hot issues in women’s health: hormones, menopause and ... · health: hormones, menopause and...
TRANSCRIPT
Hot Issues in Women’s Health: Hormones,
Menopause and Metabolism Nanette Santoro, MD
Professor and E Stewart Taylor Chair of Obstetrics and Gynecology
University of Colorado School of Medicine
Learning Objectives
At the end of this session, the learner is expected to be able to:
Recite the stages of the menopausal transition and relate these stages to specific hormone alterations.
Predict the hormonal changes associated with changes in metabolism
Understand how common menopausal symptoms influence metabolism apart from hormones
Provide patients with evidence based guidelines to promote metabolic health in midlife
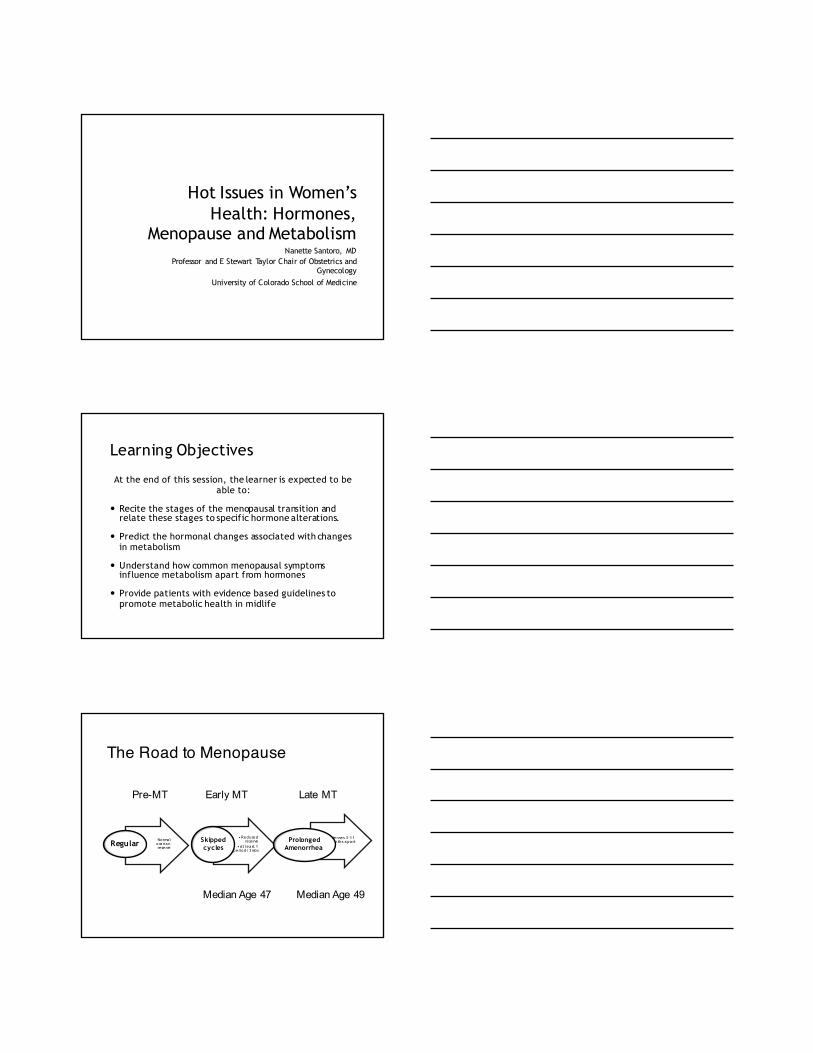
The Road to Menopause
Norma l ova rian reserve
Regular •Reduced
reserve•At lea st 1
