hiv and hepatitis workshop kathleen clanon, md [email protected] 8/06
Post on 21-Dec-2015
214 views
TRANSCRIPT
HIV and Hepatitis Workshop
Kathleen Clanon, MDKathleen Clanon, [email protected]@jba-cht.com
8/068/06
Treatment of HCV in Coinfected Patients
Why Do We Need to Treat HIV/HCV Coinfected Patients?
HCV is common in HIV patients (approx 25-40% in U.S.)
HCV is a more serious disease in coinfected patients than in monoinfected.
HCV has become one of the leading causes of death in the HIV population.
HCV coinfection carries significant morbidity, limits ARV options, decreases QoL.
Epidemiology
About 400,000 HIV/HCV + in U.S.About 400,000 HIV/HCV + in U.S.● overall 30-50% of HIV+ are co-infected
Prevalence of HCV in HIV+ individuals:Prevalence of HCV in HIV+ individuals:● approx. 90% in IVDU● 60-85% in hemophiliacs● 4-8% in HIV+ MSM
HIV/HCV Coinfection
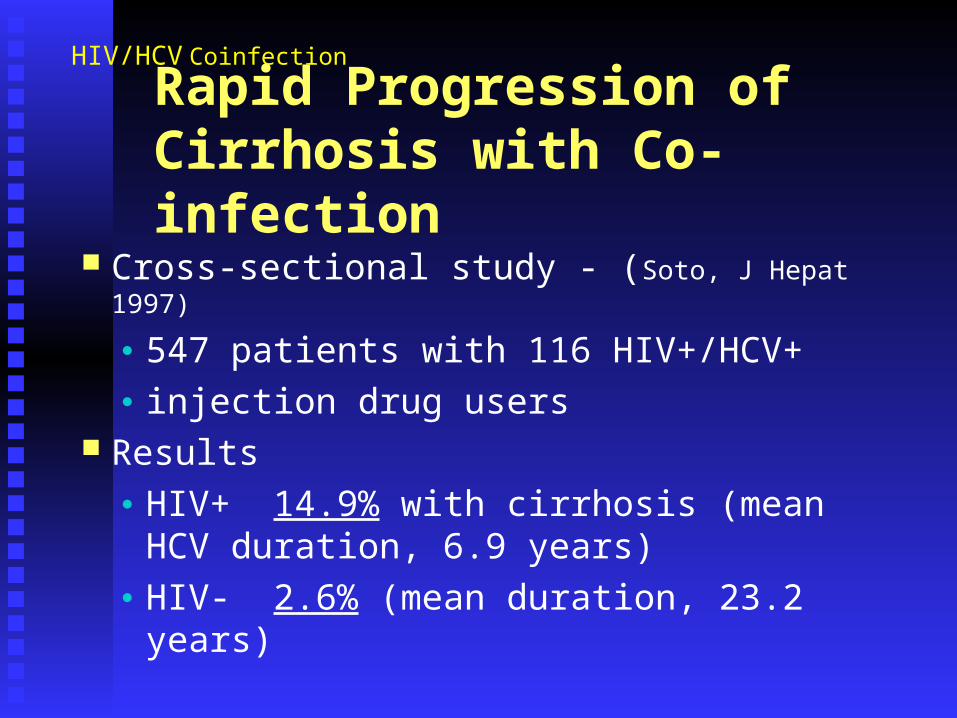
Rapid Progression of Cirrhosis with Co-infection
Cross-sectional study - (Soto, J Hepat 1997)
● 547 patients with 116 HIV+/HCV+● injection drug users
Results● HIV+ 14.9% with cirrhosis (mean HCV
duration, 6.9 years)● HIV- 2.6% (mean duration, 23.2 years)
HIV/HCV Coinfection
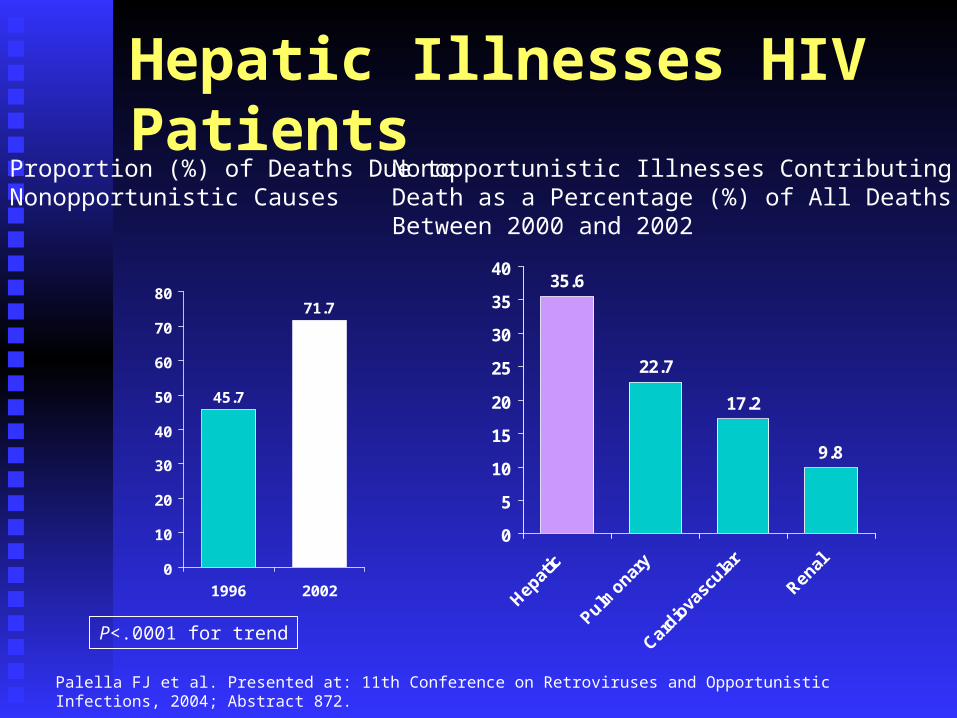
Hepatic Illnesses HIV Patients
Palella FJ et al. Presented at: 11th Conference on Retroviruses and Opportunistic Infections, 2004; Abstract 872.
45.7
71.7
0
10
20
30
40
50
60
70
80
1996 2002
35.6
22.7
17.2
9.8
0
5
10
15
20
25
30
35
40
Proportion (%) of Deaths Due to Nonopportunistic Causes
Nonopportunistic Illnesses Contributing to Death as a Percentage (%) of All Deaths Between 2000 and 2002
P<.0001 for trend
Potential Benefits of HCV Therapy in Patients Infected With HIV Viral eradication Delay fibrosis progression Prevent/delay bad clinical outcomes
Liver decompensation Hepatocellular carcinoma Death
Improve tolerance and effectiveness of HAART Permit aggressive antiretroviral drug therapy Enhance immune reconstitution?
