high altitude, hypoxia and the physiology of adaptation - …€¢ also critical for the maintenance...
TRANSCRIPT

High altitude, hypoxia and the physiology of adaptation
David Polaner, MD, FAAPProfessor of Anesthesiology and PediatricsUniversity of Colorado School of Medicine
Children’s Hospital ColoradoUniversity of Colorado Altitude Research Center
disclosures
none
objectives
• understand the acute physiological changes that areprecipitated by ascent to high altitude
• appreciate the adaptations that occur with acuteascent to altitude
• gain an introduction to altitude related illnesses andtheir prophylaxis and treatments

“We live submerged at the bottom of an ocean of the element air, which by un- questioned experiments is known to have weight.”
Evangelista Torricelli (1608–1647)
why study high altitude physiology?
• large numbers of people live or recreate at altitude
• many of the adaptive (or maladaptive) mechanisms are applicable to various disease states, especially those that are manifest by hypoxia
• understanding the basic physiology can lead to better understanding and therapies of disorders characterized by hypoxic conditions

physical conditions at altitude
as altitude increases:
• barometric pressure falls
• PAO2 falls with lower PB
• partial pressure of water vapor in the lung assumes agreater proportion of alveolar pressure
• temperature falls (~6 - 9oC per 1000m)
• UV exposure increases
• humidity decreases

Pb, PO2, PaO2 and altitude
from West JB. The physiologic basis of high-altitude diseases. Annals of Internal Medicine 2004.
acute adaptive effects of ascent
• increased carotid body discharge acceleratesrespiratory rate
• most important of the early mechanisms ofacclimatization
• also critical for the maintenance of adequate PaO2 at
extreme altitude
• increased Vm
• why does this help?
acute adaptive effects of ascent
• total pressure in the alveolus is the sum of thepartial pressures of CO2, O2, N2, and water vapor
PaO2 = PB - (PaCO2 + PN2 + PH2O)
• Only the PaCO2 can be reduced by altering
respiratory rate, therefore (assuming R=1):
PaO2 = PIO2 - PaCO2

acute adaptive effects of ascent
from Young AJ, Reeves JT. Human adaptation to high terrestrial altitude. in Medical Aspects of Harsh Environments 2002.

