hypertension - pathology research
DESCRIPTION
Hypertension - Pathology researchTRANSCRIPT


ContentNames ................................................3Systemic Hypertension .....................4-11Portal Hypertension .......................12-19Intracranial Hypertension ...............20-23Pulmonary Hypertension ................24-29
REFERENCES..................................30-31

NamesMahmoud GhonimAhmed NassarMohamed Hammad Ahmed RagabMostafa HarhashOmar MasoudMohamed KabeelMoaz SharsharIslam NaserIbrahim Kandeel
Hypertension
page
3
Under supervision of :Prof. Dr. Rehab SamakaDr.Asmaa Shams

Systemichypertension
page
4
Systemic hypertension
Definition:
Blood pressure is the force of blood pushing against the vascularwalls’ resistance .

Hypertension
page
5
Systemic hypertension means increased blood pressure above normalvalues
Diastolic Blood pressure(mmHg)
Systolic blood pressure(mmHg)
Category
< 80< 130Optimal< 85< 130Normal
85-89130-139High normalHypertension
90-99140-159mild (grade 1)100-109160-179moderate (grade 2)>= 110>= 180severe (grade 3)
Isolated SystolicHypertension
< 90> 140-159grade 1< 90>= 160grade 1
According to Aetiology hypertension is classified into Primary and secondary ;
1. Primary (essential) hypertension: a far more common condition and accounts for 95% of hypertension. The cause of essential hypertension is multifactor, that is, there are several factors whosecombined effects produce hypertension.Nevertheless, certain associations have been recognized in people with essential hypertension. For ex- ample, essential hypertension develops only in groups or societies that have a fairly high intake of salt,exceeding 5.8 grams daily. Salt intake may be a particularly important factor in relation to essential hy- pertension in several situations, and excess salt may be involved in the hypertension that is associated with advancing age, African American background, obesity, hereditary (genetic) susceptibility, and kidney failure (renal insufficiency
Genetic factors are thought to play a prominent role in the development of essential hypertension. How- ever, the genes for hypertension have not yet been identified. The current research in this area is focused on the genetic factors that affect the renin-angiotensin-aldosterone system. This system helps to regulateblood pressure by controlling salt balance and the tone of the arteries.
The vast majority of patients with essential hypertension have in common a particular abnormality of the arteries: an increased resistance (stiffness or lack of elasticity) in the peripheral arteries or arterioles. The arterioles supply oxygen-containing blood and nutrients to all of the tissues of the body. what makes the peripheral arteries become stiff is not known. Yet, this increased peripheral arteriolar stiffness is present in those individuals whose essential hypertension is associated with genetic factors, obesity, lack of exerciseoveruse of salt, and aging.
Aetiology:
Systemichypertension
page
6
2. Secondary hypertension, which accounts for 5% of hypertension, the high blood pressureis secondary to a specific abnormality in one of the organs or systems of the body Secondary hypertension is caused by a specific disorder of a particular organ or blood vessel, such as thekidney, adrenal gland, &pancrease…….
A. Renal (kidney) hypertension Diseases of the kidneys can cause secondary hypertension. One important cause of renal hypertension isRenal artery stenosis. In younger individuals, usually women, the narrowing is caused by a thicken-ing of the muscular wall of the arteries going to the kidney In older individuals, the narrowing gener-ally is due to hard, fat-containing (atherosclerotic) plaques that are blocking the renal artery.
The stenosis impairs the circulation to the kidneys Causing release of renin and angiotensin which leadsto Aldosterone secretion . this causes peripheral vasoconstriction leading to hypertension
Renal artery stenosis may be treated by balloon angioplasty.
Any of the other types of chronic kidney disease that reduces the function of the kidneys can also causehypertension due to hormonal disturbances and/or retention of salt.
It is important to remember that not only can kidney disease cause hypertension, but hypertension can also cause kidney disease. Therefore, all patients with high blood pressure should be evaluated for thepresence of kidney disease so they can be treated appropriately.
B. Adrenal gland tumors Adrenal gland tumors produce excessive amounts of adrenal hormones that cause high blood pressure.These tumors can be diagnosed from blood tests, urine tests, and imaging studies of the adrenal glands.
1. Primary hyperaldosteronism: because the tumor produces excessive amounts of the hormonealdosterone. In addition to the hypertension, this condition causes the loss of excessive amounts of potas-sium from the body into the urine, which results in a low level of potassium in the blood. Hyperaldos- teronism is generally first suspected in a person with hypertension when low potassium is also found inthe blood
2. Pheochromocytoma: This tumor produces excessive catecholamines, which include several adrenaline-related hormones. The diagnosis of a pheochromocytoma is suspected in individuals who have sudden and recurrent episodes of hypertension that are associated with flushing of the skin, rapidheart beating, and sweating, in addition to the symptoms associated with high blood pressure.
Mechanism :

Hypertension
page
7
C. The metabolic syndrome and obesityGenetic factors play a role in the constellation of findings that make up the «metabolic syndrome.» Indi-viduals with the metabolic syndrome have insulin resistance and a tendency to have type 2 diabetes mel- litus.Obesity, especially associated with a marked increase in abdominal girth, leads to high blood sugar, El-evated blood lipids, vascular inflammation, endothelial dysfunction (abnormal reactivity of the blood ves- sels), and hypertension. All leading to: premature atherosclerotic vascular disease.
The presence of hypertension must be confirmed by blood pressure measurements obtained with proper technique. Two readings separated by 2 minutes should be averaged. Hypertension is confirmed onlywhen an accurately measured blood pressure is high on 3 separate occasions.
The Sixth Report of the Joint National Committee on Prevention Detection, Evaluation, andTreatment of High Blood Pressure, designates 6 categories of blood pressure :
- Optimal—SBP less than 120 mm; DBP less than 80 mm
- Normal—SBP less than 130 mm; DBP less than 85 mm
- High normal—SBP is 130 to 139 mm; DBP is 85 to 89 mm
- Stage 1 hypertension—SBP is 140 to 159 mm; DBP is 90 to 99 mm
- Stage 2 hypertension—SBP is 160 to 179 mm; DBP is 100 to 109 mm
- Stage 3 hypertension—SBP is 180 mm or higher; DBP is 110 mm or higher
It is important to note that the recommended diagnostic evaluation not be considered evidence-based.
A complete history, physical examination, and limited diagnostic testing (urinalysis, complete bloodcount, potassium, sodium, fasting glucose, creatinine, total cholesterol, high-density cholesterol, and elec- trocardiogram) are recommended once the presence of hypertension has been confirmed. This evaluationhas 3 purposes:
1. Identify other cardiovascular risk factors. Most patients with hypertension have multiple car-diovascular risk factors at the time of initial evaluation. Risk factors include smoking, hyperlipidemia, dia- betes, age older than 60 years, sex (men or postmenopausal women), and family history of cardiovasculardisease in a female relative before age 65 years or a male relative before 55 years. This information is used to identify 3 risk groups: Group A includes patients with no other cardiovascular risk factor, cardiovascular disease, or evidence of end-organ damage; group B includes patients who do not have cardiovascular disease or end-organ damage but have 1 or more of the major risk factors other than diabetes mellitus; and group C includes patients who have cardiovascular disease, other end-organ damage, or diabetes mellitus. The risk associated with hypertension and the intensity of recommendedtreatment increases progressively as a person moves from risk group A through risk group C.
DIAGNOSIS:
Systemichypertension
page
8
2. Identify end-organ damage. Evidence of end-organ damage includes left ventricular hypertro- phy, angina, previous myocardial infarction, previous angioplasty or coronary revascularization, heartfailure, stroke or transient ischemic attack, nephropathy, peripheral arterial disease, and retinopathy.
3. Identify secondary causes of hypertension. Estimating the pretest probability of a secondary(identifiable) cause of hypertension is problematic, because referral bias is a major problem in hyperten- sion prevalence studies; patients are typically included in these studies only after being referred to a study center by their primary care physician for resistant or difficult to control hypertension. On the basis of thebest available estimates, it would be reasonable to assume that patients presenting to primary care physi-cians have a 5% probability of an identifiable cause of hypertension.
Patients whose initial history, physical, and laboratory evaluation suggest the possibility of a secondarycause of hypertension should undergo additional testing. The search for the secondary cause of hyper-
tension should focus on chronic renal disease, renovascular hypertension, pheochromocytoma, Cushing syndrome, and primary aldosteronism, depending on the clinical scenario
Chronic renal disease will be evident from the blood urea nitrogen, creatinine, and the urinalysis results.The diagnostic approach to other causes of hypertension is more complicated.
Although renal artery stenosis is suggested by the presence of an abdominal or flank bruit, it is an insen- sitive test (sensitivity=65%; specificity=90%). It is useful when positive (positive likelihood ratio=6.5)but does not rule out renal artery stenosis when negative (negative likelihood ratio=0.4). A clinical deci- sion rule has been developed and validated that integrates several findings from the history and physicalexamination. Software to implement this decision rule in clinical practice, using Palm or PocketPC hand-held computers, is available at no charge from the JFP Web site at PC download. Duplex sonography is very accurate (sensitivity=98%; specificity=98%) when the study is adequate but is often nondiagnostic in obese patients. For these patients, magnetic resonance angiography (MRA) isbetter (sensitivity=93%; specificity=95%). Captopril renal scanning (CRS) is less sensitive and less spe- cific than either sonography or MRA. Renal artery stenosis is confirmed by the highly accurate but moreinvasive reference standard test of conventional angiography. Pheochromocytoma is rare even in the presence of suggestive symptoms (headache, palpitations, andexcessive and inappropriate perspiration), but failure to identify this disease can have disastrous conse-quences. Therefore, patients who have suggestive signs and symptoms should be screened for pheochro- mocytoma. However, the standard for screening pheochromocytoma remains controversial. A 24-hour urinary metanephrine (cutoff point of >3.70 nmol/day ) is highly sensitive and specific when done well, but urine collection is inconvenient and may be incomplete. Plasma metanephrines (metanephrine >0.66 nmol/L or normetanephrine >0.30 nmol/L) are easy to obtain, 100% sensitive, and may represent a good screening test for pheochromocytoma. Because they have limited specificity (85%), a positive plasma metanephrine should be confirmed by the 24-hour urinary metanephrine-to-creatinine ratio (cutoff pointof >0.354; specificity=98%) before proceeding to anatomical localization of the tumor. Two imaging studies are commonly used to localize pheochromocytomas. Metaiodobenzylguanidine
Diagnostic Strategy

