hiv-1 resistance - implications for clinicians joseph j. eron jr., md professor of medicine...
TRANSCRIPT
HIV-1 Resistance - Implications For Clinicians
Joseph J. Eron Jr., MD
Professor of Medicine
University of North Carolina
Disclosures
Types of Resistance Tests
Genotype and Phenotype
Types of Resistance Tests
• Genotype– HIV gene sequencing of the patient’s virus to detect
mutations known to confer drug resistance
• Phenotype– Measures ability of a recombinant virus derived from the
patient sample to grow in different concentrations of antiretroviral drugs
Hirsch et al. Clin Infect Dis. 2003;37:113-28.
Interpretation of Genotypic Assays
• Is an indirect measure of resistance– Requires knowledge of which mutation are associated with a
change in susceptibility
• Expert advice– May not be available– Experts’ views may be inconsistent
• Rules-based algorithms– Provided by most labs, third-party sites– Need regular updating
• Virtual Phenotype (VircoType)– Phenotypic information using genotype– Database of matched genotypes and phenotypes
Question: What is the significance of the RT mutation K103N?
Confers resistance to 3TC/FTC
Confers resistance to tenofovir
Confers resistance to efavirenz
All of the above
None of the above
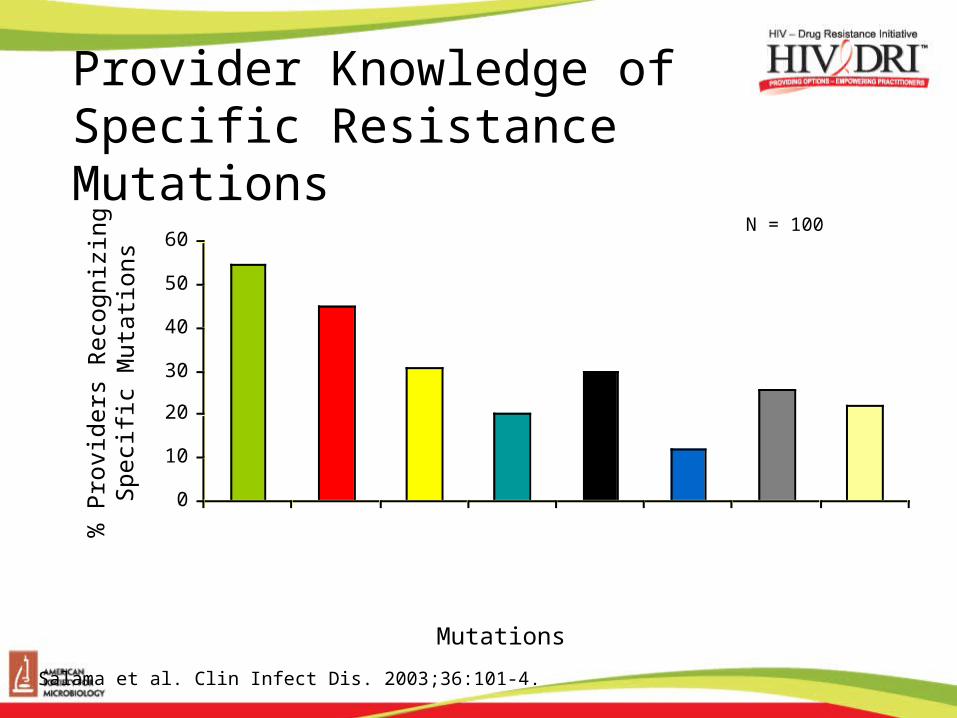
Provider Knowledge of Specific Resistance Mutations
0
10
20
30
40
50
60
3TC:184VAny NNRTIAny ABC > 2 ABC
1 TAM> 2 TAMs
NFV:30 or 90Pan NRTI
Mutations
% P
rovi
ders
Rec
ogni
z ing
Spe
cific
Mut
atio
ns
Salama et al. Clin Infect Dis. 2003;36:101-4.
