hiv associated cns infn - final
TRANSCRIPT
HIV-associated opportunistic infections of the CNS
Introduction About 7000 new HIV infections occur daily, 95% of which are in low-
income and middle-income countries, where only about a third of patients who require antiretroviral drugs have access to them.
In high-income countries, the combination antiretroviral therapy (cART)since 1996 reduced the incidence of neurological opportunistic infections, from 13.1 per 1000 patient-years in 1996–97 to 1.0 per 1000 in 2006–07
The annual incidence of new infections has declined by 19% since the peak of the worldwide HIV epidemic in 1999,
In 2009 about 2.6 million individuals were newly infected.
CNS opportunistic infections in HIV
Many of the opportunistic infections that affect the CNS are AIDS defining conditions.
o Progressive multifocal leukoencephalopathy (PML)o CNS cytomegalovirus infectiono CNS tuberculosis.o Cryptococcal meningitis.o Cerebral toxoplasmosis, including toxoplasmic encephalitis.Associated with high associated mortality.
AIDSHIV infection is characterized by three stages:o acute primary infection, o an asymptomatic (latent) stage, ando symptomatic chronic illness.Disease progression is highly variable: from 6 months
after seroconversion to more than 20–30 years,Mean survival after AIDS develops is 1.3 –3.7 yearsMost CNS opportunistic infections result from
reactivation of latent pathogens which occur when there is depletion of the CD4-cell count
General Principles of Diagnosis and Management
CNS opportunistic infections typically occur when the CD4-cell count is less than 200 cells per μL
Diagnosis should be based on clinical presentation, temporal evolution, CSF, and radiographic features
Multiple infections are present in 15% of cases and some infections might be revealed only after combination antiretroviral therapy is started
Combination antiretroviral therapy should be started, modified, or continued with appropriate antimicrobial therapy
Antimicrobial treatment is generally required until immune recovery (CD4-cell count more than 200 cells per μL) is achieved with antiretroviral therapy

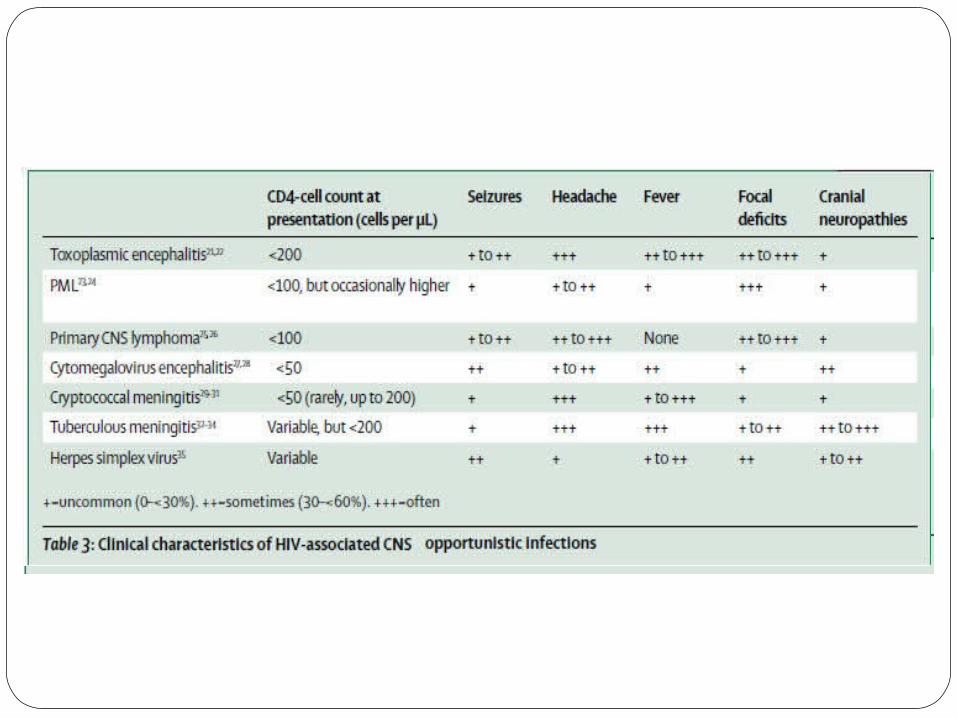
Clinical presentation
Infections such as toxoplasmic encephalitis and cryptococcal meningitis evolve over hours.
