histeroscopia e infertilidad: indicaciones y...
TRANSCRIPT

HISTEROSCOPIA E INFERTILIDAD: INDICACIONES Y COMPLICACIONES
Gíneco-Obstetra
Máster en Reproducción Humana IVI - España
Med. Asistente del Servicio de Medicina Reproductiva del INMP
Dr. Marco Garnique Moncada
IMPACTO
FÍSICO.
PSICOLÓGICO.
ECONÓMICO.
SOCIAL.
The impact of social relations among men and women in fertility treatment on the decision to terminate treatment D Vassard, R Lund, A Pinborg, J Boivin, L Schmidt - Human reproduction, 2012 - ESHRE
Hasta hace poco, las
PAREJAS INFÉRTILES se
veían OBLIGADAS A
ACEPTAR SU CONDICIÓN o
en su defecto a optar por la
ADOPCIÓN.
Avances científicos, médicos y técnicos han logrado
devolver a estas parejas la esperanza…
• Una estimación conservadora permite asumir que hasta el 10% de las parejas presentan algún problema de fertilidad a lo largo de su vida reproductiva, lo que representaría de 50 a 80 millones de personas en todo el mundo
UNDP/UNFPA/WHO/World Bank. Development and research training in Human Reproduction porgram
EVALUACIÓN DE LA PAREJA INFÉRTIL
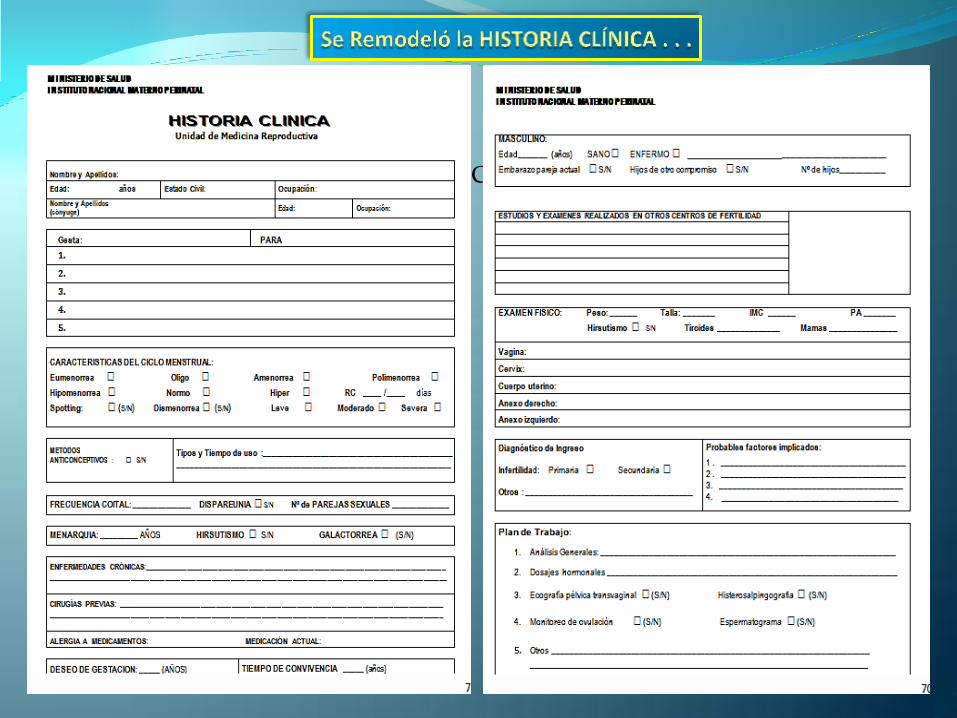
PONER LA HC DE INFERTILIDAD
HISTORIA CLÍNICA : ANAMNESIS - EXAMEN FÍSICO
LABORATORIO : HORMONAS – OTROS
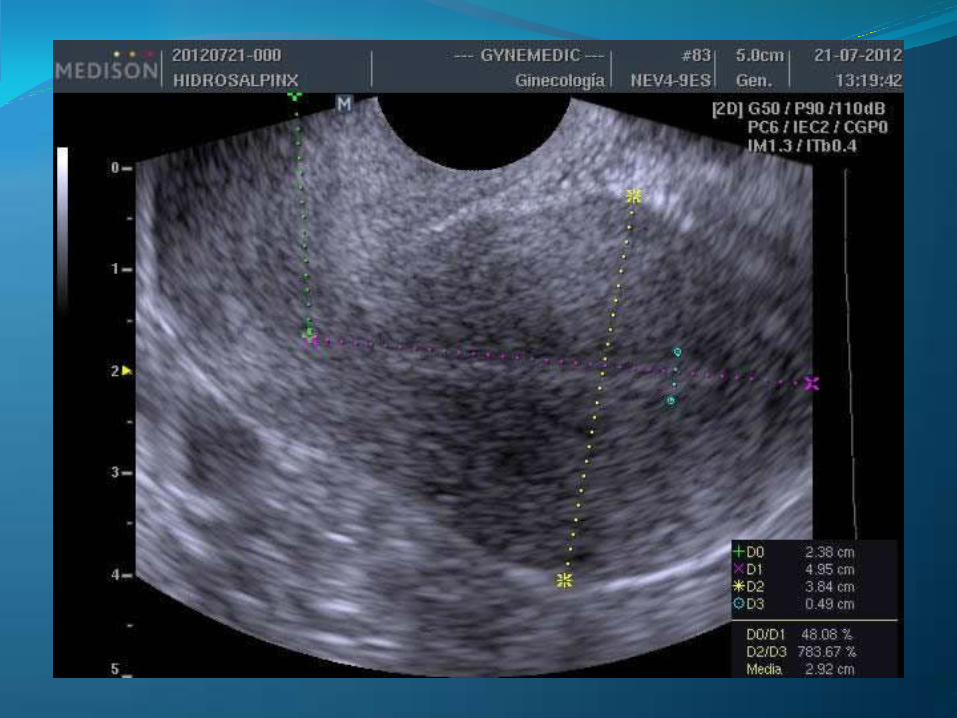
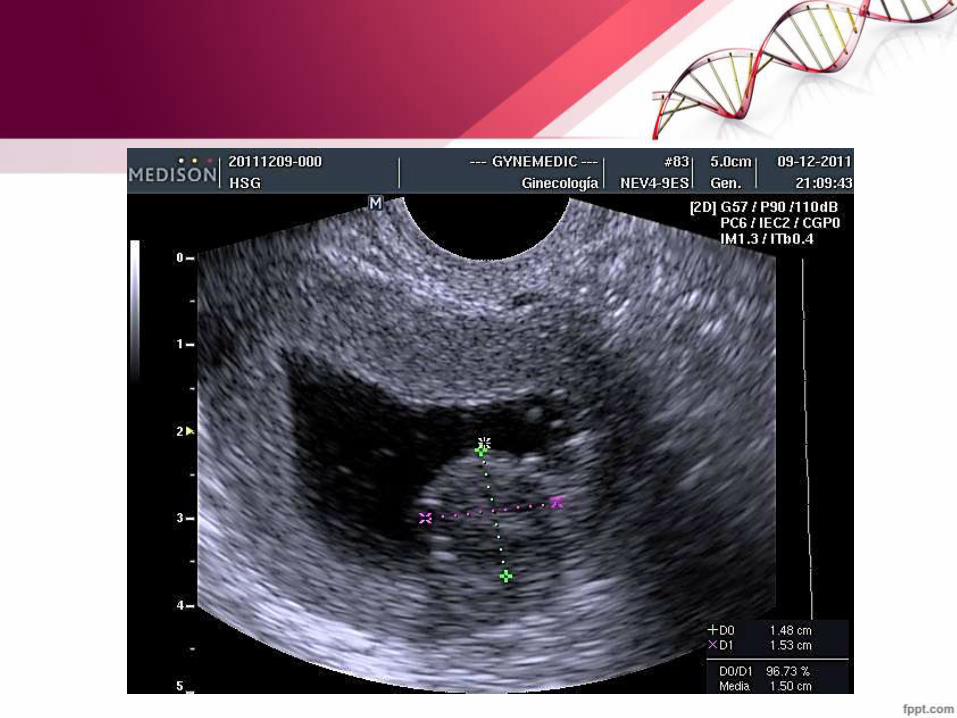
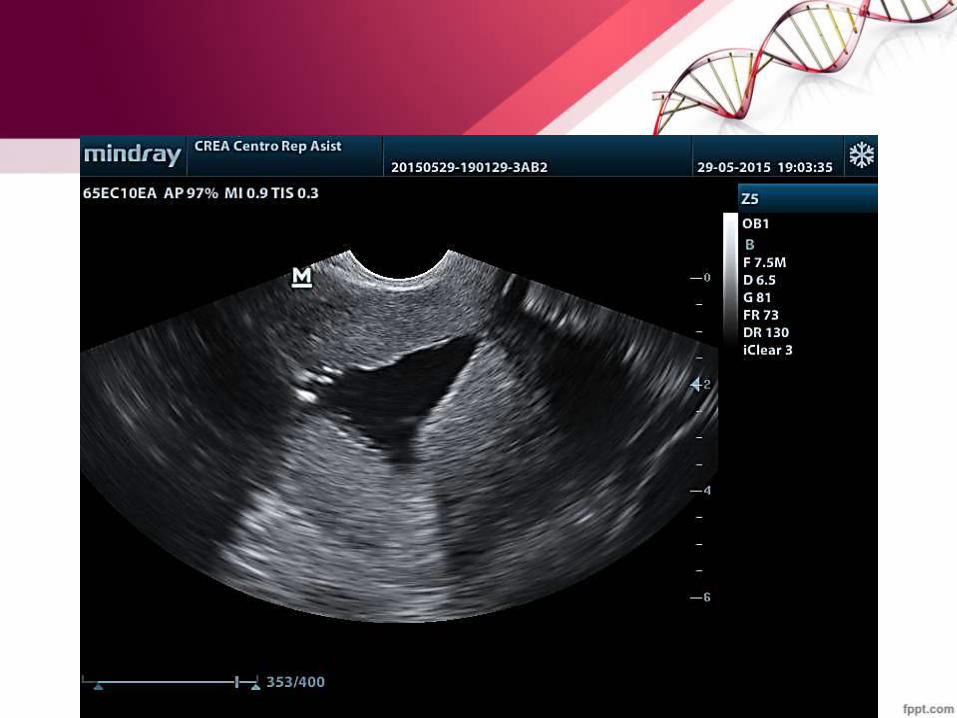
ECOGRAFÍA: 2D / 3D / HISTEROSONOGRAFÍA.
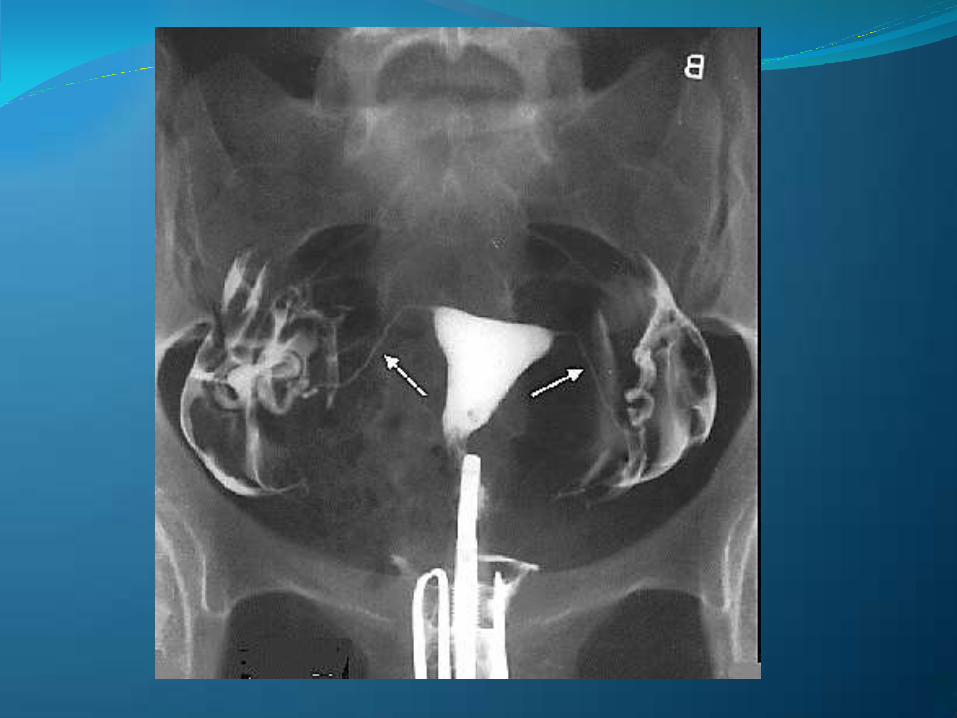
RADIOLOGÍA: HISTEROSALPINGOGRAFÍA.
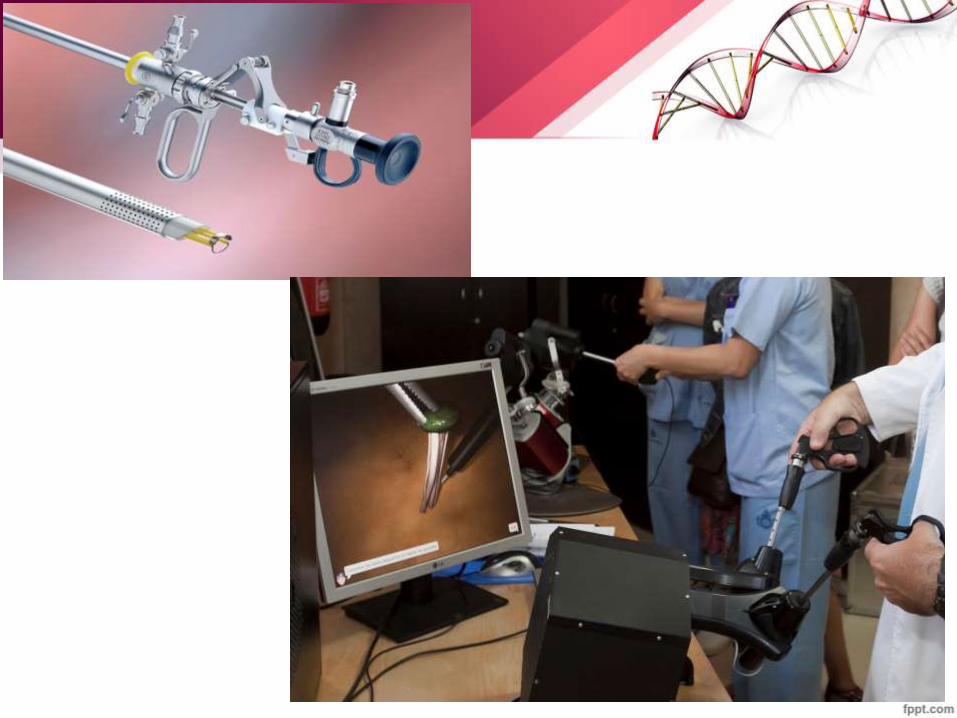
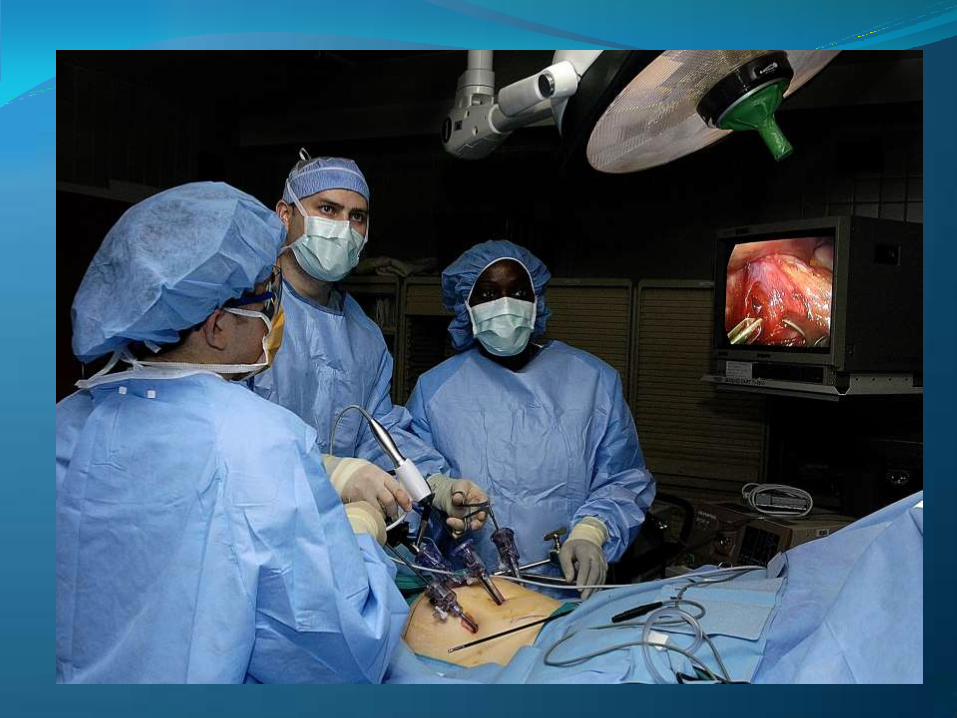
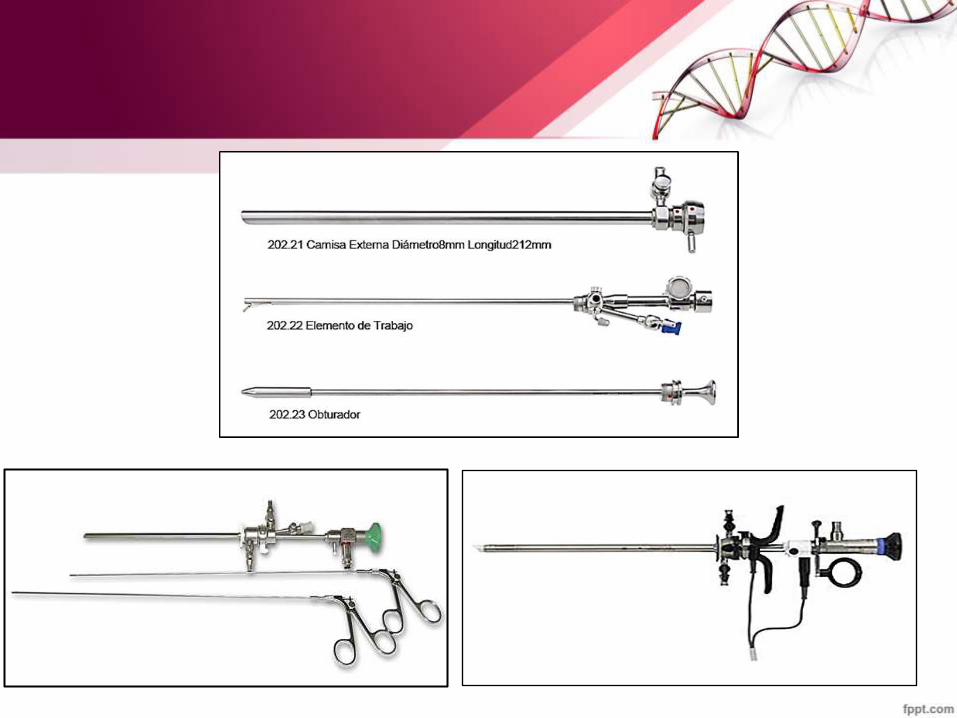
ENDOSCOPIA GINECOLÓGICA:
HISTEROSCOPÍA - LAPAROSCOPÍA
RMN.