N = 100
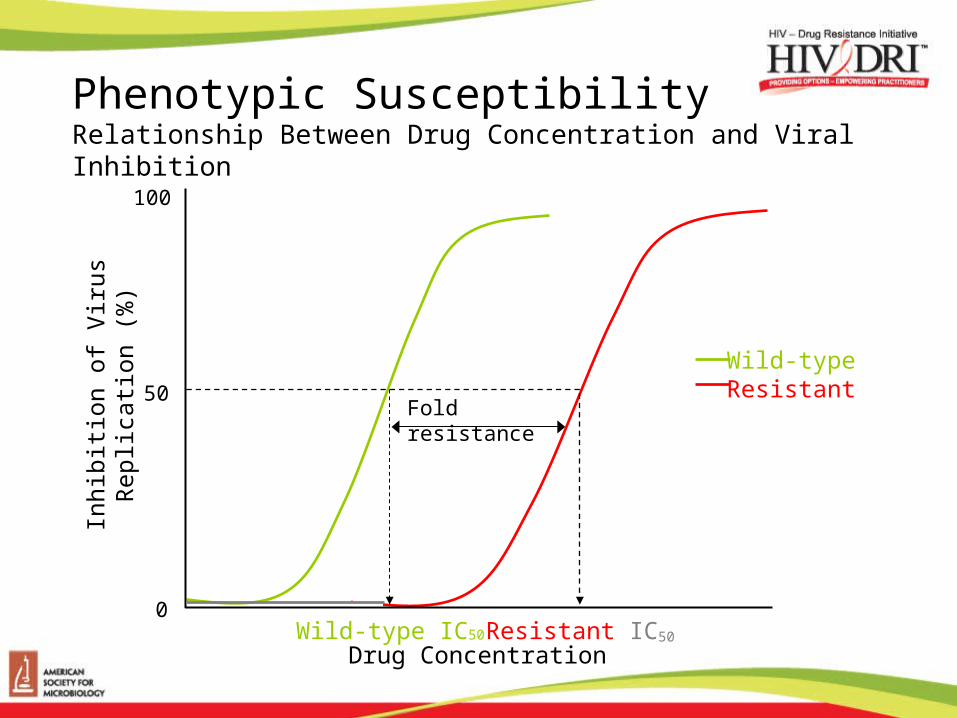
Phenotypic SusceptibilityRelationship Between Drug Concentration and Viral Inhibition
Inhi
bitio
n of
Viru
s R
eplic
atio
n (%
)
50
0
100
Fold resistance
Wild-type IC50 Resistant IC50
Wild-typeResistant
Drug Concentration
Interpretation of Phenotypic Assays• Results reported as IC50 or fold-change (FC)
compared with IC50 of wild-type virus
• Individual results provided for each drug
• Thresholds to define reduced susceptibility– Biologic cutoff: based on biologic variations in treatment-
naïve patients (usually 2 SD > median)– Clinical cutoff:
• As good as clinical data used to estimate cut points• Resistance is a continuum – precise breakpoints unlikely• Two relevant breaks?
– Decreased response and – Minimal response
Question:Resistance testing should be obtained in which treatment naïve patients?
Only in HIV infected patients with acute infection
