hibiscus as an alternative treatment for hypertensioncoralrudie.yolasite.com/resources/hibiscus...
TRANSCRIPT
+ Hibiscus as an
Alternative Treatment for Hypertension
Cara Montesano, Coral Rudie, Esther Lee, Helaine Krasner
December 17, 2012
++
Mahan, L.K. & Stump, S. (2008) Krause’s food & nutrition therapy. (12th ed.) St. Louis, MO.: Saunders/Elsevier.
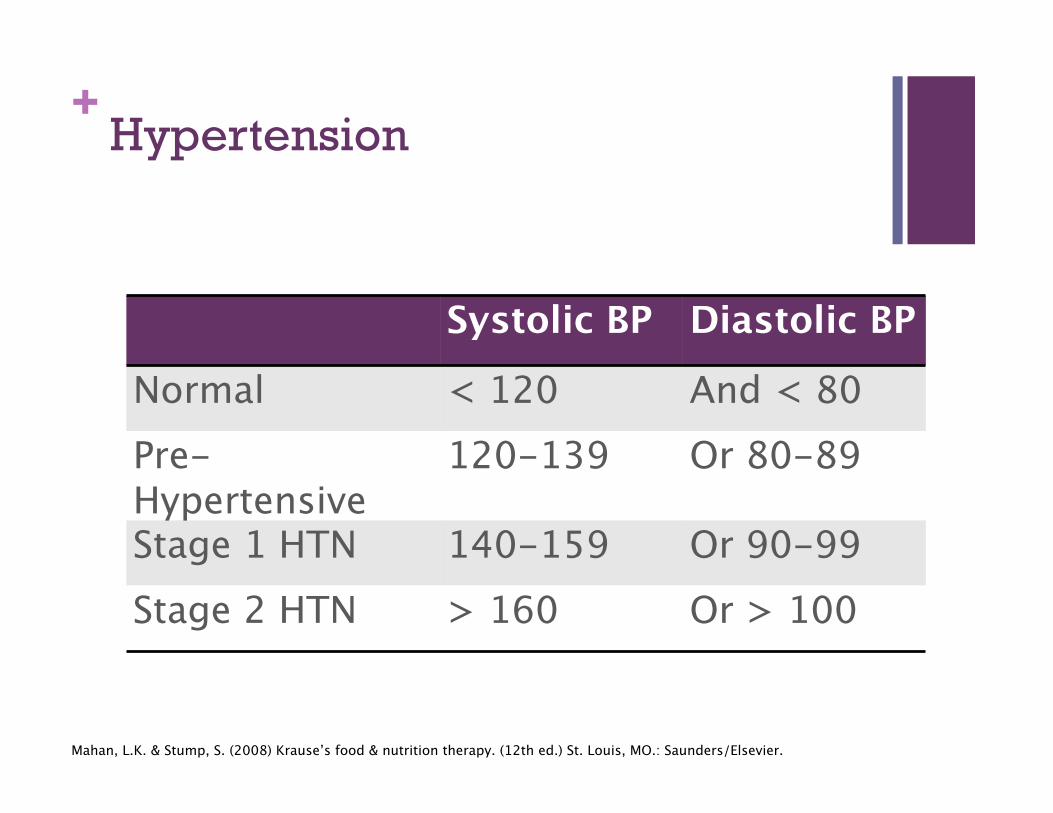
Systolic BP Diastolic BP
Normal < 120 And < 80 Pre-Hypertensive
120-139 Or 80-89
Stage 1 HTN 140-159 Or 90-99 Stage 2 HTN > 160 Or > 100
Hypertension
++ Importance of Controlling Hypertension
Avoid disease progression
Prevent cardiovascular complications
Untreated HTN leads to degenerative diseases such as HF, ESRD, PVD, and Stroke
To maintain a good quality of life
Reduce the mortality associated with this disease
Mahan, L.K. & Stump, S. (2008) Krause’s food & nutrition therapy. (12th ed.) St. Louis, MO.: Saunders/Elsevier.
++ Blood Pressure Homeostasis
Body regulates BP via Sympathetic nervous system (short term) and the kidneys (long term control)
Sympathetic nervous system can stimulate both vasoconstriction and vasodilatation
Kidney regulates BP by controlling extracellular fluid volume and secreting renin which initiates the renin-angiotensin system system
Mahan, L.K. & Stump, S. (2008) Krause’s food & nutrition therapy. (12th ed.) St. Louis, MO.: Saunders/Elsevie
++ Physiological Mechanisms Involved in the Development of Essential Hypertension
Cardiac Output
Peripheral Resistance
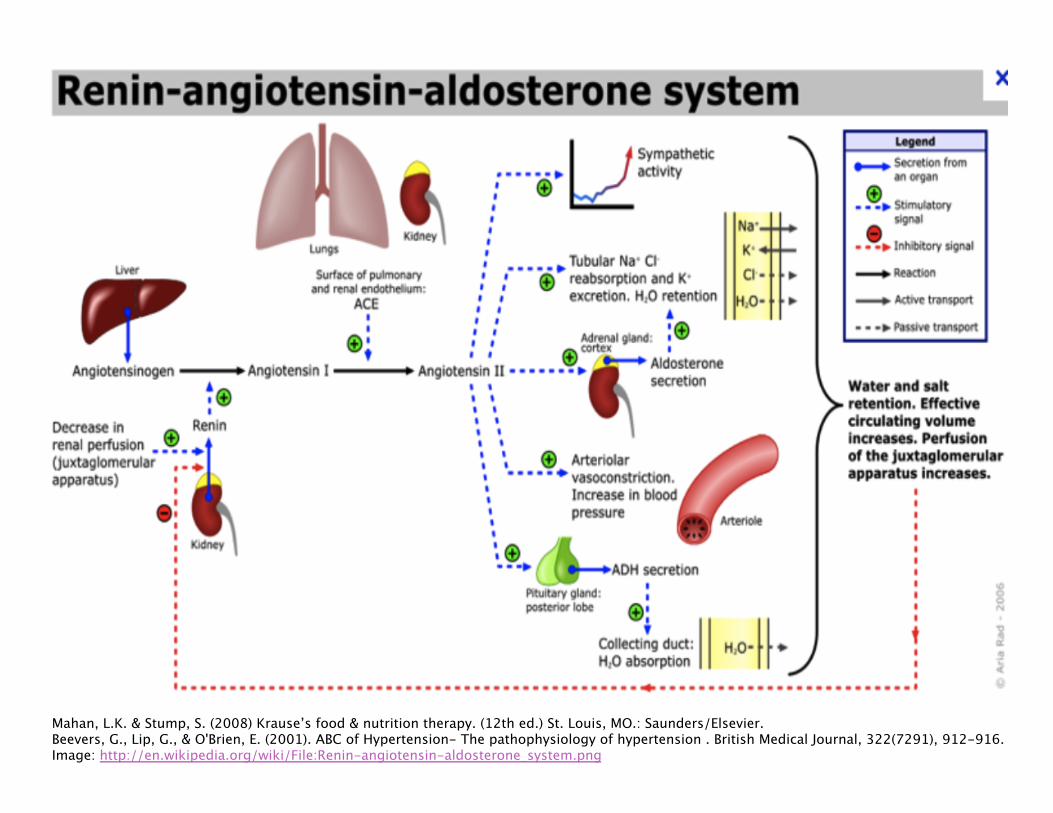
Renin-Angiotesin-Aldosterone System
Autonomic Nervous System
Other Factors: Bradykinin, Endothelin, Endothelial derived relaxing factor (EDRF) or nitric oxide, Atrial Natriuretic peptide (ANP), Ouabain
Beevers, G., Lip, G., & O'Brien, E. (2001). ABC of Hypertension- The pathophysiology of hypertension . British Medical Journal, 322(7291), 912-916..
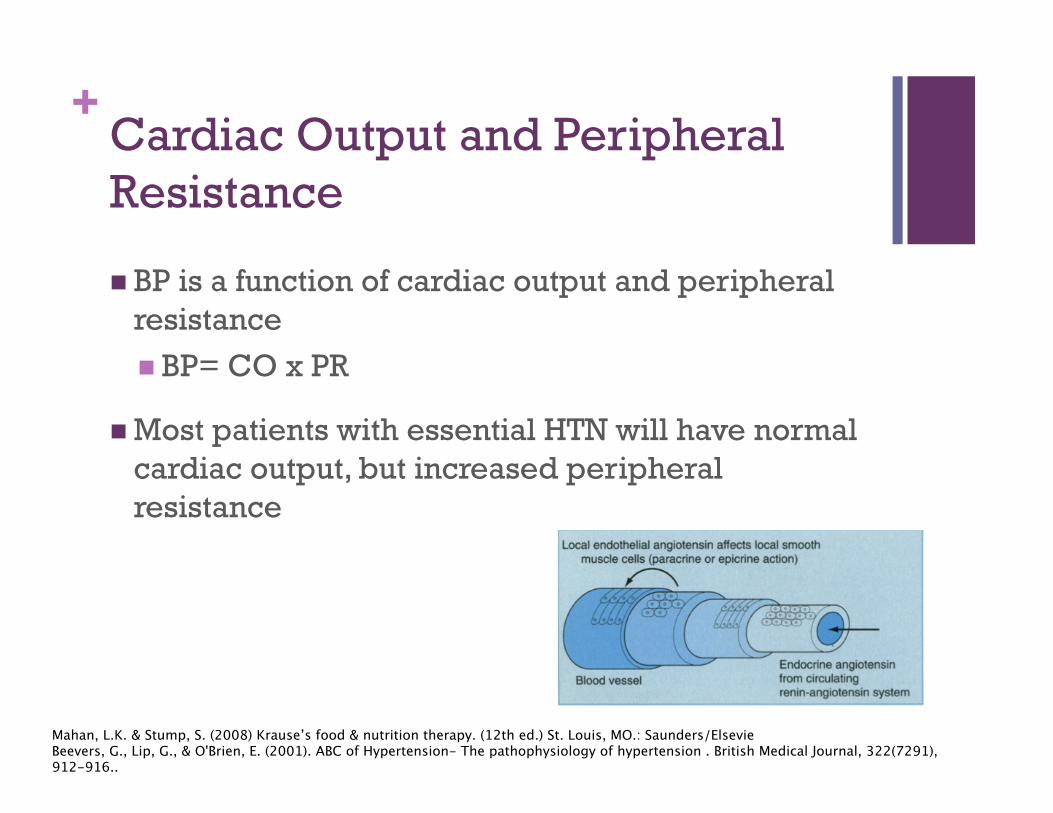
++ Cardiac Output and Peripheral Resistance
BP is a function of cardiac output and peripheral resistance BP= CO x PR
Most patients with essential HTN will have normal cardiac output, but increased peripheral resistance
Mahan, L.K. & Stump, S. (2008) Krause’s food & nutrition therapy. (12th ed.) St. Louis, MO.: Saunders/Elsevie Beevers, G., Lip, G., & O'Brien, E. (2001). ABC of Hypertension- The pathophysiology of hypertension . British Medical Journal, 322(7291), 912-916..
