how to refer a cancer patient · medical oncology referrals 902 473 6079(f) •all referrals need...
TRANSCRIPT
HOW TO REFER A CANCER PATIENTA PRACTICAL GUIDE ON WHAT TO DO IF “TUMOR IS THE RUMOR”

ACKNOWLEDGEMENTS
• I have had been involved in research and ad boards with many
pharmaceutical companies however declare that this talk does not involve
them and I therefore have no conflicts
• I have coordinated this talk with the Nova Scotia Cancer Care Program and
would like to thank them and praise them for working to fulfill their mission
statement “Led by compassion and driven by evidence, together we work to
alleviate the burden of cancer”
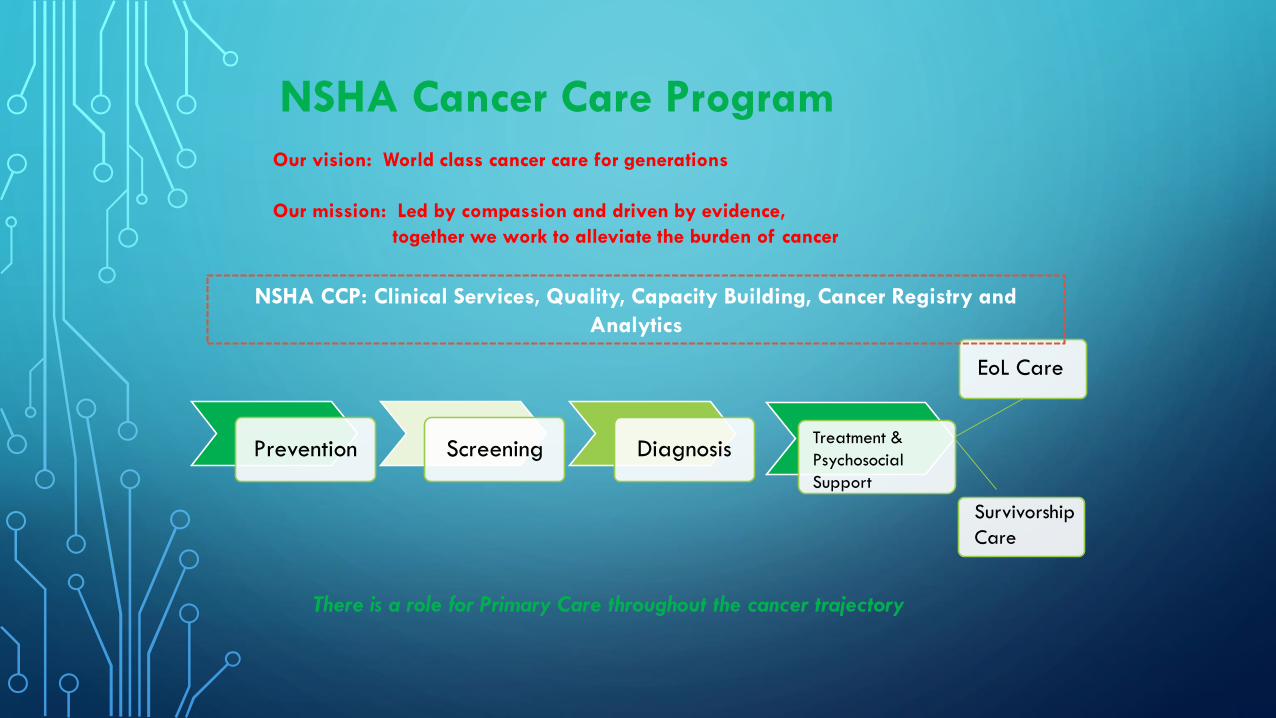
NSHA Cancer Care Program
Our vision: World class cancer care for generations
Our mission: Led by compassion and driven by evidence,
together we work to alleviate the burden of cancer
Prevention Screening DiagnosisTreatment &
Psychosocial
Support
EoL Care
Survivorship
Care
There is a role for Primary Care throughout the cancer trajectory
NSHA CCP: Clinical Services, Quality, Capacity Building, Cancer Registry and
Analytics