PML and CNS lymphoma have a more indolent course often taking weeks to months
Most often non-specific symptoms, such as fever and lethargyThe combination of new pattern of headache or headache
lasting longer than 3 days, new-onset seizures, or altered mental function strongly suggest an acute focal brain lesion

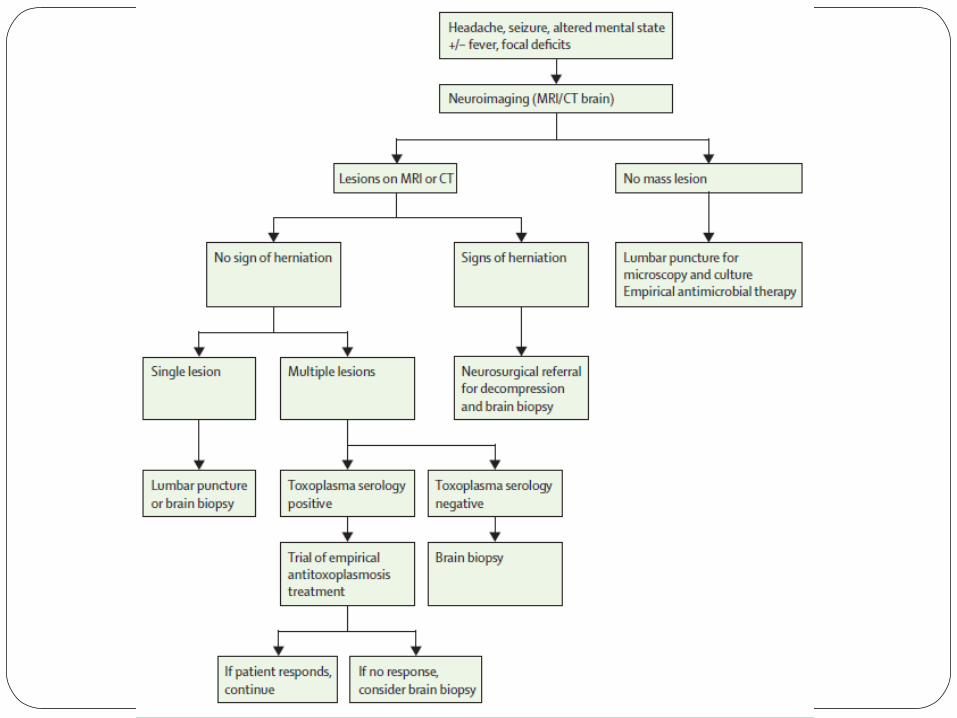
Diagnostic work-up
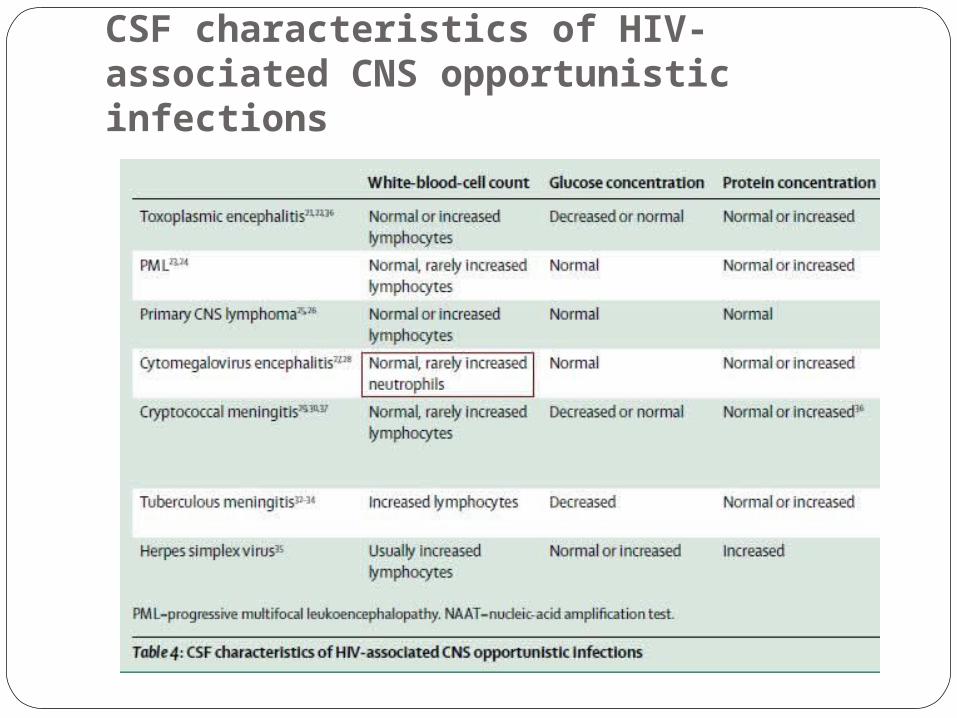
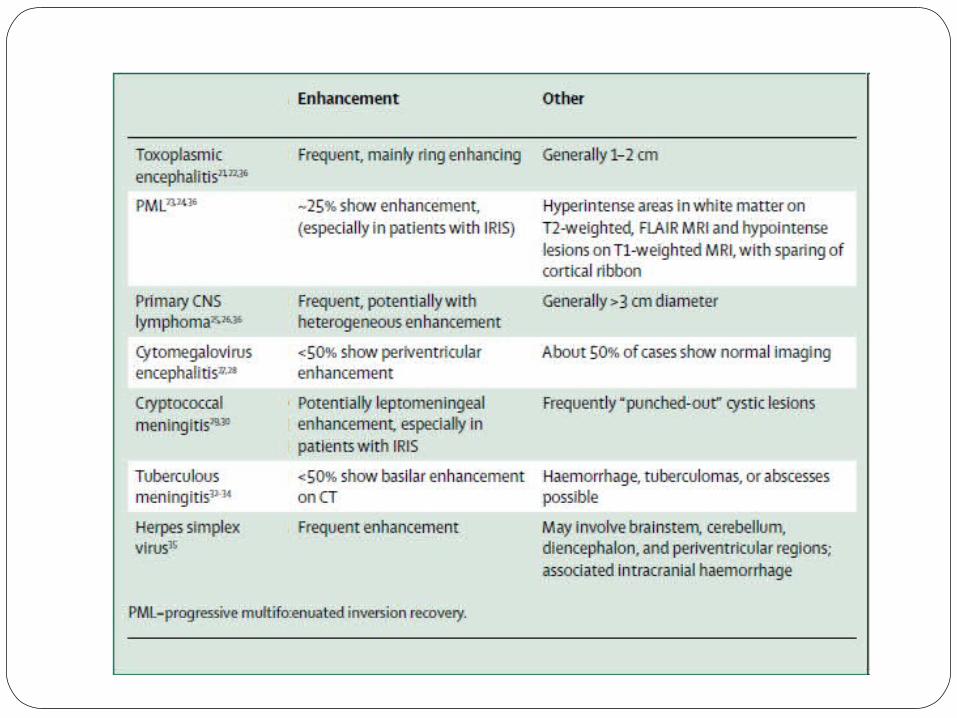
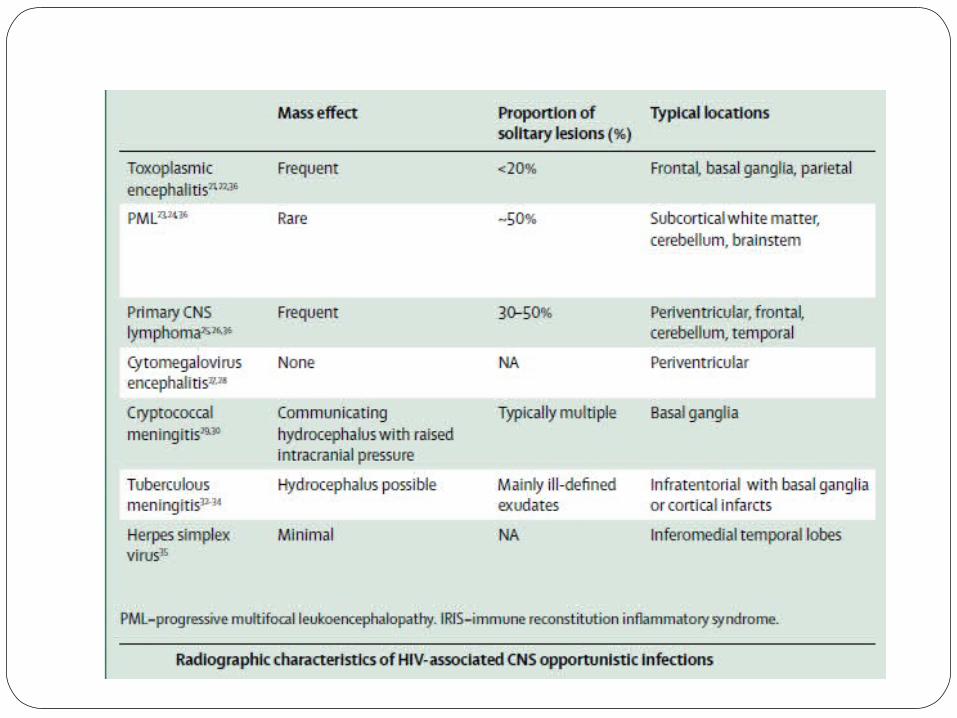
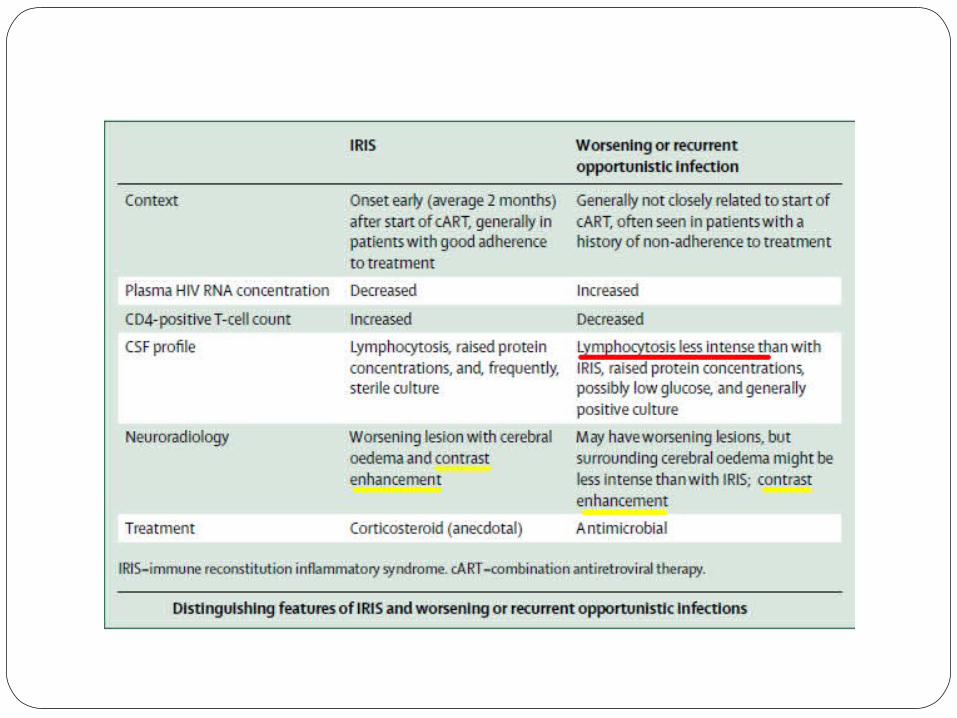
CSF characteristics of HIV-associated CNS opportunistic infections
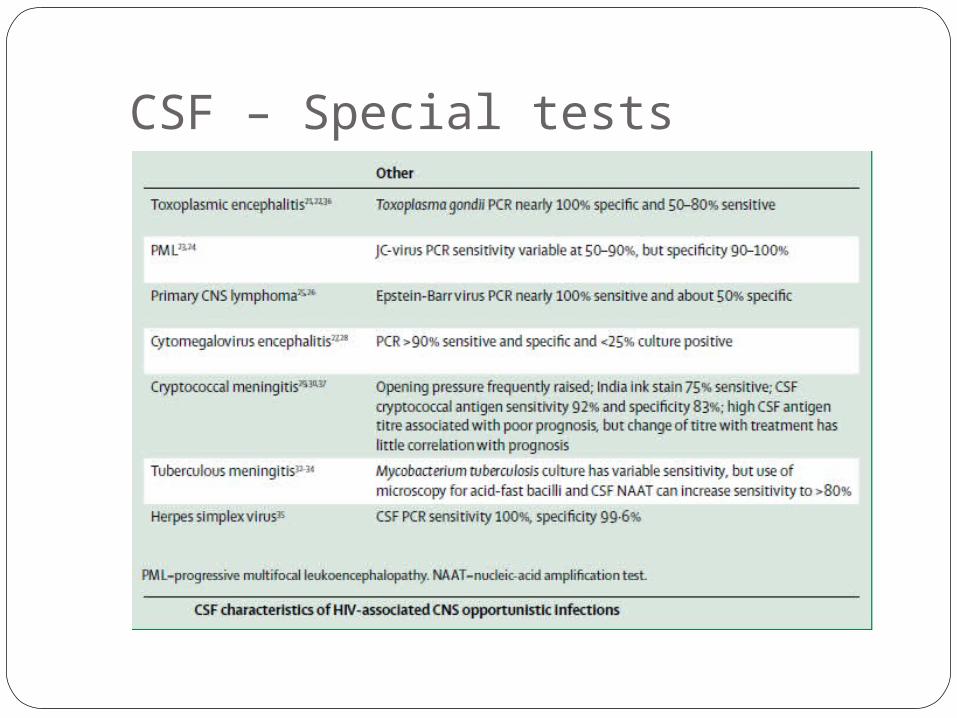
CSF – Special tests
Tuberculous meningitis and brain abscessesDetection of acid-fast bacilli or the causative organism
by positive culture or PCR is often difficultSensitivities for these tests have been poor at about
50%, but pts with HIV have higher yield rates of up to 80% possibly owing to incomplete immune responses and increased bacterial loads.
Repeated, large-volume lumbar punctures might improve the yield

Treatment of TbTreatment for tuberculosis does not differ
