hypersensitivity i & ii ch. 18-19 march 6th, 2006 ricky chang
Post on 20-Dec-2015
214 views
TRANSCRIPT
Hypersensitivity I & IICh. 18-19
March 6th, 2006
Ricky Chang
Objectives
• Know the mechanism of Type I hypersensitivity
• Know the mediators of Type I hypersensitivity
• Know the diseases associated with Type II hypersensitivity
Hypersensitivity
• Adaptive immunity is important against is important against microbial infections, microbial infections, butbut it is also capable of it is also capable of causing causing tissue injurytissue injury and and diseasedisease (autoimmune diseases)(autoimmune diseases)
• Occurs when immune responses are directed Occurs when immune responses are directed against against self-agself-ag and also from uncontrolled or and also from uncontrolled or excessive responses to against excessive responses to against foreign agforeign ag, , such as microbes and allergenssuch as microbes and allergens
Hypersensitivity
• Common cause is failure of Common cause is failure of self-toleranceself-tolerance, , which ensures that individuals do not respond which ensures that individuals do not respond to their own antigensto their own antigens
• Leads to tissue injury that occurs in Leads to tissue injury that occurs in autoimmune diseases due to the autoimmune diseases due to the same same effector mechanismseffector mechanisms used to protect against used to protect against microbesmicrobes
Hypersensitivity
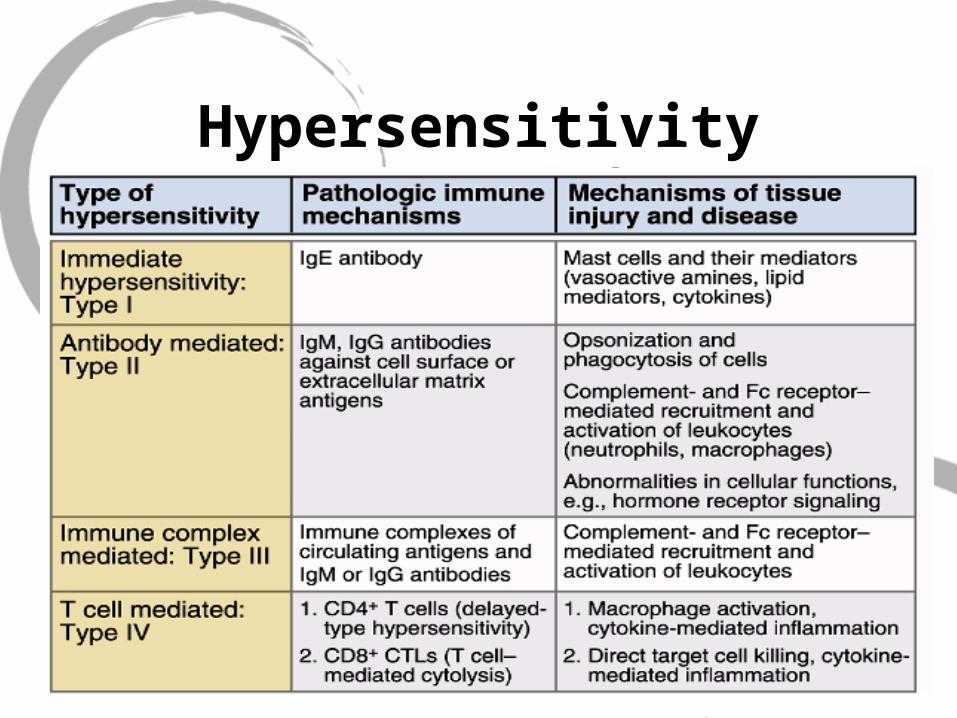
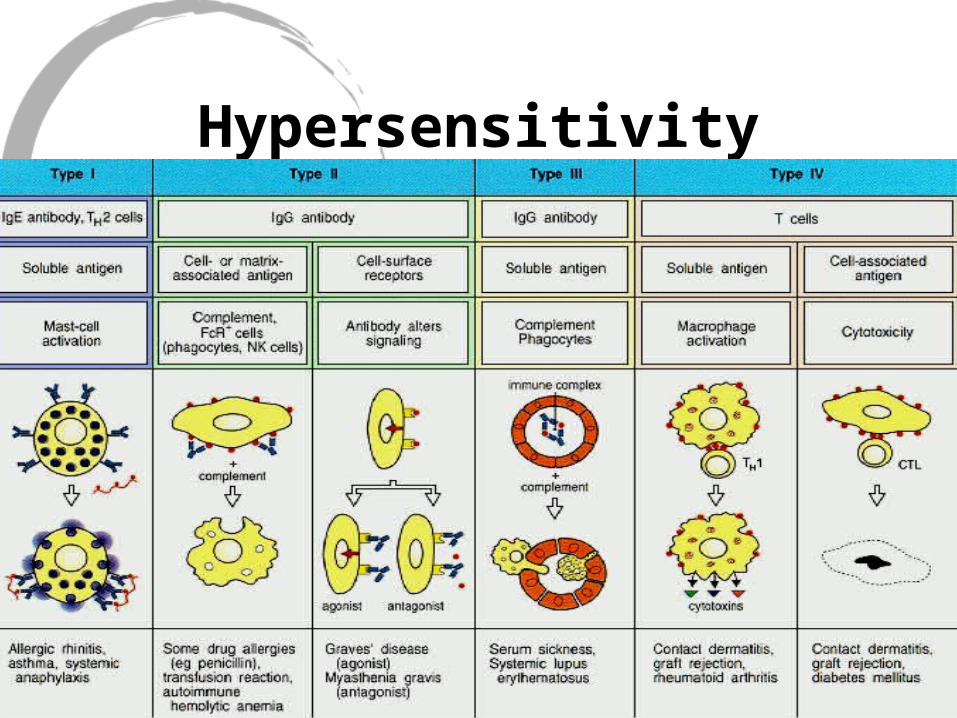
• Type I: IgE antibodies bind to Fc receptors on mast cells. IgE induces mast cell degranulation and release inflammatory mediators
• Type II: Ab mediated immune response against self antigen or foreign antigen (ie ag on transfused RBC)
• Type III: Immune complexes are deposited in tissue
• Type IV: T-cell mediated response where Ag sensitized T-cells release lymphokines
Hypersensitivity
Hypersensitivity
Roles of Mast Cells
• Part of connective tissue (contains granules of histamine and heparin)
