hyperhidrotic and control subjects have similar sweating responses to pilocarpine administration
TRANSCRIPT
J AM ACAD DERMATOL
VOLUME 64, NUMBER 3Letters 603
the higher medication cost associated with approval ofcolchicine for the treatment of gout.
Daniel J. Hogan, MD, FAAD
NOVA Southeastern University College of Osteo-pathic Medicine, Internal Medicine (Dermatol-ogy), Largo Medical Center, Largo, Florida
Funding sources: None.
Conflicts of interest: None declared.
Correspondence to: Daniel J. Hogan, MD, FAAD,14046 Joel Ct, Largo, FL 33774.
E-mail: [email protected]
REFERENCES
1. Kesselheim AS, Solomon DH: Incentives for drug developmente
the curious case of colchicine. N Engl J Med 2010;362:2045-7.
2. Lebwohl M, Heymann WR, Berth-Jones J, Coulson I, editors.
Treatment of skin disease. 2nd ed. London: Mosby; 2006.
3. Available at: http://www.fda.gov/Drugs/DrugSafety/DrugSafety
Podcasts/ucm079097.htm. Accessed August 17, 2010.
4. Letter fromFDAonColcrys.Availableat: http://www.rheumatology.
org/advocacy/Colcrys_Letter_from_Woodcock.pdf. Accessed Au-
gust 17, 2010.
5. Available at: http://www.colcrys.com/healthcare-professional/
patient-assistance-program.htm. Accessed August 17, 2010.
6. Available at: https://mprsetrial.mckesson.com/colcrys/colcrys
CouponMain.jsp. Accessed August 17, 2010.
doi:10.1016/j.jaad.2010.09.004
RESEARCH LETTERS
p=.028
0
2
4
6
8
10
12
14
)5=n(slortnocyhtlaeH)6=n(scitordihrepyH
TE
WL
(g
.m
-2
.h
r-1
)
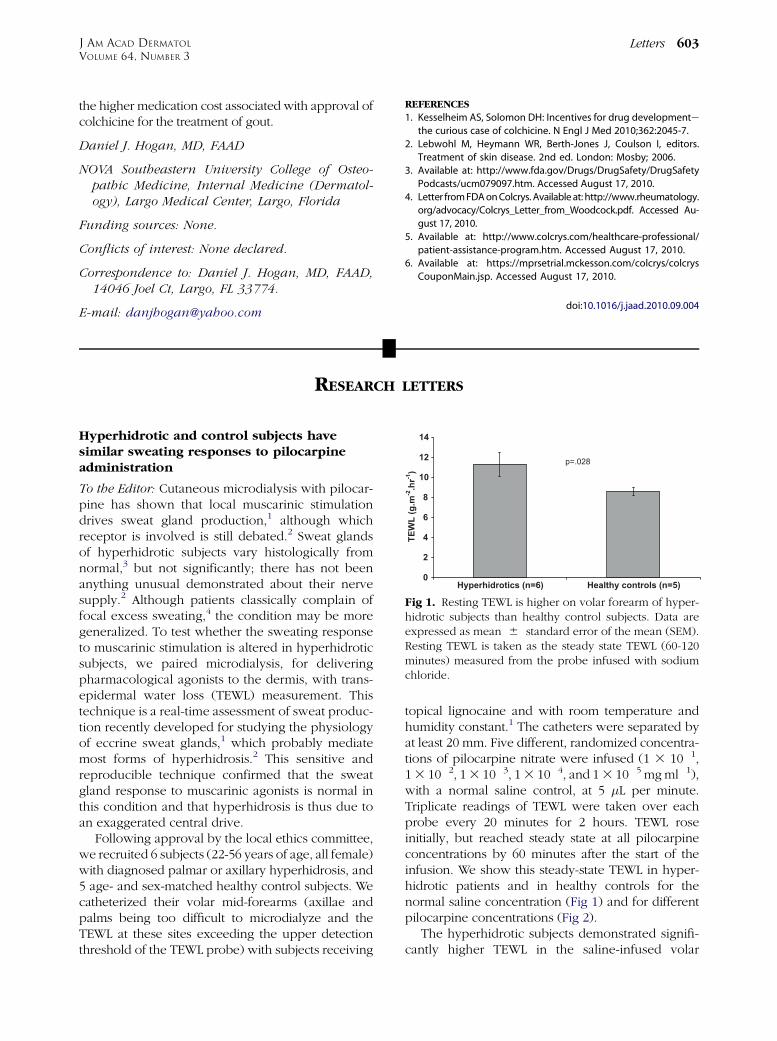
Fig 1. Resting TEWL is higher on volar forearm of hyper-hidrotic subjects than healthy control subjects. Data areexpressed as mean 6 standard error of the mean (SEM).Resting TEWL is taken as the steady state TEWL (60-120minutes) measured from the probe infused with sodiumchloride.
Hyperhidrotic and control subjects havesimilar sweating responses to pilocarpineadministration
To the Editor: Cutaneous microdialysis with pilocar-pine has shown that local muscarinic stimulationdrives sweat gland production,1 although whichreceptor is involved is still debated.2 Sweat glandsof hyperhidrotic subjects vary histologically fromnormal,3 but not significantly; there has not beenanything unusual demonstrated about their nervesupply.2 Although patients classically complain offocal excess sweating,4 the condition may be moregeneralized. To test whether the sweating responseto muscarinic stimulation is altered in hyperhidroticsubjects, we paired microdialysis, for deliveringpharmacological agonists to the dermis, with trans-epidermal water loss (TEWL) measurement. Thistechnique is a real-time assessment of sweat produc-tion recently developed for studying the physiologyof eccrine sweat glands,1 which probably mediatemost forms of hyperhidrosis.2 This sensitive andreproducible technique confirmed that the sweatgland response to muscarinic agonists is normal inthis condition and that hyperhidrosis is thus due toan exaggerated central drive.