Individuals thought to have been infected within the last 2 years
All treatment naïve patients
Transmitted ARV Resistance
Clinically Important in the Developed World
Surveillance Essential in the Developing World
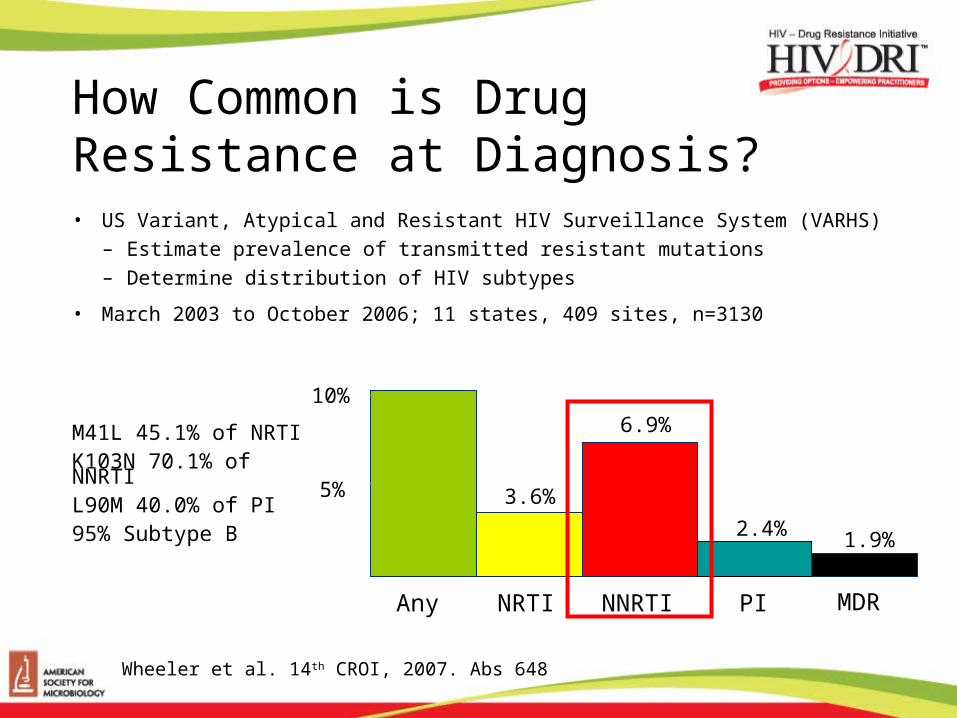
How Common is Drug Resistance at Diagnosis?• US Variant, Atypical and Resistant HIV Surveillance System (VARHS)
– Estimate prevalence of transmitted resistant mutations– Determine distribution of HIV subtypes
• March 2003 to October 2006; 11 states, 409 sites, n=3130
10%
5%
Any NRTI NNRTI PI MDR
M41L 45.1% of NRTIK103N 70.1% of NNRTIL90M 40.0% of PI95% Subtype B
Wheeler et al. 14th CROI, 2007. Abs 648
6.9%
3.6%
2.4% 1.9%
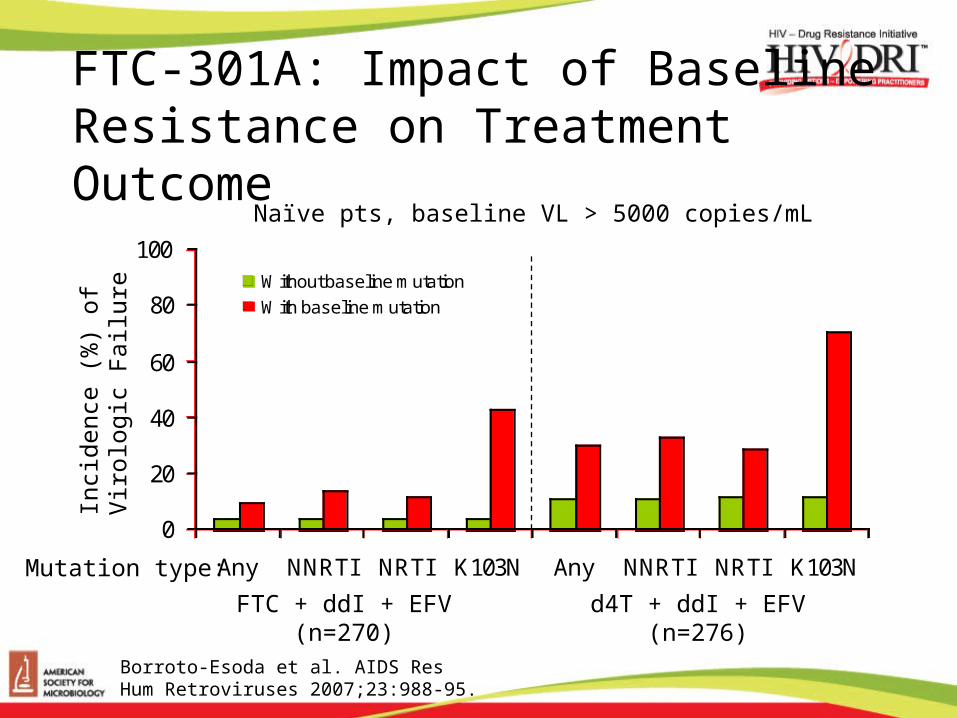
FTC-301A: Impact of Baseline Resistance on Treatment Outcome
0
20
40
60
80
100
Any NNRTI NRTI K103N Any NNRTI NRTI K103N
Without baseline mutation
With baseline mutation
Borroto-Esoda et al. AIDS Res Hum Retroviruses 2007;23:988-95.