Are we treating HCV in our patients?
HIV ACCESS Alameda County, CAChart survey done of 1021 HIV patients in care in 2000.
Most patients screened for HCV. 36% co-infected (271) Counseling: ETOH use rarely documented. Hep A & B vaccinations approx. 42%. Only 5 pts (1.8%) ever received IFN treatment with
one SVR.
Who Chooses Who Gets Treated? Chart review study of monoinfected HCV pts in an urban
GI specialty clinic. 293 patients evaluated for HCV, only 83 (28%) were
treated. Reasons for not treating were:1. Nonadherence to visits 37%2. Medical contraindication 34%3. Active substance use 13%4. Patient preference 11%
Authors concluded most patients couldn’t benefit from IFN/RBV therapy.
Falck-Ytter Ann Intern Med 2002; 136:288-92.
Is this similar to your experience?
• What provider barriers have you experienced?
• What system barriers?
• What patient barriers?
• What other barriers have we missed?
HIV Clinics Know How to Support Adherence
Can we do better than traditional HCV Can we do better than traditional HCV treatment models in other care settings?treatment models in other care settings?
Elements of HCV/HIV ManagementPhase I: Screening and diagnosis
Phase II: Counseling and health care maintenance
Phase III: Evaluation for treatment
Phase IV: Monitoring treatment
Phase V: Managing progressive liver disease
How far are you going in your practice?
Screening and Diagnosis
Test all HIV patients for anti-HCV EIA ab.1
If IDU and neg HCV ab, check HCV PCR.
(False-neg ab has been reported, 3.4% in one
HIV cohort).2 If HCV pos., check PCR to confirm active infection
(10-15% spontaneous clearance in monoinfected).
1. USPHS Guidelines for Preventing OI in PWHIV, 1999.1. USPHS Guidelines for Preventing OI in PWHIV, 1999.2. Boyle B and Vaamonde C. DDW, May 2002, San Francisco, Abs 106665.2. Boyle B and Vaamonde C. DDW, May 2002, San Francisco, Abs 106665.
Counseling and HCM
Counseling Topics:
Prognosis & treatment basics. Avoid EtOH, hepatotoxic meds. Limit acetaminophen < 2 gm/day. Limit Vitamin A and complementary meds. Prevent transmission (sex, drugs, needle exchange).
NIH Consensus Statement 2002.NIH Consensus Statement 2002.

Counseling and HCM
Health Care Maintenance:
Alcohol & drug treatment referral. Referral to peer support resources. Hep A and B vaccines
Prognosis: Effect of HAART on HCV PIs have no activity against HCVPIs have no activity against HCV Control of HIV to < 400 copies/ml does Control of HIV to < 400 copies/ml does
not affect HCV RNA levelsnot affect HCV RNA levels May see transient elevation of ALT after May see transient elevation of ALT after
initiationinitiation PI vs NNRTI, no difference in rate of PI vs NNRTI, no difference in rate of
liver fibrosis liver fibrosis (Deitrich, CROI 2005)(Deitrich, CROI 2005)
HIV/HCV Coinfection
Phase III: Evaluating for Treatment
Whom Do We Treat?
HIV stable (No AZT/ ddI in regimen.) If HIV not stable, needs to be addressed
first (judgment call!) Treatment/follow-up adherence Mostly drug & alcohol free (methadone
okay) Willing to undergo treatment Pre-treatment liver biopsy necessary
Whom Do We Treat (2)
Depression under control No other contraindications for treatment
(renal failure, severe cardiac disease, severe anemia/neutropenia/thrombocytopenia, uncontrolled diabetes, autoimmune diseases)
Compensated liver disease Pretreatment vaccine for Hep A/Hep B
When to Delay or Avoid Treatment
CD4+ cells < 100/mm³, active opportunistic infections Uncontrolled HIV viral load Decompensated liver disease Untreated depression Ongoing substance abuse Nonadherence Active ischemic heart disease Untreatable malignancy Severe autoimmune disease Pregnancy plans
HIV/HCV Coinfection
Whom Do We Treat?
Liver Biopsy evaluation: Stage 1/Grade 1: treatment optionalStage 2-4/Grade 2-4: treatment indicated
Persistently elevated AST Compliance with follow-up appointments
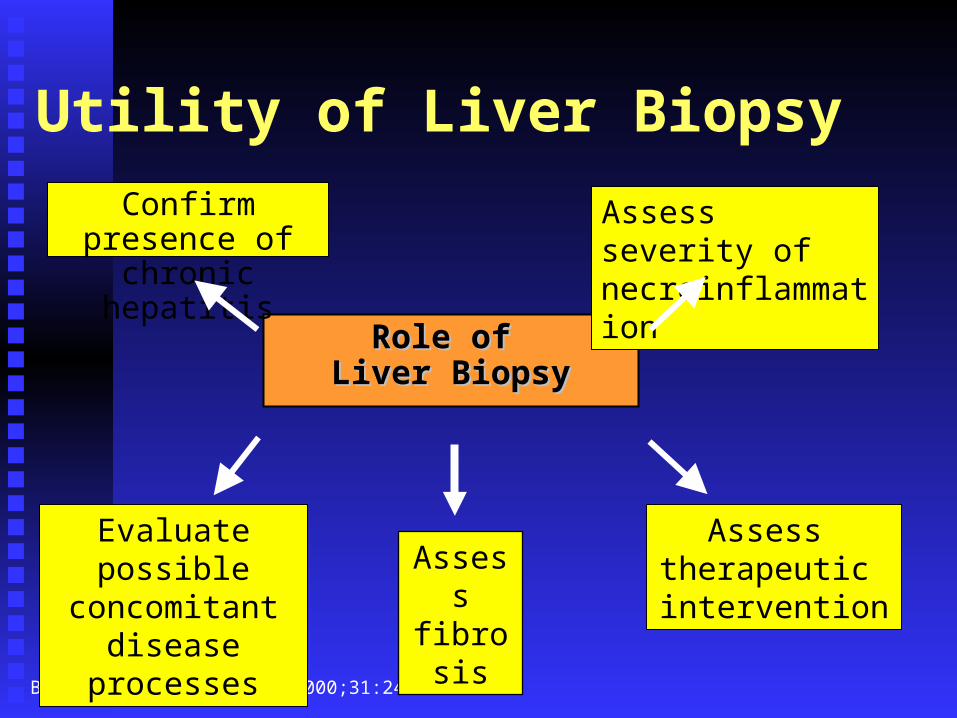
Utility of Liver Biopsy
Role of Role of Liver BiopsyLiver Biopsy
Confirm presence of chronic hepatitis
Brunt et al. Hepatology. 2000;31:241-246..
