how is perinatal/neonatal care changing?...jama pediatrics journal club slides: variation in...
TRANSCRIPT

10/28/2018
1
How is perinatal/neonatal care changing?
Reese H. Clark, MD
10/28/2018
Disclosure Statements
•We have no relevant financial relationships to disclose or conflicts of interest to resolve.
• The off-label use of any drug will be identified, discussed and strongly discouraged.
10/28/2018
Premature Birth is Still a Problem
10/28/2018
Describing the Increase in Preterm Births in the United States, 2014–2016. Joyce A. Martin, M.P.H., and Michelle J.K. Osterman, M.H.S. NCHS Data Brief. No. 312 June 2018
10/28/2018
Describing the Increase in Preterm Births in the United States, 2014–2016. Joyce A. Martin, M.P.H., and Michelle J.K. Osterman, M.H.S. NCHS Data Brief. No. 312 June 201810/28/2018
Describing the Increase in Preterm Births in the United States, 2014–2016. Joyce A. Martin, M.P.H., and Michelle J.K. Osterman, M.H.S. NCHS Data Brief. No. 312 June 201810/28/2018

10/28/2018
2
Describing the Increase in Preterm Births in the United States, 2014–2016. Joyce A. Martin, M.P.H., and Michelle J.K. Osterman, M.H.S. NCHS Data Brief. No. 312 June 201810/28/2018
Neonatal Abstinence is Still a Problem
10/28/2018
This report, the information contained herein, and the underlying data from which the report is drawn, are proprietary and constitute Patient Safety Work Product ("PSWP") pursuant to the Patient Safety and Quality Improvement Act of 2005 and the regulations promulgated thereunder. 10/28/2018 10/28/2018
The Opioid Epidemic Continues to Kill Indiscriminately
10/28/2018 10/28/2018

10/28/2018
3
10/28/2018 10/28/2018
10/28/2018
Changes in Prenatal/Neonatal Care and Improvement in Outcomes
10/28/2018
JAMA. 2015;314(10):1039-1051. doi:10.1001/jama.2015.10244
10/28/2018
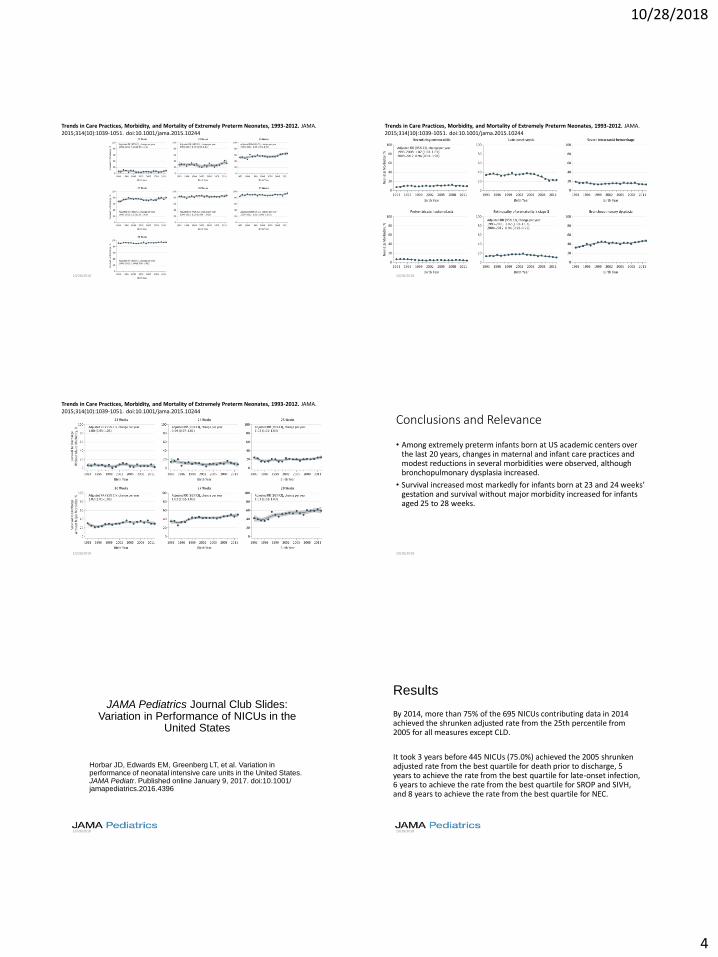
Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993-2012. JAMA. 2015;314(10):1039-1051. doi:10.1001/jama.2015.10244
10/28/2018
10/28/2018
4
Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993-2012. JAMA. 2015;314(10):1039-1051. doi:10.1001/jama.2015.10244
10/28/2018
Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993-2012. JAMA. 2015;314(10):1039-1051. doi:10.1001/jama.2015.10244
10/28/2018
Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993-2012. JAMA. 2015;314(10):1039-1051. doi:10.1001/jama.2015.10244
10/28/2018
Conclusions and Relevance
• Among extremely preterm infants born at US academic centers over the last 20 years, changes in maternal and infant care practices and modest reductions in several morbidities were observed, although bronchopulmonary dysplasia increased.
