how to design, conduct, and analyze vitamin d clinical trials · pdf filehow to design,...
TRANSCRIPT

How to Design, Conduct, and Analyze Vitamin D Clinical Trials
William B. Grant, PhDSunlight, Nutrition and Health Research

Disclosure
• I receive funding from Bio-Tech Pharmacal, Inc. (Fayetteville, Arkansas, USA), a supplier of research-grade vitamin D3.
Outline – Part 1
• Benefits of UVB exposure and vitamin D for
– Cancer
– Cardiovascular disease
– Respiratory tract infections

Outline – Part 2
• Background – few successful vitamin D trials
• Reason: based on guidelines for drugs resulting in vitamin D dose being used.
• Should be based on 25(OH)D concentrations
• Examples: cancer; premature birth
• Steps involved for trials based on 25(OH)D
• Colorectal cancer survival
• Coronary heart disease

UVB, Vitamin D and Cancer
Ecological Studies of UVB and Cancer Incidence and Mortality – The Garland brothers made the first ecological
study of cancer and solar UVB.
– They realized that cancer rates were lowest in the sunniest part of the country and highest in the least sunny part.
– They hypothesized that since vitamin D production is the most important physiological effect of solar radiation, vitamin D was likely the agent.

Colon Cancer Mortality Rates, White Males, United States, 1950-69
4
5
050
0
40
0
50
045
0
35
0
30
0
30
0
35
0
30
0
300
35
0
40
0
35
0
Dotted lines indicate annualsolar radiation doses

UVB Dose Map from NASA

prostatebreast
kidney, urinarystomach

Types of Cancer Reduced by UVB Exposure in the U.S.
• Digestive tract: colon, esophageal, laryngeal, oral, pharyngeal, rectal, small intestine
• Female: breast, endometrial, ovarian, vulvar
• Urogenital: bladder, kidney, prostate, testicular
• Miscellaneous organs: gallbladder, lung, pancreatic, thyroid
• Blood: Hodgkin’s lymphoma, leukemia, non-Hodgkin’s lymphoma

Occupational UVB Exposure
• Data on cancer standardized incidence ratios (SIRs) by sex and 54 occupation categories based on 1.4 million male and 1.36 million female cancer cases for 1961–2005 in the five Nordic countries.
• UVB index used was standardized incidence rate for lip cancer less that for lung cancer.
• Outdoor occupations had the highest UVB index.
• Grant, Dermato-Endocrinology, December 2012
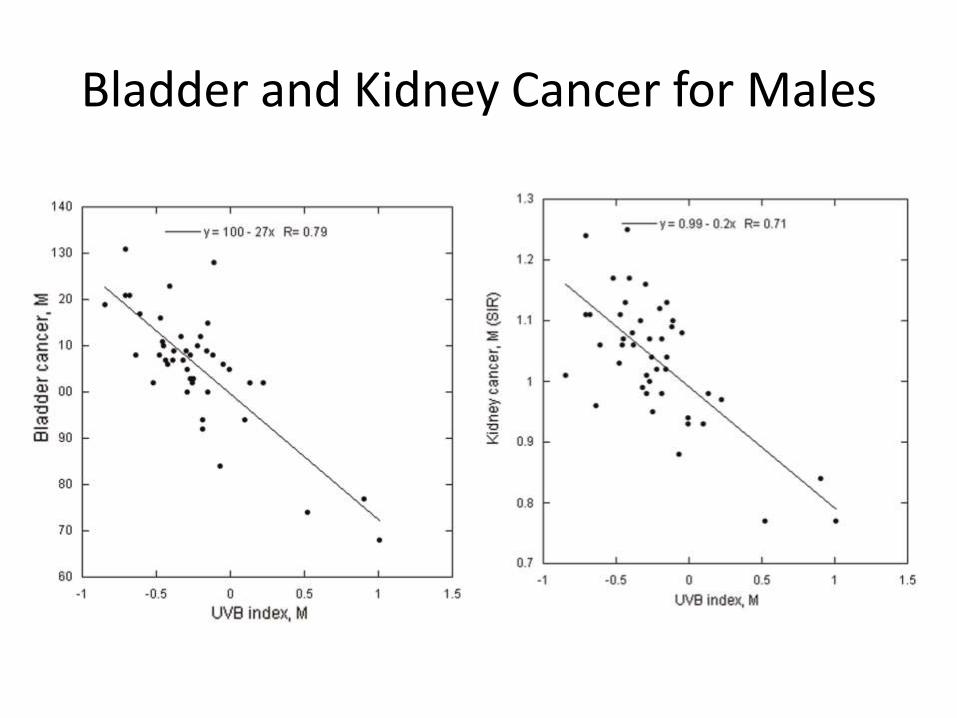
Bladder and Kidney Cancer for Males

