how to live longer and feel better - even with cancer
TRANSCRIPT

IntroductionIn 1968 Linus Pauling introduced the
word ‘Orthomolecular’ in his Sciencearticle,”Orthomolecular Psychiatry.” 1
With this report, now a classic, he an-nounced to the world his entry into a newfield of medicine, much to the discomfortof the medical profession and equally tothe delight of the public at large. He hadbeen familiar with the old vitamins-as-pre-vention paradigm, but within a brief pe-riod of time he had jumped into the vita-mins-as-treatment paradigm, the modernparadigm which is sweeping into medicineso rapidly today. Adherents to the old para-digm accepted as articles of truth: (1) thatvitamins were needed only to prevent vi-tamin deficiency diseases; (2) that onlysmall quantities were required since theywere catalysts; and (3) that they were con-traindicated for every other condition notaccepted as a vitamin deficiency disease.
Within the past five years the medi-cal profession has begun to distance itselffrom this paradigm. The modern paradigmis based on a different set of beliefs: (1)that vitamins are useful in a large numberof conditions or diseases, not only to pre-vent vitamin deficiency diseases such asberi beri, pellagra or scurvy; (2) that theyare needed in optimum, or orthomolecu-lar amounts, which may be small or large.
The early roots of the vitamins-as-treatment paradigm began about 1940when pellagrologists discovered thatchronic pellagrins required much largerdoses of vitamin B3 to remain free ofpellagra. But these and other studies, in-cluding the double blind prospective stud-ies2,3,4,5,6,7 we did on schizophrenic patientsbeginning in 1952, remained totallyobscure and were ignored. The discovery
How to Live Longer and Feel Better -
Even With Cancer
A. Hoffer, Ph.D., M.D., F.R.C.P.(C)
that niacin lowered serum cholesterol lev-els8 was the first major attack on the old para-digm, but only after our findings were con-firmed by Parsons9,10 and his colleagues at theMayo Clinic. We used doses up to threegrams daily, about 300 times the recom-mended daily requirement, to lower choles-terol, which was not considered to be avitamin deficiency disease.
Linus Pauling’s book11, Vitamin C andThe Common Cold, was the first report thatengaged the attention of the whole worldto the use of vitamins, in this case vitaminC, to the prevention and treatment of adisease not considered a vitamin deficiencydisease. This was the first major frontalassault on the old paradigm and it elicitedthe expected reaction from its defenders.
There was an enormous outpouringof rage from the medical establishment,as well as from dietitians and other adher-ents to the old paradigm. This rage coloredmost of the early attacks on Pauling. Thus,one author reported in an Australian jour-nal that after Pauling had publicized theuse of vitamin C there had been an enor-mous increase in the use of vitamin C,accompanied by a significant increase inthe prevalence of kidney stones. The samejournal rejected a critique I had writtenwhere I pointed out that using the author’sown statistics, it was clear that the increasein kidney stones was well developed longbefore Dr. Pauling made his original an-nouncement and long before his book couldhave appeared in Australia, and that afterthe information became available there wasno further significant change. They ofcourse refused to publish my rebuttal.
By 1968 fewer than 12 physicians andpsychiatrists were using orthomoleculardoses of vitamins. The first 500 mg tab-lets were made by a small company in Port-
1. 3A Quadra Street, Victoria, B.C. V8T 4E5
147
148
Journal of Orthomolecular Medicine Vol. 11, No. 3, 1996
land, Oregon, in 1960 as a favor to a Cali-fornia physician. He wanted to treat histwelve year old son who had been diag-nosed as having untreatable schizophrenia.He had been advised to commit and for-get him in a mental hospital. His son re-covered in a few months and has been wellsince. He is a research psychiatrist. Dr.Humphry Osmond and I had organized theAmerican Schizophrenia Association, laterthe Huxley Institute of Biosocial Research.By this time we were improving our pa-tients’ nutrition as well as adding supple-ments of vitamins and minerals. We con-cluded that the term orthomolecular wasjust what we needed to create a division ofmedicine and psychiatry which would ac-curately draw attention to the kind of prac-tices we were following. Dr. Pauling’s con-tribution was the largest single influencewhich kept orthomolecular medicine aliveand growing. The medical conferences heldover the past five years dealing with cancerand the use of nutrients would have beenimpossible without his brilliant and dedi-cated support to the development of thenew paradigm.
Dr. Linus Pauling and CancerIn 1979 Drs. Ewan Cameron and
Linus Pauling published their book Can-cer and Vitamin C,12 updated in 1993.13
This was the culmination of a number ofreports published in the medical literatureby both Cameron and Pauling. Theyfound that as of August 10, 1976, all ofthe 1,000 control patients were dead, com-pared with 18 of the 100 treated withascorbate who were still alive. The meantime of survival for the treated group was4.2 times as great as it was for the control.They lived more than 300 days longer. Dr.J. Hoffer14 noted, in his recent analysis ofthis research, “the favorable effect of vita-min C in the Vale of Leven cancer patients,while not excellent, was far from negligi-ble. Indeed it was comparable to the ef-fect reported for IL-2 in later NCI-fundedPhase II trials that attracted wide interest
in the scientific medical community. Mostimportant from the biologic perspectivewere the cases in which vitamin C inducedcatastrophic tumor hemorrhage and necro-sis. Although IL-2 occasionally producesrapid remissions, it has never had an ef-fect as dramatic as this.” The Cameron-Pauling studies were in effect an attack onthe common cancer treatment paradigmand, therefore, were totally unacceptable.
In 1977 a woman with obstructivejaundice was found at laparotomy to havean inoperable cancer of the head of thepancreas. She was given a bypass and ad-vised she had only a few months to live.She had started to take ascorbic acid 10 gdaily. When she told her physician, he ad-vised her to see me. I increased her dose to40 g and added other nutrients, since bythat time I had been using multiple nutri-ents for psychiatric patients who were re-ferred to me. Six months later her tumorwas gone. She is still alive and well today.
One case does not constitute proofbut, like the white crow, it suggests thatthere is something there worth lookinginto. It shows that the rule that no cancersyield to nutrient therapy is wrong, in thesame way that the rule all crows are blackis no longer tenable.
I then recalled two earlier patients, aretired professor15 who developed inoper-able bronchiogenic cancer of the lung, forwhich he was given cobalt bomb radiation.He became psychotic. After two monthswith no improvement I started him onniacin, 3 g daily and ascorbic acid, 3 gdaily. This was my standard treatment forthis type of psychosis. He was mentallynormal in four days. I continued him onthe two vitamins until he died 30 monthslater. One year after he started, his lungswere clear. The cancer clinic saw a gradualrecession of the lesion every three months.His lungs were clear after one year.
About a year later I placed a 16 yearold girl with Ewing’s sarcoma of the rightarm on niacinamide 3 g daily and ascor-bic acid, 3 g daily. She was booked for sur-

149
How to Live Longer and Feel Better–Even with Cancer
gery to amputate her arm, but her surgeonwas persuaded to wait for a month. Shemade a complete recovery and is still well33 years later.
I concluded that the main therapeu-tic factor was the vitamin B3 (niacin or ni-acinamide), as it is for schizophrenia.16 Itdoes have anti-tumor properties.17,18 How-ever, after studying Cameron and PaulingI was convinced that the main therapeuticnutrient was vitamin C, and that vitaminB3 had lesser anti-tumor properties. Thiscase was significant, for it widened mypractice of psychiatry by adding to it pa-tients with cancer with significant depres-sion and/or anxiety. The pancreatic can-cer patient who had been cured publicizedthis fact widely to her friends, relatives andcustomers. Ironically, the only one who didnot believe her was her younger brother, apsychiatrist, who knew vitamins could nothelp anyone. Gradually, physicians referredmore patients to me until by 1988 I hadseen 134.
In 1985, after I had seen 41 patients,I realized that the patients given at least12 grams of ascorbic acid daily had a bet-ter outlook. For patients seen between1978 and 1983, out of 11 who did notfollow the regimen none were alive andthe mean survival was 4.8 months, whileout of 26 who took the full dose of vita-min C, 18 were alive, for a mean survivalof 16.2 months.19
A few years later at a Festschrift for Dr.Arthur Sackler, I discussed this data withLinus Pauling. He asked me if I intended topublish and I replied that I did not. I didnot think I could persuade any medical jour-nal to accept my paper. However he urgedme to follow up each patient carefully and Iagreed that I would.
Two years later he asked me how I wasgetting along. I was embarrassed to admit Ihad not done what I had said I would dobut, I added, I would do so immediately. Icontacted every patient I had seen from 1978to 1988, or their relatives or their physicians,or the cancer clinic. I sent this data to Dr.
Pauling who analyzed it.20,21
In the first study22 134 patients seenbetween August 1977 and March 1988were followed until December 31, 1989.We concluded that orthomolecular treat-ment given to female related cancers hadimproved life expectancy about 20 timescompared to our non random controls and12 times for other cancers.
In our second paper23 a second cohortof 170 patients seen between April 1988to December 31, 1989 was followed toDecember 31, 1992. These results wereabout the same as those we had earlierpublished. We concluded that while vita-min C alone led to about 10% excellentresponders the addition of the other nu-trients increased this to about 40%.
I examined the first cohort of 134 fur-ther.24 In the first year after treatment, 75%of the control group of 33 died, comparedto 25% from the treated group of 101. Janu-ary 1, 1992, 41 patients were still alive fromthe treated group and one from the control.The average survival was 49 months for thetreated group compared to 15 months forthe control. The survival data suggested thatthe original Hoffer and Pauling estimates ofsurvival were not far off the mark. As ofDecember 31, 1993, 34 were still alive fromthe treated group and none from the con-trols.
In order to obtain a comparison groupwe used the 33 patients from the originalseries of 134 who had not followed theprogram for at last two months. They rep-resent the results of standard therapy whichthey had had or were still receiving. I havedivided the group previously used as a con-trol, into two control groups; (1) the groupwho did not live for two months after theyfirst saw me - there were 14 and they livedon average 51 days; (2) the group who livedlonger than 2 months and did not starton the vitamin program, of whom therewere 19. They were alive on average 458days or 15 months.