Mutation type:
Naïve pts, baseline VL > 5000 copies/mL
FTC + ddI + EFV(n=270)
d4T + ddI + EFV(n=276)
Inci
denc
e (%
) of
V
irolo
gic
Fai
lure
How Important Are Minority Variants?

Standard Genotype181C
103N
190A
108I
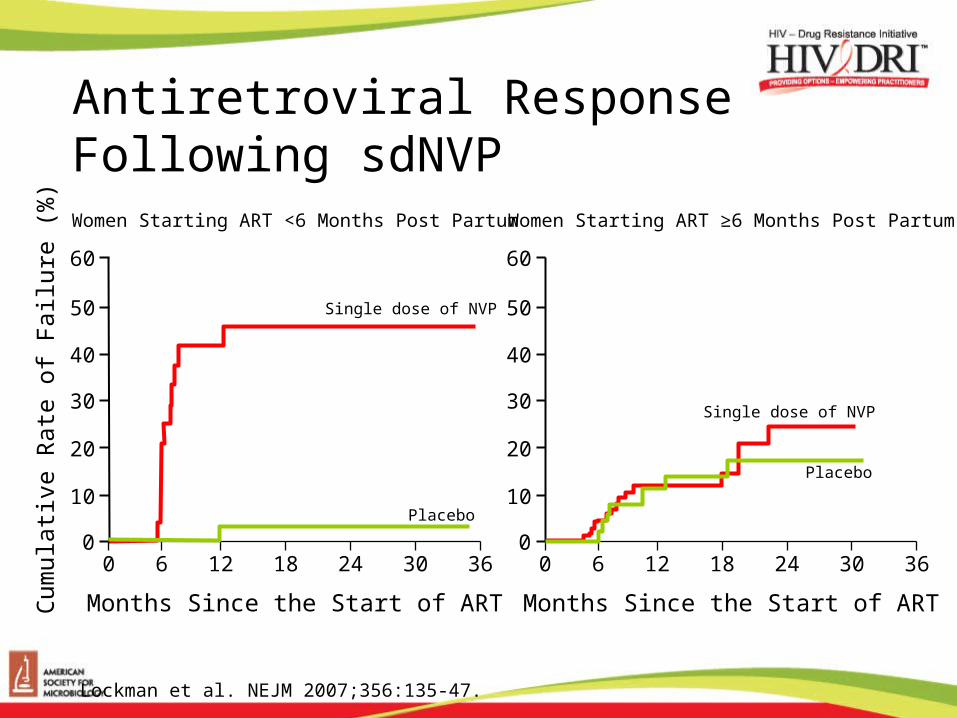
Antiretroviral Response Following sdNVP
Lockman et al. NEJM 2007;356:135-47.
Cum
ulat
ive
Rat
e of
Fai
lure
(%
)
Women Starting ART <6 Months Post Partum
Months Since the Start of ART
Women Starting ART ≥6 Months Post Partum
60
50
40
30
20
10
0Placebo
Single dose of NVP
Placebo
Single dose of NVP
0 6 12 18 24 30 36
Months Since the Start of ART
60
50
40
30
20
10
00 6 12 18 24 30 36
Resistance and Virologic Failure
Multiple Causes of Virologic Failure
Replication in the Presence of Antiretrovirals Results in Resistance

Resistant virus
Social/personal issues
Regimen issues
ToxicitiesPoor potency
Wrong dose
Host genetics
Poor absorption
Rapid clearance
Poor activation
Drug interactions
Insufficient drug level
Viral replication in the presence of drug
Resistant virus
Poor adherence
Treatment-Experienced Patients:ARV Treatment Failure
ART resistance testing. National resource center. Available at: http://www.aidsetc.org/aidsetc?page=et-01-00. Accessed November 29, 2006.