NSHA Cancer Care ProgramNSHA Cancer Care Program
Tertiary/Quaternary
Cancer Centers
Community Cancer
Clinics
*
www.nscancercare.ca
Photo credit: McCallum

PRACTICAL TIPS
• Consider patients preference, age, comorbidities and life expectancy when
determining extent of work up’
• Does the patient need further tests before referral ie biopsy, metastatic work
up, tumor markers, etc
• If you do not know what to do phone and ask
REFERRALS
• All Gyne onc and Heamatology consults are centrally triaged at the QEII
• Med Onc consults are triaged in Halifax or Sydney
• If you want a certain oncologist specify on the referral and tell the patient
they might have to wait longer and they may not treat that type of cancer
and you will someone else.

REFERRALS
• Required Information is almost always the final path report and all imaging. We triage by
tumor type and staging determines treatment.
• Use the Phone if need be.
• Urgent referrals mean something if we hear why ( worry is not unique enough to be
urgent)
• QEII referral Office 902-473-5140 or med onc/heam on call 902 473 2220
• Cape Bretton 902-567-7771
• Unfortunately we are full. Urgent consults may result in bumping. We do not have a wait list
because they cannot wait. We cannot see all patients locally or at certain times.
• Unattached patients are becoming a problem with followup.
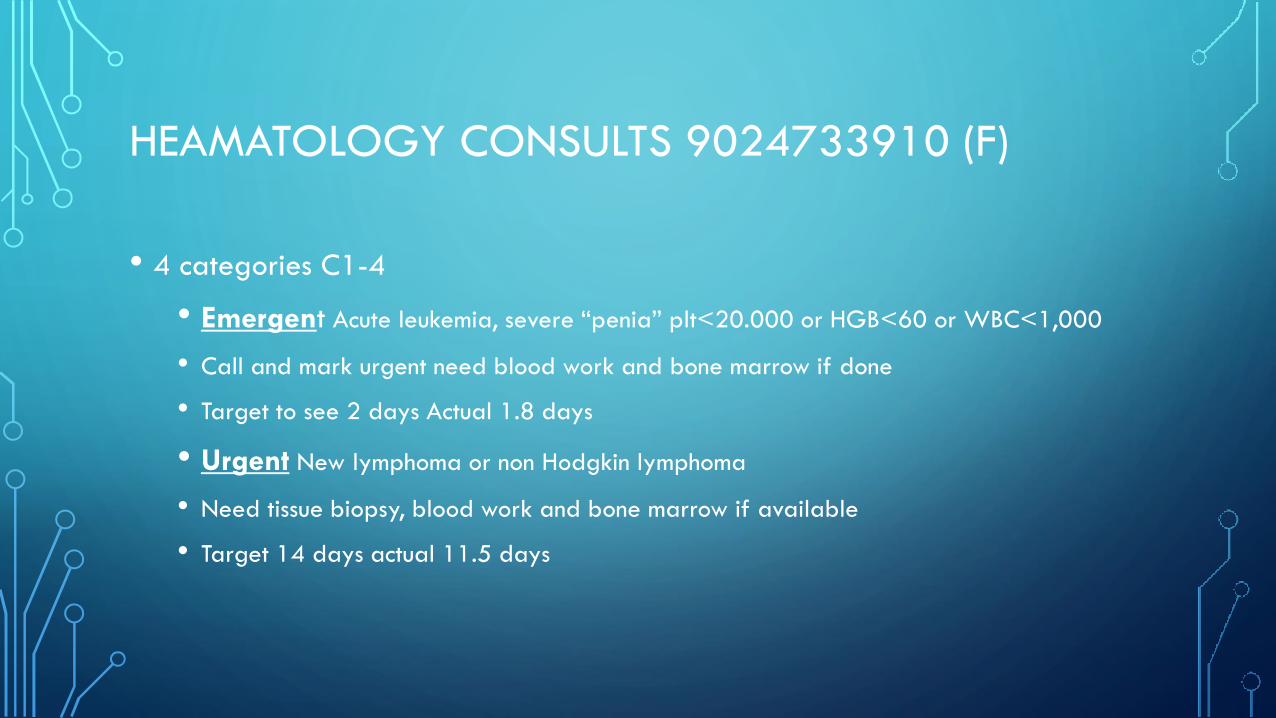
HEAMATOLOGY CONSULTS 9024733910 (F)
• 4 categories C1-4
• Emergent Acute leukemia, severe “penia” plt<20.000 or HGB<60 or WBC<1,000
• Call and mark urgent need blood work and bone marrow if done
• Target to see 2 days Actual 1.8 days
• Urgent New lymphoma or non Hodgkin lymphoma
• Need tissue biopsy, blood work and bone marrow if available
• Target 14 days actual 11.5 days