Assess severity of necroinflammation
Evaluate possible concomitant
disease processes
Assess therapeutic intervention
Assessfibrosis
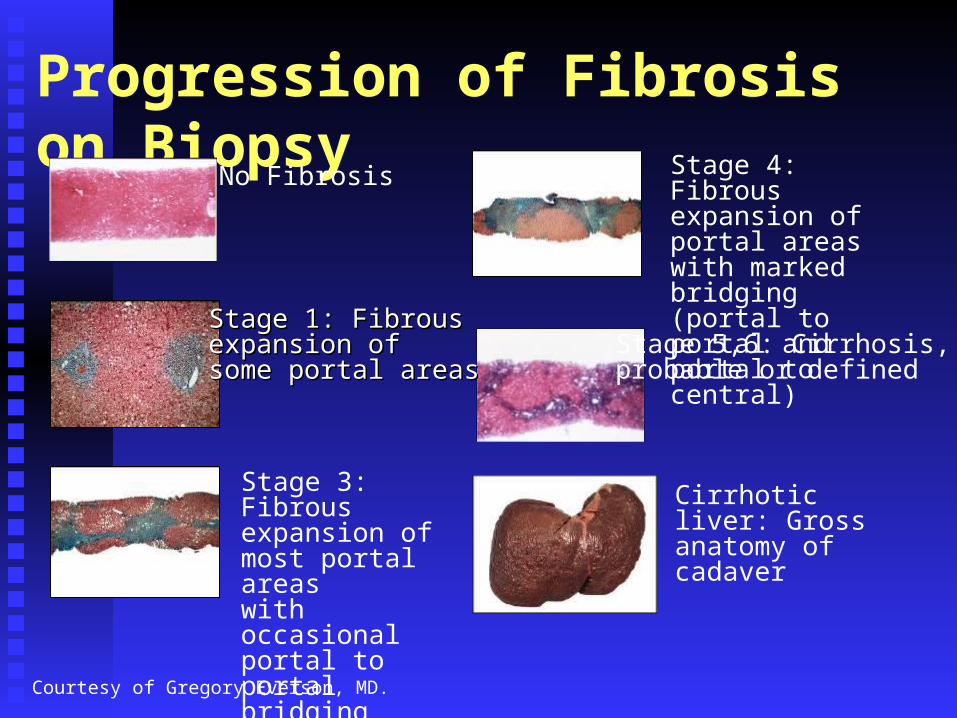
Progression of Fibrosis on BiopsyNo Fibrosis
Stage 1: Fibrous Stage 1: Fibrous expansion of expansion of some portal areassome portal areas
Stage 3: Fibrous expansion of most portal areas with occasional portal to portal bridging
Stage 4: Fibrous expansion of portal areas with marked bridging (portal to portal and portal to central)
Stage 5,6: Cirrhosis, probable or defined
Cirrhotic liver: Gross anatomy of cadaver
Courtesy of Gregory Everson, MD.
Elements of HCV/HIV ManagementPhase I: Phase I: Screening and diagnosisScreening and diagnosis
Phase II:Phase II: Counseling and health care Counseling and health care maintenancemaintenance
Phase III:Phase III: Evaluation for treatmentEvaluation for treatment
Phase IV:Phase IV: Monitoring treatmentMonitoring treatment
Phase V:Phase V: Managing progressive liver Managing progressive liver diseasedisease
Does HCV Treatment Work In Coinfected Patients?
Defining Success
EVR = Early viral response, 12 week viral load is undetectable or decreased by 2 logs.
ETR = End of treatment response, undetectable viral load at end of treatment.
SVR = Sustained viral response, undetectable 6 or more months after therapy.