period/3mos
Skipped cycles
Menses 3 -11 months apa rtProlonged
Amenorrhea
Pre-MT Early MT Late MT
Median Age 47 Median Age 49
Hormone Changes in the Pre- and Early Menopause Transition
‘Monotropic’ rise in FSH: first described in 1976 (Sherman)
Erratic estradiol patterns (Santoro, 1996)
Reduced progesterone production across the transition (Prior, Santoro, 2008)
Shorter menstrual cycles (Klein, 2002)
Less frequent ovulationSherman BM JCEM 1976; 42:629; Santoro JCEM 1996; 81: 1495; Santoro JCEM
2008; 93:1711; Prior JC Nov Found Symp 2002; 242:172; Klein JCEM 2002; 87: 5746
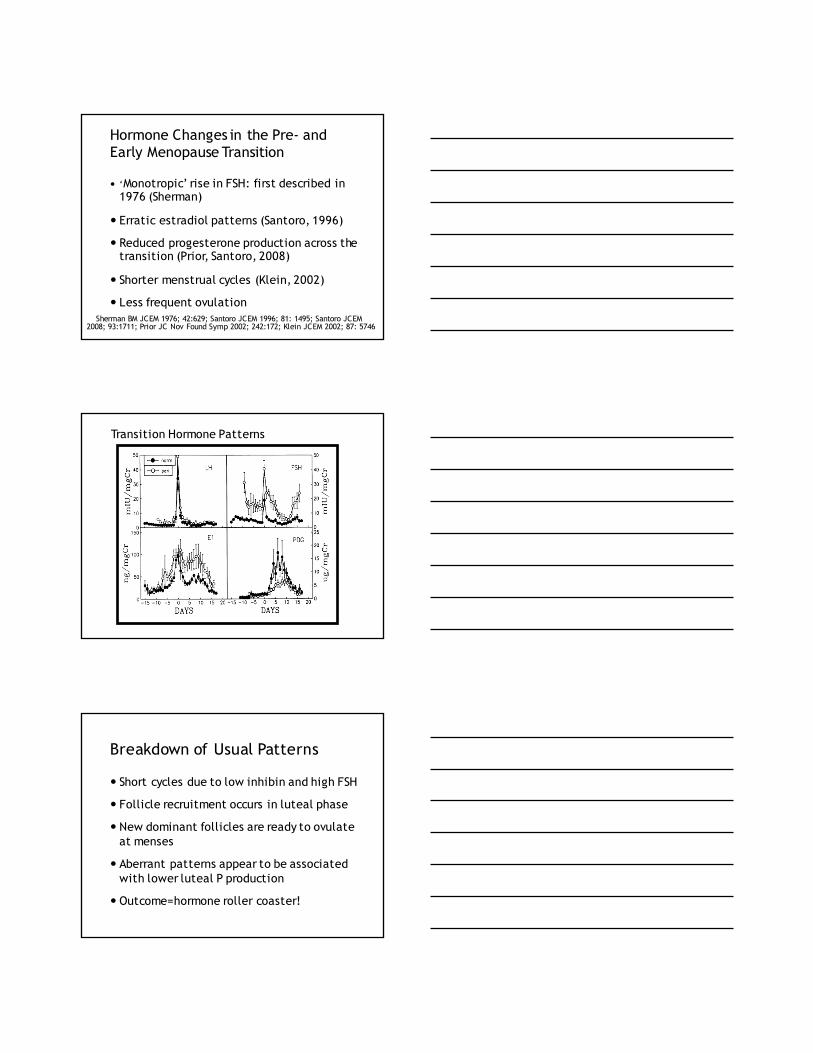
Transition Hormone Patterns
Breakdown of Usual Patterns
Short cycles due to low inhibin and high FSH
Follicle recruitment occurs in luteal phase
New dominant follicles are ready to ovulate at menses