acute effects of ascent to altitude
• heart rate (and cardiacoutput) increases
• however, maximal heartrate decreases (? fromincreased parasympatheticdrive?)
• as high altitude diuresisensues resulting inhemoconcentration, restingheart rate falls
acute effects of ascent to altitude
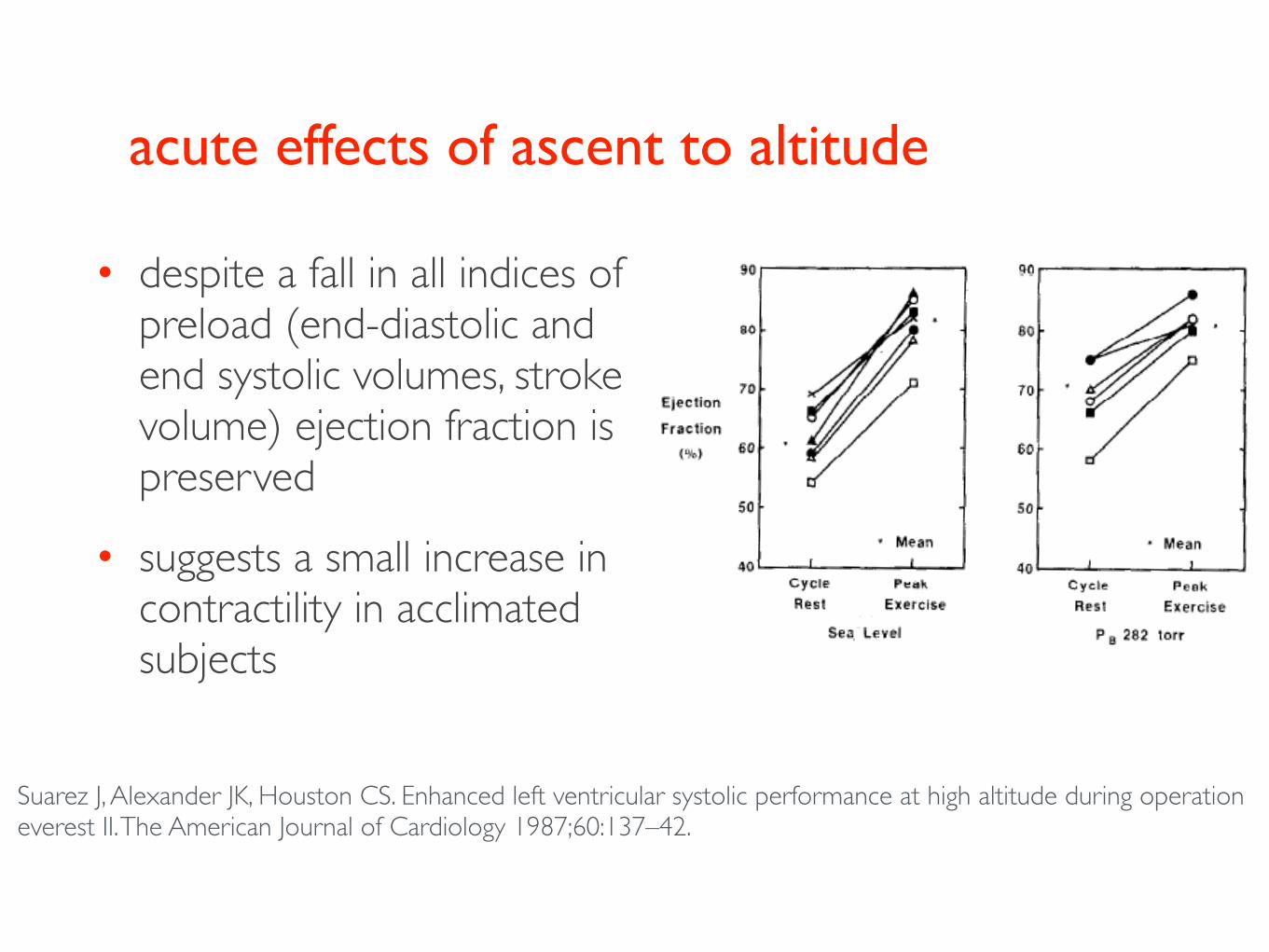
• despite a fall in all indices ofpreload (end-diastolic andend systolic volumes, strokevolume) ejection fraction ispreserved
• suggests a small increase incontractility in acclimatedsubjects
Suarez J, Alexander JK, Houston CS. Enhanced left ventricular systolic performance at high altitude during operation everest II. The American Journal of Cardiology 1987;60:137–42.

circulatory adaptation to altitude
• diuresis begins within 3-6 hours of ascent
• decreased plasma volume with maintained RCM =>hemoconcentration
• 2,3 DPG increases (48h-3 weeks after ascent)resulting in increased Hb O2 affinity
• EPO secretion is increased (but subject to highindividual variability)- response takes 3+ weeks

adaptation to altitude: hemoglobin
from Storz, et al. High Alt Med Biol. 2008 Jun; 9(2): 148–157.

maladaptation to altitude: high altitude illness
general principals
• although there are those who are genetically moresusceptible and those who are genetically resistant tohigh altitude illness, anyone will get sick if they gohigh enough fast enough
• the best treatment, when possible, for any highaltitude illness is DESCENT

when descent is impossible• pharmacotherapy (steroids, beta agonists, vasodilators, NO
analogs)
• oxygen
• Gamow bag

acute mountain sickness (AMS)
• may affect at least 25% of lowlanders ascendingrapidly >2500m
• diagnosed by symptoms (Lake Louise score):headache plus
• lightheadedness• breathlessness• fatigue• insomnia• anorexia• nausea

acute mountain sickness (AMS)
• usually self limited (3-4 days)
• etiology may be mild cerebral edema
• hypoxia upregulates the expression of neuropeptide corticotrophin releasing factor, which activates the water channel aquaporin-4 and facilitates water (from CSF) influx into glial cells
• less common > age 50
• those who are more hypoxic at altitude may be more susceptible (Roach RC, et al. Aviat Space Environ Med 1998;69:1182–5.)

