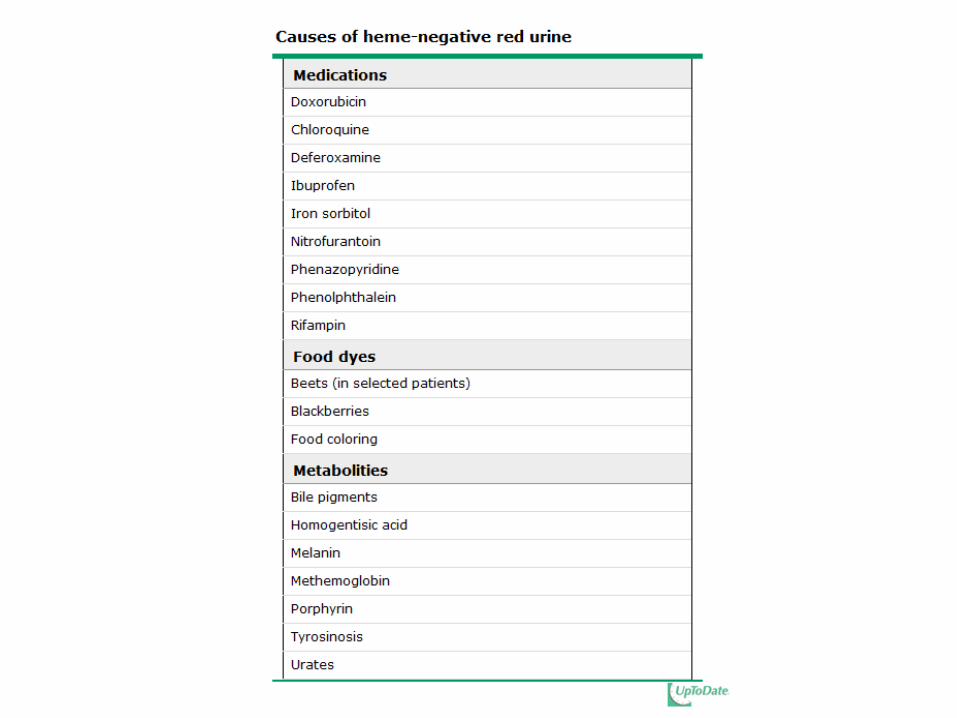
hurricane katrina aug 29, 2005. gross hematuria presenting to er uti50% perineal/urethral...
TRANSCRIPT

Hurricane Katrina Aug 29, 2005


Gross Hematuria Presenting to ER
• UTI 50%• Perineal/Urethral Irritation 18%• Trauma 7%• Acute Nephritis 4%• Coagulopathy 3%• Stone 2%• No etiology identified 10%• Don’t forget about tumors (Wilms)
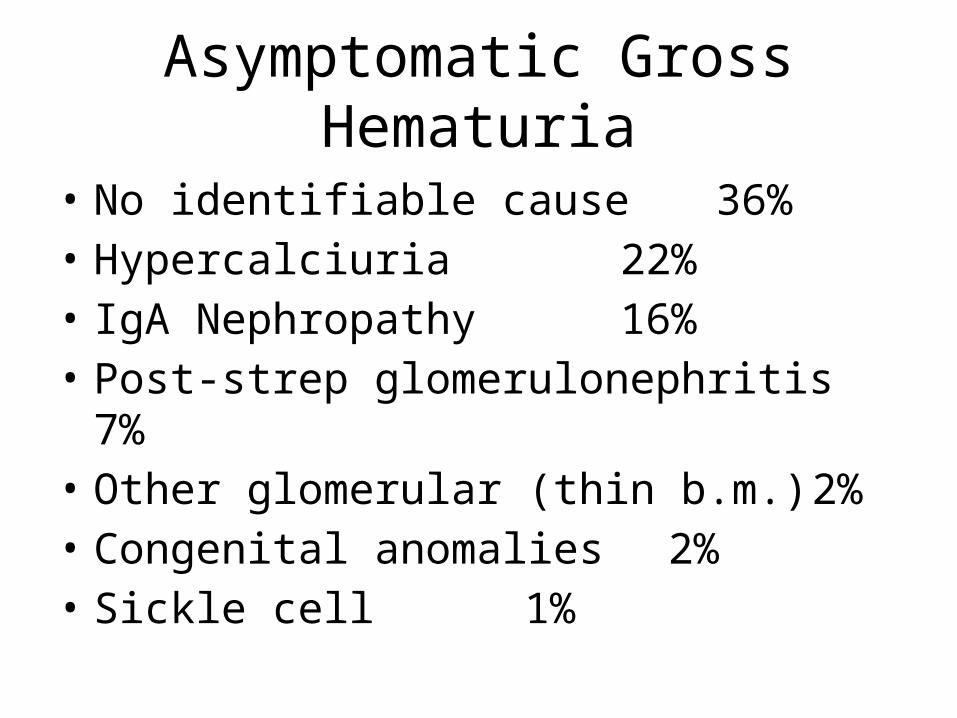
Asymptomatic Gross Hematuria
• No identifiable cause 36%• Hypercalciuria 22%• IgA Nephropathy 16%• Post-strep glomerulonephritis 7%• Other glomerular (thin b.m.) 2%• Congenital anomalies 2%• Sickle cell 1%