++
Mahan, L.K. & Stump, S. (2008) Krause’s food & nutrition therapy. (12th ed.) St. Louis, MO.: Saunders/Elsevier. Beevers, G., Lip, G., & O'Brien, E. (2001). ABC of Hypertension- The pathophysiology of hypertension . British Medical Journal, 322(7291), 912-916. Image: http://en.wikipedia.org/wiki/File:Renin-angiotensin-aldosterone_system.png
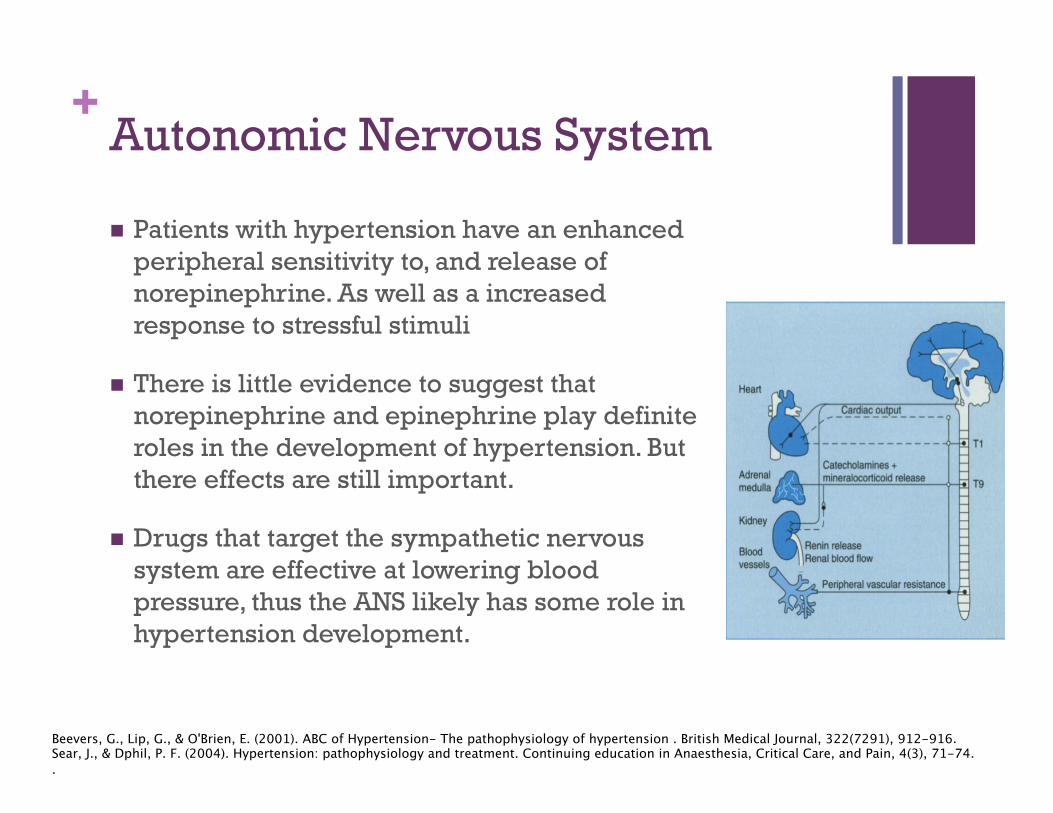
++ Autonomic Nervous System
Patients with hypertension have an enhanced peripheral sensitivity to, and release of norepinephrine. As well as a increased response to stressful stimuli
There is little evidence to suggest that norepinephrine and epinephrine play definite roles in the development of hypertension. But there effects are still important.
Drugs that target the sympathetic nervous system are effective at lowering blood pressure, thus the ANS likely has some role in hypertension development.
Beevers, G., Lip, G., & O'Brien, E. (2001). ABC of Hypertension- The pathophysiology of hypertension . British Medical Journal, 322(7291), 912-916. Sear, J., & Dphil, P. F. (2004). Hypertension: pathophysiology and treatment. Continuing education in Anaesthesia, Critical Care, and Pain, 4(3), 71-74. .
++ Conventional Treatments
Lifestyle Modifications
Drug Therapy Diuretics
Beta- Blockers
Calcium Channel Blockers
Angiotensin Converting Enzyme (ACE) Inhibitors
Angiotensin II Receptor Blockers
Alpha-1 Andrenergic blockers
Direct Vasodilators
Central Adrenergic Inhibitors
Natriuretic Peptides
Sear, J., & Dphil, P. F. (2004). Hypertension: pathophysiology and treatment. Continuing education in Anaesthesia, Critical Care, and Pain, 4(3), 71-74.
++ Alternatives to Medication
Good evidence to support hibiscus as an integrative therapy for hypertension.
Hibiscus has antioxidant properties and can be an effective treatment for hypertension.
Treatment of hypertension with hibiscus tea has roots in Ayurvedic, Chinese, and folk medicine.
Natural Standard: The authority on integrative medicine (2012). Hypertension.
++ Hibiscus
Hibiscus sabdariffa Linn. (HS) belongs to the Malvaceae family
Syn: Roselle, Indian sorrel, Sour tea and Karkade, Jamaica or Flor de Jamaica
Annual shrub that grows to 8 ft in height and typically consists of a red calyx with five large sepals.
Tropical plant native to India and Malaysia Naturalized in many parts of the Americas
Deyanira Ojeda, (8 January 2010). Inhibition of angiotensin convertin enzyme (ACE) activity by the anthocyanins delphinidin- and cyanidin-3-O-sambubiosides from Hibiscus sabdariffa Journal of Ethnopharmacology, Volume 127, Issue 1, Pages 7–10 Francisco J. Alarcon-Aguilar, (8 October 2007,). Effect of Hibiscus sabdariffa on obesity in MSG mice Journal of Ethnopharmacology, Volume 114, Issue 1, Pages 66–71
++ Hibiscus (cont.)
Hibiscus has been used for centuries in indigenous medicine Diuretic Treatment for gastrointestinal disorders, liver disease,
fever, hypercholesterolemia, and hypertension
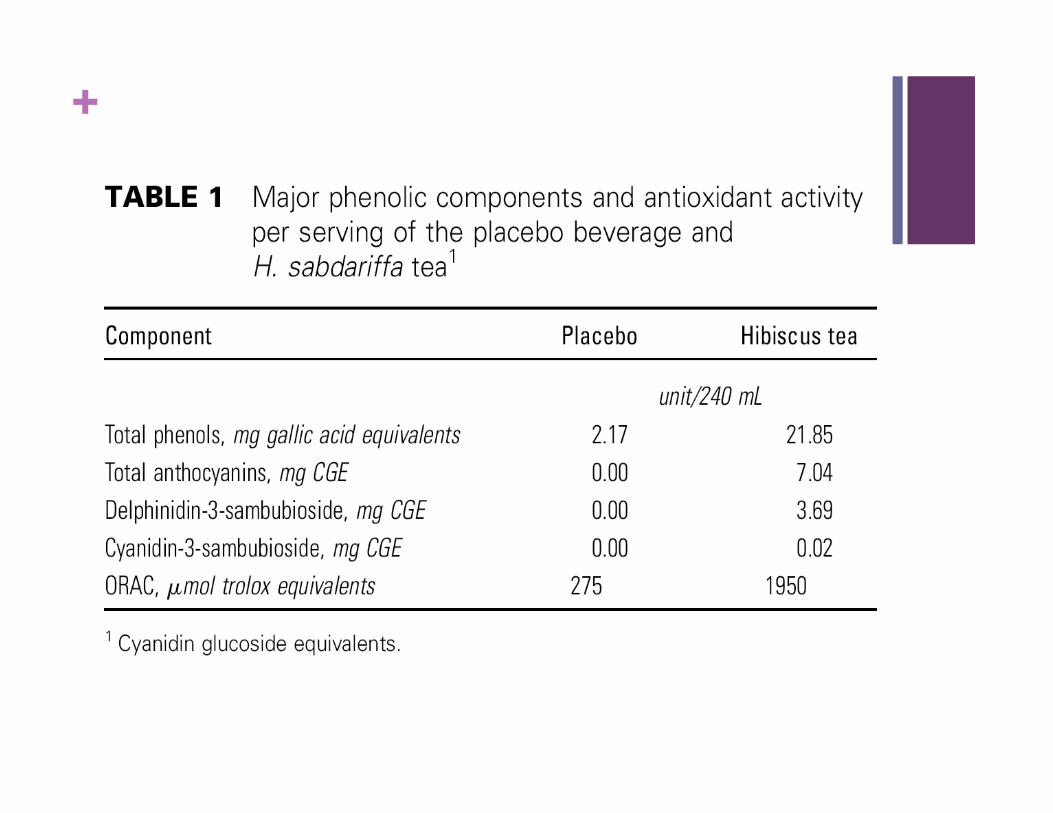
What’s in Hibiscus? Phenolics, organic acids, sterols, terpenoids,
polysaccharides and some minerals.
The extracts of HS exert potent antioxidant effects in vitro, achieved via the presence of several active constituents chief among which are flavonoids and vitamins. *Active compounds: Anthocyanins (delphini- din 3-
sambubioside and cyanidin 3-sambubioside)*
M. Ajay, H.J. Chai, A.M. Mustafa, A.H. Gilani, M.R. Mustafa. (February 2007). Mechanisms of the anti-hypertensive effect of Hibiscus sabdariffa L. calyces. Journal of Ethnopharmacology, Volume 109, Issue 3, 12 Pages 388–393,
++ Mechanism of Action
Vasodilator/Vasorelaxant Relaxes aortic rings through endothelium-dependent and
independent vasodilator pathways.
Endothelium-dependent vasodilator component results through activation of endothelium-derived nitric oxide/cGMP-relaxant pathway Endothelium-independent component could be due to inhibition of
Ca2+ influx into vascular smooth muscle cells.