Pre-existing resistance
Management of Virologic Failure in Treatment Experienced Patients• Definition: detectable plasma HIV RNA on therapy
• ‘Is it time to switch therapy?’– Obtain resistance testing– Assess clinical situation
• Adherence• Previous treatment history – ARV tolerability and toxicity
• Balance clinical urgency with availability of active agents including new drugs and expanded access
• New agents – especially those in a new class are likely to have the most activity
New Agents in Existing Classes (PI and NNRTI) Resistance Patterns
Are More ComplexDarunavir
10 codons; 11 substitutions
Tipranavir
16 codons; 21 substitutions
Etravirine
8 codons; 13 substitutions
New Agents in Existing Classes
• Mutations to older agents are likely to be present– Majority variants
– Minority variants
• Some degree of cross resistance can be anticipated– Cross resistance increases with the number and type of
mutations
• The activity of a new agent from a new class is likely to be more predictable even with state of the art resistance testing
New Agents in New Classes
CCR5 Inhibitors
Integrase Inhibitor
CCR5 Inhibitors
• HIV-1 entry into CD4 cells is dependent on a second receptor: CCR5 (R5 viruses) or CXCR4 (X4 viruses)
• Early in HIV disease course most individuals have only R5 virus detectable
• In more advanced disease and highly treatment experienced patients dual tropic virus or mixtures of R5 and X4 viruses are more common
• CCR5 Inhibitors bind to CCR5 blocking entry– Activity only in patients with R5 virus
– Maraviroc and vicriviroc
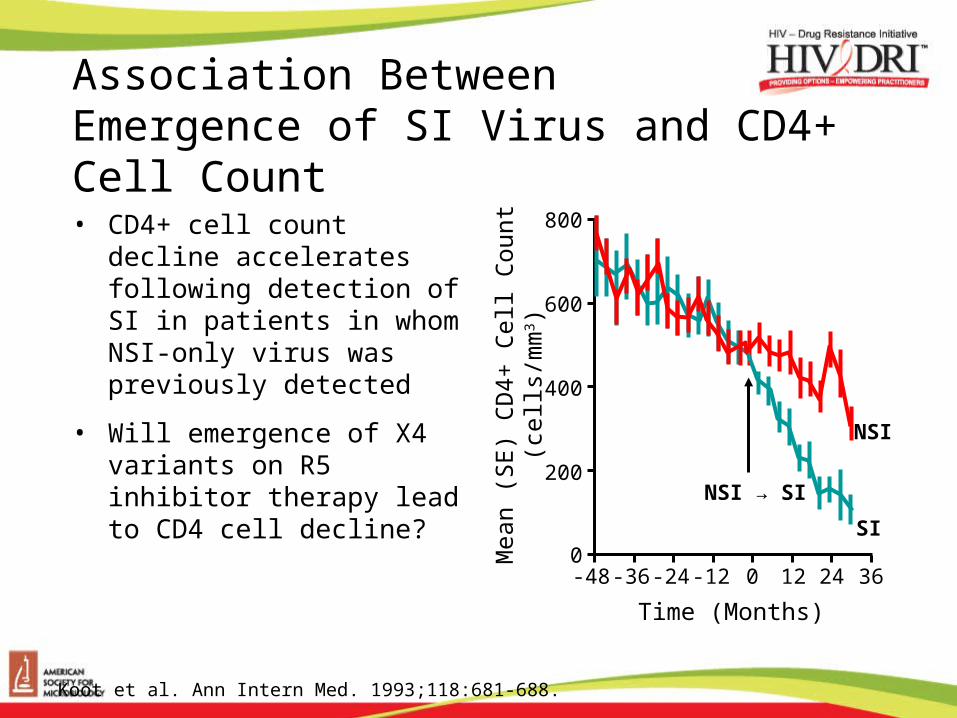
Association Between Emergence of SI Virus and CD4+ Cell Count
• CD4+ cell count decline accelerates following detection of SI in patients in whom NSI-only virus was previously detected
• Will emergence of X4 variants on R5 inhibitor therapy lead to CD4 cell decline?
-36
Mea
n (S
E)
CD
4+ C
ell C
ount
(c
ells
/mm
3 )
Koot et al. Ann Intern Med. 1993;118:681-688.