Observational Studies
• Observational studies of vitamin D and cancer incidence, survival or mortality rates are generally based on 25(OH)D concentrations.
• In prospective studies, 25(OH)D near the time of cancer diagnosis is a better value than one measured many years prior to cancer diagnosis.
• There is very little evidence that having cancer changes 25(OH)D concentration.
• Thus, case-control studies should be preferred.

Risk of Breast Cancer with Respect to 25(OH)D as Function of Follow-up Period
Grant, Dermato-Endocrinology, 2011

Breast Cancer Incidence Odds Ratio vs. 25(OH)D Concentration
0
0.5
1
1.5
2
2.5
3
0 20 40 60 80 100 120 140 160
OR adjustedOR adjusted low 95% CIOR adjusted high 95% CI
OR
ad
juste
d
25OHD (nmol/L)
Grant WB, Boucher BJ. PLoS One. 2017 May 1;12(5):e0176448.

Clinical Trials on Cancer Incidence
• Three vitamin D clinical trials have found that vitamin D plus cancer reduces risk of cancer
• Lappe et al., 2007
– 1000 IU/d vitamin D, 1450 mg/d calcium
• Women’s Health Initiative [Bolland, 2011]
– 400 IU/d vitamin D3, 1000 mg/d calcium
• Lappe et al., 2017
– 2000 IU/d vitamin D, 1500 mg/d calcium

Cancer Survival in Norway[Tretli, 2012]
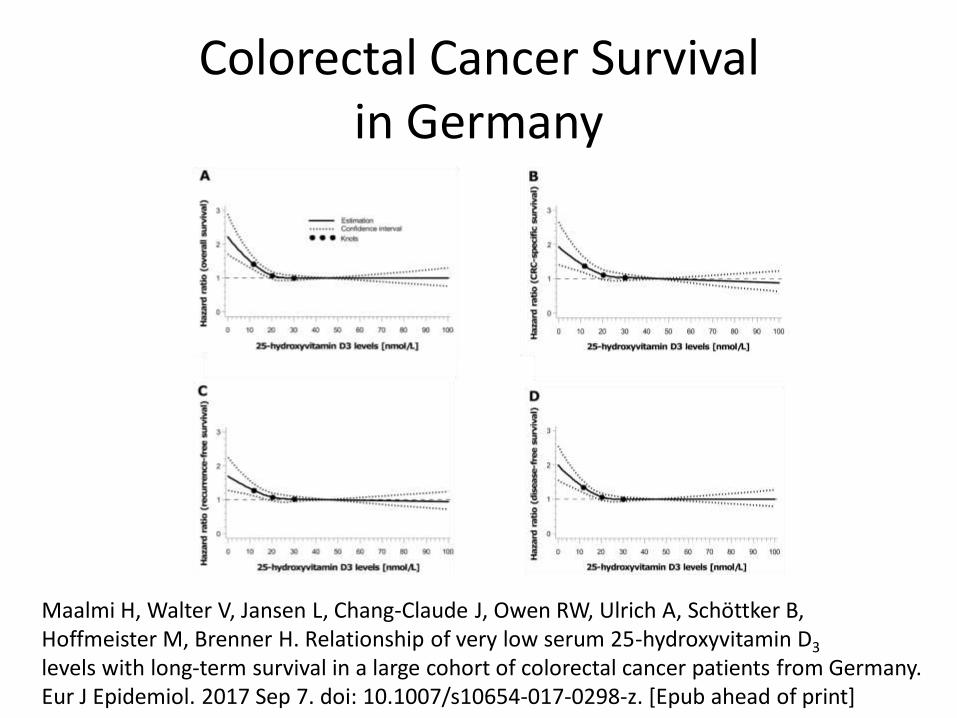
Colorectal Cancer Survivalin Germany
Maalmi H, Walter V, Jansen L, Chang-Claude J, Owen RW, Ulrich A, Schöttker B, Hoffmeister M, Brenner H. Relationship of very low serum 25-hydroxyvitamin D3
levels with long-term survival in a large cohort of colorectal cancer patients from Germany. Eur J Epidemiol. 2017 Sep 7. doi: 10.1007/s10654-017-0298-z. [Epub ahead of print]