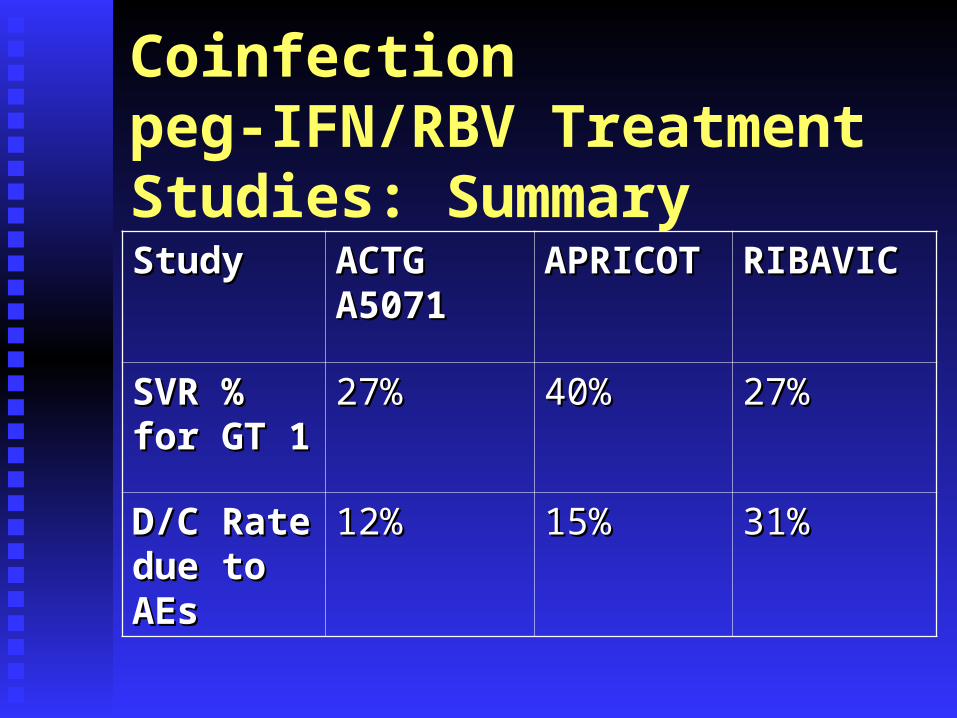
Coinfection peg-IFN/RBV Treatment Studies: Summary
StudyStudy ACTG ACTG A5071A5071
APRICOTAPRICOT RIBAVICRIBAVIC
SVR % for SVR % for GT 1GT 1
27%27% 40%40% 27%27%
D/C Rate D/C Rate due to AEsdue to AEs
12%12% 15%15% 31%31%
Coinfection Treatment Studies Consensus Lessons Peg-IFN/RBV is best current treatmentPeg-IFN/RBV is best current treatment RBV full dose is critical early in RxRBV full dose is critical early in Rx Lack of early response predicts no SVRLack of early response predicts no SVR AZT + RBV = anemiaAZT + RBV = anemia ddI + RBV = lactateddI + RBV = lactate

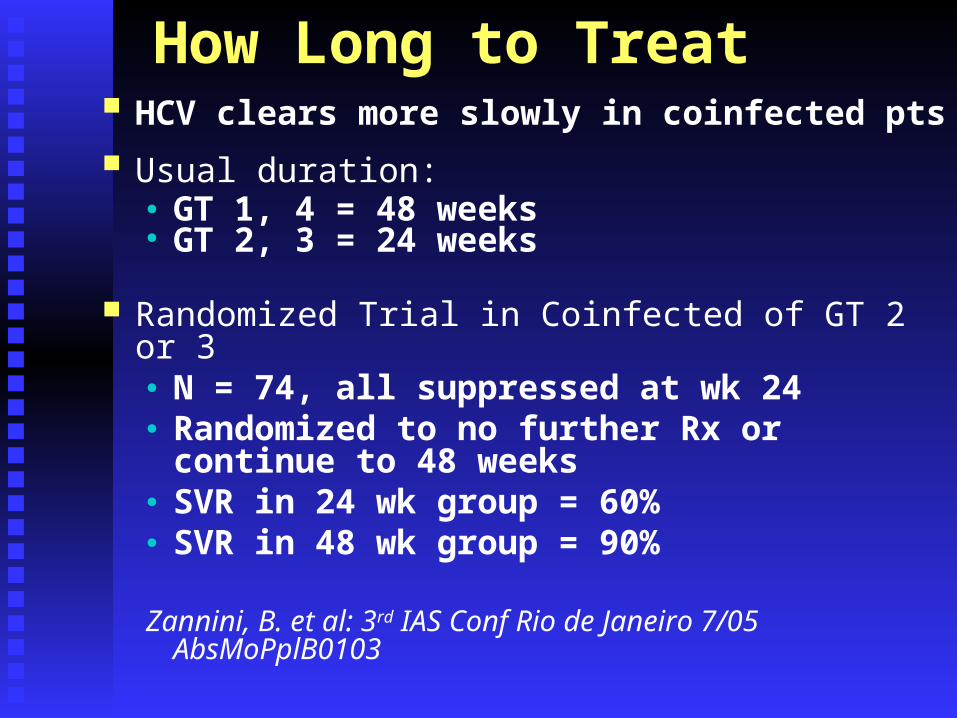
How Long to Treat HCV clears more slowly in coinfected pts
Usual duration:● GT 1, 4 = 48 weeks● GT 2, 3 = 24 weeks
Randomized Trial in Coinfected of GT 2 or 3● N = 74, all suppressed at wk 24● Randomized to no further Rx or continue to 48
weeks● SVR in 24 wk group = 60%● SVR in 48 wk group = 90%
Zannini, B. et al: 3rd IAS Conf Rio de Janeiro 7/05 AbsMoPplB0103
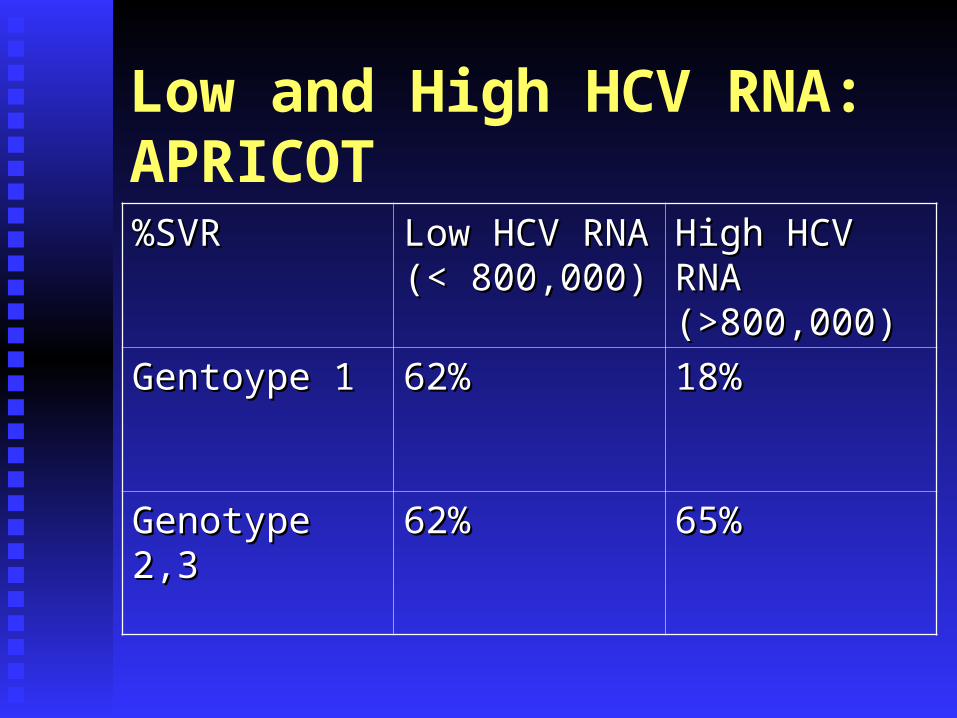
Low and High HCV RNA:APRICOT%SVR%SVR Low HCV RNA Low HCV RNA
(< 800,000)(< 800,000)High HCV RNA High HCV RNA (>800,000)(>800,000)
Gentoype 1Gentoype 1 62%62% 18%18%
Genotype 2,3Genotype 2,3 62%62% 65%65%
Does Rx Improve Liver Health if No SVR?