• Survival increased most markedly for infants born at 23 and 24 weeks’ gestation and survival without major morbidity increased for infants aged 25 to 28 weeks.
10/28/2018
JAMA Pediatrics Journal Club Slides:Variation in Performance of NICUs in the
United States
Horbar JD, Edwards EM, Greenberg LT, et al. Variation in performance of neonatal intensive care units in the United States. JAMA Pediatr. Published online January 9, 2017. doi:10.1001/ jamapediatrics.2016.4396
10/28/2018
Results
By 2014, more than 75% of the 695 NICUs contributing data in 2014 achieved the shrunken adjusted rate from the 25th percentile from 2005 for all measures except CLD.
It took 3 years before 445 NICUs (75.0%) achieved the 2005 shrunken adjusted rate from the best quartile for death prior to discharge, 5 years to achieve the rate from the best quartile for late-onset infection, 6 years to achieve the rate from the best quartile for SROP and SIVH, and 8 years to achieve the rate from the best quartile for NEC.
10/28/2018

10/28/2018
5
Risk-Adjusted Rates of Outcomes in the NICU at the 10th, 25th, 50th, 75th, and 90th
Percentiles, 2005-2014, With the Dark Blue, Light Blue, and Dotted Red Curves Indicating 10th/90th, 25th/75th, and 50th Percentiles, Respectively
0%2%4%6%8%
10%12%14%16% Mortality
0%
5%
10%
15%
20%
25%
30%Late-Onset Infection
0%5%
10%15%20%25%30%35%40%
CLD
0%2%4%6%8%
10%12%14%
NEC
0%2%4%6%8%
10%12%14%
SIVH
0%2%4%6%8%
10%12%14%16%
SROP
10/28/2018
Comment
• By 2014, more than 75% of NICUs in the United States had learned to perform as well or better than the best 25% of NICUs performed in 2005 for major morbidities other than CLD.
• The increased adoption of evidence-based practices and their implementation using quality improvement methods may have contributed to these gains.
• These findings provide a novel way to quantify the magnitude and pace of improvement in neonatology.
10/28/2018
Treatment of ROP
10/28/2018
Mintz-Hittner HA, Kennedy KA, Chuang AZ. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med 2011;364(7):603-615.
• Enrolled 150 infants (total sample of 300 eyes); 143 infants survived
to 54 weeks' postmenstrual age, and the 7 infants who died.
• Retinopathy of prematurity recurred in 4 infants in the bevacizumab
group (6 of 140 eyes [4%]) and 19 infants in the laser-therapy group
(32 of 146 eyes [22%], P=0.002).
• A significant treatment effect was found for zone I retinopathy of
prematurity (P=0.003) but not for zone II disease (P=0.27).