acute mountain sickness (AMS)
• Cheyes-Stokes respiration and periodic breathing arecommon
• unclear mechanism:
• hypoxia induced instability of central ventilatorydrive
• hypocarbia/ hypercarbia• hypoxia-induced arousal
• best treated with acetazolamide, NOT sedatives orsleep agents
acute mountain sickness: prevention & treatment
• slow ascent!
• acetazolamide(Diamox) - 125mgBID
• dexamethasone -2mg QID

HPV and pulmonary arteriolar hypertension
• HPV response to acutehypoxia varies amongindividuals
• those with the briskestresponse, most dramaticelevation in PAP and mostheterogeneity are most at riskfor acute PAH with ascent
• in severe cases R heartfailure can develop Grunig E, Mereles D, Hildebrandt W,
Swenson ER, et al. (2000). J Am Coll Cardiol. 35:980–987.

High Altitude Pulmonary Edema (HAPE)
• presents with dyspnea, cough,low grade fever, progressing tofrank pulmonary edema
• usually presents within 2-3days of ascent >2500m
• exacerbated by rapid ascentcoupled with exertion
• susceptible individuals haveabnormally brisk elevations inPAP in response to hypoxia
• elevated PAP > wall stress inpulmonary capillaries andultrastructural damage

High Altitude Pulmonary Edema (HAPE)
• central - basilar infiltrates on CXR,usually worse on the left
• caused by HPV that is out ofproportion to the hypoxic stimulus& is unevenly distributed
• high pulmonary capillary pressuresresult in exudate, inflammatoryresponse and lung injury
• treatment with PEEP, vasodilators(nifedipine), steroids, ᵝ2 agonists (salbutemol), iNO or sildinafil have been effective