Retrospective analysis of APRICOTRetrospective analysis of APRICOT N = 64 pts with paired pre – and post -Rx bxN = 64 pts with paired pre – and post -Rx bx Histologic response defined as Histologic response defined as ↓ at least 2 pts ↓ at least 2 pts
in indexin index 1/3 of pts without SVR had + histologic 1/3 of pts without SVR had + histologic
responseresponse
Lissen, E. et al, 3Lissen, E. et al, 3rdrd IAS Conf., Rio de Janeiro, 7/02 Aos IAS Conf., Rio de Janeiro, 7/02 Aos TuPel.1C21TuPel.1C21
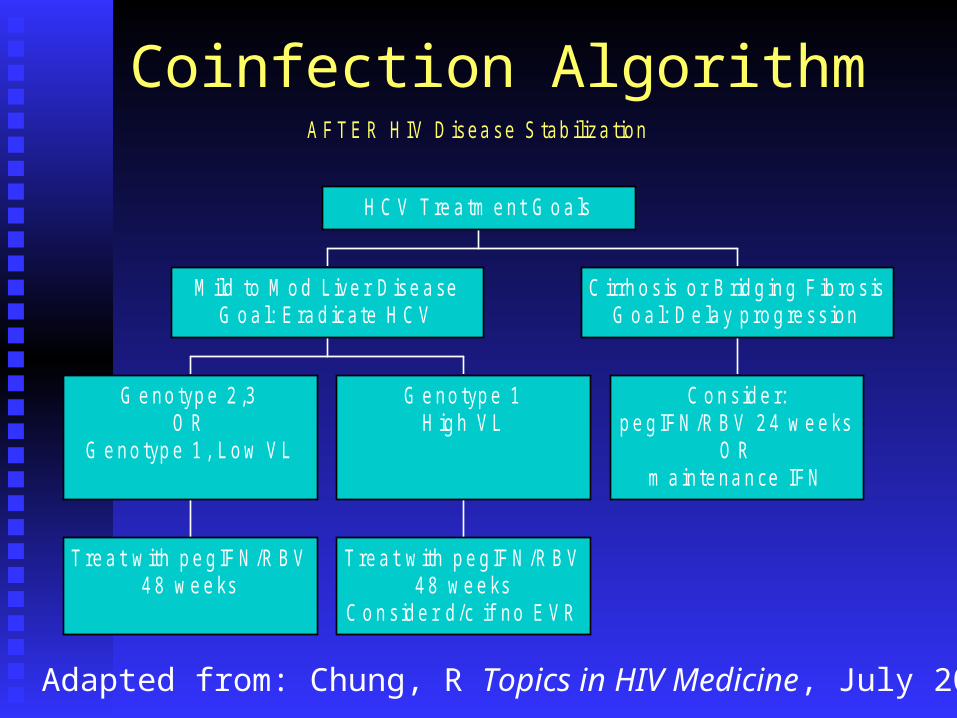
Coinfection AlgorithmA F T E R H IV D isea se S tab iliza tion
T re a t w ith p e g IF N /R B V4 8 w e e ks
G e no typ e 2 ,3O R
G e no typ e 1 , L o w V L
T re a t w ith p e g IF N /R B V4 8 w e e ks
C o n s id e r d /c if no E V R
G e no typ e 1H ig h V L
M ild to M o d L ive r D ise a seG o a l: E ra d ica te H C V
C o n s id e r:p e g IFN /R B V 2 4 w e e ks
O Rm a in te na n ce IFN
C irrh o s is o r B rid g in g F ib ro s isG o a l: D e la y p ro g re ss ion
H C V T re a tm e nt G o a ls
Adapted from: Chung, R Topics in HIV Medicine, July 2006

Management of HCV/HIV in 2006 Select ART with lower potential for toxicity
Avoid: High-dose ritonavir, nevirapine ddI (in advanced liver disease), d4T, ZDV
in patients on RBV Monitor CBC and AST/ALT closely, q 2
weeks initially Treat through “minor” elevations of serum
ALT (<5 X normal) and avoid “switching” or discontinuing regimens if possible
Practical Lessons: HCV Rx in the HIV Clinic
Severe anemia is common, start epo early, monitor often.
Monitor closely for depression. SSRI’s for everyone! Warn pts that abs CD4 will fall due to IFN (%CD4 is
preserved). HIV VL decreased in non-HAART pts.
Water (2-3 liters per day) is the best side effect management tool.
Open questions for HIV/HCV patients
Will weight-based RBV improve SVR? Should coinfected patients be treated for
extended periods >48 weeks? Can fibrotests replace liver biopsy? (Not
looking good as of CROI 2006.)
HIV/HCV Coinfection
Sheila E.
38 yo with CD4 280, VL 20K, both worsening over the past 6 months.
• Never on HAART.• Persistent elevation of ALT/AST.• HCV genotype 1.• Biopsy last month shows bridging fibrosis
and moderate inflammation (Stage 2, Grade 3).
Sheila E. ~ Questions
1. Will you recommend starting HAART, HCV Treatment, or both for Ms. E at this time?
2. Any specific HAART drugs to use or avoid if she does start HAART?
Jorge X.
41 yo being treated with pegIFN/RBV.
• CD4 300, HIV VL 20K.• Not on HAART.• HCV genotype II.• No liver biopsy was done before starting Tx.• History of depression, started on SSRI just prior
to starting HCV Tx.• Now week 8 of HCV Tx, complaint of severe
fatigue, not leaving house. Wants to quit Tx.
Jorge X. ~ Questions
1. Differential Dx for complaint of fatigue?1. Differential Dx for complaint of fatigue?
2. Next steps to address Jorge’s complaint?2. Next steps to address Jorge’s complaint?
3. For future reference, how would you discuss the 3. For future reference, how would you discuss the issue of biopsy before therapy for patients like issue of biopsy before therapy for patients like Jorge (and what if Jorge had genotype 1?)Jorge (and what if Jorge had genotype 1?)
Yolanda R.35 yo being treated with simultaneous HAART and
pegIFN/RBV. You are afraid she is failing Tx.
• CD4 250, HIV VL <75• On HAART regimen of ddI/TDF/LPVr for 6
months.• HCV genotype I, HCV VL 2.5M.• Pretreatment liver biopsy shows Stage 2, Grade 3.• On pegIFN/RBV and you believe she is adherent.• Week 12, HCV viral load is still 1M.
Yolanda R. ~ Questions
1. What are the pro and con arguments of stopping 1. What are the pro and con arguments of stopping Yolanda’s HCV Tx?Yolanda’s HCV Tx?
2. Will you recommend changes in HAART if 2. Will you recommend changes in HAART if Yolanda continues on HCV Tx?Yolanda continues on HCV Tx?