• Semi-urgent Myeloma, CML, moderate anemia <80 or thrombocytopenia
<50,000
• Need blood work and bone marrow if available
• Target 42 days, actual 32.6 days
• Non urgent perioperative management of anticoagulation, CLL,
heamachromatosis, etc.
• Target 90 days A lot are not seen and advise given via phone
HEAMATOLOGY CONSULTS 9024733910 (F)

MEDICAL ONCOLOGY REFERRALS902 473 6079(F)
• All referrals need Pathology, staging ( imaging and bloodwork) and note
• Emergent (target 1 day) SVC syndrome from Small Cell Lung cancer.
Fax, write “emergency”, and call the Medical Oncologist on call
• Urgent ( target 7 days)Ewing’s Sarcoma (preoperative therapy),
Inflammatory breast cancer, metastatic testicular cancer, Osteosarcoma (
preoperative therapy), Small cell lung cancer, any urgent request with
explanation
MEDICAL ONCOLOGY REFERRALS902 473 6079(F)
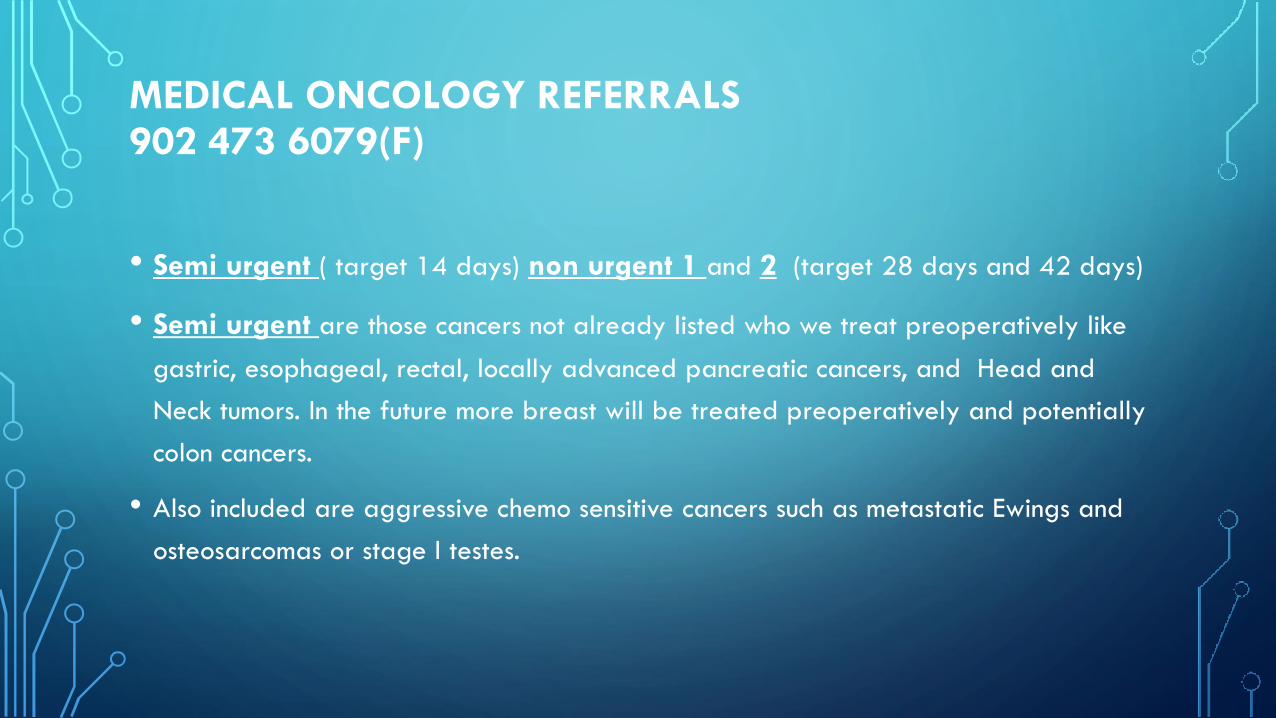
• Semi urgent ( target 14 days) non urgent 1 and 2 (target 28 days and 42 days)
• Semi urgent are those cancers not already listed who we treat preoperatively like
gastric, esophageal, rectal, locally advanced pancreatic cancers, and Head and
Neck tumors. In the future more breast will be treated preoperatively and potentially
colon cancers.
• Also included are aggressive chemo sensitive cancers such as metastatic Ewings and
osteosarcomas or stage I testes.

