hip and pelvis radt 1512 - weber state universityradpacs.weber.edu/images/t_rigby/radt 1512/1512 ppt...
TRANSCRIPT
Hip and Pelvis RADT 1512
Tiera Rigby MS, RT(R)(MR) Additional slides provided by Weber Faculty
1
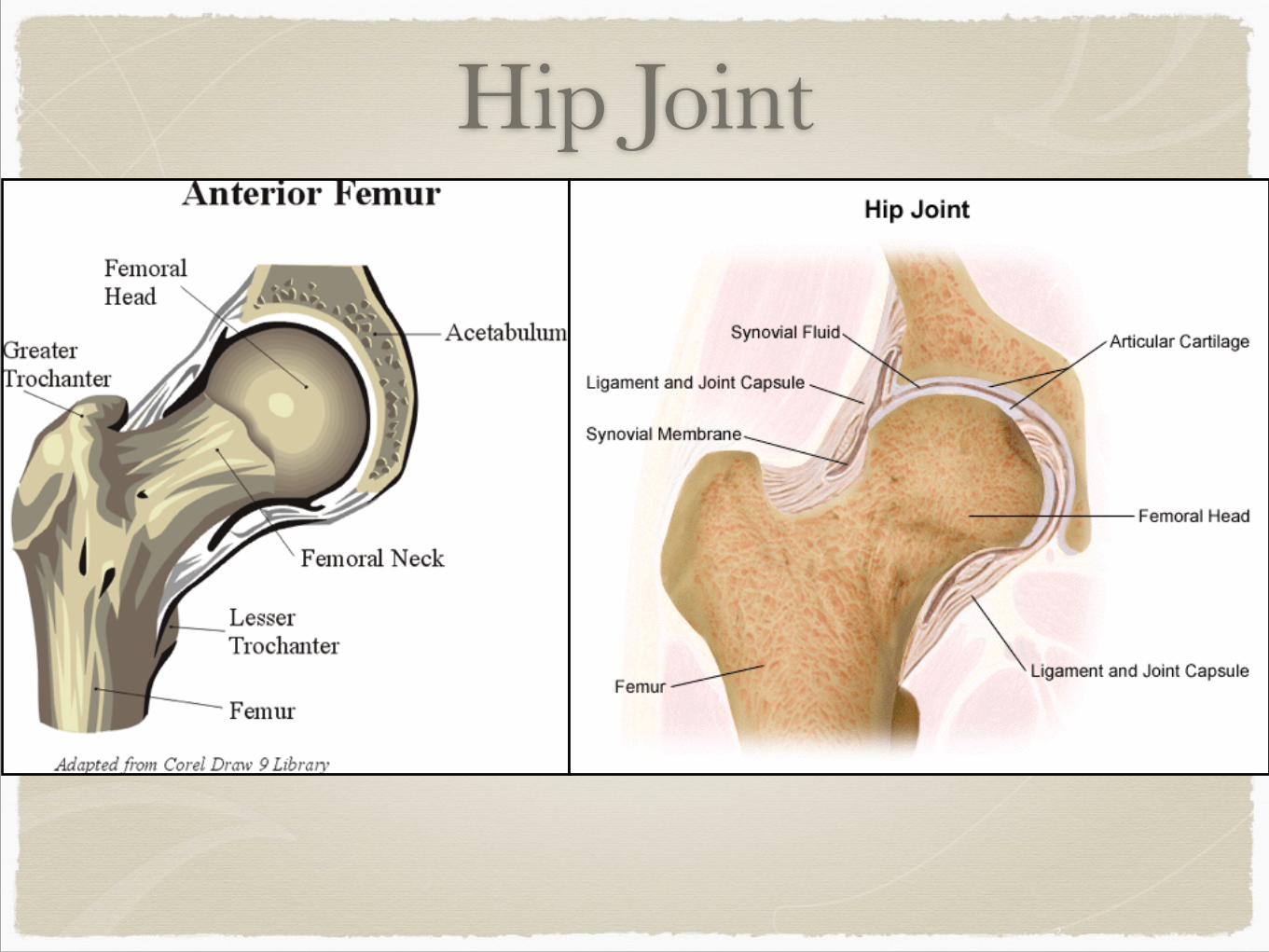
Hip Joint
2
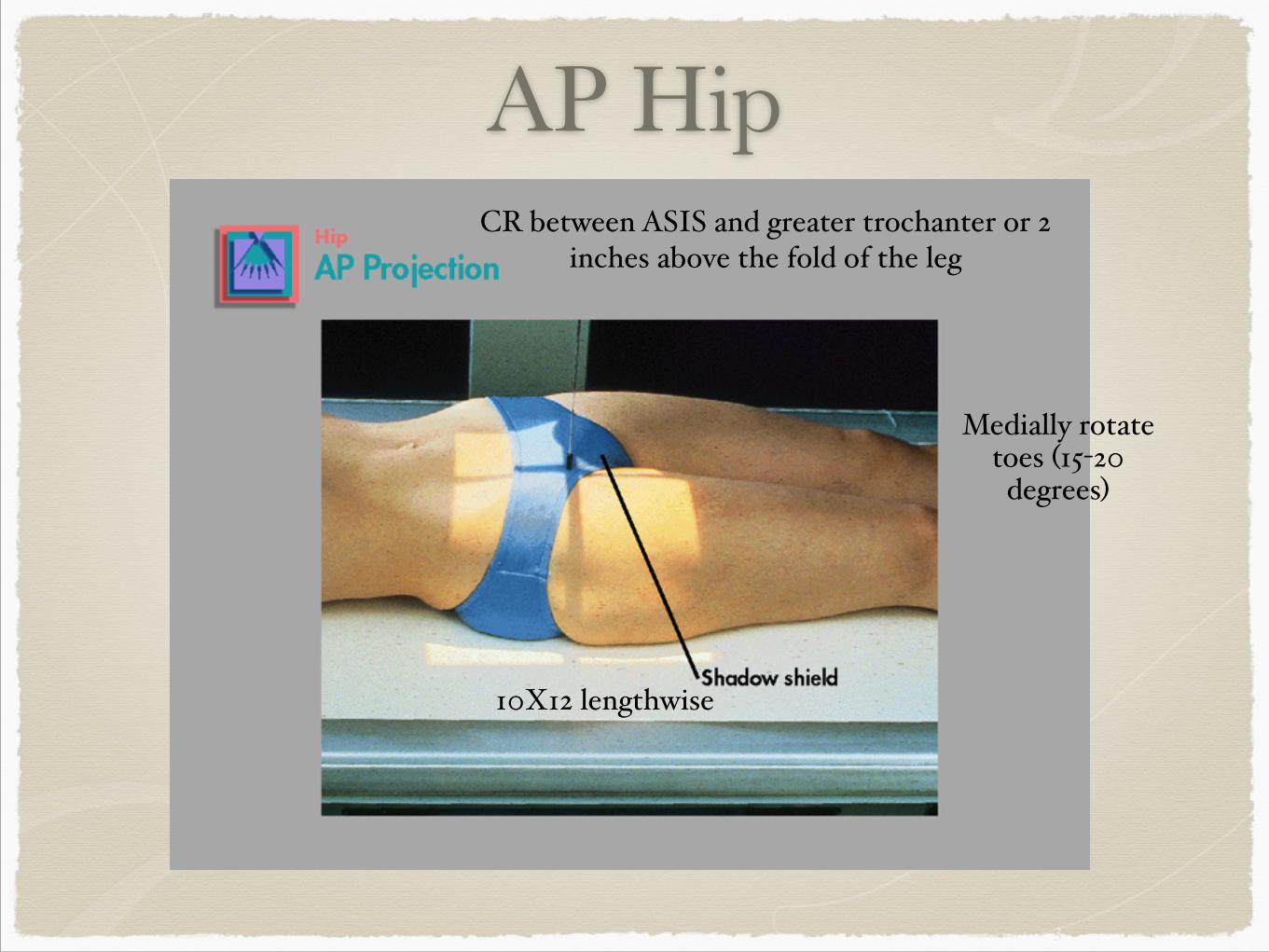
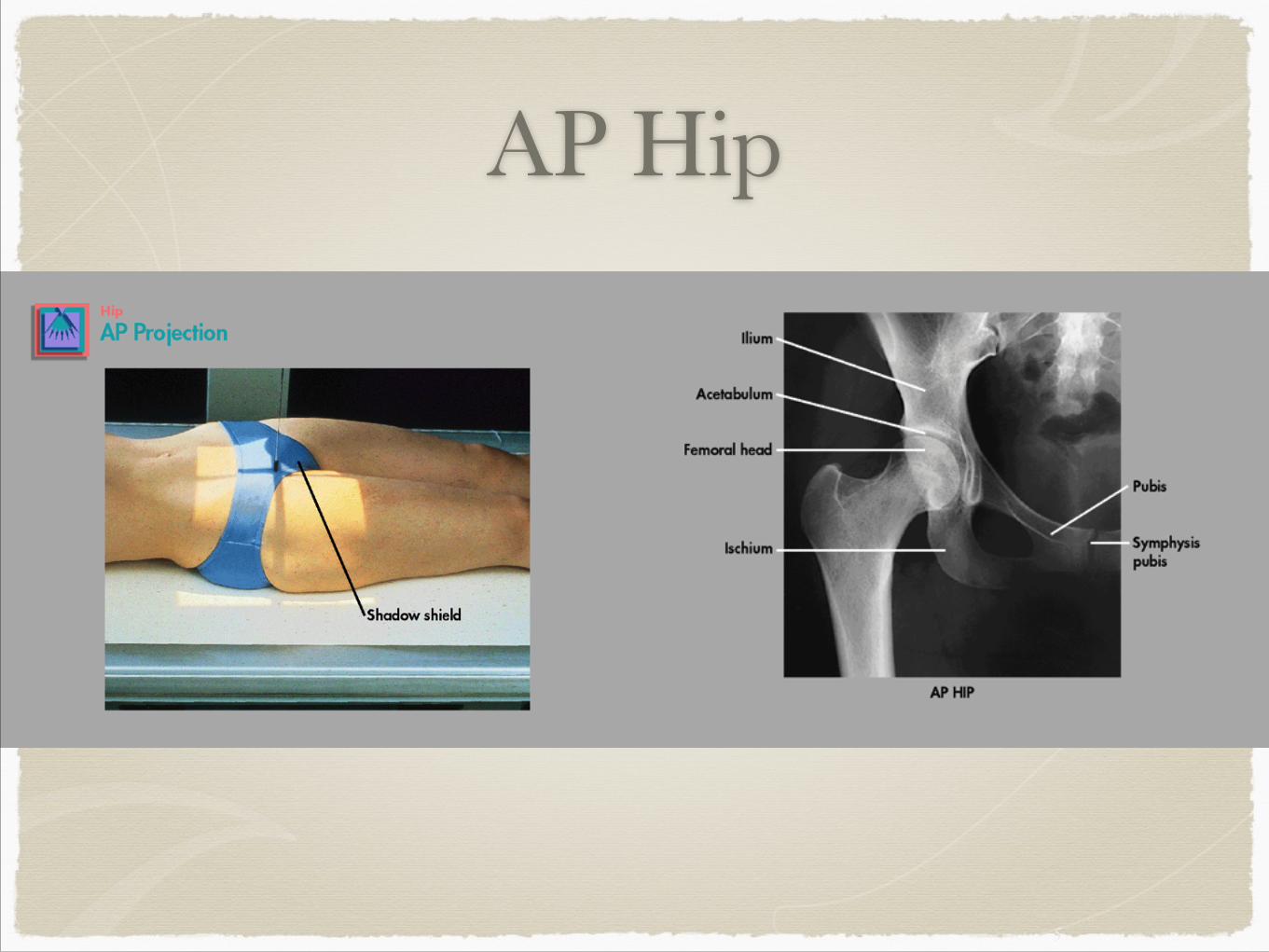
AP Hip
3
10X12 lengthwise
Medially rotate toes (15-20 degrees)$
CR between ASIS and greater trochanter or 2 inches above the fold of the leg
4
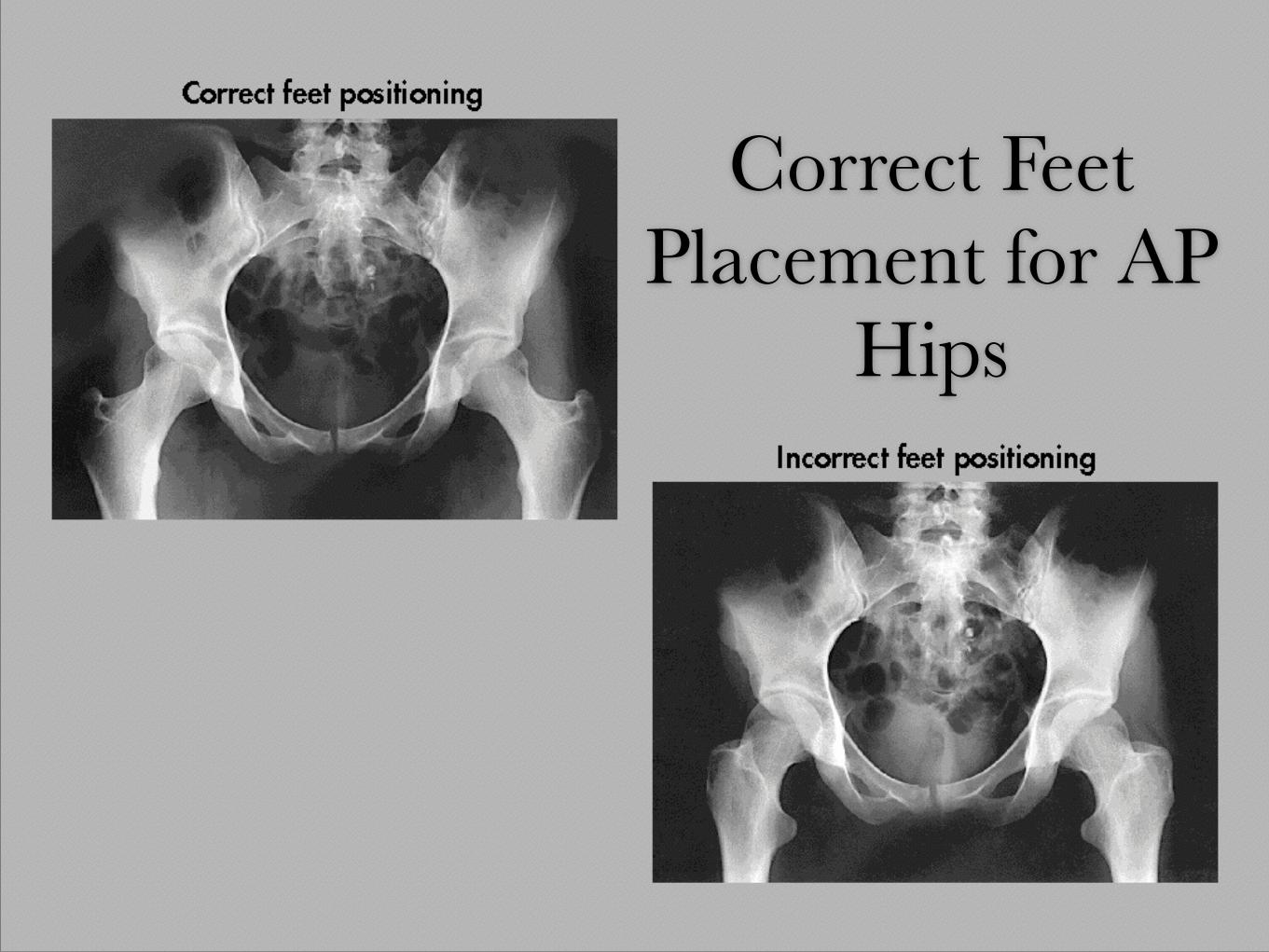
Correct Feet Placement for AP
Hips
AP Hip
5
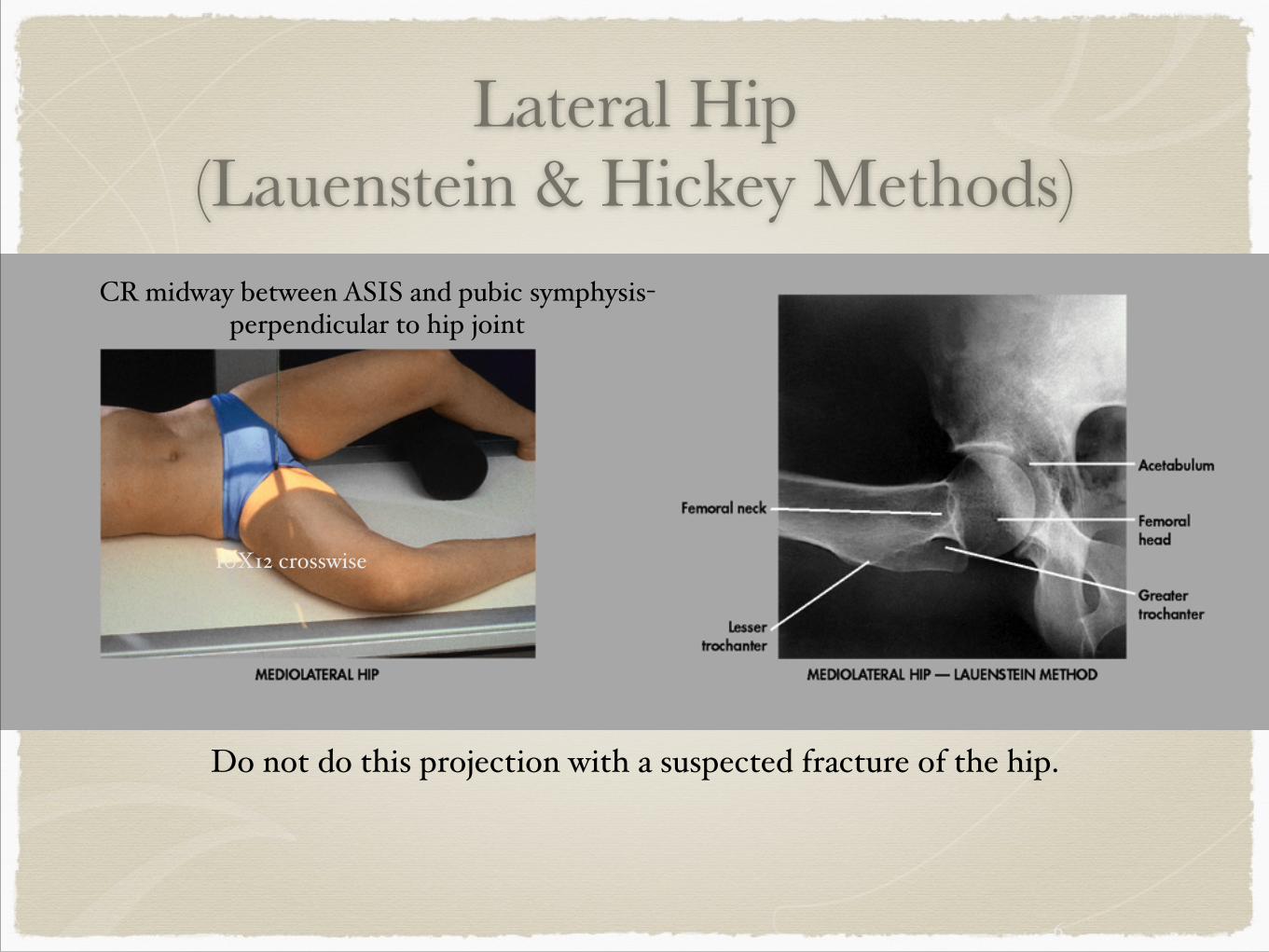
Lateral Hip (Lauenstein & Hickey Methods)
6
Do not do this projection with a suspected fracture of the hip.
