hybrid coronary revascularization
TRANSCRIPT

Hybrid Coronary Revascularization

Hybrid coronary revascularization (HCR) was first introduced in the 1996 as a pioneering treatment approach to multivessel coronary artery disease (CAD), hoping to bring together the “best of both worlds”.
HCR aims to reduce surgical trauma while preserving long-term survival and minimizing adverse cardiovascular event.

The intial concept was launched by Dr.Gianni Angelini et al from Imperial College, London and included a small number of patient population (6pts) and received favorable outcomes in terms of hospital stay ,duration of extubation and 6 month survival.

In the era of BMS when restenosis after PCI was more frequent than the modern PCI results, multiple revascularization procedures were common, only they were staged by days, weeks, or perhaps months.

In the modern era, a hybrid procedure refers to the combination of CABG and PCI, staged by minutes, hours, or at most, days.
It has gained interest as cardiac surgeons have improved techniques for minimally invasive surgical approaches, while interventional cardiologists have at their disposal improved devices and have developed skills that have enabled them to become more aggressive in their percutaneous interventions.

As interventional cardiologists are becoming “surgeons” with more invasive tools, surgeons are becoming “interventional cardiologists” with less invasive tools.
Hence, the division between the 2 specialties is becoming blurred, and we are meeting in the middle.

The hybrid approach includes left internal mammary artery (LIMA) anastomosis to the left anterior descending coronary artery (LAD), typically via a minimally invasive approach, and percutaneous coronary intervention (PCI) for the remaining (non-LAD) lesions.


RATIONALE ,INDICATIONS AND CONTRAINDICATIONS
Several trials have compared the outcomes of CABG surgery versus PCI in multivessel disease.
In a review of 23 randomized studies comparing PCI and CABG, survival at 10 years was similar even among the diabetic population; however, the rate of repeat revascularization rate was higher in PCI than CABG along with lower rate of relief from angina.

LIMA–LAD graft has excellent patency rates, which correlates with increased eventfree survival in CABG pts and LIMA-LAD graft may be responsible for the majority of the benefit of CABG surgery.
Whether the non LAD lesions are treated with SVG or PCI, it becomes statistically less significant than LIMA.

This is the premise on which the modern era of hybrid coronary revascularization is based. Conversely, with PCI, the location of the lesion in the proximal LAD has been identified as an independent risk factor for in-stent restenosis with rates between 19% and 44%.

With the advance of the stent technology it has shown favorable clinical outcomes with DES as compared to SVG in non LAD territories.

Indications for hybrid CABG/PCI (MIDCAB and TECAB) include patients with multivessel disease who have high-grade proximal disease of the LAD along with favorable lesions for PCI in the left circumflex and right coronary artery territories.

Other indications where PCI may represent a superior alternative to SVG conduit are lack or poor quality of the conduit, a nongraftable but stentable vessel (e.g., LCX lesion in the atrioventricular groove with small diffuse obtuse marginal)

The rationale for HCR lies in the well-established survival benefit conferred by LIMA-to-LAD grafts and the use of new stent platforms featuring lower stent restenosis and thrombosis rates compared with venous graft stenosis and occlusion rates, respectively.
Individually the patency rates and survival rates of arterial conduits are better than the venous grafts in patients undergoing CABG.

THE SURVIVAL BENEFIT OF A SURGICAL LIMA-TO-LAD GRAFT
A unique conduit, the LIMA powerfully resists thrombosis and atherosclerosis.
Furthermore, a LIMA graft protects the native coronary tree from the deleterious effects of disease progression

Because of the higher arterial pressures and unfavorable venous wall anatomy it is not suitable to carry blood at such higher pressures and hence is vulnerable to reocclusion.
Some studies suggest 75.9% 5 yr survival rates in SVG grafts as compared to 86.6% in LIMA grafts. While patency being 96% in LIMA as compared to 81.1% in SVG.(NEJM 1986)

WHAT FAVOURS LIMA OVER SVG LIMA even has a superior thrombotic profile in
terms of thrombosis when compared to DES. It is termed as relatively resistant to
atherosclerosis and has a protective role on native coronary tree.
WHY??? Endothelial layer has fewer fenestrations. Intercellular junctions have lower permeability. Higher eNOS activity Resistant to transfer of lipoproteins.