Cardiovascular DiseaseMeta-analysis [Wang, 2012]
Vitamin D Supplementation forCardiovascular Health Outcomes.
• Forty-five RCTs were identified. Eight RCTs with BP and 6 RCTs with large artery stiffness as the end points were found to comply with guidelines for the optimal design of clinical trials evaluating nutrient effects. Only 2 of the RCTs with an optimal design were effective in decreasing BP with vitamin D supplementation, although these were of moderate sample size (<150) and very short duration (8 weeks for both), whilst no RCT was effective in reducing large artery stiffness. Similar results were observed for atherosclerotic and endothelial function markers as end points. Only 1 RCT reported cardiovascular events as an end point and found neither increased nor decreased incident cardiovascular events over 7 years of follow-up.
• Veloudi P, Jones G, Sharman JE. Pulse (Basel). 2017 Jan;4(4):193-207

25(OH)D, PTH and Risk of Coronary Heart Disease
Qi L et al. Independent and Synergistic Associations of Biomarkers of Vitamin D Status With Risk of Coronary Heart Disease. Arterioscler Thromb Vasc Biol. 2017 Sep 7
Mean 25(OH)D for quartiles: 43, 58, 69, 84 nmol/L

Respiratory Tract Infections
• Sunlight exposure was the common treatment for tuberculosis before the widespread use of antibiotics.
• Vitamin D fights bacteria and some viruses through induction of cathelicidin, a polypeptide with antimicrobial and antiendotoxin properties.

Influenza
• John Cannell proposed that influenza was largely seasonal due to seasonal variations in solar UVB doses.
• Two clinical trials, one involving post-menopausal African-American women, the other involving Japanese school children, supported that hypothesis.
• (Cold temperature also contributes to the seasonality.)
Acute Respiratory Tract Infections (ARIs) - Clinical Trials
• A trial with 100,000 IU/mo vitamin D3 in New Zealand failed to reduce risk of ARIs [Murdoch, 2012].
– Reason: mean baseline 25(OH)D was 72 nmol/L.
• A trial in Mongolia with 300 IU/d reduced risk of ARIs by 50% [Camargo, 2012].
– Reason: mean baseline 25(OH)D was 17 nmol/L.
Meta-analysis of Vitamin D Clinical Trials for Prevention of ARIs - 1
• 25 eligible randomised controlled trials (total 11 321 participants, aged 0 to 95 years) were identified. Vitamin D supplementation reduced the risk of ARI among all participants (adjusted OR 0.88, 95% confidence interval 0.81 to 0.96; P for heterogeneity <0.001). In subgroup analysis, protective effects were seen in those receiving daily or weekly vitamin D without additional bolus doses (aOR 0.81, 0.72 to 0.91) but not in those receiving one or more bolus doses.

Meta-analysis of Vitamin D Clinical Trials for Prevention of ARIs - 2
• Among those receiving daily or weekly vitamin D, protective effects were stronger in those with baseline 25(OH)D levels <25 nmol/L (aOR0.30, 0.17 to 0.53) than in those with baseline 25(OH)D levels ≥25 nmol/L (aOR 0.75, 0.60 to 0.95; P for interaction=0.006).
• Martineau A, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ, 2017.

How to Design Vitamin D Clinical Trials Based on 25(OH)D Concentration
• With the foregoing as background, we now turn to how to design vitamin D clinical trials based on 25(OH)D concentrations.
Observational Sutdies
• Observational studies based on 25(OH)D concentrations are considered weak evidence for establishing causality.
• 25(OH)D concentrations could be due to:– Dietary components such as meat and eggs with
health effects
– Non-vitamin D effects of UV exposure
– Exercise
– Obesity (generally corrected)

Background
“Our findings suggest that vitamin D supplementation with or without calcium does not reduce skeletal or non-skeletal outcomes in unselected community-dwelling individuals by more than 15%. Future trials with similar designs are unlikely to alter these conclusions.”
• Bolland MJ, Grey A, Gamble GD, Reid IR. Lancet Diabetes Endocrinol. 2014
Problems with Traditional Vitamin D Clinical Trials
1 – Based on the inappropriate guidelines for pharmaceutical drugs
– The trial is the only source of the agent
– There is a linear dose-response relationship
2 – Doses often too low
3 – Baseline 25(OH)D concentration often too high
4 – Poor compliance