Diuretic Aldosterone antagonist
Inhibits Angiotensin-converting enzyme (ACE) ACE inhibitory effect attributed to anthocyanins, delphinidin-3-O-
sambubioside (Compound 1) and cyanidin-3-O-sambubioside (Compound 2)
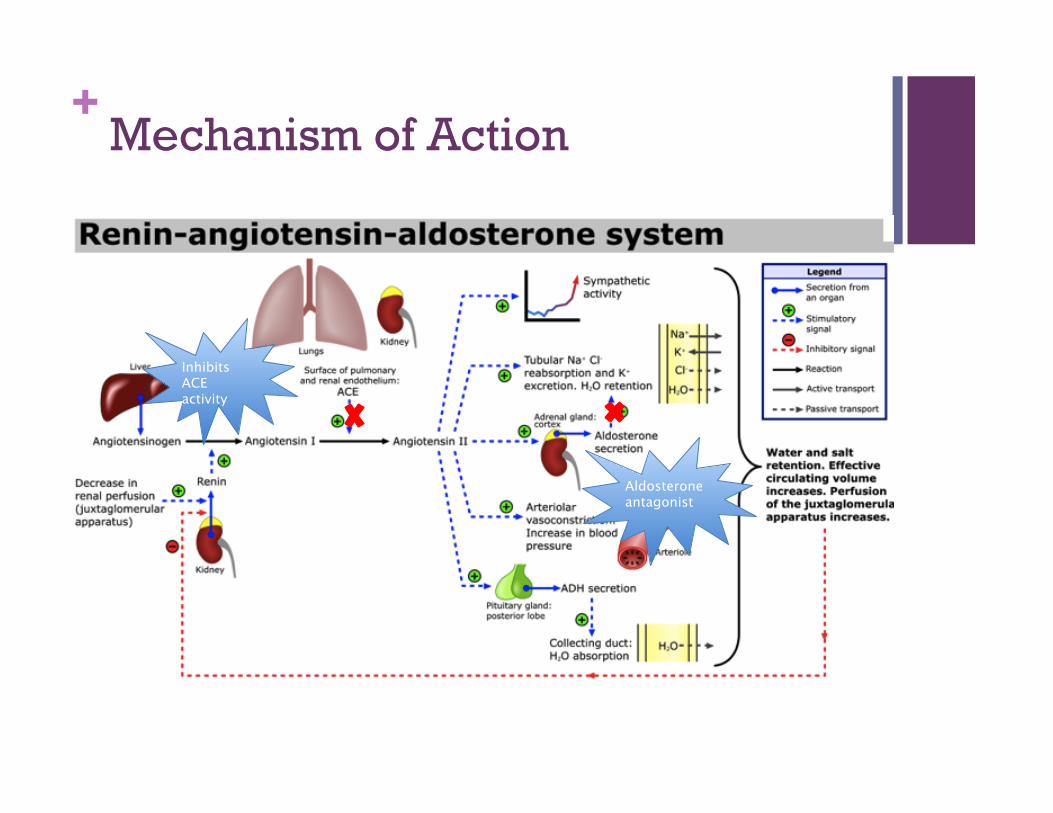
++ Mechanism of Action
Aldosterone antagonist
Inhibits ACE activity
+ 15 Hibiscus sabdariffa L. tea (1sane)
lowers blood pressure in prehypertensive and mildly
hypertensive adults
Diane L. Mckay, C-Y Oliver Chen, Edward Saltzman, Jeffery B. Blumberg
++ Study Details
Purpose of study: examine antihypertensive effects of H. sabdariffa tisane (hibiscus tea) consumption in humans.
Study design: randomized, double-blind, placebo-controlled clinical trial
Objective: determine if hibiscus tea reduced HTN in pre-mildly hypertensive adults > placebo
++ Materials & Methods
Standardized method was used to measure BP at baseline and at weekly intervals while consuming test beverage and placebo.
Sixty-five pre-mildly hypertensive adults age 30-70 yrs, not on HTN meds, consumed either 3 (240 mL) svgs/day of hibiscus tea or placebo beverage for 6 weeks.
++ Treatment
Tea bag contained 1.25 g H. sabdariffa (ground dried calyces)
Participants were instructed to steep bag in 240 mL boiled water for 6 minutes
Placebo group received an artificial hibiscus flavor concentrate to be added to 240 mL water via 16-18 drops (1.2 mL)
Participants could consume either beverage hot or cold, but had to consume within 12 hrs of prep
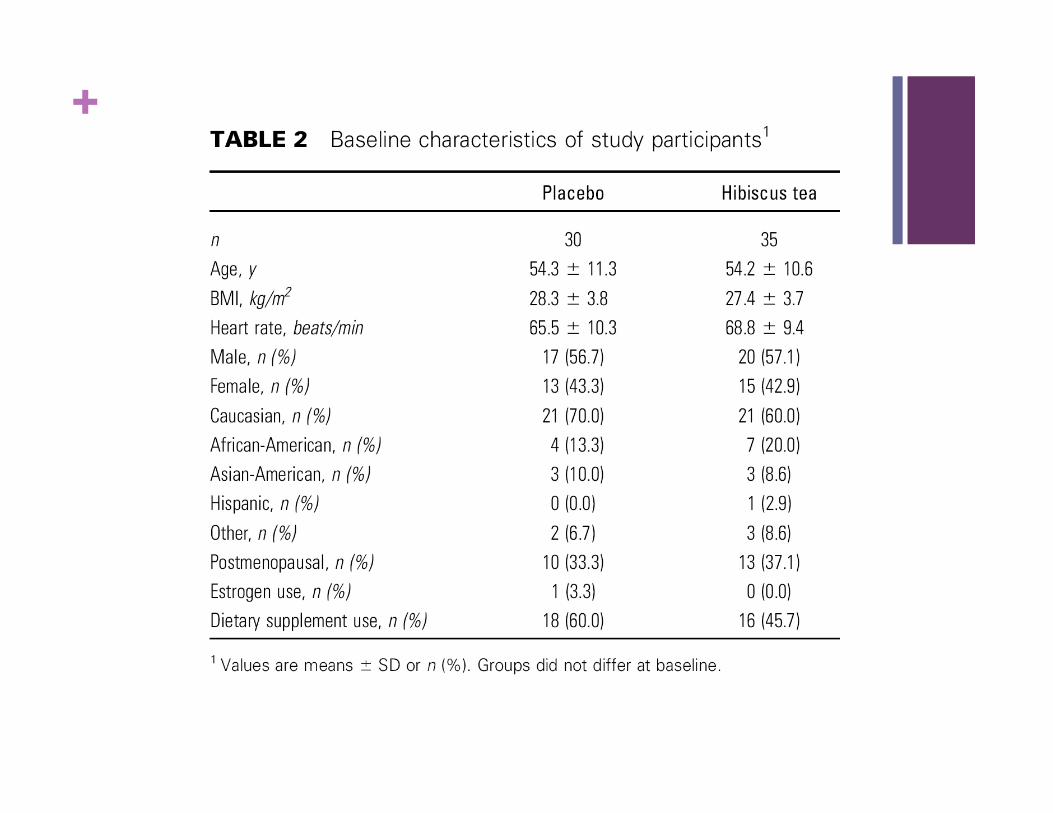
++ Participants
65 non-smoking males and females age 30-70 yrs w/ BMI 18.5-35.0
SBP 120-150 mmHg and DBP < 95 mmHg
Excluded if: taking meds known to affect BP active CVD, RD, endocrine or GI disease, RA bw chg > 5% or preg w/in last 6 mos caffeine intake > 425 mg/d, ethanol > 28g/d vit C supp > 500 mg/d, illegal drug use high intensity aerobic exercise >30 min/d, abnormal EKG or std labs
++
++
++ Results
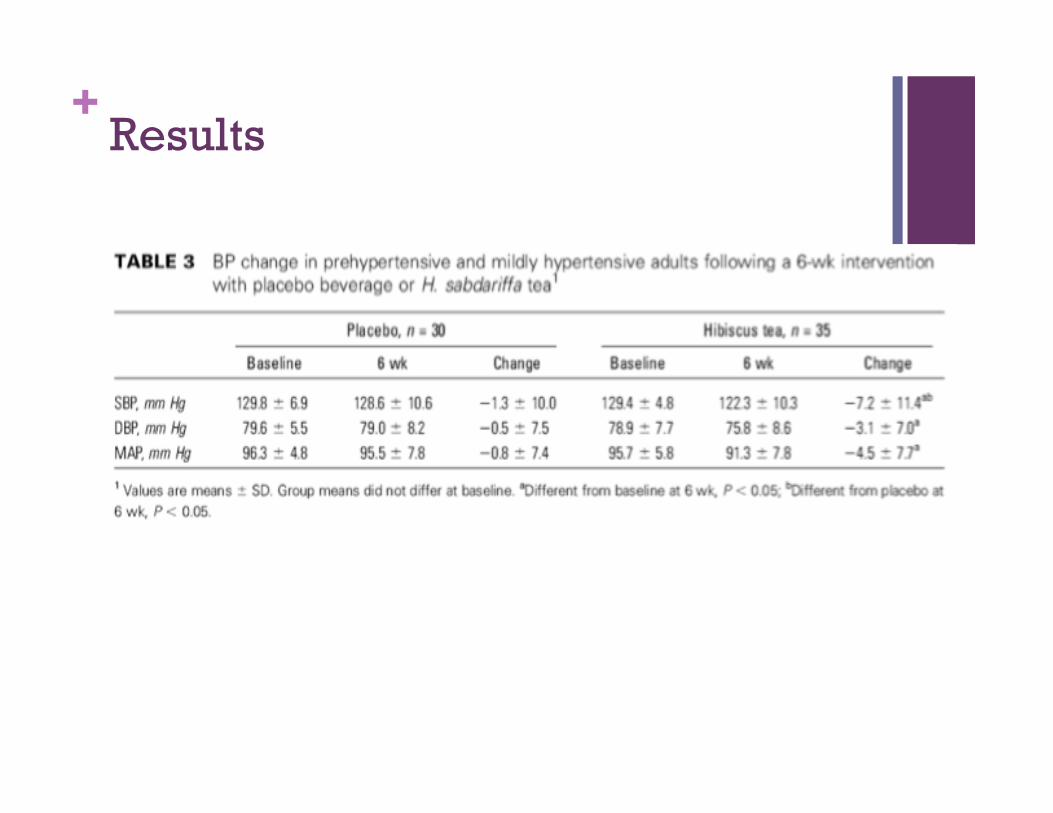
Hibiscus tea significantly lowered SBP compared to placebo (-7.2 ± 11.4 vs - 0.3 ± 10mmHg; P=0.03).
Diastolic BP was lower for both tea and placebo, but not significant.