Hypertension
page
9
(MIBG) scintigraphy is more specific but less sensitive than computed tomography (CT). Relying on CT to guide surgery is less likely to miss tumors than MIBG scintigraphy (CT sensitivity = 100% vs MIBG=88%) but is more likely to result in unnecessary surgery because of the lower specificity (CTspecificity = 50%; MIBG=89%).
The 24-hour urinary free cortisol (cutoff point >90 mg/day; sensitivity=100%; specificity=98%) is a use- ful screening test for Cushing syndrome. It is very sensitive, but false-positives may be seen in patientswith depression and polycystic ovarian syndrome. The single-dose (1 mg) overnight dexamethasone sup- pression test is equally sensitive but is a little less specific than the 24-hour urinary cortisol. However, this test is relatively simple for patients. The patient takes 1 mg of dexamethasone at midnight, and the plasma cortisol level is drawn in the morning (cutoff point >100 nmol). The combined dexamethasone and corticotropin-releasing hormone (CRH) suppression test, which has both a sensitivity and a specificity of almost 100%, can be used to confirm the diagnosis of Cushing syndrome. However, it is a little more complicated for the patient. The patient takes 0.5 mg of dexamethasone at noon on the first day and repeats this dose every 6 hours for a total of 8 doses (ending at 6 am on the third day). Two hours after the last dose the patient is given an intravenous bolus of CRH (1 μg/kg), and 15 minutes later a plasma cortisol isdrawn. A cortisol level greater than 38 nmol is the cutoff point for this test. The coexistence of hypertension and spontaneous or diuretic-induced hypokalemia is strongly suggestive of primary aldosteronism. However, it is important to remember that many (if not most) patients withprimary aldosteronism do not have hypokalemia. In the past, screening for primary aldosteronism was ac- complished by measuring urinary aldosterone levels after oral or intravenous salt loading. The sensitivity of these tests is 90% to 95%, and they carry a risk of precipitous elevation of blood pressure due to volumeexpansion or hypokalemia. Measuring the plasma renin and aldosterone levels can be used to test for hy- peraldosteronism. Various cut points and ratios have been suggested, but the plasma aldosterone-to-renin ratio (cutoff point >25) is currently the most useful screening test for hyperaldosteronism. For this test the patient is asked to rise at 6 am and remain ambulatory for 2 hours, at which time the plasma aldosterone and renin levels are drawn. Beta-blockers and dihydropyridine calcium channel blockers must be stopped for 2 weeks, and spironolactone and loop diuretics must be stopped for 6 weeks before the test. Primaryaldosteronism can be confirmed by the fludrocortisone suppression test.
The goal of treatment is to reduce blood pressure so that you have a lower risk of complications. You andyour health care provider should set a blood pressure goal for you.
1. Pharmacologically :
There are many different medicines that can be used to treat high blood pressure, including:• Alpha blockers• Angiotensin-converting enzyme (ACE) inhibitors• Angiotensin receptor blockers (ARBs)• Beta blockers• Calcium channel blockers• Central alpha agonists• Diuretics• Renin inhibitors, including aliskiren (Tekturna)• Vasodilators
Treatment:

Systemichypertension
page
10
Your health care provider may also tell you to exercise, lose weight, and follow a healthier diet. If you have pre-hypertension, your health care provider will recommend the same lifestyle changes to bringyour blood pressure down to a normal range. Often, a single blood pressure drug may not be enough to control your blood pressure, and you may need to take two or more drugs. It is very important that you take the medications prescribed to you. If youhave side effects, your health care provider can substitute a different medication.
2. Non Pharmacologically :
In addition to taking medicine, you can do many things to help control your blood pressure, including:• Eat a heart-healthy diet, including potassium and fiber, and drink plenty of water.• Exercise regularly -- at least 30 minutes a day.• If you smoke, quit -- find a program that will help you stop.• Limit how much alcohol you drink -- 1 drink a day for women, 2 a day for men.• Limit the amount of sodium (salt) you eat -- aim for less than 1,500 mg per day.• Reduce stress -- try to avoid things that cause stress for you. You can also try meditation or yoga.• Stay at a healthy body weight -- find a weight-loss program to help you, if you need it.
Lifestyle changes are important for everyone, and patients should routinely monitor their blood pressureat home. Drug treatment needs to be planned on an individual basis. About 30% of patients with hyper-tension are not treated at all, and less than 50% have adequately controlled blood pressure. It is not always clear when drugs should be started, particularly for people with prehypertension or mild high blood pressure. To help make treatment choices, the U.S. National Heart, Lung, and Blood Institutehas created categories (groups A, B, and C) according to a patient’s risk factors for heart disease. Apply- ing these categories to the severity of hypertension helps determine whether lifestyle changes alone ormedications are needed .
Side Effects and Problems in Compliance. One of the most difficult issues that patients face, is that the treatment may make them feel worse than the disease, which usually has no symptoms. Whatever the difficulties, compliance with a drug and lifestyle program is worth the effort. It is very important thatpatients discuss medication concerns with their doctors. If current blood pressure drugs are causing un-comfortable side effects, the doctor may adjust dosages or combinations.
Withdrawal from Anti-Hypertensive Medications. Patients whose blood pressure has beenwell-controlled and who are able to maintain a healthy life style may be able to withdraw from medica- tions. They should do so in a step-down manner (gradual reduction) and be monitored regularly. Stopping too quickly can have adverse effects, including serious effects on the heart. The highest success rates are more likely in those who lose weight and reduce sodium intake, in patients who have been treated with a single drug, and in those who have maintained lower systolic blood pressure during treatment. People over 75 years old may have more trouble than younger adults in maintaining normal blood pressure afterwithdrawal.
Hypertension
page
11
Treatment of Resistant Hypertension
Some patients are unable to meet target blood pressure goals despite consistently following a treatmentplan that includes three or more medications. Factors that contribute to resistant hypertension include old- er age (especially age 75 or older), high baseline blood pressure, and medical conditions such as obesity, sleep apnea, diabetes, and chronic kidney disease. Treating any underlying medical condition is important for helping control blood pressure. Patients should be sure to adhere to lifestyle changes (weight loss and dietary changes) and may require modifications to their drug regimens. Patients with severe resistant hypertension should consider seeking a consultation with a doctor who specializes in treating high bloodpressure.
Treatment of Children
Children with high blood pressure should first be treated with lifestyle changes, including weight reduc- tion, increased physical activity, and diet modification. If blood pressure is not controlled with lifestylechanges, drug treatment may be required. Results of studies evaluating outcomes of children with hyper- tension suggest that early abnormalities, including enlarged heart and abnormalities in the kidney and eyes, may occur even in children with mild hypertension. Children and adolescents with hypertensionshould be monitored and evaluated for any early organ damage. Secondary hypertension (high blood pres-sure due to another disease or drug) is more common in children than adults. abnormalities in the kidney and eyes, may occur even in children with mild hypertension. Children and adolescents with hypertension should be monitored and evaluated for any early organ damage. Secondaryhypertension (high blood pressure due to another disease or drug) is more common in children than adults.
Prevention
Lifestyle changes can help you prevent high blood pressure. These changes are especially impor- tant for people who have risk factors for high blood pressure that cannot be changed, including familyhistory, race, or age. Here are some things you can do :
• Stay at a healthy weight. • Eat less salt.• Get regular exercise • Cut back on drinking. • Eat heart-healthy foods.
Portalhypertension
page
12
Portal hypertension
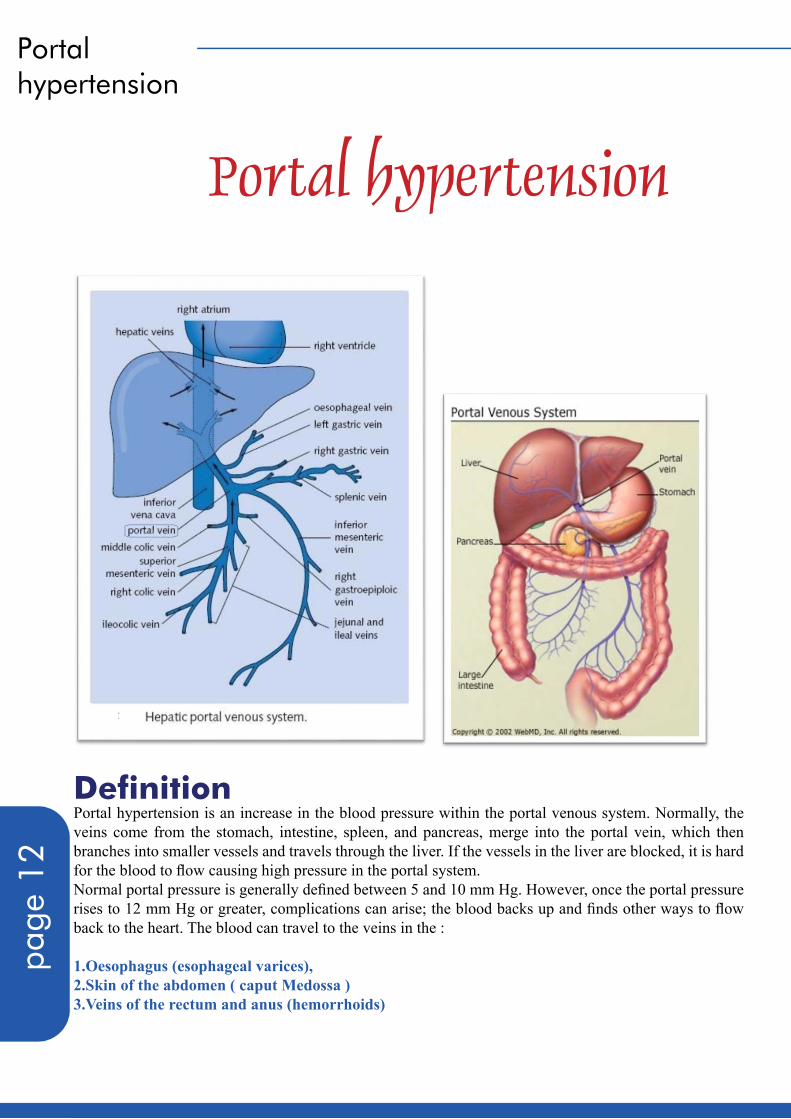
Definition Portal hypertension is an increase in the blood pressure within the portal venous system. Normally, the veins come from the stomach, intestine, spleen, and pancreas, merge into the portal vein, which then branches into smaller vessels and travels through the liver. If the vessels in the liver are blocked, it is hardfor the blood to flow causing high pressure in the portal system. Normal portal pressure is generally defined between 5 and 10 mm Hg. However, once the portal pressure rises to 12 mm Hg or greater, complications can arise; the blood backs up and finds other ways to flowback to the heart. The blood can travel to the veins in the :
1.Oesophagus (esophageal varices), 2.Skin of the abdomen ( caput Medossa ) 3.Veins of the rectum and anus (hemorrhoids)

Hypertension
page
13
Aetiology : Portal hypertension can be classified according to the cause into :
1. Intrahepatic:
A. Post-sinusoidal :- Hepatic cirrhosis- Acute alcoholic hepatitis - Schistosomiasis (advanced stage) - Primary biliary cirrhosis (advanced stage) - Idiopathic portal hypertension (advanced stage) - Acute and fulminant hepatitis - Congenital hepatic fibrosis - Vitamin A toxicity:
- Peliosis hepatitis - Venoocclusive disease - Budd-Chiari syndrome
B.Pre-sinusoidal :- Schistosomiasis (early stage) - Primary biliary cirrhosis (early stage) - Idiopathic portal hypertension (early stage) - Nodular regenerative hyperplasia:
- Polycystic disease - Hepatic metastasis - Granulomatous diseases (sarcoidosis, tuberculosis):
Noncirrhotic portal fibrosis is observed with various toxic injuries, and one of these includes vitamin A toxicity. This probably is due to vascular injury. Excessive doses of vitamin A taken for months or years can lead to chronic hepatic disease. Intake of doses ranging from as small as 3-fold the recommended daily dose continued for years to doses as high as 20-fold the approved dose in a few months can lead to hepatic disease. The pericellular fibrosis characteristic of vitamin A toxicity may lead to portal hypertension.
Pathogenesis probably is obliterative venopathy. The presence of nodules that press on the portal system also has been postulated to play a role, although nodularity is present in most cases without clinical evidence of portal hypertension.Myeloproliferative diseases: These act by direct infiltration by malignant cells
Clinical liver dysfunction is rare in sarcoidosis. Portal hypertension is an unusual, althoughwell-recognized manifestation of hepatic sarcoidosis. Sarcoid granulomas frequently lo- calize in the portal areas, resulting in injury to the portal veins.