HCV WebsitesFor providers: www.cdc.gov/ncidod/diseases/hepatitis www.hivandhepatitis.com www.va.gov/hepatitisc
For clients/patients: www.thebody.com www.hcvadvocate .org www.hivandhepatitis.com

HBV/HIV Coinfection
Relative needlestick and sexual exposure risk
Place in order – highest>>lowestPlace in order – highest>>lowest Hepatitis B, C, and HIV??Hepatitis B, C, and HIV??
Needlestick:Needlestick:
Sexual transmission:Sexual transmission:
Relative Risk of Infection: “Rule of Three” HBV contaminated needle:HBV contaminated needle:
eAg+ 30% risk of transmissioneAg+ 30% risk of transmission eAg- 10% riskeAg- 10% risk
HCV contaminated needle:HCV contaminated needle: 3% risk3% risk
HIV contaminated needle:HIV contaminated needle: 0.3% risk0.3% risk
Sexual transmission: HBV>HIV>HCVSexual transmission: HBV>HIV>HCV
HBV-HIV Coinfection Common and more rapidly progressiveCommon and more rapidly progressive HBV DNA levels higher and spontaneous HBV DNA levels higher and spontaneous
seroconversion less frequentseroconversion less frequent ALT lower and histology worseALT lower and histology worse HAART may induce severe exacerbationHAART may induce severe exacerbation Interferon Interferon αα minimally effective (<10% loss of minimally effective (<10% loss of
HBeAg)HBeAg) 3TC induces rapid fall in HBV DNA but few have 3TC induces rapid fall in HBV DNA but few have
sustained loss of HBeAg (YMDD variants)sustained loss of HBeAg (YMDD variants) Nuc analog combinations under study Nuc analog combinations under study
Evaluation and monitoring“should” include: HBsAg, HBeAg, anti-HBe, anti-HDVHBsAg, HBeAg, anti-HBe, anti-HDV
HBV DNAHBV DNA
Liver enzymesLiver enzymes
Liver synthetic testsLiver synthetic tests
Abdominal ultrasoundAbdominal ultrasound
Consider Liver biopsy if abnormal ALTConsider Liver biopsy if abnormal ALT
Minimum - every 6 monthsMinimum - every 6 months ALTALT HBV DNAHBV DNA HBeAgHBeAg
HCC screen every 6 months if :HCC screen every 6 months if : CirrhosisCirrhosis Strong family historyStrong family history > 45 years of disease> 45 years of disease High AFP >20 ?High AFP >20 ?
Evaluation and monitoring
Goals of Therapy for HIV/HBV
Induce sustained suppression of HBV replication.
Slow liver disease progressionAvoid HBV flare with immune
reconstitution Eradication is NOT a likely outcome
Conversion to HBsAg- rare in coinfection
Conversion to HBeAg- rare in anyone
1 Lok, et al. J Hepatology 2003: 38; S90-S103.

Treatment Endpoints for HBV
Biochemical (AST) normalizationVirological (serum HBV-DNA
suppression)Histological improvementRare: Serological (HBeAg &/or
HBsAg seroconversion)
1 Lok, et al. J Hepatology 2003: 38; S90-S103.
Algorithm assumes detectable HBV DNA prior to start or change anti-HBV therapy:
> 105 copies/ml for Wild Type> 104 “ for HBeAg negative variants
Anti-HBV therapy if:
ALT > 2X ULN (Lok 2004)ALT elevated (Keefe 2004) *
* normal ALT pts may have significant fibrosis liver biopsy
HIV/HBV: Initiating HBV Therapy George R: A 36-year-old man with HIV and HBV co-infection:
CD4 520, VL 18,000; Never on HAART. Persistent 3-5x increase in ALT/AST levels.HBsAg+; HBeAg+; HBV DNA: 6 x 108 IU/ml.Liver biopsy not performed
Questions:1. What medications are now FDA-approved for treatment of HBV?
2. What approved medications have activity against HBV, but do not have indications for HBV treatment?
DHS/HIV/PP
Medications with anti-HBV Activity
FDA ApprovedFDA Approved 3TC 100mg/d3TC 100mg/d IFN alpha-2b 5 mIU IFN alpha-2b 5 mIU
sq qdsq qd pegIFN alfa-2a 180 pegIFN alfa-2a 180
mcg/week for 48 wksmcg/week for 48 wks Adefovir 10 mg/dAdefovir 10 mg/d Entecavir 0.5-1.0 mg/d Entecavir 0.5-1.0 mg/d
NOT Approved for HBVNOT Approved for HBV TenofovirTenofovir EmtricitabineEmtricitabine

HIV/HBV: Initiating HBV TherapyThe following patients are co-infected with HBV and HIV.
All have HBsAg(+), persistent elevations of ALT (> 2-3x), and HBV DNA levels > 106. None has ever received ARV Rx or HBV Rx.
Patient 1: CD4 490, HIV RNA=23,000; HBeAg(+).
Patient 2: CD4 524; HIV RNA=38,000; HBeAg(-).
Patient 3: CD4 210; HIV RNA = 112,000; HBeAg(+).
QuestionHow would you approach treatment of HBV infection in these 3 patients?