HISTEROSONOGRAFÍA

EN BUSCA DE PATOLOGÍA ENDOCAVITARIA . . .
PATOLOGÍA ENDOCAVITARIA
• Cavidad Hipoplásica.
• Cavidad Dismórfica congénita o adquirida
• Sinequias Endocavitarias.
• Tumores Endocavitarios:
– Pólipos
– Hiperplasia Endometrial
– Miomas Submucosos
– Miomas Intramurales que deforman de la Línea Endometrial.
CAVIDAD HIPOLPLÁSICA
• Volumen endocavitario entre 3-9 cc.
• Cirugía de Remodelación de la Cavidad Uterina.
• Histeroscopia Quirúrgica Asistida por Laparoscopía y/o Ecografía
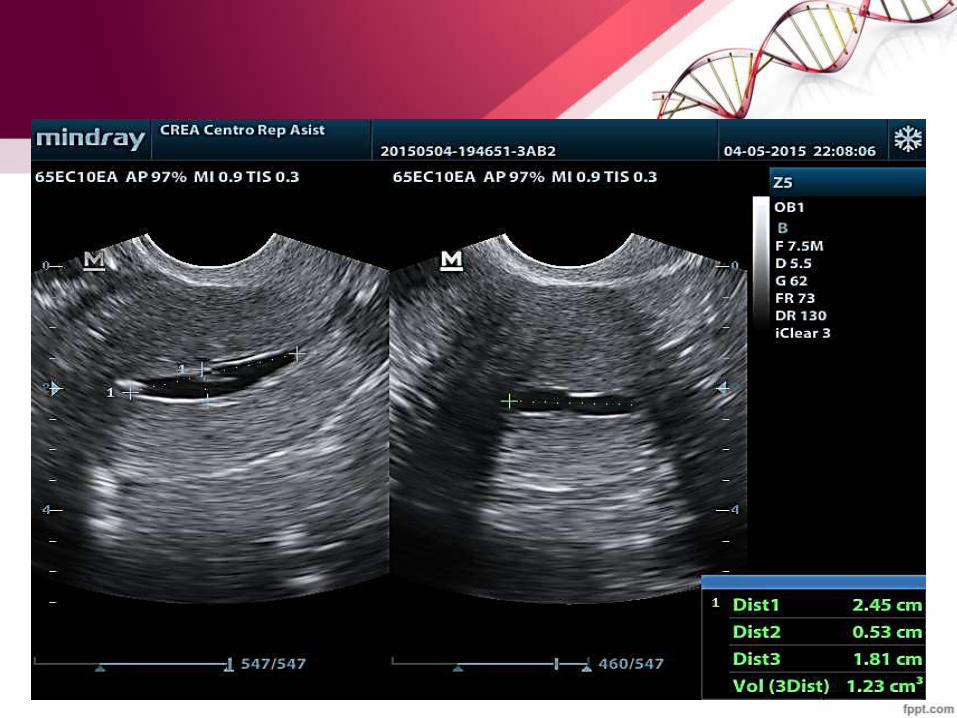
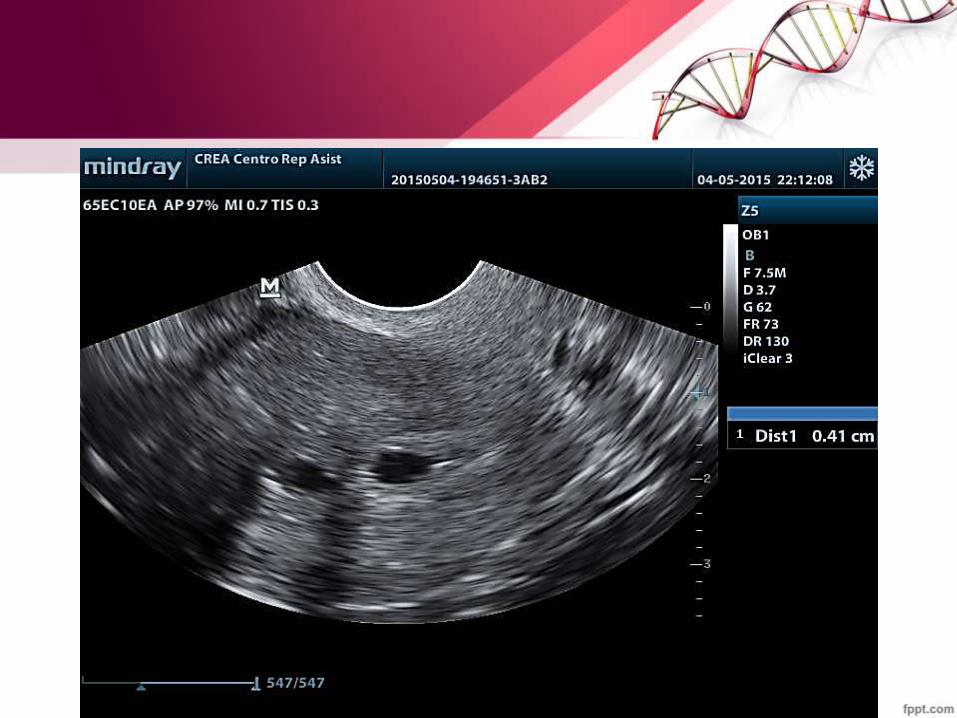
SINEQUIAS ENDOCAITARIAS
• Pueden ser Laxas – Rígidas
• Limitadas - Extensas
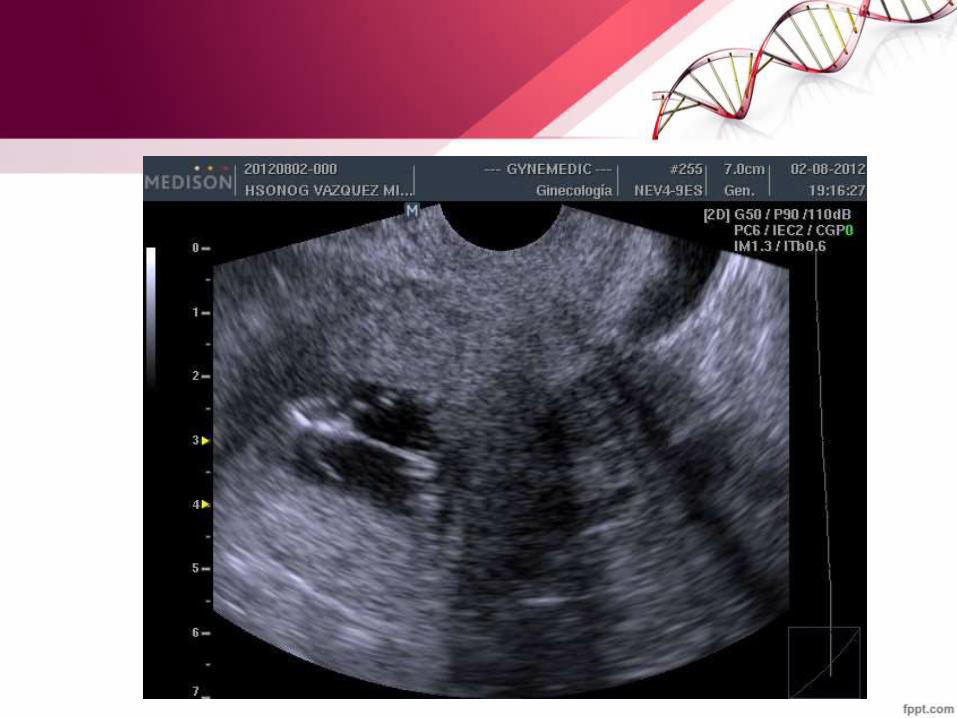
TUMORES ENDOCAVITARIOS
– Pólipos
– Hiperplasia Endometrial
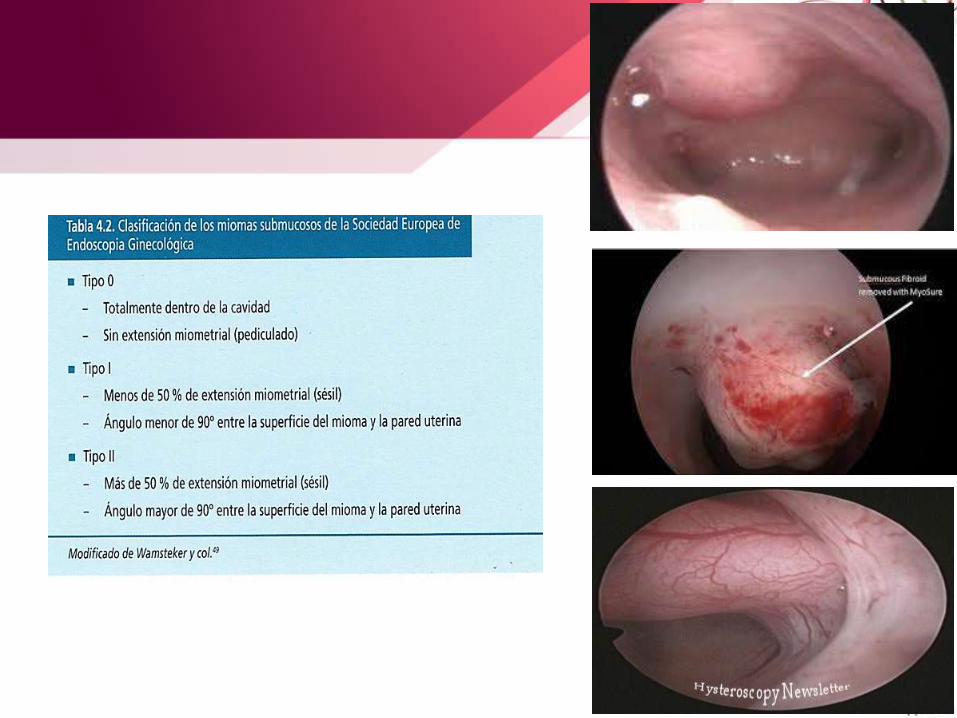
– Miomas Submucosos
– Miomas Intramurales que deforman de la Línea Endometrial.