Aberrant patterns appear to be associated with lower luteal P production
Outcome=hormone roller coaster!
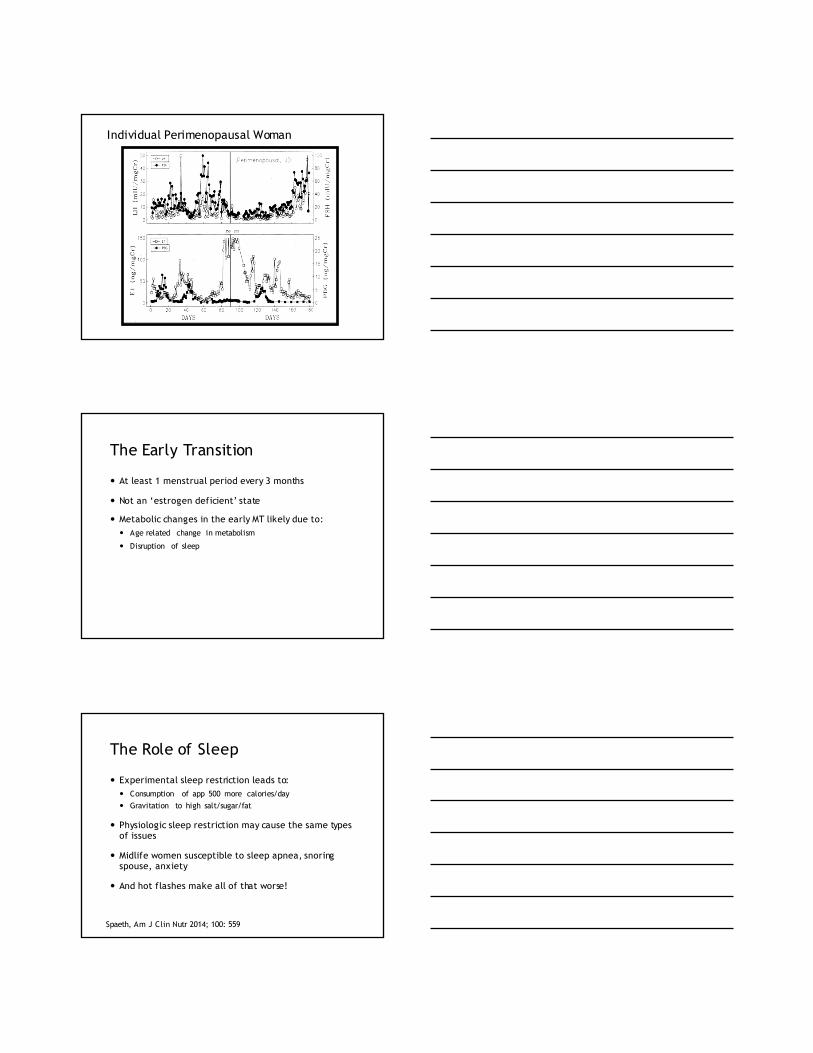
Individual Perimenopausal Woman
The Early Transition
At least 1 menstrual period every 3 months
Not an ‘estrogen deficient’ state
Metabolic changes in the early MT likely due to: Age related change in metabolism
Disruption of sleep
The Role of Sleep
Experimental sleep restriction leads to: Consumption of app 500 more calories/day Gravitation to high salt/sugar/fat
Physiologic sleep restriction may cause the same types of issues
Midlife women susceptible to sleep apnea, snoring spouse, anxiety
And hot flashes make all of that worse!
Spaeth, Am J Clin Nutr 2014; 100: 559
Copyr ight r est r ict ions m ay apply.
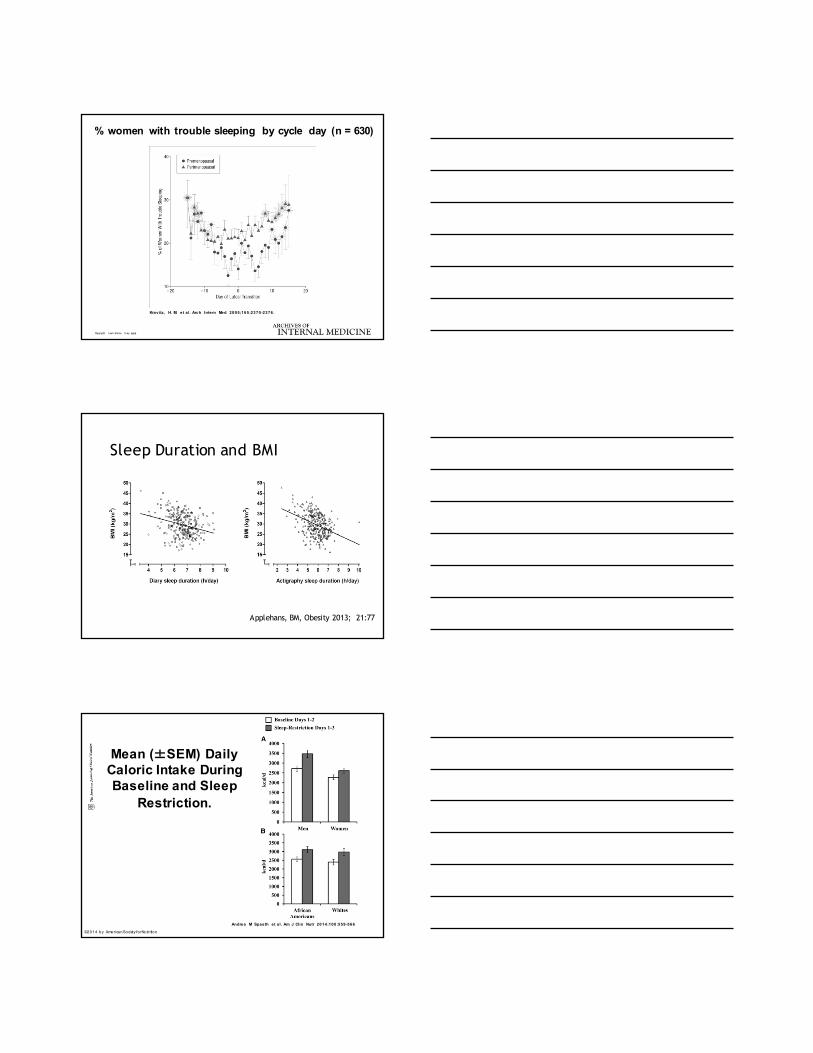
Kravitz , H. M. et a l. Arch Intern Med 2005;;165:2370-2376.