Thus, PCI and stenting provide strong competition for SVG revascularization because, unlike an LIMA-LAD graft, disease progression in the proximal native coronary segment occurs alongside SVG deterioration

Moreover, significant angiographic SVG stenosis occurs at least twice as frequently as in-stent restenosis using the latest technology platforms.
However, ischemia-driven revascularization rates are considerably higher in stented patients with treated multivessel CAD.
Furthermore, even though SVG occlusion occurs at a higher rate compared with stent thrombosis , the clinical consequences of the latter are more dramatic, as it is more frequently associated with major adverse clinical events.

CONTRAINDICATIONS
1. LAD is non graftable.2. LAD is intramyocardial.3. Previous surgery involving left chest cavity.4. Left SCA stenosis causing LIMA graft unsuitable.5. Lack of tolerance of single lung ventilation.

PATIENT SELECTION FOR HCR
CONCEPT OF HEART TEAM

HEART TEAM
First introduced in ESC 2013 as a followup of tumour boards of 1968.
While decision-making for patients with acute indications or less complex coronary disease may be straightforward, for patients with stable complex (e.g. left main and/or multivessel) coronary artery disease (CAD), a Heart Team consisting of a clinical/non-invasive cardiologist, interventional cardiologist, and cardiac surgeon is considered optimal to best assess the advantages and disadvantages of the various treatment strategies.

The Heart Team has recently become a class 1C recommendation in European and American guidelines on myocardial revascularization.

A study from Circulation 2010 done in New York suggests that in patients with an indication for coronary artery bypass grafting (CABG), only 53% received such treatment, 34% underwent percutaneous coronary intervention (PCI), 12% received medical management, and 1% did not receive any treatment.

Following consultation with the institutional heart team the decision should be taken for HCR
Factors to consider are the coronary tree anatomy,proximal LAD lesion, renal status and history of previous cardiopulmonary interventions.

Important anatomical feature favoring HCR should be plaque burden in the proximal LAD well characterized by the SYNTAX (SYNergy Between PCI With TAXUS and Cardiac Surgery) score.
The classic indication for HCR is multivessel CAD including:
1) a proximal complex LAD lesion with optimal distal anatomy amenable to LIMA-to-LAD grafting;
2) non- LAD lesions amenable to PCI, in a patient with no contraindications to dual antiplatelet therapy (DAPT)
3) a high likelihood of achieving “reasonable incomplete revascularization” with such an approach.
Complex distal left main lesions are also ideal for HCR if the circumflex artery territory is amenable for PCI.
HCR appears particularly appealing for patients with the aforementioned coronary anatomy and others considered too high risk for open cardiopulmonary bypass surgery via midline sternotomy.

HIGH RISK CASES FOR CABG High risk of deep sternal wound infection
(e.g., diabetics, morbidly obese) Severely impaired left ventricular
function Chronic kidney disease Significant carotid or neurological
disease Severe aortic calcification Prior sternotomy.
The 2011 American College of Cardiology Foundation/American Heart Association guidelines for CABG state that the “primary purpose of performing HCR is to decrease the morbidity rate of traditional CABG in high-risk patients”

In ESC/EACTS latest guidelines HCR has a Class IIb recommendation for specific patient subsets and only at experienced centers.
The lack of several large randomized controlled trials (RCTs) involving different risk groups, hinders the identification of an HCR target group.

According to STS database at present .48% of patients ideal for HCR actually undergo the procedure and primarily that is because of the lack of RCTs and proper identification of the patient group.

TECHNICAL ISSUES
1- VERSUS 2-STAGED APPROACH. HCR can be performed either simultaneously or as a “2-staged” procedure.The former implies concurrent CABG and PCI in a single operative suite, with PCI following CABG within minutes. In the “2-staged” approach, the optimal order PCI first versus CABG first is debated because each approach has advantages and disadvantages.