The first group represents a terminalgroup who had failed to respond to stan-
150
Journal of Orthomolecular Medicine Vol. 11, No. 3, 1996
dard treatment, or who had suffered a re-lapse after an initial response to previoustreatment, and who may have been com-promised by the treatment they had al-ready received. It would have been desir-able for patients who had decided for per-sonal reasons never to accept anyxenobiotic therapy to become a controlgroup, but this was simply not possible inthis study, nor would I recommend thisto my patients for ethical reasons. As well,it is quite likely that some of the 101 pa-tients in the treated group would also havedied within that two month interval hadthey not been started on orthomoleculartherapy, but this cannot be determined forthese patients. Perhaps an equal numberlived longer than two months as did thosewho did not make it for the two monthsafter they first saw me. Taking all thesefactors into account, I think it is fair andreasonable to use the second controlgroup as another valid comparison group,a concurrent group. This should also sat-isfy critics who maintain that every pa-tient entered into the study must be re-tained in it, even if they did not followthe treatment protocol.
Using this comparison group therewere 101 patients who were able to follow
the program, although some of them didnot live very long after I first saw them.None were excluded from this group. Theresults of the treatment on the 101 can becompared with the results of the xenobiotictreatment on the 19. I now have seen over750 patients in my series. With this en-larged sample it will be possible to exam-ine these issues more thoroughly.25
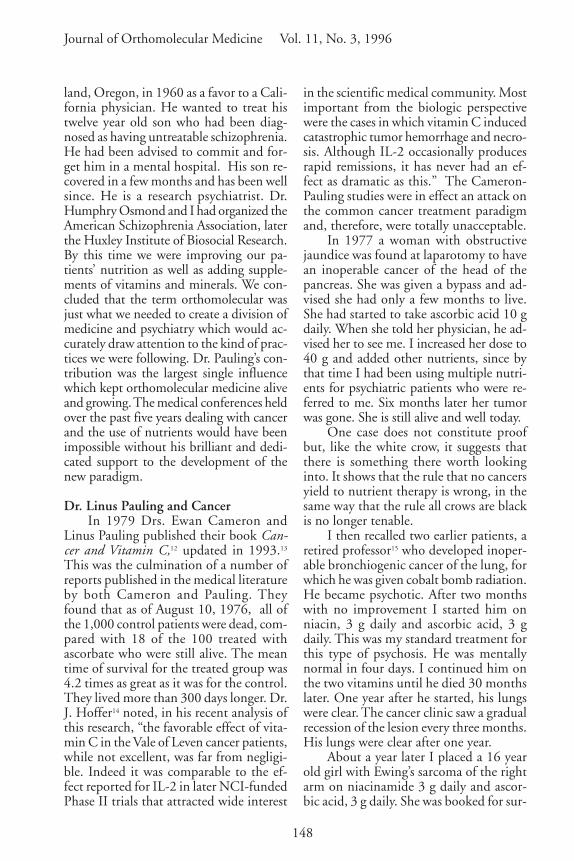
I found that the difference betweenthe vitamin treated patients and those whowere not on the program was sustained.Survival of the two groups, the treatedgroup of 101 and the pseudocontrol groupof 19 treated only with xenobiotic therapy,is shown in Figure 1.
The difference in outcome betweenthese two groups remained large. In thefirst year, 75% of the group not on theorthomolecular program died, and at theend of five years 5% were alive. From theorthomolecular group 25% died by theend of the first year, and at the end of the5th year 39% were alive. By January 1,1992, 41 patients were still alive. The av-erage duration of life from the time I firstsaw them until this date was 49 months,compared to 15 months for the grouptreated with xenobiotic therapy only.
Pauling, as reported by J. Challem,
Figure 1. Effect of Orthomolecular Treatment on Survival of Cancer Patients
0 1 2 3 4 5Years
120
100
80
60
40
20
0
On Vitamins
Not on Vitamins
Perc
ent
surv
ivor
s
151
How to Live Longer and Feel Better–Even with Cancer
stated, “Based on the results so far, I pre-dict that they will live five to seven years.So many are still alive that it’s hard topredict how long they’ll live.”26 The meansurvival time estimate for both groups isabout 80 months. The survival of thexenobiotic group resembled much moreclosely our original group of 33. There-fore, even with this control group whichcontains all the patients who followed theprogram for as little as a few days, theoutcome of treatment was still support-ive of our conclusion that orthomolecu-lar treatment combined with xenobiotictreatment is much superior to xenobiotictherapy alone. As a clinician working withpatients for 42 years, I still think the origi-nal control group is the sounder one touse scientifically.
Twenty patients out of 59 (34%) sur-vived eight years. They were first seen be-tween 1978 and 1984. From the remain-ing 75, seen between 1985 and 1988, 22(29%) survived four years. This suggeststhat over the next four years this groupwill also yield a 25%, eight year survival.The first group included the followingtypes of cancers: pancreas (1), lung (2),sarcoma (2), lymphoma (3), throat (2),uterus (2), ovary (1), breast (5), cervix (1)
and colon (1).Another way to compare the effect of
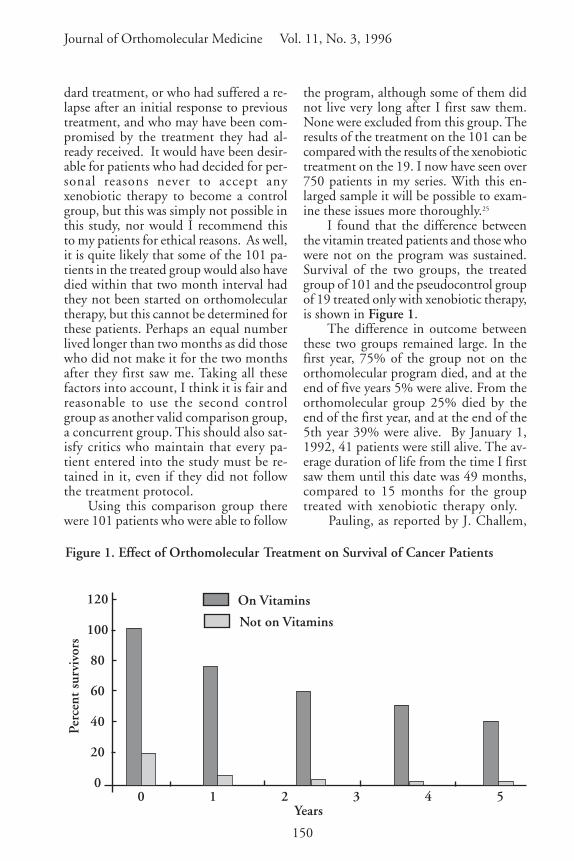
orthomolecular against the standardtherapy is to eliminate every patient I haveseen who did not survive two months af-ter I first saw them. Following this methodI have examined the survival by years of562 patients all seen from 1978 to Febru-ary 24, 1994. From this group there were457 on orthomolecular treatment and 52who were not (Figure 2). The latter is thecontrol group and represents the results ofstandard treatment they had been gettingfrom the time they first were diagnosed.This data is to be used only to comparethese two treatments. It cannot be used topredict the outcome of treatment sincemany of the patients were seen too recently.But it does show that arbitrarily removingpatients from the treated group who havenot been on the program at least two yearswill not distort the data showing what thefinal outcome will be.
In my last report27 I examined furtherthe first cohort of 134 patients as of De-cember 1993. Thirty-four were still alivefrom the treated group, all having survivedat least five years.
None survived from the control group.Seventeen survived more than ten years. As
Figure 2. Comparison of Adjunctive (Orthomolecular and Standard) AgainstStandard Treatment
•
100
90
80
70
60
50
40
30
20
10
01 2 3 4 5 6
•
•
•
• •••••
•
Years
Perc
ent
surv
ivor
s
•
•
Treated N=457
Control N=52

152
Journal of Orthomolecular Medicine Vol. 11, No. 3, 1996
of July 1994 another 17 patients are alive.Four will reach ten years in four years, sevenin three years, four in two years and two intwo years. I expect that there will be 34who will have reached a ten year survival.Half of the six deaths in 1992 died of otherphysical disease, not directly from their can-cer. One died in 1993.
Examination of Hardin Jones Estimateof Survival as Estimated by Linus Pauling
In our first study 134 patients, seenbetween August 1977 and March 1988,were followed until December 31, 1989.We concluded that orthomolecular treat-ment given to female-related cancers hadimproved life expectancy about 20 timescompared to our non random controls and12 times for other cancers. I have exam-ined the survival of this group as of theend of 1995. I have examined the outcomeof the 32 good responders. These were thepatients who had lived more than one year.Over the 11 year follow up the mean sur-vival was 6.56 years or 79 months. Eightpatients are alive and can reach the 11 yearfollow up. Their mean age is 56. Assum-ing all will reach 11 year survival they willadd 15 more years and the average for the32 will be 7.06 or 85 months. Theoreti-cally these 8 patients, if they live the nor-mal life span for women of 85 years, canadd 240 more years to be averaged. Thiswould bring the total survival to 14.6 yearsor 175 months.
From the whole series of treated pa-tients 33 are alive today. Their mean age is58. This series includes both the good andpoor responders although most will be inthe good responder group. If they live an-other 20 years (less than the 25 years theymight be expected to live) this will increasethe total survival of the group of 101 to 11years. This is about 22 times the controlgroup of patients on standard treatmentonly. The actual survival and the projectedfuture survival appear to be very close tothat predicted by the use of the Hardin-Jones method as developed by Linus Pauling
and illustrated in our first joint paper.
Coenzyme Q10 (CoQ10 or Ubiquinone)28
In 1992 I began to give some of mypatients coenzyme Q10. Q10 is presentin the highest concentration in heart mus-cle. Generally it is present in the greatestconcentration where it is needed the most.It is a major respiratory enzyme which, incombination with nicotinamide adeninedinucleotide, forms factor one in the res-piratory chain, and is itself a major anti-oxidant as are vitamins E, C andselenium. Vitamin E and selenium helpto regenerate Q10. It is disturbing thatsome of the statin drugs used to lowercholesterol levels inhibit the formation ofcoenzyme Q10 in the body.
