herbal technology – challenges and opportunities for india – csir experience p. pushpangadan...
TRANSCRIPT

Herbal technology – challenges Herbal technology – challenges and opportunities for India – CSIR and opportunities for India – CSIR
experienceexperience
P. PushpangadanP. PushpangadanNational Botanical Research InstituteNational Botanical Research InstituteRana Pratap Marg, Lucknow-226001Rana Pratap Marg, Lucknow-226001

21st Century21st Century
2121stst century is the century of Biology powered and century is the century of Biology powered and propelled by scientific knowledge and technological propelled by scientific knowledge and technological expertiseexpertise
Three technologies namely Biotechnology Herbal technology Information technology (Bioinformatics)
are going to be the most powerful elements that are crucial for prosperity and welfare for the people of nations.

Herbal technologyHerbal technology
All technologies for the manufacture of All technologies for the manufacture of value added plant products can be value added plant products can be called as herbal technologycalled as herbal technology• Herbal drugs and pharmaceuticals,Herbal drugs and pharmaceuticals,• Nutraceuticals,Nutraceuticals,• Functional foods, designer foods or Functional foods, designer foods or
health foods and health drinkshealth foods and health drinks• CosmaceuticalsCosmaceuticals• Biocontrol agentsBiocontrol agents• BiopesticidesBiopesticides

WORLD TRADE AND ECONOMIES: THE PARADIGM
SHIFT “Resource – based economies’
to ‘Knowledge –based economies’
21 st Century will be the Century of Knowledge”……
“A nation’s ability to convert knowledge in to wealth and social good through the process of innovation will determine its future” ( R A Mashelkar, 2001)

Some features of international health careSome features of international health care Health care policies largely market driven by the Health care policies largely market driven by the
pharmaceutical industry diverting attention from health pharmaceutical industry diverting attention from health preservation to illness curepreservation to illness cure
Prevention and eradication of diseases undermines the Prevention and eradication of diseases undermines the economic basis of this industryeconomic basis of this industry
No satisfactory drugs available for most of the degenerative No satisfactory drugs available for most of the degenerative disorders characteristic of graying population and for re-disorders characteristic of graying population and for re-emerging resistant infectionsemerging resistant infections
Many currently used modern drugs do not have valid Many currently used modern drugs do not have valid proven clinical utility.proven clinical utility.
USA has among the highest per capita annual expenditure USA has among the highest per capita annual expenditure on health care ($3600) but still about 15% population is on health care ($3600) but still about 15% population is denied even basic care facilities (the best Indian state like denied even basic care facilities (the best Indian state like Kerala have an annual per capita expenditure ~ $15)Kerala have an annual per capita expenditure ~ $15)

Herbal drugs in international health careHerbal drugs in international health care Economic aspects:Economic aspects:
Global market of herbal drugs, Nutraceuticals ~$60 billion with 6% Global market of herbal drugs, Nutraceuticals ~$60 billion with 6% annual growth rate. Major share of Chinese and Koreans. Indian annual growth rate. Major share of Chinese and Koreans. Indian share variously estimated at 0.35-3.0%. Chinese production share variously estimated at 0.35-3.0%. Chinese production increased 200% between 1995-1999.increased 200% between 1995-1999.
Local acceptance:Local acceptance: DevelopedDeveloped
USA:USA: 42% use CAM spending over 29 billion US$ and 629 million visits in 42% use CAM spending over 29 billion US$ and 629 million visits in 1998. 1998. UK:UK: 28% use, spent 1.6 billion pounds and 127 million visits in 1998. 28% use, spent 1.6 billion pounds and 127 million visits in 1998. Australia:Australia: 60% use, A$ 620 billion in 1999. 60% use, A$ 620 billion in 1999.
Developing Developing Malaysia:Malaysia: Per capita consumption of traditional drugs, more than double of Per capita consumption of traditional drugs, more than double of modern pharmaceuticals. modern pharmaceuticals. S.Korea:S.Korea: Per capita consumption of traditional drugs 36% more than Per capita consumption of traditional drugs 36% more than modern drugs.modern drugs.African countries:African countries: 9 to 10 patients attending hospital OPD have first 9 to 10 patients attending hospital OPD have first consulted a traditional healer. consulted a traditional healer.