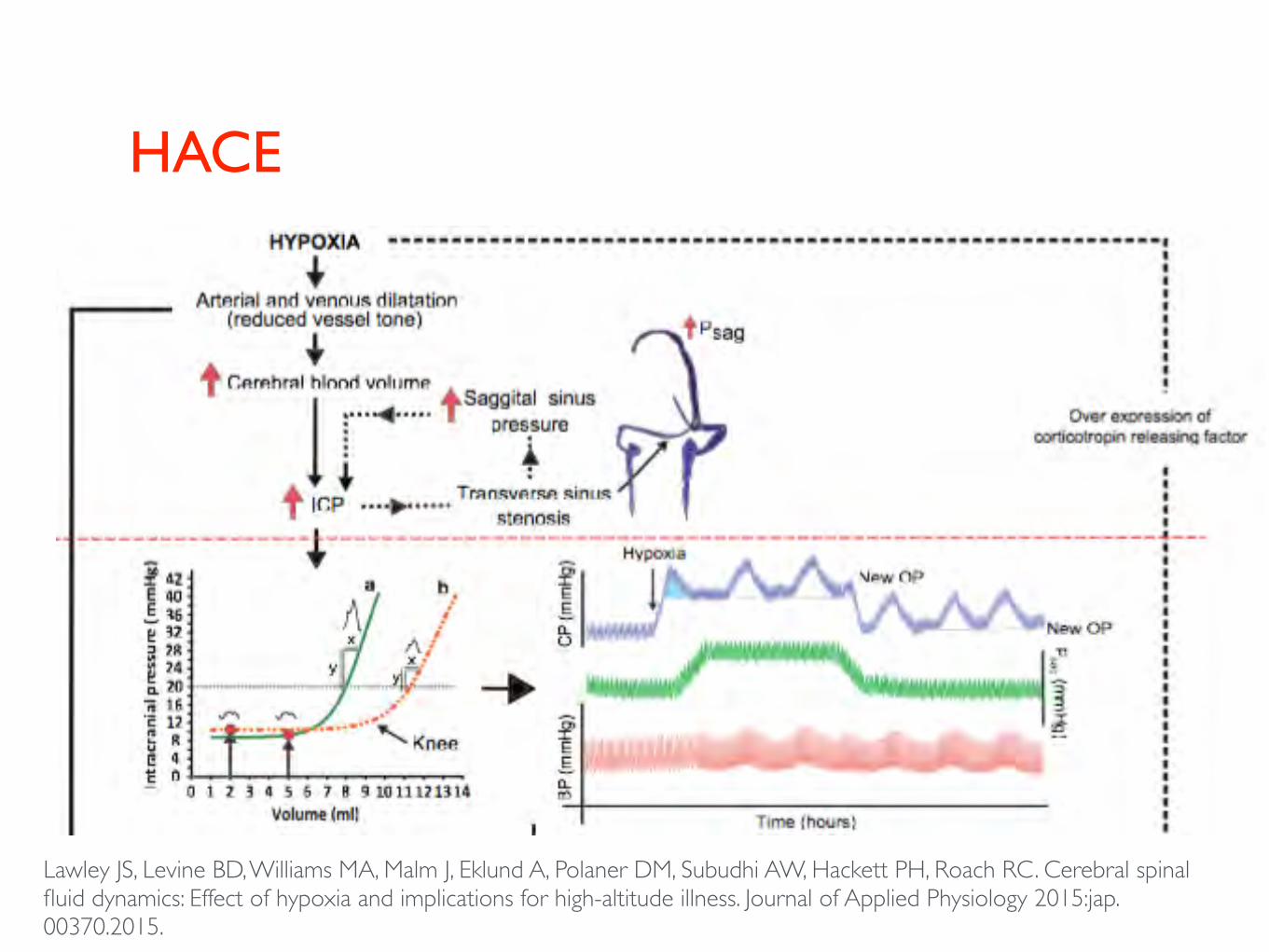
High Altitude Cerebral Edema (HACE)

HACE• inability to compensate for elevation in ICP
• greater compliance-• translocation• “tight fit”
• vasogenic cerebral edema withbreakdown of blood brain barrier,extravasation
• presents with ataxia, confusion,depressed consciousness, papilledema, hemiparesis, coma
• descent, O2, steroids mandatory
HACE
Lawley JS, Levine BD, Williams MA, Malm J, Eklund A, Polaner DM, Subudhi AW, Hackett PH, Roach RC. Cerebral spinal fluid dynamics: Effect of hypoxia and implications for high-altitude illness. Journal of Applied Physiology 2015:jap.00370.2015.

conclusions
• hypoxia from ascent to altitude mandates a multitudeof physiologic adaptations that permit humans tosurvive under conditions that would otherwise beimpossible
• maladaptation, whether due to genetics or exceedingthe ability of the system to compensate, can lead toserious and life-threatening illness
• successful adaptation requires understandingphysiology & the limits of the organism, andoccasional intervention with pharmacotherapy