Coenzyme Q10 is not classed as a vi-tamin due to inconsistencies in vitamin ter-minology. Dr. Karl Folkers regretted this.A vitamin is defined as a natural substancewhich is required in tiny amounts and can-not be made in the body. Using this rulevitamin C is not a vitamin since it is re-quired in large doses, and vitamin B3 is nota vitamin since some can be made in thebody from tryptophan. However, these areby tradition classical vitamins. Q10 can bemade in ample quantities in healthy youngpeople, but when anyone is sick or old itbecomes more difficult to make enough.Thus, for the chronic diseases such as can-cer, senility, and arthritis, it is really a vita-min and ought to be called vitamin Q10.It is possible the high correlation betweenaging and chronic disease may be due tothe increasing difficulty in making and get-ting enough Q10.
In experimental animals it has beenfound to decrease the toxicity of chemo-therapy, especially adriamycin and to mark-edly suppress the growth of induced can-cers. Folkers and his colleagues reportedeight new cases of cancer plus two earlierones where Q10 allowed the survival of fiveto 15 years with no side effects.29
In a second report (not yet published),by Lockwood K, Moesgaard S & Folkers, K
153
How to Live Longer and Feel Better–Even with Cancer
entitled, Partial and Complete Remission ofBreast Cancer in Patients in Relation toDosage of Coenzyme Q10 in NutritionalTherapy, the authors reported an open trialof 18 months on 32 women with breastcancer of ‘high risk’. They were treatedwith 1.2 g of gamma-linolenic acid, 3.5 gof omega 3 essential fatty acids and 90mg of Q10 daily. No patient died and allexpressed a feeling of well being. Theywould have expected three to have died.In six there was a complete remission, lessmorphine was needed and distantmetastases were not seen. In one patientthey increased the Q10 to 300 mg dailyafter she had been on it for one year at 90mg daily. Her tumor had stabilized at 1.5to 2.0 cm. After three weeks on the higherdose it was gone. K.L. stated that inpracticing oncology for 20 years and hav-ing treated countless cases of breast can-cer he had never seen a spontaneous re-mission of this size and had never seen acomparable regression of any conventionalanti-tumor therapy.
Based upon these observations I con-cluded that Coenzyme Q10 should be anintegral component of all cancer therapyat the higher dose levels. If the cancer isentirely gone a lower maintenance doseprobably would be adequate, perhaps 100to 150 mg daily. It should be taken withthe other vitamins and minerals.
Between November 1, 1993 and April
30, 1994 I started 43 patients on 300 mgof Q10 in addition to their usual nutrientprogram. During that same interval onepatient died. For comparison I examinedthe same statistics for patients seen be-tween November 1, 1992 and April 30,1993. None of this group were receivingQ10. They were on the same program aswere the group given Q10 one year later.Every patient seen during these intervals wasincluded. From the earlier group of 32, 6died within the same interval. Chi Sq forthis distribution is 5.85, i.e. P < .02.
This is not a comparison of patientsall seen after six months of treatment. Themean follow up was only three months,but both groups are treated equally. How-ever it is rare in biological (especially hu-man) studies, to achieve such a respectableprobability of around two percent. It sug-gests that Coenzyme Q10 has in realityadded something to the curative propertiesof the previous vitamin mineral regimen.
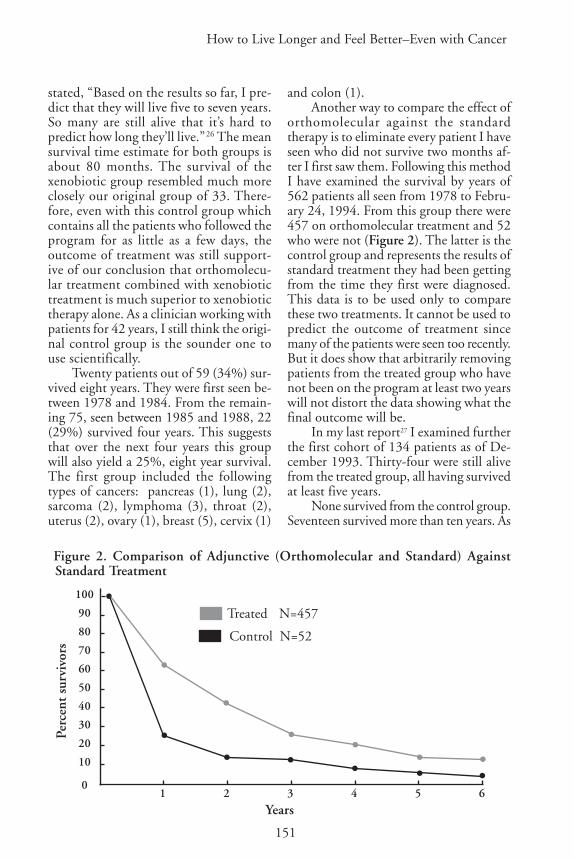
The one and two year survival for thesmaller group of patients placed on Q10is shown in Table 1.
Quality of LifeAfter working with over 750 patients
with cancer since 1978, I have no doubtthat the orthomolecular program has im-proved the quality of their life. It has giventhem more energy, has eased depressionand anxiety, has created a sense of well
Table 1. Survival of Patients With Coenzyme Q10 Added to Their OrthomolecularRegimen.
Q10 added 13 1992 13 (100%) 8(62%)Not on Q10 55 1992 36 (65%) 29(53%)
Q10 added 37 92–93 32(86%) Not availableNot on Q10 101 92–93 67(66%)
Treatment Number Year Alive AliveOne Year Two Years

154
Journal of Orthomolecular Medicine Vol. 11, No. 3, 1996
being, has eased pain and often has elimi-nated it entirely. So far not a single familyhas complained to me about the treatmentand many have told me how grateful theywere, for the program had made life somuch more tolerable for them. A recentremarkable response will illustrate the ef-fect of this program.
J.A. born in 1922 was seen January 6,1994. She had a mastectomy in March1990, right side. In March 1992 she devel-oped low back pain which did not respondto chiropractic treatment or physio-therapy. In August 1992 she discovered anode in her neck. A bone scan showed twoareas in the spine. She was given tamoxifenwhich made the pain intolerable and shewould not take any more after five daysagainst the wishes of her oncologist. Afterthat she started on herbs and massage andwas well in three months. September 1993the pain recurred. Now she had metastasesin her sternum and lower back. Pain in herchest was severe. She started on tamoxifenagain and the pain again became intolerable.Two weeks later she started on ascorbic acid15 g daily and on shark cartilage, but couldonly tolerate eight capsules of the cartilage.After starting vitamin C she slowly began toimprove. She was able to leave her bed, butshe still needed morphine every 12 hours.
I advised her to follow the orthomo-lecular program which included 15 g ofascorbic acid plus Coenzyme Q10, 300mg. On February 1, 1994 she was free ofpain and had discontinued the morphine.This she appreciated since the severe nau-sea generated by the morphine was gone.By February 23, 1994 the lumps had de-creased to half their original size and shewas able to move freely without pain. Bothshe and her husband were delighted.
Quality of life involves physical andemotional health. Physically a large numberof symptoms will seriously interfere withthe enjoyment of life. These include pain;restriction of movement; inability to func-tion, for example to swallow; nausea andvomiting; loss of weight, appetite and the
ability to meet energy requirements. I con-sider a person has a good quality of life whenthese factors are not present or are presentto such a limited degree that they do notinterfere with one’s lifestyle. Emotionalhealth is equally if not more important.
The main changes in cancer patientsare shock, depression, anxiety and the ef-fect this mood has upon thinking andbehavior. It is generated by the diagnosis,by the way it is given to them and by theknowledge that it is a major killing dis-ease. One of the main problems is the fearshared by too many oncologists, surgeonsand radiotherapists of the peculiar combi-nation of words “false hope.” This is a ba-sic contradiction of terms. There are vari-ous degrees of hope ranging from none toexcessive. The term derives from the fearof the physicians that they will give a prog-nosis which is too optimistic and cannotbe confirmed by follow up. They have goneto the other extreme and have been proneto give the patients zero hope.
Dr. William Osler, the famous Cana-dian-American physician, wrote about theimportance of hope, and to illustrate it hetold the following story about himself. Hewas asked to examine a man who had al-ready been examined by two physicianswho had advised the family that he woulddie that day. The family wanted anotheropinion. After his examination, Dr. Oslertold the family that in his opinion the manwould not die that day. But he did die thatevening. The next morning the family ap-proached Dr. Osler and thanked him pro-fusely. He was, they said, the only physi-cian who had given them some hope.
If there is anything at all to the pla-cebo response, to the value of hope in thetreatment of disease, then physicians mustnot remove this important variable. Evenwhen it looks very grim indeed, the pa-tient and family must be allowed some ofthe comforts of hope, but it must be real-istic. It is essential not to exaggerate thehope. The patient should be advised thatno matter how grim the situation is, there

155
How to Live Longer and Feel Better–Even with Cancer
is some hope, and that the physician willhelp in any way possible. The best way toenhance hope is to be able to honestly re-port about other patients equally ill whohave had their lives prolonged and thequality of life improved.
Levine30 describes the effect of hopeon two cancer patients. A 55 year oldwoman was found to have an inoperablesquamous cell carcinoma invading themediastinal nodes. It was biopsied. Thenext morning the resident told her “Well,it’s cancer, and we couldn’t really resectit, so we just opened and closed.” She re-peated, “opened and closed” several times.She died that night. At autopsy there wasno specific cause of death. The residenthad removed all hope.
