hpb cancer pathway board - · pdf file1 hpb cancer pathway board annual report 2015/16...
TRANSCRIPT
1
HPB Cancer Pathway Board Annual Report 2015/16
Pathway Clinical Director: Mr. Derek O’Reilly Pathway Manager: Rebecca Price
Version 1.0
2
Executive summary: HPB Pathway Board 1. The Hepato-Pancreato-Biliary (HPB) Pathway Board has active representation for all ten
trusts in Greater Manchester and Cheshire that comprise Manchester Cancer. There is also patient and primary care representation.
2. From October 6, 2014, a single IOG compliant HPB Service has been located at the Manchester Royal Infirmary, Central Manchester NHS Foundation Trust (CMFT). This is now a well-established and successful unit.
3. The HPB Board have embraced the principle of wider engagement and educational
meetings. HPB Pathway Board meetings take place at two monthly intervals at each of the ten participating Trusts, with the additional feature of an educational event for the benefit of the local MDT.
4. We held our main educational event ‘Manchester Pancreatic Cancer Symposium 2016’ in Manchester Town Hall on 14th April 2016
5. We have delivered on our annual plan of 2015; making significant progress on implementing a regional jaundice pathway; establishing a prehabilitation programme; addressing patient experience; succeeding in recruiting to clinical trials and delivering a wide range of educational events throughout the region.
6. Research and Innovation is strength of the HPB Pathway board with a strong track record of leadership in academic activities: we are the lead recruiter for NIHR portfolio studies for HPB cancers.
7. We have successfully implemented the regional Jaundice Pathway through the Acceleration, Coordination and Evaluation (ACE) program. This provides one-stop jaundice clinics and fast-track surgery. We urgently need to establish a source of on-going funding
8. We have successfully established a prehabilitation programme for patients about to undergo HPB cancer surgery. This optimises patients for surgery through physical, nutritional and psychological support.
9. A comprehensive set of clinical guidelines and chemotherapy algorithms for HPB has been created.

3
1. Introduction – the Pathway Board and its vision This is the annual report of the Manchester Cancer HPB Pathway Board for 2015/16. This annual report is designed to:
Provide a summary of the work programme, outcomes and progress of the Board – alongside the minutes of its meetings, its action plan and it scorecard it is the key document for the Board.
Provide an overview to the hospital trust CEOs and other interested parties about the current situation across Manchester Cancer in this particular cancer area
Meet the requirements of the National Cancer Peer Review Programme
Be openly published on the external facing website. This annual report outlines how the Pathway Board has contributed in 2015/16 to the achievement of Manchester Cancer’s four overarching objectives:
Improving outcomes, with a focus on survival
Improving patient experience
Increasing research and clinical innovation
Delivering compliant and high quality services
1.1. Vision
Our key aims and vision are:
Better Patient Outcomes
Better Patient Experience
Research and Innovation
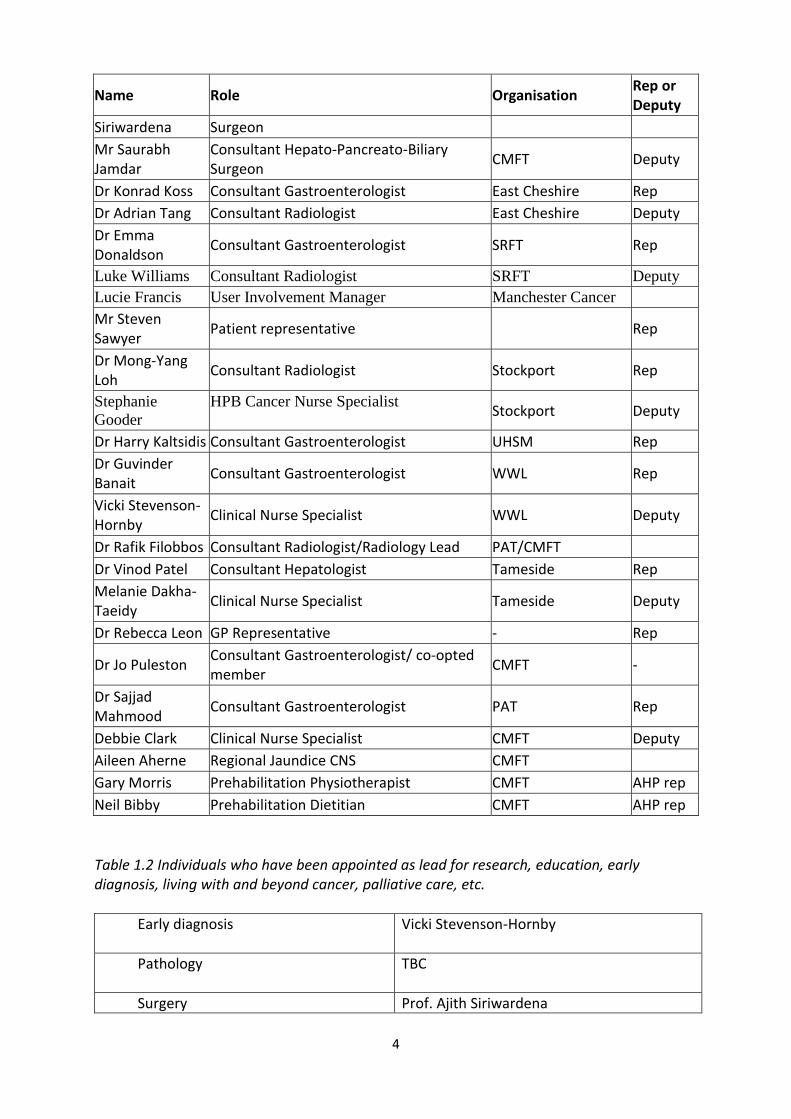
1.2. Membership Table1.1 The membership of the Pathway Board and the trusts/specialties of all individuals.
Name Role Organisation Rep or Deputy
Mr Derek O’Reilly
HPB Pathway Clinical Director CMFT/Manchester Cancer
Rebecca Price Pathway manager Manchester Cancer
Dr Mahesh Bhalme
Consultant Gastroenterologist/Hepatologist
Bolton Rep
Amanda Corfield-Halliwell
Clinical Nurse Specialist Bolton Deputy
Professor Juan Valle
Consultant Medical Oncologist/Pathway Board Research Lead
Christie Rep
Dr Mairead MacNamara
Consultant in Medical Oncology Christie Deputy
Professor Ajith Consultant Hepato-Pancreato-Biliary CMFT Rep
4
Name Role Organisation Rep or Deputy
Siriwardena Surgeon
Mr Saurabh Jamdar
Consultant Hepato-Pancreato-Biliary Surgeon
CMFT Deputy
Dr Konrad Koss Consultant Gastroenterologist East Cheshire Rep
Dr Adrian Tang Consultant Radiologist East Cheshire Deputy
Dr Emma Donaldson
Consultant Gastroenterologist SRFT Rep
Luke Williams Consultant Radiologist SRFT Deputy
Lucie Francis User Involvement Manager Manchester Cancer
Mr Steven Sawyer
Patient representative Rep
Dr Mong-Yang Loh
Consultant Radiologist Stockport Rep
Stephanie
Gooder
HPB Cancer Nurse Specialist Stockport Deputy
Dr Harry Kaltsidis Consultant Gastroenterologist UHSM Rep
Dr Guvinder Banait
Consultant Gastroenterologist WWL Rep
Vicki Stevenson-Hornby
Clinical Nurse Specialist WWL Deputy
Dr Rafik Filobbos Consultant Radiologist/Radiology Lead PAT/CMFT
Dr Vinod Patel Consultant Hepatologist Tameside Rep
Melanie Dakha-Taeidy
Clinical Nurse Specialist Tameside Deputy
Dr Rebecca Leon GP Representative - Rep
Dr Jo Puleston Consultant Gastroenterologist/ co-opted member
CMFT -
Dr Sajjad Mahmood
Consultant Gastroenterologist PAT Rep
Debbie Clark Clinical Nurse Specialist CMFT Deputy
Aileen Aherne Regional Jaundice CNS CMFT
Gary Morris Prehabilitation Physiotherapist CMFT AHP rep
Neil Bibby Prehabilitation Dietitian CMFT AHP rep
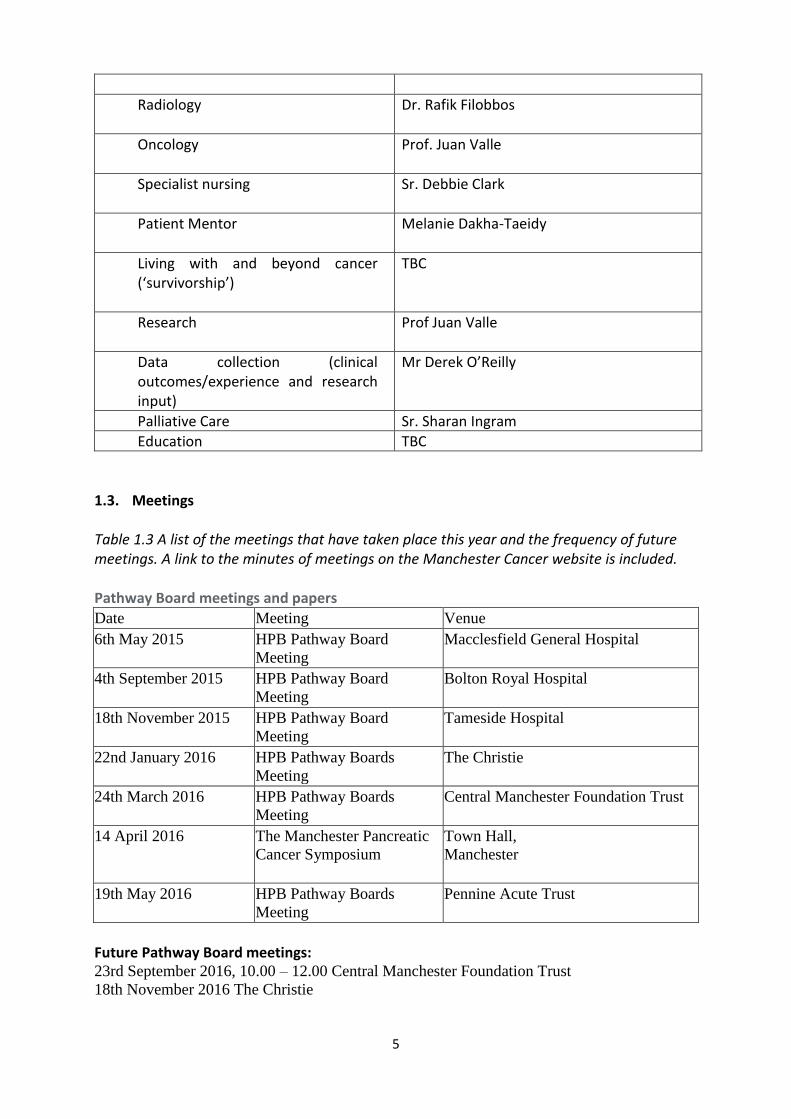
Table 1.2 Individuals who have been appointed as lead for research, education, early diagnosis, living with and beyond cancer, palliative care, etc.