10X12 crosswise
CR midway between ASIS and pubic symphysis-perpendicular to hip joint
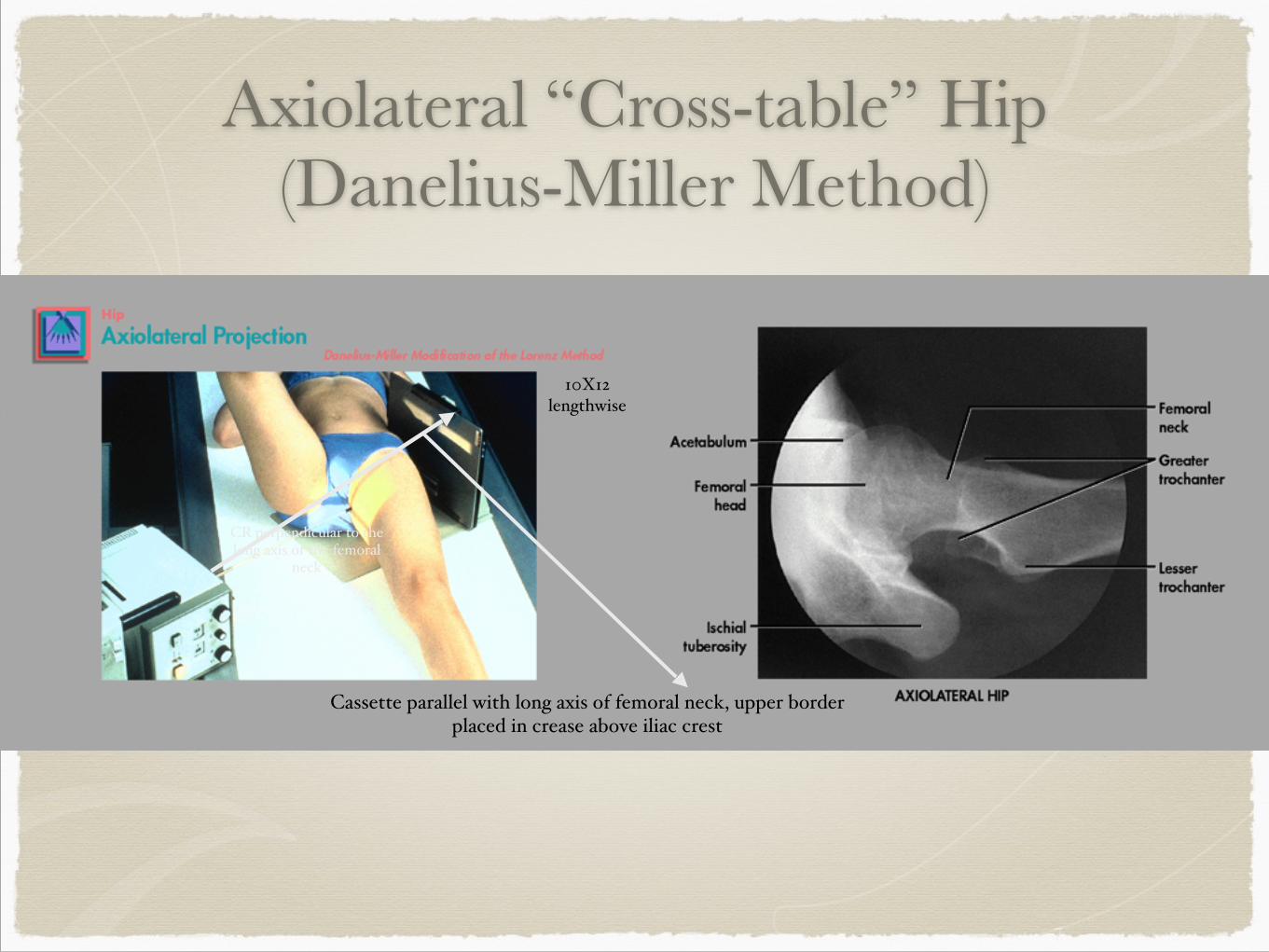
Axiolateral “Cross-table” Hip (Danelius-Miller Method)
7
Cassette parallel with long axis of femoral neck, upper border placed in crease above iliac crest
CR perpendicular to the long axis of the femoral
neck
10X12 lengthwise
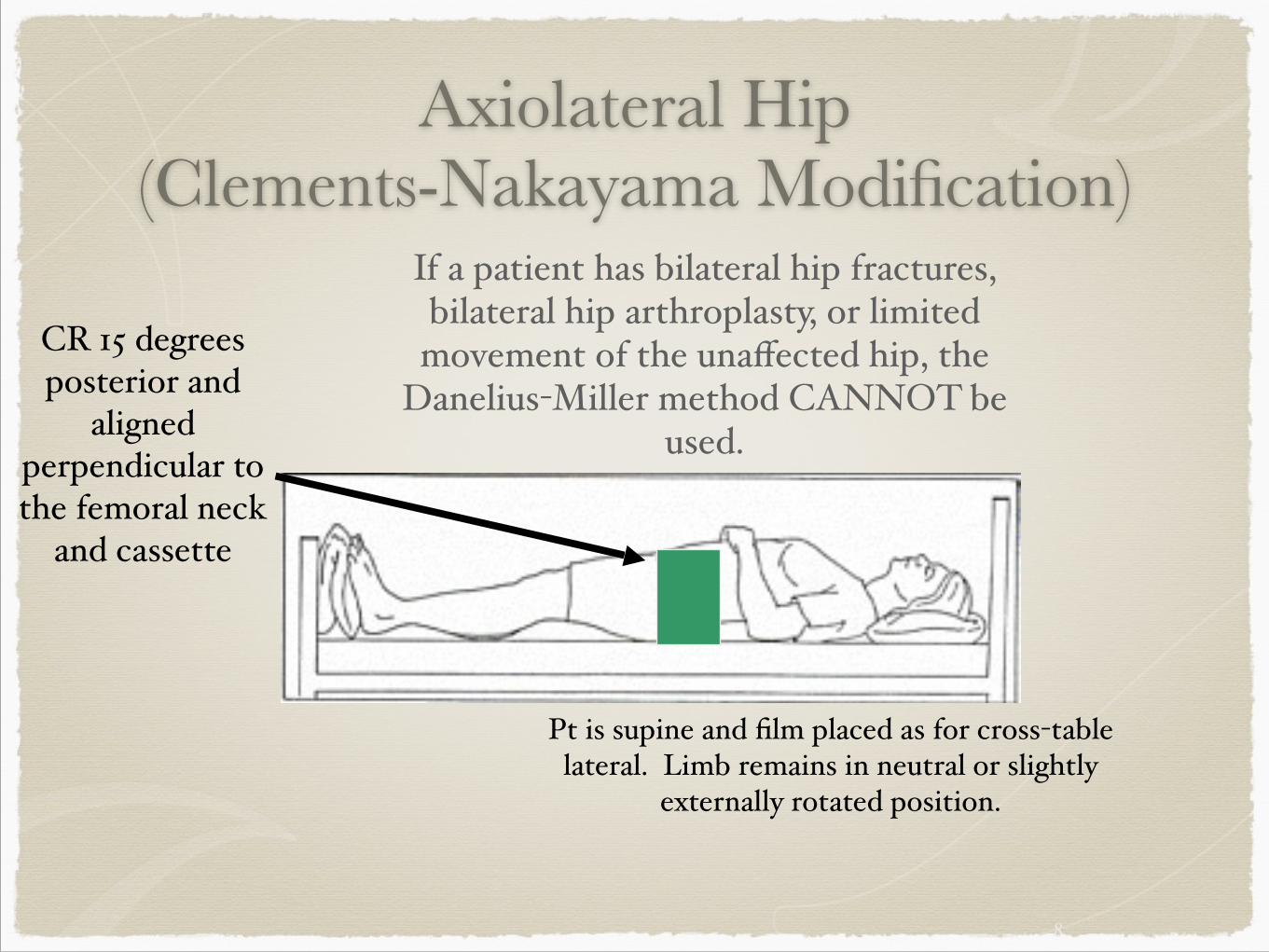
Axiolateral Hip (Clements-Nakayama Modification)
$ If a patient has bilateral hip fractures, bilateral hip arthroplasty, or limited movement of the unaffected hip, the
Danelius-Miller method CANNOT be used.
8
Pt is supine and film placed as for cross-table lateral. Limb remains in neutral or slightly
externally rotated position.
CR 15 degrees posterior and
aligned perpendicular to the femoral neck
and cassette
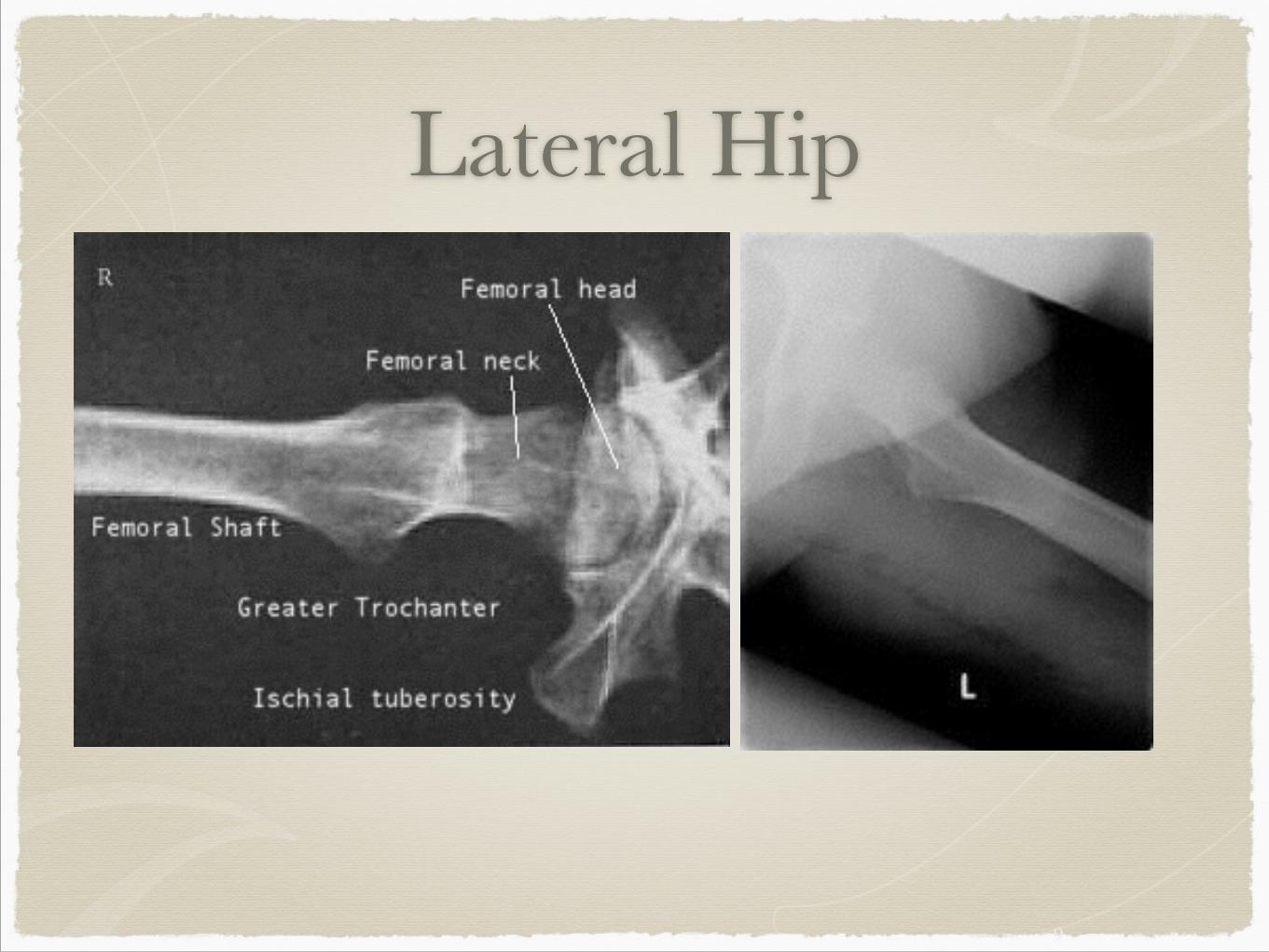
Lateral Hip
9
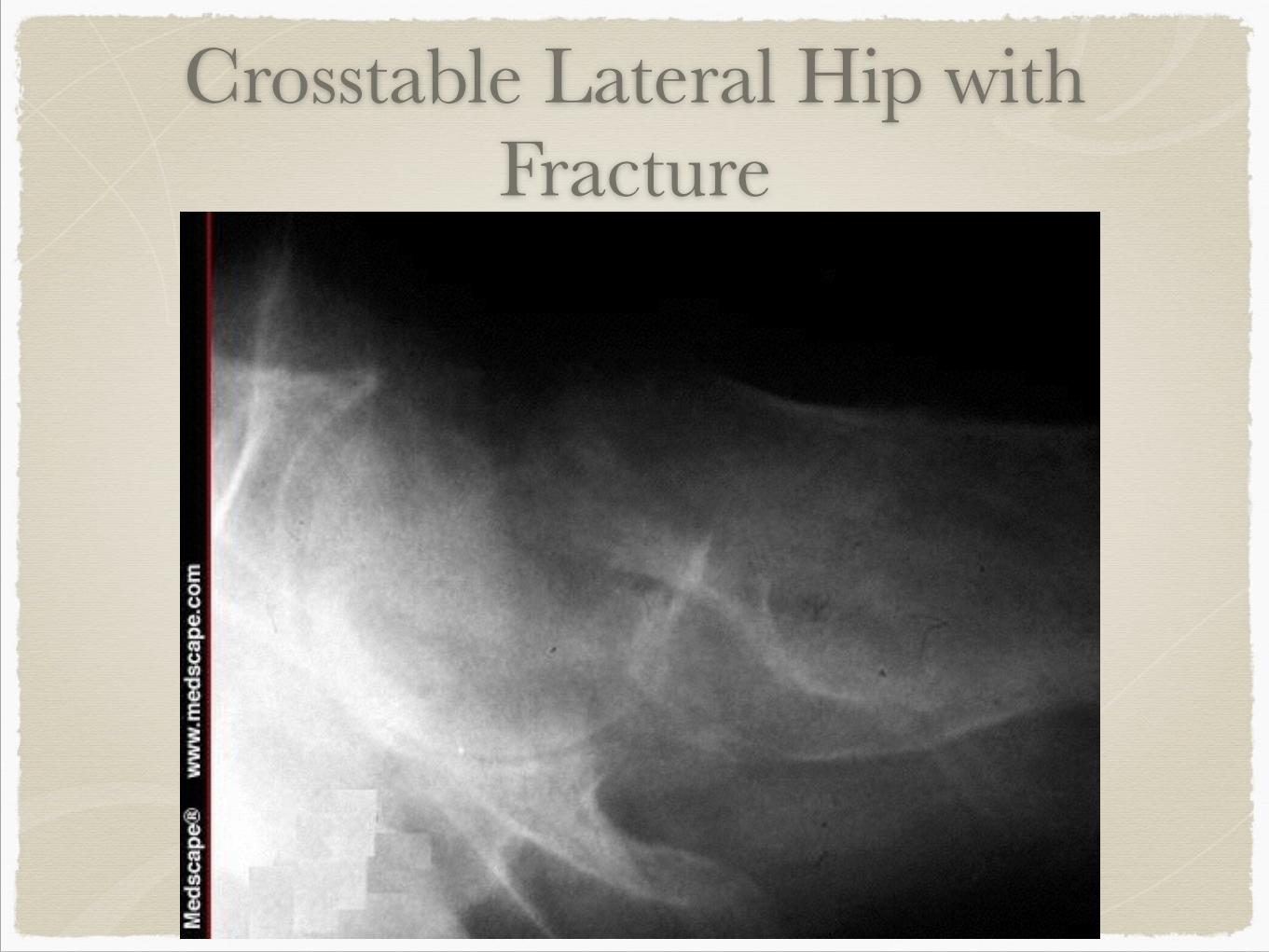
Crosstable Lateral Hip with Fracture
10
Review – What would you do?
Complication$
1. Patient unable to lie flat.$
2. Patient unable to move affected leg or fracture is suspected$
3. Both legs are affected and patient cannot move either legs.
11
12
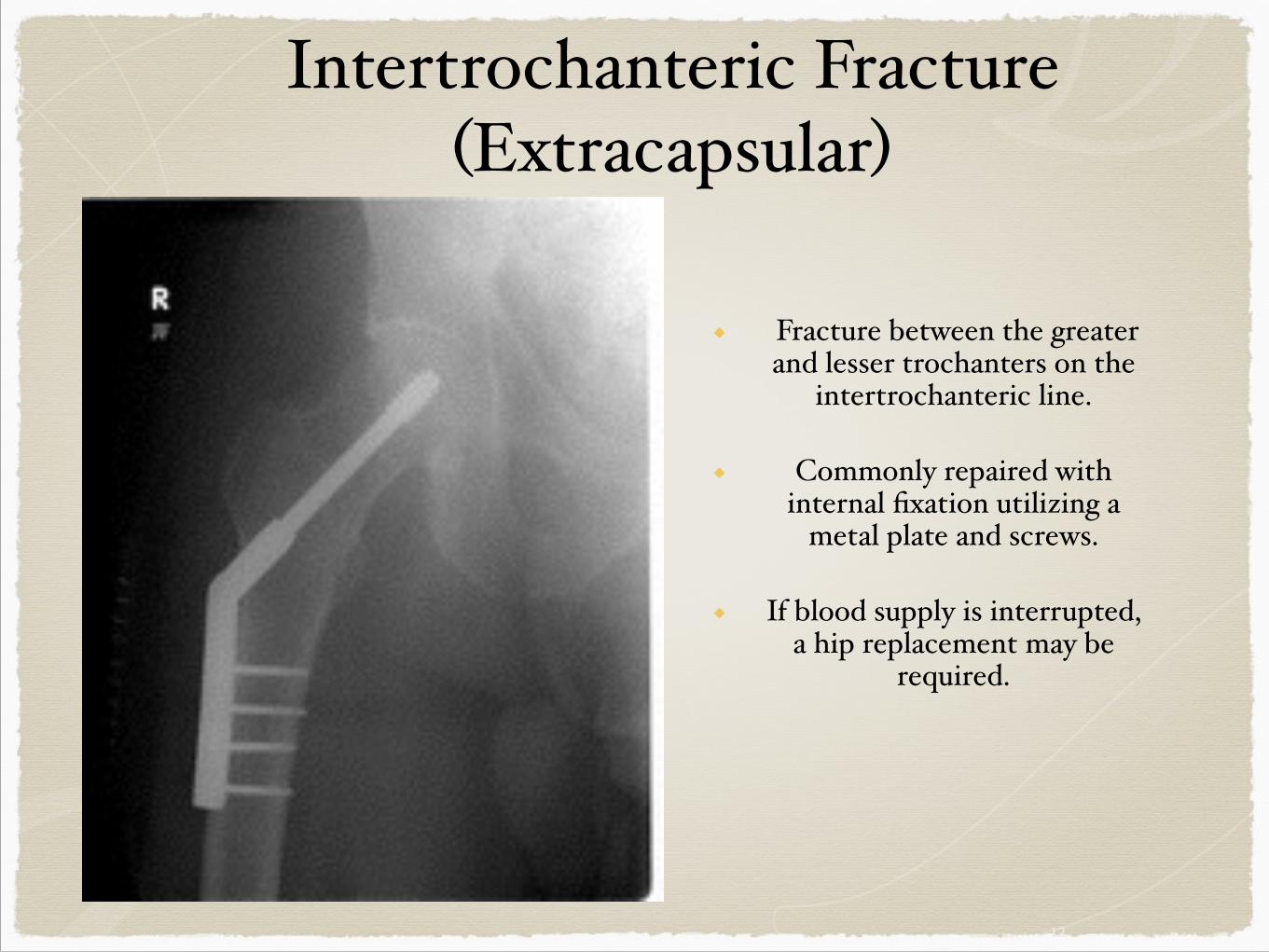
Intertrochanteric Fracture(Extracapsular)
◆ Fracture between the greater and lesser trochanters on the
intertrochanteric line.$!