Participants w/higher SBP at baseline had better response to tx (r = -0.421; P=0.01)
No effects based on age, gender, suppl use
++ Results
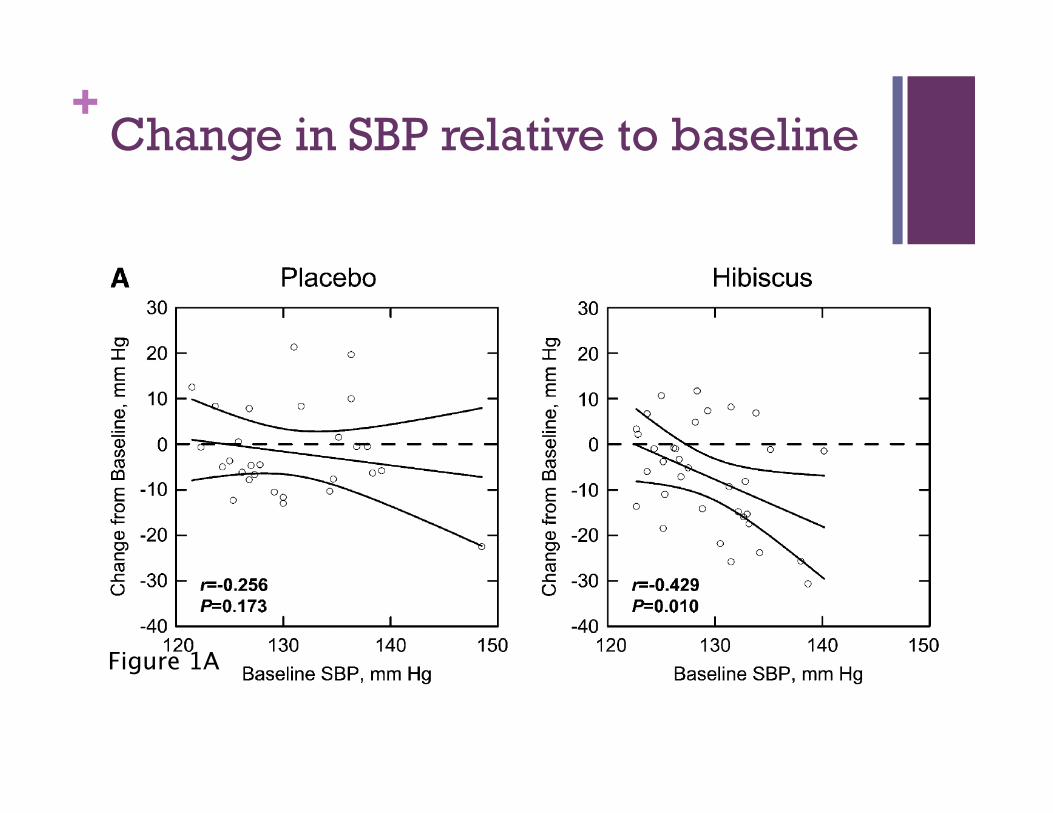
++ Change in SBP relative to baseline
Figure 1A
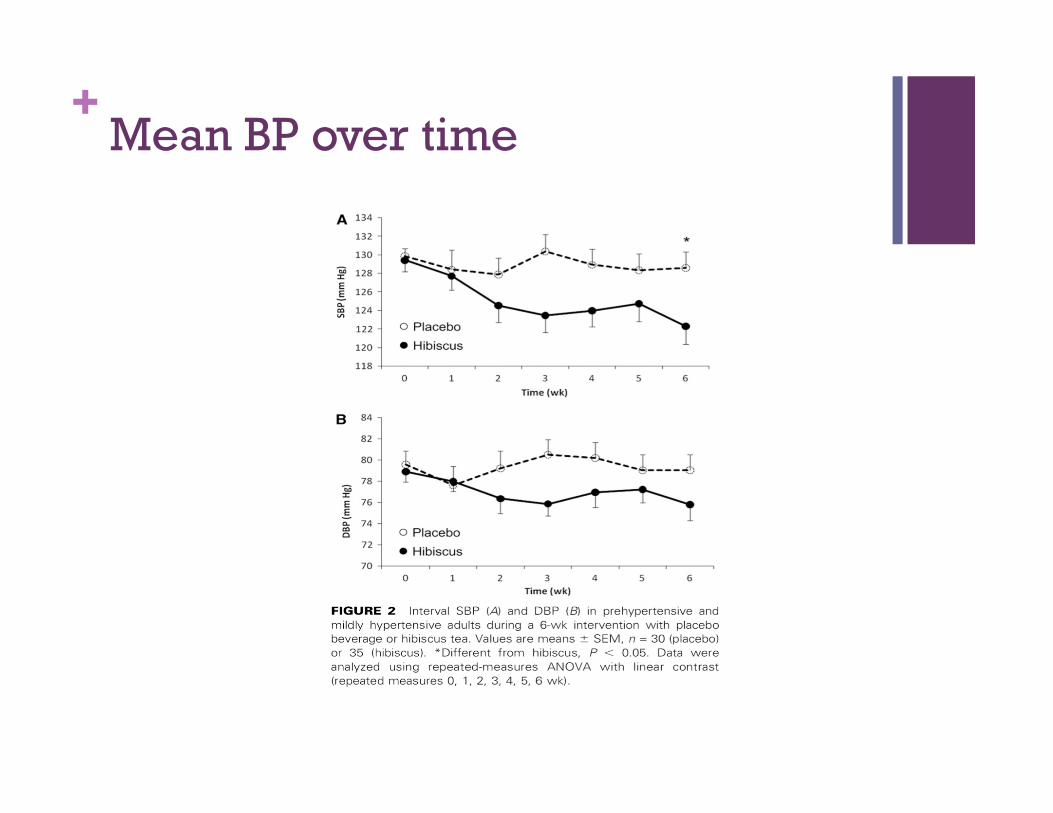
++ Mean BP over time
++ Study Conclusion
Daily consumption of 3 svgs Hibiscus sabdariffa tea in an amt easily and readily incorporated into the diet reduced BP in pre-mildly hypertensive adults
BP lowering effects were similar to those reported in previous large dietary intervention studies (DASH, PREMIER)
+ 27 Effec1veness and tolerability of a standardized extract from Hibiscus sabdariffa in pa1ents with mild to
moderate hypertension: a controlled and randomized
clinical trial
A. Herrera-Arellanoa, S. Flores-Romerob, M.A. Cha!vez-Sotoc, J. Tortorielloa
++ Purpose
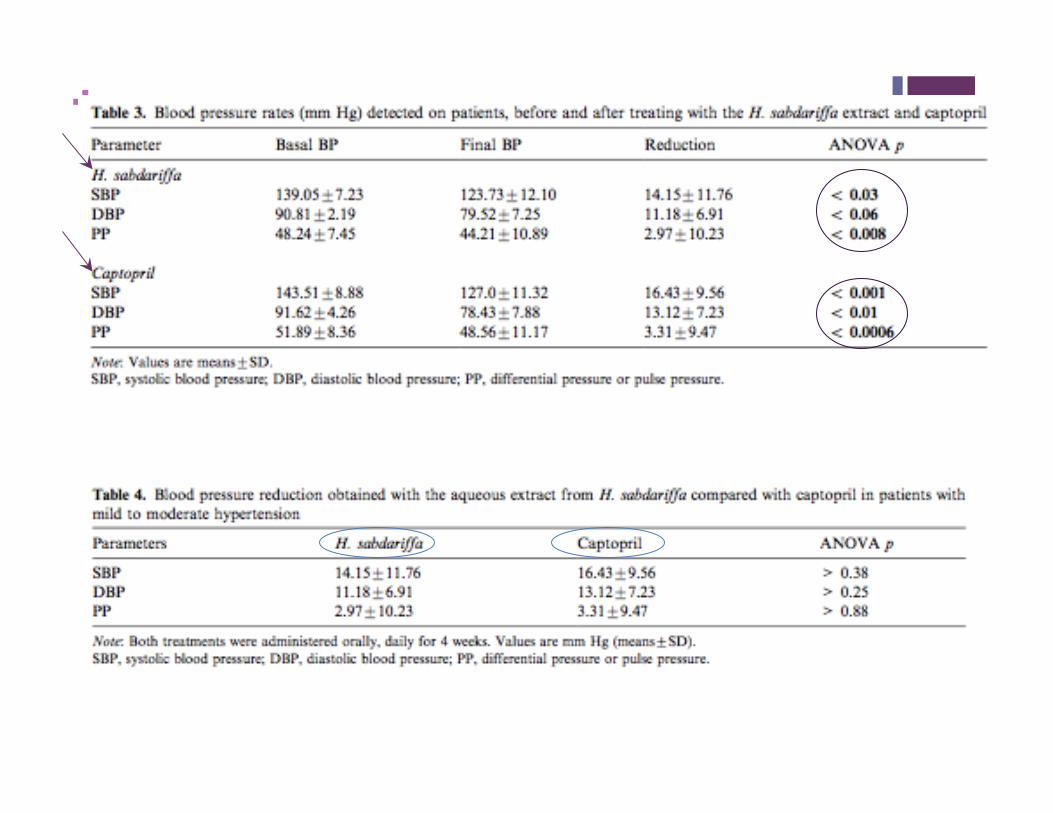
The aim of the present study was to compare the antihypertensive effectiveness and tolerability of the dry calyx from H. sabdariffa (standardized on 9.6 mg of anthocyanins/ dose) with captopril.
As well as to determine the modifications on the urinary electrolytes induced by the experimental treatment.