% women with trouble sleeping by cycle day (n = 630)
Sleep Duration and BMI
Applehans, BM, Obesity 2013; 21:77
Mean (±SEM) Daily Caloric Intake During Baseline and Sleep
Restriction.
Andrea M Spaeth et a l. Am J Clin Nutr 2014;;100:559-566
©2014 by American Society for Nutri tion
The Late Menopause Transition
60+ days of amenorrhea
Estrogen deficiency predominates Sleep gets even worse! Hot flashes get worse—up to 85% of
women affected SHBG and androgen metabolism shifts Changes in cardiometabolic markers
become evident
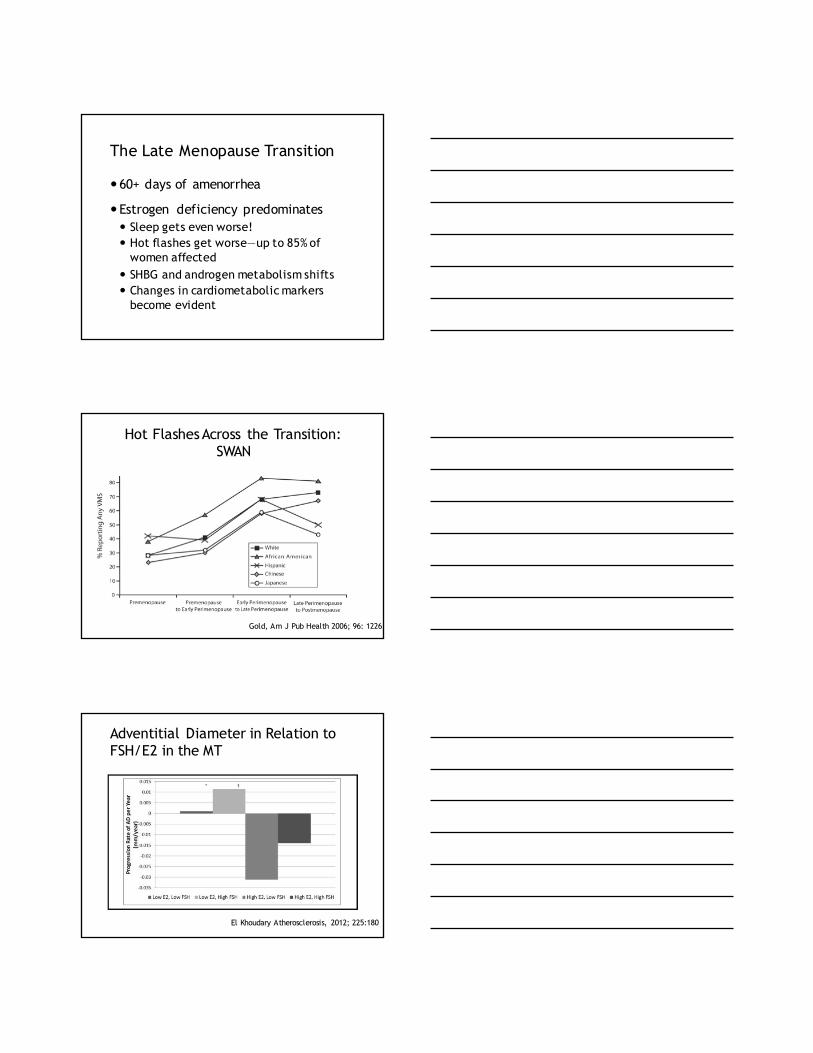
Hot Flashes Across the Transition: SWAN
Gold, Am J Pub Health 2006; 96: 1226
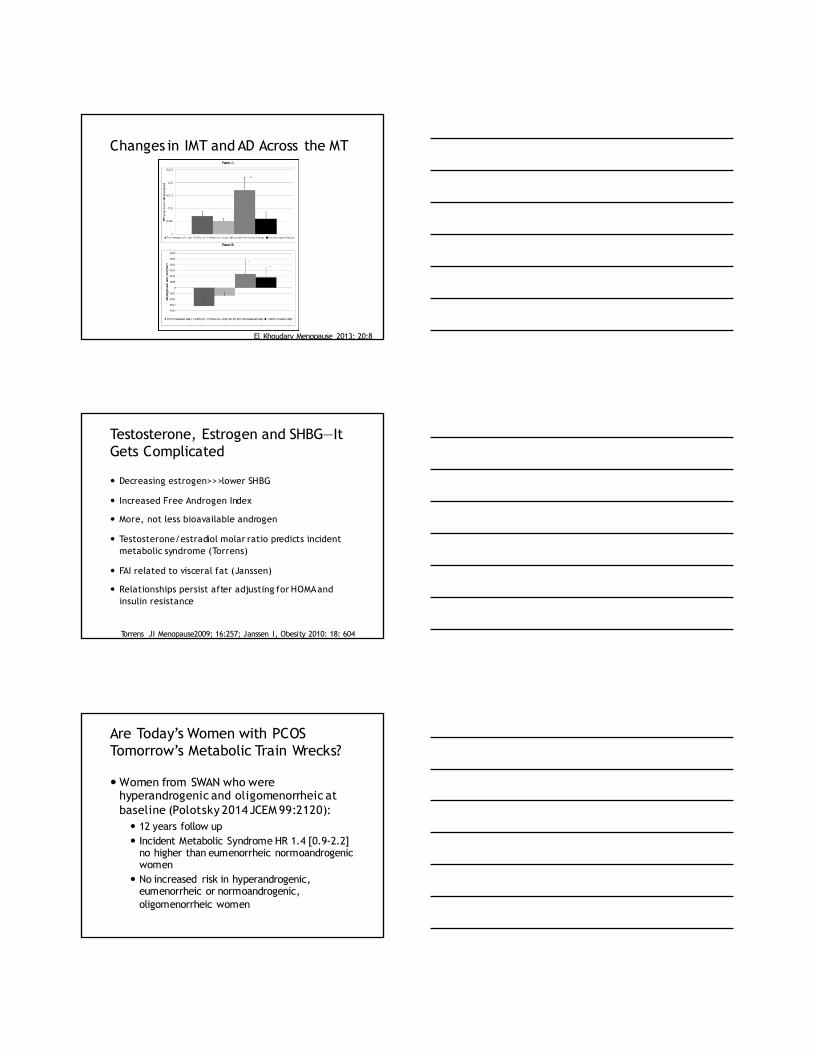