NSI
NSI → SI
800
600
400
200
-12-24 0 12 24 36
Time (Months)
0-48
SI
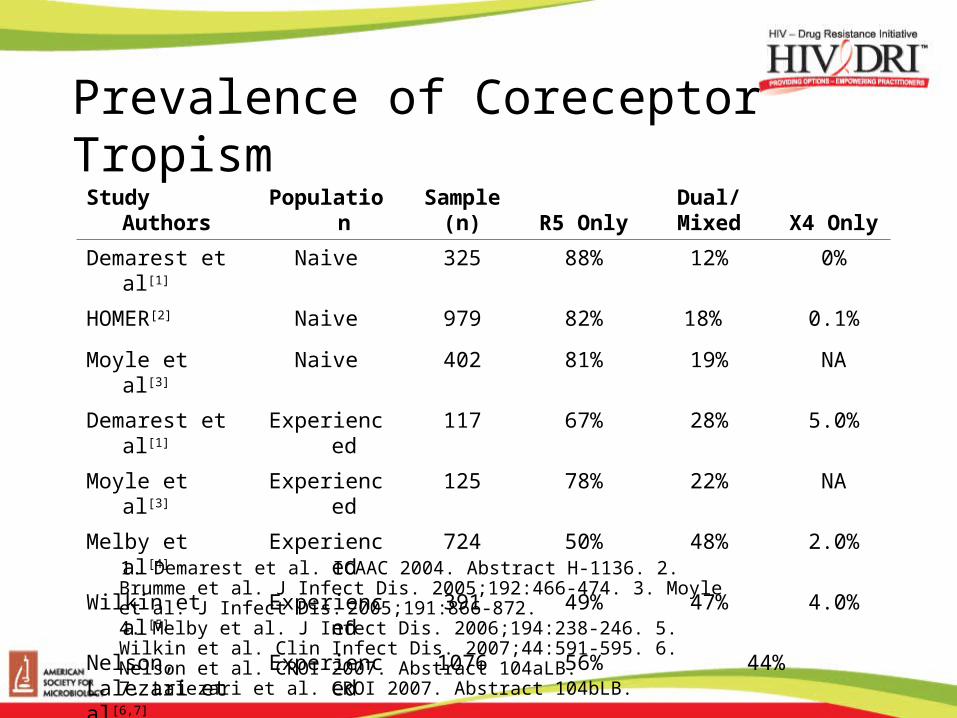
Prevalence of Coreceptor Tropism
1. Demarest et al. ICAAC 2004. Abstract H-1136. 2. Brumme et al. J Infect Dis. 2005;192:466-474. 3. Moyle et al. J Infect Dis. 2005;191:866-872. 4. Melby et al. J Infect Dis. 2006;194:238-246. 5. Wilkin et al. Clin Infect Dis. 2007;44:591-595. 6. Nelson et al. CROI 2007. Abstract 104aLB. 7. Lalezari et al. CROI 2007. Abstract 104bLB.
Study Authors Population Sample (n) R5 Only Dual/Mixed X4 Only
Demarest et al[1] Naive 325 88% 12% 0%
HOMER[2] Naive 979 82% 18% 0.1%
Moyle et al[3] Naive 402 81% 19% NA
Demarest et al[1] Experienced 117 67% 28% 5.0%
Moyle et al[3] Experienced 125 78% 22% NA
Melby et al[4] Experienced 724 50% 48% 2.0%
Wilkin et al[5] Experienced 391 49% 47% 4.0%
Nelson, Lalezari et al[6,7]
Experienced 1076 56% 44%
HIV-1 Resistance to CCR5 Antagonists• Two mechanisms
– Selection for (emergence of) viral variants that use CXCR4 (dual tropic viruses or mixed populations)• Occurs about 2/3 of the time• As yet NOT associated with rapid fall in CD4 cell count
– Alterations (mutations) in HIV gp 120• No Change in viral tropism• Allows virus to use CCR5 with inhibitor bound• Plateau in antiviral effect as opposed to change in IC50
– The drug is unable to fully inhibit virus regardless of concentrations achieved
Integrase Inhibitors
• Integrase mechanism has 3 steps– Association with dsHIV DNA – pre-integration complex
– 3’ processing by integrase enzyme
– Strand transfer of HIV DNA into host chromosome
• Potent inhibitors of stand transfer now in development– Raltegravir – Phase III studies recently presented
– Elvitegravir – Phase II studies
Integrase Inhibitor Resistance
• Primary mutations surround the catalytic site
• Raltegravir– Resistance emerged in 3/4 patients with virologic failure
who had genotype results
– Two major pathways with apparent primary mutations but one or more additional mutations• Likely compensatory for fitness
– Cross resistance between integrase inhibitors currently in development appears likely
Question: In those patients who have experienced virologic failure on multiple regimens including NNRTI, NRTI and PI, which agent is most likely to be fully active?
Darunavir
Etravirine
Tipranavir
Integrase Inhibitors
CCR5 inhibitors
4 and 5