◆ Commonly repaired with internal fixation utilizing a
metal plate and screws. $!
◆ If blood supply is interrupted, a hip replacement may be
required.$
13
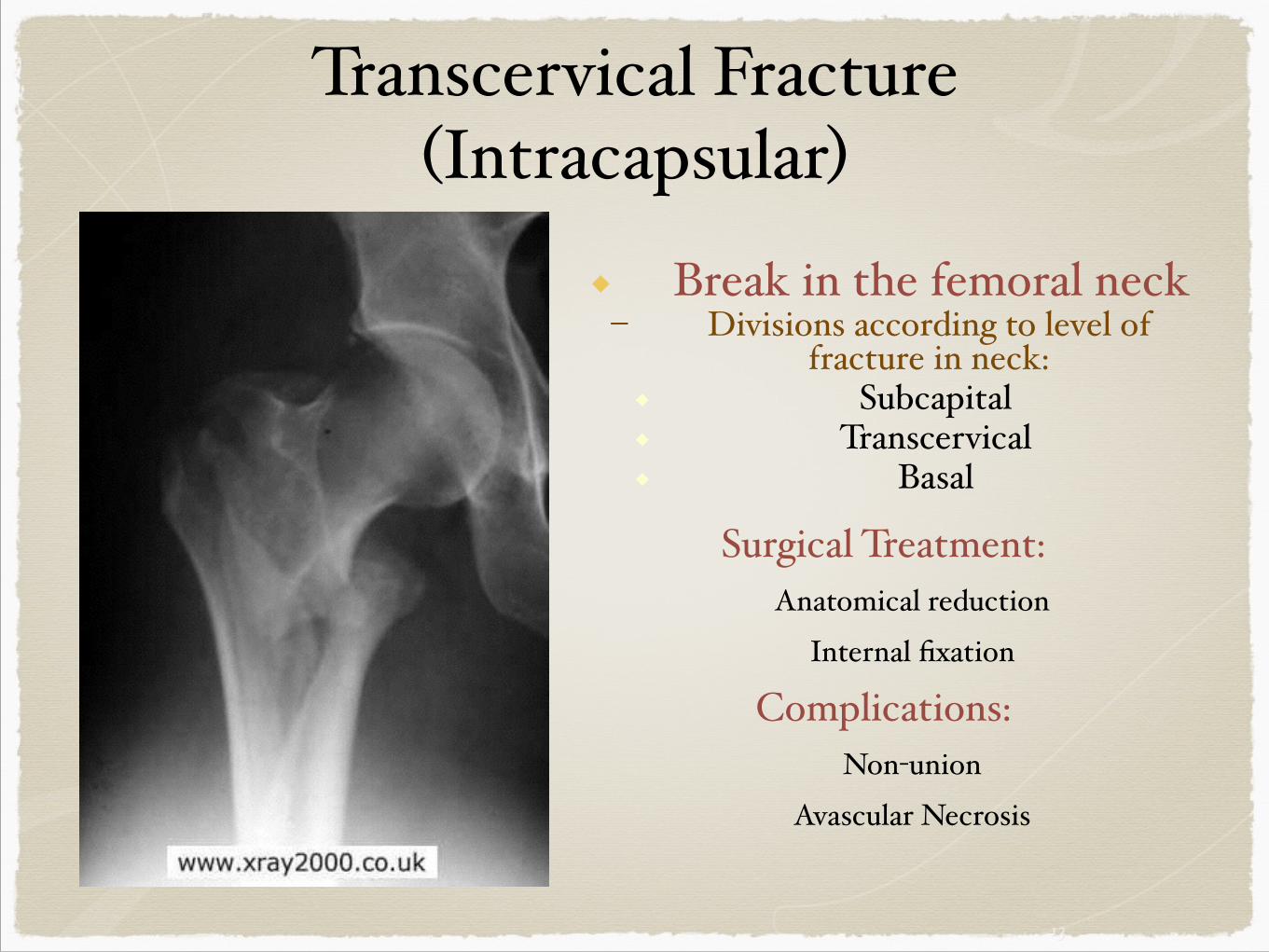
Transcervical Fracture(Intracapsular)
◆ Break in the femoral neck$– Divisions according to level of
fracture in neck:$◆ Subcapital $◆ Transcervical$◆ Basal$
!!Surgical Treatment:$
$ Anatomical reduction$$ Internal fixation$
Complications:$$ Non-union$
$ Avascular Necrosis
14
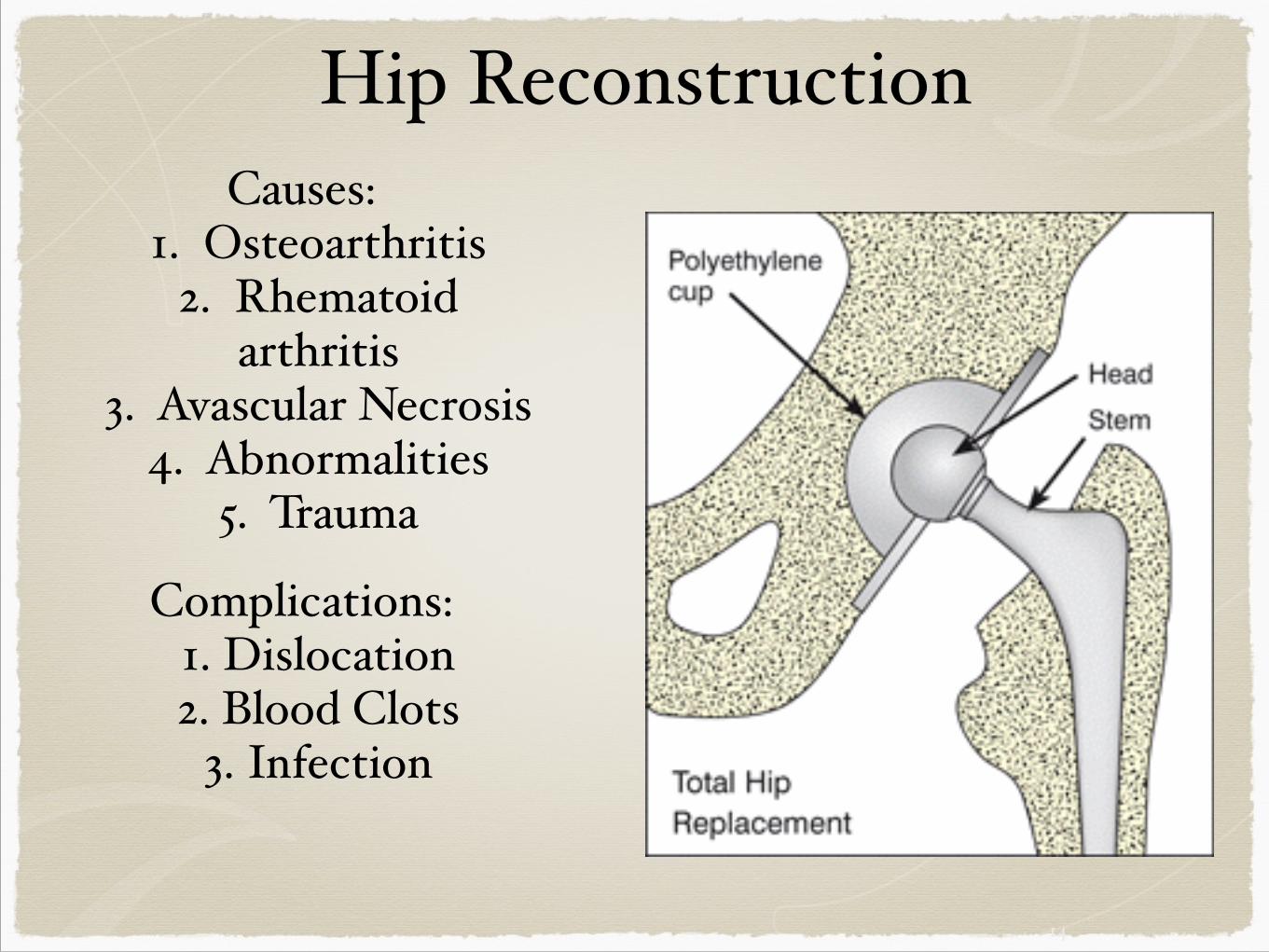
Hip ReconstructionCauses:$
$ 1. Osteoarthritis$$ 2. Rhematoid $ $$ arthritis$
$ 3. Avascular Necrosis$$ 4. Abnormalities$$ 5. Trauma$
!Complications:$$ 1. Dislocation$$ 2. Blood Clots$$ 3. Infection$
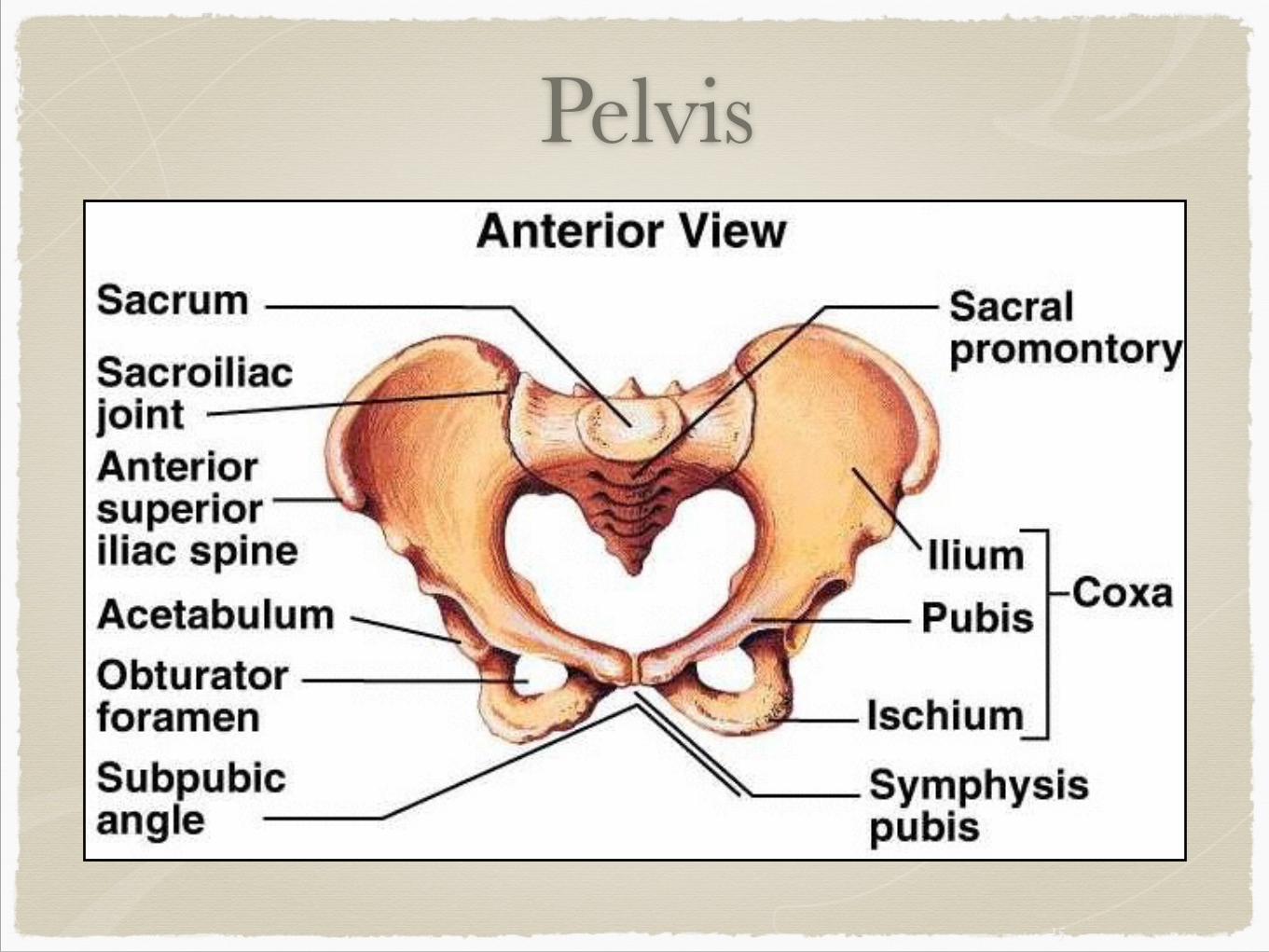
Pelvis
15