significantly between patients with and without HIV infection
Isoniazid, pyrazinamide, ethambutol, and rifampicin for 2 months.
Rifabutin is an alternative for rifampicin which lowers levels of protease inhibitors.
After this initial phase, isoniazid and rifampicin or rifabutin are continued for at least 9–12 months.
Treatment of TbThe role of corticosteroids and the optimum timing of
the initiation of cART in conjunction with antituberculosis therapy remain controversial issues
Delayed initiation of cART is recommended for patients with HIV-associated tuberculous meningitis.
Mortality from HIV-associated tuberculous meningitis is more than 50%, no improvement with addition of cART.
Mortality is extremely high in multidrug-resistant tuberculosis and extensively drug-resistant disease
Toxoplasmic encephalitis
Toxoplasmic encephalitis is the most commonly reported neurological opportunistic infection.
The incidence is declining.
In HIV patients toxoplasma serology may be negative.
Definitive diagnosis of CNS toxoplasmosis requires the following 1. Compatible clinical findings2. Identification of one or more mass lesions by CT, MRI, or other
radiographic testing3. Detection of T gondii in a clinical sample (CSF) by PCR

Toxoplasmic encephalitis - diagnosis
Lumbar puncture may be usually contraindicated.
So empiric treatment is usually initiated.Primary CNS lymphoma is often the principal differential
diagnosis.
o MRI, 18-fluorodeoxyglucose PET, or thallium-201 SPECT Brain biopsy could be necessary if equivocal or worsened
response to empirical treatment. (The presence of Epstein-Barr virus DNA in the CSF favors the
diagnosis of lymphoma. )
Toxoplasmic encephalitis - treatment
Combined pyrimethamine, folinic acid, and sulfadiazine has traditionally been used, although trimethoprim-sulfamethoxazole equally effective.
91% respond within 14 daysFailure to improve within 10–14 days of starting treatment
should, therefore, prompt reassessment of the diagnosis, with either thallium SPECT or brain biopsy
Corticosteroids are indicated only if substantial mass effect is present and should be discontinued as soon as possible
Toxoplasmic encephalitis - treatment
Induction treatment should be continued for at least 6 weeks till radiographic improvement is recorded
Maintenance therapy should be continued in all patients until immune reconstitution is achieved (persistent CD4-cell count of more than 200 cells per μL
Mortality for toxoplasmic encephalitis remains high at 20–60% within 1 year of diagnosis

Cryptococcal meningitis
Cryptococcal meningitis is thought to be the result of reactivation of latent infection in the immunocompromised
The CSF opening pressure is typically raised during LPThe CSF profile can be normal in about 30% of patientsMicroscopic detection with India ink staining and fungal culture
of the CSF Immunoassays of cryptococcal antigens are rapid, sensitive, and
specificUrinary antigen detection has high sensitivity (Resource poor)
High propensity to cause communicating hydrocephalus with increased intracranial pressure (15%)
Guidelines recommend serial daily lumbar punctures if the opening pressure is persistently greater than 25 cm H2O
Recommended treatment is intravenous amphotericin B in combination with oral flucytosine for a minimum of 2 weeks, followed by oral fluconazole for at least 8 weeks.