Adventitial Diameter in Relation to FSH/E2 in the MT
El Khoudary Atherosclerosis, 2012; 225:180
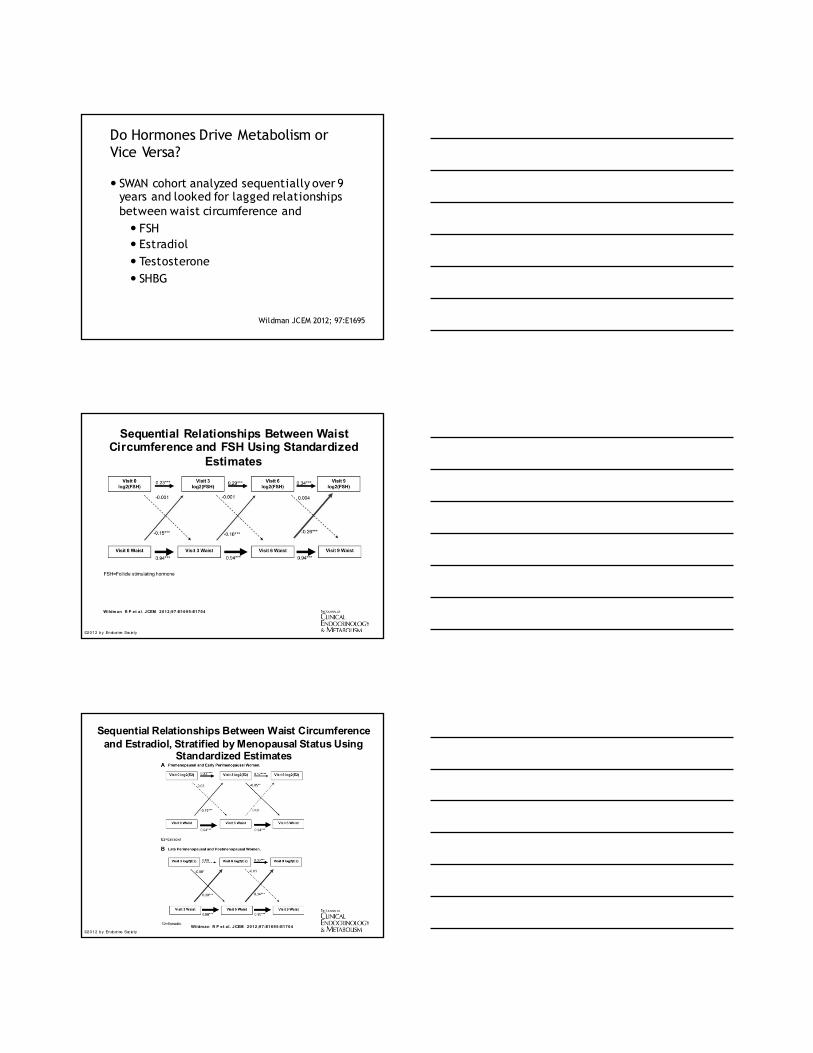
Changes in IMT and AD Across the MT
El Khoudary Menopause 2013; 20:8
Testosterone, Estrogen and SHBG—It Gets Complicated
Decreasing estrogen>>>lower SHBG
Increased Free Androgen Index
More, not less bioavailable androgen
Testosterone/estradiol molar ratio predicts incident metabolic syndrome (Torrens)
FAI related to visceral fat (Janssen)
Relationships persist after adjusting for HOMA and insulin resistance
Torrens JI Menopause2009; 16:257; Janssen I, Obesity 2010: 18: 604
Are Today’s Women with PCOS Tomorrow’s Metabolic Train Wrecks?