The second patient had an aggres-sive T-cell immunoblastic sarcoma. Herefused chemotherapy after being in-formed it likely would not help much.Dr. Levine, however, told him that therewas a chance, albeit a slim one. He wentinto remission and was well for one year.Unfortunately the cancer clinics too of-ten leave their patients bereft of hope.Recently I saw on follow up a man withlymphoma who is well after 3.5 years.He told me that when he was diagnosedthe cancer clinic had told him there wasnothing that could be done and that hehad a very few months left. He and hiswife left the clinic beaten and depressed.When he saw me recently he still wasangry and resentful over the way theyhad treated him. I believe that after apatient leaves a doctors’ office he shouldfeel better than when he entered. In mostcases they leave their oncologists’ officesfeeling much worse. They appear to en-courage what I have called an obecalpreaction (placebo spelled backwards). Ifthey are very depressed or anxious or suf-fer from any combination of these mooddisorders I will treat them with the ap-propriate medication for this.
Recently Sapolsky31 in discussing theMeasures of Life referred to the investi-
gations of two psychologists, Amos N.Tversky of Stanford University and Dan-iel Kahneman of the University of Cali-fornia at Berkely. They investigated whypeople regard scenarios as unequal whenin fact they are formally equivalent. Hepresented two scenarios: “You are a phy-sician and you have a hundred sick peo-ple on your hands. If you perform treat-ment A, 20 people will die. If you opt fortreatment B everyone has a 20% chanceof dying.” and “You have a hundred sickpeople. If you perform treatment A, 80people will live. If you opt for treatmentB, everyone has an 80 % chance of liv-ing.” I was not surprised to learn thatmost people in the first scenario preferredtreatment B and in the second one theypreferred treatment A. Sapolsky wrote“The two scenarios are formally identi-cal; they are merely framed differently.But it turns out that for the first scenario,which states things in terms of death,people will prefer option B, whereas forthe second scenario, stated in terms ofsurvivorship, people prefer option A.When thinking about life, people prefercertainty; when thinking about death,they prefer odds, because it is alwaysconceivable the odds can be beaten.” Mypatients and I assume the vast majorityof cancer patients prefer to bet on theodds they will survive and not on thecertainty of death. The oncologists, sur-geons, radiologists and physicians whotreat these patients must take these ob-servations to heart. These therapists canrealistically convey to their patients thatadding the orthomolecular componentto the total treatment regimen will in-crease the probability they will survivelonger and with a better quality of life.That is what patients with cancer wantto know. They will be given, not falsehope, but a realistic and accurate pres-entation of the facts. Patients will be ableto follow their regimen more faithfully,and more comfortably.

156
Journal of Orthomolecular Medicine Vol. 11, No. 3, 1996
A Hypothesis Relating The AdrenalinAdrenochrome System to Cancer and toSchizophrenia
The autonomic nervous system con-trols physiological responses to stress. Itschemical mediators on the sympatheticside are the catecholamines, dopamine,noradrenalin and adrenalin, particularlythe last two. Dr. Cannon’s original descrip-tion of the flight or fight mechanism isstill valid. An emergency or a perceivedemergency is a major stimulus to the au-tonomic nervous system which releaseslarge amounts of adrenalin and noradrena-lin. This prepares the body so it can re-spond best to the emergency. In animalsan inadequate response will lead to eitherdeath (the victim), or to no meal (thepredator). A rabbit which respondsoptimally may escape. A coyote which re-sponds optimally may have a meal.Adrenalin alerts the body, increases heartrate and blood pressure, increases the rateof breathing and diverts blood from vis-cera to the muscles where it is most needed.It increases sweating to cool the body. Itdecreases the sensation of pain. This physi-ological response has been developed overbillions of years and is still fully functionaleven though civilized mankind very seldomhas the same need to respond to emergen-cies the same as do animals in the wild.
Adrenochrome and CancerAdrenalin is very toxic because it el-
evates the blood pressure. The body mustremove it as quickly as possible. To do soit has developed two main pathways forconverting it to other substances.32,33,34 Onepathway leads to adrenochrome whichdoes not elevate blood pressure. The otherpathway leads to non indolic derivatives.The second pathway is controlled by sev-eral enzymes called amine oxidases. Thusa highly reactive compound which elevatespressure is replaced by other compoundsthat do not have this property.
But adrenochrome (and the otherchrome indoles from noradrenalin and
from dopamine) have other properties.Adrenochrome is a mitotic poison, i.e. itdecreases the rate of cell division. In heartmuscle and in leukocytes about 80% ofthe adrenalin is converted into adreno-chrome. And adrenochrome is toxic inother ways. It is an hallucinogen. This isfully described in our book “The Halluci-nogens35(1967). There we discussed itsbiochemical, physiological, and psycho-logical properties. It is a highly reactivecompound with a short half-life in thebody where it is quickly converted intoadrenolutin, 3,5,6 tri hydroxy N-methylindole, which is also hallucinogenic andto 5,6 dihydroxy N-methyl indole whichis not. On the contrary this compound, alsocalled leuko adrenochrome (white adreno-chrome), has good anti-anxiety properties.These substances circulate in the body. Thehallucinogenic properties of adrenochromeand adrenolutin led to our adrenochromehypothesis of schizophrenia36–45 i.e. that thisdisease came about due to the increased for-mation of these oxidation products ofadrenalin. For the rest of this discussion Iwill consider its anti mitotic properties andits hallucinogenic properties.
In our 1967 discussion35 we wrote“Adrenochrome markedly inhibits mitoticrate of cells, probably by interfering in theglycolytic cycles. Bullough found thatwhen mice were stressed by overcrowding,the adrenal medulla increased in size 80%.At the same time the epidermal mitoticrate fell 60%. In vitro adrenaline had noanti mitotic effect on epidermis but whenit was injected it did. In contrast adreno-chrome was anti mitotic both in vitro andin vivo. Bullough suggested that duringstress the increased quantity of adrenalinewas converted into adrenochrome whichproduced the antimitosis.”
These two properties, antimitosis andhallucinogenic, suggest that adrenochromeis involved in two conditions (a) the con-trol of mitosis in the body; (b) schizo-phrenia. Elsewhere I46 have suggested thatschizophrenia is a defense mechanism

157
How to Live Longer and Feel Better–Even with Cancer
against stress which has gone too far. It ishighly likely that since adrenochrome ispresent in the body that it would be usedto control excess mitosis and that it is in-volved in the prevention of cancer. This isthe hypothesis I will elaborate, i.e that toolittle adrenochrome will increase incidenceof cancer and decrease the incidence ofschizophrenia, while too much will de-crease the incidence of cancer and increasethe incidence of schizophrenia.
Small amounts of adrenalin are pro-duced all the time, even during sleep, butduring the day and when exposed to stressthe amount is increased. The continual,even if fluctuating level of adrenalin willensure a constant production of adreno-chrome and its conversion to adrenolutinand other indoles. I suggest that this is oneof the mechanisms the body uses to dealwith excess mitotis. The leukocytes prob-ably destroy abnormal cells by releasingadrenochrome which has the properties ofa free radical and will destroy the cell. It isrecognized that pro oxidants are neededto destroy cancer cells. Adrenochrome isprobably the best and safest natural prooxidant in the body. This hypothesis sug-gests a number of testable sub hypotheses.
A) A deficiency in the production ofadrenochrome will increase the incidenceof cancer and decrease the incidence ofschizophrenia. This can arise from (1) in-adequate production of adrenalin (2) a defi-ciency of enzymes which convert adrenalinto adrenochrome (3) a deficiency of oxy-gen and (4) a deficiency of auto oxidizingsystems such as copper or iron.
A deficiency of adrenalin can arisefrom a deficiency of tyrosine but this ishighly unlikely. It can also arise from ex-tirpation of the adrenal glands, one of themajor sources of adrenalin. It could arisefrom a lack of stimulation of the sympa-thetic nervous system. Factors such as stay-ing in bed all day would decrease the needfor adrenalin to help control blood pres-sure. An absence of challenges to the bodyboth psychological and physical could also
produce a deficiency of adrenalin. It couldalso come about by the use of anti anxietydrugs and tranquilizers which effectivelyisolate the individual from stress. Infec-tions are stressful and increase the activityof the immune system. The use oftranquilizers since 1950 has effectively re-moved this spur to the immune system formany people and may be another factorin decreasing adrenalin and thereforeadrenochrome production. Helen ColeyNauts47 made the very sensible suggestionthat the loss of repeated episodes of infec-tion by bacteria since the introduction ofantibiotics may be a major factor in therising prevalence of cancer in the highlyindustrialized world. According to thishypothesis repeated infections acted as aspur to continually re-invigorate the im-mune system. According to the adreno-chrome hypothesis it would act as a spur toincrease the production of adrenochrome.
B) Excessive formation of adreno-chrome will decrease the prevalence of can-cer and will increase the prevalence ofschizophrenia. This can arise from the fol-lowing factors (1) An overproduction ofadrenalin for prolonged periods of timedue to excessive stress of various types, (2)an increase in the production of adreno-chrome due to an increase in the condi-tions which favor this reaction such asmore of the oxidizing enzymes, too littleactivity of the other enzymes which con-vert adrenalin to other non indolic sub-stance, an increase in oxygen tension, anincrease in oxidizing metals such as cop-per or iron and finally too much inhibi-tion of the reaction by any factor whichwould normally take adrenalin down thenon adrenochrome pathway.
If cancer did develop in a schizo-phrenic person it would probably be lessinvasive and easier to treat with a betteroutcome. Patients with cancer would beless likely to become schizophrenic andpatients with schizophrenia would be lesslikely to get cancer.
Both of these propositions are true.