HERBAL DRUGS : RESURGENCE, HERBAL DRUGS : RESURGENCE, OPPORTUNITY AND COMPETITIONOPPORTUNITY AND COMPETITION
WORLD-WIDE
THE USE OF PHYTOPHARMACEUTICALS IS INCREASING @ 15% AGAINST 3% FOR MODERN PHARMACEUTICALS.
THE NUMBER OF PEOPLE USING HERBAL PRODUCTS ROSE BY 50% LAST YEAR.
35% OF OUT PATIENTS AND 22% OF INPATIENTS USE T.C.M. 940 HERBAL DRUG MANUFACTURING UNITS. HERBAL DRUG PRODUCTION ~ 18 BILLION CHINESE YUAN (DOMESTIC MARKETS). SALE OF HERBAL MEDICINE HAS 33% OF THE TOTAL DRUG MARKET.
U. S. A.
CHINA
Handa 2003
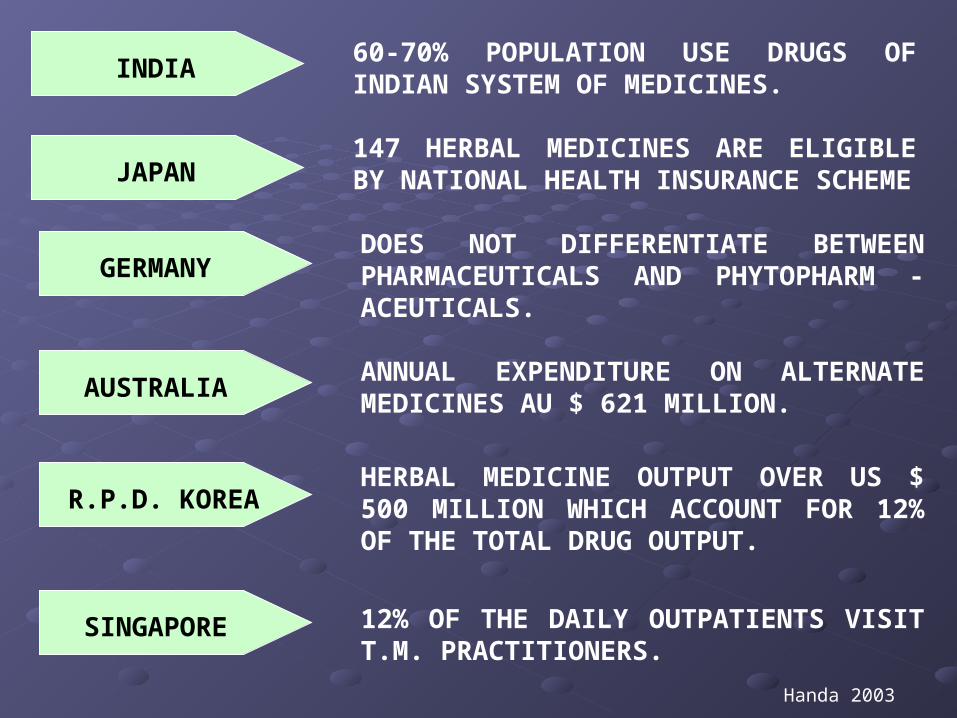
GERMANYDOES NOT DIFFERENTIATE BETWEEN PHARMACEUTICALS AND PHYTOPHARM -ACEUTICALS.
ANNUAL EXPENDITURE ON ALTERNATE MEDICINES AU $ 621 MILLION.
HERBAL MEDICINE OUTPUT OVER US $ 500 MILLION WHICH ACCOUNT FOR 12% OF THE TOTAL DRUG OUTPUT.
INDIA60-70% POPULATION USE DRUGS OF INDIAN SYSTEM OF MEDICINES.
JAPAN147 HERBAL MEDICINES ARE ELIGIBLE BY NATIONAL HEALTH INSURANCE SCHEME
AUSTRALIA
12% OF THE DAILY OUTPATIENTS VISIT T.M. PRACTITIONERS.
R.P.D. KOREA
SINGAPORE
Handa 2003