• Allergic diseases (asthma,eczema,itch)• Anaphylaxis (systemic shock to allergens such
as bee sting,nuts,drugs)• Autoimmune disorders/Acute or chronic
inflammation (MS, Rheumatoid arthritis)• Wound healing • Innate response for clearing bacteria and
viruses
BasophilMast Cell
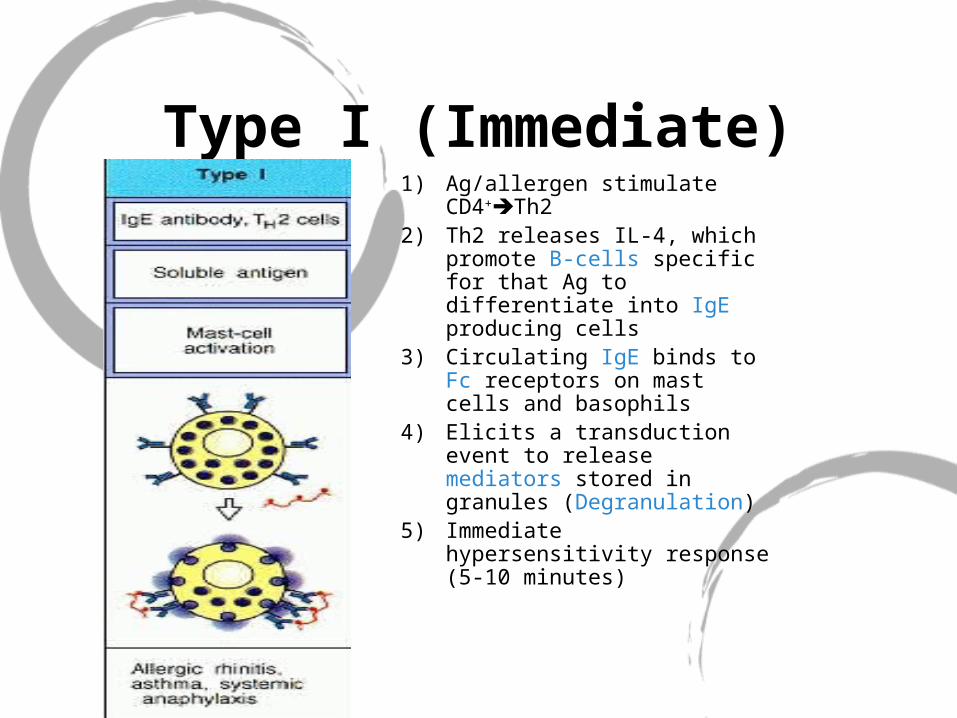
Type I (Immediate)1) Ag/allergen stimulate
CD4+Th2 2) Th2 releases IL-4, which
promote B-cells specific for that Ag to differentiate into IgE producing cells
3) Circulating IgE binds to Fc receptors on mast cells and basophils
4) Elicits a transduction event to release mediators stored in granules (Degranulation)
5) Immediate hypersensitivity response (5-10 minutes)
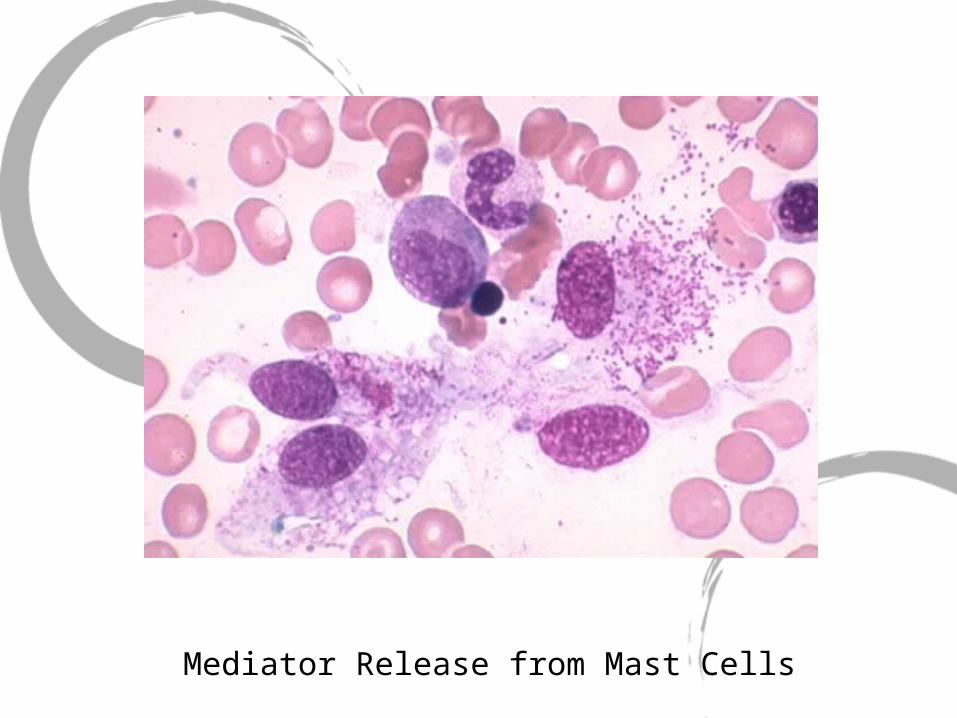
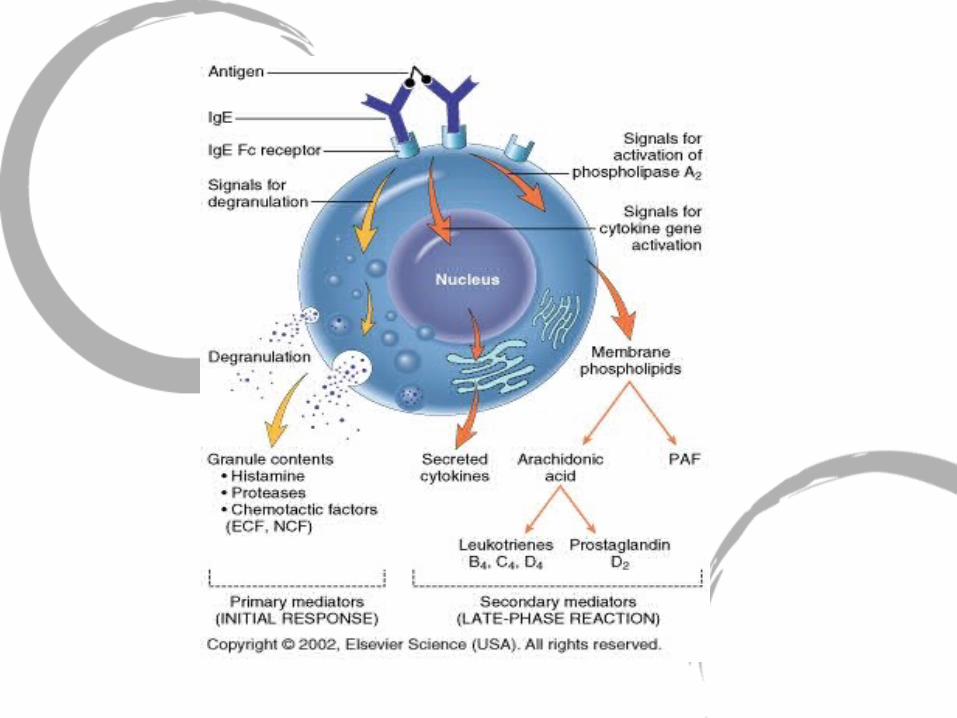
Mediator Release from Mast Cells
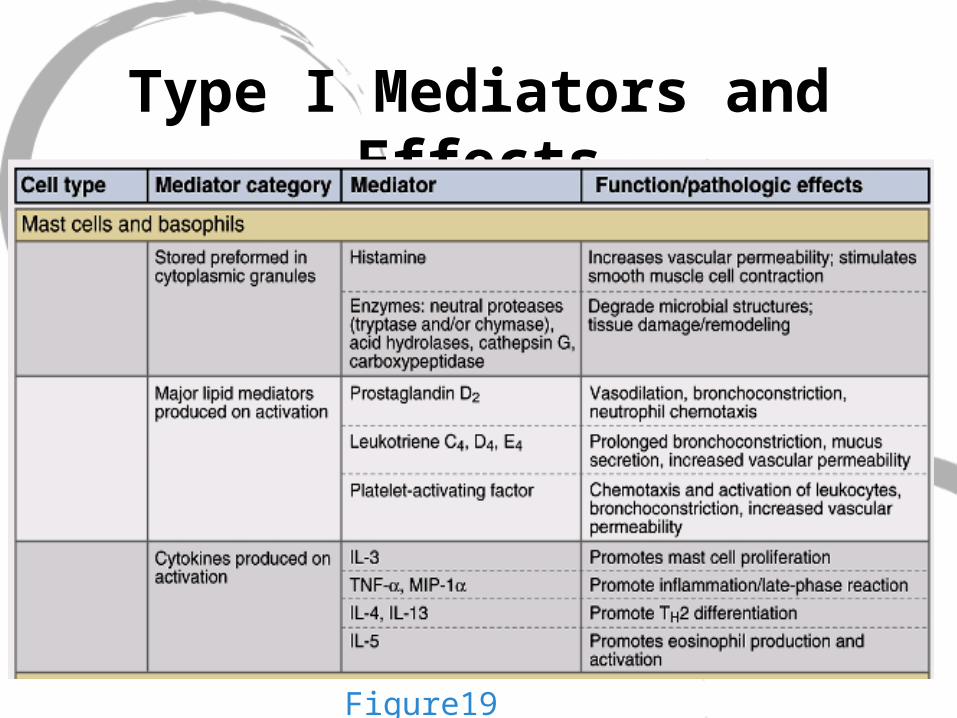
Type I Mediators and Effects
Figure19.3
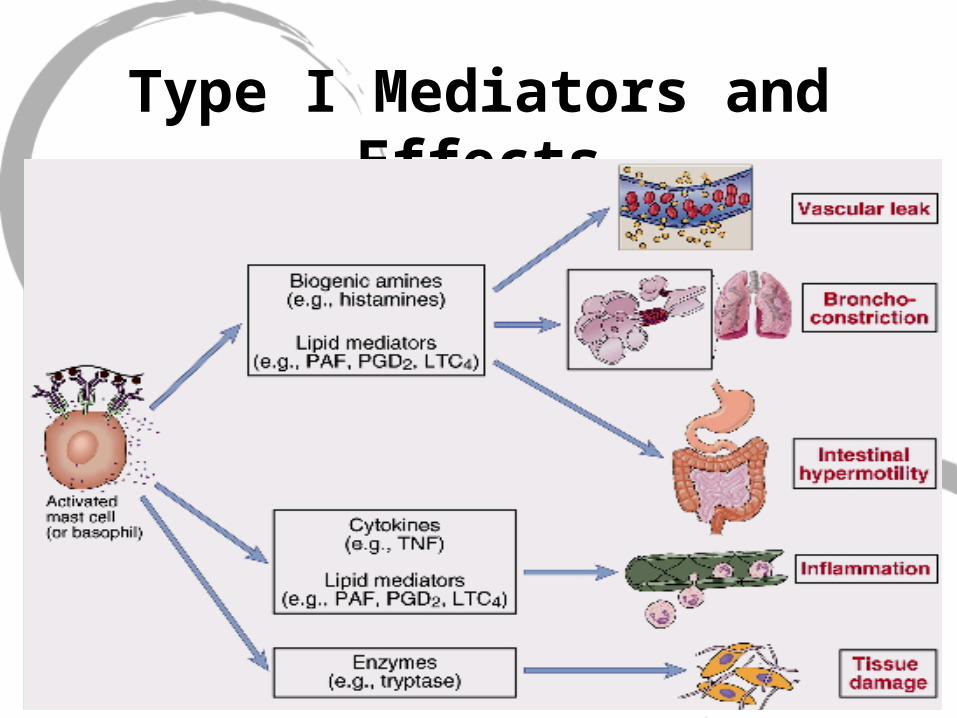
Type I Mediators and Effects
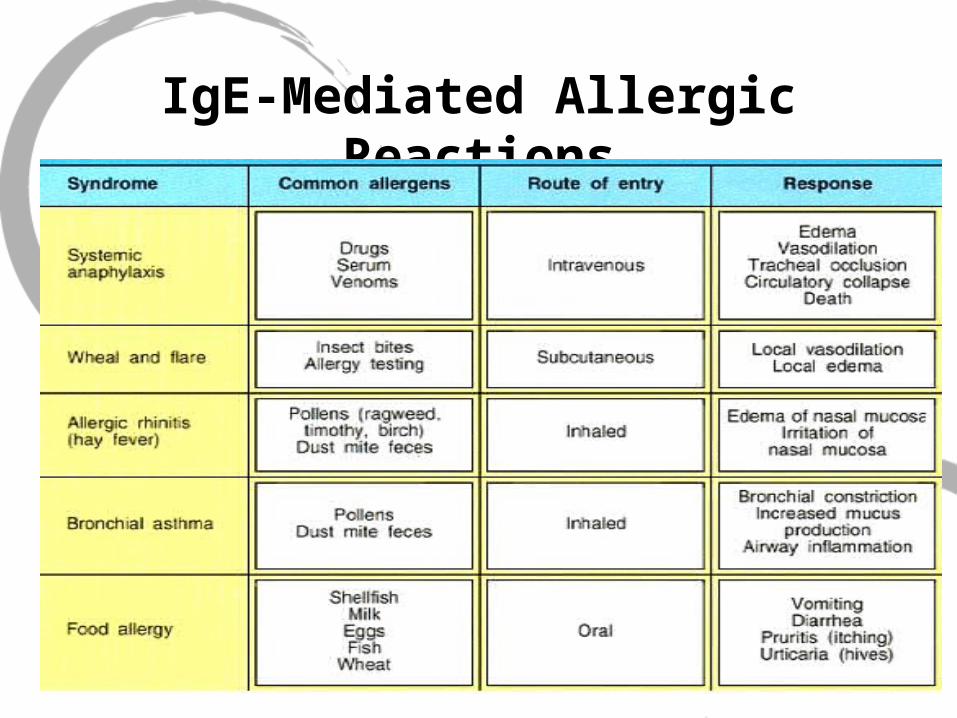