16
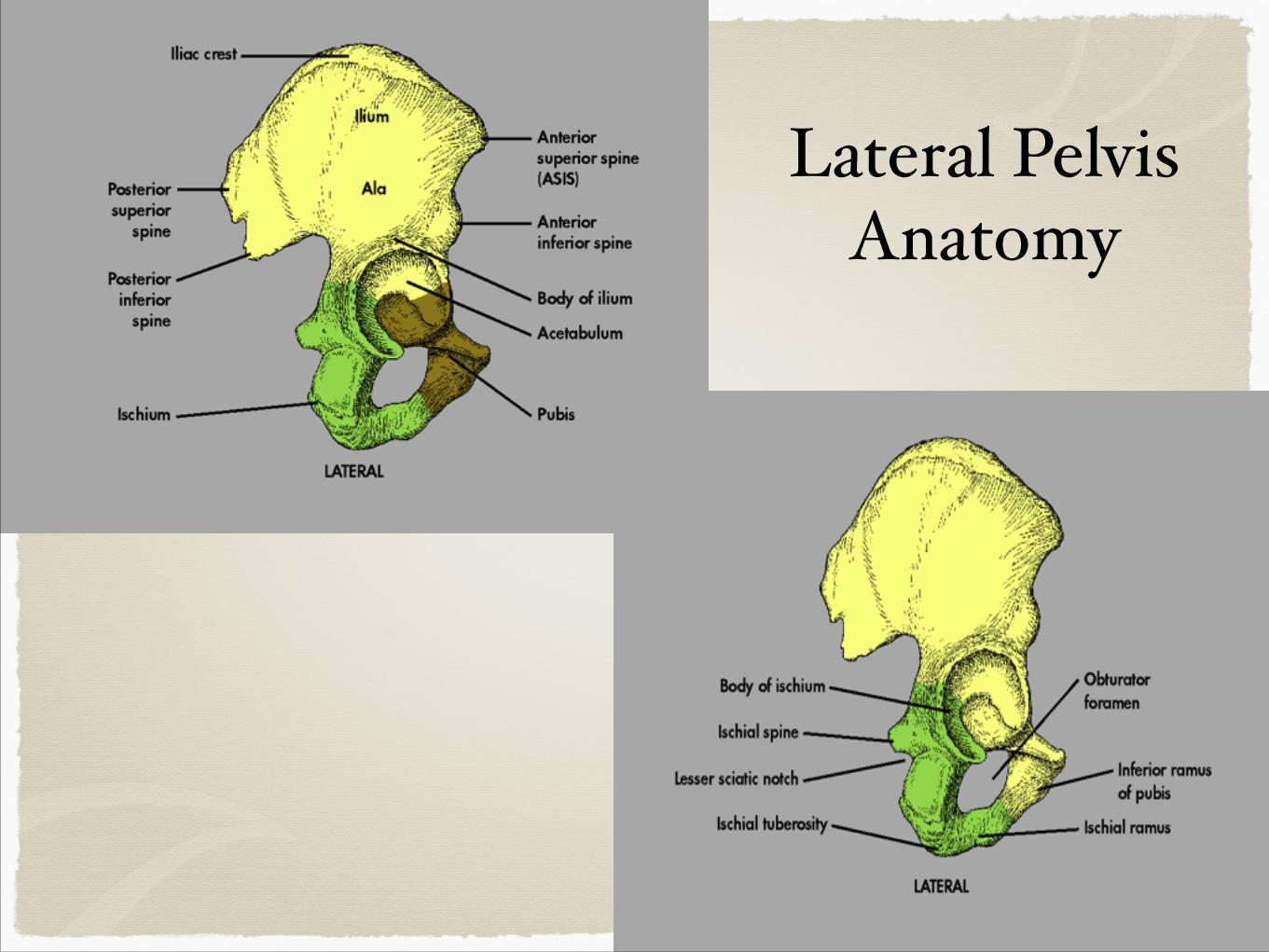
Lateral Pelvis Anatomy
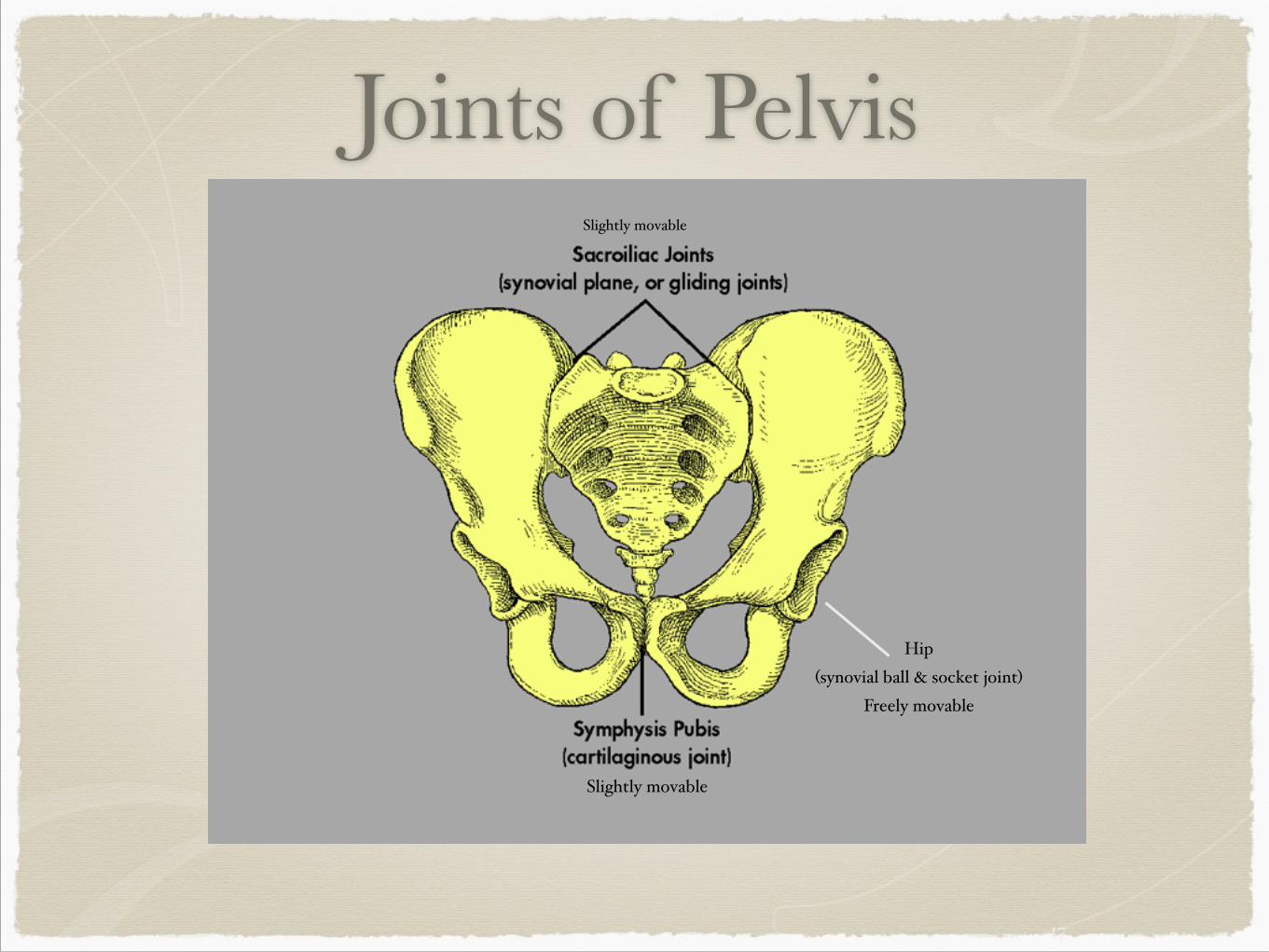
Joints of Pelvis
17
Slightly movable
Slightly movable
Hip$(synovial ball & socket joint)$
Freely movable
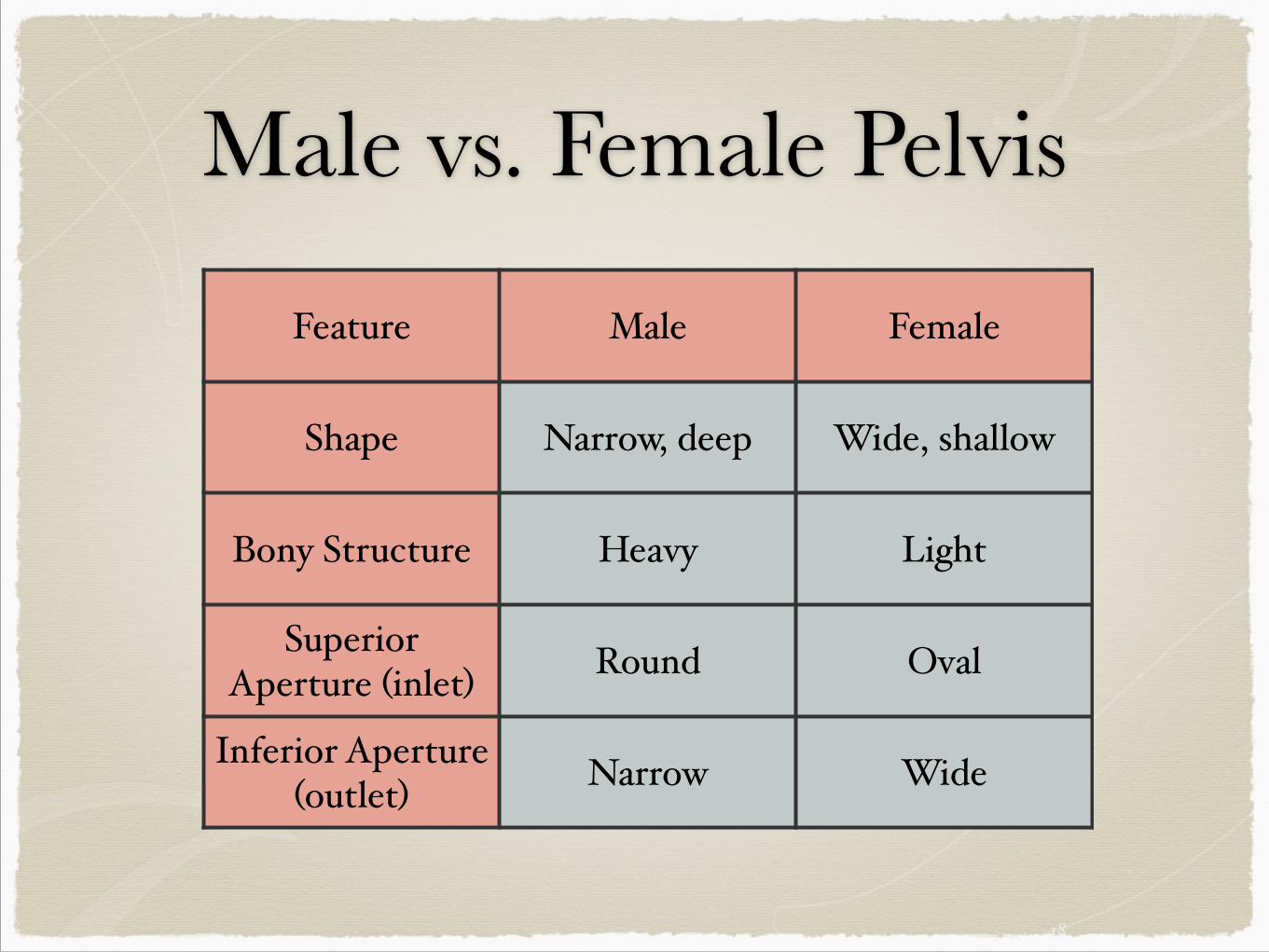
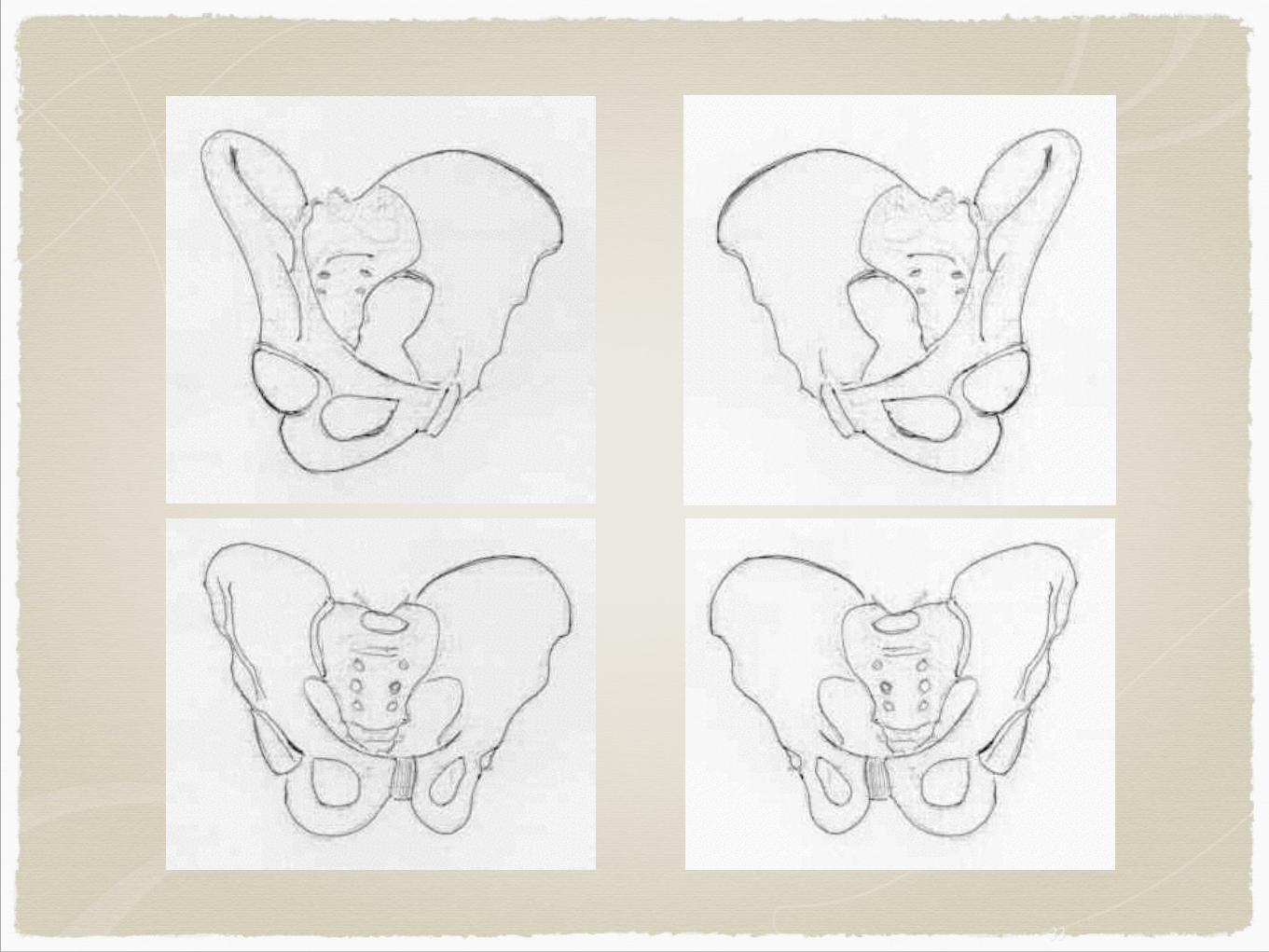
Male vs. Female Pelvis
18
Feature Male Female
Shape Narrow, deep Wide, shallow
Bony Structure Heavy Light
Superior Aperture (inlet) Round Oval
Inferior Aperture (outlet) Narrow Wide
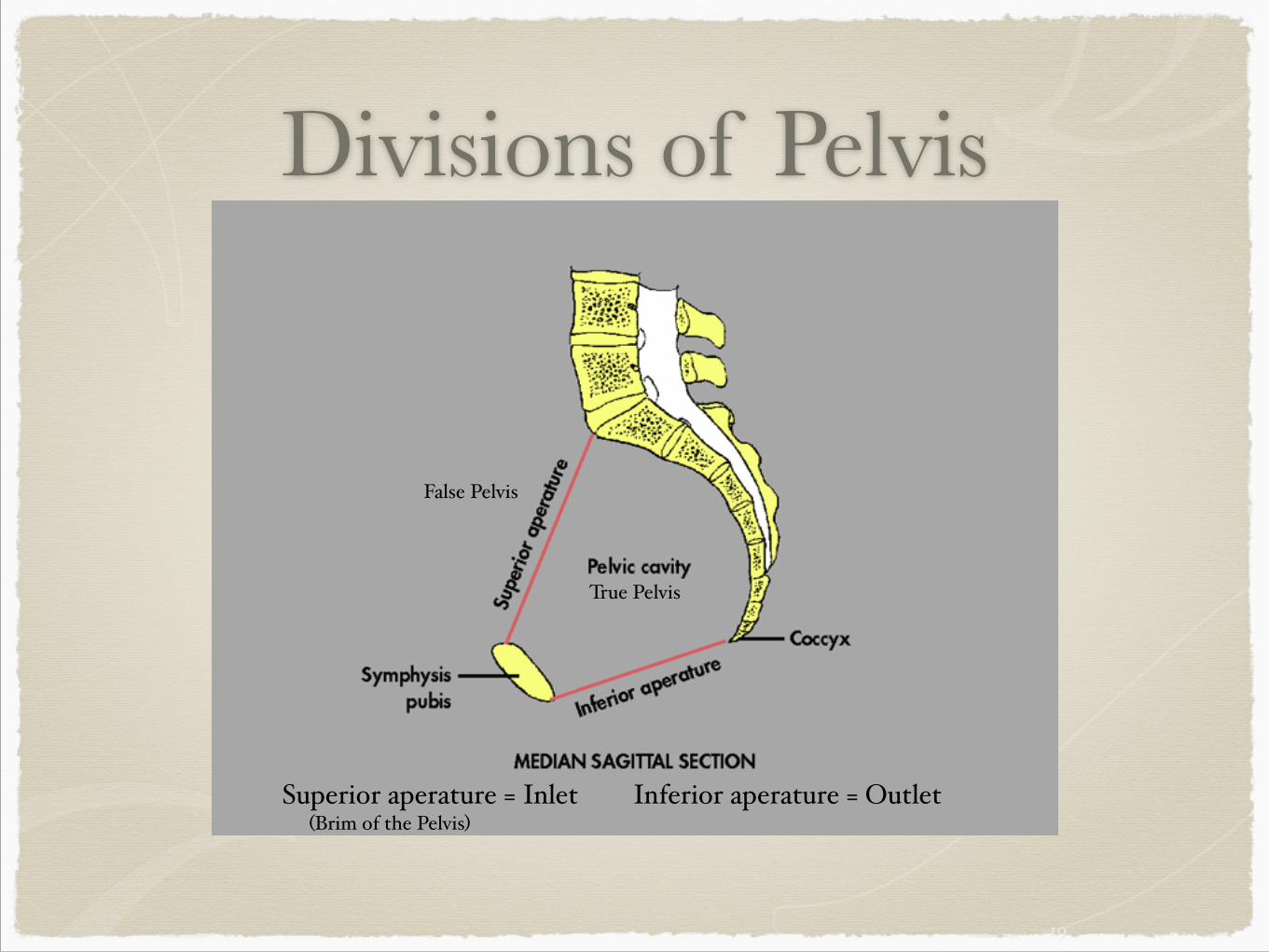
Divisions of Pelvis
19
True Pelvis
False Pelvis
Superior aperature = Inlet Inferior aperature = Outlet(Brim of the Pelvis)
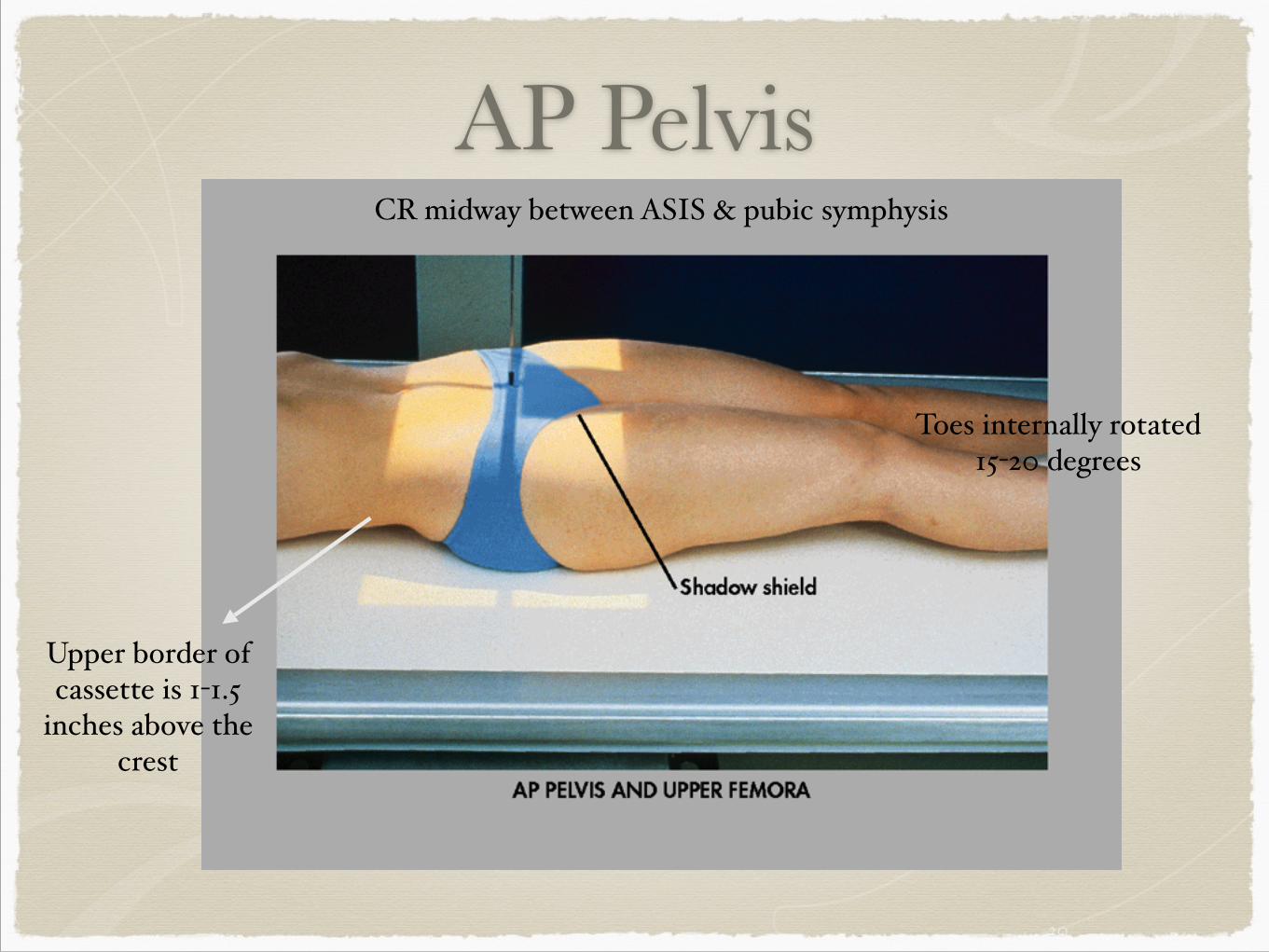
AP Pelvis
20
CR midway between ASIS & pubic symphysis
Upper border of cassette is 1-1.5