Early diagnosis
Vicki Stevenson-Hornby
Pathology
TBC
Surgery Prof. Ajith Siriwardena
5
Radiology
Dr. Rafik Filobbos
Oncology
Prof. Juan Valle
Specialist nursing
Sr. Debbie Clark
Patient Mentor
Melanie Dakha-Taeidy
Living with and beyond cancer (‘survivorship’)
TBC
Research
Prof Juan Valle
Data collection (clinical outcomes/experience and research input)
Mr Derek O’Reilly
Palliative Care Sr. Sharan Ingram
Education TBC
1.3. Meetings Table 1.3 A list of the meetings that have taken place this year and the frequency of future meetings. A link to the minutes of meetings on the Manchester Cancer website is included. Pathway Board meetings and papers
Date Meeting Venue
6th May 2015 HPB Pathway Board
Meeting
Macclesfield General Hospital
4th September 2015 HPB Pathway Board
Meeting
Bolton Royal Hospital
18th November 2015 HPB Pathway Board
Meeting
Tameside Hospital
22nd January 2016 HPB Pathway Boards
Meeting
The Christie
24th March 2016 HPB Pathway Boards
Meeting
Central Manchester Foundation Trust
14 April 2016
The Manchester Pancreatic
Cancer Symposium
Town Hall,
Manchester
19th May 2016 HPB Pathway Boards
Meeting
Pennine Acute Trust
Future Pathway Board meetings: 23rd September 2016, 10.00 – 12.00 Central Manchester Foundation Trust
18th November 2016 The Christie
6
1-2 December 2016 The Pancreatic Society of Gt.Britain and Ireland Annual meeting, Hilton
Hotel, Manchester
24th Jan 2017, 14.00 -16.00: Wigan Infirmary The record of the attendance at each meeting to-date is in Appendix 1. The HPB Board have embraced the principle of wider engagement and educational meetings. HPB Pathway Board meetings take place at two monthly intervals at each of the ten participating Trusts, with the additional feature of a wider meeting/educational event for the benefit of the local MDT. Table 1.4 Educational events organised by the HPB Pathway Board.
Date Venue Speakers & Lecture
06th May 2015 Macclesfield 1. “HPB Services and Strategy in the Manchester Cancer Region” Mr. Derek O’Reilly, 2. “Improving Outcomes in Pancreatic Cancer” Prof. Juan Valle, Professor of Medical Oncology, Christie Hospital.
18.11.2015 Lecture theatre, Werneth House, Tameside Hospital
1. “HPB Services and Strategy in the Manchester Cancer Region” Mr. Derek O’Reilly, HPB Pathway Clinical Director, Manchester Cancer 2.“An Insight into HCC: Past, Present & Future” Dr Vinod Patel, Consultant Gastroenterologist, Tameside Hospital
18.11.2015 The Nowgen Centre, 29 Grafton Street, Manchester
A CMFT HPB Unit and Manchester Cancer Research Event Guest Speaker: Andrew G Renehan PhD FRCS Professor of Cancer Studies and Surgery Manchester Academic Health Science Centre “Obesity & HPB Cancers” See appendix 2
14 April 2016
Town Hall, Manchester
The Manchester Pancreatic Cancer Symposium 2016 – see appendix 3
7

8
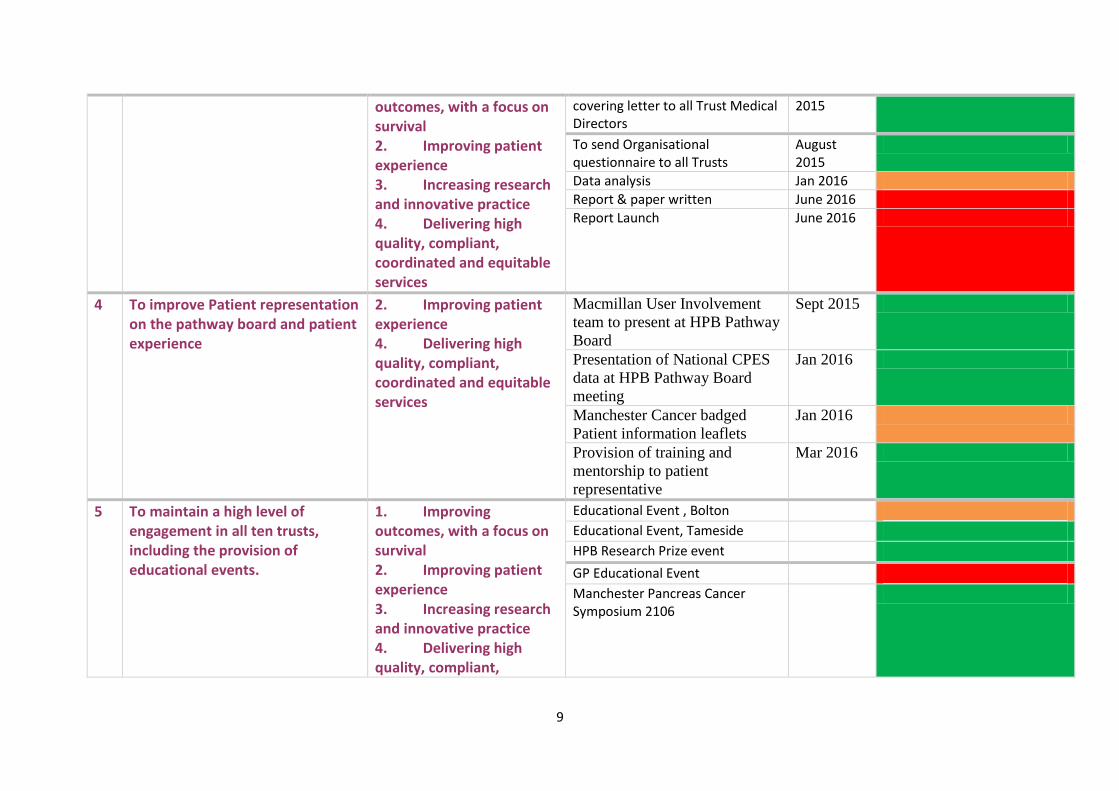
2. Summary of delivery against 2014/15 plan
No Objective Alignment with Provider Board objectives
Tasks By Status Green = achieved Amber = partially achieved Red = not achieved
1 Implement a regional jaundice pathway
1. Improving outcomes, with a focus on survival 2. Improving patient experience 3. Increasing research and innovative practice 4. Delivering high quality, compliant, coordinated and equitable services
Recruitment of Jaundice CNS August 2015
Recruitment of data collector August 2015
Establish on-going funding commitments from local commissioners
Feb 2016
Establishment of fast track pancreatic surgery at CMFT
Mar 2016
Establishment of further one-stop diagnostic sites
Mar 2016
Data analysis and completion of initial report
July 2016
2 To implement a Prehabilitation Programme: Nutritional Exercise and Psychological Assessment & Support.
1. Improving outcomes, with a focus on survival 2. Improving patient experience 3. Increasing research and innovative practice 4. Delivering high quality, compliant, coordinated and equitable services
To establish funding for additional personnel (Physio, dietician) To establish a Prehabilitation programme at CMFT To ensure elements of the program continue into LW&BC phase Initial data collection and analysis in annual report
Nov 2015 Feb 2016 July 2016 July 2016
3 To conduct a regional EUS audit 1. Improving To send EUS document and August
9
outcomes, with a focus on survival 2. Improving patient experience 3. Increasing research and innovative practice 4. Delivering high quality, compliant, coordinated and equitable services