Prophylaxis with fluconazole is required until a durable immune reconstitution with a CD4-cell count higher than 200 cells per μL is achieved.
Cryptococcal meningitis -treatment
Cryptococcal meningitis -treatment
Recommended treatment is intravenous amphotericin B in combination with oral flucytosine for a minimum of 2 weeks, followed by oral fluconazole for at least 8 weeks.
Prophylaxis with fluconazole is required until immune reconstitution with a CD4-cell count higher than 200 cells per μL is achieved.
IRIS affects 10–40% of patients with cryptococcal meningitis and has mortality 33–66%.
Appropriate management of IRIS includes continuation of cART, antifungal therapy, and a course of corticosteroids.
Cytomegalovirus encephalitis
Cytomegalovirus usually causes asymptomatic or clinically benign infections and most people have been infected by the time they reach adulthood
In HIV, neurological diseases caused by cytomegalovirus are rare but very serious.
Encephalitis, retinitis, radiculomyelitis, or mononeuritis multiplex. MRI : meningeal enhancement or periventricular inflammation -
but not specific
CSF neutrophil predominant pleocytosis
PCR of CSF is highly sensitive and specific

A combination of ganciclovir and foscarnet was generally used before the introduction of cART but has severe side effects.
The use of cART plus one anticytomegalovirus (usually Ganciclovir) is favoured
Foscarnet is used when patients develop leucopenia while taking ganciclovir or in ganciclovir-resistant cases
Secondary prophylaxis with long-term oral anticytomegalovirus therapy should be continued till sustained immune recovery is achieved with cART
Cytomegalovirus encephalitis - treatment

Progressive multifocal leukoencephalopathy
The incidence of PML has declined with cART (7/1000 patient-years to 0.7/1000)
In the brain, JC virus infects mainly oligodendrocytes and astrocytes, and, occasionally, cerebellar granular cells and cortical pyramidal neurons
PML typically causes multifocal demyelinating lesions JC-virus granule cell neuronopathy with cerebellar ataxia, JC-
virus encephalopathy, and JC-virus meningitis
PML - diagnosis
MRI T2 & Flair hyperintense, T1 well demarcated hypo intense lesions. The cortical ribbon is classically spared. Minimal tissue oedema or no contrast enhancement is usual unless PML is complicated by IRIS
Rarely, the only radiological finding is severe cerebellar atrophy
Definitive diagnosis of PML is established by the detection of JC virus in
CSF by PCR
Sensitivity varies across laboratories, but specificity is high
Brain biopsy might occasionally be required to confirm the diagnosis.
PML - treatment
The mainstay of treatment for PML in patients infected with HIV is immune reconstitution with cART
This improved survival from 10% before the introduction of cART to 50–75%
No antiviral therapy with proven efficacy is available.
IRIS – treated with steroids
Herpes simplex virus encephalitis
Infrequent cause of CNS opportunistic infections Herpes simplex virus type 1 typically causes encephalopathy
that might develop subacutely over several weeks
Herpes simplex virus type 2 typically causes a diffuse meningoencephalitis that can recur.
PCR of the CSF is highly sensitive (100%) and specific (99.6%) for herpes simplex virus DNA
HSV Encephalitis -management
T2-hyperintensities in most cases and sometimes gadoliniumenhancing lesions involving the inferomedial temporal
Lesions may also involve the brainstem, cerebellum, diencephalon, and periventricular zones
The treatment of choice is 30 mg/kg aciclovir daily, given intravenously for 14–21 days (Resistance reported)
Progression can occur despite treatment, especially if CD4-cell counts are low
Ganciclovir and foscarnet have also been used with some success Rare relapses within 3 months of treatment Clinical trial of 90 days of valaciclovir after induction treatment – results
awaited.

ConclusionsConclusions Though CNS opportunistic infections in HIV pts are decreasing with cART,
still concern in those with delayed diagnosis or HIV treatment is inadequate.