MEDICAL ONCOLOGY REFERRALS902 473 6079(F)
• The non urgent categories are all others but the time lines are not always
clear in that adjuvant therapies are measured from time of OR not referral
arrival so a 8 week timing for adjuvant breast cancer is sometimes sent to us
at 6 weeks and we need to try to fit in in 2 weeks
• Currently my next new patient appointment is FEB 25th . We have a locum
Medical oncologist in town awaiting credentialing and nursing resources to
help. Work load statistics show every oncologists exceeds their target as a
group are 23% over their target
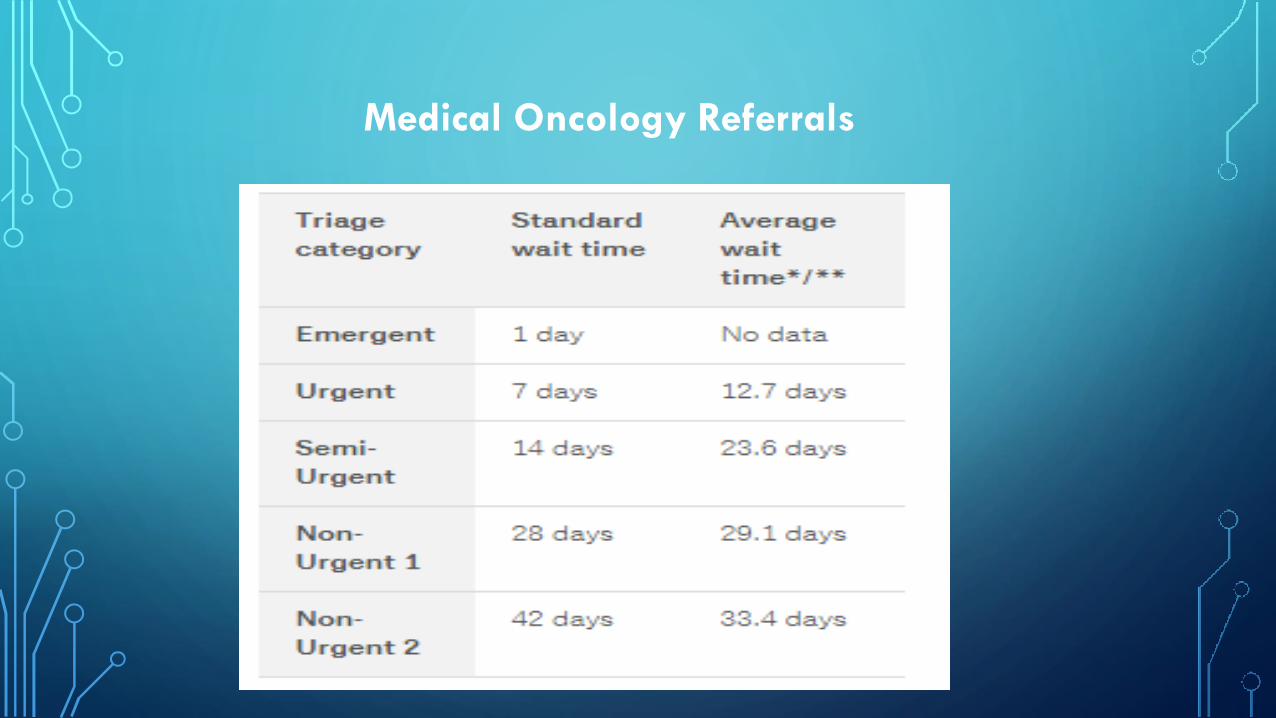