covering letter to all Trust Medical Directors
2015
To send Organisational questionnaire to all Trusts
August 2015
Data analysis Jan 2016
Report & paper written June 2016
Report Launch June 2016
4 To improve Patient representation on the pathway board and patient experience
2. Improving patient experience 4. Delivering high quality, compliant, coordinated and equitable services
Macmillan User Involvement
team to present at HPB Pathway
Board
Sept 2015
Presentation of National CPES
data at HPB Pathway Board
meeting
Jan 2016
Manchester Cancer badged
Patient information leaflets
Jan 2016
Provision of training and
mentorship to patient
representative
Mar 2016
5 To maintain a high level of engagement in all ten trusts, including the provision of educational events.
1. Improving outcomes, with a focus on survival 2. Improving patient experience 3. Increasing research and innovative practice 4. Delivering high quality, compliant,
Educational Event , Bolton Educational Event, Tameside HPB Research Prize event
GP Educational Event Manchester Pancreas Cancer Symposium 2106
10
coordinated and equitable services
11
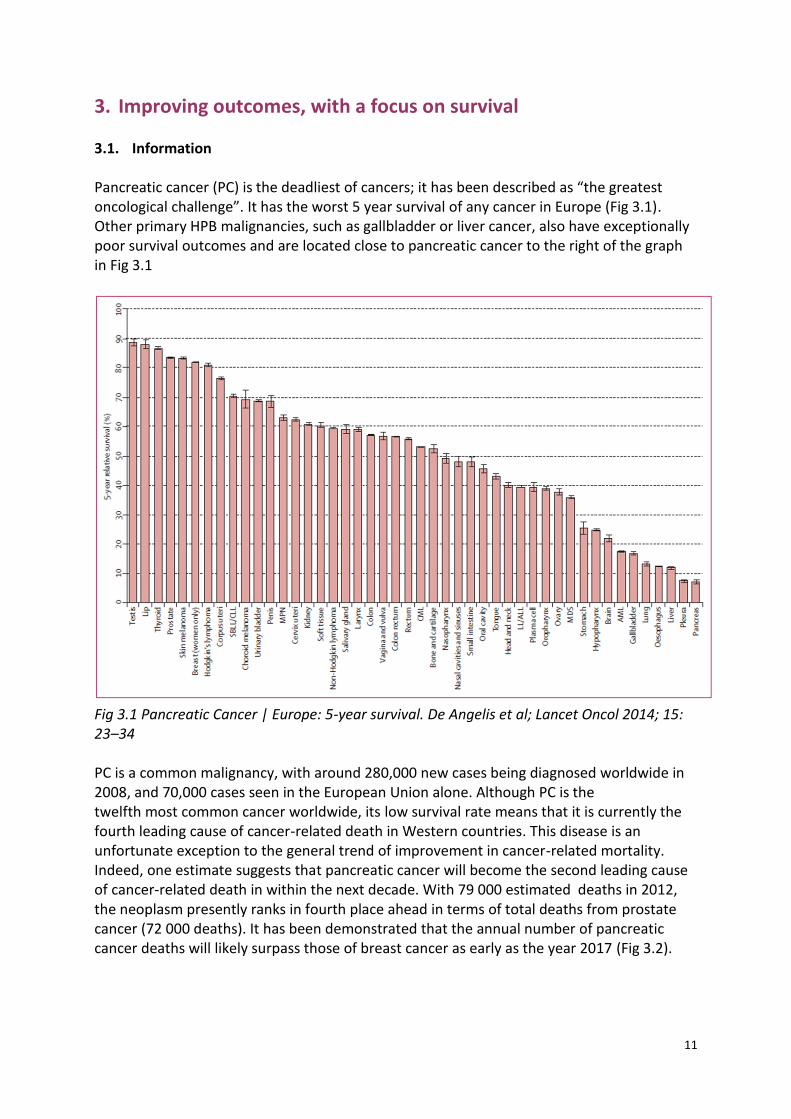
3. Improving outcomes, with a focus on survival 3.1. Information Pancreatic cancer (PC) is the deadliest of cancers; it has been described as “the greatest oncological challenge”. It has the worst 5 year survival of any cancer in Europe (Fig 3.1). Other primary HPB malignancies, such as gallbladder or liver cancer, also have exceptionally poor survival outcomes and are located close to pancreatic cancer to the right of the graph in Fig 3.1
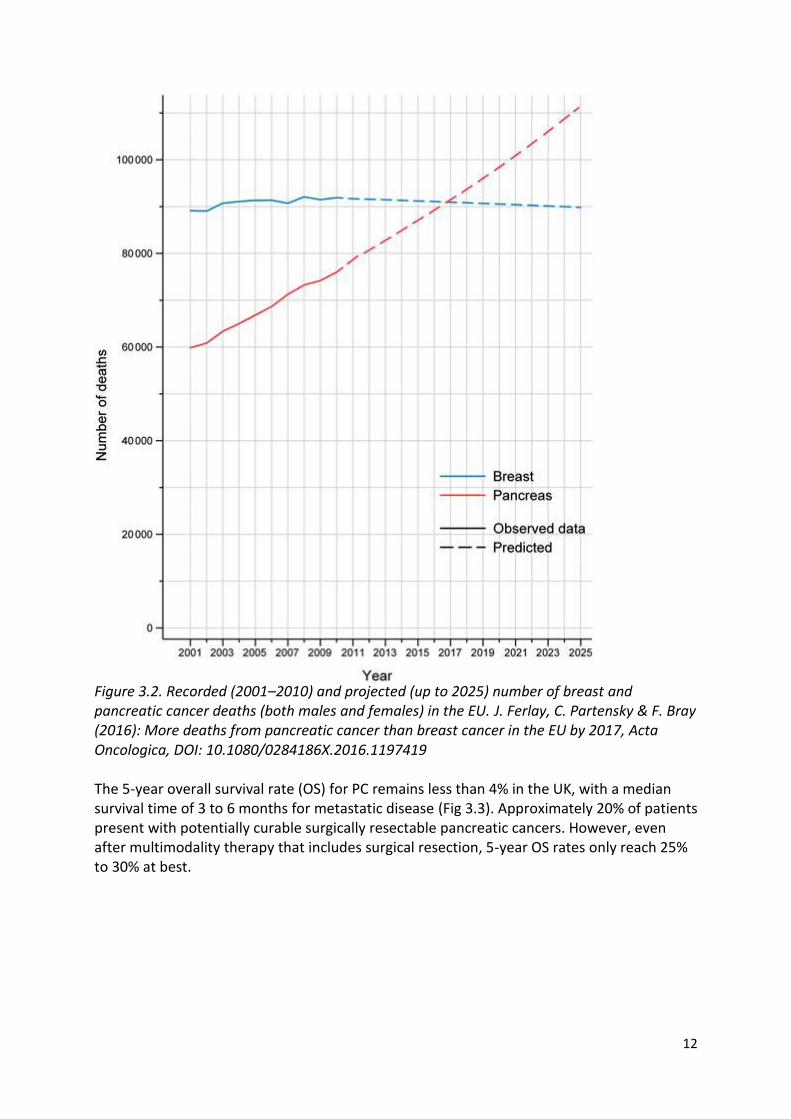
Fig 3.1 Pancreatic Cancer | Europe: 5-year survival. De Angelis et al; Lancet Oncol 2014; 15: 23–34 PC is a common malignancy, with around 280,000 new cases being diagnosed worldwide in 2008, and 70,000 cases seen in the European Union alone. Although PC is the twelfth most common cancer worldwide, its low survival rate means that it is currently the fourth leading cause of cancer-related death in Western countries. This disease is an unfortunate exception to the general trend of improvement in cancer-related mortality. Indeed, one estimate suggests that pancreatic cancer will become the second leading cause of cancer-related death in within the next decade. With 79 000 estimated deaths in 2012, the neoplasm presently ranks in fourth place ahead in terms of total deaths from prostate cancer (72 000 deaths). It has been demonstrated that the annual number of pancreatic cancer deaths will likely surpass those of breast cancer as early as the year 2017 (Fig 3.2).
12
Figure 3.2. Recorded (2001–2010) and projected (up to 2025) number of breast and pancreatic cancer deaths (both males and females) in the EU. J. Ferlay, C. Partensky & F. Bray (2016): More deaths from pancreatic cancer than breast cancer in the EU by 2017, Acta Oncologica, DOI: 10.1080/0284186X.2016.1197419 The 5-year overall survival rate (OS) for PC remains less than 4% in the UK, with a median survival time of 3 to 6 months for metastatic disease (Fig 3.3). Approximately 20% of patients present with potentially curable surgically resectable pancreatic cancers. However, even after multimodality therapy that includes surgical resection, 5-year OS rates only reach 25% to 30% at best.
13
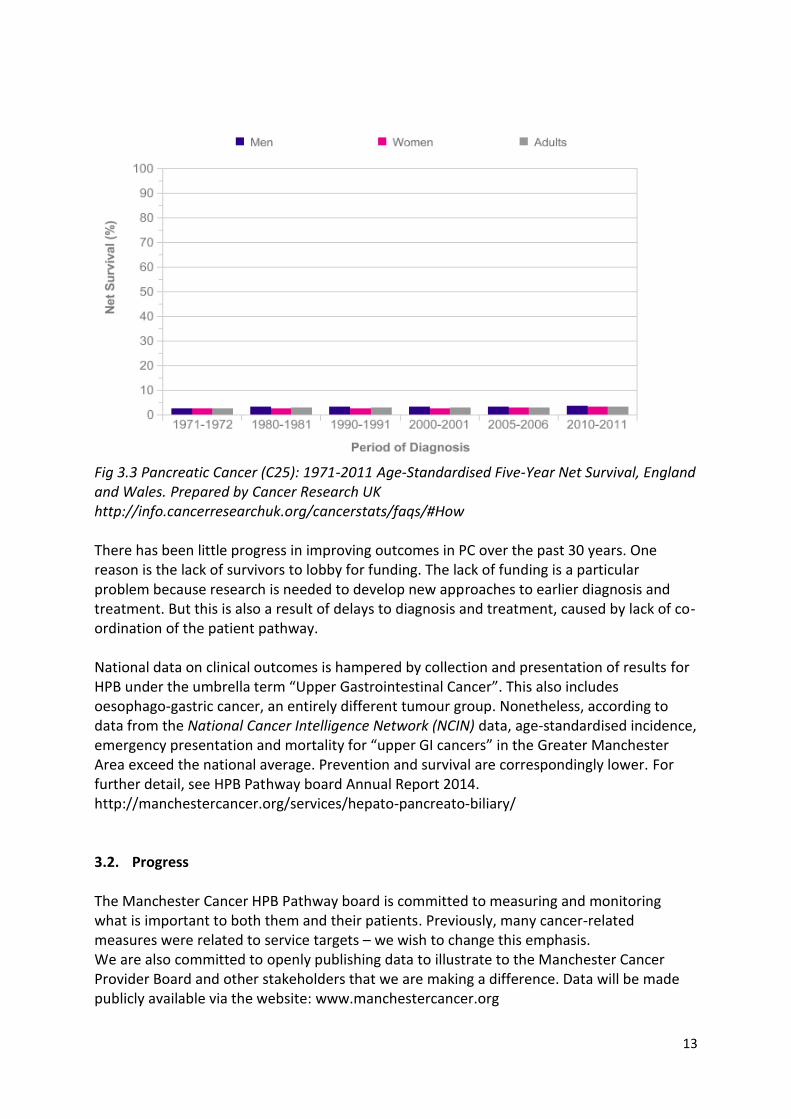
Fig 3.3 Pancreatic Cancer (C25): 1971-2011 Age-Standardised Five-Year Net Survival, England and Wales. Prepared by Cancer Research UK http://info.cancerresearchuk.org/cancerstats/faqs/#How There has been little progress in improving outcomes in PC over the past 30 years. One reason is the lack of survivors to lobby for funding. The lack of funding is a particular problem because research is needed to develop new approaches to earlier diagnosis and treatment. But this is also a result of delays to diagnosis and treatment, caused by lack of co-ordination of the patient pathway. National data on clinical outcomes is hampered by collection and presentation of results for HPB under the umbrella term “Upper Gastrointestinal Cancer”. This also includes oesophago-gastric cancer, an entirely different tumour group. Nonetheless, according to data from the National Cancer Intelligence Network (NCIN) data, age-standardised incidence, emergency presentation and mortality for “upper GI cancers” in the Greater Manchester Area exceed the national average. Prevention and survival are correspondingly lower. For further detail, see HPB Pathway board Annual Report 2014. http://manchestercancer.org/services/hepato-pancreato-biliary/ 3.2. Progress The Manchester Cancer HPB Pathway board is committed to measuring and monitoring what is important to both them and their patients. Previously, many cancer-related measures were related to service targets – we wish to change this emphasis. We are also committed to openly publishing data to illustrate to the Manchester Cancer Provider Board and other stakeholders that we are making a difference. Data will be made publicly available via the website: www.manchestercancer.org
14
The HPB Pathway Board has agreed a small number of meaningful measures that it will monitor closely. This set of measures will cover the whole cancer pathway, including where appropriate, measures for early diagnosis, patient experience and survivorship as well as the treatment phase of the pathway. Core measures include:
Percentage of cancers diagnosed by stage
Percentage of cancers diagnosed as emergencies
Resection rates
Operative morbidity and mortality
Cancer survival (at 1, 3 and 5 years)
measures of patient satisfaction
the research involvement of patients CMFT HPB SMDT WORKLOAD The HPB MDT takes place each Wednesday morning at 8am. The cut off point for referring any patient to the MDT is 1pm on a Monday; this is to allow for sufficient time for clinicians / MDT co-ordinators to review the imaging or pathology and to prepare the agenda. A web-based electronic referral proforma (ERP) has been developed and is accessible from each referring Trust at: https://cmftreferrals.cmft.nhs.uk/ All new HPB cancer patients are reviewed by the HPB sMDT for discussion of initial treatment plan. Urgent cases can also be discussed outside of the MDT meeting, through the on-call HPB surgeon. The local referral/diagnostic teams are the local Upper GI and Colorectal Multidisciplinary teams at:
Bolton NHS Foundation Trust
Central Manchester University Hospitals NHS Foundation Trust
East Cheshire NHS Trust
Pennine Acute NHS Trust
Salford Royal NHS Foundation Trust
Stockport NHS Foundation Trust
Tameside Hospital NHS Foundation Trust
The Christie NHS Foundation Trust
University Hospital of South Manchester NHS Foundation Trust;
Wrightington, Wigan and Leigh NHS Foundation Trust Urgent cases can be discussed outside of the formal MDT, however in this case the following protocol is to be followed:
15
Telephone discussion between the relevant treating consultant or their deputy and another SMDT surgeon/clinical oncologist/medical oncologist. This discussion to include all available radiology and pathology evidence.