10/28/2018
Morin J, Luu TM, Superstein R et al. Neurodevelopmental Outcomes Following Bevacizumab Injections for Retinopathy of Prematurity. Pediatrics 2016;137(4).Canadian Neonatal Follow-Up Network
• Concerns about systemic absorption and effect on developing tissues including brain. Infants born at <29 weeks' in 2010-2011 with treated ROP were studied.
• Of 125 treated infants, 27 received bevacizumab and 98 laser. At least 11 infants who received laser ablation did not fulfill current recommendations for ROP treatment.
• Odds of severe neurodevelopmental disabilities (Bayley scores <70, severe cerebral palsy, hearing aids, or bilateral blindness) was 3.1 times higher (95% confidence interval: 1.2-8.4) in infants treated with bevacizumab versus laser.
• Statistically adjusted for gestational age, gender, maternal education, Score for Neonatal Acute Physiology-II score, bronchopulmonary dysplasia, sepsis, and severe brain injury.
10/28/2018
Wallace DK, Kraker RT, Freedman SF et al. Assessment of Lower Doses of Intravitreous Bevacizumab for Retinopathy of Prematurity: A Phase 1 Dosing Study. JAMA Ophthalmol 2017;135(6):654-656.http://jamanetwork.com/journals/jamaophthalmology/article-abstract/2621875
• Objective: To find a dose of intravitreous bevacizumab that was lower than previously used for severe ROP, was effective in this study, and could be tested in future larger studies.
• Between May 2015 and September 2016, 61 premature infants with type 1 ROP in 1 or both eyes were enrolled in a masked, multicenter, phase 1 dose de-escalation study.
• One eye of 10 to 14 infants received 0.25 mg of intravitreous bevacizumab. If successful, the dose was reduced for the next group of infants (to 0.125 mg, then 0.063 mg, and finally 0.031 mg).
• Main Outcomes and Measures: Success was defined as improvement in preinjection plus disease or zone I stage 3 ROP by 5 days after injection or sooner, and no recurrence of type 1 ROP or severe neovascularization requiring additional treatment within 4 weeks.
10/28/2018

10/28/2018
6
Wallace DK, Kraker RT, Freedman SF et al. Assessment of Lower Doses of Intravitreous Bevacizumab for Retinopathy of Prematurity: A Phase 1 Dosing Study. JAMA Ophthalmol 2017;135(6):654-656.http://jamanetwork.com/journals/jamaophthalmology/article-abstract/2621875
• Results: Fifty-eight of 61 enrolled infants had 4-week outcomes completed; mean birth weight was 709 g and mean gestational age was 24.9 weeks. Success was achieved in 11 of 11 eyes at 0.25 mg, 14 of 14 eyes at 0.125 mg, 21 of 24 eyes at 0.063 mg, and 9 of 9 eyes at 0.031 mg.
• Conclusions and Relevance: A dose of bevacizumab as low as 0.031 mg was effective in 9 of 9 eyes in this phase 1 study and warrants further investigation.
• (0.625/0.031= 20)
10/28/2018
VanderVeen DK, Melia M, Yang MB, Hutchinson AK, Wilson LB, Lambert SR. Anti-Vascular Endothelial Growth Factor Therapy for Primary Treatment of Type 1 Retinopathy of Prematurity: A Report by the American Academy of Ophthalmology. Ophthalmology 2017;124(5):619-633.
• Level II and III evidence indicates that intravitreal anti-VEGF therapy is as effective as laser photocoagulation for achieving regression of acute ROP.
• Although there are distinct ocular advantages to anti-VEGF pharmacotherapy for some cases (such as eyes with zone I disease or aggressive posterior ROP), the disadvantages are that the ROP recurrence rate is higher, and vigilant and extended follow-up is needed because retinal vascularization is usually incomplete.
