hst.187: physics of radiation oncology #9. radiation therapy: optimization in the presence of...
TRANSCRIPT

HST.187: Physics of Radiation Oncology
#9. Radiation therapy: optimization in the presence of uncertainty
Alexei Trofimov, [email protected]
Jan Unkelbach, [email protected]
Dept of Radiation Oncology MGH
April 3, 2007

Uncertainties in RT• Intro
– Sources of uncertainty, e.g. -• Set-up, target localization (inter-fractional)• Intra-fractional motion
– Methods to counter the uncertainties• Volume definitions/ margins, treatment techniques
– Effect of uncertainties on the dose distribution
• Probabilistic planning techniques in the presence of uncertainties– Inter-fractional motion and set-up uncertainties – Proton range variations in tissue
• Handling of intra-fractional motion (respiratory) – Image-guided radiation therapy IGRT and “4D” planning– Probability-based motion-compensation– Intro to robust optimization

Target definition: inter-observer variation
Steenbakkers et al R&O 77:182 (2005)


Target motion (intra-fractional)
Targeting

Interplay between internal motion and the multi-leaf collimator sequence
JH Kung
P Zygmanski

Target motion (intra-fractional)
Targeting
Radiological depth changes
Inhale Exhale

Planned dose at exhale phase
Liver Tx plan, PA field Planned by J.Adams(TPS: CMS XiO)
As would be delivered at inhale
50%

Set-up uncertainties: day-to-day variation
Images: © 2007 Elsevier IncZhang et al IJROBP 67:620 (2007)
Variation over 8 weeks of treatment

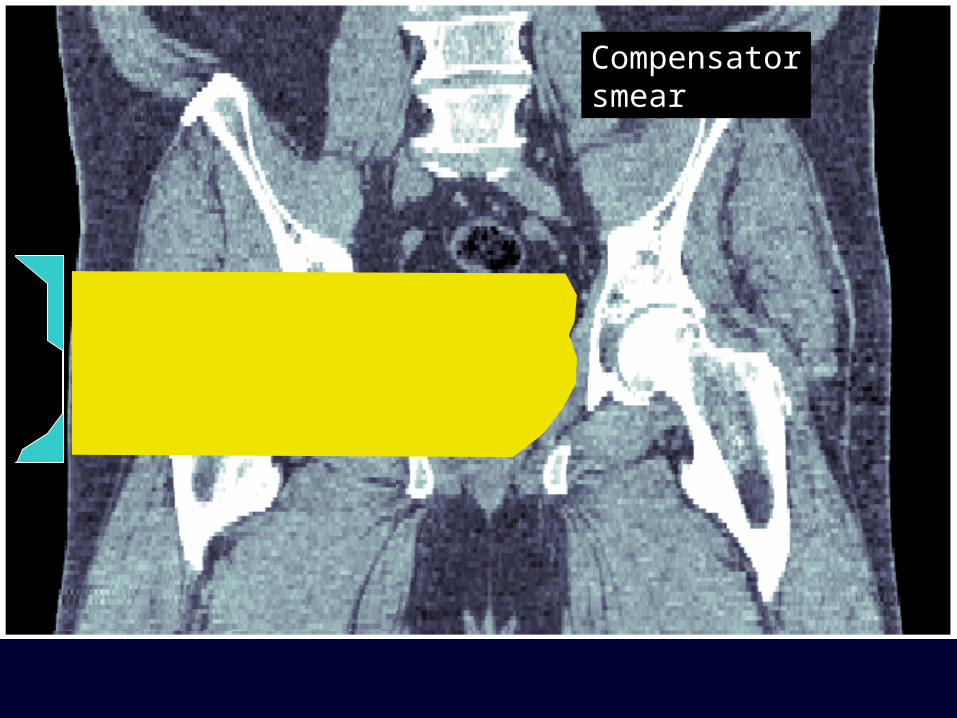
Prostate treatment with protons



Compensatordesign

Variation In set-up

Compensatorsmear
Compensatorsmear

Intrafractional motion

Part 2:Probabilistic
approach to account for uncertainty in
IMRT/IMPT optimization