A simultaneous approach is only feasible in hybrid suites featuring state-of-the-art surgical and interventional equipment.
Often, CABG is performed first, allowing the interventional cardiologist to study the LIMA-LAD graft before stent implantation.
Thus, PCI to high-risk, non-LAD lesions is performed with a protected LAD territory. In case of unsuccessful stent implantation, surgical bailout graft implantation remains an option.

Additionally, the simultaneous HCR approach can be cost effective by reducing hospital length of stay, the risk of lesion destabilization, and recurrent hospital admissions between staged procedures.
An additional advantage is improved patient satisfaction, as it condenses revascularization into 1 patient encounter.

But the challenge is balancing the need for appropriate antiplatelet therapy, to avoid stent thrombosis, with surgical bleeding risk.
Performing the LIMA-LAD anastomosis under DAPT can be difficult, particularly when a minimally invasive approach and video-assisted LIMA take-down are used.
Also The response of DES to protamine administration at the end of CABG has not been fully investigated

When DAPT is not administered to reduce surgical bleeding risk, PCI becomes risky and is not recommended.
Another challenging scenario for “1-stop” HCR is the patient with chronic kidney disease, who is exposed in a short period of time to the dual nephrotoxic insult of surgery and contrast media.

When the HEART TEAM favors a 2-step procedure, the sequence of PCI and CABG should be guided by clinical presentation and coronary anatomy.
2011 ACC/AHA guidelines favor performing CABG first followed by PCI.

This strategy allows1. Angiographic visualization of the LIMA-
LAD graft2. complete antiplatelet inhibition following
CABG with no perioperative bleeding risk3. Provides a protected anterior wall,
lowering procedural risks during PCI of non-LAD vessels.

On some occasions after minimally invasive LIMA to LAD, patients become asymptomatic in the immediate post-operative period.
In these cases, when the residual non-LAD lesions are angiographically intermediate, optimal medical therapy and watchful waiting may be in the patients’ best interest

The disadvantages of a CABG-first approach include the risk of ischemia of non-LAD territories during the LIMA-LAD grafting and the potential for a high risk surgical reintervention following unsuccessful PCI.
However, a PCI-first approach is reasonable in patients presenting with acute coronary syndrome (ACS) who undergo non-LAD culprit lesion PCI followed by CABG of the LAD.


ANTIPLATELET MANAGEMENT Balancing the risk of perioperative
bleeding with that of stent thrombosis. In the majority of HCR registries
following the “CABG-first” approach CABG was performed on aspirin; a second antiplatelet agent was started >4 h post-bypass after ensuring that no bleeding complications had occurred

In the “PCI-first” approach, DAPT is typically commenced ahead of the PCI procedure and is continued uninterrupted during CABG.
In most series of simultaneous HCR, patients are not pre medicated with clopidogrel and undergo the LIMA LAD graft taking only aspirin, followed by a single loading dose of clopidogrel 300 mg either when the LIMA-LAD graft is completed, just before its completion, or immediately post-PCI.