158
Journal of Orthomolecular Medicine Vol. 11, No. 3, 1996
Since 1977 I have examined and treatedover 750 patients with cancer covering al-most the entire spectrum of types of can-cers and organs involved. Only five wereschizophrenic. Three had cancer of thebreast, one had a lymphoma and one can-cer of the thyroid. In every case the re-sponse to treatment was excellent. Theyare all alive, averaging six years. The usualstated life time incidence of schizophre-nia is said to be 1%. I think it is closer to2 %. Therefore I would expect that out ofthis series I would have seen more thanthese five. Kanofsky48 (1994) concludedthat schizophrenic patients have a lowerincidence of lung cancer compared to thegeneral population even though they aremuch heavier smokers. He also found thatsmoking did not lower their ascorbic acidblood levels as much as it does in otherpeople. This he thought lowered their riskon exposure to smoking but according tothis adrenochrome hypothesis it mightequally have arisen from the increasedconcentration of adrenochrome.Kanofsky pointed out on the basis of aliterature search that in general schizo-phrenics have a higher death rate than dothe general public. Some studies haveshown they have a greater rate for nonlung cancer and a lesser or greater ratefor all other cancers. The earlier litera-ture had concluded that cancer was rarein schizophrenics who were catatonic andhebephrenic, terms no longer in generaluse. On the contrary, the death rate fromcancer in paranoid schizophrenics washigher than it was in the general popula-tion. The only clear finding is the decrease
in lung cancer. Perhaps if they were nonsmokers their rate of lung cancer wouldbe even lower.
I have seen over 4,000 schizophrenicpatients since 1952. Currently I have atleast 500 chronic patients under my care.The total incidence of cancer is very low.From my current list only five have can-cer, the same five that I referred to in thecancer series. A few characteristics of thisgroup is shown in Table 2.
If adrenochrome is synthesized ingreater amounts in schizophrenia, duringremission (spontaneous or due to treat-ment) there may not be enough adreno-chrome to prevent the cancer from appear-ing but enough to greatly enhance theirprognosis. They have all recovered fromtheir cancer. The lymphoma patient is stillfree of cancer but he is not well mentally.
From the much larger series I treated Icannot recall any cases of cancer. I wouldexpect a much higher incidence of cancer inthe schizophrenic group unless there was thisincompatibility between the two conditions.
There is other evidence as well. Pro-fessor Rudy Falk,49 University of TorontoMedical School, formerly Chief of Oncol-ogy at St. Michael’s Hospital, Toronto, es-timated that he had seen over 25,000 pa-tients during his long career and Dr. J.Holt,50 an oncologist in Australia had seennearly 18,000 patients over his 41 yearsof practice. They cannot recall a single pa-tient who was also schizophrenic. Dr. Holthad been puzzled by this incompatibilityfor many years. Out of nearly 48,000 casesonly five are known to have had schizo-phrenia. Dr. Holt’s group also had treated
Number Sex Type Schiz first Alive, years
1 F Breast Yes 42 F Thyroid Yes 43 F Breast Yes 64 F Breast Yes 25 M Lymphoma No 12
Table 2. A Few Characteristics of the Group With Both Cancer and Schizophrenia

159
How to Live Longer and Feel Better–Even with Cancer
about 700 patients with AnkylosingSpondylitis and he estimated about six hadbeen schizophrenic with another 12 dis-turbed psychiatrically. Apparently thisphysical condition did not protect againstschizophrenia.
It occurred to me that this protectiveeffect might also be found in the mostclosely related relatives of these patients i.e.parent, siblings and children. These rela-tives do have some evolutionary advantage.51
Over the past year I have asked each cancerand each schizophrenic patient I have seenabout the presence of either condition intheir first order relatives. The results of thisclinical survey are shown in Table 3.
Chi Sq. for the distribution for thelast two columns is 18 i.e. P<.001. For thedistribution of schizophrenic patients onlybetween the two groups it is 11.1 and forcancer cases only it is 22.
About 12% of the cancer relatives de-veloped cancer. From the schizophrenicrelatives only six percent did. From thecancer relatives only two (0.4%) hadschizophrenia. The incidence among thegeneral population is between one and twopercent which from this group should yieldbetween five and ten patients. And fromthe schizophrenic relatives 12 had cancer.This data supports the hypothesis i.e. thatpatients liable to get cancer are much lessapt to get schizophrenia and that patientswho have or have had schizophrenia aremuch less apt to have had cancer. Patientswith a predisposition to cancer do not makeenough adrenochrome to become psy-chotic, while other people who only makeenough adrenochrome now and then will
get schizophrenia and will be protected toa degree from getting cancer. And schizo-phrenic patients who do get cancer will havea much better outlook with treatment.
This inverse association between thesetwo killing diseases, cancer which destroyslife and schizophrenia which destroys nor-mal life, leads to the prediction that if apatient has cancer and then developsschizophrenia the cancer will be destroyedby the adrenochrome.
Perhaps my first cancer case in 1960who was psychotic for at least two monthsrepresents one of these cases. Perhaps his re-covery was due to the combination of hispsychosis which cleared very rapidly on ni-acin and ascorbic acid, the vitamins and thecobalt bomb radiation.
Brown and Foster52 examined thegeographical relationship between theprevalence of schizophrenia and seleniumdeficiency in the soil. Their careful de-tailed examination of nine surveys led tothe conclusion that there is a connectionbetween selenium deficiency and theprevalence of schizophrenia and to thesuggestion that selenium supplementa-tion might be valuable in preventing andtreating schizophrenic patients. There isalso a similar relationship between theprevalence of esophageal cancer and sele-nium deficiency. This appears to suggestthat both schizophrenia and cancer oughtto be positively related and they are not.It is possible that a deficiency of seleniumincreases the probability of developingboth diseases but that it plays a muchgreater role in preventing cancer. Thusboth are increased in the absence of
Table 3. The Presence of Cancer and Schizophrenia in First Order Relatives ofPatients With Cancer or Schizophrenia
Index Patients Relatives With Schizophrenia With CancerCondition N Number Number Number
Schizophrenia 79 382 12 22
Cancer 80 529 2 61
160
Journal of Orthomolecular Medicine Vol. 11, No. 3, 1996
enough selenium but at the same time theassociation between the two diseases isnegative.
Pyrolleuria and CancerKryptopyrrole(KP) is found in the
urine of the majority of schizophrenic pa-tients and in very few normal people. (SeeEva Edelman53 for a comprehensive reviewof kryptopyrrole). It is highly correlatedwith schizophrenia and its presence estab-lished the diagnosis, pyrolleuria. It is alsopresent in some patients with cancer, es-pecially if they have cancer of the lung.Seven out of eight patients with lung can-cer were positive for KP while four out offour tested after treatment were negative.Two of seven ovarian and uterine cancerpatients were positive. From both groups80% had pyrolleuria. But from all othercancers 24 out of 79 or 30% were posi-tive. In my review54 of the psychophysiol-ogy of cancer I summarized the cancer lit-erature which showed that lung and ovar-ian cancers had the highest incidence ofpsychotic change, usually a form of de-mentia. This group also had the highestincidence of KP in their urine.
This puzzled me for many years. Inthinking about these results it occurred to
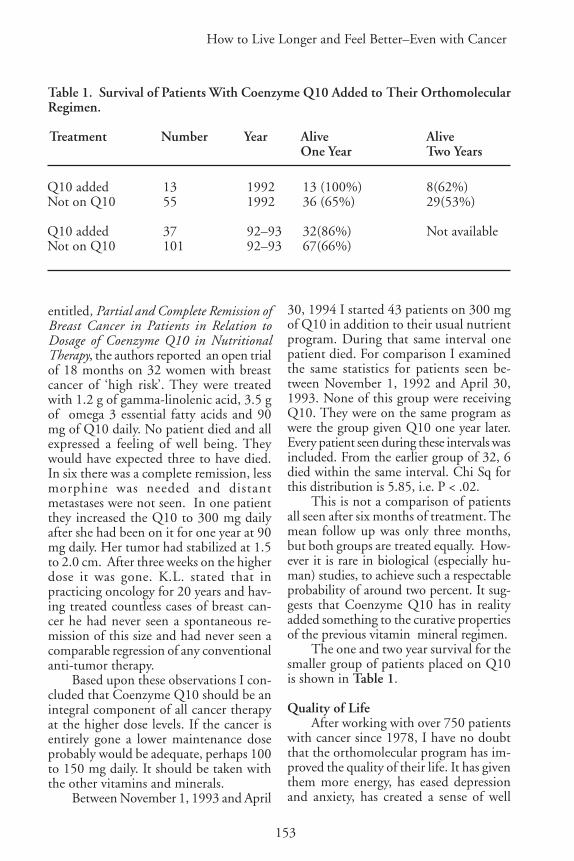
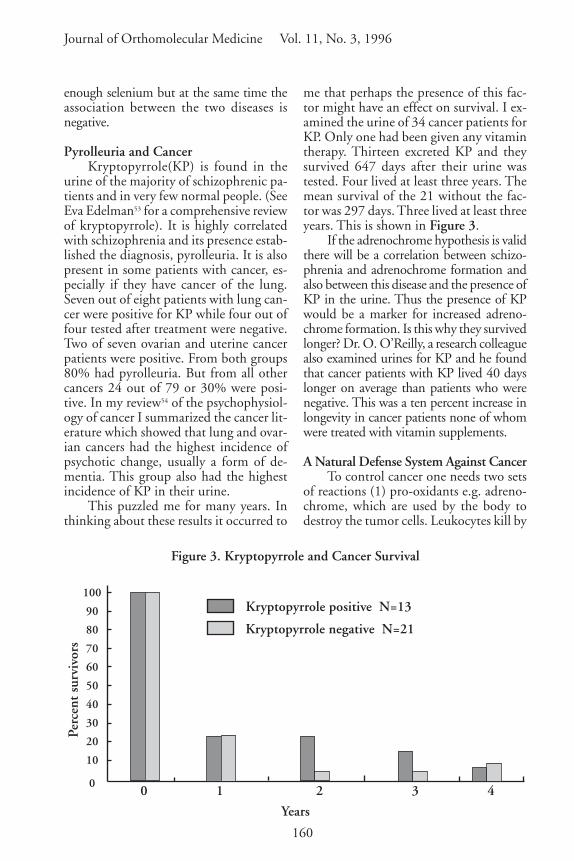
me that perhaps the presence of this fac-tor might have an effect on survival. I ex-amined the urine of 34 cancer patients forKP. Only one had been given any vitamintherapy. Thirteen excreted KP and theysurvived 647 days after their urine wastested. Four lived at least three years. Themean survival of the 21 without the fac-tor was 297 days. Three lived at least threeyears. This is shown in Figure 3.