Formal written letter to follow telephone discussion as a permanent record.
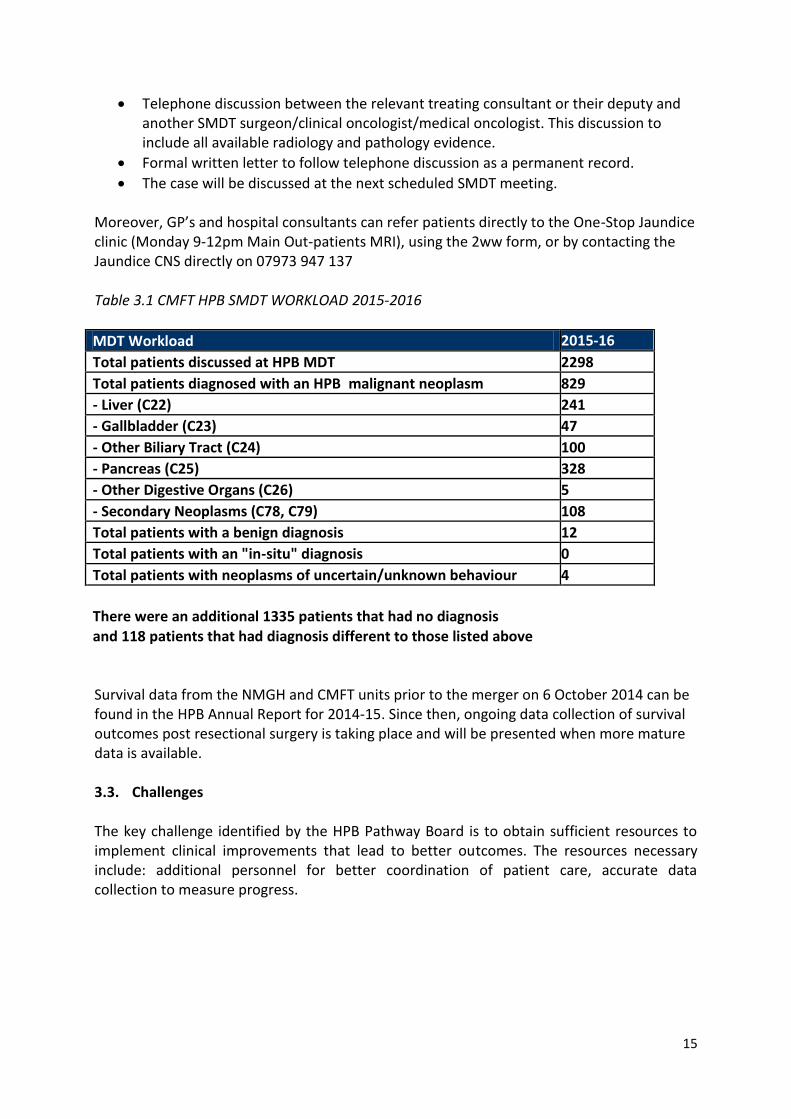
The case will be discussed at the next scheduled SMDT meeting. Moreover, GP’s and hospital consultants can refer patients directly to the One-Stop Jaundice clinic (Monday 9-12pm Main Out-patients MRI), using the 2ww form, or by contacting the Jaundice CNS directly on 07973 947 137 Table 3.1 CMFT HPB SMDT WORKLOAD 2015-2016
MDT Workload 2015-16
Total patients discussed at HPB MDT 2298
Total patients diagnosed with an HPB malignant neoplasm 829
- Liver (C22) 241
- Gallbladder (C23) 47
- Other Biliary Tract (C24) 100
- Pancreas (C25) 328
- Other Digestive Organs (C26) 5
- Secondary Neoplasms (C78, C79) 108
Total patients with a benign diagnosis 12
Total patients with an "in-situ" diagnosis 0
Total patients with neoplasms of uncertain/unknown behaviour 4
There were an additional 1335 patients that had no diagnosis
and 118 patients that had diagnosis different to those listed above Survival data from the NMGH and CMFT units prior to the merger on 6 October 2014 can be found in the HPB Annual Report for 2014-15. Since then, ongoing data collection of survival outcomes post resectional surgery is taking place and will be presented when more mature data is available. 3.3. Challenges The key challenge identified by the HPB Pathway Board is to obtain sufficient resources to implement clinical improvements that lead to better outcomes. The resources necessary include: additional personnel for better coordination of patient care, accurate data collection to measure progress.
16
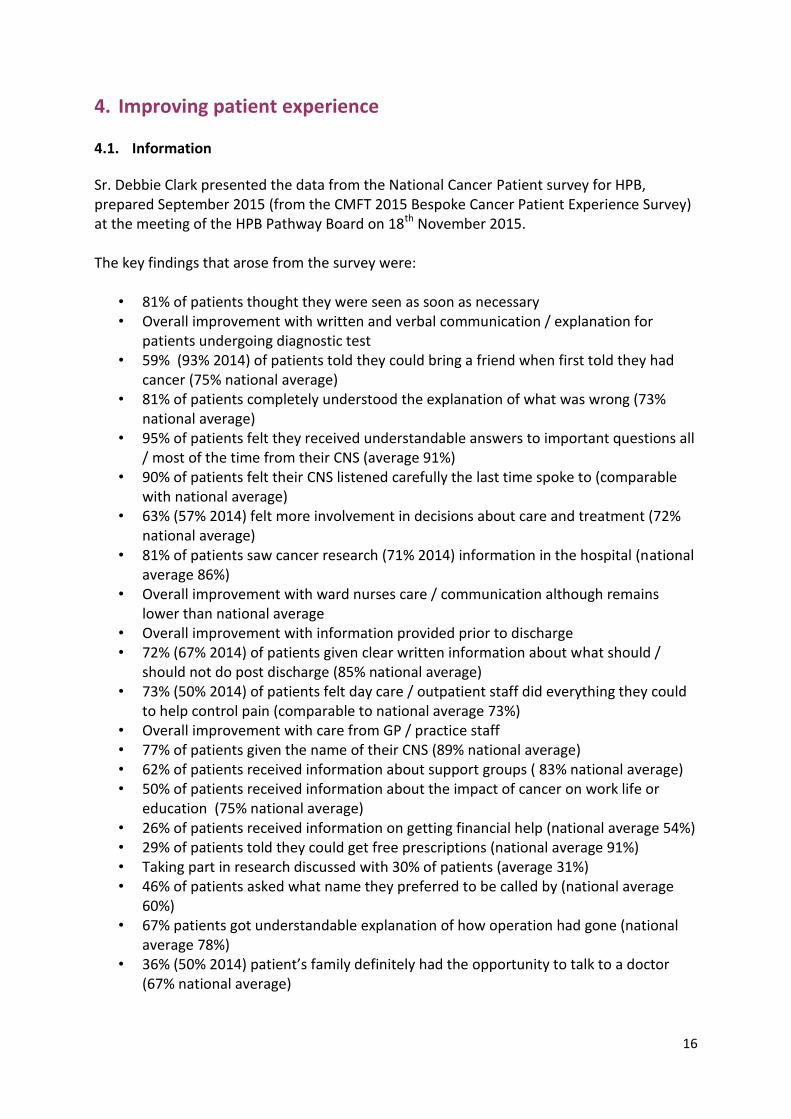
4. Improving patient experience 4.1. Information Sr. Debbie Clark presented the data from the National Cancer Patient survey for HPB, prepared September 2015 (from the CMFT 2015 Bespoke Cancer Patient Experience Survey) at the meeting of the HPB Pathway Board on 18th November 2015. The key findings that arose from the survey were:
• 81% of patients thought they were seen as soon as necessary • Overall improvement with written and verbal communication / explanation for
patients undergoing diagnostic test • 59% (93% 2014) of patients told they could bring a friend when first told they had
cancer (75% national average) • 81% of patients completely understood the explanation of what was wrong (73%
national average) • 95% of patients felt they received understandable answers to important questions all
/ most of the time from their CNS (average 91%) • 90% of patients felt their CNS listened carefully the last time spoke to (comparable
with national average) • 63% (57% 2014) felt more involvement in decisions about care and treatment (72%
national average) • 81% of patients saw cancer research (71% 2014) information in the hospital (national
average 86%) • Overall improvement with ward nurses care / communication although remains
lower than national average • Overall improvement with information provided prior to discharge • 72% (67% 2014) of patients given clear written information about what should /
should not do post discharge (85% national average) • 73% (50% 2014) of patients felt day care / outpatient staff did everything they could
to help control pain (comparable to national average 73%) • Overall improvement with care from GP / practice staff • 77% of patients given the name of their CNS (89% national average) • 62% of patients received information about support groups ( 83% national average) • 50% of patients received information about the impact of cancer on work life or
education (75% national average) • 26% of patients received information on getting financial help (national average 54%) • 29% of patients told they could get free prescriptions (national average 91%) • Taking part in research discussed with 30% of patients (average 31%) • 46% of patients asked what name they preferred to be called by (national average
60%) • 67% patients got understandable explanation of how operation had gone (national
average 78%) • 36% (50% 2014) patient’s family definitely had the opportunity to talk to a doctor
(67% national average)
17
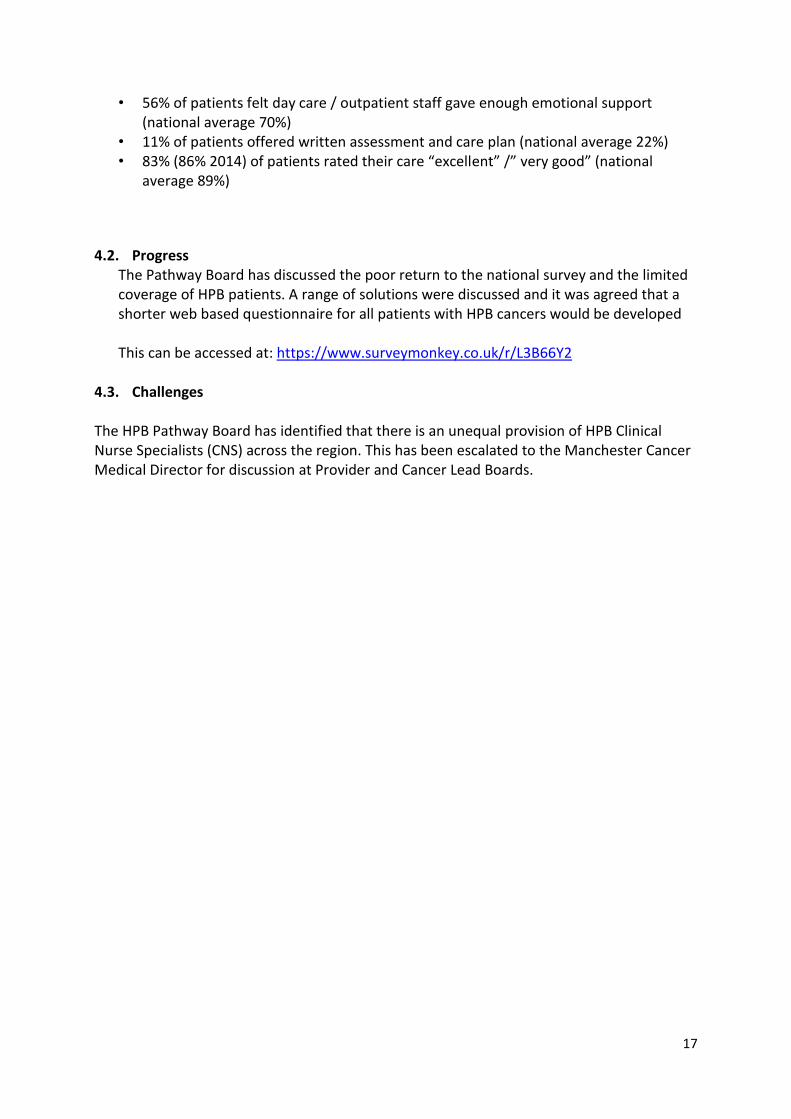
• 56% of patients felt day care / outpatient staff gave enough emotional support (national average 70%)
• 11% of patients offered written assessment and care plan (national average 22%) • 83% (86% 2014) of patients rated their care “excellent” /” very good” (national
average 89%)
4.2. Progress The Pathway Board has discussed the poor return to the national survey and the limited coverage of HPB patients. A range of solutions were discussed and it was agreed that a shorter web based questionnaire for all patients with HPB cancers would be developed This can be accessed at: https://www.surveymonkey.co.uk/r/L3B66Y2
4.3. Challenges The HPB Pathway Board has identified that there is an unequal provision of HPB Clinical Nurse Specialists (CNS) across the region. This has been escalated to the Manchester Cancer Medical Director for discussion at Provider and Cancer Lead Boards.