Portalhypertension
page
14
2. Prehepatic:
- Portal vein thrombosis[5]- Splenic vein thrombosis - Congenital atresia or stenosis of portal vein - Extrinsic compression (tumors) - Splanchnic arteriovenous fistula
3. Post hepatic: - Inferior vena cava (IVC) obstruction - Right heart failure - Constrictive pericarditis - Tricuspid regurgitation - Budd-Chiari syndrome - Arterial-portal venous fistula - Increased portal blood flow - Increased splenic flow
Pathophysiology Applying Ohm’s Law to vascular flow, i.e., P = FR, where P is the pressure gradient through the portal venous system, F is the volume of blood flowing through the system, and R is the resistance to flow. Changes in either F or R affect the pressure. In most types of portal hypertension, both the blood flow and the resistance to blood flow are altered.
1.Increase in vascular resistance The initial factor in the pathophysiology of portal hypertension is the increase in vascular resistance to the portal blood flow.Changes in portal vascular resistance are determined primarily by blood vessel radius. Because portal vas- cular resistance is indirectly proportional to the fourth power of the vessel radius, small decreases in thevessel radius cause large increases in portal vascular resistance and, therefore, in portal blood pressure .Liver disease is responsible for a decrease in portal vascular radius, producing a dramatic increase in por- tal vascular resistance. In cirrhosis, the increase occurs at the hepatic microcirculation (sinusoidal portal hypertension). Increased hepatic vascular resistance in cirrhosis is not only a mechanical consequence of the hepatic architectural disorder, but a dynamic component also exists due to the active contraction of myofibroblasts, activated stellate cells, and vascular smooth-muscle cells of the intrahepatic veins.Endogenous factors and pharmacological agents that increase hepatic vascular resistance include endothe- lin, alpha-adrenergic agonists, and angiotensin II.
2.Increase in portal blood flow The second factor that contributes to the pathogenesis of portal hypertension is the increase in blood flowin the portal veins, which is established through splanchnic arteriolar vasodilatation caused by an exces- sive release of endogenous vasodilators (eg, endothelial, neural, humoral). The increase in portal blood flow aggravates the increase in portal pressure and contributes to why portal hypertension exists despite the formation of an extensive network of portosystemic collaterals that may divert as much as 80% of portal blood flow.

Hypertension
page
15
Manifestations of splanchnic vasodilatation include increased cardiac output, arterial hypotension, andhypervolemia. This explains the rationale for treating portal hypertension with a low-sodium diet and diu-retics to attenuate the hyperkinetic state.
Differential Diagnosis:
- Budd-Chiari Syndrome- Cirrhosis - Myeloproliferative Disease - Pericarditis, Constrictive - Polycystic Kidney Disease - Sarcoidosis - Schistosomiasis - Tricuspid Regurgitation - Tuberculosis - Vitamin A Toxicity
Complications:

Portalhypertension
page
16
Oesophageal Varices: An elevated portal venous pressure (>10 mm Hg) distends the veins proximal to the site of the block andincreases capillary pressure in organs drained by the obstructed veins. Because the portal venous system lacks valves, resistance at any level between the right side of the heart and the splanchnic vessels results in retrograde flow of blood and transmission of elevated pressure. Theanastomoses connecting the portal and systemic circulation may enlarge to allow blood to bypass the ob- struction and pass directly into the systemic circulation. “Studies have demonstrated the role of endothelin-1 (ET-1) and nitric oxide (NO) in the pathogenesis ofportal hypertension and esophageal varices.[2, 4] ET-1 is a powerful vasoconstrictor synthesized by sinu- soidal endothelial cells that has been implicated in the increased hepatic vascular resistance of cirrhosis and in the development of liver fibrosis. NO is a vasodilator substance that is synthesized by sinusoidal endothelial cells. In the cirrhotic liver, the production of NO is decreased, and endothelial nitric oxidesynthase (eNOS) activity and nitrite production by sinusoidal endothelial cells are reduced.”Gastro esophageal varices have 2 main inflows, the first is the left gastric or coronary vein. The other ma- jor route of inflow is the splenic hilus, through the short gastric veins. The gastro esophageal varices are important because of their propensity to bleed. Studies of hepatic microcirculation have identified several mechanisms that may explain the increasedintrahepatic vascular resistance. These mechanisms may be summarized as follows:
- A reduction of sinusoidal caliber due to hepatocyte enlargement - An alteration in the elastic properties of the sinusoidal wall due to collagen deposition in the space of Disse- Compression of hepatic venules by regeneration nodules - Central vein lesions caused by perivenous fibrosis - Venoocclusive changes - Perisinusoidal block by portal inflammation, portal fibrosis, and piecemeal necrosis
The following are risk factors for variceal hemorrhage:
- Variceal size: The larger the varix, the higher the risk of rupture and bleeding. However, patients may bleed from small varices too.- The presence of endoscopic red color signs (eg, red whale markings, cherry red spots) - The Child classification, especially the presence of ascites, increases the risk of hemorrhage. - Active alcohol intake in patients with chronic alcohol-related liver diseases - Local changes in the distal esophagus (eg, gastroesophageal reflux) have been postulated to increase the risk of variceal hemorrhage.
However, evidence to support this view is weak. Studies indicate that gastroesophageal reflux does not initiate or play a role in esophageal hemorrhage. A well-documented association exists between variceal hemorrhage and bacterial infections, and this mayrepresent a causal relationship. Infection could trigger variceal bleeding by a number of mechanisms, including the following:
- The release of endotoxin into the systemic circulation - Worsening of hemostasis - Vasoconstriction induced by contraction of stellate cells

Hypertension
page
17
Ascites:Ascites takes place when excess fluid accumulates in the peritoneal cavity. Low albumin levels in the blood as associated with portal hypertension is also a contributing factor. The obvious signs of ascites are a swollen belly (abdomen). At that point evaluation tests on the liver maybe performed which include urinalysis, and kidney function testing. Common treatment includes diuretics, limiting salt in the diet, antibiotics (if infection is present), not to mention the avoidance of alcohol. If the patient does not respond to the common treatments, then the placement of a tube in the abdomen may be used to drain large amounts of fluid from the area. Lastly aTransjugular Intrahepatic Portosystemic Shunt (TIPS) is a radiology technique that reduces portal pres- sure and may be the most effective treatment for patients with ascites that are resistant to diuretics. The procedure is performed with the patient under conscious sedation or general anaesthesia. A radiologistplaces a stint through the skin from the right jugular vein into the hepatic vein. A connection is made be- tween the portal and systemic circulations.
Splenomegaly:
Diagnosis
1. Laboratory Studies: Lab studies are directed towards investigating etiologies of cirrhosis, which is the most common cause ofportal hypertension. Lab studies include the following:- Liver function tests - Prothrombin time - Albumin - Viral hepatitis serologies - Platelet count - Antinuclear antibody, antimitochondrial antibody, antismooth muscle antibody - Iron indices - Alpha1-antitrypsin deficiency - Ceruloplasmin, 24-hour urinary copper - To be considered only in individuals aged 3-40
years who have unexplained hepatic, neurologic, or psychiatric disease
One of the most common findings with portal hyper- tension is splenomegaly, as seen here. The spleen isenlarged from the normal 300 grams or less to be- tween 500 and 1000 gm. Another finding here is the irregular pale tan plaques of collagen over the purplecapsule known as “sugar icing” or “hyaline perisple- nitis” which follows the splenomegaly and/or multipleepisodes of peritonitis that are a common accompani-ment to cirrhosis of the liver.
Portalhypertension
page
18
2. Imaging Studies:
- Duplex-Doppler ultrasonography Ultrasound (US) is a safe, economical, and effective method for screening for portal hypertension. It also can demonstrate portal flow and helps in diagnosing cavernous transformation of the portal vein, portal vein thrombosis, or splenic vein thrombosis.[6]Features suggestive of hepatic cirrhosis with portal hypertension include the following:
•Nodular liver surface is suggestive. However, this finding is not specific for cirrhosis and can be observed with congenital hepatic fibrosis and nodular regenerative hyperplasia.•Splenomegaly is a suggestive finding.•Patients may demonstrate the presence of collateral circulation
Limitations of US include the following:
•Reproducibility of data is problematic.•Many variables, such as circadian rhythm, meals, medications, and the sympathetic nervous sys-tem, affect portal hemodynamics.•Significant interobserver and intraobserver variation exist in quantitative ultrasonographic meas-urement.
- CT scan CT scan is a useful qualitative study in cases where sonographic evaluations are inconclusive.
CT scan is not affected by patients’ body habitus or the presence of bowel gas. With improvement of spiral CT scan and 3-dimensional angiographic reconstructive techniques, portal vasculature may be visualized more accurately.
Findings suggestive of portal hypertension include the following:• Collaterals arising from the portal system are suggestive of portal hypertension.• Dilatation of the IVC also is suggestive of portal hypertension.Limitations of CT scan include the following:• It cannot demonstrate the venous and arterial flow profile.• Intravenous contrast agents cannot be used in patients with renal failure or contrast allergy.
- MRIMRI provides qualitative information similar to CT scan when Doppler findings are inconclusive. MRI angiography detects the presence of portosystemic collaterals and obstruction of portal vasculature.MRI also provides quantitative data on portal venous and azygos blood flow.
- Liver-spleen scanThis is described for historical interest only.Liver-spleen scan uses technetium sulfur colloid taken up by cells in the reticuloendothelial system.A colloidal shift from the liver to the spleen or bone marrow is suggestive of increased portal pressure. Limitations include the following:• Portal hypertension cannot be ruled out in the absence of this shift.• Liver-spleen scan images lack spatial resolution.• It has been superseded by US and CT scan.