selected references: anesthesia and altitude
Leissner KB, Mahmood FU. Physiology and pathophysiology at high altitude: considerations for the anesthesiologist. J Anesth 2009;23:543–53.
Rabbitts JA, Groenewald CB, Dietz NM, Morales C, Räsänen J. Perioperative opioid requirements are decreased in hypoxic children living at altitude. Pediatric Anesthesia 2010;20:1078–83.
Firth PG, Pattinson KTS. Anaesthesia and high altitude: a history. Anaesthesia 2008;63:662–70.
Moser B, Röggla G. Emergency anaesthesia at high altitude. Anaesthesia 2008;63:101.
Lawley JS, Levine BD, Williams MA, Malm J, Eklund A, Polaner DM, Subudhi AW, Hackett PH, Roach RC. Cerebral spinal fluid dynamics: Effect of hypoxia and implications for high-altitude illness. Journal of Applied Physiology 2015:jap.00370.2015.
Fan J-L, Subudhi A, Evero O, Bourdillon N, Kayser B, Julian C, Panerai R, Lovering A, Roach R. AltitudeOmics: the effect of high altitude ascent and acclimatisation on cerebral blood flow regulation (885.1). FASEB J 2014;28:885.1.

selected references: acute mountain sickness and high altitude illnesses
Hackett PH, Roach RC. High-Altitude Illness. N Engl J Med 2001;345:107–14.
Schoene RB. Illnesses at High Altitude. Chest 2007;134:402–16.
Roach RC, Hackett PH. Frontiers of hypoxia research: acute mountain sickness. Journal of Experimental Biology 2001;204:3161–70.
Bloch J, Duplain H, Rimoldi SF, Stuber T, Kriemler S, Allemann Y, Sartori C, Scherrer U. Prevalence and Time Course of Acute Mountain Sickness in Older Children andAdolescents After Rapid Ascent to 3450 Meters. PEDIATRICS 2009;123:1–5.
Swenson ER. Pharmacology of Acute Mountain Sickness: Old Drugs and Newer Thinking. Journal of Applied Physiology 2015:jap.00443.2015.
van Patot MCT, Leadbetter G III, Keyes LE, Maakestad KM, Olson S, Hackett PH. Prophylactic Low-Dose Acetazolamide Reduces the Incidence and Severity of Acute Mountain Sickness. High Altitude Medicine & Biology 2008;9:289–93.
Swenson ER, Teppema LJ. Prevention of acute mountain sickness by acetazolamide: as yet an unfinished story. Journal of Applied Physiology 2006;102:1305–7.

selected references: altitude physiology
West JB. The physiologic basis of high-altitude diseases. Annals of Internal Medicine 2004;141:789-800.
Swenson ER. Hypoxic pulmonary vasoconstriction. High Altitude Medicine & Biology 2013;14:101–10.
Fan J-L, Subudhi A, Evero O, Bourdillon N, Kayser B, Julian C, Panerai R, Lovering A, Roach R. AltitudeOmics: the effect of high altitude ascent and acclimatisation on cerebral blood flow regulation (885.1). FASEB J 2014;28:885.1.
Julian CG, Subudhi AW, Hill RC, Wilson MJ, Dimmen AC, Hansen KC, Roach RC. Exploratory proteomic analysis of hypobaric hypoxia and acute mountain sickness in humans. Journal of Applied Physiology 2014;116:937–44.
Subudhi AW, Fan J-L, Evero O, Bourdillon N, Kayser B, Julian CG, Lovering AT, Panerai RB, Roach RC. AltitudeOmics: cerebral autoregulation during ascent, acclimatization, and re-exposure to high altitude and its relation with acute mountain sickness. Journal of Applied Physiology 2014;116:724–9.
Sharma M, Singh SB, Sarkar S. Genome wide expression analysis suggests perturbation of vascular homeostasis during high altitude pulmonary edema. West J, ed. PLoS ONE 2014;9:e85902.
Wilson MJ, Julian CG, Roach RC. Genomic analysis of high altitude adaptation: innovations and implications. Curr Sports Med Rep 2011;10:59–61.
Laurie SS, Yang X, Elliott JE, Beasley KM, Lovering AT. Hypoxia-induced intrapulmonary arteriovenous shunting at rest in healthy humans. Journal of Applied Physiology 2010;109:1072–9.
Wilson MH, Milledge J. Direct Measurement Of Intracranial Pressure At High Altitude And Correlation Of Ventricular Size With Acute Mountain Sickness. Neurosurgery 2008;63:970–5.