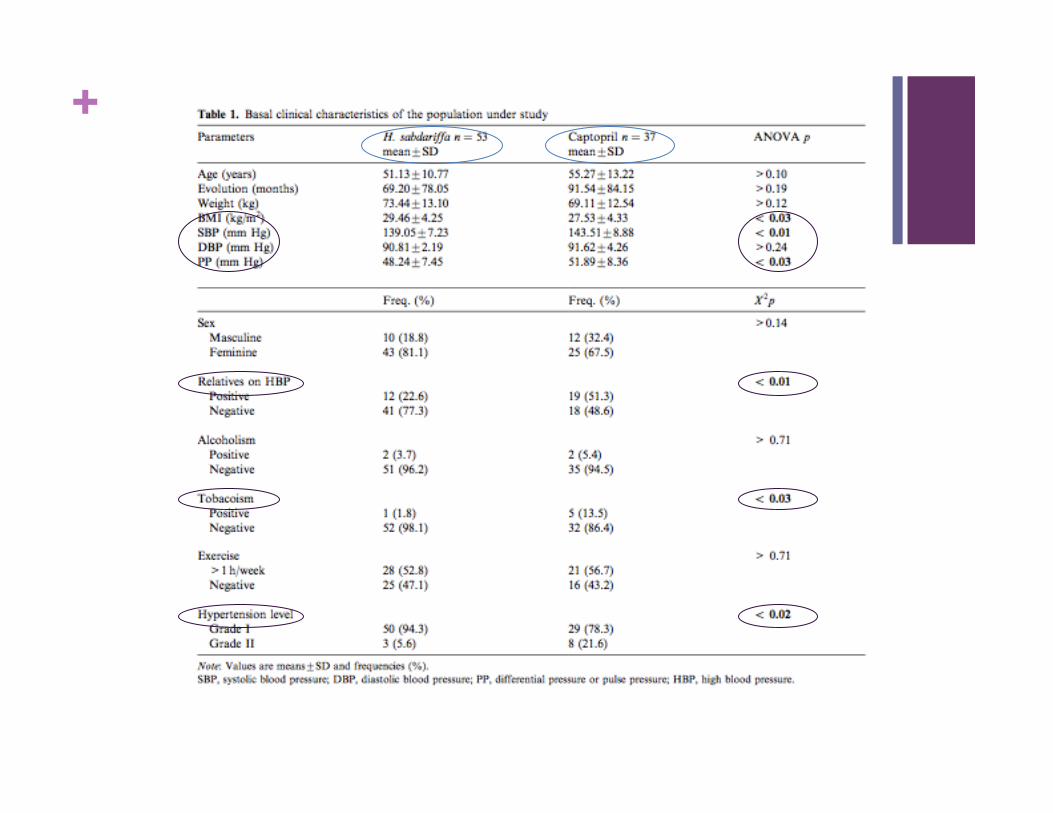
++ Materials and Methods
Subjects: 90 participants Both sexes Between 30 and 80 years of age Diagnosed with mild to moderate hypertension Have not received antihypertensive treatment in
the last month Granted consent
++ Preparation of Treatments
Hibiscus sabdariffa Collected from a controlled crop Dried under dark conditions at room
temperature Ground in an electric mill to obtain particles 10g given to the patient in powder form with
instructions
Captopril 25mg Administered every 12 hr for 4 weeks
++ Measurements
Therapeutic tolerability
Hypotensive effect
Urine test to determine urine electrolyte
Statistical analysis ANOVA
++ Procedure
Experimental group- 53 patients
Control group- 37 patients
Basal blood pressure
Oral and written instructions given
++
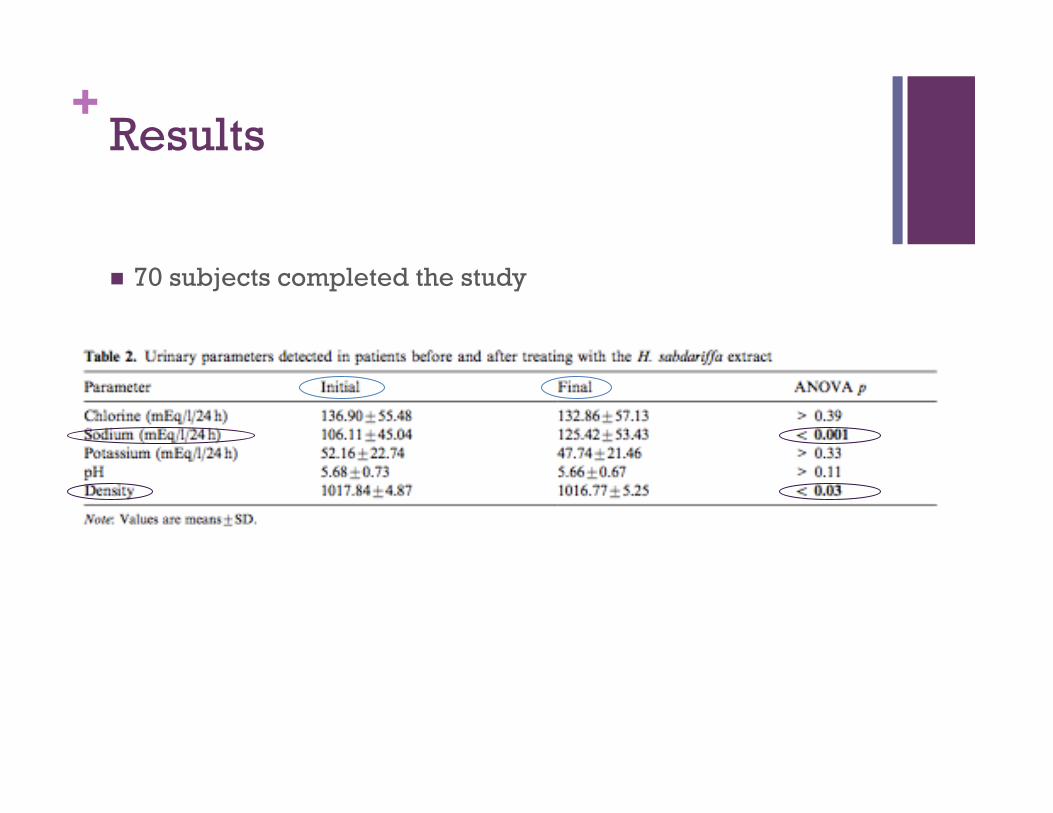
++ Results
70 subjects completed the study
++
++ Therapeutic Effectiveness/ Failure
Therapeutic Effectiveness: 78.95% from experimental group 84.38% from the control group
Therapeutic Failure: 23.08% from experimental group 25% from the control group
++ Conclusion
The study contributes further evidence of the acceptance of the short- and long-term administration of aqueous extract from H. sabdariffa, because no side-effects or intolerability was detected.
+ 38 Clinical Effects Produced by a Standardized Herbal Medicinal Product of Hibiscus sabdariffa on Pa1ents with Hypertension. A
Randomized, Double-‐blind, Lisinopril-‐Controlled Clinical Trial.
Armando Herrera-Arellano, Judith Miranda-Sánchez, Pedro Ávila-Castro, Sara Herrera-Álvarez, Jesús Enrique Jiménez-Ferrer, Alejandro Zamilpa, Rubén Román-Ramos, Héctor Ponce-Monter, Jaime Tortoriello
++ Purpose of the Study
“The aim of this project was to compare the antihypertensive effectiveness, tolerability, and safety, as well as the effect on serum electrolytes and the ACE inhibitory effect of a herbal medicinal product prepared from H. sabdariffa extract with lisinopril in patients with stage 1 or 2 HT.”
++ Research Question
How does the effectiveness, tolerability, and safety of H. sabdariffa extract compare to that of lisinopril in people with stage 1 and 2 Hypertension?
++ Study Background
Study Design: Randomized, controlled, double-blind clinical trial
Study Selection Criteria: Inclusion:
Males and Females 25 ± 61 years of age Stages 1 or 2 Hypertension classification Without antihypertensive treatment (at least during the previous 30
days) Exclusion:
Subjects with nephropathy, heart or hepatic diseases, cancer, non-controlled diabetes mellitus
Pregnant or breast-feeding women Subjects with evidence of secondary hypertension Known hypersenstivity or intolerance to ACE inhibitors or to Hibiscus
sabdariffa
Study Duration: 4 weeks Study occurred between August 2004 to March 2005
++ Study Intervention
Experimental Group: Hibiscus sabdariffa calyxes (HsHMP), 250mg of
total anthocyanins per dose
Control Group: Lisinopril (USP, 10 mg) mixed with artificial
flavor and color
The treatments were dissolved in 250 ml of water
Treated daily for 4 weeks
++ Study Outcomes
Effectiveness: diastolic blood pressure (DBP) reduction, >10 mmHg
Tolerability: absence of intensive or severe side effects
Safety: absence of pathological modifications in bio-chemical tests for hepatic and renal function (ALT, AST, ALP, urea, and creatinine).
Effect on serum electrolytes (Na, K, Cl)
Effect on ACE activity
++ Data Collection & Analysis
At the initial interview, measurement of basal conditions was conducted
Clinical evaluation, variables outcome, and treatment adherence were evaluated weekly.
Blood samples for biochemical analysis were obtained at the beginning and the end of treatment.
Statistical Analysis: Differences between mean pairs of data with normal
distribution The hypothesis test with analysis of variance (ANOVA) The X2 test was used for comparing two groups of
proportions. Stratified analysis was used for dichotomized confounding
variables. Values of p < 0.05 were considered for rejecting the nullity
hypothesis.