Evaluation (H&P!!!)
• Trauma: CT Scan• S/S of malignancy?– Wilm’s– Neuroblastoma

Evaluation
• Post-infectious Acute Glomerulonephritis (strep)– 10 days post pharyngitis– 21 days post impetigo– Edema, HTN (85%)– Strep antibody titers– Low C3

Evaluation
• IgA– Most common presentation recurrent hematuria– 5 days post URI– Can be associated with edema, HTN, renal
insufficiency– Dx: Kidney biopsy

Anatomic Abnormalities and Hematuria
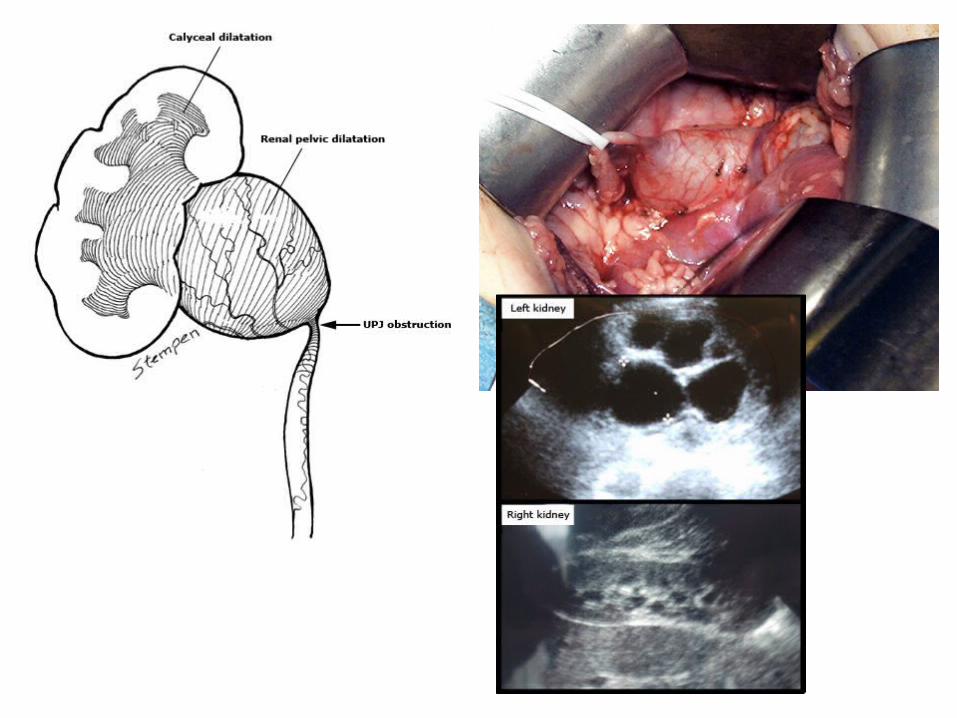
UPJ Obstruction
• Blockage (often partial) of urine flow where ureter enters kidney.
• Both congenital and acquired• Most common pathologic cause of antenatally
detected hydronephrosis• Intrinsic narrowing (most common)• Extrinsic compression (10%) aberrant renal a.
UPJ Obstruction: Presentation
• Fetal/neonatal: Fetal U/S, palpable abd mass, UTI, hematuria, FTT
• Children: Intermittent flank pain, hematuria with minor trauma, calculi, HTN

UPJ Obstruction: Treatment
• Asymptomatic: Watchful waiting• Symptomatic: Surgery
ADPKD
• Most common hereditary kidney dz• Presents from neonate to 5th decade• Hematuria, B flank pain, abdominal masses, HTN,
UTI• Cysts in liver, pancreas, spleen, ovaries• Mitral valve prolapse 12% of peds pts• Intracranial aneurysms (adults)• Dx by U/S, bilateral macrocysts• Tx: Supportive

ARPKD
• Infantile PKD• Neonatal B flank mass, oligohydramnios, pulm
hypoplasia, potter facies• Severe hepatic cirrhosis and portal HTN• 30% die as neonates• If survive 1st year, 10 year survival 80%• ESRD >50%