If the adrenochrome hypothesis is validthere will be a correlation between schizo-phrenia and adrenochrome formation andalso between this disease and the presence ofKP in the urine. Thus the presence of KPwould be a marker for increased adreno-chrome formation. Is this why they survivedlonger? Dr. O. O’Reilly, a research colleaguealso examined urines for KP and he foundthat cancer patients with KP lived 40 dayslonger on average than patients who werenegative. This was a ten percent increase inlongevity in cancer patients none of whomwere treated with vitamin supplements.
A Natural Defense System Against CancerTo control cancer one needs two sets
of reactions (1) pro-oxidants e.g. adreno-chrome, which are used by the body todestroy the tumor cells. Leukocytes kill by
Figure 3. Kryptopyrrole and Cancer Survival
0 1 2 3 4
Years
Perc
ent
surv
ivor
s
Kryptopyrrole positive N=13
Kryptopyrrole negative N=21
100
90
80
70
60
50
40
30
20
10
0

161
How to Live Longer and Feel Better–Even with Cancer
discharging free radicals into the bacteriaor cell they are attacking. Adrenochromeis a natural superb free radical. (2) Anti-oxidants to neutralize the free radicals assoon as their work is done to prevent in-jury to other cells and tissues. Theadrenalin-adrenochrome system providesa very good system for controlling mito-sis. The adrenalin is maintained by re-peated exposure to stress. The adrenalin isconverted to adrenochrome and is used bythe body as needed and the excess is neu-tralized by conversion into other indoleswhich are not as toxic. This is done by thenatural anti-oxidants such as ascorbic acid,vitamin E, the carotenes and other antioxidants found in food.
Treatment For Cancer Based Upon ThisHypothesisIncrease the production of adrenalin.
(a) By psychological means. Anger willincrease the secretion of adrenalin but itshould be mobilized as an attack on thetumor, and not directed inward towardoneself. Many cancer patients have recog-nized this and use visualization against thetumor. Anger directed against oneself tendsto produce depression. The patient musthave a combination of anger against thecancer and hope that it will come undercontrol. Too many oncologists have for-gotten the powerful effect of hope andtherefore by negative hope increase thedeath rate of their patients.
(b) Bacterial infection. About 100 yearsago Dr. Coley,37 a New York surgeon, re-viewed the clinical evidence then availablewhich indicated that in some patients a se-rious infection with staphyloccus or strepto-coccus led to a cure of the cancer. Later hedeveloped a vaccine which he used very suc-cessfully for many years. Infections increasestress on the body which mobilizes the im-mune system and creates fever which in-creases the rate of reactions in the body. Thecombination must increase the productionof adrenalin and therefore also of adreno-chrome. Similar vaccines are in use today by
several physicians with some success.(c) Hyperthermia. This should also
increase the secretion of adrenalin andtherefore of adrenochrome.Increase production of adrenochrome.
(a) An increase in activity of the enzymeswhich oxidize adrenalin to adrenochrome i.e.activating the phenolases which catalyze thisreaction. Decreasing the activity of amineoxidases by using inhibitors should have thiseffect by forcing more adrenalin into theadrenochrome pathway. Parnate should bea very good amine oxidase inhibitor used inlow doses, under 20 mg daily. At this doselevel it will rarely cause side effects, may im-prove mood and should increase the forma-tion of adrenochrome. I have seen psychoticdelirious reactions produced by large dosesof parnate. The effect on adrenochrome pro-duction has not been tested.
(b) Using adrenochrome derivatives.55–57
(c) Increasing the amount of oxygenin the tissue by using oxygen (hyperbaric)or by increasing blood flow through thetumor. Tumor tissue tends to be anoxicwith the most virulent tumors being themost anoxic. Niacinamide has been shownto increase the circulation this way.58
Niacin would have the same property, per-haps to a larger degree.
(d) Increasing auto oxidation ofadrenalin by increasing copper or iron inthe body. Based upon this adrenochromehypothesis, therapy for cancer should in-clude substances which counteract the hal-lucinogenic effect of adrenochrome andcompounds which facilitate its conversionto other less toxic compounds. Vitamin B3
(niacin and nicotinamide) is the best anti-dote to the hallucinogenic properties ofadrenochrome39 and adrenolutin as it isagainst d l lysergic acid diethylamide.59 Theanti-oxidants will promote the conversionof adrenochrome to leuko adrenochromeand to adrenolutin. These include ascor-bic acid, the best water soluble anti-oxi-dant and vitamin E, the best fat solubleanti-oxidant in the body. It will also in-clude the carotenes, coenzyme Q10, glu-

162
Journal of Orthomolecular Medicine Vol. 11, No. 3, 1996
tathione, the bioflavonoids and the anti-oxidant trace element selenium.
Why are vitamin B3 and these anti-oxidants therapeutic for a large variety ofconditions? Both vitamin C and vitaminB3 have an enormous range of therapeuticactivities.60–66 This suggests that except forthe two diseases cancer and schizophrenia,which have a direct relationship to adreno-chrome, these vitamins have a general sys-temic effect which reduces the body’spathological reaction to stress and thus al-lows the natural repair processes of thebody to operate at a more efficient level.Since every disease results from or createsstress on the body because of the impactof increased production of adrenalin andadrenochrome these anti stress vitaminsshould have a general therapeutic effect onevery disease. Every disease, or every stressrelated activity will benefit from the addi-tion of optimum amounts of the B-vita-mins especially B3 and the anti-oxidantnutrients including vitamin C, vitamin E,the carotenes, Coenzyme Q10 and the anti-oxidant trace element selenium. There isalready ample evidence in addition to theevidence presented here that life is extendedand its quality enhanced by this program.Niacin prolongs life,67 vitamin E should doso as it decreases the frequency of coronarydisease,68,69 and vitamin C prolongs the lifeof cancer patients. They each work whenused alone but there is a growing consen-sus that the combination of these anti-oxi-dants has a synergistic effect.70 Prasad,71 us-ing cell cultures, found that using individualvitamins might be effective, ineffective oreven counter productive depending uponthe vitamin, dose and type of tumor. Incontrast the mixture of four vitamins (vita-min C, alpha tocopherol succinate, betacarotene and retinoic acid) consistently re-duced growth of both cell lines studied andenhanced the growth inhibitory effects ofchemotherapeutic agents on these cells.Unprocessed food does not contain onlyone vitamin. It contains them all even if invery small amounts. It is not surprising that
they work better in combination with eachother for that is what nature has been do-ing since life originated.
Orthomolecular Treatment of Parkinson’sDisease
Parkinson’s disease is another exam-ple of a condition which is related to ex-cessive oxidation72–76 (auto-oxidation),yielding too many free radicals. Jenner76
writes “There has been reluctance by sci-entists, grant-giving bodies, and the phar-maceutical industry to accept that free-radical mechanisms are an importantcomponent of neurodegenerative disease.A decade ago the concept was thoughtfacile but at least now some acceptancehas been gained. Nobody is claiming thatfree radicals explain every unique featureof neurodegenerative disease. Rather, weare proposing that they are a commonfeature of the process of cell death inmost, if not all, such illnesses. If so, thetherapeutic rewards may be great. It maybecome possible to stop or slow the pro-gression of common disorders, such asAlzheimer’s or Parkinson’s disease, with asingle therapeutic approach.”
I have evidence that the combinationof niacin (and perhaps niacinamide as well)and anti-oxidants will be therapeutic forParkinson’s disease. Over the past thirtyyears I have treated patients with Parkin-son’s disease with niacin, 500 to1000 mgtid. It has been very effective in removingpsychiatric symptoms but has been of novalue in treating the neurological compo-nent. This disease is considered to be adopamine deficiency disease and is treatedwith large doses of l-dopa, in one form oranother. But large doses produce schizo-phrenic-like symptoms, the higher the dosethe greater the incidence.77,78 This is notsurprising since dopachrome must haveproperties similar to adrenochrome, i.e. isan hallucinogen. More likely Parkinson’sdisease is a combination of too littledopamine and too much dopachrome i.e.there is excessive conversion of dopamine

163
How to Live Longer and Feel Better–Even with Cancer
into dopachrome. Dopachrome is neuro-toxic and by increasing destruction of neu-rons will accelerate the development of thedisease while at the same time masking someof the symptoms. Adrenalin is oxidized tooxidized adrenalin losing one electron. In thepresence of the NAD<——>NADH systemthe oxidized adrenalin is reduced back toadrenalin and the cycle continues. Whenthere is too little NAD or NADH or bothanother electron is lost and adrenochromeis formed. This last reaction is irreversible.Vitamin B3, therefore, can decrease the pro-duction of adrenochrome. This has notbeen tested experimentally but in arecent series of reports, Professor J. G. D.Birkmayer and his associates at theBirkmayer Institute for Parkinson Therapy,in Vienna, Austria, studied a stable form ofNADH. They found that their stable prepa-ration using 5 mg doses was therapeutic forParkinson’s disease, for Alzheimer’s, and fordepression.79–82 They wrote, “When we firstused NADH with regard to its clinical effi-cacy the effect was not convincing. This wasmost likely due to the rapid dissolution (ap-proximately 10-15 minutes) of the capsuleleading to a release of NADH into the acidconditions of the stomach. Since NADHis rapidly oxidized below pH 7.6 the con-ditions in the stomach will inactivateNADH by converting it to NAD. The in-vestigations of this report were therefore per-formed with NADH capsules coated withan acid stable film and a release time of twoto three hours. With this galenic formula-tion of NADH an improvement in disabil-ity could be achieved which was compara-ble to that of intravenously appliedNADH.”