Women from SWAN who were hyperandrogenic and oligomenorrheic at baseline (Polotsky 2014 JCEM 99:2120): 12 years follow up Incident Metabolic Syndrome HR 1.4 [0.9-2.2]
no higher than eumenorrheic normoandrogenicwomen
No increased risk in hyperandrogenic, eumenorrheic or normoandrogenic, oligomenorrheic women
Do Hormones Drive Metabolism or Vice Versa?
SWAN cohort analyzed sequentially over 9 years and looked for lagged relationships between waist circumference and FSH Estradiol Testosterone SHBG
Wildman JCEM 2012; 97:E1695
Sequential Relationships Between Waist Circumference and FSH Using Standardized
Estimates
Wildman R P et a l. JCEM 2012;;97:E1695-E1704
©2012 by Endocrine Soc iety
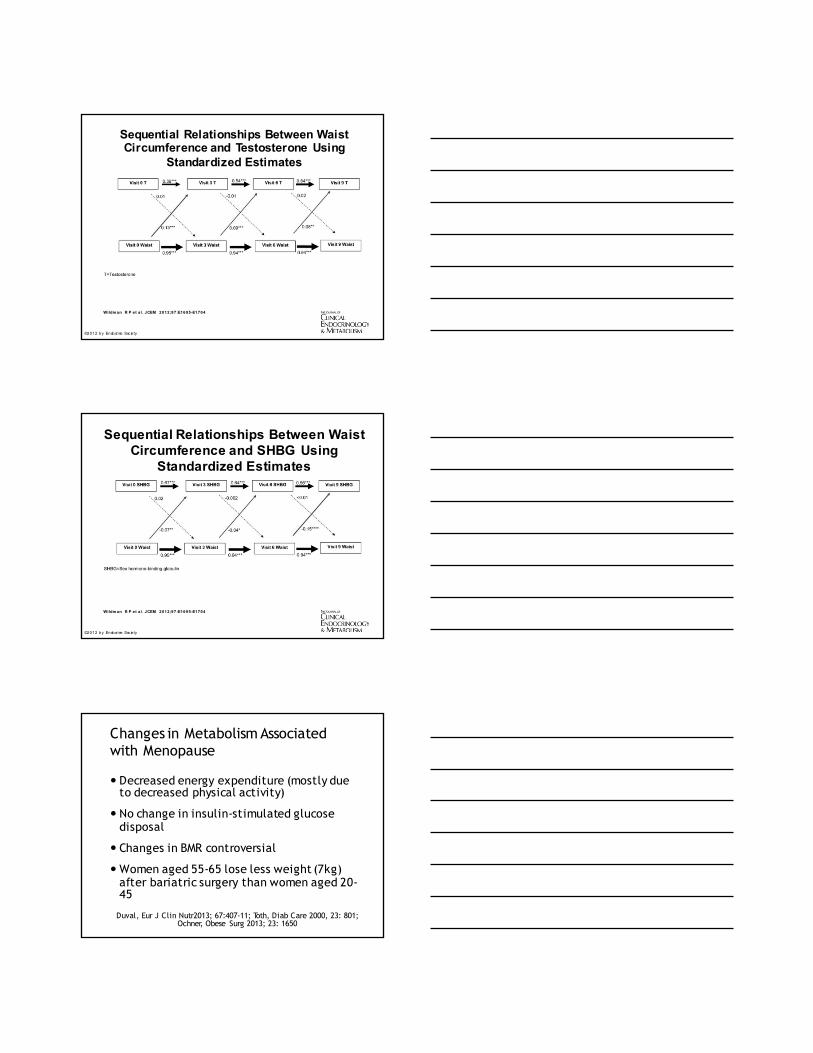
Sequential Relationships Between Waist Circumference and Estradiol, Stratified by Menopausal Status Using
Standardized Estimates
Wildman R P et a l. JCEM 2012;;97:E1695-E1704©2012 by Endocrine Soc iety
Sequential Relationships Between Waist Circumference and Testosterone Using
Standardized Estimates
Wildman R P et a l. JCEM 2012;;97:E1695-E1704
©2012 by Endocrine Soc iety
Sequential Relationships Between Waist Circumference and SHBG Using
Standardized Estimates
Wildman R P et a l. JCEM 2012;;97:E1695-E1704
©2012 by Endocrine Soc iety
Changes in Metabolism Associated with Menopause