Medical Oncology Referrals
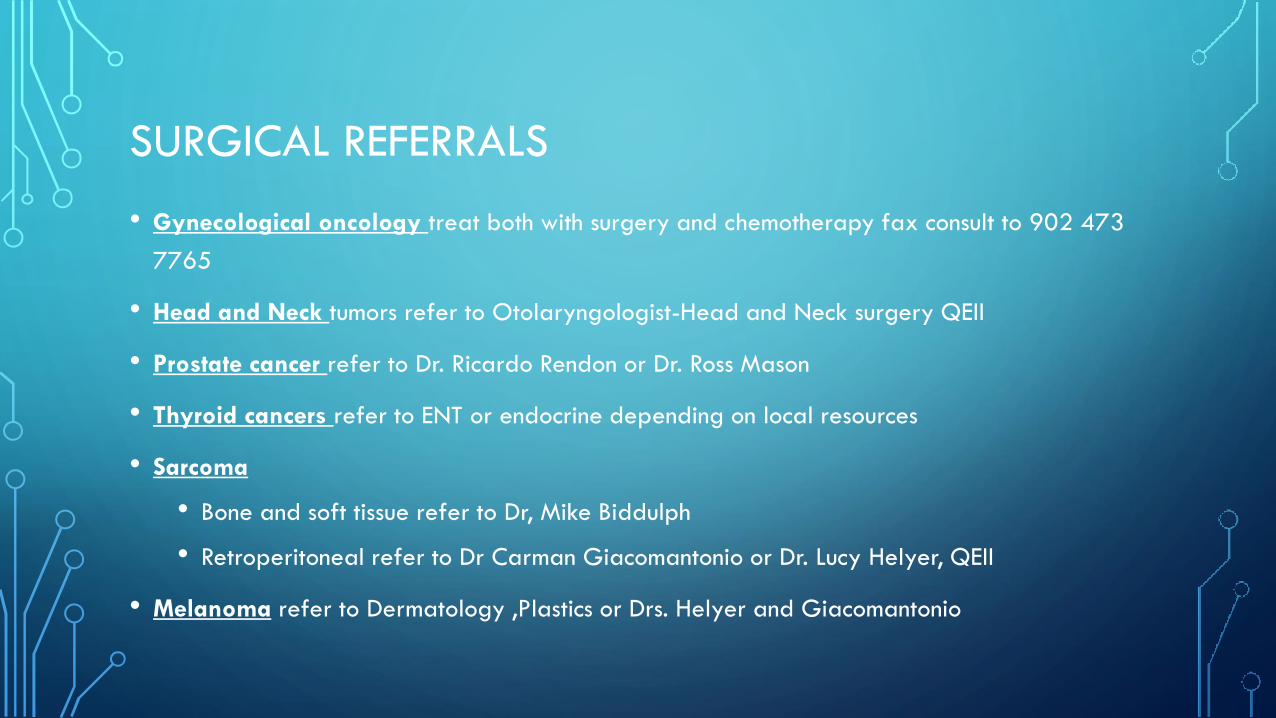
SURGICAL REFERRALS
• Gynecological oncology treat both with surgery and chemotherapy fax consult to 902 473
7765
• Head and Neck tumors refer to Otolaryngologist-Head and Neck surgery QEII
• Prostate cancer refer to Dr. Ricardo Rendon or Dr. Ross Mason
• Thyroid cancers refer to ENT or endocrine depending on local resources
• Sarcoma
• Bone and soft tissue refer to Dr, Mike Biddulph
• Retroperitoneal refer to Dr Carman Giacomantonio or Dr. Lucy Helyer, QEII
• Melanoma refer to Dermatology ,Plastics or Drs. Helyer and Giacomantonio