18
5. Increasing research and innovative practice
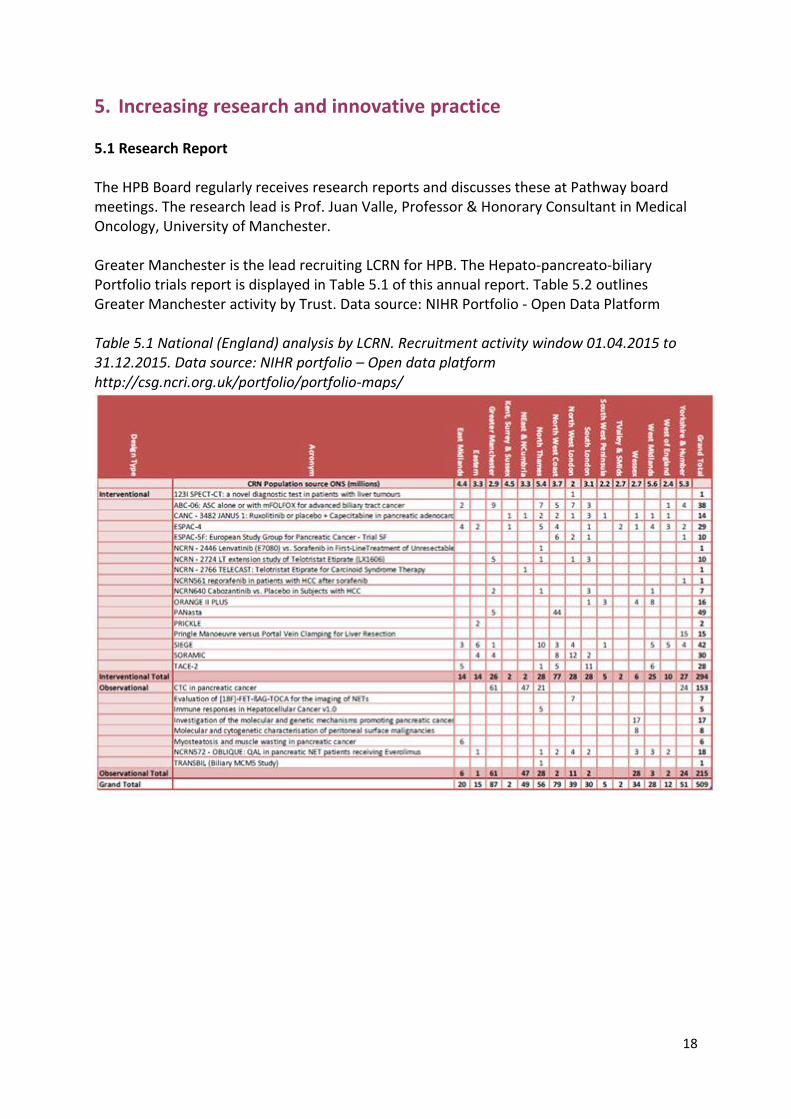
5.1 Research Report The HPB Board regularly receives research reports and discusses these at Pathway board meetings. The research lead is Prof. Juan Valle, Professor & Honorary Consultant in Medical Oncology, University of Manchester. Greater Manchester is the lead recruiting LCRN for HPB. The Hepato-pancreato-biliary Portfolio trials report is displayed in Table 5.1 of this annual report. Table 5.2 outlines Greater Manchester activity by Trust. Data source: NIHR Portfolio - Open Data Platform Table 5.1 National (England) analysis by LCRN. Recruitment activity window 01.04.2015 to 31.12.2015. Data source: NIHR portfolio – Open data platform http://csg.ncri.org.uk/portfolio/portfolio-maps/
19
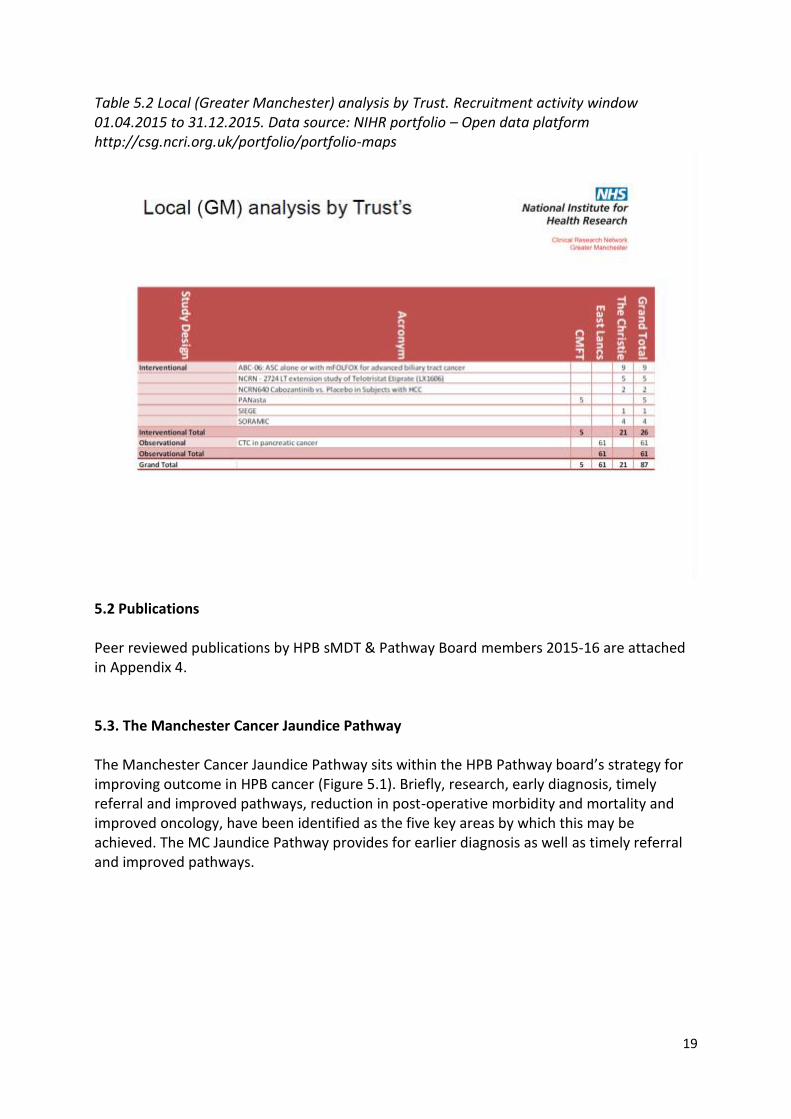
Table 5.2 Local (Greater Manchester) analysis by Trust. Recruitment activity window 01.04.2015 to 31.12.2015. Data source: NIHR portfolio – Open data platform http://csg.ncri.org.uk/portfolio/portfolio-maps
5.2 Publications Peer reviewed publications by HPB sMDT & Pathway Board members 2015-16 are attached in Appendix 4. 5.3. The Manchester Cancer Jaundice Pathway The Manchester Cancer Jaundice Pathway sits within the HPB Pathway board’s strategy for improving outcome in HPB cancer (Figure 5.1). Briefly, research, early diagnosis, timely referral and improved pathways, reduction in post-operative morbidity and mortality and improved oncology, have been identified as the five key areas by which this may be achieved. The MC Jaundice Pathway provides for earlier diagnosis as well as timely referral and improved pathways.