GLOBAL MEDICINAL PLANTS PRODUCT GLOBAL MEDICINAL PLANTS PRODUCT MARKETMARKET
NUTRACEUTICALSNUTRACEUTICALS HERBAL DRUGS HERBAL DRUGS
US $ 250 BILLIONUS $ 250 BILLION US $ 12.4 BILLION US $ 12.4 BILLION
REGION % MARKET SHARE
ECM 48
REST OF EUROPE 03
JAPAN 17
REST OF ASIA 20
NORTH AMERICA 12
CHINESE HERBS 18.7%
HERBAL TEA 14.5%
OTHER ASIAN PLANTS 6.0%
LOCAL AND OTHER IMPORTS 60.8%
REF P. Brevoort, 1997
% SHARES IN US HERBAL PRODUCT MARKET

GLOBAL SALE OF HERBAL GLOBAL SALE OF HERBAL DRUGS DRUGS
(BILLION US $; RETAIL)(BILLION US $; RETAIL)
EUROPE 7.0 8.9 1.9 27
ASIA 5.1 6.0 0.9 17
N.AMERICA 3.8 4.5 0.7 18
AUSTRALASIA 0.12 0.14 0.02 17
AFRICA +
MIDDLE EAST 0.19 0.21 0.02 24
S. AMERICA 0.6 0.83 0.23 38
E. EUROPE 0.37 0.40 0.03 8
REST OF WORLD 0.2 0.3 0.130

WORLD PHYTOPHARMACEUTICAL MARKET
PLANT-DRUG CATEGORY
SALE VALUE (Million US $) 1997 2002
AAGR %
TERPENOIDS 7,660 12,400 10.1
GLYCOSIDES 7,300 9,230 4.8
ALKALOIDS 3,600 4,045 2.4
OTHERS 4,048 5,013 4.4
TOTAL 22,608 30,668 6.3
SOURCE : BUSINESS COMMUNICATION COMPANY INC.

SALE OF HERBAL MEDICINES IN DIFFERENT REGIONS OF THE WORLD
REGION SALE VALUE (BILLION US $)
1994 1997 1999 2002 *
EUROPE 6.00 7.00 7.00 8.90
NORTH AMERICA 1.50 1.60 3.80 4.50
JAPAN 1.80 2.40 2.20 2.90
ASIA 2.70 2.20 5.10 6.00
AUSTRAL-ASIA - - 0.12 0.14
AFRICA & MIDDLE EAST - - 0.19 0.21
LATIN AMERICA - - 0.60 0.83
EASTERN EUROPE - - 0.37 0.40
REST OF WORLD 0.50 0.80 0.20 0.30
TOTAL 12.40 14.00 19.58 24.18
* Estimates Source : IMS 1994; Gruenwald, 1997; Gruenwald, 2000

MOST FREQUENTLY PRESCRIBED MONOMOST FREQUENTLY PRESCRIBED MONO--HERBAL PREPARATIONS IN GERMANYHERBAL PREPARATIONS IN GERMANY
Herbal drugs Botanical source Therapeutic class Retail sale value (million US$)
Ginkgo Ginkgo biloba Circulatroy agent 284 Horse chestnut Aesculus hippocastanum In varicose veins 70 Yeast preparations Fungal Source Antidiarrhoel 36 St. John’s wort Hypericum perforatum Antidepressant 36 Myrtle Myrtus communis Cough suppressant 22 Stinging nettle Urtica dioica Urologic 20 Saw palmetto Serenoa repens Urologic/Prostrate 19 Milk thistle Silybum marianum Urologic 18 Ivy leaf Hedera helix Cough suppressant 18 Mistletoe Viscum album Cancer treatment 14 Soy beans Glycine max Dermatological uses 9 Chamomile Matricaria chamomilla Dermatological uses 9 Comfrey Symphytum officinale Dermatological uses 8 Kava-kava Piper methysticum Tranquillizer 8 Greater celandine Chelidonium majus Gastrointestinal
treatments 8
Bromelain (from Pineapples)
Ananas comosus Anti-inflammatory, proteolytic
7
Cineole (essential oil)
Eucalyptus spp. Cold remedy 7
Black cohosh Cimicifuga racemosa Gynaecological uses 6
Source: RIRDC, 2000