PML, primary CNS lymphoma, and multidrug-resistant tuberculosis have no effective treatment and mortality still remain high.
Early daignosis of HIV and access to cART remain most important for prevention.
Concurrent infection with more than one CNS opportunistic infection is important. (Also possibility neurosyphilis, varicella zoster, cerebral malaria, Chagas disease, and neurocysticercosis).
Knowledge acquired is useful in the context of immunosuppression for transplanted and in the testing of new immunomodulatory drugs for autoimmune diseases.
thank you

(A) Cryptococcal meningitis in a man aged 58 years who presented with headache, weight loss, anorexia, and a generalised seizure, with a CD4-cell count of 10 cells per μL. The arrow shows gadolinium enhancement of the posterior meninges on T1-weighted MRI. A cryptococcoma is present in the right basal ganglion
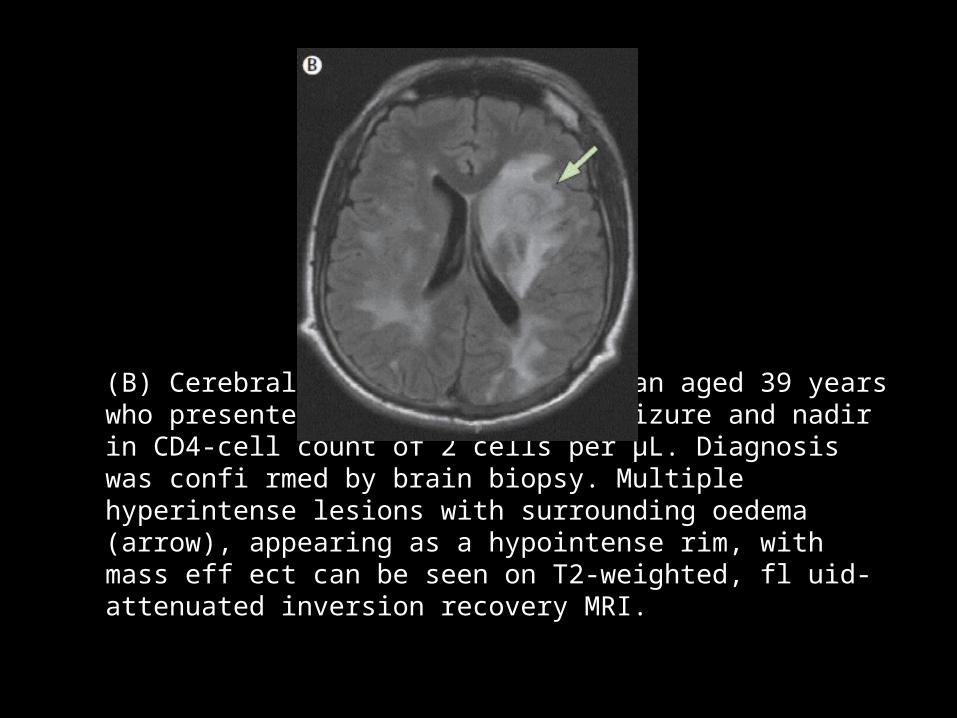
(B) Cerebral toxoplasmosis in a man aged 39 years who presented with generalised seizure and nadir in CD4-cell count of 2 cells per μL. Diagnosis was confi rmed by brain biopsy. Multiple hyperintense lesions with surrounding oedema (arrow), appearing as a hypointense rim, with mass eff ect can be seen on T2-weighted, fl uid-attenuated inversion recovery MRI.