Content
• Motivation – interfractional random setup error
• Concept of probabilistic treatment planning
• Application to interfractional motion of the prostate
• Application to range uncertainties in IMPT

MotivationConsider inter-fractional random setup error in a
fractionated treatment
How can we achieve an improvement?
• Lower dose to regions where tumor is located rarely
• Have to compensate for it by higher dose to other regions
safety margin:
irradiate entire area where tumor may be with the full dose

Motivation
25 moving voxels
45 static voxels
Example:
Question?
Are there static dose fields that yield tumor coverage and improve healthy tissue sparing?
tumor voxels are at 5 different positions equally often

Motivation
Example:
integral dose: 40.8 (instead of 45.0)

MotivationDose in the moving tumor:
frequency for moving voxel i being at static voxel j
Have to solve system of linear equations to determine static dose field which yields D = 1
dose in moving tumorstatic dose field

Motivation
special solution (safety margin)
Set of solutions is affine subspace
kernel of the mapping P:
Set of static dose fields which preserve D = 1:
kernel dimension (number of static voxels) minus (number of tumor voxels)

Motivation
Intrinsic problems:• only handles predictable motion, not uncertainty
• cannot handle systematic errors
• cannot handle irreproducable breathing pattern
Method could in principle work if motion was predictable and treatment was infinitely long
Need more general method to handle uncertainty!
(having these ideas in mind)

Idea of probabilistic methodMain assumption:
The dose delivered to a voxel depends on a set of random variables
vector of random variables which parameterize the uncertainty
fluence map to be optimized
Assign probability distribution to random variables:

Idea of probabilistic methodApplications:
G = position of voxels
P(G) = Gaussian distribution
• Inter-fractional motion
• range uncertainty
• respiratory motion
G = amplitude, exhale position, starting phase
(note: P(G) unrelated to `breathing PDF`)
G = range shifts for all beamlets

Idea of probabilistic methodPostulate:
optimize the expectation value of the objective function
• incorporate all possible scenarios into the optimization with a weighting that corresponds to its probability of occurrence

Idea of probabilistic methodExample: quadratic objective
1st order term 2nd order term
variance of the dosedifference of expected and prescribed dose
expected dose:

Alternative formulations• In this talk: optimize expectation value
• most desireable might be something in between
(can be solved by robust optimization techniques in linear programming)
• alternative: optimization of the worst case

Application to prostate
Incorporating
inter-fractional motion
of the prostate
into
IMRT optimization

application to prostateUncertainty G: positions of voxels
Probability distribution P(G): Gaussian

application to prostate
static dose field (dose per fraction)
• expected quadratic objective function
• 30 fractions
• large amplitude of motion ( 8mm AP, 5mm LR/CC)

application to prostateexpected dose in the moving tumor coordinate system
• Best estimate for the dose delivered to a voxel

application to prostateProblem: Uncertainty implies that we don‘t know the dose distribution which will be delivered
standard deviation: assess uncertainty of the dose in each point
treatment plan evaluation difficult

application to prostateProbability for the delivered dose to be below/within/above a 3% interval around the prescribed dose
below abovewithin
(D Maleike, PMB 2006)

application to prostatePrototype GUI to view probabilities for over/under dosage
(D Maleike, PMB 2006)
• user may select dose intervals of interest

Application to prostate
• Incorporate organ motion in IMRT planning to overcome the need of defining safety margins
• resemble the idea of inhomogeneous dose distributions on static targets in order to achieve better healthy tissue sparing
• control the sacrifice of guaranteed tumor homogeneity
Probabilistic approach can ...