DEMAND FOR AYURVEDIC AND UNANI DEMAND FOR AYURVEDIC AND UNANI MEDICINES FROM TOP 11 COUNTRIESMEDICINES FROM TOP 11 COUNTRIES
COUNTRY VALUE (m.us$)
COUNTRY VALUE (m.us$)
FRANCE 0.32 GERMANY 0.29 ITALY 0.60 MALASIA 0.74 NETHERLANDS 0.46 RUSSIA 0.48 SINGAPORE 0.61 SWITZERLAND 1.14 UKRAINE 0.40 UNITED ARAB EMIRATES 0.54 USA 0.49
TOTAL 8.8
SOURCE: PHARMABIZ 2001

Advantages of herbal drugsAdvantages of herbal drugs
Modern drugs can produce serious side effects Modern drugs can produce serious side effects • Latrogenic diseases fourth leading cause of death in Latrogenic diseases fourth leading cause of death in
USA and other developed nations (JAMA, April 1998). USA and other developed nations (JAMA, April 1998). • Side effects of drugs kill more Americans annually Side effects of drugs kill more Americans annually
than the world war II and Vietnam war combined (M. than the world war II and Vietnam war combined (M. Rath N. Y. Times 28.2.2003). Rath N. Y. Times 28.2.2003).
• Around 2600 persons died in the Twin Tower tragedy Around 2600 persons died in the Twin Tower tragedy on 11on 11thth September 2001 causing global repercussions. September 2001 causing global repercussions. It is, however, not recognized that about the same It is, however, not recognized that about the same number die in USA from side effects of prescription number die in USA from side effects of prescription drugs every 10 days (JAMA, April 1998). drugs every 10 days (JAMA, April 1998).

Herbal drugs are best suited for:Herbal drugs are best suited for: PRIMARY HEALTH CAREPRIMARY HEALTH CARE INFECTIOUS DISEASES INFECTIOUS DISEASES
AIDS and other viral infections AIDS and other viral infections Opportunistic infections Opportunistic infections MDR infections (e.g. T.B., Malaria) MDR infections (e.g. T.B., Malaria)
DEGENERATIVE & GERONTOLOGICAL CONDITIONS DEGENERATIVE & GERONTOLOGICAL CONDITIONS Osteoporosis Osteoporosis Chronic arthritis like osteoarthritis and rheumatoid arthritisChronic arthritis like osteoarthritis and rheumatoid arthritis Neurological like Alzheimer, Parkinsonism Neurological like Alzheimer, Parkinsonism Anti-aging Anti-aging
Metabolic disordersMetabolic disorders DiabetesDiabetes DyslipidemiasDyslipidemias
Other conditionsOther conditions Microcirculatory disordersMicrocirculatory disorders Liver diseasesLiver diseases ImmunostimulantsImmunostimulants Anti-cancerAnti-cancer Drugs affecting male libidoDrugs affecting male libido
Challenges aheadChallenges ahead
The major challenge is quality control and The major challenge is quality control and standardizationstandardization
Scientific validation of the therapeutic Scientific validation of the therapeutic claimsclaims
SafetySafety
Customer satisfaction and confidenceCustomer satisfaction and confidence

Three pillars of ideal herbal drug Three pillars of ideal herbal drug and their rational useand their rational use
QUALITY
EFFICACYSAFETY
GU
IDELIN
ES – RA
TION
AL U
SE
AVAILABILITY
ACCESSABILITY
QUALITY
SAFETY EFFICACY
APPROPRIATE USE OF Herbal Drug

Standardization of Herbal drugsStandardization of Herbal drugsRaw DrugsRaw Drugs
Passport data of Raw Plant Drugs (Crude drugs)Passport data of Raw Plant Drugs (Crude drugs) Correct taxonomic identification & authenticationCorrect taxonomic identification & authentication Study on the medicinal part: root, stem, bark, leaves, flowers, Study on the medicinal part: root, stem, bark, leaves, flowers,
fruits,nuts, gum, resins etc.fruits,nuts, gum, resins etc. Collection details: Location, stage & development/ growth of Collection details: Location, stage & development/ growth of
the plants, time, pre-processing storage etc.the plants, time, pre-processing storage etc. Organoleptic examination of raw drug:Organoleptic examination of raw drug:
Evaluation by means of sensory organs: touch, odour tasteEvaluation by means of sensory organs: touch, odour taste Microscopic & molecular examinationMicroscopic & molecular examination Chemical composition (TLC, GLC, HPLC, DNA fingerprinting)Chemical composition (TLC, GLC, HPLC, DNA fingerprinting) Biological activity of the whole plantBiological activity of the whole plant Shelf life of raw drugsShelf life of raw drugs

