against cruel and unusual punishment] establish the government’s obligation to provide medical care for those whom it is punishing by incarceration. An inmate must rely on prison authorities to treat his medical needs; if the authorities fail to do so, those needs will not be met.
US Supreme Court, Estelle v. Gamble (1976)
Prisoners are one of the only groups in this country with a constitutional right to
health care.
Image Courtesy of Ray Chavez and CA Prison Health Care Receivership

Plata v. Schwarzenegger
Largest ever prison class action lawsuit in the US
Prisoners alleged that California officials inflicted cruel and unusual punishment by being deliberately indifferent to serious medical needs.
Settlement agreement 2002:
Requires the California Department of Corrections and Rehabilitation to completely overhaul its medical care policies and procedures

California Prison Receivership
Second time in U.S. history that a federal receiver has presided over a correctional system
Receiver has access to resources and ability to override usual procedures

Historical Challenges to HCV Treatment in Prisons
1) Psychiatric Illness 2) HIV Co-infection 3) ALT Level 4) Lack of Funding 5) Access to Subspecialty Care 6) Transition Care 7) Duration of Stay
- Plata vs. Schwarzenegger
- Development of Chronic Care Programs
- CPR
Historical Challenges to HCV Treatment in Prisons
1) Psychiatric Illness 2) HIV Co-infection 3) ALT Level 4) Lack of Funding 5) Access to Subspecialty Care 6) Transition Care 7) Duration of Stay
Image Courtesy of Ray Chavez and CA Prison Health Care Receivership

HCV Epidemic in CDCR• Hepatitis C Care on the inside
– Subspecialty care onsite or telemedicine through Chronic Care Program
– Primary Care Physicians with HCV Expertise
• HCV prevalence in CA prisons ~ 34%1-2
– 175,000 x .34 ≈ 60,000– 60,000 x .80 = 48,000
1. Ruiz JD, Molitor F, Plagenhoef, JA. Trends in hepatitis C and HIV infection among inmates entering prisons in California, 1994 versus 1999. AIDS. 2002, 16:2236-38.
2. Fox RK, Currie SL, Evans J, et al. Hepatitis C virus infection among prisoners in the California state correctional system. Clin Infect Dis. 2005; 41:177-186.

Hepatitis C Team Model of Care
R & R Nurse Primary Care Physician
HCV Clinic Coordinator
Peer Education
HCV Pharmacist
Transplant Specialist
HepatologyInterventional Radiology
HCV Treating Clinician
HCV Clinic Coordinator Available
California Department of Corrections Hepatitis C Chronic Care Program
Mental Health Professional

Correctional Medicine Correctional Medicine Consultation NetworkConsultation Network Who are we?
Program of Department Family and Community Medicine, University of California, San Francisco
In collaboration with:CDCRCalifornia Prison Health Care Receivership
UCSF Faculty in prison: Primary Care Specialists

CMCN OverviewCMCN OverviewImprove quality of patient care through: Peer education and professional
development Consultation for chronic care, high risk
patients, and specialty patients Recruitment of new clinical staff Multidisciplinary team development Evaluation of medical care delivery system
components

CMCN Faculty ActivitiesCMCN Faculty Activities
Professional Development: Provider staff Training Peer Educators Collaboration with management team System evaluation and quality improvement Introduce technology Focused reviews to determine cost saving and
outcomes improvement strategies for: specialty consultations, pharmacy, laboratory, hospitalization, and emergency services
CMCN Academic Training UCSF Primary Care Medicine Residents
UCSF Family Medicine Residents: Geriatrics
Elective rotations: Residents and medical students Primary Care, HIV, Transgender
Nurse Practitioner student continuity clinics
Advanced Practice Nurse Training- CNS, Masters and PhD Projects
UCSF Medical Students: core family medicine rotation
AIDS Education and Training Center Collaboration

Clinical Consultation: Onsite and Telemedicine
Established in 2005 HIV Continuity of Care
Collaboration with PCP Training of PCP Periodic on site direct consultations 1200 patients with HIV, 7 prisons
Transgender Care 150 patients, 5 prisons
Primary care consultation

Clinical Consultation: Onsite and Telemedicine
Established 2007 Pain Consultation
Established 2008 HCV Continuity of Care
Collaboration with PCP Training of PCP Periodic on site direct consultations
Historical Challenges to HCV Treatment in Prisons
1) Psychiatric Illness 2) HIV Co-infection 3) ALT Level 4) Lack of Funding 5) Access to Subspecialty Care 6) Transition Care 7) Duration of Stay
- CDCR- CMCN

Historical Challenges to HCV Treatment in Prisons
1) Psychiatric Illness 2) HIV Co-infection 3) ALT Level 4) Lack of Funding 5) Access to Subspecialty Care 6) Transition Care 7) Duration of Stay

Image Courtesy of Ray Chavez and CA Prison Health Care Receivership

Transitioning Health Care
11 million people are released from prison and jail each year
Given a limited supply of medication
Little or no follow-up available in the community
No discharge planning from prison
Increased morbidity and mortality

Release from Prison High Risk of Death for Former Inmates
Retrospective cohort study of 30,237 released inmates
I. Binswanger, et al NEJM 2007; 356:157-65
12.7 times increased risk of death in first 2 weeks after release.
3.5 times increased risk of death in first 2 years.
The leading cause of death: drug overdose, cardiovascular disease, homicide and suicide.
Reintegration Difficulties
Employment: Unable to apply for certain jobs including all forms of public employment
Public Assistance: Prohibited from collecting food stamps, WIC, Pell grants, federal student aid
Medical Assistance: Lapse in Medicaid
Housing: Prohibited from public housing

Disenfranchisement
48 states and the District of Columbia prohibit felons from voting while serving a
sentence.
35 states prohibit felons on parole/probation
12 states disenfranchise all ex-offenders
4 million Americans have currently or permanently lost
their voting rights due to a felony
13% of all black men have lost their right to vote.

Recidivism
1994 a study looking at 272,111 persons released from prisons in 15 States.
67.5% were re-arrested for a felony or serious misdemeanor within 3 years.
46.9% were reconvicted. 25.4% re-sentenced to prison for a new crime.
California 2007, the recidivism rate = 56%National Commission on Correctional Health Care.
The health status of soon-to-be-released inmates; a report to congress.
Vol 1 and 2. Chicago: March, 2002. Available at http://www.ncchc.org/pubs/pubs_stbr.html

Historical Challenges to HCV Treatment in Prisons
1) Psychiatric Illness 2) HIV Co-infection 3) ALT Level 4) Lack of Funding 5) Access to Subspecialty Care 6) Transition Care 7) Duration of Stay
- Plata vs. Schwarzenegger
- Development of Chronic Care Programs
- CDCR- CMCN

Historical Challenges to HCV Treatment in Prisons
1) Psychiatric Illness 2) HIV Co-infection 3) ALT Level 4) Lack of Funding 5) Access to Subspecialty Care 6) Transition Care 7) Duration of Stay
- Plata vs. Schwarzenegger
- Development of Chronic Care Programs
- CDCR- CMCN

Future Directions
Build and reinforce links with community organizations and public health departments to support transition of care for HCV- infected individuals
Assess and address staffing and educational needs of CDCR
Expand peer education program statewide

Contact Information
Megan Mahoney, MD
Correctional Medicine Consultation Network
1940 Bryant Street
San Francisco, CA 94110
(415) 476-2041