Hypertension
page
19
Procedures:
- Hemodynamic measurement of portal pressure:
Direct portal measurements usually are not performed due to the invasive nature, the risk of complica-tions, and the interference of anesthetic agents on portal hemodynamics. The most commonly used meth- od is measurement of the hepatic venous pressure gradient (HVPG), which is an indirect measurement thatclosely approximates portal venous pressure. A fluid-filled balloon catheter is introduced into the femoral or internal jugular vein and advanced under fluoroscopy into a branch of the hepatic vein. Free hepatic venous pressure (FHVP) then is measured. The balloon is inflated until it is wedged inside the hepatic vein, occluding it completely, thus equalizing the pressure throughout the static column of blood. The occluded hepatic venous pressure (ie, wedged hepatic venous pressure) minus the unoccluded, or free, portal venous pressure (ie, FHVP) is the HVPG.
- Endoscopy:
Perform upper endoscopy, as appropriate, to screen for varices in every patient with suggestive findings of portal hypertension. Additionally, all patients with cirrhosis should be considered for the presence of varices at the time of the initial diagnosis of cirrhosis. Gastroesophageal varices confirm the diagnosis of portal hypertension; however, their absence does not rule it out. At times, gastroesophageal varices are incidental findings in patients undergoing upper endoscopy for other reasons (eg, dyspepsia refractory to medications, dysphagia, weight loss). These patients should undergo further investigations for etiologiesof portal hypertension. Various indirect indices, such as platelet count, spleen size, albumin, and Child-Pugh score, have been studied to help diagnose varices without endoscopy. A recent case review study revealed some of thesepredictors as unreliable. For the time being, endoscopy remains the criterion standard for screening pa-tients with cirrhosis for varices. In compensated patients without varices, repeat endoscopy at 2- to 3-year intervals to evaluate for thedevelopment of varices.In compensated patients with small varices, repeat endoscopy at 1- to 2-year intervals to evaluate the pro- gression of varices.
Intracranialhypertension
page
20
Introduction:Intracranial hypertension means that the pressure of cerebrospinal fluid (CSF) within the skull is too high.
Cerebrospinal fluid is one of three major components inside the skull; the other two are the bloodsupply that the brain requires to function and the brain itself. Under normal circumstances, these components work together in a delicate balance. A pressure and vol- ume relationship exists between CSF, the brain and the vasculature. But since the skull is made of bone and cannot expand, an increase in the volume of any one component is at the expense of the other two components. For example, if the brain swells and becomes enlarged, it simultaneously compresses bloodvessels, causing the sub-arachnoid space to fill with more spinal fluid. This results in an increase in intrac- ranial pressure (i.e. cerebrospinal fluid pressure), as well as a decrease in blood flow.
CSF has several important functions. It cushions the brain within the skull, transports nutri- ents to brain tissue and carries waste away.
CSF is produced at a site within the brain called the choroid plexus, which generates about 400-500 ml. (one pint) of the fluid each day or approximately 0.3 cc per minute. (The total volume of CSF in the skull at any given time is around 140 ml. That means the body produces, absorbs and replenishes the totalvolume of CSF about 3-4 times daily.)
When the body cannot effectively absorb or drain CSF, intracranial pressure increases within the fixed space of the skull. And since the brain and the vasculature can only be compressed so far, intracranial pressure must rise.
Intracranial hypertension in adults is generally defined as intracranial pressure .
Intracranial Hypertension

Hypertension
page
21
Causes:Causes of increased intracranial pressure can be classified by the mechanism in which ICP is increased:
1. Mass effect such as brain tumor, infarction with edema, contusions, subdural or epidural hema-toma, or abscesses all tend to deform the adjacent brain.2. Generalized brain swelling can occur in ischemic-anoxia states, acute liver failure, hyper- tensive encephalopathy, pseudotumor cerebri, hypercarbia, and Reye hepatocerebral syndrome. Theseconditions tend to decrease the cerebral perfusion pressure but with minimal tissue shifts.3. Increase in venous pressure can be due to venous sinus thrombosis, heart failure, or ob-struction of superior mediastinal or jugular veins. 4. Obstruction to CSF flow and/or absorption can occur in hydrocephalus (blockage inventricles or subarachnoid space at base of brain, e.g., by Arnold-Chiari malformation), extensive menin- geal disease (e.g., infection, carcinoma, granuloma, or hemorrhage), or obstruction in cerebral convexitiesand superior sagittal sinus (decreased absorption).
Schematic Drawing of Cerebrospinal Fluid Circulation. Elevated CSF pressure is transmitted around the brain and along the optic nerve (sub-arachnoid space)
producing papilledema.
Intracranialhypertension
page
22
5. Increased CSF production can occur in meningitis, subarachnoid hemorrhage, or choroidplexus tumor.
6. Idiopathic or unknown cause (idiopathic intracranial hypertension)7. Cerebral venous sinus thrombosis8. Acute liver failure[13]9. Craniosynostosis
Benign Intracranial Hypertension Also termed: idiopathic intracranial hypertension or Pseudotumour cerebri
Incidence Benign intracranial hypertension is an extremely rare disease. Studies from various countries estimate that the annual incidence is at the figure of 0.9 per 100,000 of general population. This figure is increased inwomen after puberty and in women with their weight 20% or more of the ideal weight.
Risk Factors Gender is a major risk factor for BIH. Before puberty, boys and girls are affected equally. After puberty, BIH affects women 9 times as often as men. Obesity is a risk factor as well, considering that the incidence rises sharply with women 20% or moreabove their ideal weight.
ProgressionThe pathogenesis of benign intracranial hypertension is still uncertain despite the fact that it has been de- scribed more than 100 years ago. Benign intracranial hypertension is characterized by:• Increased intracranial pressure;• Lack of ventricular dilatation (ventricles are fluid filled cavities in the middle of the brain);• Predilection for young, obese women;• Induced by various medications, including tetracyclines, vitamin A and oral contraceptive pills.
The exact mechanism of benign intracranial hypertension is still under debate at the moment. With pro-longed high pressure in the brain, eye changes and brain changes may occur.
SymptomsBenign intracranial hypertension can produce features similar to high blood pressure at first. After a pro- longed period, there might be complications from benign intracranial hypertension like visual problems.
Possible symptoms of benign intracranial hypertension include:
• Headache;• Momentary visual disturbances; • Tinnitus (ringing noise in the ear with no external stimuli), sometimes like heart beating andwhooshing sound;
Hypertension
page
23
• Blindness: this can just be blurred vision, partial blindness or total blindness;• Double vision;• Other minor symptoms such as neck stiffness, painful shoulder joints, wrist joints and knees, dif-ficulty maintaining balance, etc.
Diagnosis If a patient comes in with persistent headache and eye pathology, most likely a full physical examination will be necessary. These include looking at the blood function, kidney function, liver function, thyroidfunction, and the body’s iron, vitamins and electrolytes level.The diagnosis of BIH depends upon ruling out other diseases; it is thus a diagnosis of exclusion. The fol- lowing special investigations can be done: • Neuroimaging: these are imaging studies for the brain, including CT scan and MRI scan of the brain. Sometimes a more specific MRI scan called MRV (magnetic resonance venography) may be doneto look at the blood flow in the veins. • Lumbar puncture: this test involves accessing the spinal cavity through the back using a long needle under local anaesthesia. This will help to measure the CSF pressure in the cavity, which will beraised in BIH.
Prognosis Benign intracranial hypertension does not increase the death rate by itself, rather, the death rate is increased by morbid obesity which is a common association with benign intracranial hypertension. However, it does cause significant inconvenience to the patients. Eye changes can be a mortal complication of untreated benign intracranial hypertension, leading to permanent blindness. As many as 96% of the patients with benign intracranial hypertension have some degree of visual changes.
TreatmentTreatment of benign intracranial hypertension needs multiple team approach, including neurologist, oph- thalmologist, neurosurgeon and general practitioners. Treatment strategies include: • Diet and weight loss: This can either be achieved on patient self-discipline alone or with the help of medications and surgery. There have been positive improvements on signs and symptoms where patients have lost significant amount of weight. • Medications: Traditionally, diuretics (fluid tablets that removes water from the body) have been used. One such example is acetazolamide. However, it has significant side effects unpleasant taste with carbonated drinks, altered taste sensation, etc. Otherwise, other diuretics such as furosemide, thiazides, spironolactone, and triamterene can be used but with varying results. Steroids can be used to reduce the pressure in the brain rapidly but they are not suitable for long-term use. • Supportive care: A persistent headache can be treated by standard pain relief medications. • Surgery: This is indicated for visual loss or worsening visual changes due to the disease. They aim toreduce the pressure that compresses on the nerve in the eye that is responsible for normal vision.