Heaney’s [2014] Rules for individual clinical studies of nutrient effects - 1
1. Basal nutrient status must be measured, used as an inclusion criterion for entry into study.
2. The intervention must be large enough to change nutrient status and must be quantified by suitable analyses.
3. The change in nutrient status produced in those enrolled in the trials must be measured and recorded.
Heaney’s [2014] Rules for individual clinical studies of nutrient effects - 2
4. The hypothesis to be tested must be that a change in nutrient status produces the sought-for effect.
5. Conutrient status must be optimized in order to ensure that the test nutrient is the only nutrition related, limiting factor in the response.
• Heaney RP. Guidelines for optimizing design and analysis of clinical studies of nutrient effects. NutrRev. 2014;72(1):48-54.

Variation of 25(OH)D Concentration with Oral Vitamin D Intake
Garland CF, French CB, Baggerly LL, Heaney RP.Anticancer Res. 2011 Feb;31(2):607-11.

Expected Changes in 25(OH)D Concentration for 1000 IU/d vitamin D3
Garland et al. 2011

Proposal: Base Vitamin D Clinical Trials on 25(OH)D Concentration
• The proposal is that vitamin D clinical trials be based on 25(OH)D concentrations, not vitamin D dose.
• 25(OH)D should be measured perhaps 2X/yr.• Basing them on concentrations would have to be
stated in the protocol; otherwise journals may not accept the results.
• Grant WB, Boucher BJ, Bhattoa HJ, Lahore. Why vitamin D clinical trials should be based on 25-hydroxyvitamin D concentrations. JSBMB. J Steroid Biochem Mol Biol. 2017 Aug 22. pii: S0960-0760(17)30223-6.

Clinical Trial: 4 yrs with 2000 IU/d Vitamin D3 + 1500 mg/Ca vs. Placebo
• Among 2303 randomized women (mean age, 65.2 yrs; mean baseline serum 25(OH)D level, 33 ng/mL), mean BMI, 30 kg/m2. At year 1, serum 25(OH)D levels were 44 ng/mL in the vitamin D3 + calcium group and 32 ng/mL in the placebo group. A new diagnosis of cancer was confirmed in 109 participants, 45 (3.9%) in the vitamin D3 + calcium group and 64 (5.6%) in the placebo group.
Clinical Trial: 4 yrs with 2000 IU/d Vitamin D3 + 1500 mg/Ca vs. Placebo
• Kaplan-Meier incidence over 4 years was 0.042 (95% CI, 0.032 to 0.056) in the vitamin D3 + calcium group and 0.060 (95% CI, 0.048 to 0.076) in the placebo group; P = 0.06.
• Unfortunately, insignificant at P = 0.05 level.
• Lappe J, Watson P, Travers-Gustafson D, Recker R, Garland C, Gorham E, Baggerly K, McDonnell SL. JAMA. 2017;317(12):1234-1243
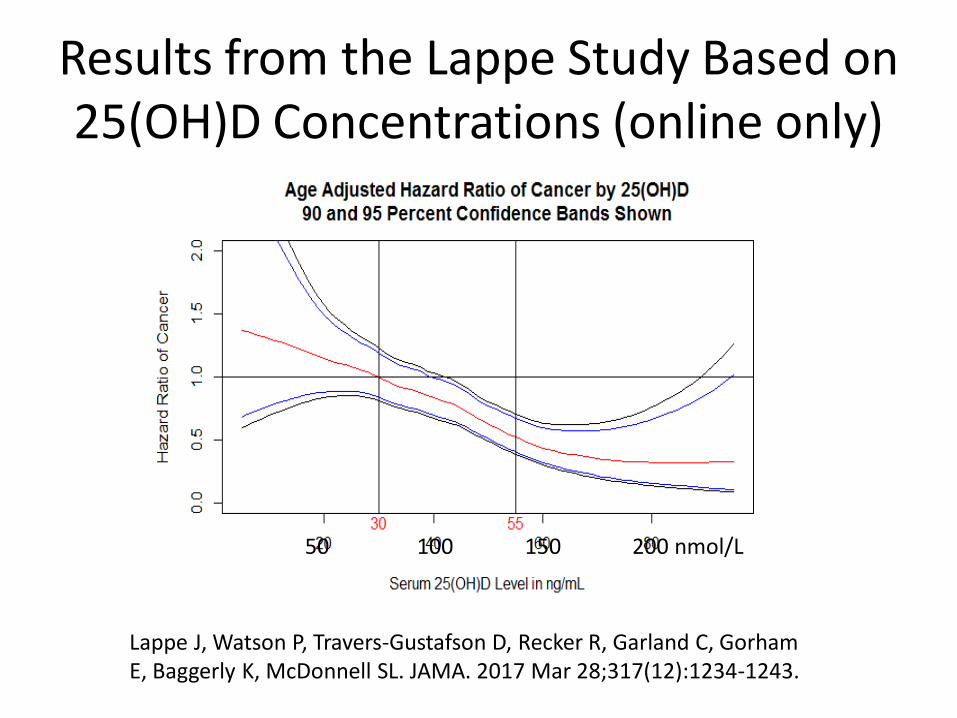
Results from the Lappe Study Based on 25(OH)D Concentrations (online only)
Lappe J, Watson P, Travers-Gustafson D, Recker R, Garland C, Gorham E, Baggerly K, McDonnell SL. JAMA. 2017 Mar 28;317(12):1234-1243.
50 100 150 200 nmol/L