IgE-Mediated Allergic Reactions
Type I: Mast Cells
• Type I reaction is dependent upon the specific triggering of IgE-sensitized mast-cells by allergen (Ag)
• Ag enter via mucosal surfaces and are taken up by APC
• Th2 cells release IL-4 to facilitate the B-cell proliferation and differentiation, producing IgE specific for the allergen
• REMEMBER: THIS IS A TH2 RESPONSE!
Activation of Mast Cells
• IgE from B-cells binds to FcRI on mast-cells
- is the heavy chain responsible for IgE isotype switching
• FcRI on mast-cells cross-links with Ag-bounded IgE and induces degranulation of mediators
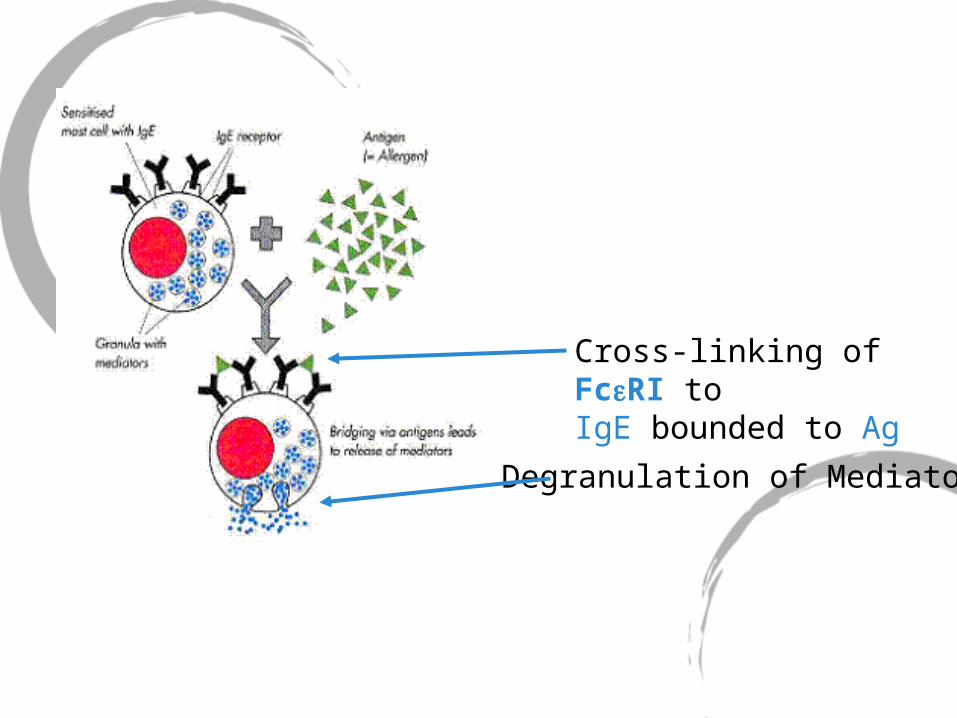
Cross-linking of FcRI toIgE bounded to Ag
Degranulation of Mediators
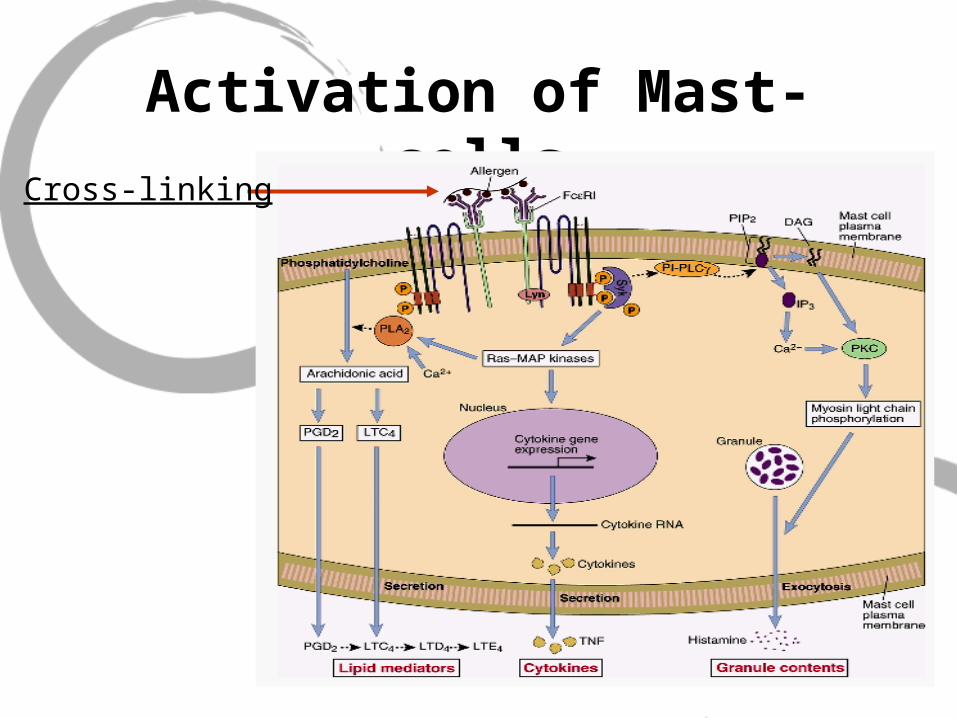
Activation of Mast-cellsCross-linking
Mast-Cell Mediators
• Inflammatory Mediators released
-Histamine
-Proteases (tryptase or chymase), acid hydrolases
-Proteoglycans (heparin, chondroitin sulfate)
Mast Cells: Lipid Mediators
• Prostaglandins D2