Pulmonaryhypertension
page
24
DefinitionThe portion of the circulation that distributes the blood from the right side of the heart to the lungs is re- ferred to as the pulmonary (lung) circulation. The pulmonary arteries are the major blood vessels that carry blood from the right side of the heart to the lungs.
When pressure in the pulmonary circulation becomes abnormally elevated, it is referred to as pulmonaryhypertension, pulmonary artery hypertension, or PAH.
“Pulmonary hypertension results from constriction, or stiffening, of the pulmonary arteries that supply blood to the lungs. Consequently, it becomes more difficult for the heart to pump blood forward through the lungs. This stress on the heart leads to enlargement of the right heart and eventually fluid can build upin the liver and other tissues, such as the in the legs “
Classification The conventional classification,
Pulmonary hypertension, which is also called pulmonary arterial hypertension, is divided into two main categories;1) Primary pulmonary hypertension (not caused by any other disease or condition)
2) Secondary pulmonary hypertension (caused by another underlying condition).
Secondary pulmonary hypertension is much more common than primary pulmonary hypertension.
A newer classification,
based on the main underlying cause of pulmonary hypertension,This system classifies the condition basedon whether it is due to:
1. Pulmonary hypertension from a variety of causes, some known and others unknown, such as: drug-induced pulmonary artery hypertension,2. pulmonary artery hypertension associated with collagen vascular diseases, HIV, and schistoso- miasis (a parasitic infection), and3. pulmonary arterial hypertension of unknown cause (idiopathic pulmonary arterial hypertension)
Pulmonary hypertension

Hypertension
page
25
4. Pulmonary arterial hypertension from left-sided heart disease, often referred to as pulmonary venous hypertension, including thickening of the heart muscle, decrease heart pump function, anddisorders of the heart valves
5. Pulmonary arterial hypertension associated with lung disease and or persistent drop in oxygenlevels (hypoxia) including: - COPD (chronic obstructive pulmonary disease), - sleep apnea, - pulmonary fibrosis, and- living at high elevations
6. Pulmonary arterial hypertension from blood clotting disorders that deliver clots to the lung (pul- monary emboli) or are formed directly in the lung arteries (pulmonary thrombosis), also known aschronic thromboembolic pulmonary hypertension;
7. Pulmonary arterial hypertension from miscellaneous causes with unclear multifactorial mecha-nisms; including diseases such as: - sarcoidosis, - tumor obstruction, - metabolic disorders (glycogen storage disease), and- kidney failure
Aetiology/Causes:There are many causes of pulmonary hypertension. Often more than one mechanism is involved in a spe-cific disease process. This can also change as the disease progresses.
1. Diseases that affect blood flow out of the heart to the rest of the body: result in backflowof blood (stacking of blood) that raises pulmonary venous pressures leading to pulmonary hypertension.
2. Hypoxic pulmonary vasoconstriction: is the process in which the lung vessels narrow in attempt to divert blood from poorly functioning segments of the lung. For instance, when pneumonia develops, a portion of lung becomes inflamed and works poorly in performing the functions of the lung. This process diverts blood from these poorly working areas and sends it to better functioning lung tissue. However, a problem develops when all the blood has a low oxygen level (hypoxia). This causes constriction of thevessels on the pulmonary arterial side and hence raises the pressure.
3. Remodeling of blood vessels also occurs in some diseases: whereby the inner lining (lu- men) of the vessel becomes narrowed due to inappropriate growth of the tissue within and around the vessel. Masses, aneurisms and scarring from other diseases can compress and narrow vessels causing increased resistance to flow resulting in elevation of pressures.
4.In a fairly common parasitic infection in the Middle East (Schistosomiasis), the blood ves-sels in the lung become blocked by the parasites causing pulmonary artery hypertension.
5. Some substances cause constriction of the blood vessels: Pulmonary hypertension has been rarely reported with the use of anti-obesity drugs, such as dexfenfluramine (Redux). These medications have been removed from the market. Some street drugs such as, cocaine and methamphetamines can cause severe pulmonary hypertension.
Pulmonaryhypertension
page
26
6. Some diseases cause pulmonary hypertension for unclear reasons: Perhaps an unknown toxin or chemical affects the blood vessels by causes constriction or inappropriate growth of the tissue within or around the vessel. For example, there is a condition known as Porto-pulmonary hypertension that is result of liver failure. When these individuals receive a liver transplant, the pulmonary hypertension disappears suggesting that the failing liver is unable to clear some biochemical that leads to pulmonary artery hypertension.
Primary pulmonary hypertensionPrimary pulmonary hypertension has no identifiable underlying cause, also referred to as idiopathic pul-monary hypertension.
• It’s more common in young people and more common in females than males.
• It’s an unusually aggressive and often fatal form of pulmonary hypertension.
• Whereas it is known that the arterial obstruction is caused by a building up of the smooth muscle cells that line the arteries, the underlying cause of the disease has long been a mystery.
A genetic cause of the familial form of primary pulmonary hypertension has been discovered. It is caused by mutations in a gene called BMPR2. BMPR2 encodes a receptor (a transforming growth factor beta typeII receptor) that sits on the surface of cells and binds molecules of the TGF-beta superfamily. Binding trig- gers conformational changes that are shunted down into the cell’s interior where a series of biochemical reactions occur, ultimately affecting the cell’s behavior. The mutations block this process. This discovery may provide a means of genetic diagnosis and a potential target for the therapy of people with familial (and possibly also sporadic) primary pulmonary hypertension.
Incidence:There are no clear statistical data on the prevalence of pulmonary hypertension. Since pulmonary hyper-tension is seen in multiple different conditions, it is perhaps better to look at the prevalence in each condi- tion. It is fairly common in patients with heart failure, COPD, and sleep apnea. It occurs in 7% to 12% of patients with collagen vascular disease and in less than 5% of HIV patients.
Signs and symptoms: Many people with pulmonary hypertension may have no symptoms at all, especially if the disease is mild or in the early stages.
symptoms may include: • Shortness of breath that worsens with activity • Other common complaints are cough, fatigue, dizziness, and lethargy. • With the advancement of the condition and ensuing right heart failure, shortness of breath may become worse and retention of fluid in the body may increase (due to failure of the heart to pump blood forward) resulting in swelling the legs.