inches above the crest
Toes internally rotated 15-20 degrees
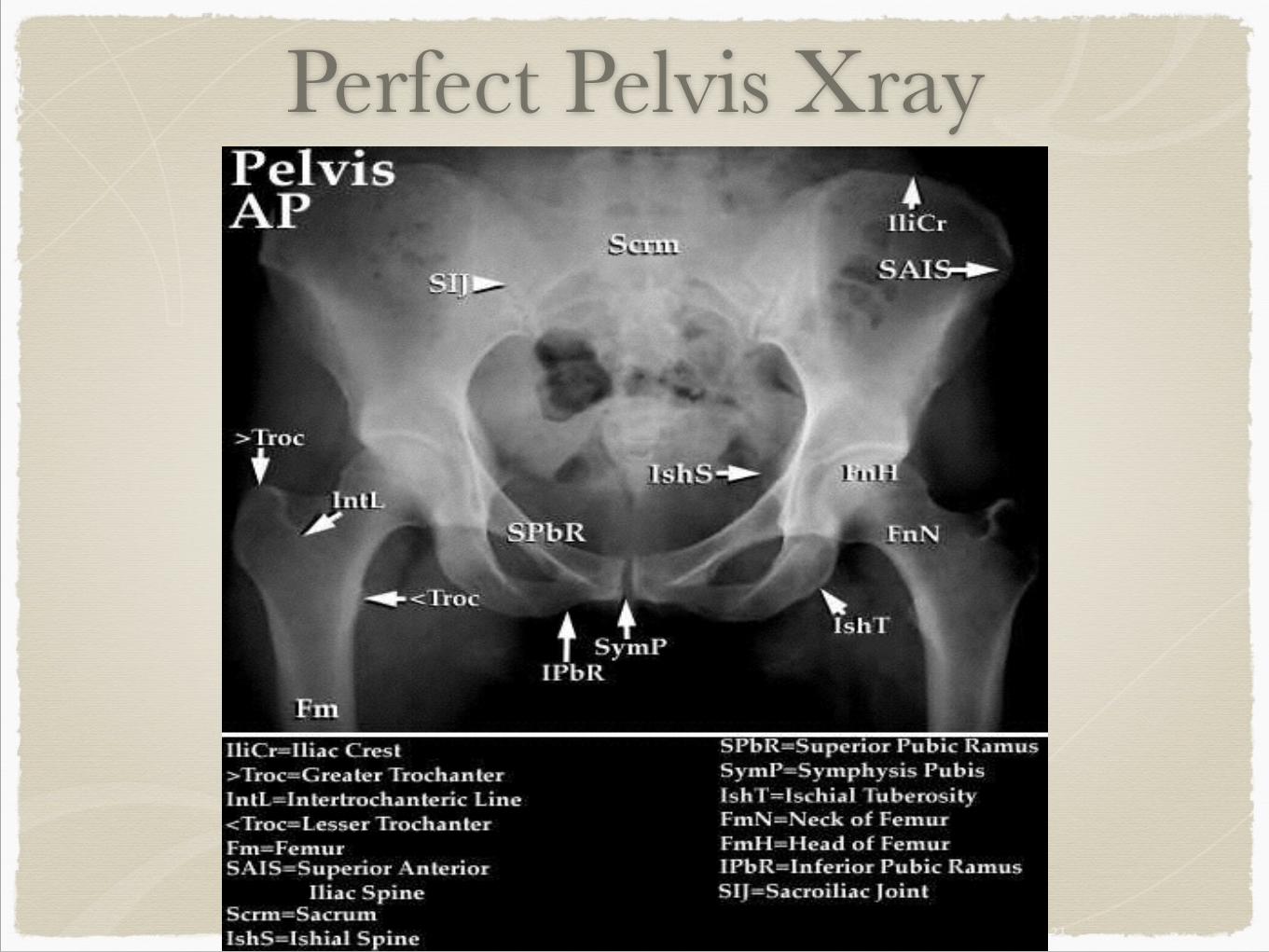
Perfect Pelvis Xray
21
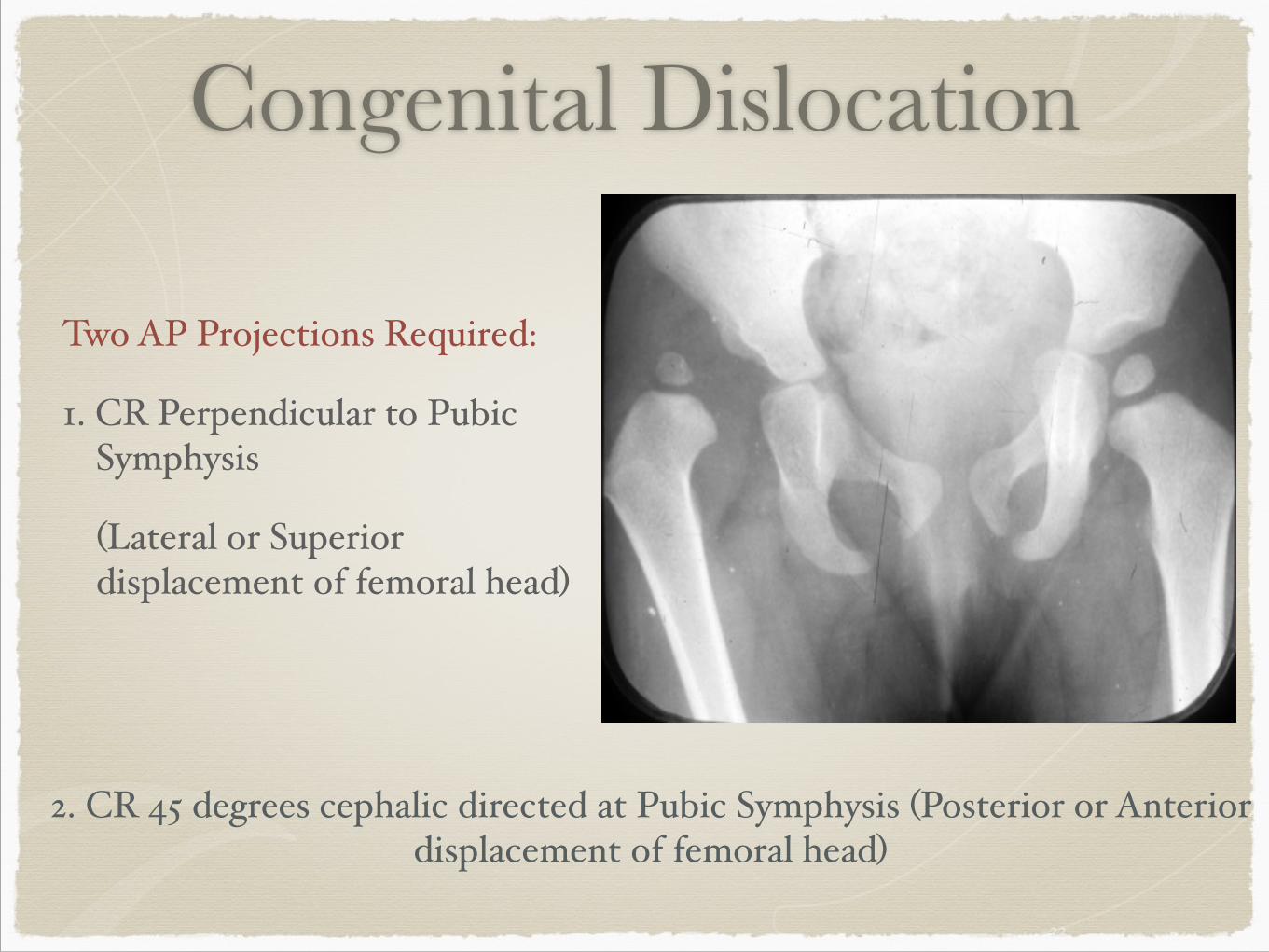
Congenital Dislocation
Two AP Projections Required:$
1. CR Perpendicular to Pubic Symphysis$
$ (Lateral or Superior displacement of femoral head)$
$
22
2. CR 45 degrees cephalic directed at Pubic Symphysis (Posterior or Anterior displacement of femoral head)$
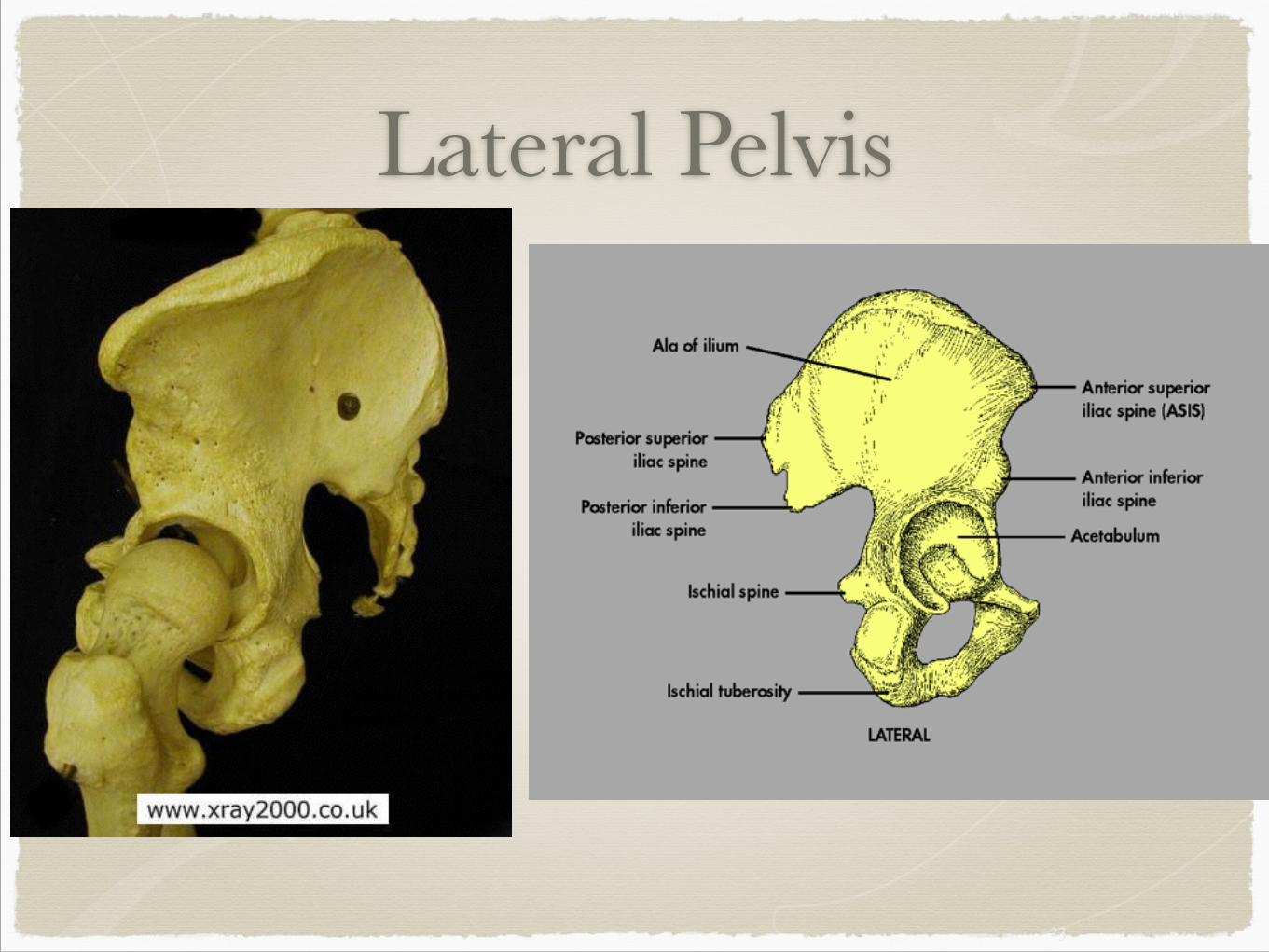
Lateral Pelvis
23
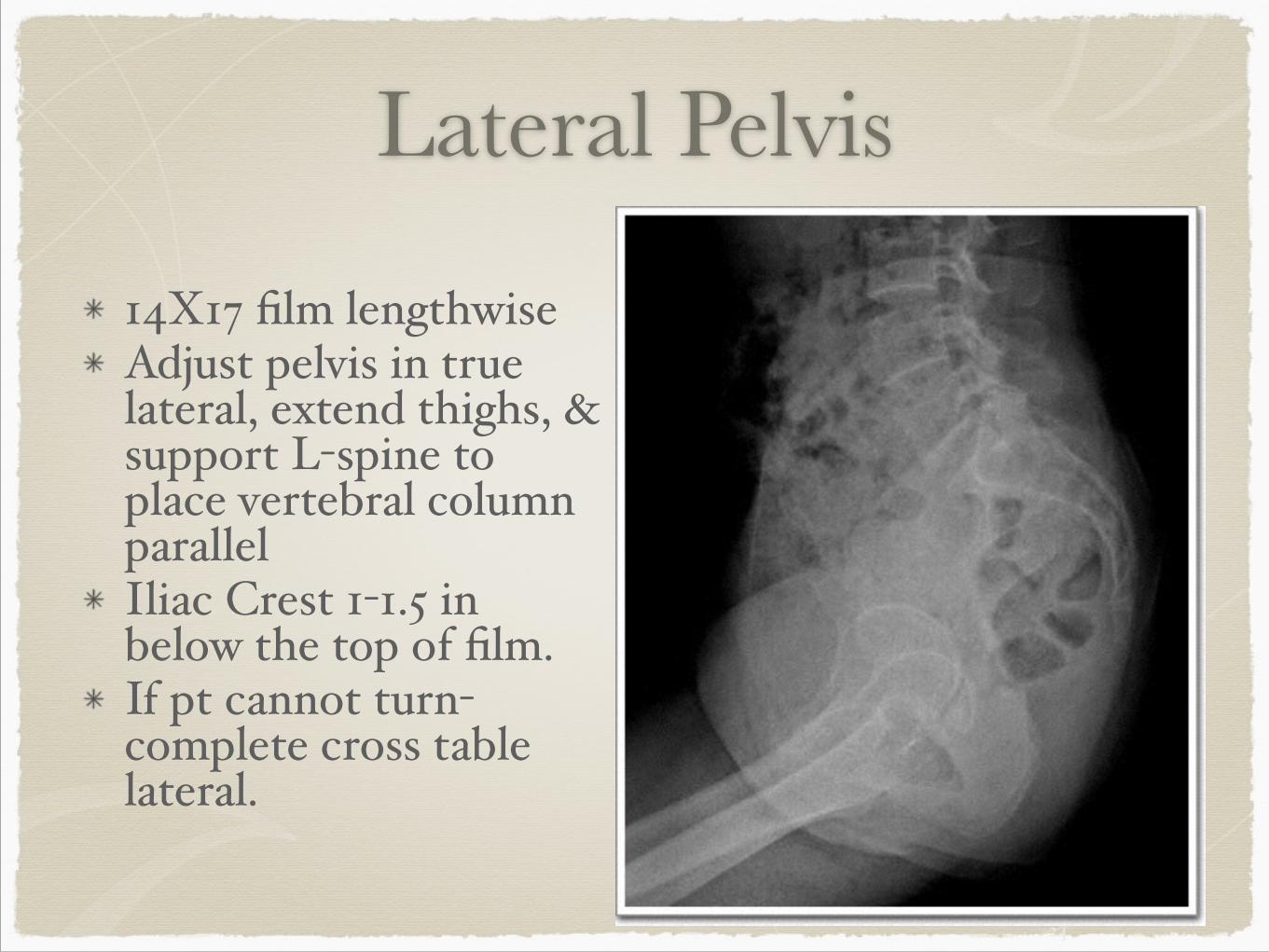
Lateral Pelvis
14X17 film lengthwise$Adjust pelvis in true lateral, extend thighs, & support L-spine to place vertebral column parallel$Iliac Crest 1-1.5 in below the top of film.$If pt cannot turn- complete cross table lateral.