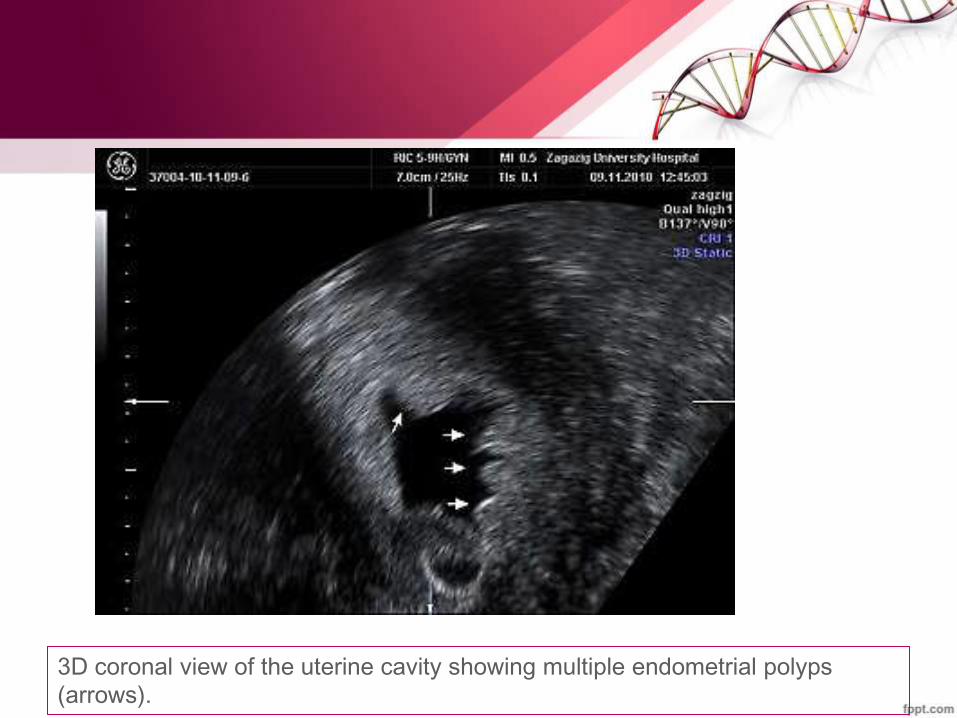
3D coronal view of the uterine cavity showing multiple endometrial polyps
(arrows).

Qué es esto ?

INFERTILIDAD I° O II°
FACTOR CERVICAL..
FACTOR UTERINO.
FACTOR TUBO PERITONEAL.
FACTOR OVULATORIO.
FACTOR METABÓLICO.
FACTOR INMUNOLÓGICO.
INFERTALIDAD DE CAUSA DESCONOCIDA.
INFERTILIDAD I° O II°
FACTOR CERVICAL: cervicitis, …
FACTOR UTERINO: Miomas, sinequias, tabiques, …
FACTOR TUBO PERITONEAL: Hidrosalpinx, obstrucción,…
FACTOR OVULATORIO: SOP, fase lútea acortada, anómala, …
FACTOR METABÓLICO: hipert, hipot, DM, …
FACTOR INMUNOLÓGICO: SAF
INFERTALIDAD DE CAUSA DESCONOCIDA: ???
EN ÉSTA CONSULTA YA TENEMOS DX PRECISOS O DE ALTA SOSPECHA DE LA CAUSA DE INFERTILIDAD Y PROCEDEREMOS DE ACUERDO A UN PLAN DE TRABAJO.
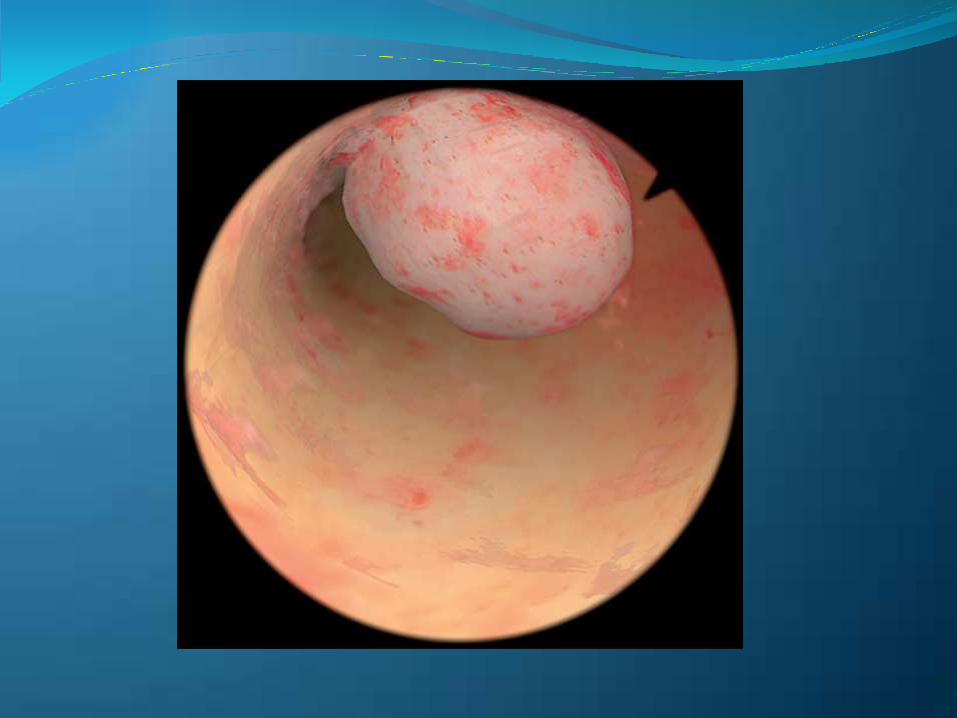