Decreased energy expenditure (mostly due to decreased physical activity)
No change in insulin-stimulated glucose disposal
Changes in BMR controversial
Women aged 55-65 lose less weight (7kg) after bariatric surgery than women aged 20-45
Duval, Eur J Clin Nutr2013; 67:407-11; Toth, Diab Care 2000, 23: 801; Ochner, Obese Surg 2013; 23: 1650
The Role of Mood
Adverse mood is a common menopausal symptom
Risk for new onset major depression increases (16% prevalence)
Anxiety follows a similar pattern
Depression and Anxiety
Adverse mood most likely in the LATE transition
Women with minimal pre-existing symptoms are most vulnerable (Soares, Drugs Aging 2013; 30:677)
Experimental induction of perimenopausewith VCD decreases P and DHT and produces anxiety symptoms in animal model (Reis, Psychoneuroendocrinology 2014: 49:130)
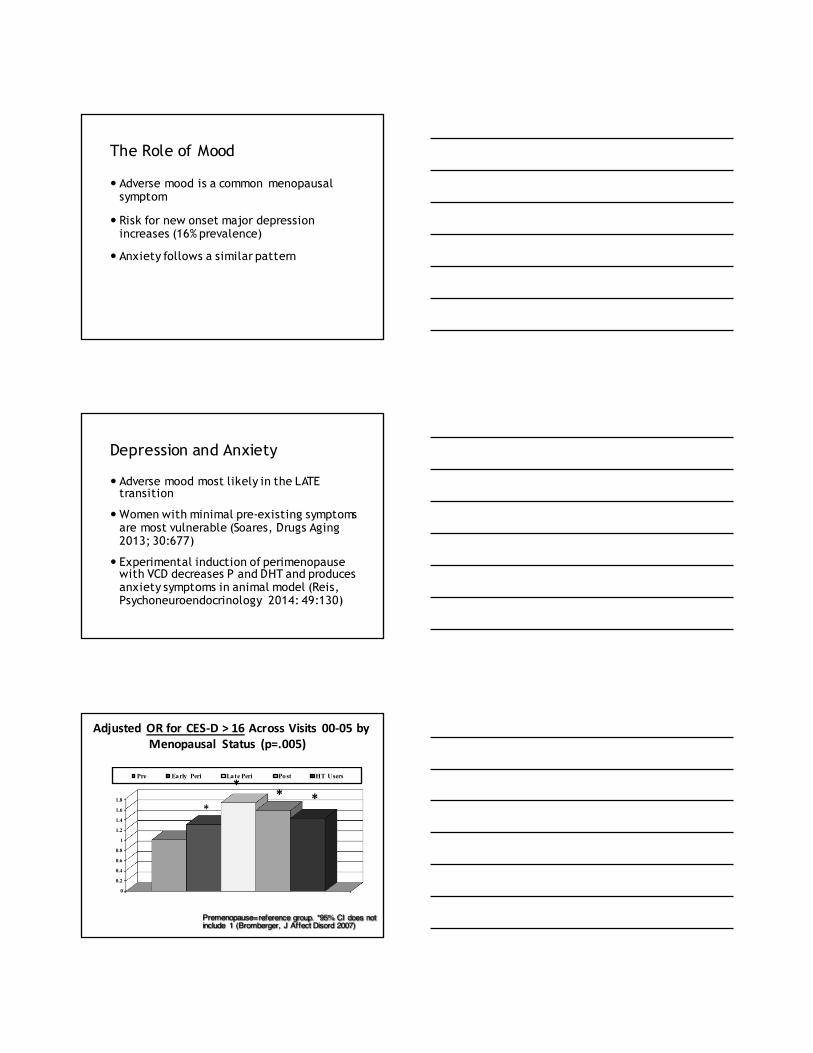
Adjusted OR for CES-‐D > 16 Across Visits 00-‐05 by Menopausal Status (p=.005)
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
Pre Early Peri Late Peri Post HT Users
Premenopause=reference group. *95% CI does not include 1 (Bromberger, J Affect Disord 2007)
***
*
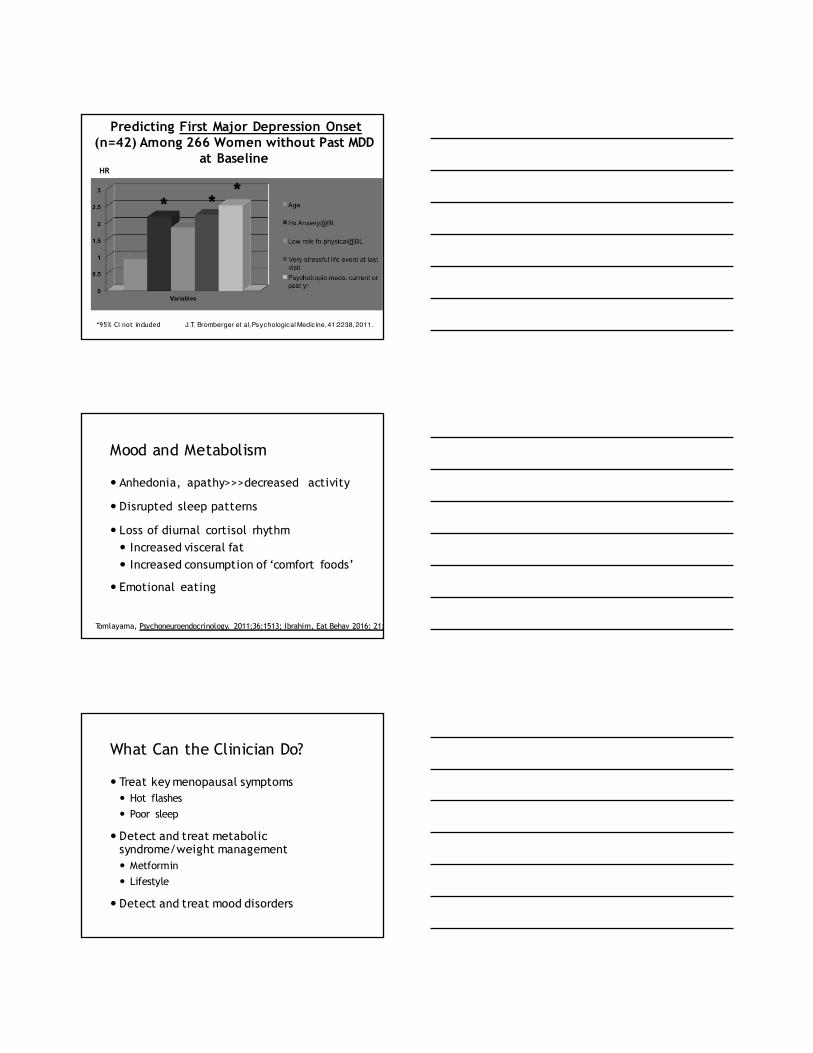
Predicting First Major Depression Onset(n=42) Among 266 Women without Past MDD
at BaselineHR