REFERRAL PATTERNS
• Children refer to IWK if 16 or under, if 16-18 depends on type of cancer
and patient
DIAGNOSTIC PATHWAYS- PANCREAS, LIVER
• Symptoms such as weight loss, fatigue, dull epigastric pain, early satiety,
steatorrhea, glucose intolerance, and jaundice
• Investigations Abdominal imaging including ERCP if required and blood work
including CA19-9 and CEA
• Refer to HPB Surgeons who will do workup and any referrals required
DIAGNOSTIC PATHWAYS- LUNG
• Symptoms – hemoptosis, stridor, new unexplained cough and dyspnea
• CXR if negative observe and repeat if still suspicious
• If positive refer to Thoracic surgery
DIAGNOSTIC PATHWAYS- ABDOMINAL MASS
• Mass found on pt suspicious for cancer and not liver lung or pancreas
• Blood work including tumor markers for germ cell tumor (AFP ,BHCG)
• Biopsy needed unless testicular or germ cell tumor
• Invasive radiology / surgery /others. ( ongoing discussion)

Onc Emergencies Guideline
• Bleeding in a Cancer Patient• Gastrointestinal bleeding, Hematuria, Hemoptysis and Vaginal bleeding
• Brain Metastases, Increased Intracranial Pressure and Seizures
• Disseminated Intravascular Coagulation
• Febrile Neutropenia (High Risk and Low Risk)
• Hyperviscosity Syndrome
• Immunotherapy Adverse Reactions (2019 edition)
• Malignancy Associated Hypercalcemia
• Malignant Airway Obstruction
• Malignant Epidural Spinal Cord Compression
• Superior Vena Cava Obstruction
• Syndrome of Inappropriate Antidiuretic Hormone Secretion
• Tumor Lysis Syndrome • Hyperuricemia, Hyperkalemia, Hyperphosphatemia and Hypocalcemia
• Venous Thromboembolism (2019 edition)
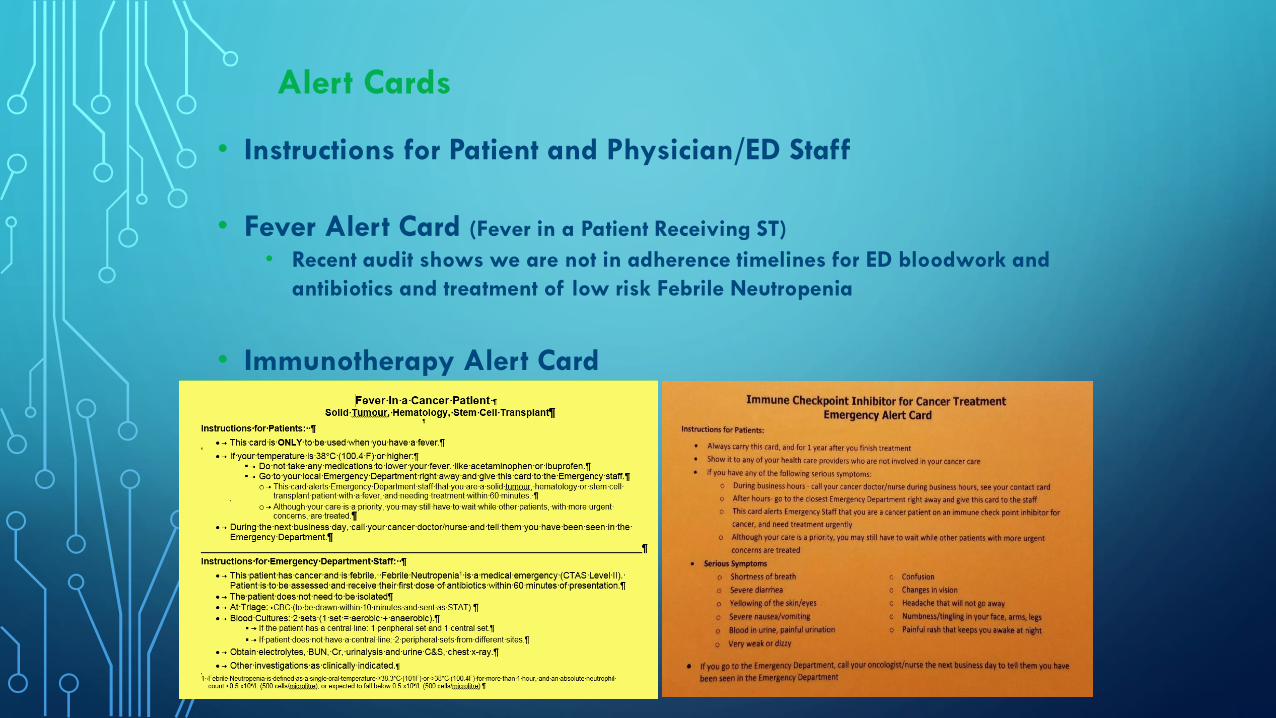
Alert Cards
• Instructions for Patient and Physician/ED Staff
• Fever Alert Card (Fever in a Patient Receiving ST)
• Recent audit shows we are not in adherence timelines for ED bloodwork and
antibiotics and treatment of low risk Febrile Neutropenia
• Immunotherapy Alert Card