Gestation Week vs. 25(OH)D Concentration
50 100 150 200 nmol/L
McDonnell SL, Baggerly KA, Baggerly CA, Aliano JL, French CB, Baggerly LL, Ebeling MD, Rittenberg CS, Goodier CG, Mateus Niño JF, Wineland RJ, Newman RB, Hollis BW, Wagner CL. PLoS One. 2017 Jul 24;12(7):e0180483.

Steps Involved
1 – Obtain 25(OH)D concentration-health outcome of interest relationship.
2 – Determine the range of baseline and achieved 25(OH)D concentrations desired.
3 – Determine the 25(OH)D concentration distribution of the population of interest (and those likely to be included in the trial).

Obtain Population Data on 25(OH)D concentration
Obtain data on known population distributions of serum 25OHD concentrations, e.g. for Canadians aged 50-79 yrs [Grant, 2016].
Decile 25OHD Decile 25OHD (nmol/L) (nmol/L)
1 28 6 652 35 7 733 42.5 8 824 50 9 905 57.5 10 100 .

Calculate the Expected Incidence vs. 25(OH)D with Supplementation
0
2
4
6
8
10
12
20 30 40 50 60 70 80 90 100
Cancer cases baselineCancer cases, 400 IU/dCancer cases, 1000 IU/dCancer cases, 2000 IU/dCancer cases 4000 IU/d
Cancer
ca
ses b
ase
line
Baseline 25OHD (nmol/L)

Relative Risk Calculations
• - Calculate relative risk (RR) using, e.g., http://www.vassarstats.net/odds2x2.html
• The number of participant-years can be varied to find the number required to achieve significant results at the p=0.05 level. Allow additional numbers to cover poor compliance, drop outs, undue lag times, etc.
• The lower the baseline 25(OH)D concentration, the fewer people needed.