DHS/HIV/PP
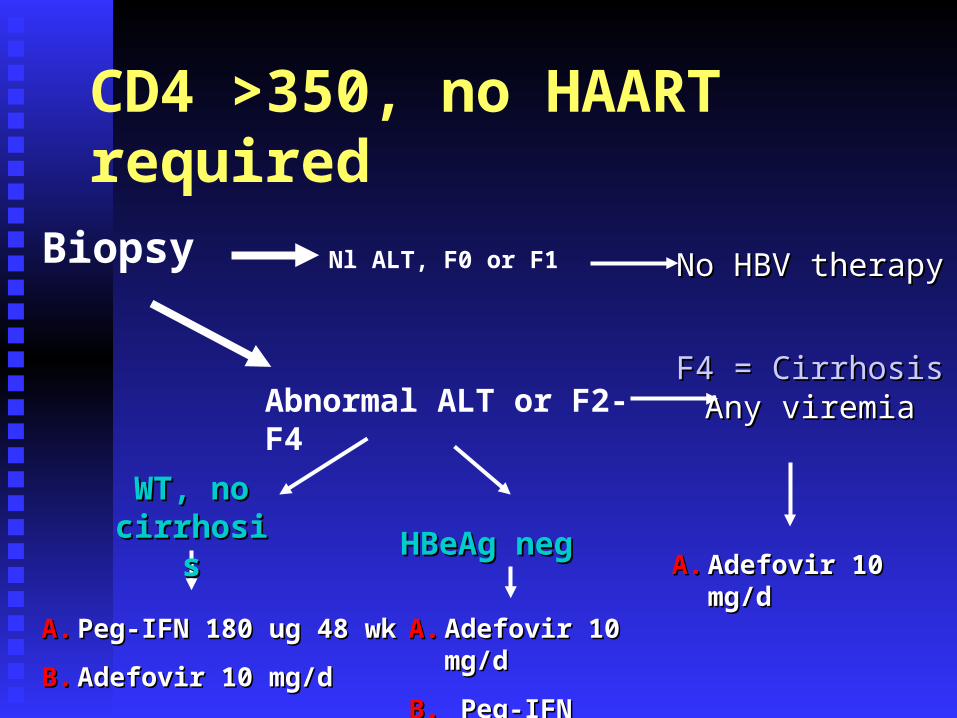
CD4 >350, no HAART required
Biopsy Nl ALT, F0 or F1 No HBV therapyNo HBV therapy
HBeAg negHBeAg neg
F4 = CirrhosisF4 = CirrhosisAny viremiaAny viremiaAbnormal ALT or F2-F4
A.A. Adefovir 10 mg/dAdefovir 10 mg/d
A.A. Peg-IFN 180 ug 48 wkPeg-IFN 180 ug 48 wk
B.B. Adefovir 10 mg/dAdefovir 10 mg/d
WT, no WT, no cirrhosiscirrhosis
A.A. Adefovir 10 mg/dAdefovir 10 mg/d
B.B. Peg-IFNPeg-IFN

CD4 >350, on HAART
Biopsy Nl ALT, F0 or F1 Keep current Keep current HAARTHAART
HBeAg HBeAg negneg
CirrhosisCirrhosisAny viremiaAny viremia
Abnormal ALT or F2-F4
A.A. Include TDFInclude TDF
B.B. Include FTC-TDFInclude FTC-TDF
C.C. Add Adefovir 10 Add Adefovir 10 mg/dmg/d
A.A. Peg-IFN 180 ug 48 wkPeg-IFN 180 ug 48 wkB.B. a. Incorporate 1 (or 2) HBV-active NAsa. Incorporate 1 (or 2) HBV-active NAs b. if YMDD mutant, include TDFb. if YMDD mutant, include TDF
WT, no WT, no cirrhosiscirrhosis
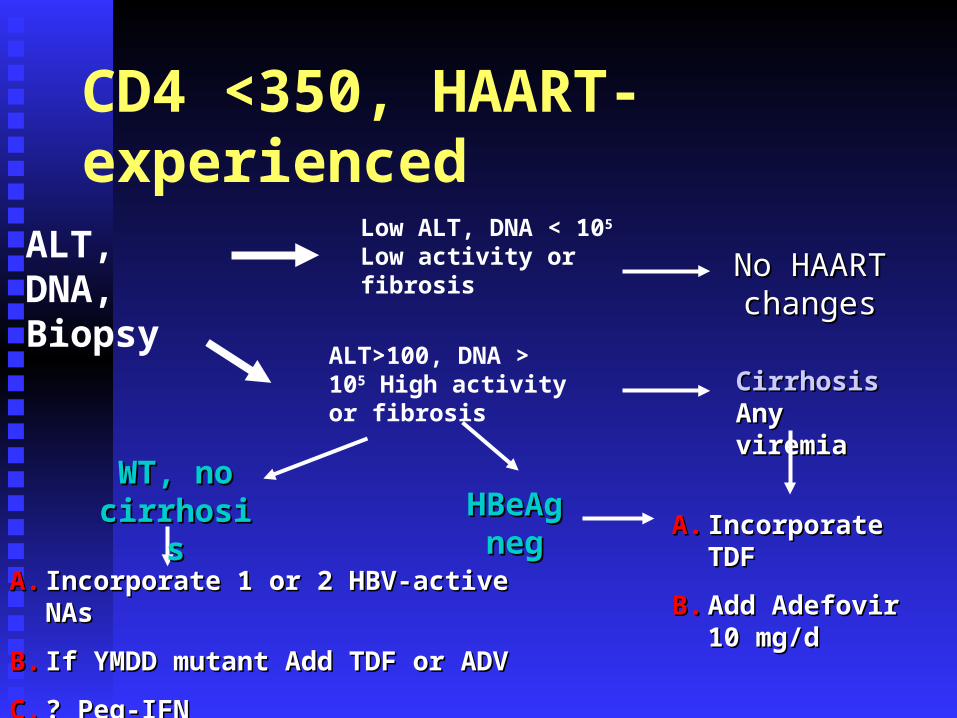
CD4 <350, HAART-experienced
ALT, DNA, Biopsy
Low ALT, DNA < 105 Low activity or fibrosis
No HAART No HAART changeschanges
HBeAg HBeAg negneg
CirrhosisCirrhosisAny viremiaAny viremia
A.A. Incorporate TDFIncorporate TDF
B.B. Add Adefovir 10 Add Adefovir 10 mg/dmg/d
A.A. Incorporate 1 or 2 HBV-active NAsIncorporate 1 or 2 HBV-active NAs
B.B. If YMDD mutant Add TDF or ADVIf YMDD mutant Add TDF or ADV
C.C. ? Peg-IFN? Peg-IFN
WT, no WT, no cirrhosiscirrhosis
ALT>100, DNA > 105 High activity or fibrosis
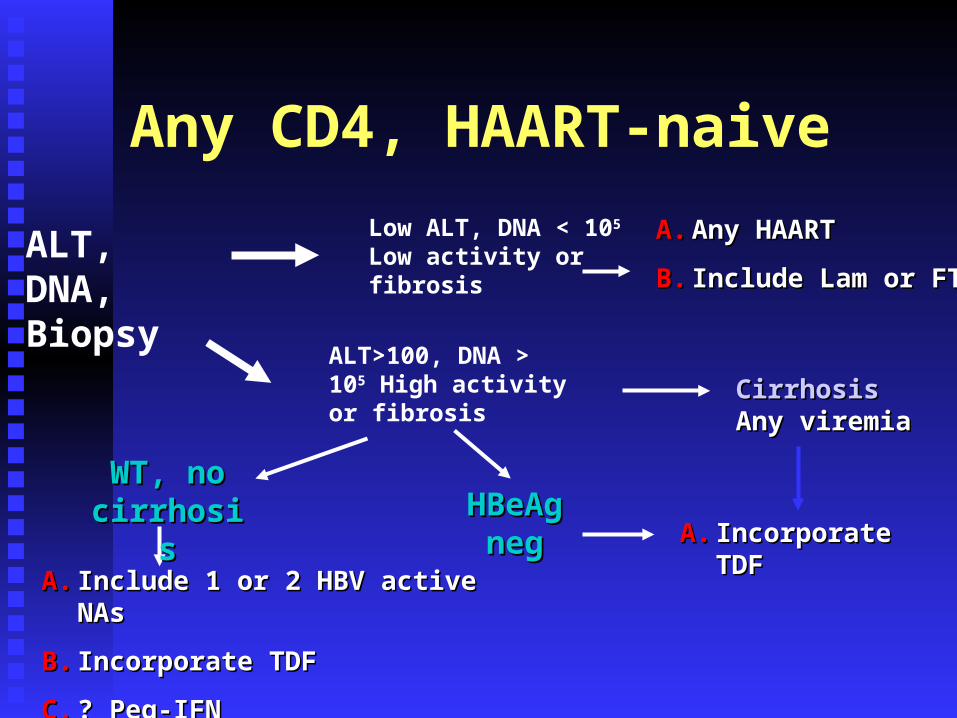
Any CD4, HAART-naive
ALT, DNA, Biopsy
Low ALT, DNA < 105 Low activity or fibrosis
A.A. Any HAARTAny HAART
B.B. Include Lam or FTCInclude Lam or FTC
HBeAg HBeAg negneg
CirrhosisCirrhosisAny viremiaAny viremia
A.A. Incorporate TDFIncorporate TDF
A.A. Include 1 or 2 HBV active NAsInclude 1 or 2 HBV active NAs
B.B. Incorporate TDFIncorporate TDF
C.C. ? Peg-IFN? Peg-IFN
WT, no WT, no cirrhosiscirrhosis
ALT>100, DNA > 105 High activity or fibrosis

HIV/HBV: Monitoring Response