PÓLIPOS ENDOMETRIALES

PÓLIPOS ENDOMETRIALES
• Es el principal problema, hasta 26% mujeres en estudio de por Infertilidad.
• Mx : Distorsión endometrial, Alteraciones contractibilidad, Citoquinas
• Menor Tasa de Embarazo, Mejoran después dela Polipectomía.
Sanders B. Uterine Factors and infertility. J Reprod Med. 2006;51:169-76 Hasegawa E y col. Expression of leukemia inhibitory factor in the endometrium in abnormal Uterine cavities during the implantation window. Fertil Steril. 2012;97(4):953-58

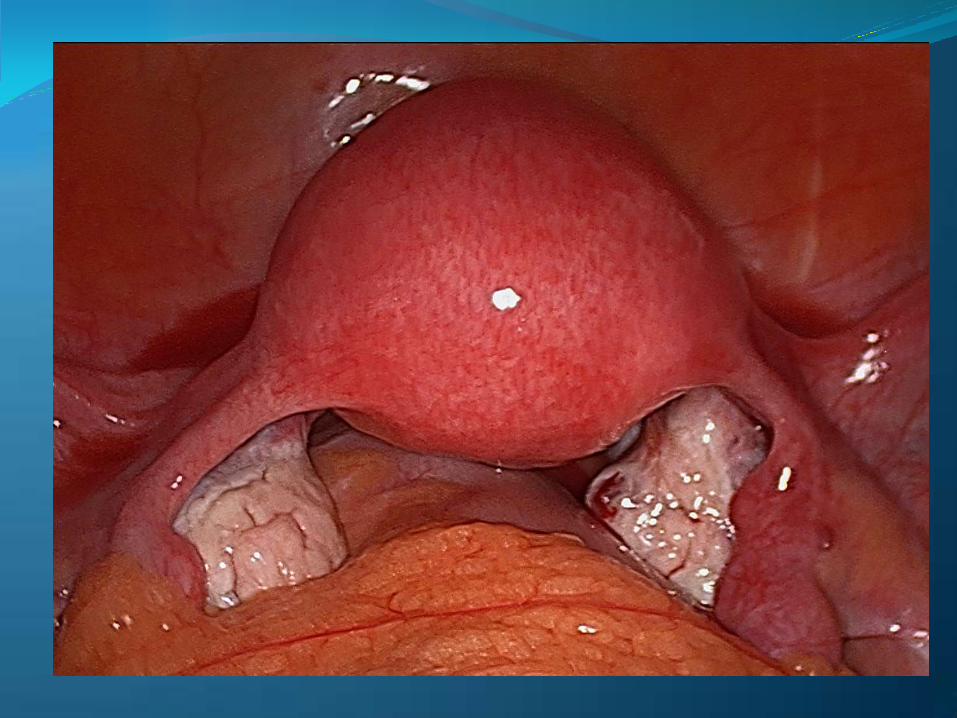
MIOMAS

MIOMAS
• El impacto de los miomas que no deforman la cavidad es aún controversial.
• Es ampliamente aceptado que los miomas submucosos sí afectan la implantación.
• El endometrio con mioma submucoso hay alteración en la expresión de genes y citosinas del endometrio pre implantatorio.
Stovall D y col. Uterine leiomyomas reduce the efficacy of assisted reprodction cycles. Hum Reprod. 1998;13:192-7 Johnson G y col. Uterine leiomyomata and fecundability in the Right from the start study. Hum Reprod.2012:2991-7
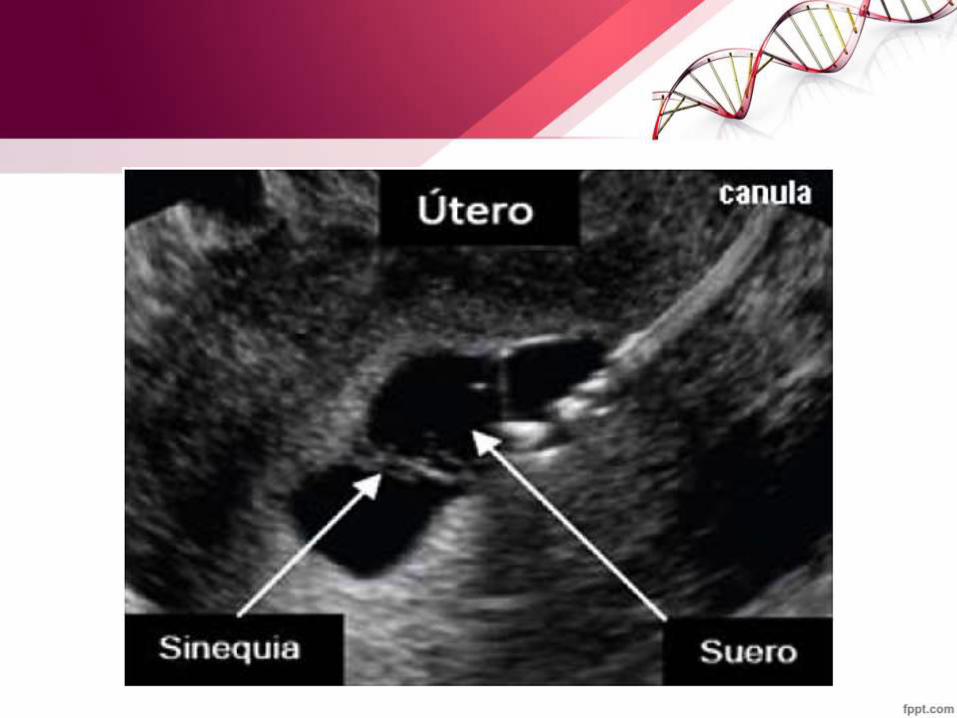
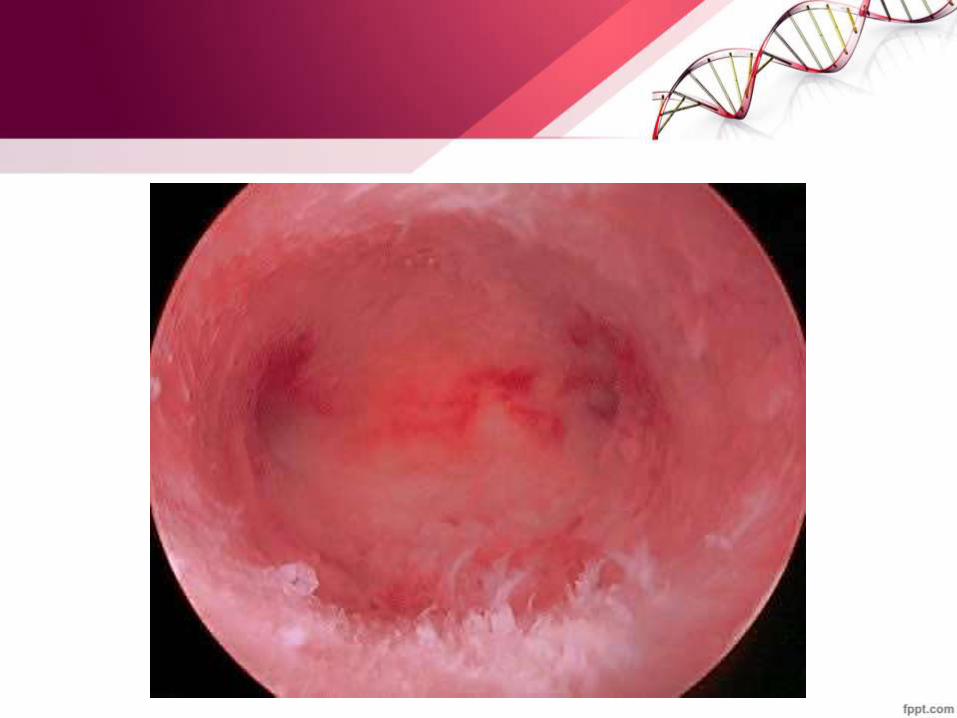
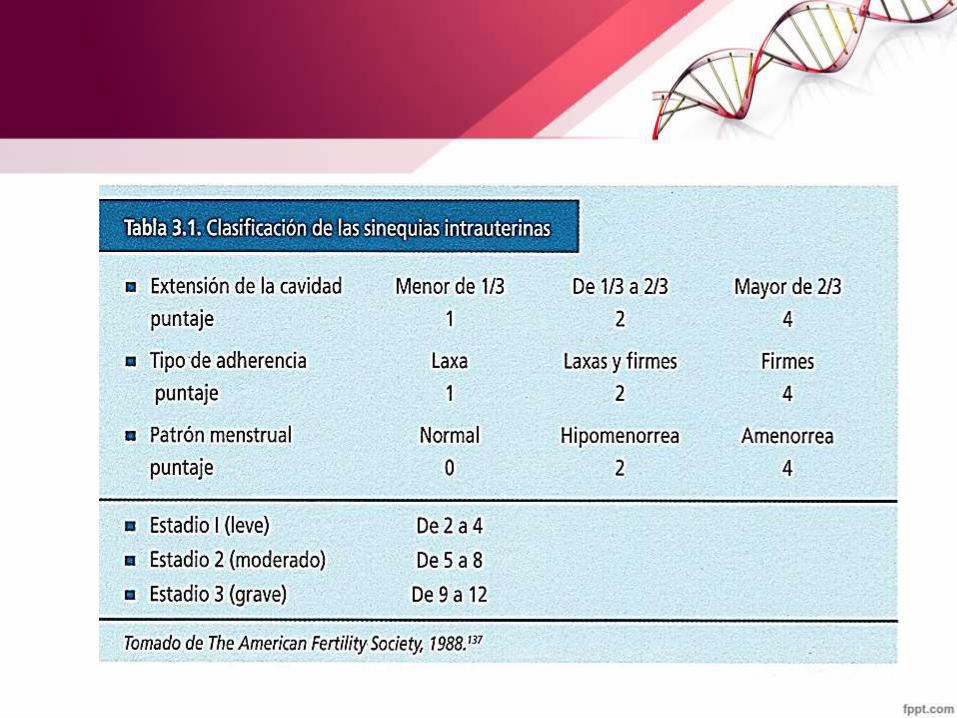
SINEQUIAS
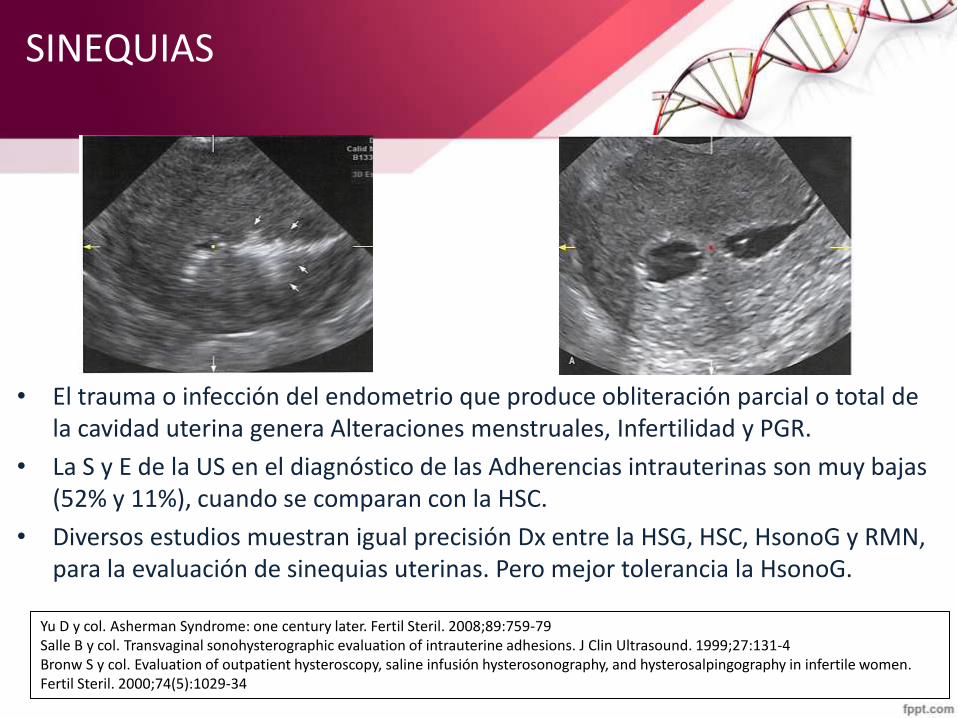
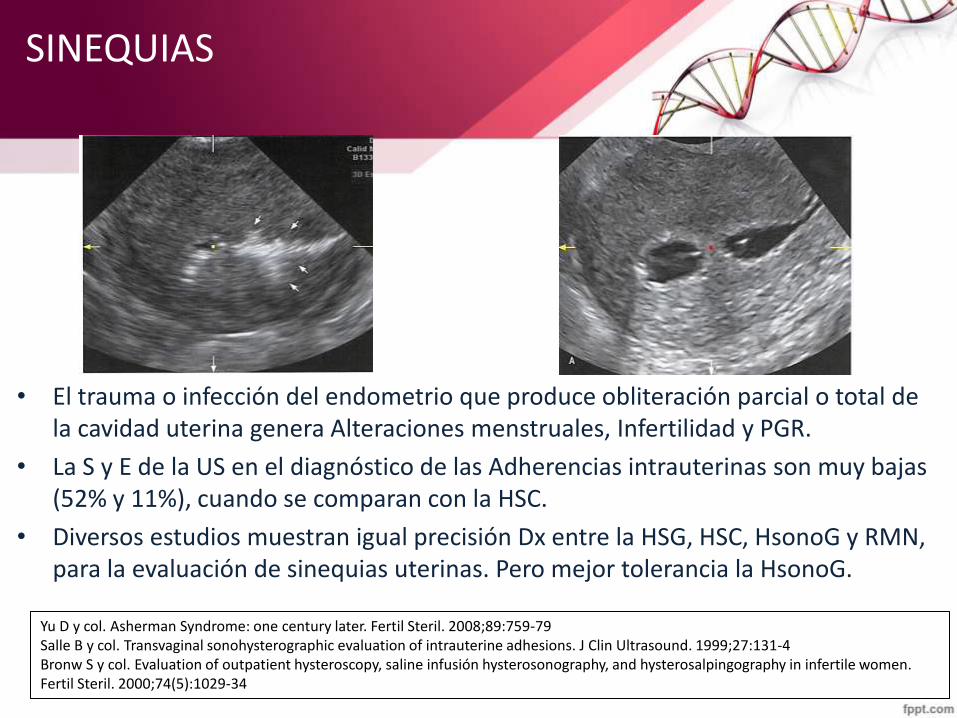
• El trauma o infección del endometrio que produce obliteración parcial o total de la cavidad uterina genera Alteraciones menstruales, Infertilidad y PGR.
• La S y E de la US en el diagnóstico de las Adherencias intrauterinas son muy bajas (52% y 11%), cuando se comparan con la HSC.