The lipid soluble vitamin E has sometherapeutic value in treating Parkinson’sdisease. Coenzyme Q10 is coming intoprominent use as a powerful anti-oxidant.Schapira et al 83 reported that NADH-ubi-quinone (Q10) reductase (Complex 1) andNADH cytochrome c reductase activitieswere reduced in Parkinson’s disease in thesubstantia nigra. It occurred to me that pro-
viding both increased amounts of niacin,the precursor of NAD and NADH, andlarge amounts of coenzyme Q10, would beof value in treating cases of Parkinson’s dis-ease. I have given this combination to onepatient with classical Parkinson’s disease.The first one, age 84, had been on the or-thomolecular regimen for at least 25 yearsand he was mentally normal. His programincluded niacin 1 gram tid and the usual anti-oxidants such as ascorbic acid, vitamin E,selenium. A couple of years ago Parkinson’sdisease was diagnosed. It was evident inhis gait, leg muscle weakness and tremor.Last year his neurologist started him onSinemetTM which may have helped slightlybut he continued to deteriorate. Late lastsummer I advised him to add coenzymeQ10, 600 mg daily to his program. Withintwo weeks he was much better. When Isaw him early in July this year he had re-gained the use of his limbs, had very littletremor and was able once more to play golfas had been his habit before. He is on Q10,300 mg daily. His neurologist was very sur-prised at the marked improvement.
Another patient had difficulty walkingfor many years. Her walk closely resembledthe walk of a patient with Parkinson’s dis-ease and the diagnosis had been consideredby her physician. I tried to help her for sev-eral years with no relief. But after she wasstarted on Q10 300 mg daily, within onemonth there was a marked improvementin her walk and also in her mood.
With a combination of vitamin B3 plusanti-oxidants, especially Q10, it may bepossible to prevent and to treat Parkinson’sdisease. The treatment would have to bestarted as early as possible before too manyneurons have been destroyed by the adreno-chrome or dopachrome. The niacin willprotect against the psychological side effectsof the l-dopa treatment and the anti-oxidants will protect against the neuromus-cular effects of the disease. One could thenuse l-dopa without the patient having tosuffer its toxic consequences and their liveswould be prolonged.

164
Journal of Orthomolecular Medicine Vol. 11, No. 3, 1996
Conclusions1) The survival trends which appeared
in the first Hoffer and Pauling paper, andreappeared in our second one and in mythird presentation, are reconfirmed in thisreport. From 101 patients on the program,a core of 33 patients remain alive as of July1, 1996. Of these 33, 24 have lived 10 years,and seven more will probably live 10 years.The ten year survival will probably be 30%out of the original group. Over half of theseven 1992 deaths were due to non-cancerphysical causes. It is likely further deathswill come increasingly from other causes.
2) This conclusion applies only topatients who have received a combinationof all the standard modalities of treatmentand orthomolecular treatment.
3) The estimated survivals from thefirst Hoffer and Pauling report are con-firmed by the actual and expected futuresurvivals of these groups.
4) Better results were found with pa-tients who were placed on the combina-tion soon after they were diagnosed andstandard treatment was started. Addingcoenzyme Q10 improved the results byabout ten percent.
5) Arbitrarily I have concluded thatthere must be a minimum two month pe-riod on the nutritional program before itcan begin to demonstrate its ability to pro-long life. More study will be required todetermine what is the minimum period.
6) The program is palatable. The onlypatients who could not follow it were thosewho were getting chemotherapy and suf-fered severe nausea and vomiting, or pa-tients who could not swallow because oflesions in their throats.
7) Orthomolecular treatment improvesthe quality of life. It also decreases the sideeffects of radiation and chemotherapy.
8) Orthomolecular therapy provides astep forward in the battle against cancerwhich must be fully explored. There canbe no logical reason today why most ofthe research funds should go toward theexamination of ever more chemotherapy
of the standard kind and more ways of giv-ing radiation. There must be a major ex-pansion in the use of orthomoleculartherapy, to sort out the variables and todetermine how to improve the therapeu-tic outcome of treatment.
9) Enterprising medical schoolsshould immediately consider establishingchairs in Orthomolecular Oncology. I rec-ommend that there should be at least oneLinus Pauling Chair of OrthomolecularOncology.
10) I have proposed a hypothesis toaccount for the apparent incompatibilitybetween schizophrenia and cancer, usingthe adrenochrome hypothesis as the basis.
References1. Pauling L: Orthomolecular Psychiatry, Science
1968;160:265-271.2. Hoffer A, Osmond H, Callbeck MJ & Kahan
I: Treatment of Schizophrenia with NicotinicAcid and Nicotinamide. J Clin ExperPsychopathol, 1957; 18:131-158.
3. Hoffer A & Osmond H: How To Live WithSchizophrenia. New York, University Books,1966. New and Revised Ed. New York, Cita-del Press, 1992.
4. Hoffer A: Treatment of schizophrenia with atherapeutic program based upon nicotinic acidas the main variable. In ed. O Walaas, Mo-lecular Basis of Some Aspects of Mental Activity,Vol II, New York, Academic Press, 1967.
5. Hoffer A: Mechanism of action of nicotinicacid and nicotinamide in the treatment ofschizophrenia. In eds. DR Hawkins and LPauling: Orthomolecular Psychiatry, San Fran-cisco, WH Freeman and Co, 1973.
6. Hoffer A: Some theoretical principles basic to or-thomolecular psychiatric treatment. In ed. LHippchen, Ecologic-Biochemical Approaches toTreatment of Delinquents and Criminals. New York.Van Nostrand-Reinhold Co, 1978; 31-55.
7. Hoffer A: Chronic schizophrenic patientstreated ten years or more. J. OrthomolecularMedicine, 1994; 9: 7-37.
8. Altschul R, Hoffer A & Stephen JD: Influenceof Nicotinic Acid on Serum Cholesterol inMan. Arch Biochem Biophys, 1955; 54: 558-559.
9. Parsons WB, Achor RWP, Berge KG et al:Changes in concentration of blood lipid levelsfollowing prolonged administration of largedoses of nicotinic acid to persons withhypercholesterolemia: preliminary observations.
165
How to Live Longer and Feel Better–Even with Cancer
Proc. Staff. Meet. Mayo Clin 1956; 31: 377-90.10.Parsons WB: Clinical alternatives. coronary heart
disease. In ed. GV Mann: The Dietary Sense andNonsense. An Evaluation by Scientists. Great Brit-ain, Janus Publishing Co. 1993.
11.Pauling L: Vitamin C and The Common Cold,San Francisco, WH Freeman, 1971.
12.Cameron E & Pauling L: Cancer and Vita-min C. Palo Alto, CA, Linus Pauling Insti-tute of Science and Medicine, 1979.
13.Cameron E & Pauling L: Cancer and Vita-min C. Updated and Expanded. Philadelphia,Camino Books, 1993.
14.Hoffer J: Nutrients as biologic response modi-fiers. In ed. P Quillin & RM: Adjuvant Nutri-tion in Cancer Treatment. Williams. 1992 Sym-posium Proceedings, Cancer Treatment Re-search Foundation and American College ofNutrition, Cancer Treatment ResearchFoundation, 3455 Salt Creek Lane Suite 200,Arlington Heights, IL 60005-1090, 1993.
15.Hoffer A: Treatment of organic psychosis withnicotinic acid (A Single Case). Dis Nerv Syst,1965; 26: 358-360.
16.Hoffer A, Osmond H, Callbeck MJ & KahanI: Treatment of schizophrenia with nicotinicacid and nicotinamide. J Clin ExperimPsychopathol, 1957; 18:131-158.
17.Jacobson EL: Niacin deficiency and cancer inwomen. J American College of Nutrition 1992;11: 597-637.
18.Jacobson EL & Jacobson MK: A biomarkerfor the assessment of niacin nutriture as a po-tential preventative factor in carcinogenesis.J Intern Med , 1993; 233: 59-62.
19.Hoffer A: Orthomolecular Medicine for Physi-cians. New Canaan, CT, Keats Publ. 1989.
20.Pauling L: Biostatistical analysis of mortalitydata for cohorts of cancer patients. Proc NatAcad Sci USA, 1989; 86:3466-3488.
21.Pauling L & Herman Z: Criteria for the validityof clinical trials of treatments of cohorts of cancerpatients based on the Hardin Jones principle. ProcNat Acad Sci USA, 1989; 86: 6835-6837.
22.Hoffer A & Pauling L: Hardin-jones bio-statistical analysis of mortality data for cohortsof cancer patients with a large fraction surviv-ing at the termination of the study and a com-parison of survival times of cancer patients re-ceiving large regular oral doses of vitamin Cand other nutrients with similar patients notreceiving those doses. J Orthomolecular Medi-cine, 1990; 5:143-154.
23.Hoffer A & Pauling L: Hardin-jonesbiostatistical analysis of mortality datafor a second set of cohorts of cancer patientswith a large fraction surviving at the termina-
tion of the study and a comparison of survivaltimes of cancer patients receiving large regu-lar oral doses of vitamin C and other nutri-ents with similar patients not receiving thesedoses. J Orthomolecular Medicine, 1993; 8:1547-1567.
24.Hoffer A: Orthomolecular Oncology. In ed. PQuillin & RMWilliams, Adjuvant Nutritionin Cancer Treatment. Cancer Treatment Re-search Foundation, 3455 Salt Creek LaneSuite 200, Arlington Heights, IL 60005-1090: 1994.
25.Hoffer A (With Major Contributions by LinusPauling), Quarry Press, in press (due 1997).
26.Pauling L: Quoted in “The NutritionReporter” Challem J, 1992; 3: 8.
27.Hoffer A: Orthomolecular oncology and sur-vival. Adjuvant Nutrition in Cancer TreatmentSymposium. San Diego, CA, March 17-19,1994.
28.Bliznakov EG & Hunt GL: The Miracle Nu-trient Coenzyme Q10. Toronto. BantamBooks, 1987.
29.Folkers K, Brown R, Judy WV & Morita M:Survival of cancer patients on therapy withCoenzyme Q10. Biochem Biophys Res Comm,1993; 192: 241-245.
30.Levine AM: The importance of hope. West JMed, 1989; 150: 609.
31.Sapolsky RM: On human nature. The Sci-ences 1994; 34:10-14.