24
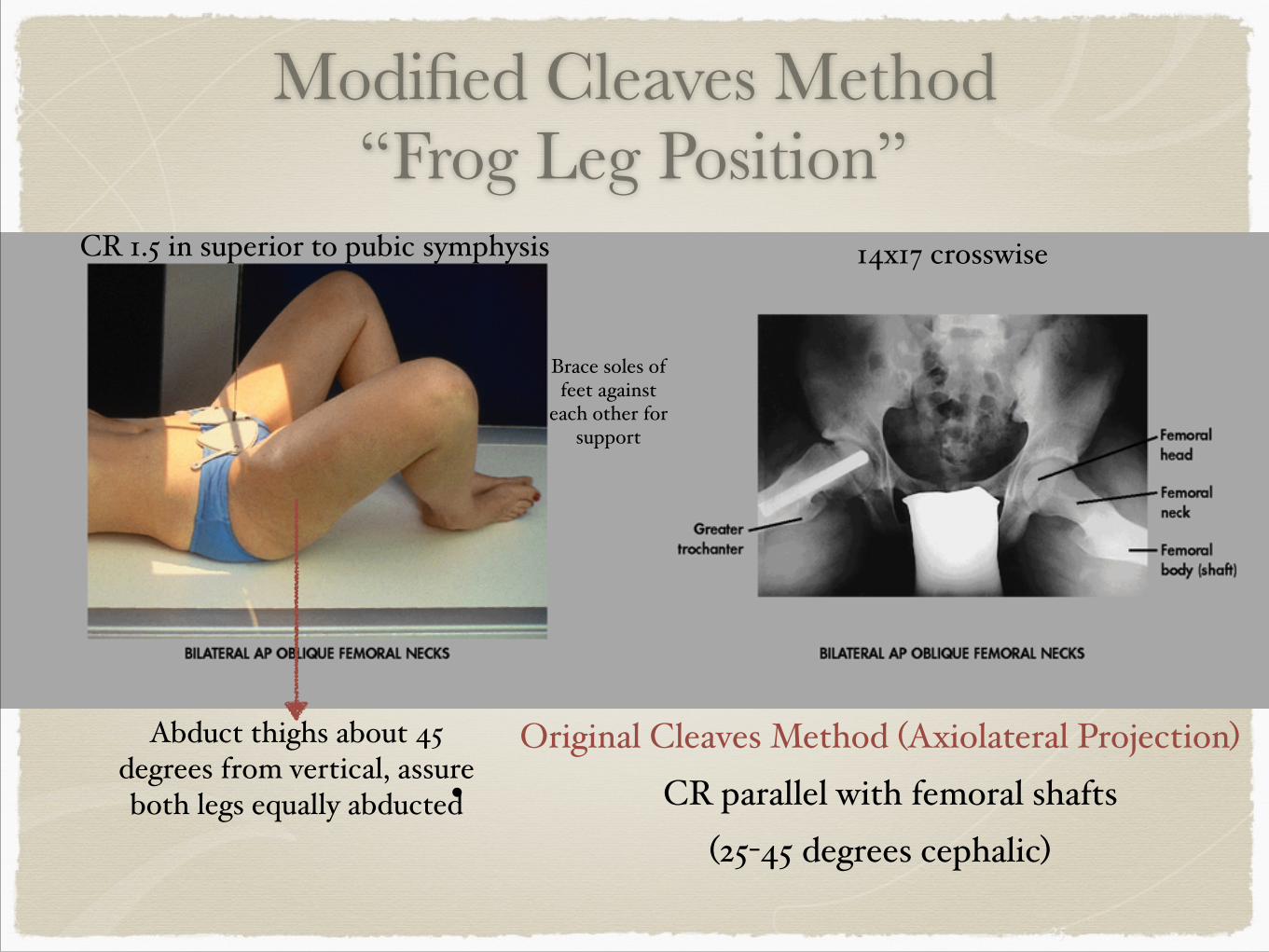
Modified Cleaves Method “Frog Leg Position”
25
14x17 crosswise
Brace soles of feet against
each other for support
Abduct thighs about 45 degrees from vertical, assure both legs equally abducted
CR 1.5 in superior to pubic symphysis
Original Cleaves Method (Axiolateral Projection)$• CR parallel with femoral shafts $
(25-45 degrees cephalic)
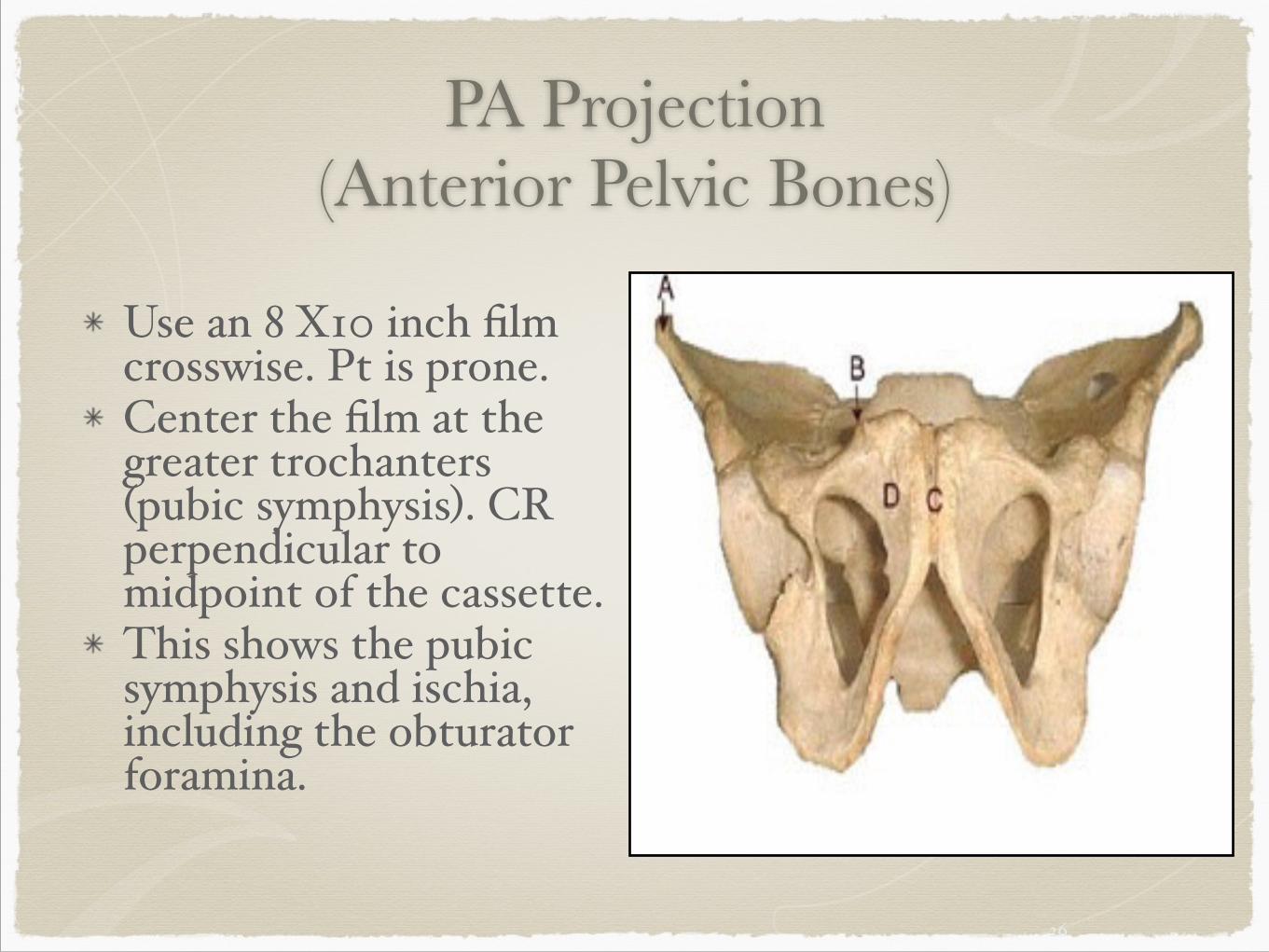
PA Projection (Anterior Pelvic Bones)
Use an 8 X10 inch film crosswise. Pt is prone.$Center the film at the greater trochanters (pubic symphysis). CR perpendicular to midpoint of the cassette.$This shows the pubic symphysis and ischia, including the obturator foramina.
26
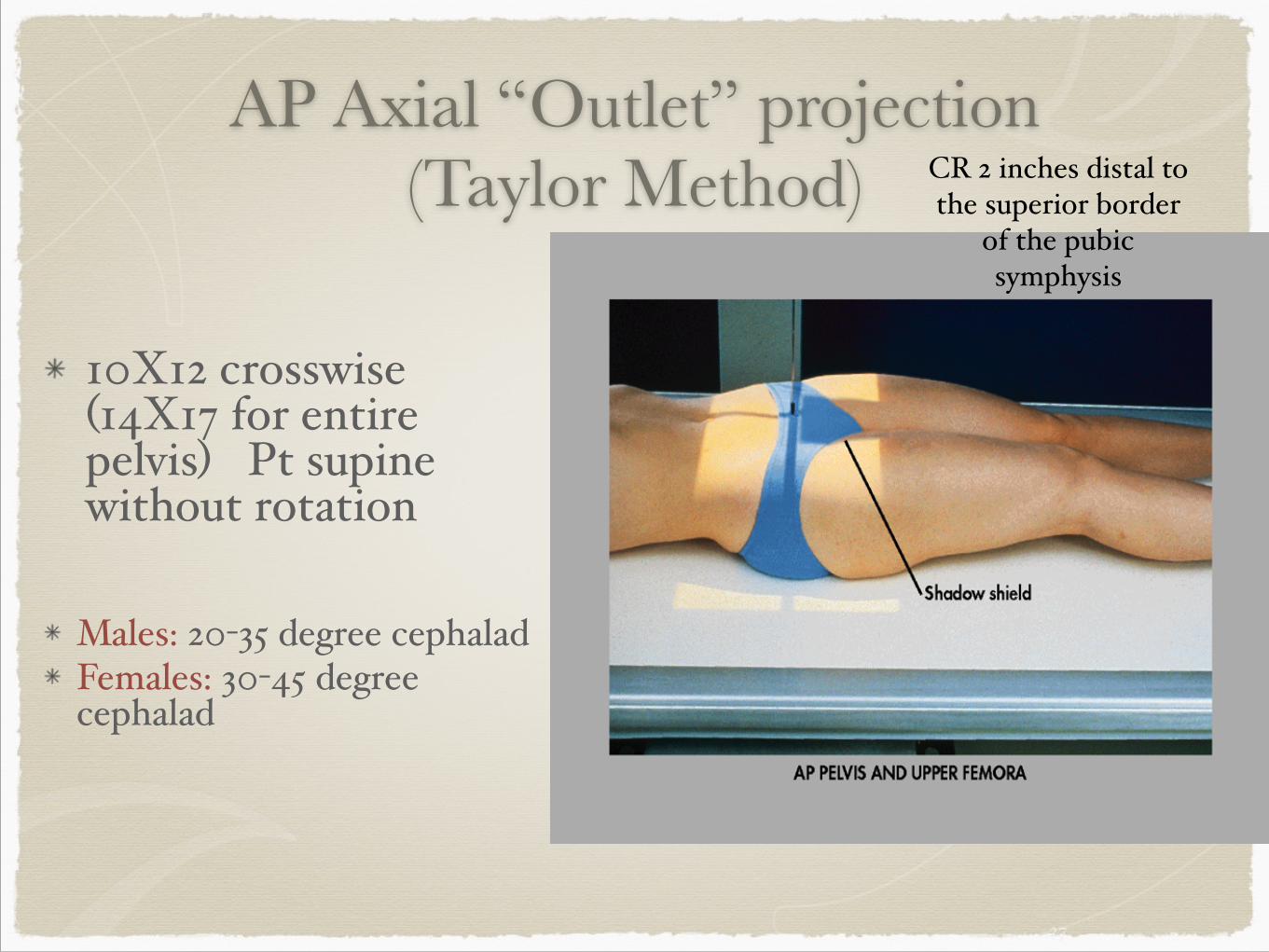
AP Axial “Outlet” projection (Taylor Method)
10X12 crosswise (14X17 for entire pelvis) Pt supine without rotation$
!Males: 20-35 degree cephalad$Females: 30-45 degree cephalad
27
CR 2 inches distal to the superior border
of the pubic symphysis
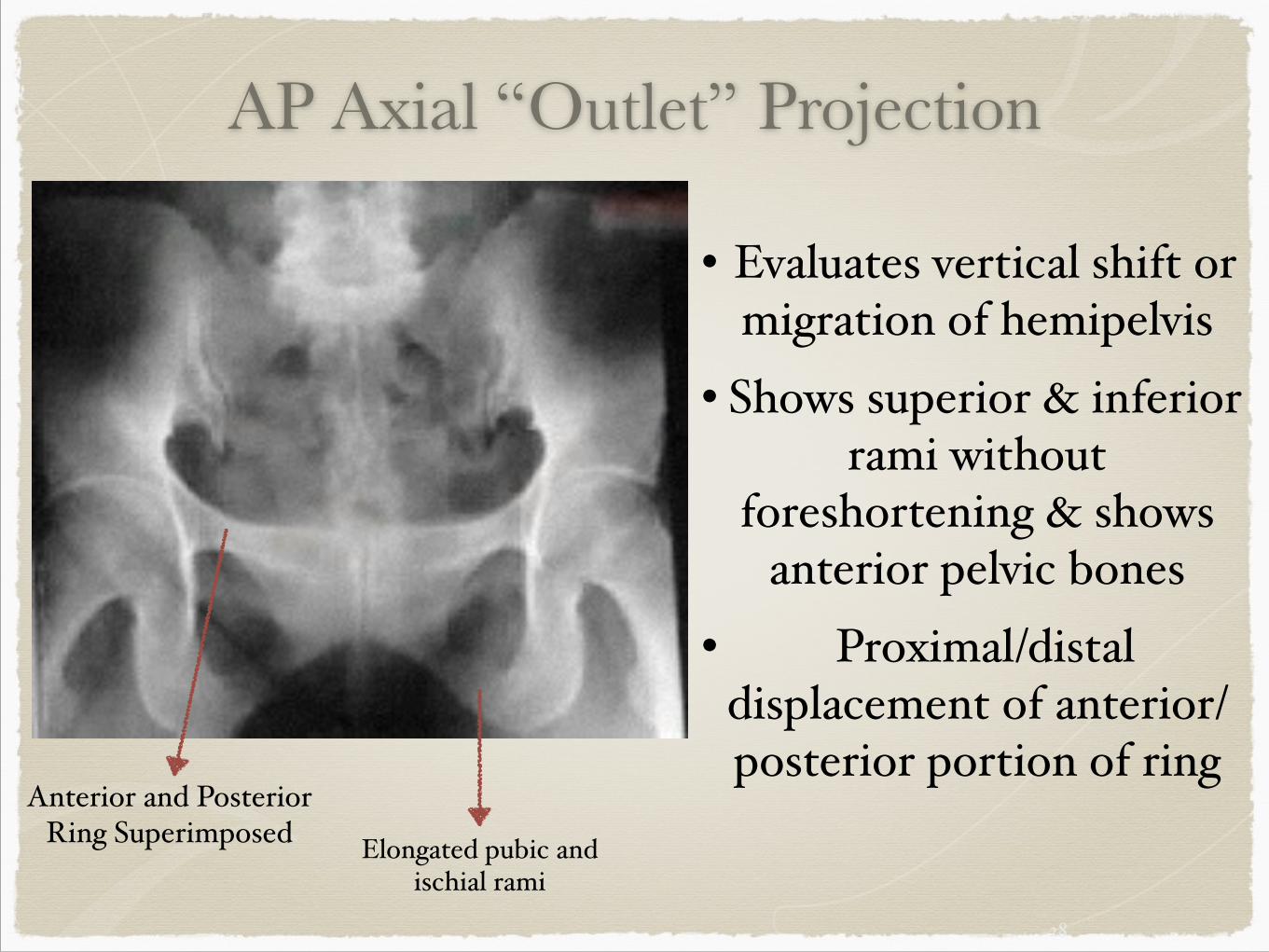
AP Axial “Outlet” Projection
28
Elongated pubic and ischial rami
• Evaluates vertical shift or migration of hemipelvis$
• Shows superior & inferior rami without
foreshortening & shows anterior pelvic bones$
• Proximal/distal displacement of anterior/posterior portion of ring
Anterior and Posterior Ring Superimposed
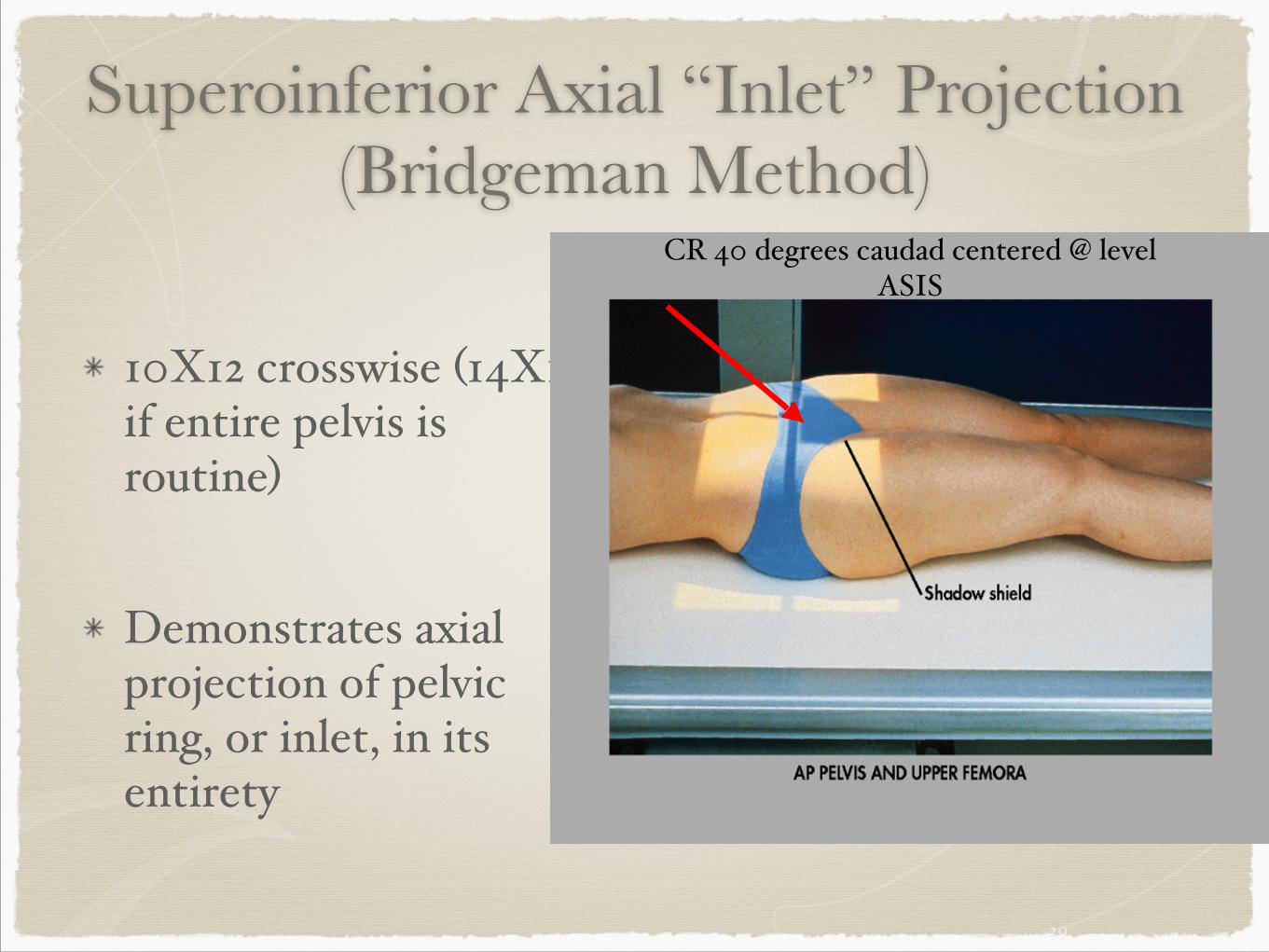
Superoinferior Axial “Inlet” Projection (Bridgeman Method)
!
10X12 crosswise (14X17 if entire pelvis is routine)$
!