• Leukotrienes C4, D4, E4
• Platelet-activating factor
Mast-Cells: Cytokines
• IL-3: Promote mast cell proliferation
• IL-4, IL-5: Promote Th2 differentiation and IgE AB production
• TNF-, MIP-1 : Enhance inflammatory reaction
Allergen Induced Hypersensitivity
• Allergen: are antigens that induce production of specific IgE AB
• Examples: plant pollens, dust, animal hair, animal anti-serum, insect venom, chemicals, and foods
• Once the allergen reaches the sensitized mast cells, the allergen crosslinks the surface-bound IgE intracelluar Ca+2 and triggers degranulation of mediators
Atopy
• Atopy: Describes individuals that produce IgE AB in response to various environmental Ag and develop immediate hypersensitivity (Type I) responses.(Asthma, eczema, hay fever, and urticaria)
• These individuals normally have a strong family history (autosomal transmission of atopy)
Atopy
• HLA vs. Allergen Responsiveness-Some allergens response have a relationship to HLA-HLA-DR2 and HLA-A2: high responder to low dos of ragweed-HLA-B8: high responder to ragweed and also associated to other forms of hyperimmunity (autoimmunity)
IgE
• IgE blood concentrations are often increased in allergic disease and are grossly elevated in parasitic infections
• IL-4: promote B-cells to differentiate into IgE-producing specific cells
Eosinophil
• Th2 produce IL-5: Promotes the synthesis and secretion of IgA from B-cells and also important in stimulating eosinophil development and activation
• IL-4 and IL-5 production by Th2 cells may account for the eosinophilia seen in type I hypersensitivity and parasitemia
Two Types of Mast Cells
1) Connective tissue mast cells (CTMCs)
2) Mucosal mast cells (MMC)
Connective Tissue Mass Cells
• CTMCs are found most in blood vessels but vary in size and number of granules at different regions of the body
• Diseases such as Crohn’s disease, ulcerative colitis, and RA all present with increase in CTMCs
Types of Fc Receptors for IgE
• There are two types of receptors for IgE