20
Figure 5.1. Manchester Cancer Strategy for improving outcomes in HPB cancer
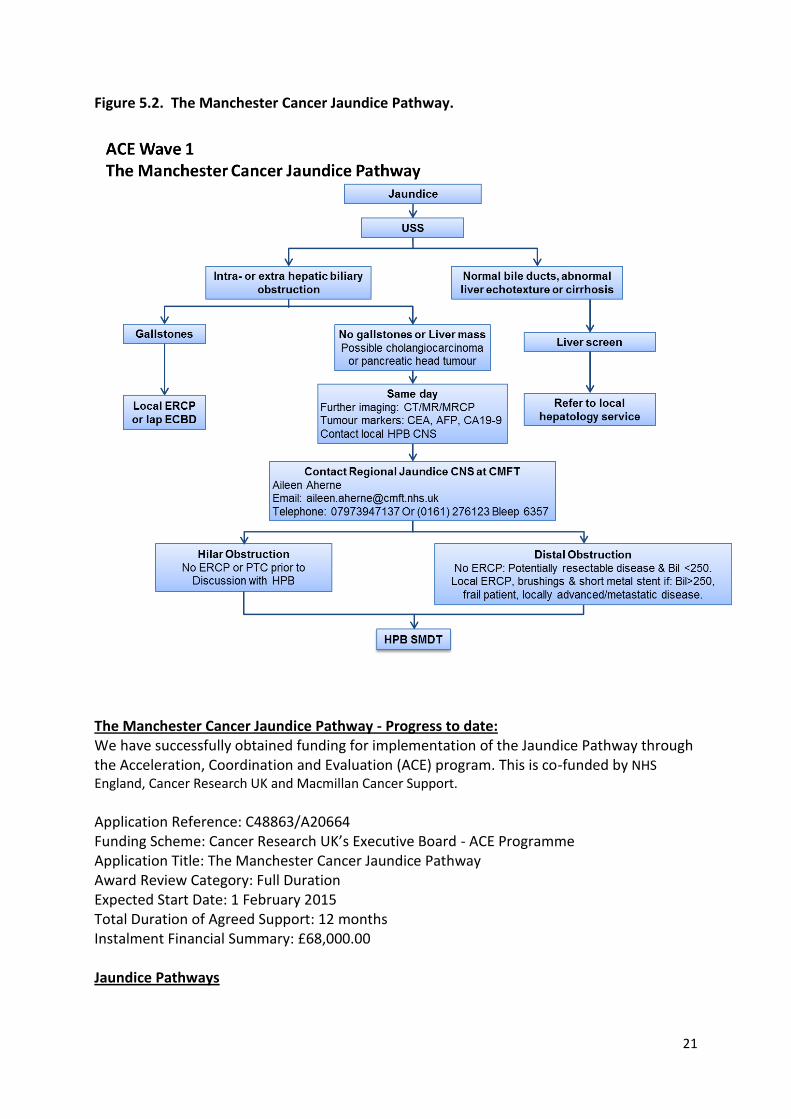
The MC Jaundice Pathway provides for earlier diagnosis as well as timely referral and improved pathways (Figure 5.2). The key innovations are twofold:
1. Same day definitive radiological imaging for patients presenting with obstructive jaundice not due to gallstones. The purpose is to provide for earlier diagnosis and timely referral and to improve patient experience.
2. Fast-track referral for jaundiced patients with pancreatic cancer for early
surgery. The aim is to reduce overall complications and prolong survival.
21
Figure 5.2. The Manchester Cancer Jaundice Pathway.
The Manchester Cancer Jaundice Pathway - Progress to date: We have successfully obtained funding for implementation of the Jaundice Pathway through the Acceleration, Coordination and Evaluation (ACE) program. This is co-funded by NHS England, Cancer Research UK and Macmillan Cancer Support.
Application Reference: C48863/A20664 Funding Scheme: Cancer Research UK’s Executive Board - ACE Programme Application Title: The Manchester Cancer Jaundice Pathway Award Review Category: Full Duration Expected Start Date: 1 February 2015 Total Duration of Agreed Support: 12 months Instalment Financial Summary: £68,000.00 Jaundice Pathways

22
Data from the initial site (Macclesfield General Hospital) to provide a one-stop diagnostic service for jaundiced patients was presented at the Manchester Cancer HPB Pathway Board meeting on 6 May 2015. Of 28 patients referred, 7 had a diagnosis of cancer. All had completion of investigation within 2 weeks. Similar pathways have now been established at PAT and CMFT (Figure 5.3). Fast track Surgery Number of Referrals: 26 Number proceeding to Surgery: 9 Number not having fast track surgery: 17 Table 5.3 Reasons patients did not undergo fast track surgery
Stone disease 1
Bilirubin excessively elevated
(>250) 3
Comorbidity preventing Fast track 3
Uncertainty of diagnosis 3
Advanced disease 5
Psychological well being 1
Failed to follow pathway 1
Patient experience of the Jaundice Pathway This is on-going using the ACE Survey Monkey tool to monitor patient experience. In addition, the CMFT Quality Team undertaking ‘patient stories’ to evaluate patient experience. Some patient experiences are quoted as follows: “….the waiting times and timescales for appointments and referrals and subsequent surgery
had been fantastic and he could not have asked for better treatment.” “….over the moon with the care and treatment I received”
“….I could have paid privately but would not have got better care”

23
Figure 5.3 The CMFT One-Stop Jaundice Clinic

24
5.4 The Manchester Cancer Prehabilitation Program The HPB Pathway Board successfully obtained a grant from Macmillan to commence our prehabilitation programme. This was “An Integrated program of Nutritional support; Exercise and improved general well-being; and Screening for anxiety and depression, right across the four phases of: Prehabilitation, Enhanced recovery, Recovery/reablement and Living with and beyond cancer”. Since 01.04.2016, all new patients being considered for cancer resectional surgery are seen in a prehabilitation clinic at first hospital consultation, prior to commencement of planned treatment. Patients with HPB cancer who are about to undergo surgery have a comprehensive prehabilitation programme, providing:
A structured exercise regimen – supported by the use of the international physical activity questionnaire (IPAQ)
Nutritional assessment and food diaries
Management of malnutrition caused by exocrine failure in pancreatic cancer
Physiotherapy advice
Psychological support (including for smoking and alcohol dependency) Figure 5.3: overview of the integrated programme of exercise and wellbeing, nutritional support and screening for anxiety and depression

25
5.1. Challenges Research and Innovation is strength of the HPB Pathway board with a strong track record of leadership in academic activities: exceeding trial recruitment targets; high impact peer-reviewed publications; and the introduction of innovative treatments. The challenges for the next year are:
1. To increase recruitment to clinical trials and observational studies 2. To obtain high impact peer reviewed publications 3. To fully implement the Jaundice Pathway in as many trusts within the region as
possible 4. Above all, to obtain on-going funding for our innovative jaundice and prehabilitation
programmes once the pilot study funding expires.
26
6. Delivering complaint and high quality services 6.1. Information Since October 6, 2014, a single IOG compliant HPB Service has been located at the Manchester Royal Infirmary, Central Manchester NHS Foundation Trust (CMFT). This is the result of the merger of the two previous HPB Units at the MRI and North Manchester General Hospital, Pennine Acute Trust. This is now a well-established and successful unit. The new merged single HPB multidisciplinary team (sMDT) and the HPB Pathway Board has been designed to be meet: • NICE Cancer Service Guidance “Improving Outcomes of Upper GI Cancers” • The NHS Commissioning Board Specialised Services Specification • The NHS Greater Manchester Framework Commissioning Specification “The Delivery of ‘World Class’ Specialist Cancer Surgery Services in the Greater Manchester and Cheshire Cancer System.” • NHS England National Peer Review Programme Manual for Cancer Services. Manchester Cancer is an integrated cancer system for Greater Manchester and East Cheshire. The Hepato-Pancreato-Biliary (HPB) Pathway Board includes active representation for all ten trusts in Greater Manchester and Cheshire that comprise Manchester Cancer. A full description of the HPB sMDT membership and service may be found in the CMFT HPB MDT Operational Policy document. 6.2. Progress
The Manchester Cancer Hepato-Pancreato-Biliary (HPB) Pathway Board meets regularly and has active representation from all ten trusts in Greater Manchester and Cheshire; primary care; and patient representation.
The Jaundice Pathway has now been implemented, funded by the “Acceleration, Coordination and Evaluation (ACE)” programme. This provides for a regional jaundice clinical nurse specialist (Aileen Aherne) and a data co-ordinator (Karen Ridyard), to implement one-stop clinics and fast-track surgery (see Section 5.3).
A Prehabilitation dietitian (Neil Bibby) and physiotherapist (Gary Morris) have been appointed to optimise patients’ fitness prior to surgery. This project has been funded by Macmillan (see Section 5.4).
The HPB Quality Improvement programme, a system for recording, analysing and reducing post-operative morbidity and mortality, has become an established part of the weekly activity. Our first year data was presented as a poster at the Pancreatic Society of Great Britain & Ireland Annual Scientific meeting, Norwich, 26-27 November 2015.
The unit is participating in the following NIHR badged clinical trials that have opened in the past year: PANasta; ESPAC-5F.
27
Prof. Ajith Siriwardena was elected President of the Pancreatic Society of Great Britain & Ireland and will host their annual scientific meeting in Manchester on 1-2 December 2016.
Mr Derek O’Reilly was appointed as the NCEPOD Clinical Co-coordinator for surgery and as a member of the NICE Clinical Guidelines Committee for pancreatic cancer.
Figure 6. New members of the HPB Pathway Board, thanks to funding obtained by the HPB Pathway board, from the ACE programme and Macmillan Cancer. From left to right: Gary Morris (Prehabilitation physiotherapist), Aileen Aherne (Regional Jaundice CNS) and Neil Bibby (Prehabilitation dietitian).
6.3. Challenges The key challenge identified by the HPB Pathway Board is to obtain sufficient resources to implement clinical improvements that lead to better outcomes. The resources necessary include: additional personnel for better coordination of patient care, accurate data collection to measure progress. Despite the current financially challenging environment for the NHS, the HPB Pathway Board is well placed to benefit from increased emphasis on to improving efficiency and eliminating waste, centralisation of complex services and the development of cancer networks and alliances. Our goals for clinical and academic development all fit with the strategic objectives of Central Manchester Foundation Trust and Manchester Cancer and will enable us to take full advantage of the opportunities that this and the devolution of health services present.
28
7. Objectives for 2015/16
To fully implement a Regional Jaundice Pathway.
To implement a Prehabilitation Programme of Nutritional, Exercise and Psychological Assessment & Support
To improve patient experience
To maintain a high level of engagement in all ten trusts through the provision of educational events.
To maintain a high level of patient involvement in research and clinical trials For full details see the HPB Pathway Board’s full 2015/16 annual plan.