• QEII Patient Line 902-473-6067 (MO) 902-473-6605
(Hem)
• QEII Oncologist On Call 902-473-2222
• Patient’s Oncologist during regular hours

Gynecologic Oncologists, QEII
Dr. Katharina Kieser, Division Chief
Dr. Jim Bentley
Dr. Lana Šačiragić
Dr. Stephanie Scott
Dr. Karla Willows
Hematologists
Dr. Sudeep Shivakumar, Division Chief, QEII
Dr. David Anderson, QEII
Dr. Mahmoud Elsawy, QEII
Dr. Louis Fernandez, QEII
Dr. Nicolas Forward, QEII
Dr. Christina Fraga, QEII
Dr. Wanda Hasegawa, QEII
Dr. Ormille Hayne, QEII
Dr. Mary Margaret Keating, QEII
Dr. Katherine Mac Innes, CBCC
Dr. K. Sue Robinson, QEII
Dr. Ismail Sharif, QEII
Dr. Darrell White, QEII

Dr. Daniel Rayson, Division Chief, QEII Breast, Neuroendocrine, Colorectal
Dr. Bruce Colwell, QEII Breast, Colorectal, Sarcoma
Dr. Arik Drucker, QEII Breast, Lung
Dr. Alwin Jeyakumar, QEII Breast, Colorectal
Dr. Kian Khodadad, CBCC All Sites
Dr. Nathan Lamond, QEII Colorectal, ENT
Dr. Robin MacFarlane, QEII Genitourinary, Melanoma
Dr. Mary MacNeil, QEII Lung, Neuro-Oncology
Dr. Ron MacCormick, CBCC All Sites
Dr. Jennifer Melvin, QEII Breast, Melanoma, Sarcoma
Dr. Julia Merryweather Breast, GI, Lung
Dr. Wojciech Morzycki, QEII Lung, Mesothelioma, Unknown Primary
Dr. Rajbil Pahil, CBCC All Sites
Dr. Ravi Ramjeesingh, QEII Breast, Hepatobiliary
Dr. Wassim Saliba, CBCC All Sites
Dr. Stephanie Snow, QEII Lung, Gastroesophageal, ENT
Dr. Lori Wood, QEII GU
Dr. Tallal Younis, QEII Breast
Medical Oncologists and tumor expertise
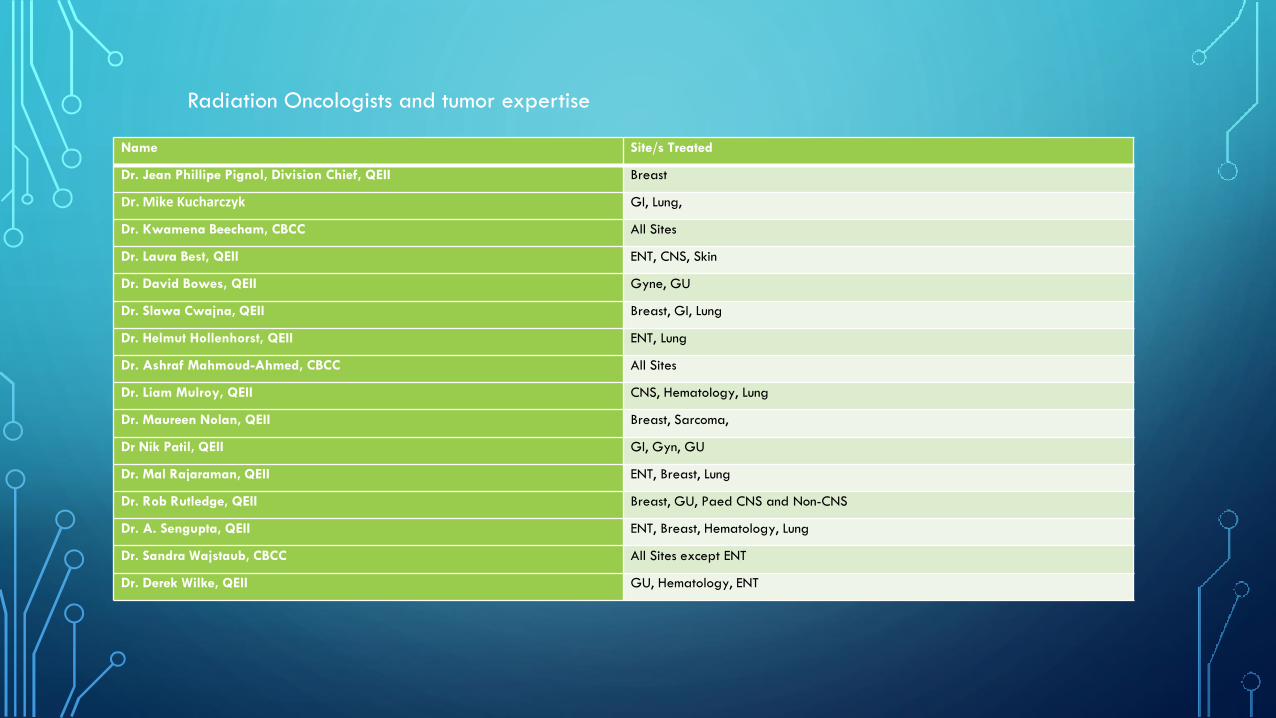
Name Site/s Treated
Dr. Jean Phillipe Pignol, Division Chief, QEII Breast
Dr. Mike Kucharczyk GI, Lung,
Dr. Kwamena Beecham, CBCC All Sites
Dr. Laura Best, QEII ENT, CNS, Skin