A 41-year-old woman with HIV and HBV co-infection: CD4 220, VL 88,000; Never on HAART. Labs show 3-4x increase in ALT/AST levels.HBsAg(+); HBeAg(-); HBV DNA: 4 x 109 IU/ml.Started on Tenofovir-DF + Lamivudine +
Efavirenz
Questions:1. What are the goals of therapy?2. What should you monitor to determine the response to therapy? DHS/HIV/
PP
0
5
10
15
20
25
30
Pa
tie
nts
wit
h r
es
po
ns
e(%
)
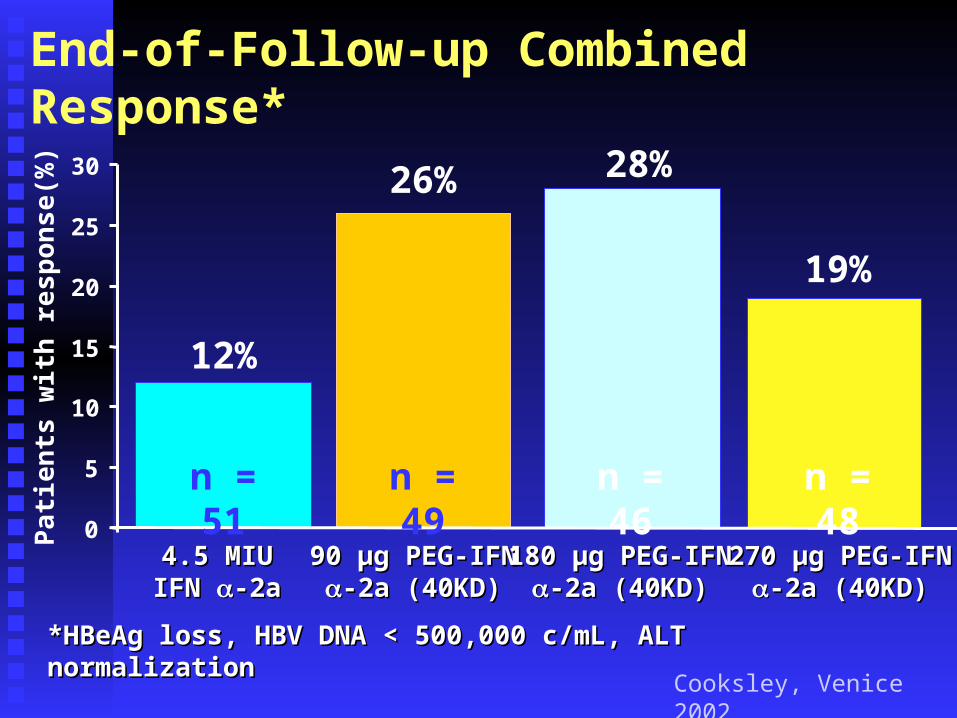
End-of-Follow-up Combined Response*
*HBeAg loss, HBV DNA < 500,000 c/mL, ALT normalization*HBeAg loss, HBV DNA < 500,000 c/mL, ALT normalization
4.5 MIU4.5 MIUIFN IFN -2a-2a
90 90 μgμg PEG-IFN PEG-IFN-2a (40KD)-2a (40KD)
180 180 μgμg PEG-IFN PEG-IFN-2a (40KD)-2a (40KD)
270 270 μgμg PEG-IFN PEG-IFN-2a (40KD)-2a (40KD)
12%
26% 28%
19%
n = 51 n = 49 n = 46 n = 48
Cooksley, Venice 2002
Adefovir in HBV patients with active replication and liver disease
Recommended treatment for HBeAg+ HBV is 12 months
Stop adefovir after HBeAg seroconversion documented on 2 occasions ~3 - 6 months apart
Prolonged treatment if HBeAg seroconversion not achieved – probably will be necessary in most
Indicated in treatment of 3TC resistance Dose adjustments in renal insufficiency Resistance much less frequent than for 3TC, but
occurs
3TC in HBeAg positive and likely HBeAg negative HBV disease
Stage liver disease to determine urgency of therapy Recommended treatment for HBeAg+ and HBeAg –
disease is 12 months – but likely too restrictive Stop lamivudine after HBeAg seroconversion
documented on 2 occasions ~3-6 months apart Prolonged treatment if HBeAg seroconversion not
achieved (?), prolonged therapy for HBeAg - pts Lamivudine resistance:
Continue lamivudine if continued benefit (clinical assessment, ALT, HBV DNA)
Consider switching to adefovir
Therapy for Hepatitis B: 2006Unanswered Questions Optimal treatment duration? What will be the role of pegylated interferon? What will be the role of combination therapy?
Nucleoside + nucleoside? Nucleoside + immunomodulator?
What will be the long-term consequences of YMDD mutants?
Therapy for pre-core mutants?