Demonstrates axial projection of pelvic ring, or inlet, in its entirety
29
CR 40 degrees caudad centered @ level ASIS
“Inlet” Projection
30
www.wheeless.com
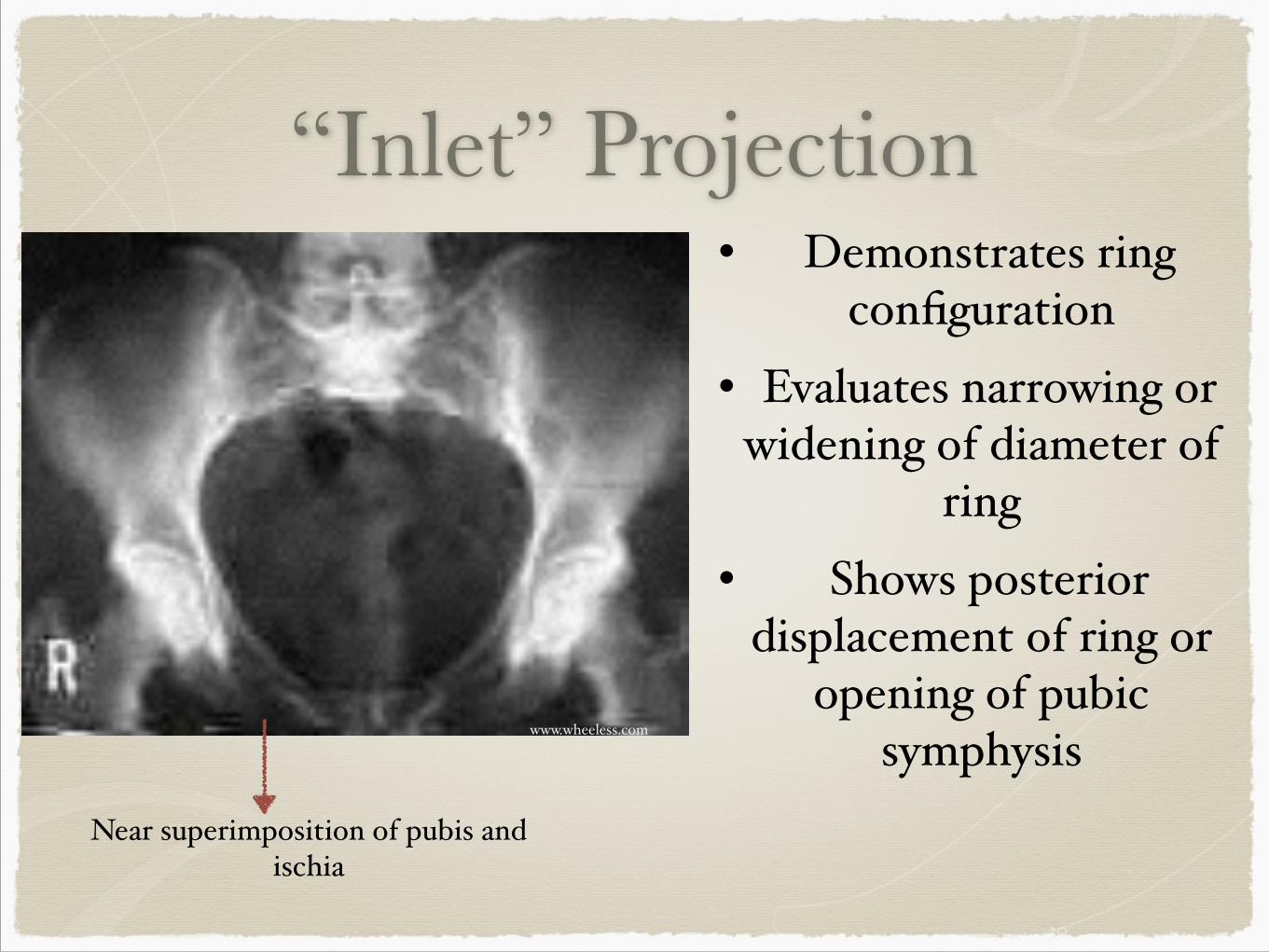
Near superimposition of pubis and ischia
• Demonstrates ring configuration$
• Evaluates narrowing or widening of diameter of
ring$• Shows posterior
displacement of ring or opening of pubic
symphysis
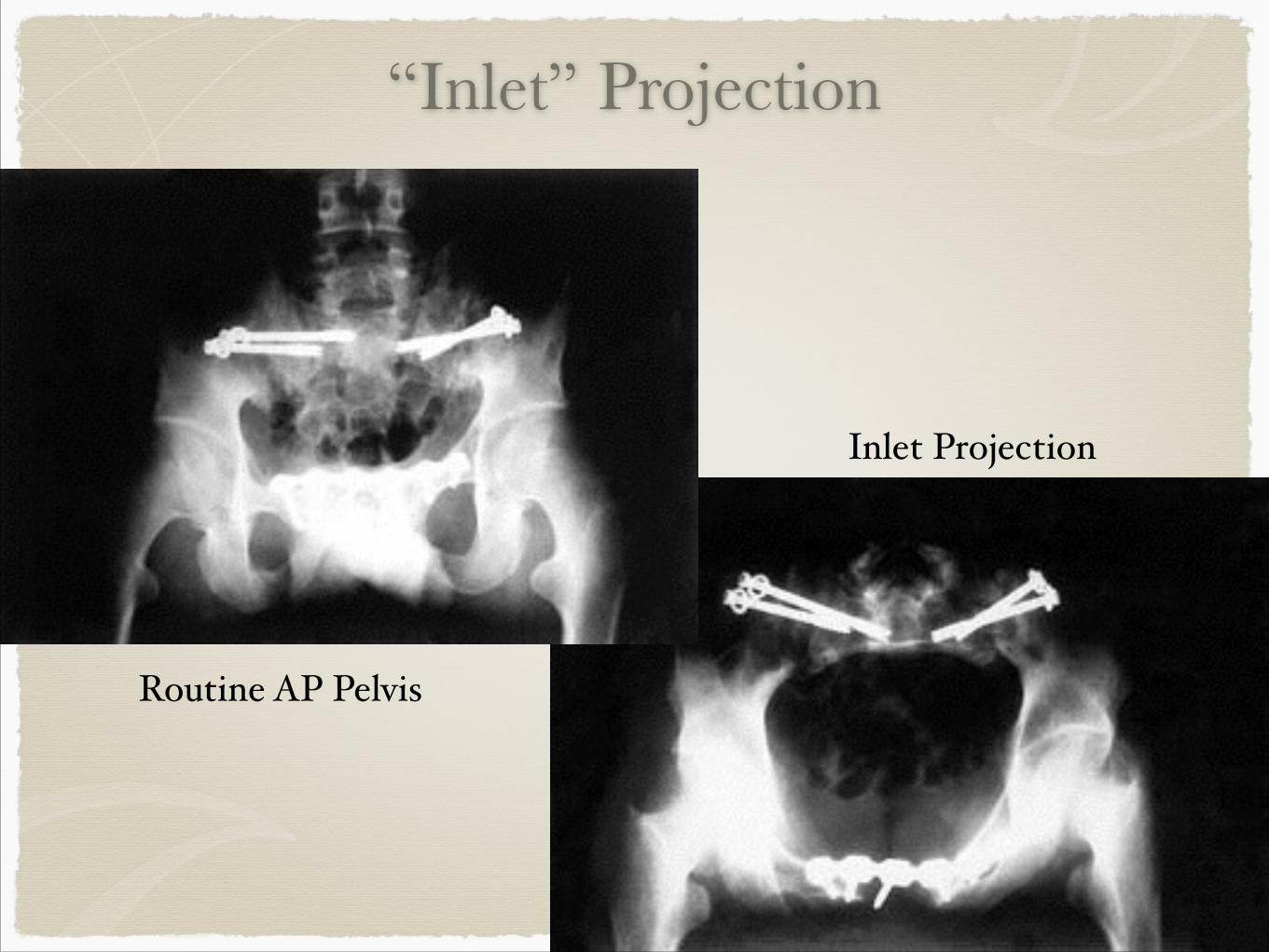
“Inlet” Projection
31
Routine AP Pelvis
Inlet Projection$
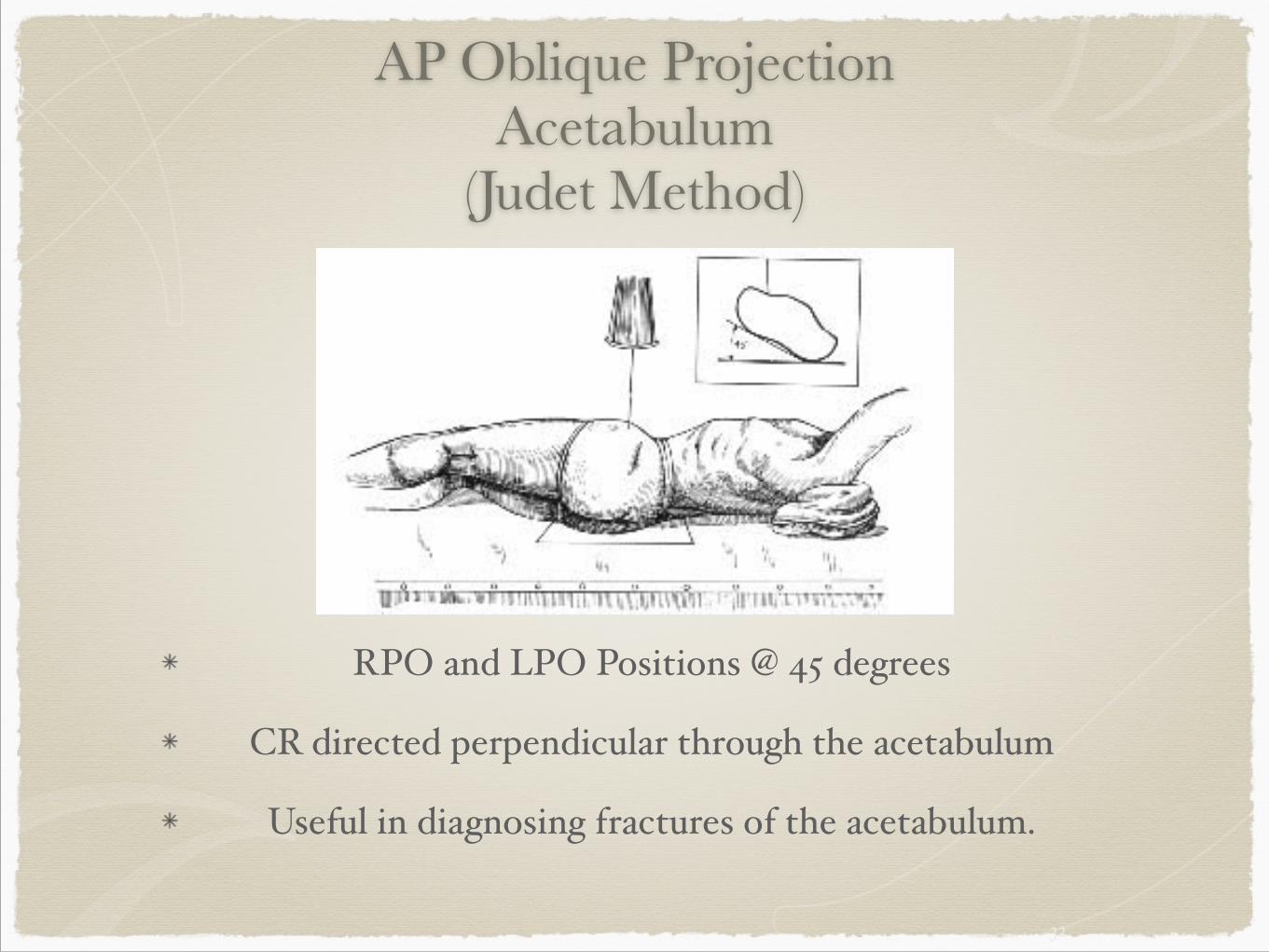
AP Oblique Projection Acetabulum
(Judet Method)
RPO and LPO Positions @ 45 degrees$
CR directed perpendicular through the acetabulum$
Useful in diagnosing fractures of the acetabulum.
32
33
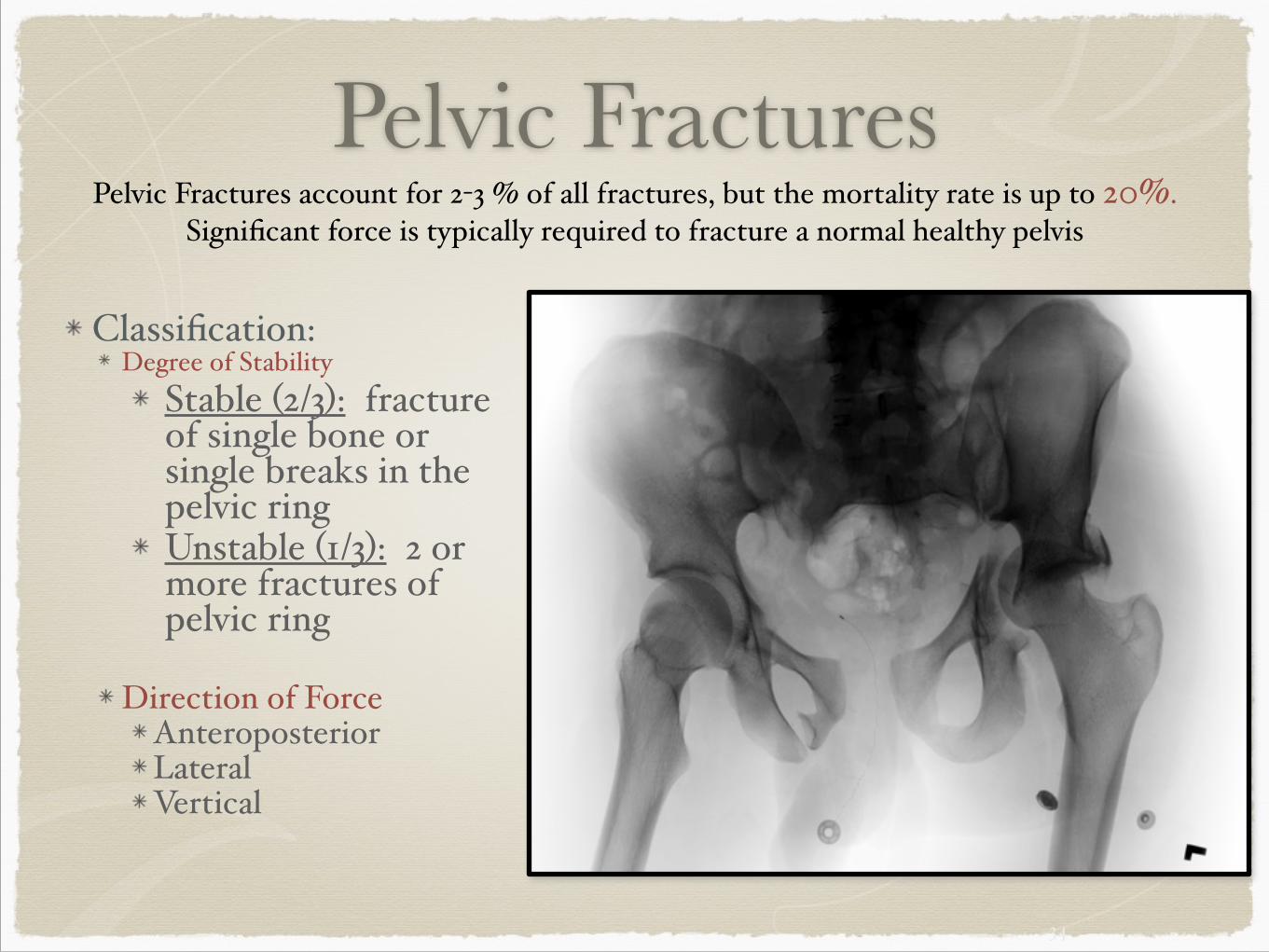
Pelvic Fractures!
Classification:$Degree of Stability$
Stable (2/3): fracture of single bone or single breaks in the pelvic ring$Unstable (1/3): 2 or more fractures of pelvic ring$!
Direction of Force$Anteroposterior$Lateral $Vertical
34
Pelvic Fractures account for 2-3 % of all fractures, but the mortality rate is up to 20%. Significant force is typically required to fracture a normal healthy pelvis
35
Pelvic Fractures
Complications:$Life threatening hemorrhage$Sitting imbalance$Leg length discrepancy$
!
Radiography: (note: do not move pt with suspected fx)$Minimum AP projection$Inlet and Outlet projections (anteroposterior displacement)
36
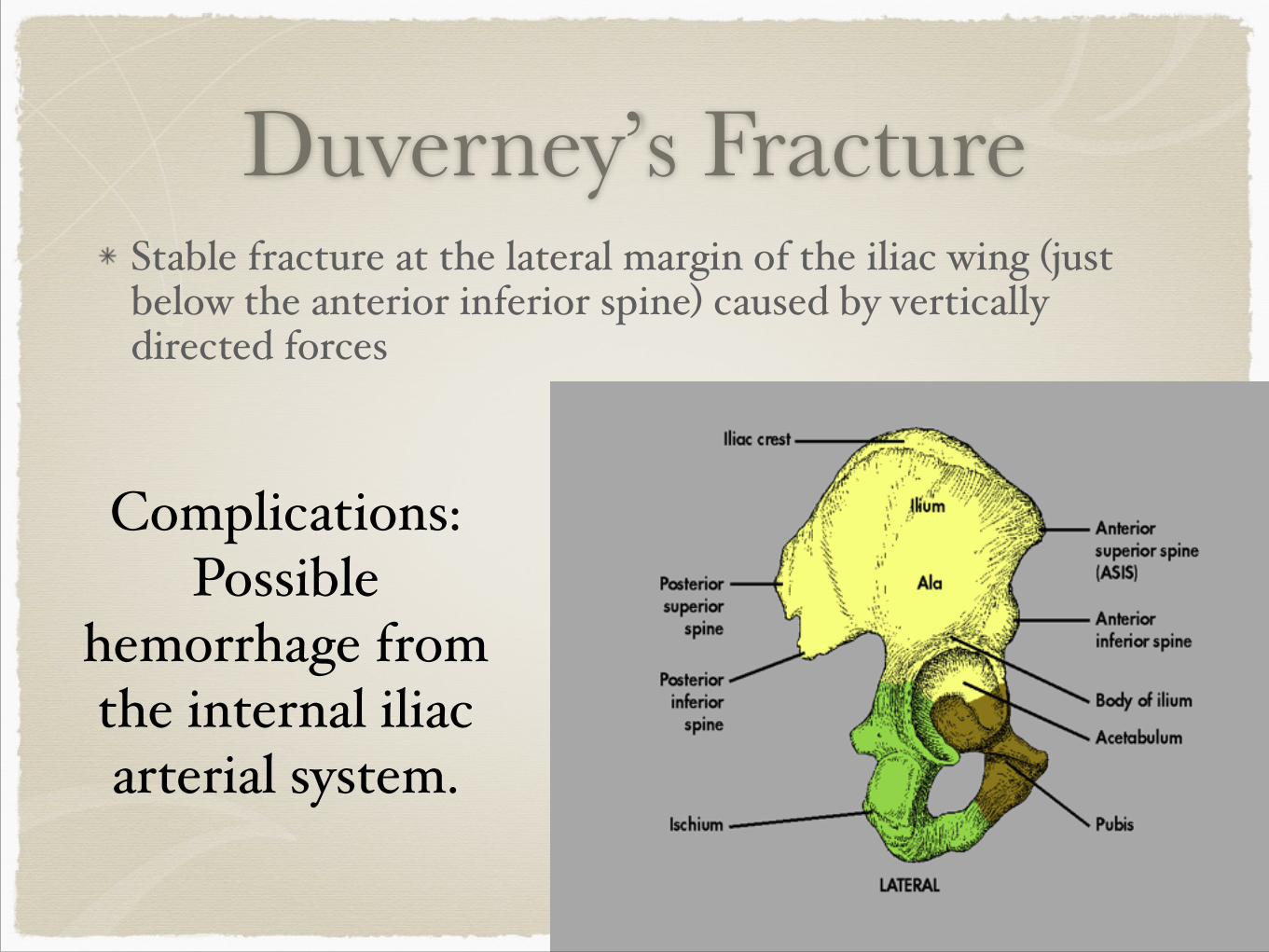
Duverney’s FractureStable fracture at the lateral margin of the iliac wing (just below the anterior inferior spine) caused by vertically directed forces
37
Complications: Possible
hemorrhage from the internal iliac arterial system.