++ Study Population
193 subjects participated in the study
100 in the experimental group and 93 in the control
22 were eliminated due to lack of treatment adherence
171 were included in the analysis
No differences found between groups in the analyzed parameters (p >0.11)
56.99% of the subjects were Stage 1 Hypertensive
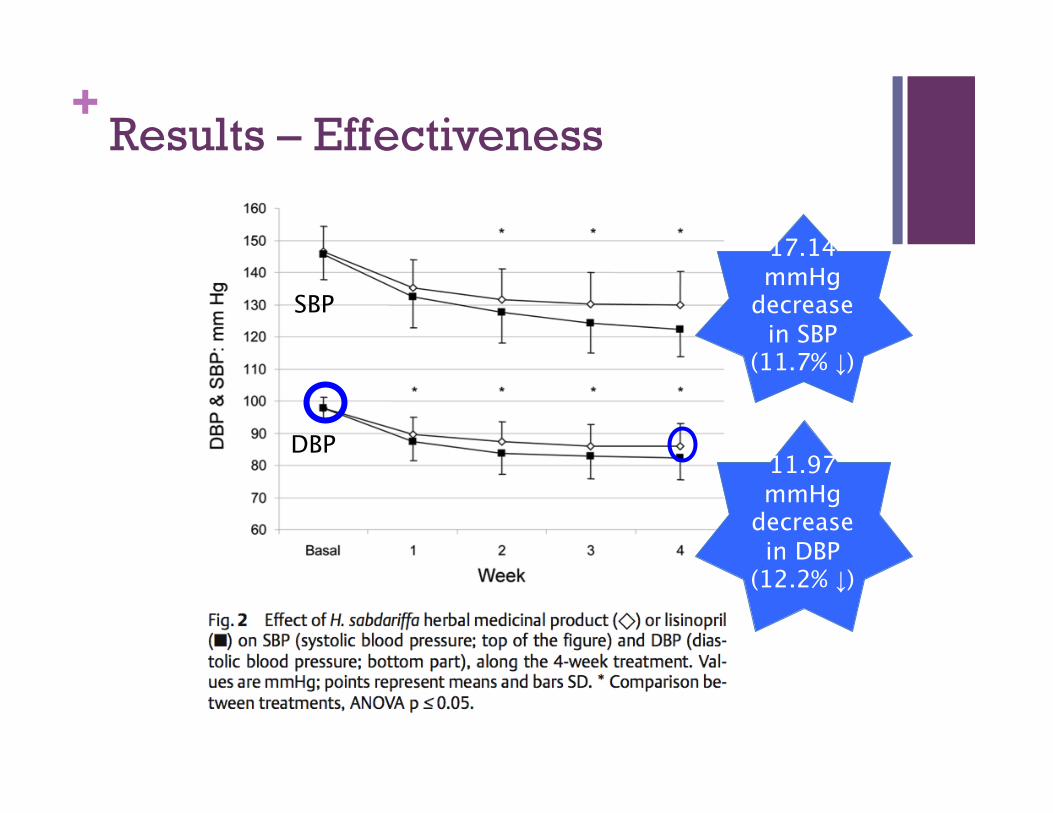
++ Results – Effectiveness
17.14 mmHg
decrease in SBP
(11.7% ↓)
11.97 mmHg
decrease in DBP
(12.2% ↓)
SBP
DBP
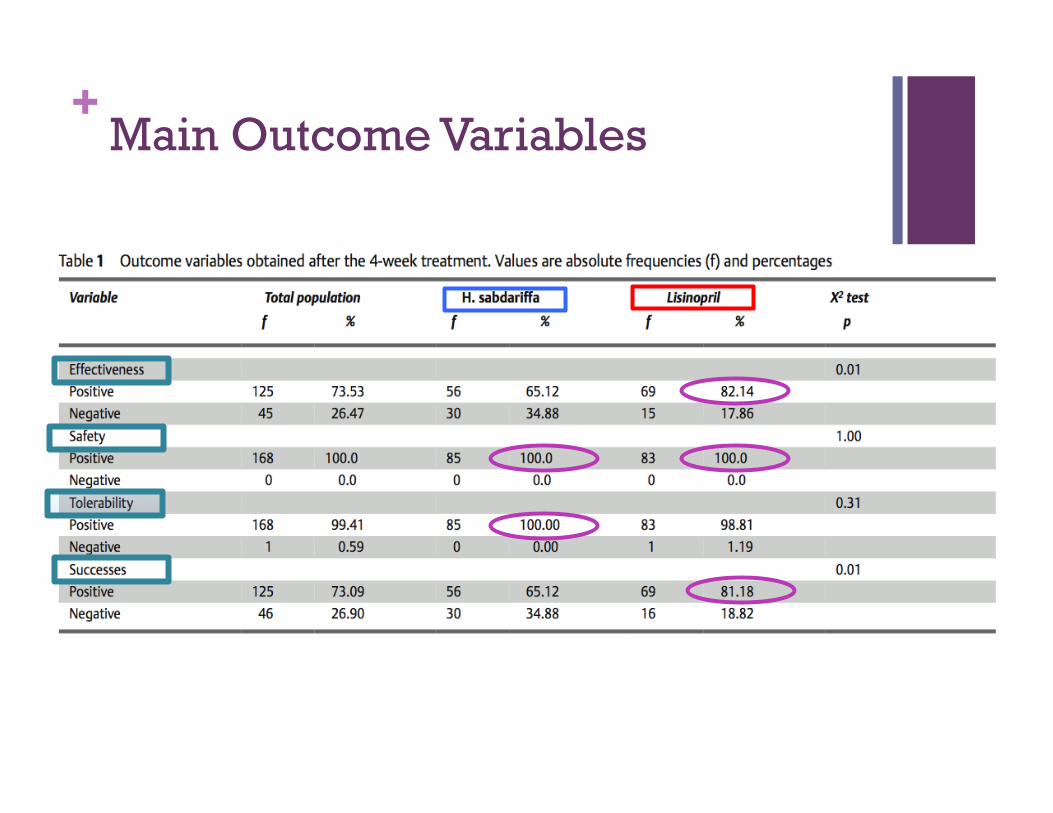
++ Main Outcome Variables
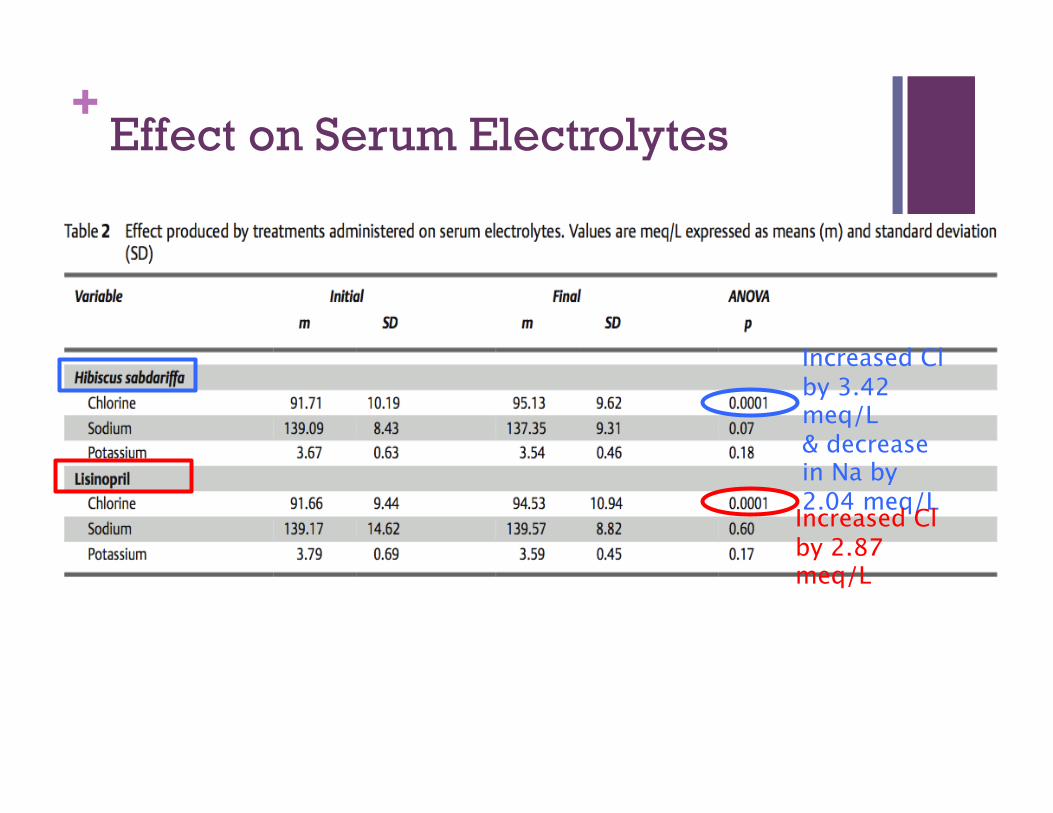
++ Effect on Serum Electrolytes
Increased Cl by 3.42 meq/L & decrease in Na by 2.04 meq/L Increased Cl by 2.87 meq/L
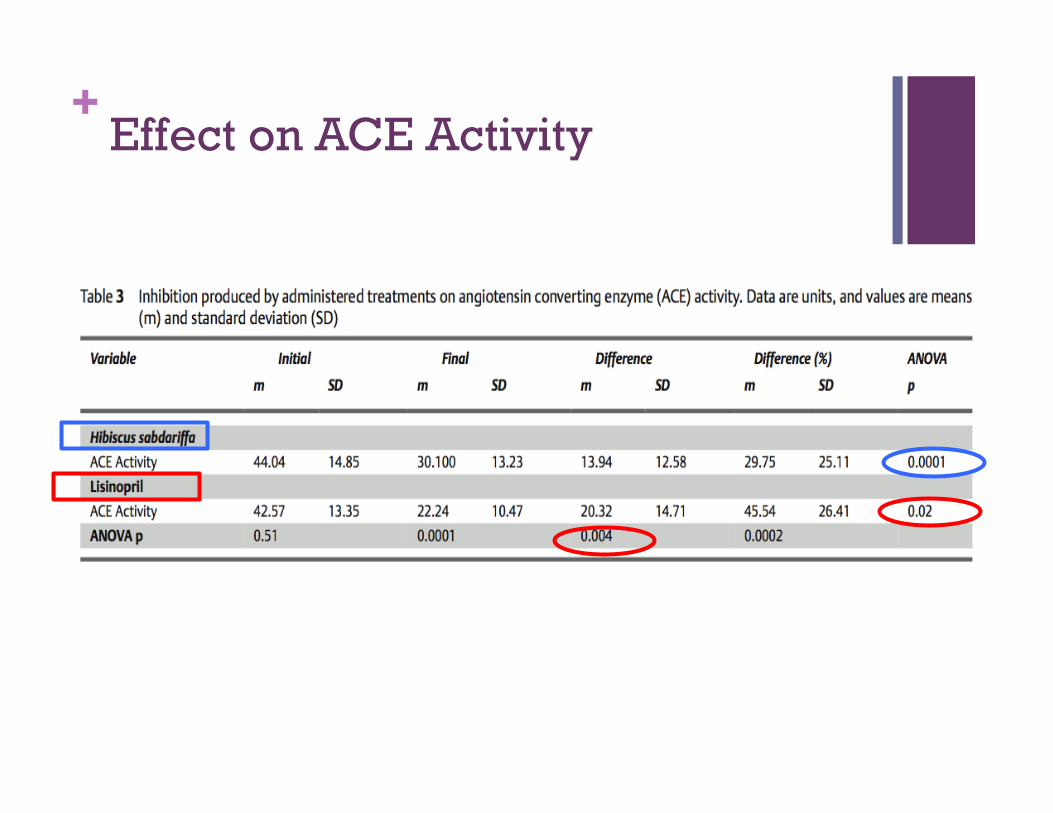
++ Effect on ACE Activity
++ Summary
The data showed that Hibiscus was effective, tolerable, and safe means to reduce blood pressure
Unlike many diuretics, hibiscus does not modify serum potassium levels
While Hibiscus was effective, Lisiprol was more effective at reducing blood pressure in Stage 1 & 2 hypertensive adults
+ 51
Okechukwu O. Ndu, Chukwuemeka S. Nworu, Chinwendu O. Ehiemere, Nichola C. Ndukwe, and Izuchukwu S. Ochiogu
Herb–Drug Interac1on Between the Extract of Hibiscus sabdariffa L.
and Hydrochlorothiazide in Experimental Animals.
++ Purpose of Study
To examine the possibility of herb-drug interaction with concomitant use of Hibsicus sabdariffa (HSE) and hydroclorothiazide (HCT), a diuretic.
Investigate any potential dangers and consequences of concomitant HSE and HCT usage
++ Research Question & Hypothesis
Question: Will concomitant use of Hibiscus sabdariffa alter the pharmacologic effects of HCT?