• After intravitreal injection, bevacizumab can be detected in serum within 1 day, and serum VEGF levels are suppressed for at least 8 to 12 weeks. The effects of lowering systemic VEGF levels on the developing organ systems of premature infants are unknown, and there are limited long-term data on potential systemic and neurodevelopmental effects after anti-VEGF use for ROP treatment.
• Anti-VEGF agents should be used judiciously and with awareness of the known and unknown or potential side effects
10/28/2018
Report of ROP Treatment For All Admissions
0.00%0.10%0.20%0.30%0.40%0.50%0.60%0.70%0.80%0.90%
199
9(2525
9)
200
0(3292
9)
200
1(3599
9)
200
2(4066
6)
200
3(4734
9)
200
4(5561
3)
200
5(6326
3)
200
6(7087
7)
200
7(7435
6)
200
8(7923
1)
200
9(7988
3)
201
0(8277
8)
201
1(8514
9)
201
2(8599
4)
201
3(8678
6)
201
4(9099
9)
201
5(9305
6)
201
6(9065
9)
Perc
ent
of
All
Ad
mis
sio
ns
Year (N)
Bevacizumab (Avastin) Laser Both Any Rx
10/28/2018
Report of ROP Treatment For All Admissions
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
22 23 24 25 26 27 28 29 30 31 32
Perc
ent
of
All
Ad
mis
sio
ns
EGA
Avastin Only Laser Both
10/28/2018
ROP RX Counts
GestAge <=500 501 to 750 751 to 1 1001 to 1250 1251 to 1500 1501 to 1750 Total
22 9 16 1 26
23 59 316 10 385
24 68 507 102 1 678
25 41 263 195 6 505
26 28 109 148 23 308
27 10 39 67 41 2 159
28 4 8 29 32 9 1 83
29 2 8 18 12 9 1 50
30 1 5 7 4 3 20
31 1 3 1 1 1 7
Total 221 1268 578 123 25 6 2221
Number of Patients Treated for ROP (Total=2221)There were 19/2221 (0.9%) that were more than 1250 grams and more than 28 weeks
All admits and discharge types. EGA >=22 and <=31 weeks and Bwt >=400 and <=1750 grams; Discharged between 2010 and 201610/28/2018
• 370 CRFs; 327 were included.
• 8112 infants with birth weight of <1500 g. 4% (327/8112, 95% CI 3.6% to 4.5%). CDW = 3.3%
• First-line treatment was diode laser photoablation of the avascular retina in 90.5% and injection of VEGF inhibitor in 8%. CDW=12%
• ROP treatment incidence in the UK is 2.5 times higher than previously estimated. 8% of treated infants receive intravitreal VEGF inhibitor, currently unlicensed.
• Research is needed urgently to establish safety and efficacy of this approach.
Adams GG, Bunce C, Xing W et al. Treatment trends for retinopathy of prematurity in the UK: active surveillance study of infants at risk. BMJ Open 2017;7(3):e013366.
10/28/2018

10/28/2018
7
Walz JM, Bemme S, Pielen A et al. The German ROP Registry: data from 90 infants treated for retinopathy of prematurity. Acta Ophthalmol 2016;94(8):e744-e752.
• The German retinopathy of prematurity (ROP) Registry
• Nine centres entered data from 90 treated ROP infants (born between January 2011 and December 2013) into a central database.
• Treatment rate for ROP was 3.2% of the screened population. The most frequent ROP stage at time of treatment was zone II, stage 3 + (137 eyes).
• Treatment patterns changed over time from 7% anti-vascular endothelial growth factor (VEGF) monotherapy in 2011 to 32% in 2014.
• Overall, laser treatment was the predominant treatment. However, all infants with zone I disease received anti-VEGF treatment.
• About 19% of infants required retreatment (16% of laser-treated and 21% of anti-VEGF treated infants).