Dr. David Bowes, QEII Gyne, GU
Dr. Slawa Cwajna, QEII Breast, GI, Lung
Dr. Helmut Hollenhorst, QEII ENT, Lung
Dr. Ashraf Mahmoud-Ahmed, CBCC All Sites
Dr. Liam Mulroy, QEII CNS, Hematology, Lung
Dr. Maureen Nolan, QEII Breast, Sarcoma,
Dr Nik Patil, QEII GI, Gyn, GU
Dr. Mal Rajaraman, QEII ENT, Breast, Lung
Dr. Rob Rutledge, QEII Breast, GU, Paed CNS and Non-CNS
Dr. A. Sengupta, QEII ENT, Breast, Hematology, Lung
Dr. Sandra Wajstaub, CBCC All Sites except ENT
Dr. Derek Wilke, QEII GU, Hematology, ENT
Radiation Oncologists and tumor expertise
DRUG SHORTAGES
• Recently we have had a number of oncology drug shortages both IV and oral
• For IV drugs we have found alternatives or solutions so far for each shortage.
• The cancer care program has no jurisdiction in supplying or managing oral
drugs at this time. We feel however obligated to assist patients by trying to
organize a strategy for pharmacies. Tamoxifen is a recent example of a huge
amount of work that was done by the program that is unnoticed
NSCCP RESOURCES FOR PRIMARY CARE
• BC Cancer Drug Manual
• Oral systemic therapy Toolkit
• Immune Checkpoint Inhibitor Toolkit

NSCCP RESOURCES - SURVIVORSHIP
• Discharge templates to primary care Physicians from oncologist outlining surveillance
tests and schedules
• General Survivorship Care Plan
• Specific survivorship plans
• Breast
• Colon
• Thyroid
• Rectum
Patient Education Resources
• 80+ NSCCP Print Resources
• Videos
• Links to other reputable organizations

EDUCATIONAL OPPORTUNITIES
• Oncology Grand Rounds every thurs 1230 in person or Skype
• Provincial Cancer Network Meetings
• CME certified workshops
• Request an in-service on any Oncology topic
• Education contact [email protected]

QUESTIONS