Application to range uncertainties
Handling range uncertainty
in
IMPT optimization

Application to range uncertainties
degraded dose distribution if the actual range differs from the assumed range
assumed range + 5 mm - 5 mm
Conventional IMPT treatment plans may be sensitive to range variations

Application to range uncertaintiesWhy? Because ...
• pencil beams stop in front of an OAR
• dose distributions of individual beams are inhomogeneous

Application to range uncertainties
Range uncertainty assumptions for probabilistic optimization:
• 5 mm uncertainty (SD) of the bragg peak location for each beam spot
• Gaussian distribution for the range shifts
• is considered a systematic error (no averaging over different range realizations in different fractions)

Application to range uncertainties
assumed range + 5 mm - 5 mm
• Probabilistic optimization can significantly reduce the sensitivity to range variations
convetional plan

Application to range uncertaintiesWhy? Because ...
• lateral fall-off of the pencil beam is used
• dose distributions of individual beams are more homogeneous in beam direction
convetional plan

Application to range uncertaintiesPrice of robustness:• lateral fall-off is more shallow
convetional plan
plan quality for the assumed range is slightly compromised
- higher dose to OAR or reduced target coverage
probabilistic plan

Application to range uncertainties
• take advantage of the characteristic features of the proton beam and the many degrees of freedom in IMPT to make treatment plans robust with respect to range variations
(which cannot be achieved by other known heuristics)
Probabilistic approach can ...

Part 3: Intrafractional motion

Continuous irradiation

IMRT delivery to a moving target
Int map no motion motion 1 fraction motion 4 fx

The effect of target motion on dose distribution

Coverage assured with planning margins

Gated Tx at MGH
Varian RPM-system
marker block with IR-reflecting dots
IR-source + CCD camera

External-internal correlation Tsunashima et al IJROBP 2003

Gierga et al IJROBP 2004:
correlation differs between markers

Phase shift
HHoisak et al IJROBP 2003

External-internal correlation
• Generally well-correlated, but…
• Not necessarily linear• Phase shift has been observed, not
necessarily constant on different days
• Proportionality coefficients, phase may vary with – marker position– respiratory “discipline” (e.g. compliance with
breath-training/coaching)

(“Fast”) tracking delivery

Inverse optimization
• Dose calculation using (Dij) matrix:
beamlet jx
voxel i

4D- influence matrix (D-ij) approach
• Dij ’s are precalculated for all beams and all instances of geometry (4D-CT phases)
• At instance (phase) k we have
k = 1, …, 5: breathing phase
beamlet jx
voxel i

Eike Rietzel, GTY Chen “Deformable registration of 4D CT data” Med Phys 33:4423 (2006)
• Determine voxel displacement vector field between Pk and P0 (reference phase)
P0 (inhale) P4 (exhale)

• Deformations are then applied to all pencil beams in Dij matrix
pencil beam in P4 (exhale)
same pencil beam transformed to P0(inhale)
x
x
A Trofimov et al PMB 50:2779 (2005)

Continuous irradiation: instantaneous dose distribution

From a different prospective: a moving instant. dose in a fixed reference geometry

Approaches to temporo-spatial optimization of IMRT
(1) Planning with optimal margins (Internal Target Volume)
(2) Planning with Motion kernel(a) Uniform approach (motion PDF)(b) Adaptive approach (sum influence matrix)
(3) Gating / Unoptimized tracking – plans optimized separately, 1 best plan chosen out of several or all delivered dynamically
(4) Optimized tracking – several plans optimized simultaneously, delivered dynamically
A Trofimov et al PMB 50:2779 (2005)

Lung: CTV vs Internal Target Volume (ITV)

Planning with “Internal” margins - ITV

App. 1: Optimal margins (ITV): lung

DVH for ITV plan recalculated for different geometries (CT phases): lung

Approaches to Temporo-Spatial Optimization of IMRT
(1) Planning with expanded margins (ITV)
(2) Planning with modified dose kernel (b) Uniform approach (motion PDF)(a) Adaptive approach (sum influence matrix)
(3) Gating / Unoptimized tracking – plans optimized separately, 1 best plan chosen out of several or all delivered dynamically
(4) Optimized tracking – several plans optimized simultaneously, delivered dynamically

Motion probability distribution function (PDF)

Motion-compensation in IMRT treatment planning• If the motion (PDF) is known
(reproducible), the dosimetric effect can be reduced – Deconvolution of intensity map– Planning with “smeared” beams
– .