10/28/2018
Report of ROP TreatmentEGA >=22 and <=31 weeks and Bwt >=400 and <=1750 grams; Discharged between 2010 and 2016
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
201
0
201
1
201
2
201
3
2014
201
5
201
6
Year (N)
Bevacizumab (Avastin) Laser Any ROP Treatment
10/28/2018
Treatment of the PDA
10/28/2018
Changes in the Diagnosis and Management of Patent
Ductus Arteriosus from 2006 to 2015 in United States
Neonatal Intensive Care Units
G. Michael Bixler, MD, George C. Powers, MD, Reese H. Clark, MD, M. Whit Walker,
MD, Veeral N. Tolia, MD
The Journal of Pediatrics
Volume 189, Pages 105-112 (October 2017) DOI: 10.1016/j.jpeds.2017.05.024
The Journal of Pediatrics Volume 189, Pages 105-112, 2017
10/28/2018
Change in the proportion of infants treated with PDA ligation, 2006-2010 compared with 2011-2015. Of 103 sites with data from both periods and at least one PDA ligation, 85 (83%) showed a decrease in PDA ligations.
10/28/2018
10/28/2018
8
Management of Infants with Suspected Sepsis
10/28/2018
IS THERE A BETTER WAY TO THINK ABOUT NEONATAL SEPSIS?
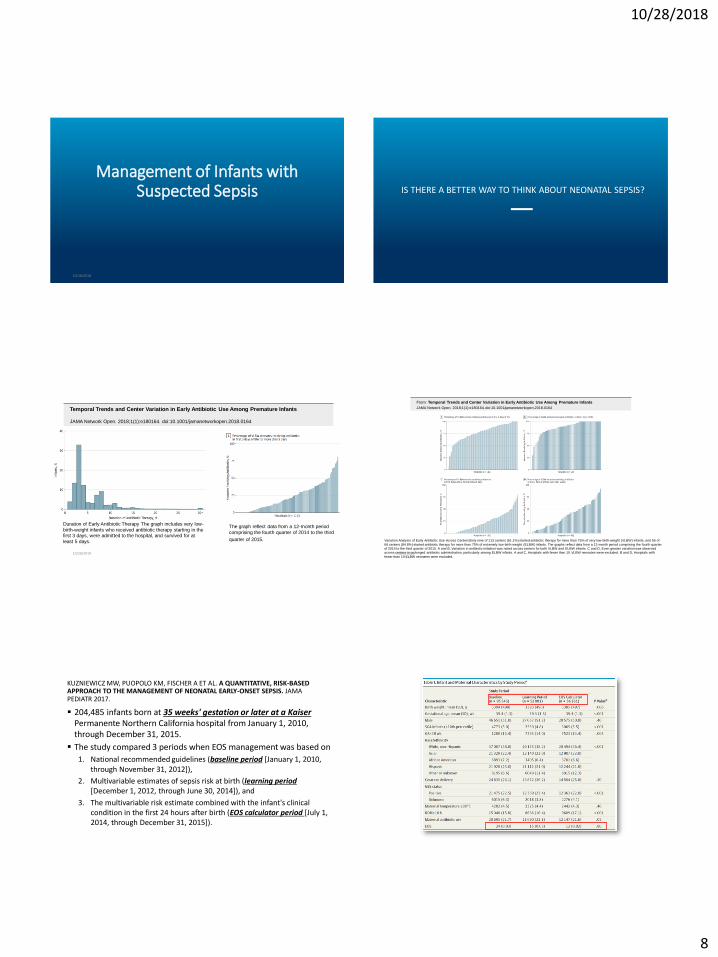
Temporal Trends and Center Variation in Early Antibiotic Use Among Premature Infants
JAMA Network Open. 2018;1(1):e180164. doi:10.1001/jamanetworkopen.2018.0164
Duration of Early Antibiotic Therapy The graph includes very low-
birth-weight infants who received antibiotic therapy starting in the first 3 days, were admitted to the hospital, and survived for at
least 5 days.
The graph reflect data from a 12-month period
comprising the fourth quarter of 2014 to the third
quarter of 2015.