29
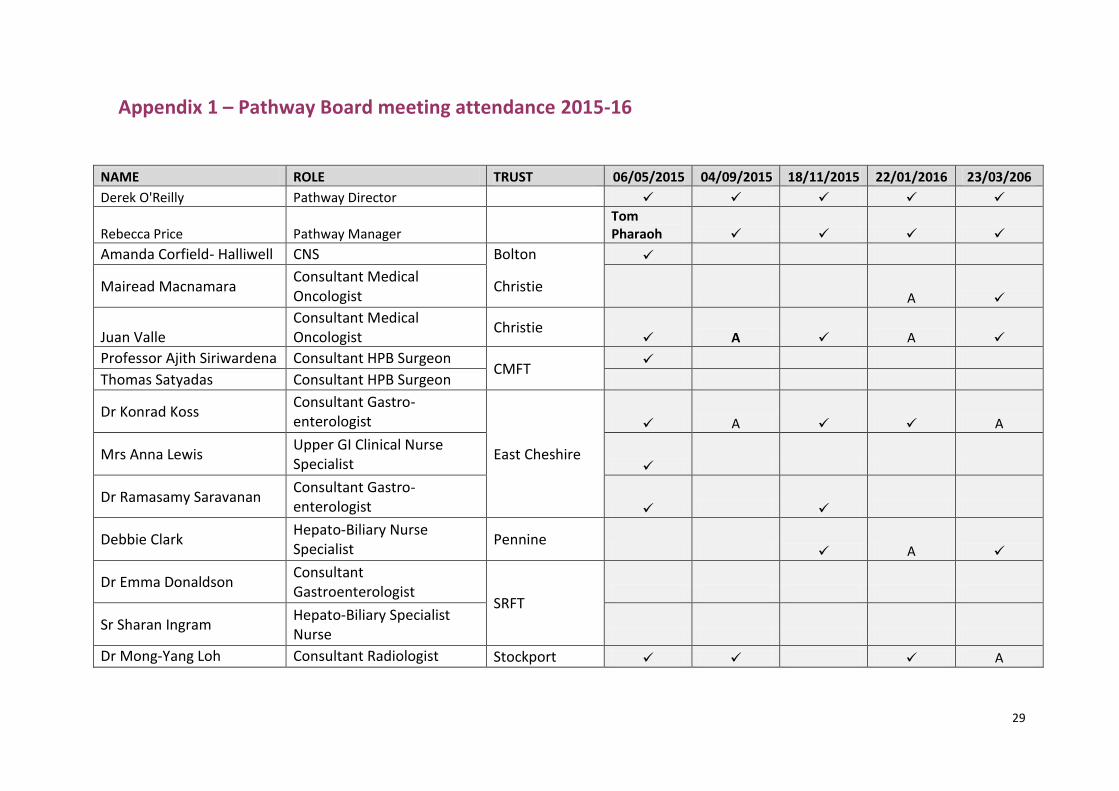
Appendix 1 – Pathway Board meeting attendance 2015-16
NAME ROLE TRUST 06/05/2015 04/09/2015 18/11/2015 22/01/2016 23/03/206
Derek O'Reilly Pathway Director
Rebecca Price Pathway Manager Tom Pharaoh
Amanda Corfield- Halliwell CNS Bolton
Mairead Macnamara Consultant Medical Oncologist
Christie A
Juan Valle Consultant Medical Oncologist
Christie A A
Professor Ajith Siriwardena Consultant HPB Surgeon CMFT
Thomas Satyadas Consultant HPB Surgeon
Dr Konrad Koss Consultant Gastro-enterologist
East Cheshire
A A
Mrs Anna Lewis Upper GI Clinical Nurse Specialist
Dr Ramasamy Saravanan Consultant Gastro-enterologist
Debbie Clark Hepato-Biliary Nurse Specialist
Pennine A
Dr Emma Donaldson Consultant Gastroenterologist
SRFT
Sr Sharan Ingram Hepato-Biliary Specialist Nurse
Dr Mong-Yang Loh Consultant Radiologist Stockport A
30
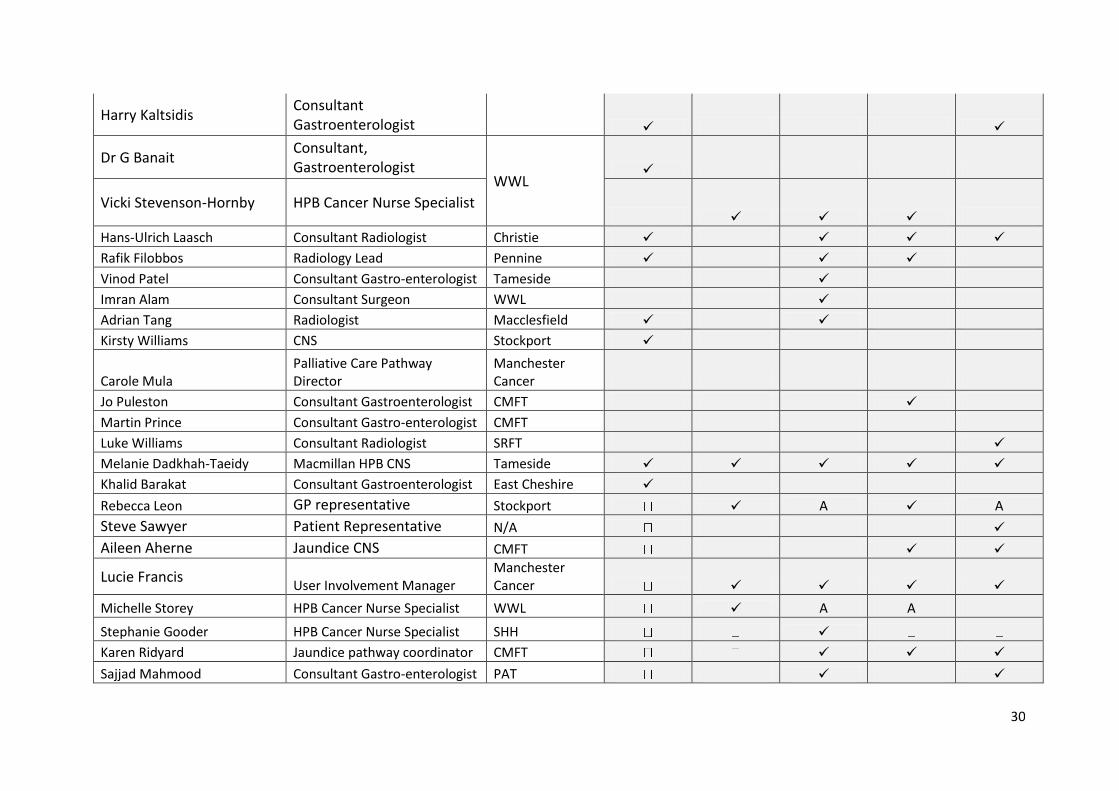
Harry Kaltsidis Consultant Gastroenterologist
Dr G Banait Consultant, Gastroenterologist
WWL
Vicki Stevenson-Hornby HPB Cancer Nurse Specialist
Hans-Ulrich Laasch Consultant Radiologist Christie
Rafik Filobbos Radiology Lead Pennine
Vinod Patel Consultant Gastro-enterologist Tameside
Imran Alam Consultant Surgeon WWL
Adrian Tang Radiologist Macclesfield
Kirsty Williams CNS Stockport
Carole Mula Palliative Care Pathway Director
Manchester Cancer
Jo Puleston Consultant Gastroenterologist CMFT
Martin Prince Consultant Gastro-enterologist CMFT
Luke Williams Consultant Radiologist SRFT
Melanie Dadkhah-Taeidy Macmillan HPB CNS Tameside
Khalid Barakat Consultant Gastroenterologist East Cheshire
Rebecca Leon GP representative Stockport A A
Steve Sawyer Patient Representative N/A
Aileen Aherne Jaundice CNS CMFT
Lucie Francis User Involvement Manager
Manchester Cancer
Michelle Storey HPB Cancer Nurse Specialist WWL A A
Stephanie Gooder HPB Cancer Nurse Specialist SHH
Karen Ridyard Jaundice pathway coordinator CMFT
Sajjad Mahmood Consultant Gastro-enterologist PAT
31
Saurabh Jamdar Consultant HPB surgeon CMFT
Neil Bibby Dietitian CMFT
Garry Morris Physiotherapist CMFT
32
Appendix 2
A CMFT HPB Unit and Manchester Cancer Research Event
Venue: The Nowgen Centre, 29 Grafton Street, Manchester, M13 9WU
Date & Time: Wednesday 18th November 2015,
17.30. Registration. Tea & Coffee
18:00 to 20:00: Research Presentations & Guest Speaker
followed by dinner at Ziya Restaurant, 65-67 Wilmslow Road , Manchester M14 5TB
Agenda: 8 x 7 mins presentations + 3 mins for questions
1. Angela Lamarca. Clinical biomarkers in patients with advanced hepatocellular carcinoma
(HCC) receiving sorafenib; a single institution experience.