J.T. Bromberger et al, Psychological Medicine, 41:2238, 2011.
* **
*95% CI not included
Mood and Metabolism
Anhedonia, apathy>>>decreased activity
Disrupted sleep patterns
Loss of diurnal cortisol rhythm Increased visceral fat Increased consumption of ‘comfort foods’
Emotional eating
Tomlayama, Psychoneuroendocrinology. 2011;36:1513; Ibrahim, Eat Behav 2016; 21:214;
What Can the Clinician Do?
Treat key menopausal symptoms Hot flashes Poor sleep
Detect and treat metabolic syndrome/weight management Metformin Lifestyle
Detect and treat mood disorders

Exercise: An Essential Modifier
Maintains weight
Maintains endothelial function
Improves insulin sensitivity
Raises HDL
Mindfulness: An Essential Modifier
May reduce BP
Reduces stress
Improves chronic pain
Improves sleep (mindfulness CBT)
Abbot J Psychosom Res 2014; 76:361; Cherkin, JAMA 2016; 315: 1240; Schramm PJ, Sleep Med 2016; 17:57
Hormones
Reduce/eliminate hot flashes
May improve sleep, vaginal symptoms, mood
Reduces incident diabetes by 7% per year
Summary
Midlife introduces a set of age and menopause related challenges that affect a woman’s homeostasis
Sleep, mood and physical activity may all be altered by the menopausal transition
Hormones may play a role in affecting metabolism directly but more likely indirectly
Clinicians can help their patients adapt