Newer antiplatelet agents like prasugrel, ticagrelor, or cangrelor(an investigational agent with rapid onset and reversal) could prove to be safer alternatives for HCR; however, this remains an “evidence-free” zone.
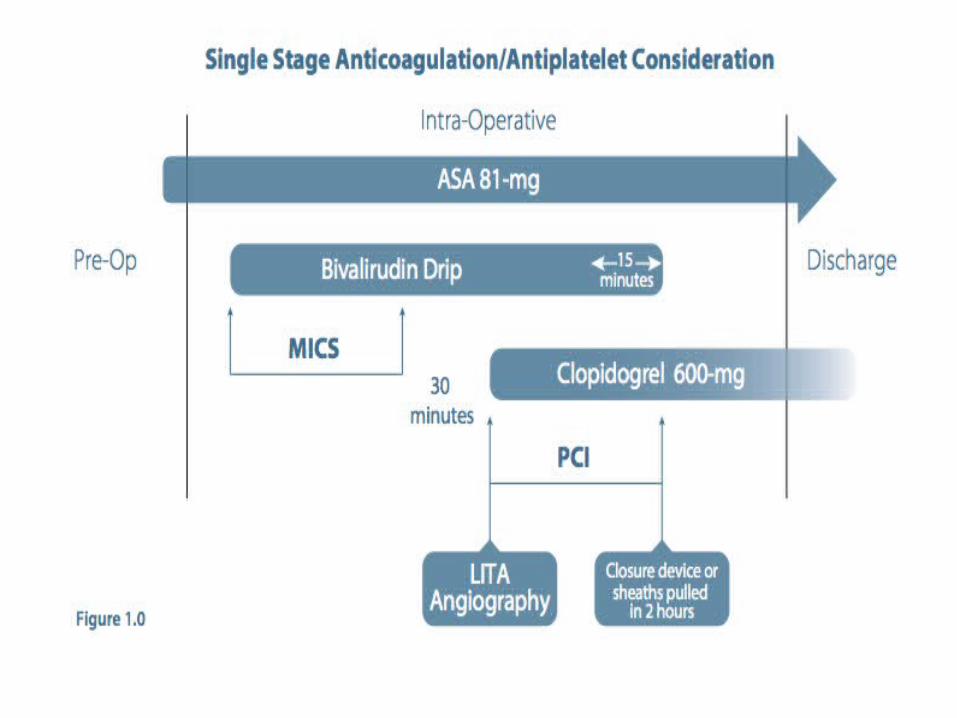

PROCEDURAL STEPS FOR SINGLE STAGED APPROACH

INDIVIDUAL COMPONENTS OF HCR
THE LIMA-LAD ANASTOMOSIS In most cases, the LIMA-LAD anastomosis can be performed using the minimally invasive approach, which aims to avoid cardiopulmonary bypass and the sternotomy incision.Minimally invasive direct coronary artery bypass grafting (MIDCAB) is performed on the beating heart through a small, left-sided thoracotomy in the 4th/5th interspace via direct visualization.

To avoid the significant chest wall manipulation associated with MIDCAB and to improve post-operative pain control, thoracoscopic and robotic techniques have been developed. These include the endoscopic atraumatic coronary artery bypass (Endo-ACAB), which allows thoracoscopic/robotic LIMA identification and mobilization followed by a direct non–rib spreading thoracotomy permitting hand-sewn anastomosis on the beating heart
Totally endoscopic coronary artery bypass grafting either on- or off-pump, in which the anastomosis is performed intracorporeally using a robot.
The latter, although challenging, produces a reported clinical freedom from graft failure as high as 98.6% at 13 months in experienced hands

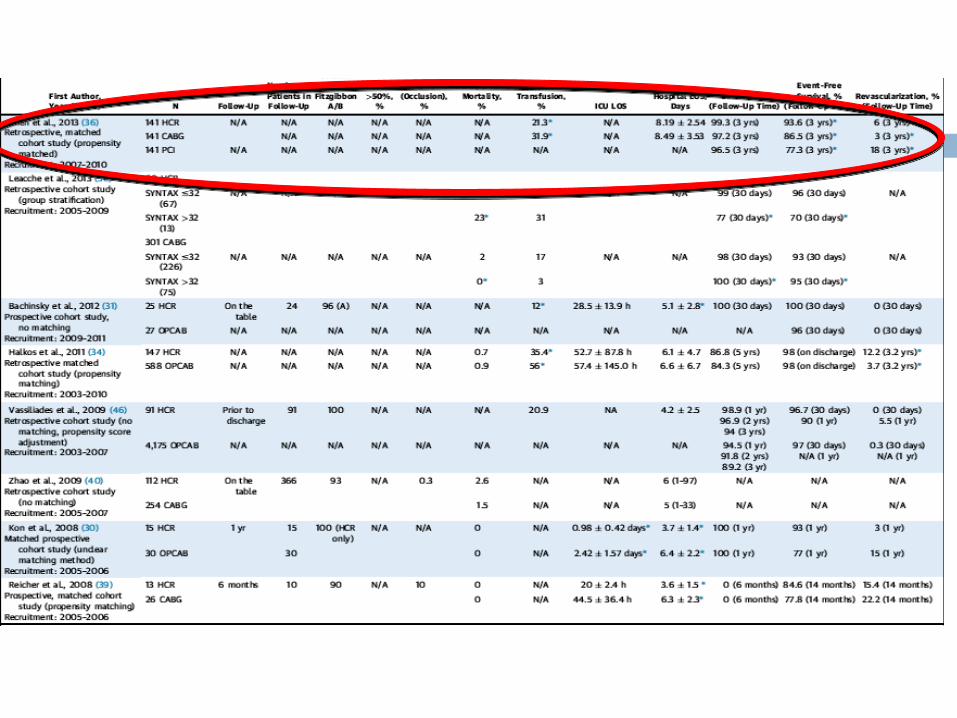
EVIDENCE BASED APPROACH Since its inception in 1996 a limted
number of large studies have been conducted regarding the efficacy of HCR.
Majority of the registries are published between 2008-2013.
Various aspects of HCR due to lack of RCTs are still under debate.