• Diversos estudios muestran igual precisión Dx entre la HSG, HSC, HsonoG y RMN, para la evaluación de sinequias uterinas. Pero mejor tolerancia la HsonoG.
Yu D y col. Asherman Syndrome: one century later. Fertil Steril. 2008;89:759-79 Salle B y col. Transvaginal sonohysterographic evaluation of intrauterine adhesions. J Clin Ultrasound. 1999;27:131-4 Bronw S y col. Evaluation of outpatient hysteroscopy, saline infusión hysterosonography, and hysterosalpingography in infertile women. Fertil Steril. 2000;74(5):1029-34
SINEQUIAS
• El trauma o infección del endometrio que produce obliteración parcial o total de la cavidad uterina genera Alteraciones menstruales, Infertilidad y PGR.
• La S y E de la US en el diagnóstico de las Adherencias intrauterinas son muy bajas (52% y 11%), cuando se comparan con la HSC.
• Diversos estudios muestran igual precisión Dx entre la HSG, HSC, HsonoG y RMN, para la evaluación de sinequias uterinas. Pero mejor tolerancia la HsonoG.
Yu D y col. Asherman Syndrome: one century later. Fertil Steril. 2008;89:759-79 Salle B y col. Transvaginal sonohysterographic evaluation of intrauterine adhesions. J Clin Ultrasound. 1999;27:131-4 Bronw S y col. Evaluation of outpatient hysteroscopy, saline infusión hysterosonography, and hysterosalpingography in infertile women. Fertil Steril. 2000;74(5):1029-34
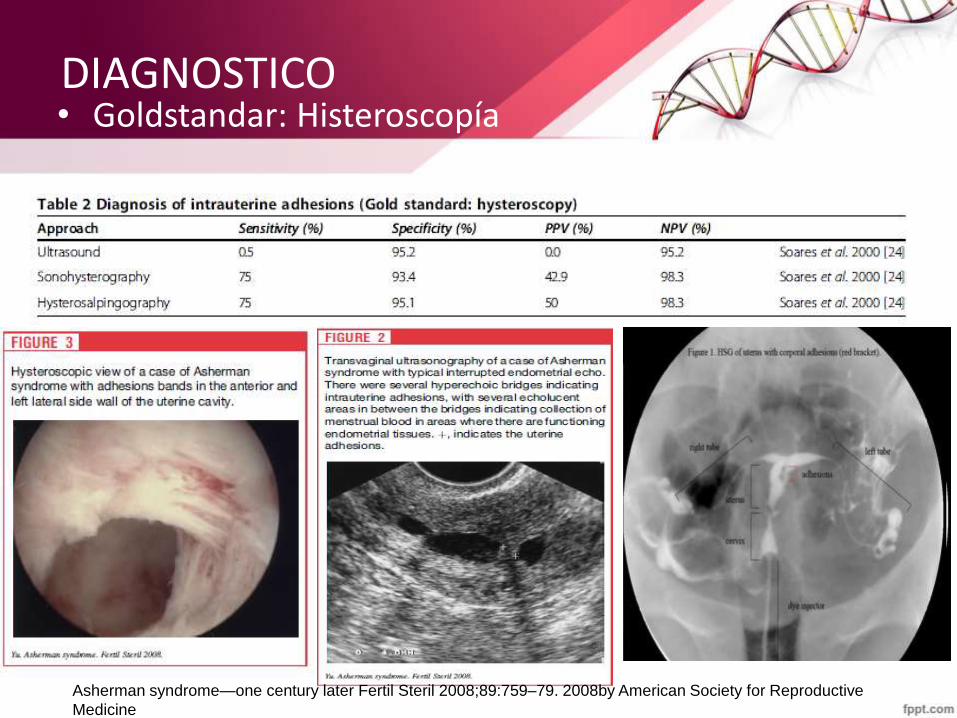
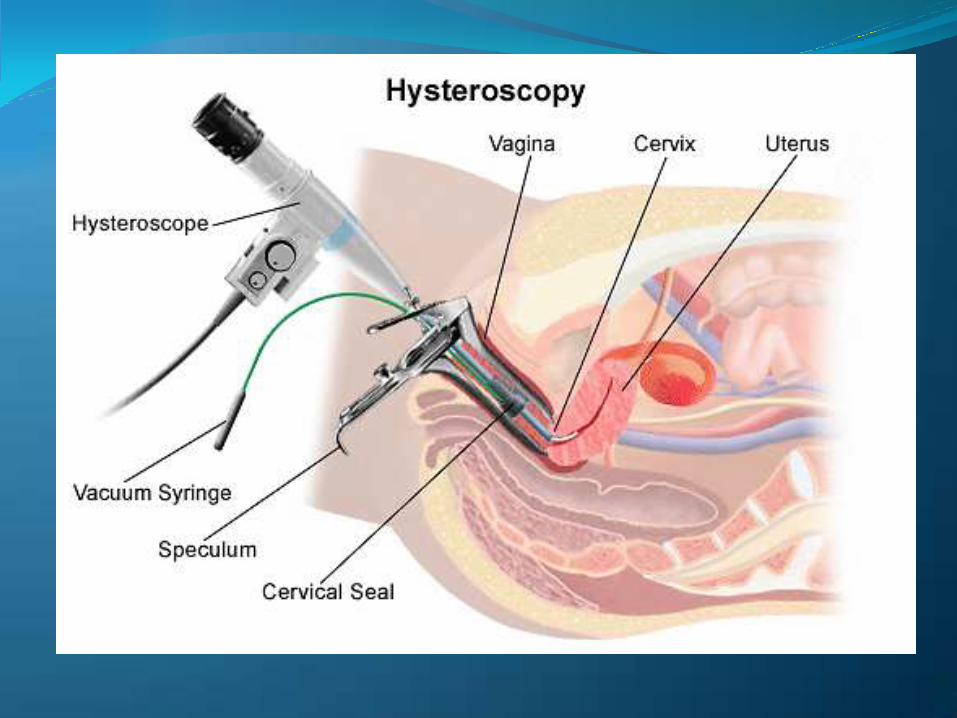
DIAGNOSTICO • Goldstandar: Histeroscopía
Asherman syndrome—one century later Fertil Steril 2008;89:759–79. 2008by American Society for Reproductive
Medicine
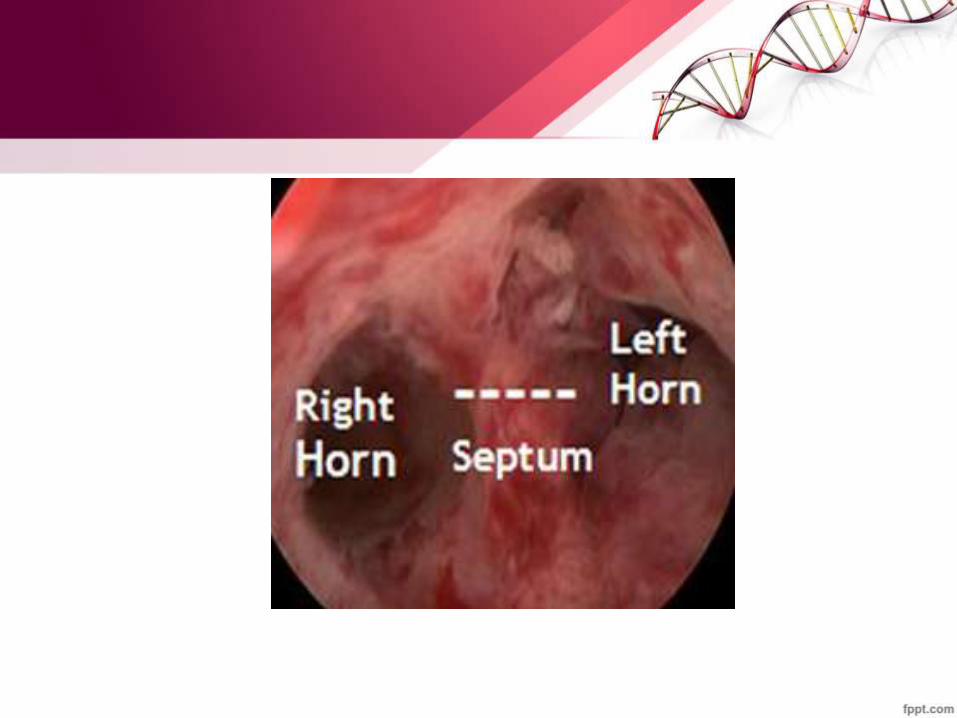