10/28/2018
From: Temporal Trends and Center Variation in Early Antibiotic Use Among Premature Infants
JAMA Network Open. 2018;1(1):e180164. doi:10.1001/jamanetworkopen.2018.0164
Variation Analysis of Early Antibiotic Use Across CentersSixty-nine of 113 centers (61.1%) started antibiotic therapy for more than 75% of very low-birth-weight (VLBW) infants, and 56 of
66 centers (84.8%) started antibiotic therapy for more than 75% of extremely low-birth-weight (ELBW) infants. The graphs reflect data from a 12-month period comprising the fourth quarter
of 2014 to the third quarter of 2015. A and B, Variation in antibiotic initiation was noted across centers for both VLBW and ELBW infants. C and D, Even greater variation was observed
across centers in prolonged antibiotic administration, particularly among ELBW infants. A and C, Hospitals with fewer than 10 VLBW neonates were excluded. B and D, Hospitals with
fewer than 10 ELBW neonates were excluded.10/28/2018
204,485 infants born at 35 weeks' gestation or later at a KaiserPermanente Northern California hospital from January 1, 2010, through December 31, 2015.
The study compared 3 periods when EOS management was based on
1. National recommended guidelines (baseline period [January 1, 2010, through November 31, 2012]),
2. Multivariable estimates of sepsis risk at birth (learning period[December 1, 2012, through June 30, 2014]), and
3. The multivariable risk estimate combined with the infant's clinical condition in the first 24 hours after birth (EOS calculator period [July 1, 2014, through December 31, 2015]).
KUZNIEWICZ MW, PUOPOLO KM, FISCHER A ET AL. A QUANTITATIVE, RISK-BASED APPROACH TO THE MANAGEMENT OF NEONATAL EARLY-ONSET SEPSIS. JAMA PEDIATR 2017.

10/28/2018
9
Readmissions for EOS (within 7 days of birth) were rare in all periods (5.2 per 100000 births in the baseline period, 1.9 per 100000 births in the learning period, and 5.3 per 100000 births in the EOS calculator period) and did not differ statistically (P = .70).
Incidence of adverse clinical outcomes, including need for inotropes, mechanical ventilation, meningitis, and death, was unchanged after introduction of the EOS calculator.
KUZNIEWICZ MW, PUOPOLO KM, FISCHER A ET AL. A QUANTITATIVE, RISK-BASED APPROACH TO THE MANAGEMENT OF NEONATAL EARLY-ONSET SEPSIS. JAMA PEDIATR 2017.
KUZNIEWICZ MW, PUOPOLO KM, FISCHER A ET AL. A QUANTITATIVE, RISK-BASED APPROACH TO THE MANAGEMENT OF NEONATAL EARLY-ONSET SEPSIS. JAMA PEDIATR 2017.
KUZNIEWICZ MW, PUOPOLO KM, FISCHER A ET AL. A QUANTITATIVE, RISK-BASED APPROACH TO THE MANAGEMENT OF NEONATAL EARLY-ONSET SEPSIS. JAMA PEDIATR 2017.
Remember fewer cultures were done during the EOS calculator period
• The infant who died during the learning period had pulmonary hypertension and respiratory failure and underwent immediate treatment with antibiotics, mechanical ventilation, and ECMO.
• The infant who died during the EOS calculator period was born with severe hypoxic-ischemic encephalopathy and underwent immediate treatment with antibiotics, mechanical ventilation, inotropic agents, therapeutic hypothermia, and ECMO.
KUZNIEWICZ MW, PUOPOLO KM, FISCHER A ET AL. A QUANTITATIVE, RISK-BASED APPROACH TO THE MANAGEMENT OF NEONATAL EARLY-ONSET SEPSIS. JAMA PEDIATR. DOI:10.1001 /JAMAPEDIATRICS.2016.4678 PUBLISHED ONLINE FEBRUARY 20, 2017.