Following approval by the local ethics committee,we recruited 6 subjects (22-56 years of age, all female)with diagnosed palmar or axillary hyperhidrosis, and5 age- and sex-matched healthy control subjects. Wecatheterized their volar mid-forearms (axillae andpalms being too difficult to microdialyze and theTEWL at these sites exceeding the upper detectionthreshold of the TEWL probe) with subjects receiving
topical lignocaine and with room temperature andhumidity constant.1 The catheters were separated byat least 20 mm. Five different, randomized concentra-tions of pilocarpine nitrate were infused (1 3 10�1,13 10�2, 13 10�3, 13 10�4, and 13 10�5 mgml�1),with a normal saline control, at 5 �L per minute.Triplicate readings of TEWL were taken over eachprobe every 20 minutes for 2 hours. TEWL roseinitially, but reached steady state at all pilocarpineconcentrations by 60 minutes after the start of theinfusion. We show this steady-state TEWL in hyper-hidrotic patients and in healthy controls for thenormal saline concentration (Fig 1) and for differentpilocarpine concentrations (Fig 2).
The hyperhidrotic subjects demonstrated signifi-cantly higher TEWL in the saline-infused volar

0
10
20
30
40
50
60
70
0.000001 0.00001 0.0001 0.001 0.01 0.1 1
Pilocarpine (mg ml-1
)
TE
WL
(g
m
-2
h
ou
r-1
)
Hyperhidrotics (n=6)Healthy controls (n=5)
Fig 2. TEWL response to pilocarpine (5 3 10�5 to5 3 10�1 mg ml�1) is the same in hyperhidrotic subjectsand control subjects. Steady-state TEWL was taken as themean of the measurements from 60 to 120 minutes. Dataare expressed as mean 6 SEM.
J AM ACAD DERMATOL
MARCH 2011604 Letters
forearm skin than did the control subjects (see Fig 1).This finding suggests that although patients maycomplain of excess sweating in sites of dense eccrinegland concentration (axillae, palms, and soles), thehyperhidrosis is a more generalized phenomenon,albeit subclinical in non-dense eccrine gland sites.
We note that though sweating in bothhyperhidrotic subjects and control subjects re-sponded to pilocarpine administration in a similarsigmoidal dose-dependent fashion, the differencesin response were not significant between groups.Although there was a trend to higher TEWL values inthe hyperhidrotic group at lower concentrations ofpilocarpine infusion, this was no more than thedifference in nonstimulated sweat production,which again probably represents higher backgroundsweating in hyperhidrotic individuals.
Thus our data support the view that hyperhidro-sis is not caused by a primary abnormality of eccrinesweat glands, but by a central cortical overdrive.Although subjects generally complain of focal ex-cess sweating, there may in fact be a more subtlegeneralized increase in sweat production. Thiswould be in keeping with the clinical experienceof one of the authors (G. M. K.) where patientspresent with focal sweating, but also volunteer onquestioning that other areas, such as the lower back,are also affected.
Joanna Taylor,a Sarah Woodcock,a Gina M.Kavanagh, FRCP,b and Richard B. Weller, MD,FRCPc
University Medical School,a Department of Derma-tology, Royal Infirmary of Edinburgh,b and theUniversity Department of Dermatology,c Edin-burgh, United Kingdom.
Funding source: Foundation for Skin Research.
Conflicts of interest: None declared.
Correspondence to: Richard B. Weller, MD, FRCP,University Department of Dermatology, Lauris-ton Bldg, Lauriston Place, Edinburgh, EH3 9HA,UK
E-mail: [email protected]
REFERENCES
1. Morgan CJ, Friedmann PS, Church MK, Clough GF. Cutaneous
microdialysis as a novel means of continuously stimulating
eccrine sweat glands in vivo. J Invest Dermatol
2006;126:1220-5.
2. Lonsdale-Eccles A, Leonard N, Lawrence C. Axillary hyperhidro-
sis: eccrine or apocrine? Clin Exp Dermatol 2003;28:2-7.
3. Bovell DL, Clunes MT, Elder HY, Milsom J, Jenkinson DM.
Ultrastructure of the hyperhidrotic eccrine sweat gland. Br J
Dermatol 2001;145:298-301.
4. Haider A, Solish N. Focal hyperhidrosis: diagnosis and manage-
ment. CMAJ 2005;172:69-75.
doi:10.1016/j.jaad.2010.03.003
Permanent chemotherapy-induced alopecia:A review
To the Editor: Hair loss in patients undergoingchemotherapy for cancer is usually reversible afterdiscontinuation of chemotherapy. However, inchemotherapy-induced permanent alopecia (CIPAL)characterized by absent or sparse hair, regrowth maynot occur.1-5
After institutional review board approval, weperformed a retrospective chart study of patientswho had attended our Hair Clinic during the previ-ous 7 years. Findings were compared with reportsidentified by a literature search.
We reviewed 8,430 records of patients with non-scarring alopecia. Of these, 7 cases of CIPAL wereidentified (0.083%), two following chemotherapywith busulphan and 5 following treatment withtaxanes (Table I). The median age of these patientswas 41 years and all showed diffuse alopecia char-acterized by short and sparse scalp hair (Fig 1),which developed a few weeks after the start ofchemotherapy. Two patients also demonstrated par-tial eyebrow loss. Histopathologic examinationshowed a marked reduction of follicular units withan increase in vellus hair formation and absence ofany significant inflammation or scarring.
Ninety case reports of CIPAL were identified in theliterature. These were associated with Bu and/or