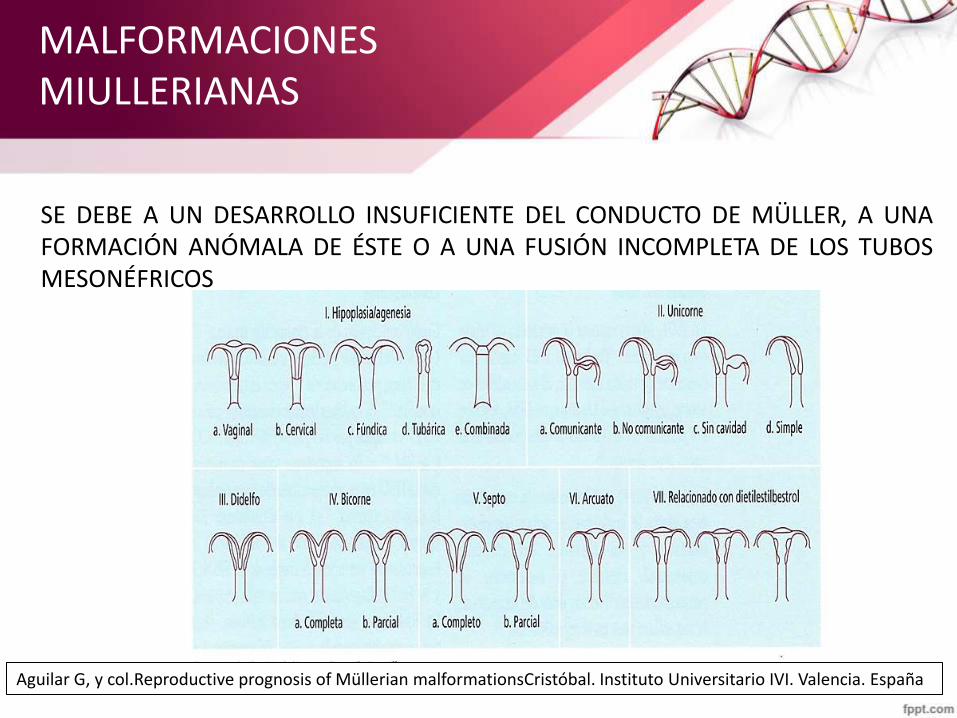
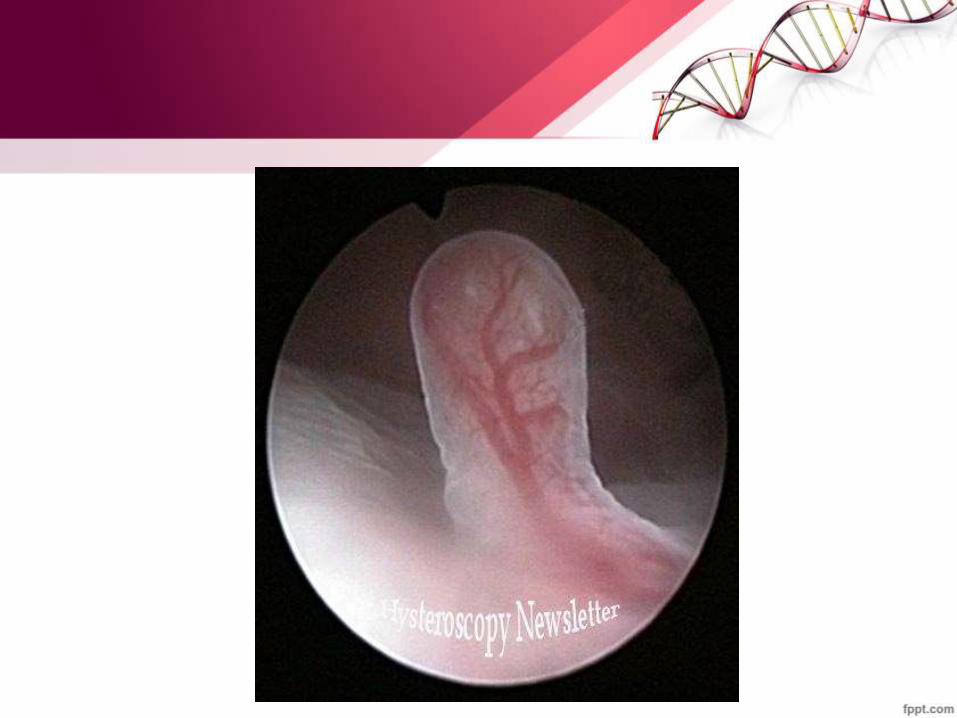
MALFORMACIONES MIULLERIANAS
SE DEBE A UN DESARROLLO INSUFICIENTE DEL CONDUCTO DE MÜLLER, A UNA FORMACIÓN ANÓMALA DE ÉSTE O A UNA FUSIÓN INCOMPLETA DE LOS TUBOS MESONÉFRICOS
Aguilar G, y col.Reproductive prognosis of Müllerian malformationsCristóbal. Instituto Universitario IVI. Valencia. España
FISIOPATOLOGÍA MALFORMACIONES UTERINAS
• Defecto de la vascularización del tabique que impediría una correcta implantación y el buen desarrollo del cigoto.
• Constricción de la cavidad uterina que dificultaría un desarrollo normal y adecuado del embarazo.
• La incompetencia cervicoístmica que obstacularizaría el mantenimiento de una correcta gestación
• Presencia de una mayor decidualización endometrial.
• Pérdida de la masa muscular miometrial.
*Golan A, Langer R, Bukovsky I, Caspi E. Congenital anomalies of the mullerian system. Fertil Steril. 1989;51:747-55. *Heinonen PK, Saarikoski S, Pystynen P. Reproductive performance of women with uterine anomalies. An evaluation of 182 cases. Acta Obstet Gynecol Scand. 1982;61:157-62
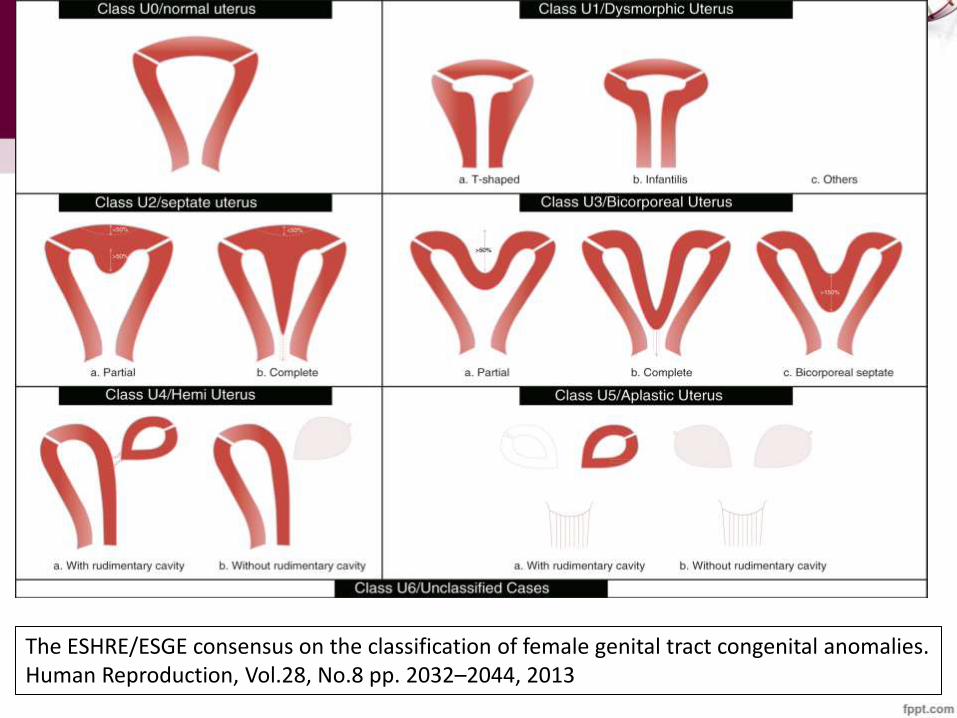
The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Human Reproduction, Vol.28, No.8 pp. 2032–2044, 2013
QUÉ IMPLICANCIAS TENDRÍA NO REALIZARLA O TENER UN DIAGNÓSTICO ERRADO EN INFERTILIDAD ?
• ALTO COSTO CUANDO NO SE DX. PATOLOGÍA ENDOCAVITARIA EN TRAAC: – Estimulación Ovárica, Aspiración Ovocitaria, Fertilización y
Transferencia de Embriones. – Congelación de los Embriones y posterior Transferencia
Diferida. – El procedimiento extra que tendrá que realizarse la
paciente al no tener un diagnóstico previo oportuno. • CONGELACIÓN, MANTENIMIENTO Y DESCONGELACIÓN DE
LOS EMBRIONES, ADEMÁS DE UNA PREPARACIÓN ENDOMETRIAL, para transferencia diferida.
• Por lo tanto hay UN GRAN IMPACTO ECONÓMICO Y EMOCIONAL, para la pareja.