1) FcRI (high affinity): Expressed on mast cells and basophils
2) FcRII (low affinity): Expressed by lymphocytes
Mast Cells Activation
• Cross-linking can be artificially induced with lectins such as PHA (Polyhydroxyaldehyde) and ConA
• These carbohydrates cross-link with IgE and cause degranulation
• This explains urticaria in individuals allergic to fruits (ie strawberries-contain large amt of lectin
Degranulation
• C’ products of C3a and C5a are very active in degranulating mast cells
• Compounds that affect Ca+2 influx into mast cells can induce degranulation
• Drugs such as morphine, codeine, synthetic ACTH can create clinical manifestations related to mast cells
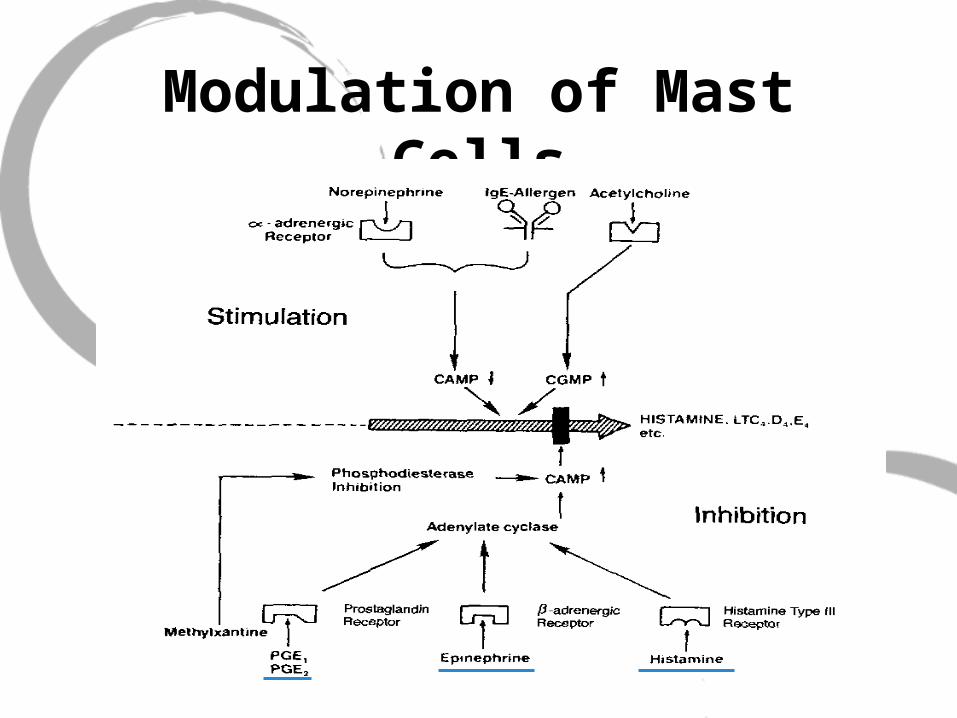
Modulation of Mast Cells
Therapy for Allergy
1) Agents that increase intracellular cAMP (-agonist)-inhibits contraction-Theophyllines: Prevents cAMP degradation
2) Blocking mediator release, such as sodium cromolyn: mechanism not clear, but seem to antagonize IgE-induced mediator release.