Hypertension
page
27
• People may also complain of chest pain and angina.
Depending on the underlying associated disease, pulmonary artery hypertension can have othermanifestations. For example, • characteristic skin changes seen in scleroderma, or the signs of liver disease seen in portopulmonaryhypertension.
Signs may include:
• Rapid breathing, hypoxia (low oxygen level in the blood), and swelling in the legs. • In severe pulmonary hypertension, the health care practitioner may hear louder than normal components of heart sounds when he or she listens to the heart with a stethoscope (auscultation).• The doctor may also feel elevation of the chest wall when the heart pumps and this may indicate enlarge-ment of the right side of the heart suggestive of pulmonary hypertension (right ventricular heave).
Diagnosis: The first step in diagnosis of pulmonary hypertension is to clinically suspect it. This may be done as part of an evaluation of another disease that can lead to pulmonary hypertension (such as scleroderma or chronicobstructive pulmonary disease), or based on patients and signs and symptoms as described above.
Many tests, such as echocardiogram, may be performed that may give clues to the possibility of pul- monary hypertension. But the gold standard (the best test available) is right heart catheterization.
This test entails inserting a catheter through the groin into the femoral vein, (or the subclavian vein) andadvancing it to the right side of the heart. The catheter is connected to a device that can monitor and meas- ure blood pressure in the right side of the heart and pulmonary arteries. During right heart catheterization, response to certain medication to treat pulmonary hypertension can be assessed. This is done by administering medications for pulmonary hypertension while the patient still has the catheter placed in heart. Then pulmonary blood pressure is monitored and the response to treatment is compared to no treatment. This can give the physicians a clue as to if an individual is a candidate for acertain therapy and also what dosage of the medicine may be appropriate.Pulmonary hypertension is defined as the mean pulmonary artery blood pressure greater than 25 mil-
limeter of mercury (mmHg) measured by right heart catheterization. The pressures can be much higher than 25 mmHg in some people. Therefore, the pulmonary hypertension can be labeled as mild, moderate, or severe based on the pressures. Mean arterial pressure is two-thirds of the difference between systolic and diastolic blood pressure (systolic is the upper number and diastolic is the lower number in measuring blood pressure). Normally, the pulmonary blood pressure is much lower pressure system than the systemicblood pressure (which is usually measured with a blood pressure cuff).
Other tests available for diagnosing pulmonary hypertension include: electrocardiogram (ECG), chest X-ray, and echocardiogram. An ECG may show some abnormalities that may be suggestive of right heart failure. Chest x-ray may also show enlargement of the chambers of the right heart. And echocardiogram(ultrasound of the heart) shows ultrasound images of the heart and can detect evidence of right heart fail-
ure and pressures in the pulmonary artery can be estimated. These tests, in the right clinical setting, arevery useful in diagnosing pulmonary hypertension.
Pulmonaryhypertension
page
28
Other tests may be useful in evaluating the conditions leading to secondary pulmo- nary hypertension. For example, a ventilation-perfusion scan (V/Q scan) can suggest blood clots in the pulmonary arteries or sometimes a CAT scan of the chest can be used. The chest CAT scan can detect pulmonary arterial clots, but also can show abnormalities of the lung tissue and surrounding structures that can contribute to pulmonary hypertension. A pulmonary function testing can be useful in diagnosingchronic obstructive pulmonary disease (COPD). This test can be used to detect many aspects of lung func- tion including airflow and evidence of obstruction, lung volumes, and the capacity for the lung to extractoxygen from the air.
Treatment The treatment for pulmonary hypertension depends on the underlying cause.
- If left sided heart failure is the primary problem, then adequate treatment of the left heart failure by a cardiologist is the main stray of treatment.
- In cases where hypoxia (low oxygen levels) due to any chronic lung disease, such as COPD, is the cause,then providing oxygen and appropriately treating the underlying lung disease by a lung doctor (pulmon-ologist) is the first step in treatment.
- In conditions, such as scleroderma, which often can cause pulmonary hypertension, a rheumatologist isinvolved in the treatment program
- Anticoagulation may be a treatment option if the main underlying cause is thought to be recurrent blood clot (chronic thromboembolic pulmonary hypertension). As indicated in previous section, referralto a specialty center may be warranted for a possible surgical removal of blood clot (thromboendarterec-
tomy).
- For patients with primary pulmonary hypertension (those with no underlying cause), more advanced therapy may be attempted. These drugs have complex mechanisms, but in general they work by dilating (opening up) the pulmonary arteries and, therefore, by reducing the pressure in these blood vessels and some help prevent the excessive overgrowth of tissue in the blood vessels (that decrease remodeling ofthe vessels, as described above).
drugs used to treat idiopathic pulmonary hypertension :
1) Prostaglandins ; such as epoprostenol. These drugs are very short-acting and often must be given in-travenously or inhaled on a very frequent or continuous basis.
2) Phosphodiesterase type-5 inhibitor; such as sildenafil and tadalafil s) are somewhat less effective than the prostaglandins, but are easily administered one to three times per day by mouth. (The dosing is much different when these drugs are used for erectile dysfunction.)
Hypertension
page
29
3) Endothelium antagonists; are the newest medications used for this condition. These include bosentanand Ambrisentan. These medications are also given by mouth one to two times per day.4) In rare cases, calcium channel blockers may be of benefit.
It is worth mentioning that regardless of the cause of pulmonary hypertension, supplemental oxygen and diuretics may play an important role in relieving the symptoms of pulmonary hypertension of any cause. Low oxygen in the atmosphere causes low blood oxygen levels and aggravates pulmonary hypertension.Therefore, patients with pulmonary hypertension may benefit from breathing supplemental oxygen, espe-cially during air travel or traveling to high altitude destinations.Despite advances in various treatments, there is no cure for pulmonary hypertension.What is the life expectancy for pulmonary hypertension? Generally, the prognosis of pulmonary varies depending on the underlying condition that is causing it. For idiopathic or familial pulmonary hypertension, the overall prognosis depends on the severity and whethertreatment was instituted. The statistics show a survival of about 3 years in idiopathic pulmonary hyperten- sion without any therapy. Some of the other factors may indicate even poorer prognosis which include severe symptoms, age of onset greater than 45 years, evidence of right sided heart failure, and failure to respond to treatment. For patients with idiopathic pulmonary hypertension who get started on treatmentand respond to it, the prognosis is better. Studies are underway to determine optimal treatment regimens.