Results for Baseline 25(OH)D = 35 nmol/L, 2000 IU/d
Approximately 1000 participant years required
0
0.5
1
1.5
0 1000 2000 3000 4000 5000
OR for 35 nmol/L95% CI, low95% CI, high
OR
for
35 n
mol/L
N
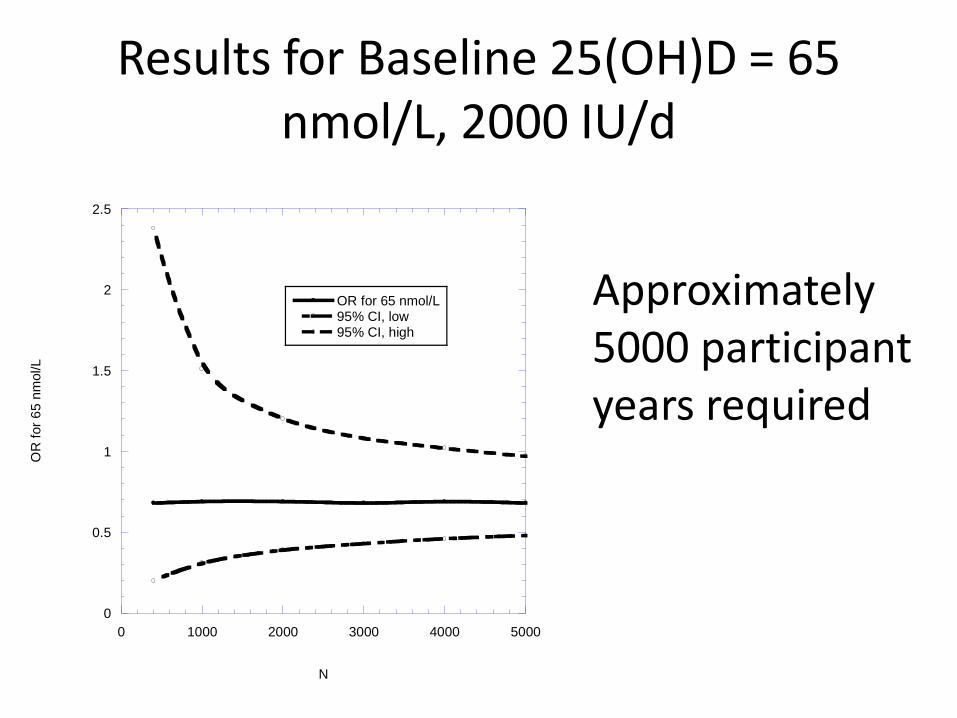
Results for Baseline 25(OH)D = 65 nmol/L, 2000 IU/d
Approximately 5000 participant years required
0
0.5
1
1.5
2
2.5
0 1000 2000 3000 4000 5000
OR for 65 nmol/L95% CI, low95% CI, high
OR
for
65 n
mol/L
N

Use 25(OH)D Results During Trial to Titrate the Vitamin D Dose
• Since there are large individual variations in 25(OH)D with respect to vitamin D dose, it is important to adjust the vitamin D dose after 3-6 months of the trial using 25(OH)D measurements.
• In addition, doing so overcomes objections that results based on 25(OH)D concentrations are merely from an observational study.

Additional Points to Consider
1. Seek participants with low baseline serum 25(OH)D values.
2. Use vitamin D3, not vitamin D2 and at sufficiently high doses, 1000–6000 IU/d.
3. Consider giving a loading dose of vitamin D3 to reach target 25(OH)D concentrations rapidly.
Additional Points to Consider
4. Measure baseline serum 25(OH)D concentrations and repeat at suitable intervals to assess compliance and the achievement of target 25(OH)D values.
5. If calcium and/or magnesium are given, give them in both arms. (Magnesium helps convert vitamin D to 25(OH)D.)

Additional Points to Consider
6. Monitor participants’ UVB exposure , as well as dietary and supplemental intakes of vitamin D3 and potential confounders, including obesity and genetic variants.
7. Allow for the natural history of disease development in planning RCT duration and dosing, and for subject age.
8. Analyze results in terms of 25(OH)D values at baseline, at completion, and at intervals before disease diagnosis.

Additional Points to Consider
9. Carefully consider vitamin D dosing interval with respect to compliance and physiological effect. Daily or weekly are likely best.
10. If, for ethical reasons, participants in the control are given 400 IU/d vitamin D, the resulting increase in 25(OH)D concentration should be factored into the selection of participants and into outcome analyses.

Ongoing Major Vitamin D Trials
• VITamin D and OmegA-3 TriaL (VITAL) (U.S.)
• D-Health Trial (Australia)
• Vitamin D Assessment (ViDA) Study (N.Z.)
• Vitamin D and Type 2 Diabetes (D2d) study (U.S.)
• Finnish Vitamin D Trial (FIND)
• These trials will complete data acquisition, analyze data and publish results in 2018-20.

Ongoing Large-scale Vitamin D3 Clinical Trials
• These trials are still based on vitamin D dose.
• 25(OH)D concentrations were measured for some of the participants, but were not used as criteria for participation.
• They are expected to provide some information on vitamin D in disease prevention.

Further Recommendations
• Important health outcomes that need additional support from vitamin D clinical trials:– Cancer survival
– Cardiovascular disease recurrence
– Pregnancy and birth outcomes
– Non-respiratory tract infection outcomes
– Surgery outcomes with raised 25(OH)D prior to surgery and maintained elevated

Summary and Conclusion
• Observational studies in the past decade indicate that vitamin D has many important health effects.
• Vitamin D clinical trials have confirmed some of these effects, but were often poorly designed.
• Basing vitamin D clinical trials on 25(OH)D concentrations should lead to confirmation of vitamin D’s benefits in disease prevention and treatment.