Hypothesis: Given Hibiscus sabdariffa’s antihypertensive properties, concomitant administration will alter HCT’s pharmacologic effect
++ Study Design
Two Phases Phase 1: Determination of the toxic range Phase 2: Co-administration of HSE and HCT and
effect in diuresis & effect of HSE on Pharmacokinetics and Pharmacodynamics of HCT
Materials and Methods: Plant Material Drug Animals
++ Study Design --Phase 1--
Group 1 1,600 mg/kg
Group 2 2,900 mg/kg
Group 3 3,600 mg/kg
Group 4 5,000 mg/kg
Acute Toxicity Test of Extract
**LD50= >5,000 mg/kg
++ Study Design --Phase 2--
Effect of Co-Administration of HSE and HCT on Diuresis
Group 1
Group 3
Group II
Group 4
Group 5
HCT (10 mg/kg)
Distilled water
HSE (40mg/kg)
HCT(10mg/kg)+ HSE (40 mg/kg)
HCT (10 mg/kg) + Distilled Water
++
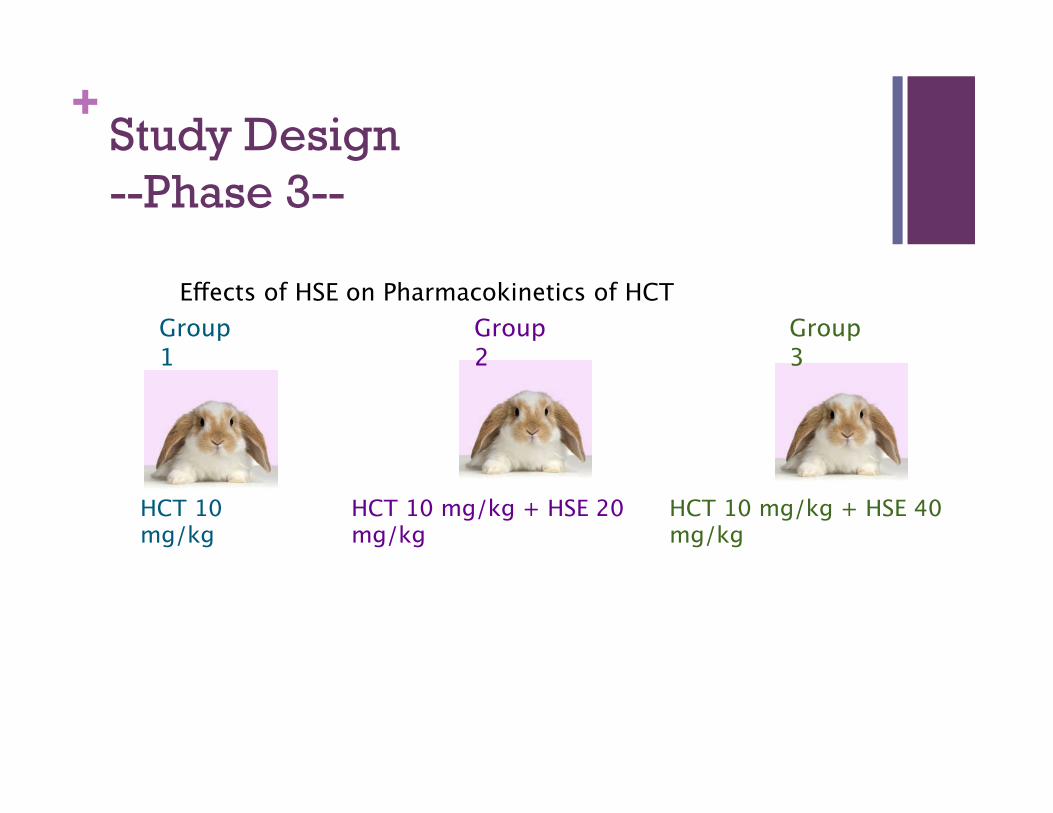
Effects of HSE on Pharmacokinetics of HCT Group 3
Group 2
Group 1
HCT 10 mg/kg
HCT 10 mg/kg + HSE 20 mg/kg
HCT 10 mg/kg + HSE 40 mg/kg
Study Design --Phase 3--
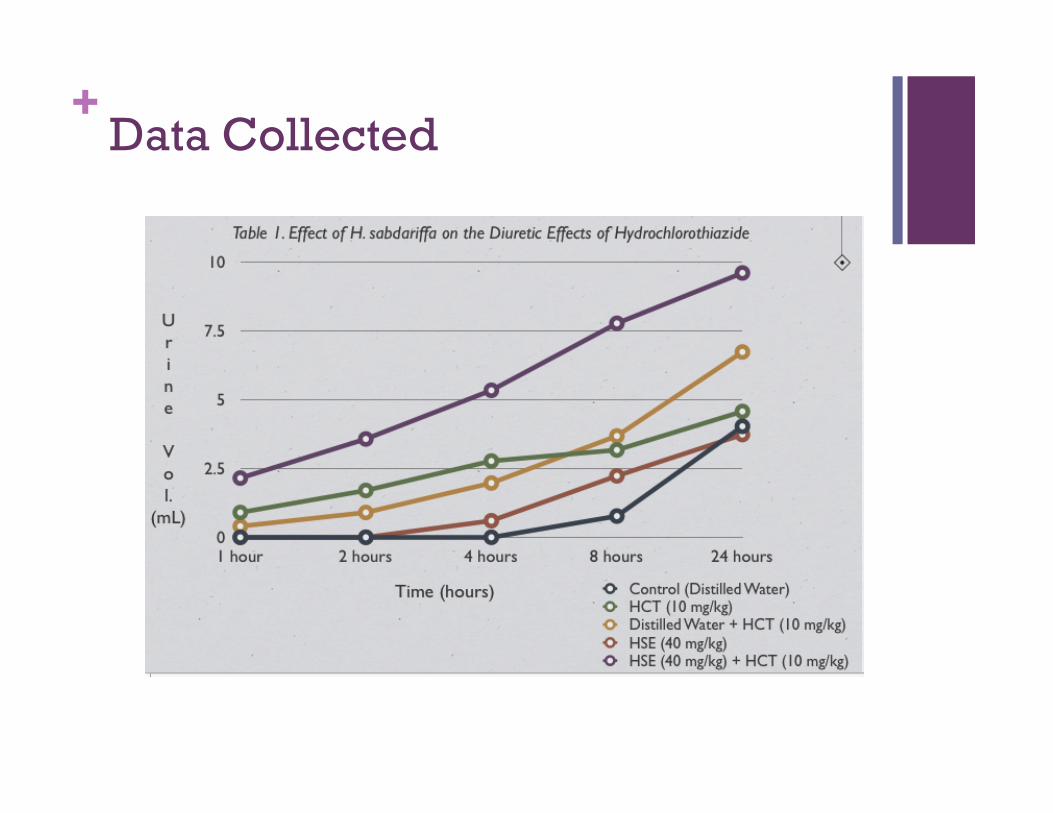
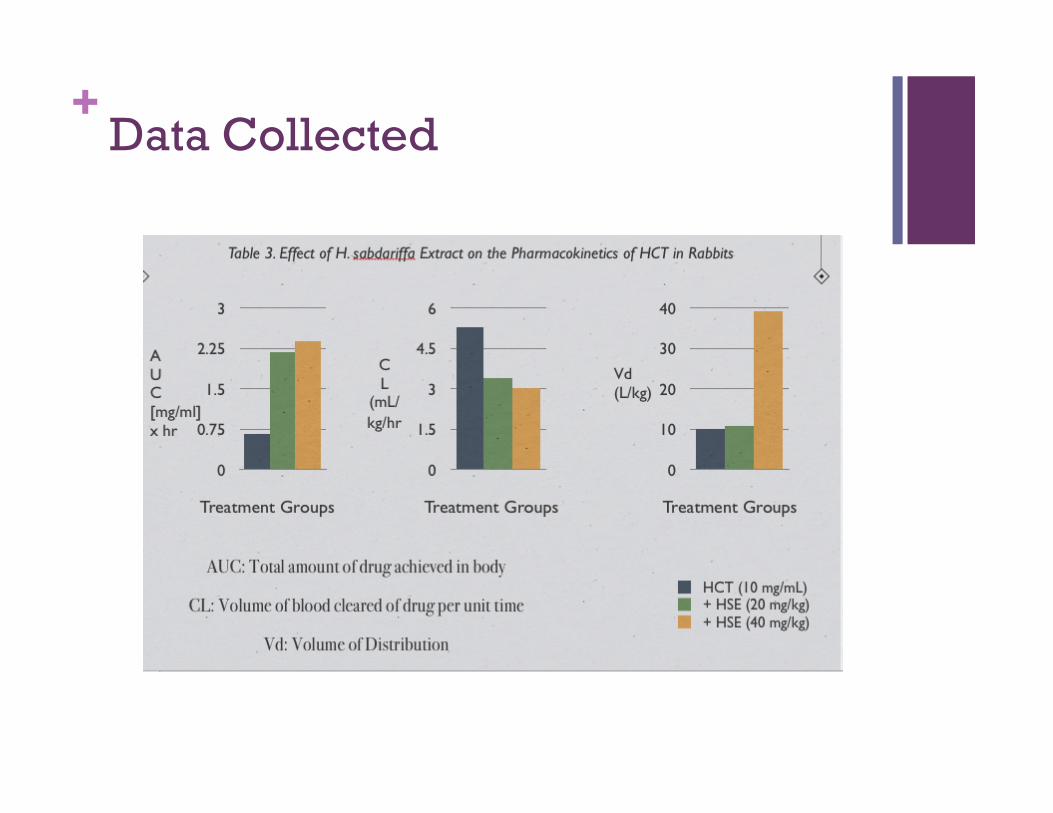
++ Data Collected
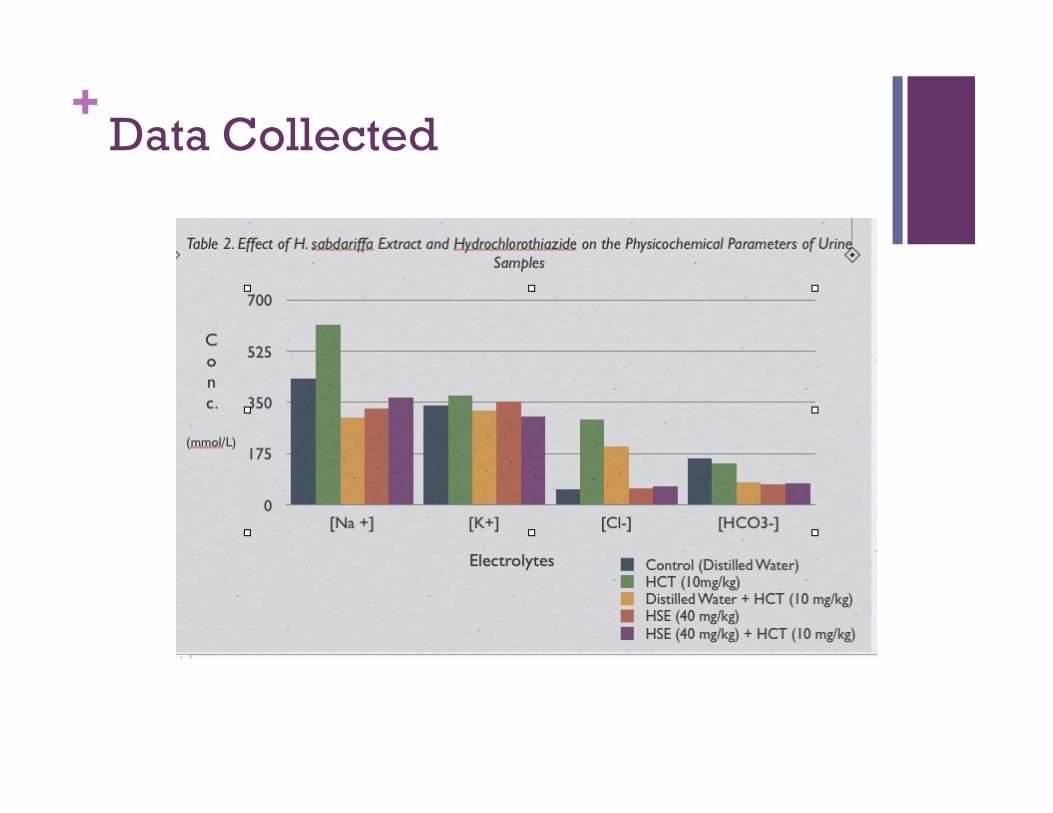
++ Data Collected
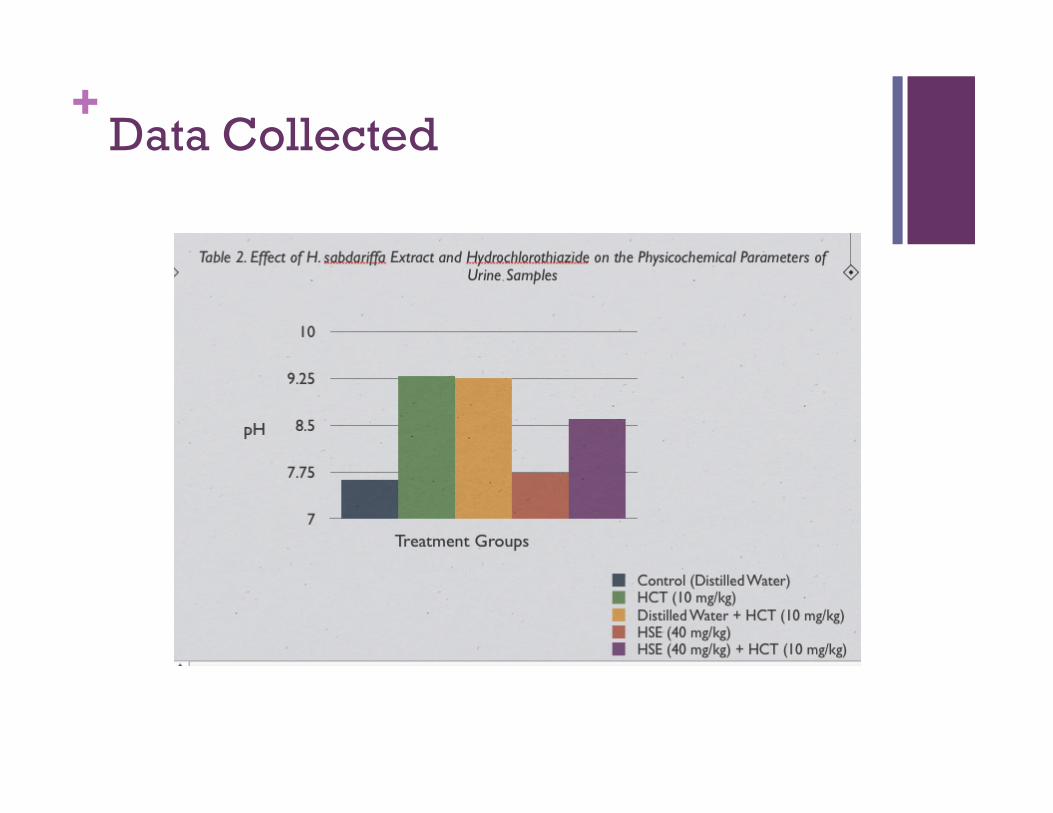
++ Data Collected
++ Data Collected
++ Results
Physiochemical Effect on Urine Administration of HSE alone Did not cause increase in urinary excretion of
Na +, Cl-, and HCO3- Decreased chance of dilutional hyponatremia
Co-adminstration of HSE and HCT Decrease in urinary pH, Na+, HCO3-, Cl-
concentrations Possibility of metabolic acidosis with
prolonged use
++ Results
Pharmacokinetic Effects:
HCT + HSE Decreased CL (volume of blood cleared of drug per unit
time) Increased AUC (total amount of drug achieved in body
Maximum AUC obtained when administered 40 mg/kg HSE
What does this mean? Co-administration possibly increases retention of HCT
elimination from the body Less HCT will be cleared from the body with increasing
dose of co-administered HSE HSE slows rate HCT is eliminated from the body
++ Summary
HSE significantly altered both pharmacodynamics and pharmacokinetic indices of HCT Increased diuretic effect Decreased pH, HCO3-, Cl- in urine Increased retention in the body
HSE is reasonably safe without evidence of acute toxicities.
Concomitant usage of H. sabdariffa and HCT diuretics in the management of hypertension should be avoided!
++ Recap of the Studies
Herbal hibiscus tea containing 21 mg anthocyanins consumed daily reduced SBP by 5.6% from baseline in pre-mildly hypertensive adults. MAP was reduced by 4.7% and DBP was reduced 3.9%.
Hibiscus supplement containing 9.6 mg anthocyanins taken daily reduced SBP by 11% and DBP by 12.4% in mild to moderate hypertensive adults.
Hibiscus supplement containing 250 mg anthocyanins taken daily in mild to moderately hypertensive adults, reduced SBP by 11.7%, and DBP by 12.2%.
Co-administration of HSE (40mg/kg) and HCT resulted in increased diuretic effect, decrease in pH, and electrolytes in urine.
++ Risk reduction analysis
5 mm Hg reduction in SBP 14% overall reduction in mortality due to stroke 9% reduction in mortality due to coronary heart
disease 7% reduction in all cause mortality
3mm Hg reduction in SBP 8% overall reduction of mortality due to stroke 5% overall reduction in mortality due to CHD
++ Conclusion
Daily consumption of hibiscus, both in the form of a tea and a capsule dissolved in water, can be an effective lifestyle intervention to reduce blood pressure in pre-moderately hypertensive adults.
Mechanism of action include function as an ACE inhibitor, K-sparing diuretic, and a vasorelaxant.
The level of blood pressure lowering effects of hibiscus are similar to those reported for studies using the DASH intervention and certain medications.