32.Matthews SB, Henderson AH & CampbellAK: The adrenochrome pathway: The majorroute for adrenalin catabolism by polymor-phonuclear leucocytes. J Mol Cell Cardiol1985; 17: 339-348.
33.Bindoli A, Rigobello MP & Deeble DJ: Bio-chemical and toxicological properties of the oxi-dation products of catecholamines. Free Radi-cal Biology & Medicine 1992;13: 391- 405.
34.Dhalla KS, Ganguly PK, Rupp H, Beamish RE& Dhalla NS: Measurement of adrenolutin asan oxidation product of catecholamines inplasma. Molecular and Cellular Biochemistry1989; 87: 85-92.
35.Hoffer A & Osmond H: The Hallucinogens.New York, Academic Press, 1967.
36.Hoffer A, Osmond H & Smythies J: Schizo-phrenia: A New Approach. II. Results of aYear’s Research. J Ment Science 1954;100: 29-45.
37.Hoffer A: Adrenochrome and adrenolutin andtheir relationship to mental disease. In eds.Garattini S & Ghetti V: Psychotropic Drugs.London, Elsevier Press, 1957; 10-20.
38.Hoffer A: The effect of adrenochrome andadrenolutin on the behavior of animals andthe psychology of man. Int Rev Neurobiol-
166
Journal of Orthomolecular Medicine Vol. 11, No. 3, 1996
ogy 1962; 4: 307-371.39.Hoffer A: The adrenochrome hypothesis of
schizophrenia revisited. J Orthomolecular Psy-chiatry 1981;10: 98-118.
40.Hoffer A: Oxidation-reduction in the brain. JOrthomolecular Psychiatry, 1983; 12: 292-301.
41.Hoffer A & Osmond H: The adrenochromehypothesis and psychiatry. J OrthomolecularMedicine, 1990; 5: 32-45.
42.Smythies J: On the function of neuromelanin.Proc Roy Soc (London) B2, 1996; 63: 491-496.
43.Smythies J: Hallucinogenic drugs. Encyclope-dia of Neuroscience. In press, 1996.
44.Smythies J: The role of ascorbate in brain:therapeutic implications. J Roy Soc of Med1996; 89: 241.
45.Smythies J: Disturbances of one-carbon me-tabolism in neuropsychiatric disorders: a re-view. Submitted to Biological Psychiatry, 1996.
46.Hoffer A: Schizophrenia: An Evolutionarydefence against severe stress. TownsendLetter for Doctors and Patients #151/152Feb/Mar 1996.
47.Nauts HC: Bacterial products in the treat-ment of cancer: past, present and future. Ineds. Jeljaszewics J, Pulverer G, Rostowski W:Bacteria and Cancer, New York. AcademicPress 1982.
48.Kanofsky JD, Norkus EP, Geller B, LowingerR, Kanofsky PB & Kennedy GK: Schizo-phrenia, lung cancer and vitamin C. Ameri-can Psychiatric Association, Poster Session,Philadelphia, May 1994.
49.Falk R: Personal communication, 1995.50.Holt JAG: Letter, September 21, 1993, Mi-
crowave Therapy Center, 311 Outram St.,W. Perth, Australia, 6005.
51.Huxley J, Mayr E, Osmond H & Hoffer A:Schizophrenia as a genetic morphism. Na-ture, 1964; 204: 220-221.
52.Brown JS & Foster HD: Schizophrenia: an up-date of the selenium deficiency hypothesis.J Orthomolecular Medicine, In press, 1996.
53.Edelman E: Natural Healing for Schizophre-nia. A Compendium of Nutritional Methods.Eugene, OR, Borage Books, 1996.
54.Hoffer A: The psychophysiology of cancer.J Asthma Res, 1970; 8: 61-76.
55.Nakatsugawa S & Sugahara T: Differentialaction on cancer and normal tissue byadrenochrome monaminoguanidine meth-ane-sulfonate and cytochrome C combinedwith radiotherapy. Int J of Radiation Oncol-ogy, Biology, Physics 29:635-638, 1994.
56.Sugamoto K, Kimura H, Kawashima H, ItojimaT, Aoyama T & Sugahara T: Radioprotec-tive effects of adrenochrome monoamino-
guanidine methanesulfonate (AMM) on irra-diated C57B1 mice and the survival of GM-CFC, a hemotopoietic progenitor cell. JRadiat Res, 29:211-219, 1988.
57.Yamashita H, Okura J & Izumi K: Protectiveeffect of adrenochrome monoguanylhydra-zone methanesulfonate (S-Adchon) on thehematopoietic organ as revealed in irradiatedcancer patients. J Radiat Res 12:41-50, 1971.
58.Kim JH, Kim SH, He S, Dragovic J, BrownS: Use of vitamins as adjunct to conven-tional cancer therapy. Second Denver Con-ference on Nutrition and Cancer, Denver,CO, Sept 7-11, 1994. In Nutrients in CancerPrevention and Treatment. Eds. PrasadKN, Santamaria L & Williams RM, HumanaPress, New Jersey, 363-372, 1995.
59.Agnew N & Hoffer A: Nicotinic acid modi-fied lysergic acid diethylamide psychosis.J Ment Science, 101:12-27, 1955.
60.Stone I: The Healing Factor: Vitamin C againstDisease. Grosset and Dunlap, New York, 1972.
61.Pauling L: How To Live Longer and FeelBetter. WH Freeman and Company, NewYork, NY, 1986.
62.Hoffer A: Vitamin B3 (Niacin). Keats Pub,New Canaan, CT, 1984.
63.McCracken RD: Niacin and Human HealthDisorders. Hygea Publishing Co., 635Peterson St., Fort Collins, CO, 80524.
64.Hoffer A & Walker M: Smart Nutrients - AGuide to Nutrients That Can Prevent and Re-verse Senility. Avery Publishing Group, Gar-den City Park, NY, 1994.
65.Hoffer A: Hoffer’s Law of Natural Nutrition.Quarry Press, Kingston, ON, 1996.
66.Hoffer A & Walker M: Putting It All Together- The New Orthomolecular Nutrition. KeatsPublishing Inc, 27 Pine Street, Box 876, NewCanaan, CT 06840-0876, 1994.
67.Canner PL, Berge KG, Wenger NK, StamlerJ, Friedman L, Prineas RJ, Friedewald W:Fifteen year mortality in coronary drugproject patients: long-term benefit withniacin. J Amer Coll of Cardiology, 8:1245-1255, 1986.
68.Rimm EB, Stampfer MJ, Ascherio A,Giovannucci E, Colditz GA & Willett WC:Vitamin E consumption and the risk of coro-nary heart disease in men. New England JMed 1993; 328: 1450-1456. In this paperthere is no reference to the work done by theShute Brothers in Ontario about 50 years ago.Their work had already established the enormousvalue of vitamin E in the treatment of coronarydisease and other diseases.
69.Stampfer MJ, Hennekens CH, Manson J,
167
How to Live Longer and Feel Better–Even with Cancer
Colditz GA, Rosner B & Willett WC: Vita-min E consumption and the risk of coronarydisease in women. New England J Med 1993;328: 1444-1449.
70.Prasad, KN Chairperson. Second Denver Con-ference on Nutrition and Cancer. Sept 7 - 11,1994, Denver, Colorado. In eds. Prasad N,Santamaria L & Williams RM: Nutrients inCancer Prevention and Treatment. New Jersey,Humana Press, 363-372, 1995.
71.Prasad KN: Cellular basis of using multipleantioxidant vitamins in cancer preventionand treatment. Nutrition in Cancer Treat-ment Symposium, Tampa, Florida, 1995.
72.Fornstedt B: Role of catechol autooxidationin the degeneration of dopamine neurons.Acta Neurol Scand,Suppl. 1990; 129: 12-14.
73.Mann DMA & Yates PO: Possible role ofneuromelanin in the pathogenesis of Parkinson’sdisease. Mech Age Dev, 1983; 21: 193-203.
74.Olanow CW: Oxidation reactions in Parkinson’sdisease. Neurology 40 (Suppl 3) 1990: 32-38.
75.Fahn S & Cohen G: The oxidant stress hy-pothesis in Parkinson’s disease: Evidence sup-porting it. Annals Neurology,1992; 32:804-812.
76.Jenner P: Oxidative damage in neuro-degenerative disease. The Lancet 1994; 344:796-798.
77.Hoffer A: L-dopa: an hallucinogen. Schizo-phrenia 1970; 2:37, and 1970; 2:127.
78.Hoffer A: Dopamine, noradrenalin andadrenalin metabolism to methylated or chromeindole derivatives: two pathways or one?J Orthomolecular Psychiatry 1985; 14: 262-272.
79.Birkmayer W & Birkmayer GJD: Nicotina-mide adenine dinucleotide (NADH): thenew approach in the therapy of Parkinson’sdisease. Ann Clin Lab Sci 1989; 19: 38-43.
80.Birkmayer JGD, Vrecko C, Volc D &Birkmayer W: Nicotinamide adenine dinu-cleotide (NADH) - a new therapeutic ap-proach to Parkinson’s disease. Acta NeurolScand, Suppl. vol. 8, 1993; 146P: 32-35.
81.Birkmayer JGD: Nicotinamide adenine dinu-cleotide (NADH) the new therapeutic ap-proach for improving dementia of the Alzhe-imer’s type. Forschungs- und Lehreinrichtung desBirkmayer Instituts fur Parkinsontherapie. Vi-enna, Austria. Menuco Corp., 350 Fifth Ave.,Suite 7509, New York, NY 10118.
82.Birkmayer JGD & Birkmayer W: Thecoenzyme nicotinamide adenine dinucle-otide (NADH) as biological antidepressiveagent. Experience with 205 Patients. NewTrends in Clinical Neuropharmacology 1991;5: 19-25 .
83.Schapira AHV, Cooper JM, Dexter D, ClarkJB, Jenner P & Marsden CD: Mitochon-drial complex I deficiency inParkinson’s dis-ease. J. Neurochem 1990; 54: 823-827.