Reduction of integral dose with motion-adaptive planning

.
Motion kernel: “one-size-fits-all” vs. “custom-made”
Original beamlet
=
Convolved “motion” beamlet Sum of deformed beamlets

IMRT with motion-compensated Tx PlanInt map no motion motion 1 fraction motion 4 fx

Patient data
lung liver

App. 2a: Motion kernel plan, DVH recalculated for 5 ph’s

MK plan: DVH recalculated for diff phases

App. 2b: with averaged Dij-matrices (liver)

App. 2b: with averaged Dij-matrices (liver)

App. 2b: with averaged Dij-matrices (liver)
Inhale (recalc’d to reference) Exhale (reference)
Inhomogeneous “per-phase” doses are designed so that the some conforms to the prescription

Approaches to Temporo-Spatial Optimization of IMRT
(1) Planning with expanded margins (ITV)
(2) Planning with modified dose kernel (Motion kernel)(a) Uniform approach (motion PDF)(b) Adaptive approach (sum influence matrix)
(3) Gating / Unoptimized tracking – plans optimized separately, 1 best plan selected for gated delivery or all delivered dynamically
(4) Optimized tracking – several plans optimized simultaneously, delivered dynamically

App. 3: Gating / Unoptimized tracking (liver)

App. 3: Gating / Unoptimized tracking (lung)

Approaches to Temporo-Spatial Optimization of IMRT
(1) Planning with optimal margins (ITV)
(2) Planning with modified dose kernel (Motion kernel)(a) Uniform approach (motion PDF)(b) Adaptive approach (sum influence matrix)
(3) Gating / Unoptimized tracking – plans optimized separately, 1 best plan selected for gated delivery or all delivered dynamically
(4) Optimized tracking – several plans optimized simultaneously, delivered dynamically

App. 4: optimized tracking (lung)

App. 4: Optimized tracking (lung)

DVH comparison for the lung case

DVH comparison for liver case

Ideal case for tracking delivery (vs gating)

DVH and dose for different “gated” (single phase) plans for the lung case

Sources of delay: RPM: 60-90 ms , 75 ms averageSystem response time : < 5 msWait for the next modulation cycle: 0-100 ms
Total delay: 65-195 ms, average 130 ms
Delivery of gated proton treatment : Timing
Delivery restricted to complete modulation cycles: on/off at the stop block position only
100 ms
Hsiao-Ming Lu

Residual motion with gating Probability distribution

Inter-fractional variability
Liver-2

Cardiac-1

Cardiac-2

Cardiac-1
Time
Positio
nPositio
n

Variability between patients
Lung-2
Liver-2Cardiac-2

Robust formulation for probabilistic treatment planning:
– Tim Chan et al: Phys Med Biol 51:2567 (2006)
– Outcome will be “acceptable” as long as the realized motion is within the expected “limits”

PDFuncertaintybounds
Realized PDF
Realized PDFPlanning PDF
Planning PDF
Dose to moving target

Summary• (Some) sources of uncertainty in RT:
imaging, target definition, dose calc, set-up, inter-, intra-fractional motion
• Margin/ITV approach is the most robust for target coverage, but substantially increases dose to healthy tissue
• Image-guided RT improves dose conformity, reduced irradiation of healthy tissues, BUT relatively complex delivery, not error-proof
• Probabilistic motion-adaptive treatment planning in combination with image-guided delivery may be the optimal solution

Acknowledgements
J Adams
T Bortfeld, PhDT Chan, PhDS Jiang, PhDJ Kung, PhDHM Lu, PhDH Paganetti, PhD
E Rietzel, PhD
C Vrancic