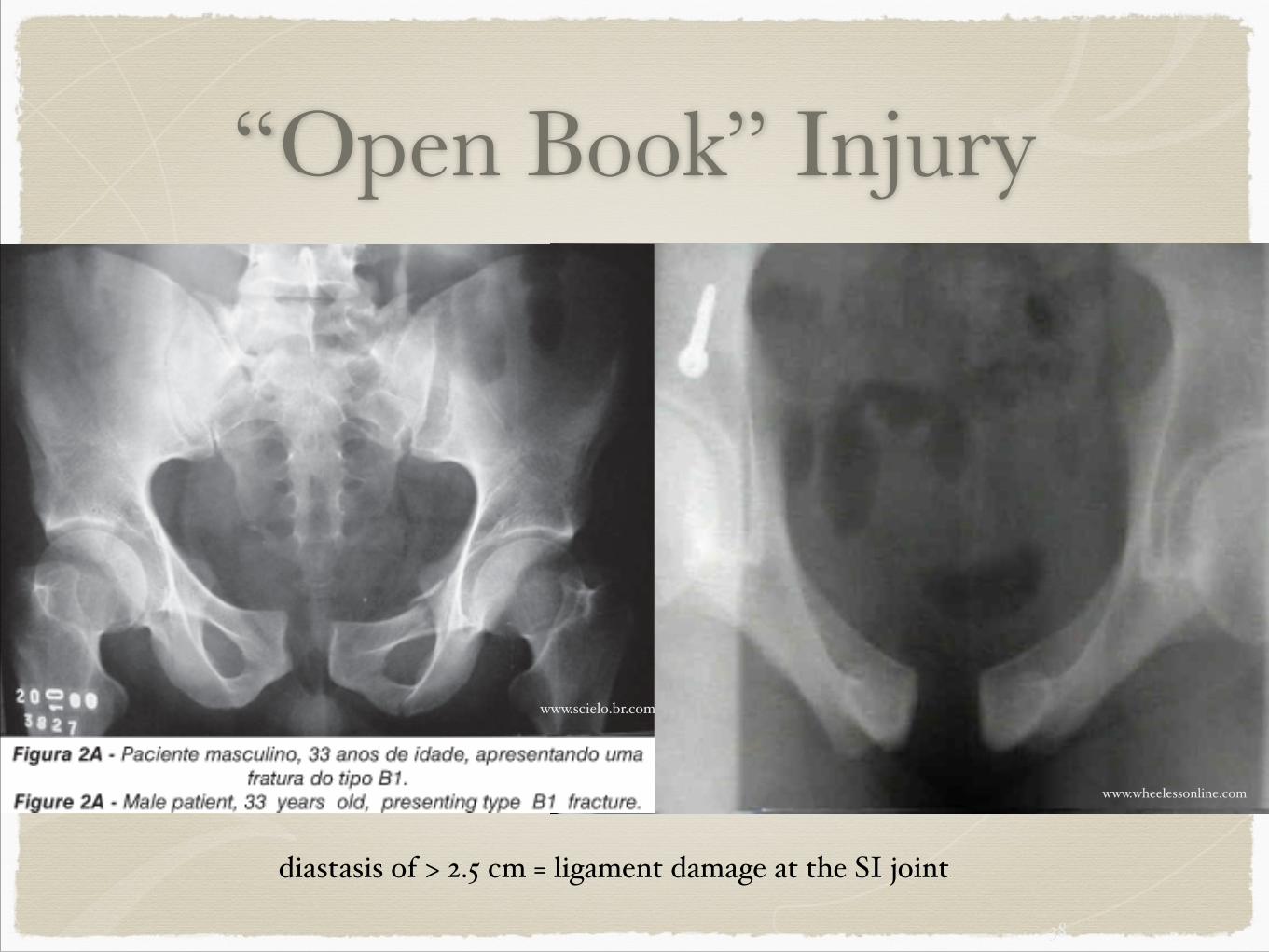
“Open Book” Injury
38
www.wheelessonline.com
diastasis of > 2.5 cm = ligament damage at the SI joint
www.scielo.br.com
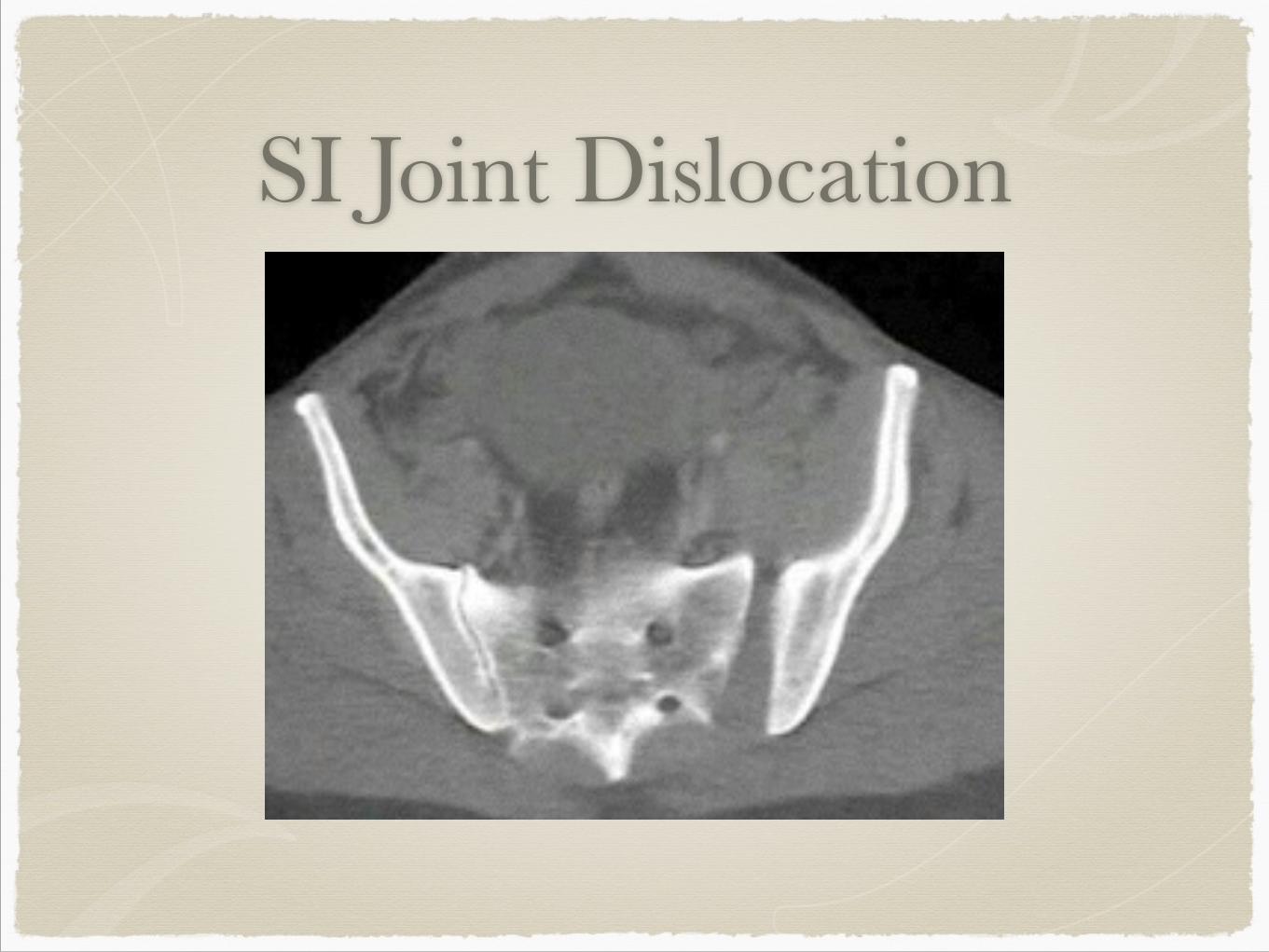
SI Joint Dislocation
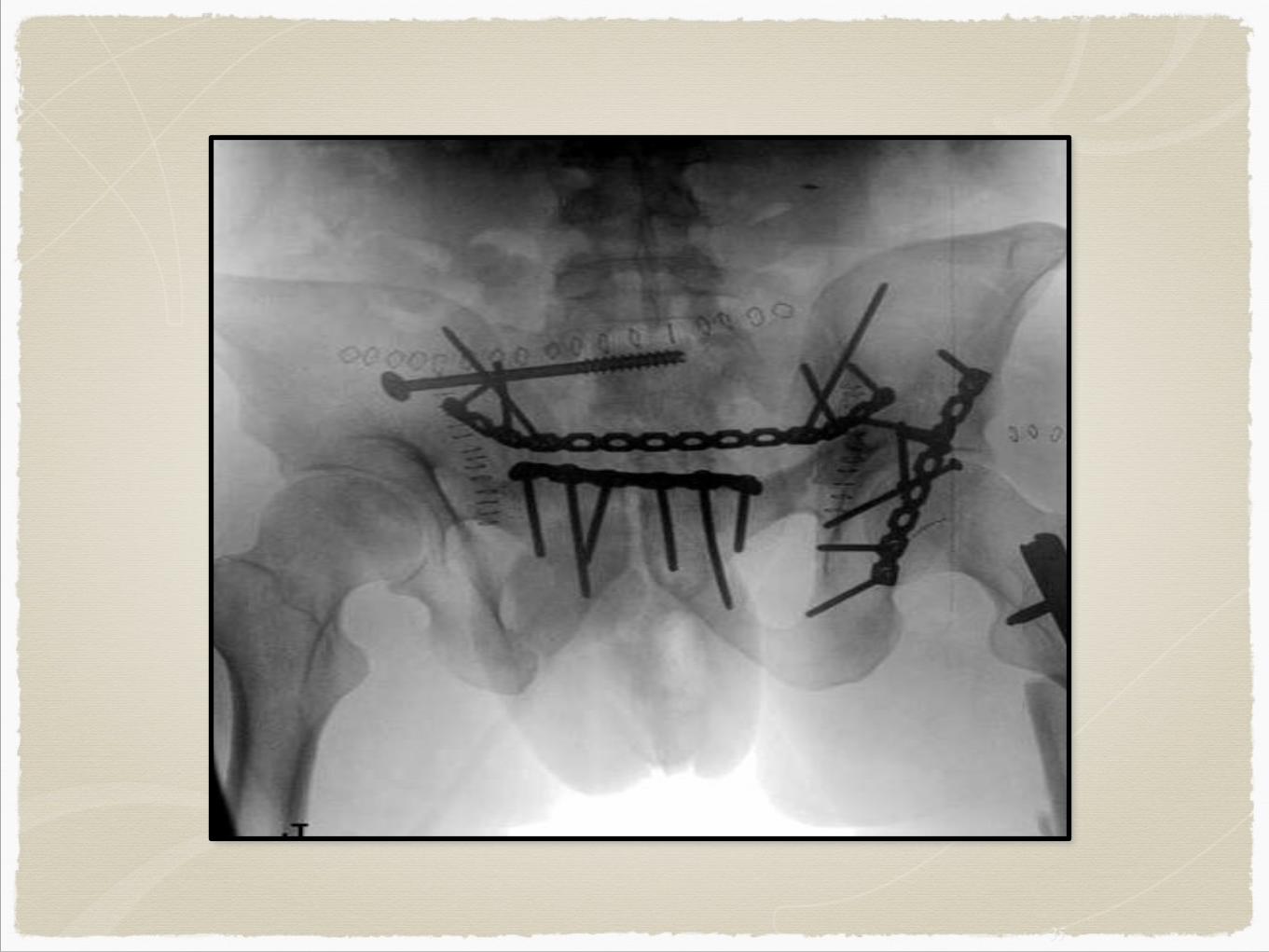
Surgery
39
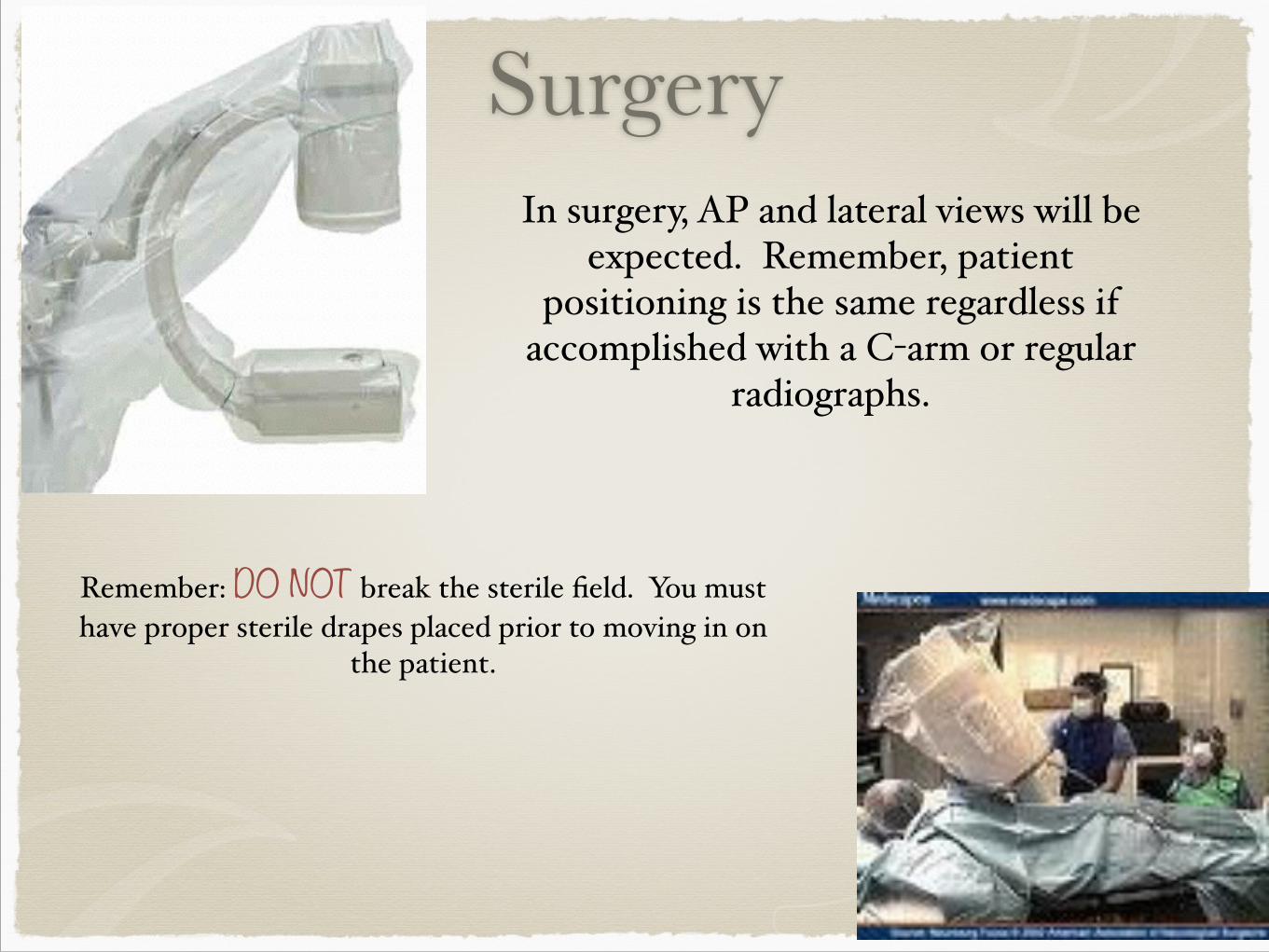
In surgery, AP and lateral views will be expected. Remember, patient
positioning is the same regardless if accomplished with a C-arm or regular
radiographs.
Remember: DO NOT break the sterile field. You must have proper sterile drapes placed prior to moving in on
the patient.
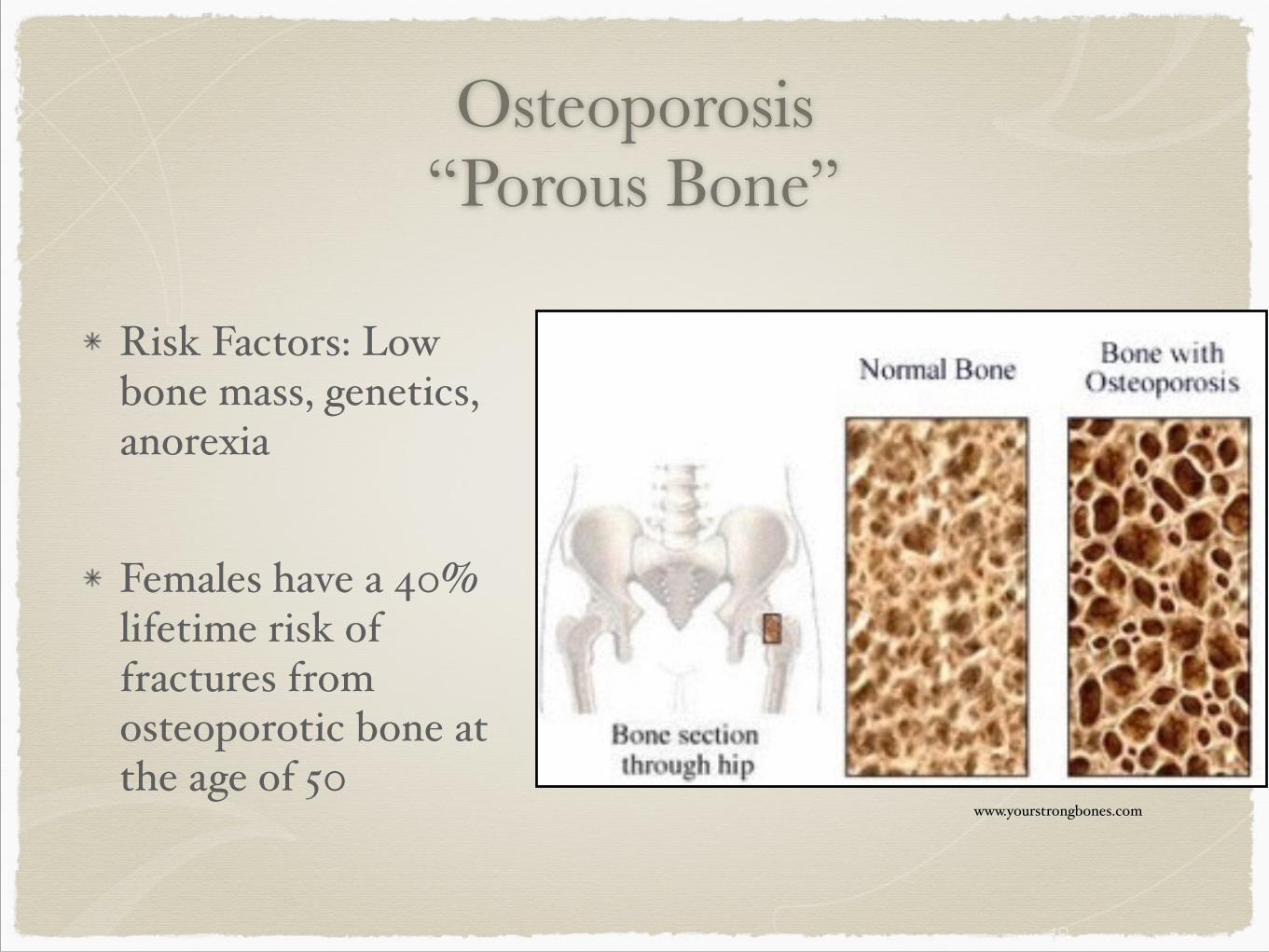
Osteoporosis “Porous Bone”
!Risk Factors: Low bone mass, genetics, anorexia$
!
Females have a 40% lifetime risk of fractures from osteoporotic bone at the age of 50
40
www.yourstrongbones.com
Bone DensitometryThe purpose of bone densitometry is to facilitate the diagnosis of osteoporosis by detecting low bone mass. $
DEXA (spine, hip, forearm) most common$QCT (spine, forearm)$SXA (heel, forearm)$RA (hand)
41
Normal bone: T-score better than -1. $Osteopenia: T-score between -1 and -2.5 $
Osteoporosis: T-score less than -2.5 $
T-SCORE: number of standard deviations below the average for a young adult at peak bone density.