Consuming hibiscus tea can be considered a safe and effective lifestyle change to reduce risks associated with HTN.
++ Concerns/ Cautions
Caution with diuretic medications
Avoid if allergic or hypersensitive to hibiscus, or members of the Malvaceae family
Hibiscus rosa-sinensis has exhibited infertility activity.
Use cautiously if pregnant, trying to become pregnant or breastfeeding
Natural Standard: The authority on integrative medicine (2012). Hypertension.
++ References Mahan, L.K. & Stump, S. (2008) Krause’s food & nutrition therapy. (12th ed.) St. Louis, MO.: Saunders/
Elsevier.
McKay, D., Chen, C. Saltzman, E., Blumberg, J., Hibiscus sabdariffa L. tea (tisane) lowers blood pressure in prehypertensive and mildly hypertensive adults. The Journal of Nutrition. 2010;140(2)298-303.
Natural Standard: The authority on integrative medicine (2012). Hypertension. Retrieved from: http://www.naturalstandard.com.ezproxy.hsclib.sunysb.edudatabases/conditions/
Ndu, O. O., Nworu, C. S., Ehiemere, C. O., Ndukwe, N. C., & Ochiogu, I. S. (2011). Herb–Drug Interaction Between the Extract of Hibiscus sabdariffa L. and Hydrochlorothiazide in Experimental Animals. Journal of medicinal food,14(6), 640-644.
Sear, J., & Dphil, P. F. (2004). Hypertension: pathophysiology and treatment. Continuing education in Anaesthesia, Critical Care, and Pain, 4(3), 71-74.
Herrera-Arellano, A., Miranda-Sánchez, J., Ávila-Castro, P., Herrera-Álvarez, S., Jiménez-Ferrer, J. E., Zamilpa, A., et al. (2007). Clinical Effects Produced by a Standardized Herbal Medicinal Product of Hibiscus sabdariffa on Patients with Hypertension. A Randomized, Double-blind, Lisinopril-Controlled Clinical Trial. Planta Med, 73, 6-12.
Herrera-Arellano, A., & Flores-Romero, S. (2004). Effectiveness and tolerability of a standardized extract from Hibiscus sabdariffa in patients with mild to moderate hypertension: a controlled and randomized clinical trial. Phytomedicine, 11, 375-382.
Ojeda, D., Jiménez-Ferrer, E., Zamilpa, A., Herrera-Arellano, A., Tortoriello, J., & Alvarez, L. (2010). Inhibition of angiotensin converting enzyme (ACE) activity by the anthocyanins delphinidin-and cyanidin-3- O-sambubiosides from Hibiscus sabdariffa.. Journal of ethnopharmacology, 127(1), 7-10.
++ References (Continued)
Sharma, J. N. (2009). Hypertension and the bradykinin system. Current Hypertension Reports , 11(3), 178-181. Retrieved December 9, 2012, from the SpringerLink database.
Hynynen, M. M., & Khalil, R. A. (2006). The Vascular Endothelin System in Hypertension – Recent Patents and Discoveries. Recent Pat Cardiovasc Drug Discov, 1(1), 195-108. Retrieved December 9, 2012, from the PubMed database.
Sodium Ions, Calcium Ions, Arterial Contractility and Ouabain Hypertension. (n.d.). University of Maryland School of Medicine. Retrieved December 9, 2012, from http://medschool.umaryland.edu/blaustein_ppg/overview.asp
Francisco J. Alarcon-Aguilar, Alejandro Zamilpa, Ma. Dolores Perez-Garcia, Julio C. Almanza-Perez, Eunice Romero-Nuñez, Efrain A. Campos-Sepulveda, Laura I. Vazquez-Carrillo, Ruben Roman-Ramos (8 October 2007,). Effect of Hibiscus sabdariffa on obesity in MSG mice. Journal of Ethnopharmacology Volume 114, Issue 1, Pages 66–71
M. Ajay, H.J. Chai, A.M. Mustafa, A.H. Gilani, M.R. Mustafa. (February 2007). Mechanisms of the anti-hypertensive effect of Hibiscus sabdariffa L. calyces. Journal of Ethnopharmacology, Volume 109, Issue 3, 12 Pages 388–393,
Beevers, G., Lip, G., & O'Brien, E. (2001). ABC of Hypertension- The pathophysiology of hypertension . British Medical Journal, 322(7291), 912-916.