Therapeutics
• Direct Inhibitors
-Theophyllines, Xanthines
-Sodium cromolyn
-Epinephrine
-PGE1, PGE2• Indirect Inhibitor
-Glucocorticoids
Histamine Receptors
• H1- Bronchial
constriction- Musous secretion- Intestinal smooth
muscle contraction- Itching and pain at
sensory nerve endings
• H1 and H2- Reduces BP- Increase
permeability in skin• H2
- Gastric secretion in stomach
Antihistamines
• Nausea,vertigo,motion sickness
-Cyclizine
-Dimenhydrinate
-Diphenhydramine (Benadryl, Tylenol PM)
-Meclizine
• H1 Antagonists
-Promethazine (Phenergan)-Cetirizine (Zyrtec)-Desloratadine (Clarinex)-Fexofenadine (Allegra)-Loratadine (Claritin)
Type II Hypersensitivity
Type II
• Antibodies are directed against ag on particular cells/tissue or extracellular matrix, causing damage (ie RBC transfusion)
• These cell- or tissue-specific Ab cause diseases -Myasthenia Gravis: Ab blocks Ach-binding and cause muscle weakness and paralysis-Graves’ Disease: Ab stimulate TSH and casue hyperthyroidism)

Type II
Type II
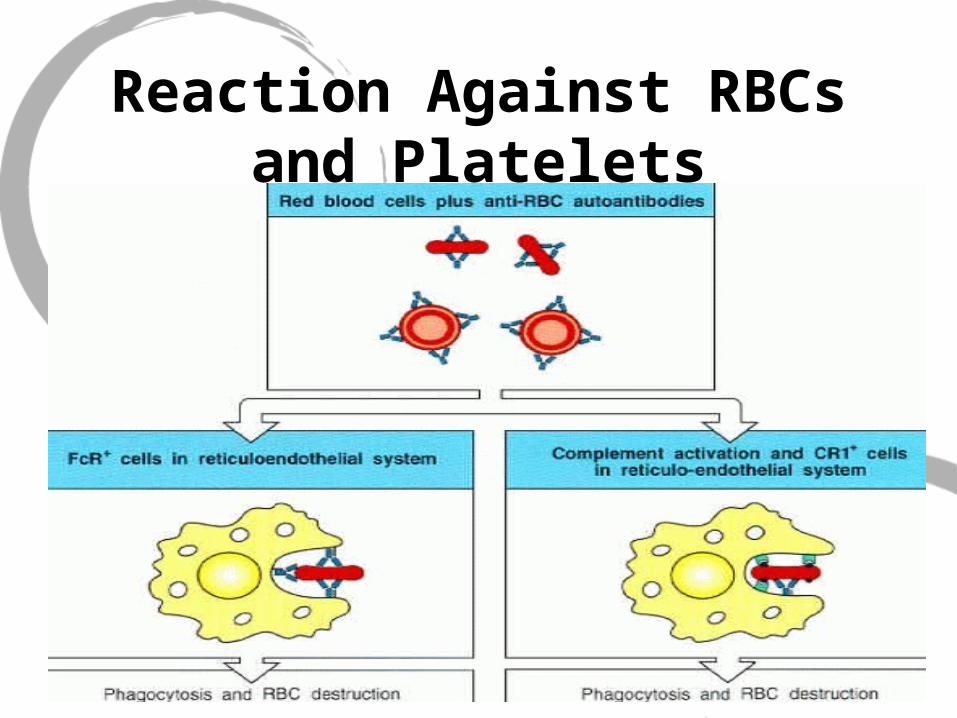
• Type II causes disease by 3 mechanism1) Opsonization and phagocytosis of cells2) Complement and Fc receptor-mediated inflammation and tissue injury3) Interference of normal cellular function by binding to important molecules or receptors
Reaction Against RBCs and Platelets
• Transfusion Reactions: There are 200 genetic variant of the RBC, but the ABO is the main designation
• The Rh system is also important because its cause of hemolytic disease in the newborn
Reaction Against RBCs and Platelets
• Hemolytic disease of the newborn (2nd born)
-RhoGam: It’s an Anti-Rh+ Antibody given to mother after the first born to prevent future complications in later newborns
• Autoimmune Hemolytic Anemia-When provoked by allergic reactions to certain drugs, including Penicillin, quinine, and sulphonamides
Reaction Against RBCs and Platelets
Idiopathic Thrombocytpenic Purpura (ITP)
• Autoantibody to platelets from the rapid removal of platelets from circulation
• Most often develop in women after bacterial or viral infections
• Associated with autoimmune disease Systemic Lupus Erythematosus (SLE)
Type II Mediated Autoimmune Diseases
• Myasthenia Gravis
• Graves’ Disease
• Insulin-resistance Diabetes
• Hemolytic Anemia
• Rheumatoid Arthritis
Advise of the Day
TYPE III & Type IV..To Be Continued…