ENTREVISTA MÍNIMA

ninguna Resolución Institucional y las cuales tampoco tenían chance de realizarlos particularmente por motivos Económicos y esto genera un gran impacto psicológico para la pareja, indignación y sentimiento de injusticia y desigualdad
por carecer de posibilidades económicas para realizar este tipo tratamientos.
IMPACTO
FÍSICO.
PSICOLÓGICO.
ECONÓMICO.
SOCIAL.
The impact of social relations among men and women in fertility treatment on the decision to terminate treatment D Vassard, R Lund, A Pinborg, J Boivin, L Schmidt - Human reproduction, 2012 - ESHRE

Procedimientos nuevos en SOP

Equipo de Trabajo
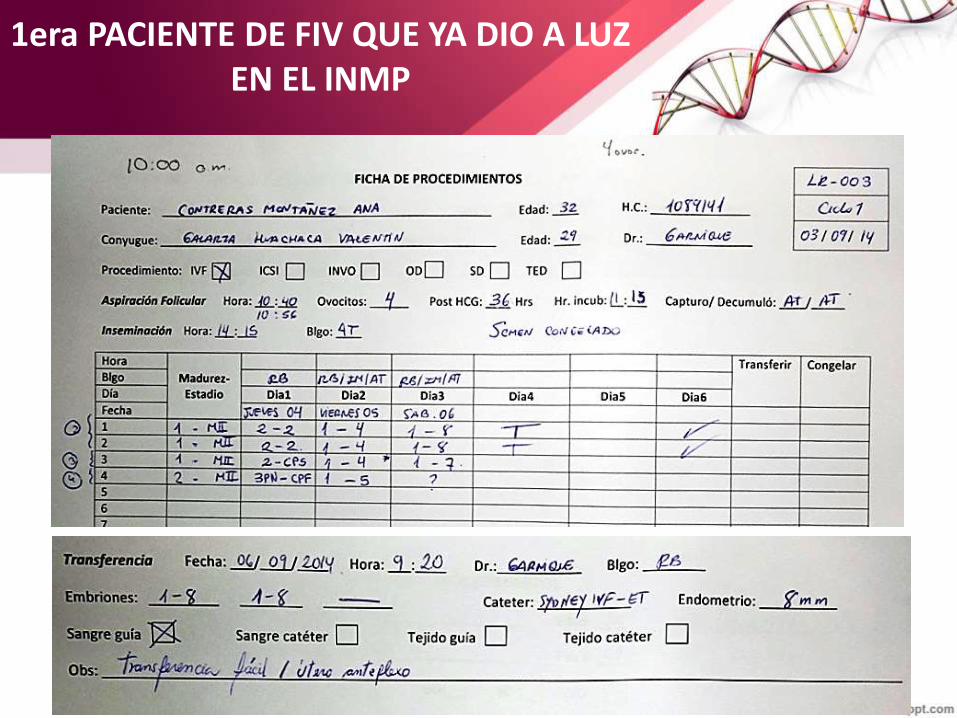
1era PACIENTE DE FIV QUE YA DIO A LUZ EN EL INMP
• ACM de 32 años
• Con TE 5 años
• Operada por cirugía tubárica.
• INDICACIÓN: FIV / TE:
– Estimulación Ovárica
– Aspiración Ovocitaria 3/9/2014
– Transferencia Embrionaria 6/9/2014
EMBARAZO DOBLE
CESÁREA EL 5/5/2015: VARÓN 2400
MUJER 2700
1era PACIENTE DE FIV QUE YA DIO A LUZ EN EL INMP