2. Peter Coe. Intra-pancreatic fat reduction within the Breast Risk Reduction Intermittent
Dietary Evaluation-2 (BRRIDE-2) study
3. Minas Baltatzis. Antibiotic Use in Acute Pancreatitis: Global Overview of Compliance with
International Guidelines
4. Giorgio Allessandri. Structural Postoperative Assessment after HPB Surgical Resections
5. Anthony Chan. Colorectal Cancer with Synchronous Liver-Limited Metastases: A novel
Propensity Score to Stratify Patients to Sequence of Surgery
6. Grazia Saturno. Patient Derived Xenografts for Pancreatic Cancer
7. Raisah Sawati. A review of biliary drainage and stenting at MRI
8. Sumit Nandi. Use of gemcitabine-loaded superparamagnetic iron oxide nanoparticles against
pancreatic cancer cells
Guest Speaker:
Andrew G Renehan PhD FRCS Professor of Cancer Studies and Surgery
Manchester Academic Health Science Centre
“Obesity & HPB Cancers”

33
Appendix 3 – The Manchester Pancreatic Cancer Symposium 2016 Agenda
TIME
08.30 Registration Tea & Coffee
09.00 Mr. Derek O’Reilly
Introduction & Welcome
09.10 Ms Anna Jewell PCUK Setting the Scene: The experience of
Pancreatic Cancer in 2016
Chairs: Translational
Research
Dr Mairead
McNamara
(Manchester)
Professor Martin J. Humphries
(Manchester)
09.30 Dr. Ged Brady
CRUK Manchester Defining the role of CTCs & cfDNA in
Pancreatic Cancer
10.00 Prof. Eithne
Costello
Liverpool The prospects for Biomarkers and early
Diagnosis
10.30 Prof. Hemant
Kocher
London Tumour-Stromal interactions
11.00 COFFEE BREAK
Chairs: Nutrition,
Prehabilitation
and Enhanced
Recovery
Miss Ambareen
Kausar
(Blackburn)
Mr Keith Roberts (Birmingham)
11.30 Prof. Andrew
Renehan
Christie Sarcopaenia and Obesity in Pancreatic
Cancer
12.00 Mrs. Mary Phillips Guildford Nutritional Assessment and Support for
patients with Pancreatic Cancer
12.30 Mr. Derek O’Reilly CMFT Prehabilitation and Enhanced Recovery
for Pancreatic Surgery
13.00 LUNCH
Chairs: Innovations in
Treatment
Prof Jorg Kleef
(Liverpool)
Mr Saurabh Jamdar (Manchester)
14.00 Mr. Chris Halloran Liverpool The Use of Iron Oxide Nanoparticles for

34
Pancreatic Cancer Therapy
14.30 Dr. Krijn Van
Lienden
Amsterdam Irreversible electroporation for locally
advanced pancreatic cancer
15.00 Mr. Rahul
Deshpande
CMFT Innovations in Pancreatic Cancer Surgery
15.30 COFFEE BREAK
Chairs: Personalised
Medicine & Future
Directions
Mr Andy Smith
(Leeds)
Mr Nicola De’Liguori Carino (Manchester)
16.00 Prof. Juan Valle The Christie Clinical Trials in Pancreatic Cancer – Past,
Present & Future
16.30 Prof. Andrew
Biankin
Glasgow Precision Medicine in Pancreatic Cancer
17.00 Prof. John
Neoptolemos
Liverpool Prospects for Improved Outcomes in
Pancreatic Cancer
35
Appendix 4 - Peer reviewed publications by members of the HPB SMDT 2015-16 1: Ruszniewski P, Valle JW, Lombard-Bohas C, Cuthbertson DJ, Perros P, Holubec L, Delle Fave G, Smith D, Niccoli P, Maisonobe P, Atlan P, Caplin ME; SYMNET study group. Patient-reported outcomes with lanreotide Autogel/Depot for carcinoid syndrome: An international observational study. Dig Liver Dis. 2016May;48(5):552-8. 2: Bridgewater J, Lopes A, Beare S, Duggan M, Lee D, Ricamara M, McEntee D, Sukumaran A, Wasan H, Valle JW. A phase 1b study of Selumetinib in combination with Cisplatin and Gemcitabine in advanced or metastatic biliary tract cancer: the ABC-04 study. BMC Cancer. 2016 Feb 24;16(1):153. 3: Lamarca A, Elliott E, Barriuso J, Backen A, McNamara MG, Hubner R, Valle JW. Chemotherapy for advanced non-pancreatic well-differentiated neuroendocrine tumours of the gastrointestinal tract, a systematic review and meta-analysis: A lost cause? Cancer Treat Rev. 2016 Mar;44:26-41. 4: Lamarca A, Asselin MC, Manoharan P, McNamara MG, Trigonis I, Hubner R, Saleem A, Valle JW. (18)F-FLT PET imaging of cellular proliferation in pancreatic cancer. Crit Rev Oncol Hematol. 2016 Mar;99:158-69. 5: McNamara MG, Lamarca A, Hubner RA, Valle JW. "If You Prick Us, Do We Not Bleed?" Whom Should We Choose? J Clin Oncol. 2016 Feb 10;34(5):513-4. 6: Yao JC, Fazio N, Singh S, Buzzoni R, Carnaghi C, Wolin E, Tomasek J, Raderer M, Lahner H, Voi M, Pacaud LB, Rouyrre N, Sachs C, Valle JW, Delle Fave G, Van Cutsem E, Tesselaar M, Shimada Y, Oh DY, Strosberg J, Kulke MH, Pavel ME; RAD001 in Advanced Neuroendocrine Tumours, Fourth Trial (RADIANT-4) Study Group. Everolimus for the treatment of advanced, non-functional neuroendocrine tumours of the lung or gastrointestinal tract (RADIANT-4): a randomised, placebo-controlled, phase 3 study. Lancet. 2016 Mar 5;387(10022):968-77. 7: Monaghan PJ, Lamarca A, Valle JW, Hubner RA, Mansoor W, Trainer PJ, Darby D. Routine measurement of plasma chromogranin B has limited clinical utility in the management of patients with neuroendocrine tumours. Clin Endocrinol (Oxf). 2016 Mar;84(3):348-52. 8: Bridgewater J, Lopes A, Wasan H, Malka D, Jensen L, Okusaka T, Knox J, Wagner D, Cunningham D, Shannon J, Goldstein D, Moehler M, Bekaii-Saab T, McNamara MG, Valle JW. Prognostic factors for progression-free and overall survival in advanced biliary tract cancer. Ann Oncol. 2016 Jan;27(1):134-40. 9: Adaway JE, Dobson R, Walsh J, Cuthbertson DJ, Monaghan PJ, Trainer PJ, Valle JW, Keevil BG. Serum and plasma 5-hydroxyindoleacetic acid as an alternative to 24-h urine 5-hydroxyindoleacetic acid measurement. Ann Clin Biochem. 2015 Oct 5. pii: 0004563215613109. 10: Valle JW, Wasan H, Lopes A, Backen AC, Palmer DH, Morris K, Duggan M, Cunningham D, Anthoney DA, Corrie P, Madhusudan S, Maraveyas A, Ross PJ, Waters JS, Steward WP, Rees C, Beare S, Dive C, Bridgewater JA. Cediranib or placebo in combination with cisplatin and gemcitabine chemotherapy for patients with advanced biliary tract cancer (ABC-03): a randomised phase 2 trial. Lancet Oncol. 2015 Aug;16(8):967-78.

36
11: McNamara MG, Lamarca A, Hubner RA, Valle JW. To BRCA or Not to PALB. J Clin Oncol. 2015 Aug 10;33(23):2581-2. 12: Lamarca A, Benafif S, Ross P, Bridgewater J, Valle JW. Cisplatin and gemcitabine in patients with advanced biliary tract cancer (ABC) and persistent jaundice despite optimal stenting: Effective intervention in patients with luminal disease. Eur J Cancer. 2015 Sep;51(13):1694-703. 13: Primrose JN, Cunningham D, Garden OJ, Maughan TS, Pugh SA, Stanton L, Falk SJ, Rees M, Finch-Jones M, Valle JW, O'Reilly D, Hornbuckle J, Hickish T, Bridgewater JA. Cetuximab Is Contraindicated in the Perioperative Treatment of Colorectal Liver Metastases. J Clin Oncol. 2015 Jul 20;33(21):2405-6. 14: Carrato A, Falcone A, Ducreux M, Valle JW, Parnaby A, Djazouli K, Alnwick-Allu K, Hutchings A, Palaska C, Parthenaki I. A Systematic Review of the Burden of Pancreatic Cancer in Europe: Real-World Impact on Survival, Quality of Life and Costs. J Gastrointest Cancer. 2015 Sep;46(3):201-11. 15: Grunnet M, Christensen IJ, Lassen U, Jensen LH, Lydolph M, Knox JJ, McNamara MG, Jitlal M, Wasan H, Bridgewater J, Valle JW, Mau-Sorensen M. Decline in CA19-9 during chemotherapy predicts survival in four independent cohorts of patients with inoperable bile duct cancer. Eur J Cancer. 2015 Jul;51(11):1381-8. 16: Howell M, Valle JW. The role of adjuvant chemotherapy and radiotherapy for cholangiocarcinoma. Best Pract Res Clin Gastroenterol. 2015 Apr;29(2):333-43. 17: Abdel-Rahman O, Lamarca A, Valle JW, Hubner RA. Somatostatin receptor expression in hepatocellular carcinoma: prognostic and therapeutic considerations. Endocr Relat Cancer. 2014;21(6):R485-93. 18: Chan AK, Bruce JIe, Siriwardena AK. Glucose metabolic phenotype of pancreatic cancer. World J Gastroenterol. 2016 Mar 28;22(12):3471-85. 19: Baltatzis M, Jegatheeswaran S, O'Reilly DA, Siriwardena AK.Antibiotic use in acute pancreatitis: Global overview of compliance with international guidelines. Pancreatology. 2016 Mar-Apr;16(2):189-93. 20: Baltatzis M, Chan AK, Jegatheeswaran S, Mason JM, Siriwardena AK. Colorectal cancer with synchronous hepatic metastases: Systematic review of reports comparing synchronous surgery with sequential bowel-first or liver-first approaches. Eur J Surg Oncol. 2016 Feb;42(2):159-65. 21: Miranda CJ, Mason JM, Babu BI, Sheen AJ, Eddleston JM, Parker MJ, Pemberton P, Siriwardena AK. Twenty-four hour infusion of human recombinant activated protein C (Xigris) early in severe acute pancreatitis: The XIG-AP 1 trial. Pancreatology. 2015 Nov-Dec;15(6):635-41. 22: James AD, Patel W, Butt Z, Adiamah M, Dakhel R, Latif A, Uggenti C, Swanton E, Imamura H, Siriwardena AK, Bruce JI. The Plasma Membrane Calcium Pump in Pancreatic Cancer Cells Exhibiting the Warburg Effect Relies on Glycolytic ATP. J Biol Chem. 2015 Oct 9;290(41):24760-71. 23: Halloran CM, Platt K, Gerard A, Polydoros F, O'Reilly DA, Gomez D, Smith A, Neoptolemos JP, Soonwalla Z, Taylor M, Blazeby JM, Ghaneh P. PANasta Trial; Cattell
37
Warren versus Blumgart techniques of panreatico-jejunostomy following pancreato-duodenectomy: Study protocol for a randomized controlled trial. Trials. 2016 Jan 15;17:30. 24: Khaled YS, Malde DJ, Packer J, De Liguori Carino N, Deshpande R, O'Reilly DA, Sherlock DJ, Ammori BJ. A Case-matched Comparative Study of Laparoscopic Versus Open Distal Pancreatectomy. Surg Laparosc Endosc Percutan Tech. 2015 Aug;25(4):363-7. 25: Parkin E, O'Reilly DA, Plumb AA, Manoharan P, Rao M, Coe P, Frystyk J, Ammori B, de Liguori Carino N, Deshpande R, Sherlock DJ, Renehan AG. Digital histology quantification of intra-hepatic fat in patients undergoing liver resection. Eur J Surg Oncol. 2015 Aug;41(8):1020-7. 26: O'Reilly DA, Bouamra O, Kausar A, Malde DJ, Dickson EJ, Lecky F. The epidemiology of and outcome from pancreatoduodenal trauma in the UK, 1989-2013. Ann R Coll Surg Engl. 2015 Mar;97(2):125-30. 27: Hamza N, Darwish A, O'Reilly DA, Denton J, Sheen AJ, Chang D, Sherlock DJ, Ammori BJ. Perioperative Enteral Immunonutrition Modulates Systemic and Mucosal Immunity and the Inflammatory Response in Patients With Periampullary Cancer Scheduled for Pancreaticoduodenectomy: A Randomized Clinical Trial. Pancreas. 2015 Jan;44(1):41-52.