page
30
REFERENCESSystemic hypertension :
1. Burt V, Whelton P, Rocella E, Brown C, Cutler J. Prevalence of hypertension in the US population: results from the Third National Healthand Nutrition Examination Survey, 1988-1991. Hypertension 1995;25:305–13.2. Barker W, Mullooly J, Linton K. Trends in hypertension prevalence, treatment, and control: in a well-defined older population. Hyperten-sion 1998;31:552–59.3. Schappert S, Nelson C. National Ambulatory Medical Care Survey: 1995-96 summary. Vital Health Stat 1999;142:1–122.4. Stason W. Opportunities to improve cost-effectiveness of treatment of hypertension. Hypertension 1991;18:1161–66.5. Lander E, Schork N. Genetic dissection of complex traits. Science 1994;265:2037–48. 6. Stevens V, Obarzanek E, Cook N, Lee I-M. Long-term weight loss and changes in blood pressure: results of the trials of hypertensionprevention, phase II. Ann Intern Med 2001;134:1–11. 7. Moore R, Levine D, Southard J, Entwisle G, Shapiro S. Alcohol consumption and blood pressure in the 1982 Maryland HypertensionSurvey. Am J Hypertens 1990;3:1–7. 8. Chasan-Taber L, Willett W, Manson J, et al. Prospective study of oral contraceptives and hypertension among women in the United States.Circulation 1996;94:483–89. 9. Nieto F, Young T, Lind B, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study:Sleep Heart Health Study. JAMA 2000;283:1829–36.10. Reeves R. Does this patient have hypertension? How to measure blood pressure. JAMA 1995;273:1211–18.11. Joint National Committee on Prevention. Evaluation and Treatment of High Blood Pressure. The sixth report of the Joint National Com-mittee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VI). Arch Intern Med 1997;157:2413–46. 12. Fuster V, Pearson T. 27th Bethesda conference: matching the intensity of risk factor management with the hazard for coronary diseaseevents. September 14-15, 1995. J Am Coll Cardiol 1996;27:957–1047.13. Rudnick K, Sackett D, Hirst S, Holmes C. Hypertension in a family practice. Can Med Assoc J 1977;117:492–97. 14. Sinclair A, Isles C, Brown I, Cameron H, Murray G, Robertson J. Secondary hypertension in a blood pressure clinic. Arch Intern Med1987;147:1289–93. 15. Anderson G, Blakeman N, Streeten D. The effect of age on prevalence of secondary forms of hypertension in 4429 consecutively referredpatients. J Hypertens 1994;12:609–15. 16. Tucker R, Labarthe D. Frequency of surgical treatment for hypertension in adults at the Mayo Clinic from 1973 through 1975. Mayo ClinProc 1977;52:549–55.17. Gifford R. Evaluation of the hypertensive patient. Chest 1973;64:336–40.18. Krjnen P, Jaarsveld B, Steyerberg E, Schalekamp M. A clinical prediction rule for renal artery stenosis. Ann Intern Med 1998;129:705 11.19. Berglund AS, Hulthen UL, Manhem P, Thorsson O, Wollmer P, Tornquist C.Metaiodobenzylguanidine (MIBG) scintigraphy and com- puted tomography (CT) in clinical practice: primary and secondary evaluation for localization of phaeochromocytomas. J Intern Med2001;249:247–51.20. Yanovski J, Cutler G, Chrousos G, Nieman L. Corticotropin-releasing hormone stimulation following low-dose dexamethasone adminis-tration: a new test to distinguish Cushing’s syndrome from pseudo-Cushing’s states. JAMA 1993;269:2232–38.21. Blumenfeld J, Sealey J, Schussel Y, Vaughan E. Diagnosis and treatment of primary aldosteronism. Ann Intern Med 1994;121:877–85. 22. Fardella C, Lorena M, Gomez-Sanchez C, Cortes J. Primary hyperaldosteronism in essential hypertensives: prevalence, biochemicalprofile, and molecular biology. J Clin Endocrinol Metabol 2000;85:1863–67.23. Streeten D, Tomycz N, Anderson G. Reliability of screening methods for the diagnosis of primary aldosteronism. Am J Med 1979;67:403–13.24. Bravo E, Tarazi R, Dustan H, Fouad F. The changing clinical spectrum of primary aldosteronism. Am J Med 1983;74:641–51.25. Gordon R. Primary aldosteronism. J Endocrinol Invest 1995;18:495–511.26. Anderson G, Blakeman N, Streeten D. Prediction of renovascular hypertension. Am J Hypertens 1988;1:301–04.27. Manger W, Gifford R. Clinical and experimental pheochromocytoma. Cambridge, Mass: Blackwell Science; 1996.28. Nugent C, Warner H, Dunn J, Tyler F. Probability theory in the diagnosis of Cushing’s syndrome. J Clin Endocrinol Metabol 1964;24:621–.
Portal hypertension :
1. Theodorakis NG, Wang YN, Wu JM, Maluccio MA, Sitzmann JV, Skill NJ. Role of endothelial nitric oxide synthase in the development of portal hypertension in the carbon tetrachloride induced liver fibrosis model. Am J Physiol Gastrointest Liver Physiol. Jul 23 2009;[Medline]. 2. Sanyal AJ, Bosch J, Blei A, Arroyo V. Portal hypertension and its complications. Gastroenterology. May 2008;134(6):1715-28. [Medline]. 3. W. Ray KimRobert S. Brown Jr.Norah A. TerraultHashem El-Serag. Burden of liver disease in the United States: Summary of a workshop conducted by the AASLD. May 2001. 4. Hou W, Sanyal AJ. Ascites: diagnosis and management. Med Clin North Am. Jul 2009;93(4):801-17, vii. [Medline]. 5. Chawla Y, Duseja A, Dhiman RK. Review article: Modern management of portal vein thrombosis. Aliment Pharmacol Ther. Aug 12 2009;[Medline]. 6. Singal AK, Ahmad M, Soloway RD. Duplex Doppler Ultrasound Examination of the Portal Venous System: An Emerging Novel Technique for the Estimation of Portal Vein Pressure. Dig Dis Sci. Jul 23 2009;[Medline]. 7. Sass DA, Chopra KB. Portal hypertension and variceal hemorrhage. Med Clin North Am. Jul 2009;93(4):837-53, vii-viii. [Medline]. 8. Rimola A, Garcia-Tsao G, Navasa M. Diagnosis, treatment and prophylaxis of spontaneous bacterial peritonitis: a consensus document. International Ascites Club. J Hepatol. Jan 2000;32(1):142-53. [Medline].
Hypertension

Hypertension
page
31
9. Cheng LF, Wang ZQ, Li CZ, Lin W, Yeo AE, Jin B. Low incidence of complications from endoscopic gastric variceal obturation with butyl cyanoacrylate. Clin Gastroenterol Hepatol. Sep 2010;8(9):760-6. [Medline]. 10. García-Pagán JC, Caca K, Bureau C, Laleman W, Appenrodt B, Luca A. Early use of TIPS in patients with cirrhosis and variceal bleeding. N Engl J Med. Jun 24 2010;362(25):2370-9. [Medline]. 11. Garcia-Tsao G, Sanyal AJ, Grace ND, Carey W. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology. Sep 2007;46(3):922-38. [Medline].12. Ferreira FG, Ribeiro MA, de Fátima Santos M, Assef JC, Szutan LA. Doppler Ultrasound Could Predict Varices Progression and Rebleed- ing After Portal Hypertension Surgery: Lessons from 146 EGDS and 10 Years of Follow-Up. World J Surg. Aug 13 2009;[Medline]. 13. Bonnet S, Sauvanet A, Bruno O, Sommacale D, Francoz C, Dondero F, et al. Long-term survival after portal vein arterialization for portal vein thrombosis in orthotopic liver transplantation. Gastroenterol Clin Biol. Jul 28 2009;[Medline]. 14. Abraczinskas DR, Ookubo R, Grace ND. Propranolol for the prevention of first esophageal variceal hemorrhage: a lifetime commitment?. Hepatology. Dec 2001;34(6):1096-102. [Medline]. 15. Baik SK, JeTheodorakis NG, Wang YN, Wu JM, Maluccio MA, Sitzmann JV, Skill NJ. Role of endothelial nitric oxide synthase in the development of portal hypertension in the carbon tetrachloride induced liver fibrosis model. Am J Physiol Gastrointest Liver Physiol. Jul 23 2009;[Medline]. 16. Sanyal AJ, Bosch J, Blei A, Arroyo V. Portal hypertension and its complications. Gastroenterology. May 2008;134(6):1715-28. [Medline].
Intracranial hypertension :
1. Durcan FJ, Corbett JJ, Wall M. The incidence of pseudotumor cerebri: Population studies in Iowa and Louisiana. Arch Neurol. 1988;45(8):875-7. 2. Goodwin J. Pseudotumor cerebri [online]. Omaha, NE: eMedicine; 2005 [cited 25 October 2005]. 3. Friedman DI. Pseudotumor cerebri. Neurol Clin. 2004;22(1):99-131.4. Kesler A, Gadoth N. Epidemiology of idiopathic intracranial hypertension in Israel. J Neuroophthalmol. 2001;21(1):12-4 5. Radhakrishnan K, Ahlskog JE, Cross SA, et al. Idiopathic intracranial hypertension (pseudotumor cerebri). Descriptive epidemiology in Rochester, Minn, 1976 to 1990. Arch Neurol. 1993;50(1):78-80. 6. Radhakrishnan K, Sridharan R, Ashok PP, Mousa ME. Pseudotumour cerebri: Incidence and pattern in North-Eastern Libya. Eur Neurol. 1986;25(2):117-24. 7. Lee AG, Wall M. Idiopathic intracranial hypertension (pseudotumor cerebri) [online]. Waltham, MA: UpToDate; 2005 [cited 25 October 2005].8. http://en.wikipedia.org/wiki/Intracranial_pressure#Causes
Intracranial hypertension :
1. Fauci, Anthony S., et al. Harrison’s Principles of Internal Medicine. 17th ed. United States: McGraw-Hill Professional, 2008.
2. Raza, T and Dilawar, M; Pulmonary Hypertension; A Comprehensive Review; Heart Views Vol. 8 No.3 Sept-Nov 2007; 90-99
3. Simonneau, G, Galie, N, Rubin, LJ, et al. Clinical classification of pulmonary hypertension. J Am Coll Cardiol 2004; 43:5S.
4. Simonneau, et al. Updated Clinical Classification of Pulmonary Hypertension. J Am Coll Cardiol 2009;54:43-54, doi:10.1016/j.jacc.2009.04.012