Standardization of Herbal drugs-Standardization of Herbal drugs-Herbal FormulationHerbal Formulation
Follow defined Good Manufacturing Practices (GMP)Follow defined Good Manufacturing Practices (GMP) Scientific VerificationScientific Verification
Toxicity evaluationToxicity evaluation Chemical profilingChemical profiling Pharmacodynamics – effect of drug in the bodyPharmacodynamics – effect of drug in the body Pharmacokinetics – absorption, distribution, metabolism, Pharmacokinetics – absorption, distribution, metabolism,
mechanism of action and executionmechanism of action and execution DosageDosage Stability and shelf lifeStability and shelf life Presentation and PackingPresentation and Packing Therapeutic merits – Compared with other drugsTherapeutic merits – Compared with other drugs

Good Survey of literature (Ancient & Modern)Good Survey of literature (Ancient & Modern) Develop and Observe Norms of:Develop and Observe Norms of:
Good Agricultural Practices (GAP)Good Agricultural Practices (GAP) Good Collection/Harvesting and Post Harvest Good Collection/Harvesting and Post Harvest
Handling Practices (GCP/ GHP & GPHP)Handling Practices (GCP/ GHP & GPHP) Good Laboratory Practices (GLP)Good Laboratory Practices (GLP) Good Clinical Practices (GCP)Good Clinical Practices (GCP) Good Manufacturing Practices (GMP)Good Manufacturing Practices (GMP) Good Marketing Techniques (GMT)Good Marketing Techniques (GMT)
Good Practices/Techniques in Good Practices/Techniques in Herbal ProductsHerbal Products

Physico-chemical value
Parameters required for quality evaluation of herbal drugs

QUALITY EVALUATION QUALITY EVALUATION OF HERBAL DRUGSOF HERBAL DRUGS
CHEMICALCHEMICAL
BIOLOGICAL
BIOLOGICAL
ORGANOLEPTIC
ORGANOLEPTICBOTANICALBOTANICAL
PH
YS
ICA
LP
HY
SIC
AL
• Moist. Cont.• Extrac. Values• Ash Values• Fluores. Analy.
Macroscopic Microscopic
• Qualitative • Quantitative• SEM Studies • Powder Studies
•Shape
•External
•Marking
• Colour • Odour• Taste• Texture • Fracture
Antagonistic
Microbial Contamination
•Toxicological•Pharmacological
•Other specific activities
• Bacterial• Fungal
• Qualitative• Quantitative • Chromatography• Heavy metal • Pesticide residue• Mycotoxin
HPTLC GLC HPLC
HPTLC Finger printing Sec. Metabolites DNA Finger printing
Standardization & Quality Evaluation of Herbal drugs

Vision of Herbal Drug Industry
“To provide intellectual capital to make available safe, cost effective, affordable therapeutics to the people of Indo-Pacific region – to help to reduce the percentage of mortality, morbidity and to emerge as significant players in the global market place.”

Problems faced by Indian Traditional Medicine
• Reluctance to accept adopt and assimilate modern scientific methods and tools,
• Lack of consistency in quality in batch to batch products
• Absence of standardization
• Lack of systematic scientific documentation of the herbal drugs
• Rare and endangered position of many important medicinal plants

CSIR initiatives in Traditional Medicine
• 20 laboratory networked programme on discovery of bioactive molecules mainly based on the clues from traditional medicine.
• New Millennium India Technology Leadership Initiative (NMITLI) Programme. In this a number of non CSIR laboratories and pharmaceutical industries are also joining hands. It is intended to establish pharmacoepidemeological evidence base to Ayurvedic medicines, practice and development of standardized herbal formulations.