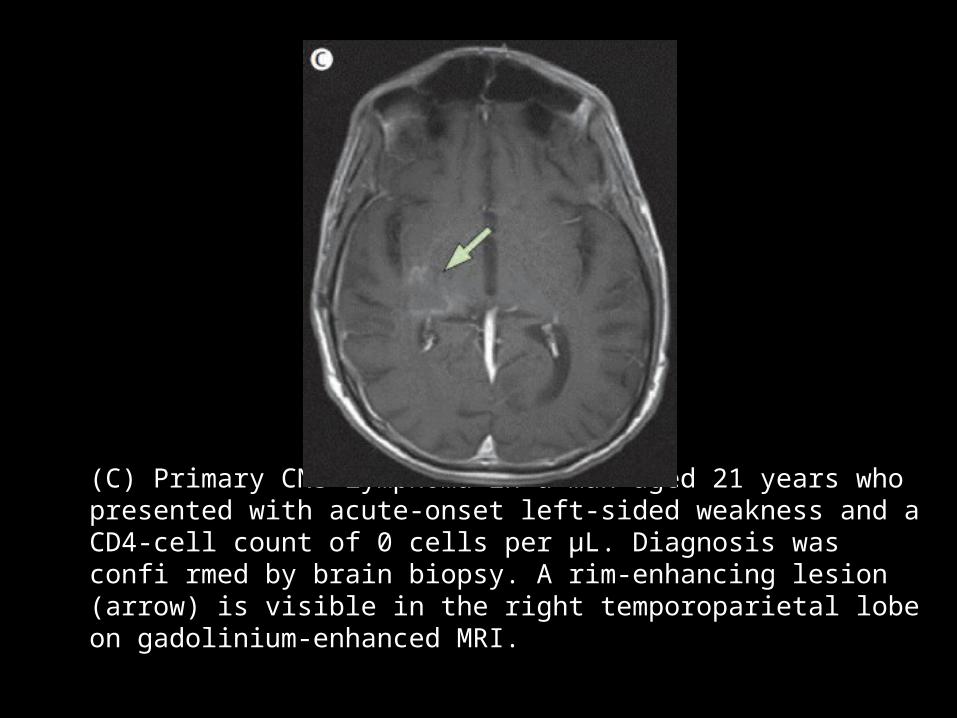
(C) Primary CNS lymphoma in a man aged 21 years who presented with acute-onset left-sided weakness and a CD4-cell count of 0 cells per μL. Diagnosis was confi rmed by brain biopsy. A rim-enhancing lesion (arrow) is visible in the right temporoparietal lobe on gadolinium-enhanced MRI.
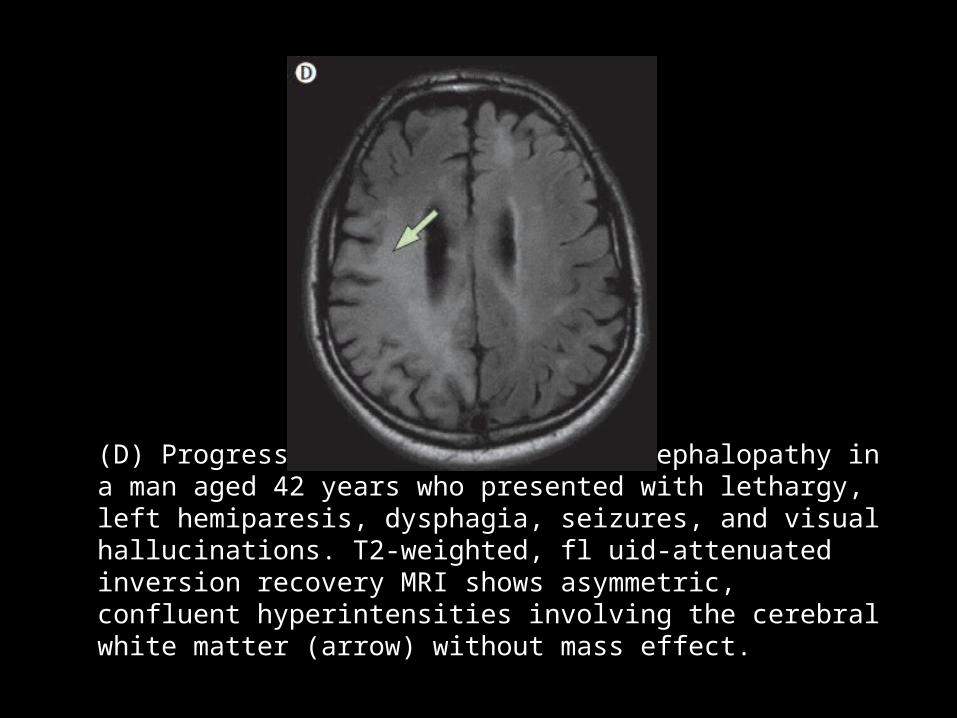
(D) Progressive multifocal leukoencephalopathy in a man aged 42 years who presented with lethargy, left hemiparesis, dysphagia, seizures, and visual hallucinations. T2-weighted, fl uid-attenuated inversion recovery MRI shows asymmetric, confluent hyperintensities involving the cerebral white matter (arrow) without mass effect.