In a recent metaanalysis by Harskamp et al. comprising 1,190 no significant differences were found for the composite of death, myocardial infarction, stroke, or repeat revascularization at 1 year.
In the most recent registries, CABG was performed before PCI in about one-half of the HCR procedures,whereas PCI was performed first in quarter of the pts.

One-stop HCR proved the least popular, highlighting the practical difficulties of setting up and running a hybrid operating room.
However, among cohort studies comparing HCR with conventional CABG, 1-stop HCR appears to be the most popular strategy, highlighting that the simultaneous approach is considered the gold standard for comparisons with other revascularization strategies.

The majority of HCR patients are just over 60 years of age, are predominantly male, and have a diabetes prevalence varying from 23% to 40.7%.
The presentation mode varied across the studies, with ACS prevalence as low as 0% to as high as 74%.
In the majority of HCR cases, left ventricular ejection fraction was preserved or, at most, mildly impaired.

Most reports focus on the lower morbidity related to the minimally invasive nature of the procedure’s surgical component as compared with conventional CABG.
Low morbidity is mirrored by reduced blood transfusion requirements, shorter intensive care and hospital length of stay, and faster recovery

PATENCY RATES
Fitzgibbon A or B LIMA patency rates (A [excellent], B [fair], or O [occluded]) have been reported in a high percentage of patients: ranging from 93% to 100% of patients in the perioperative period ,90% and 94% of patients at 6 months and 91% of HCR patients at 2 years post-grafting.
Only 2 studies in the last 5 years reported angiographic follow-up of patients who underwent HCR.
In a study of 60 patients, Kiaii et al reported 2-year angiographic follow up in 54 (90%) patients. In-stent restenosis rates were 13%, whereas in-stent thrombosis was observed in 3.7% of patients.

In another study of 94 HCR patients with 6-month angiographic follow-up , instent restenosis was reported in 9% of patients, whereas in-stent thrombosis was seen in 2.2%.
These figures concur with those reported from studies using first-generation DES





CONTROVERSIES
Why should institutes adopt a complex, costly procedure when similar survival and morbidity outcomes can be obtained with a well-established, safe procedure available in most hospitals

FIRST a recent study, shows signals of improved MACE outcomes in the HCR versus conventional CABG group for patients in the highest EuroSCORE tertile (>6), suggesting a potential target population that would benefit the most from this complex procedure

SECOND, the use of HCR in lower- to intermediate risk groups could be justified by improved patient satisfaction, shorter intensive care and hospital stays, faster return to work and quicker return to normal daily activities.
For patients who undergo LIMA to LAD first as part of an intended staged HCR, and who become asymptomatic postprocedure, the benefits of PCI to residual intermediate non-LAD lesions should be questioned.
Optimal medical therapy watchful waiting alongside ischemia testing when symptomatology is unclear provides a reasonable alternative, albeit not evidence based.