hypertension update 2009 adena health system 2009 cardiovascular symposium october 2009
Post on 19-Dec-2015
232 views
TRANSCRIPT

Hypertension Update 2009
Adena Health System
2009 Cardiovascular Symposium
October 2009
Key ConceptsKey Concepts
• Hypertension is commonHypertension is common
• Hypertension increases cardiovascular riskHypertension increases cardiovascular risk
• Effective treatment confers benefitEffective treatment confers benefit
• Lessons from recent clinical trialsLessons from recent clinical trials
• Compelling indications for certain Compelling indications for certain antihypertensive agents and blood antihypertensive agents and blood pressure targetspressure targets
2

Epidemiology
• Over 65 million Americans age 20 and older have HTN
• Prevalence increases with age• Prevalence of hypertension varies by ethnic Prevalence of hypertension varies by ethnic
group several-fold higher in young African group several-fold higher in young African AmericansAmericans – >60% of Caucasians over 60>60% of Caucasians over 60– >70% of African American over 60>70% of African American over 60
• Primary Hypertension 95%Primary Hypertension 95%• Secondary Hypertension 5%Secondary Hypertension 5%
• Over 65 million Americans age 20 and older have HTN
• Prevalence increases with age• Prevalence of hypertension varies by ethnic Prevalence of hypertension varies by ethnic
group several-fold higher in young African group several-fold higher in young African AmericansAmericans – >60% of Caucasians over 60>60% of Caucasians over 60– >70% of African American over 60>70% of African American over 60
• Primary Hypertension 95%Primary Hypertension 95%• Secondary Hypertension 5%Secondary Hypertension 5%
Epidemiology
• Level of BP directly correlates with LVH/microalbuminuria
• LVH and hypertension:• Strong predictor of sudden death and MI
• Microalbuminuria and hypertension:(Persistent urinary albumin excretion of 30-300mg/24hrs)
• Increased risk of CVD
• Marker for endothelial dysfunction

Mortality Due to CHD per Quartile Mortality Due to CHD per Quartile of Usual SBPof Usual SBP
van den Hoogen et al. N Engl J Med 2000;342:1. 5
USA
Japan

Impact of Impact of High-Normal High-Normal
BP on the BP on the Risk of CV Risk of CV DiseaseDisease
Vasan RS et al. N Engl J Med
2001;345:1291.6
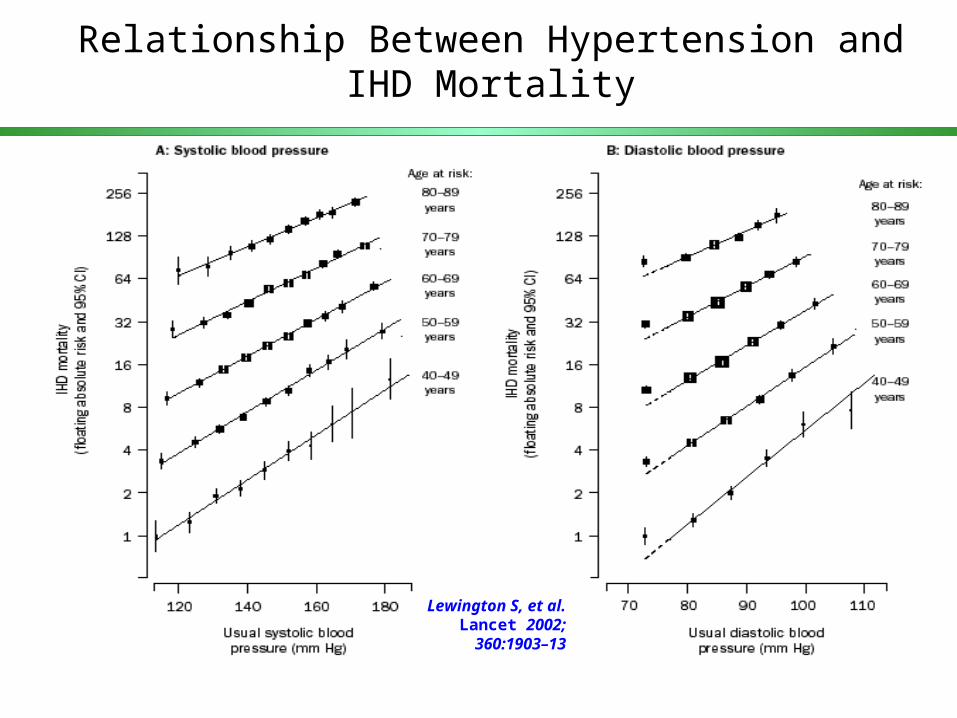
Relationship Between Hypertension and IHD Mortality
Lewington S, et al. Lancet 2002; 360:1903–13

Update Hypertension 2009Main Themes
• What level of BP should we achieve?
• What does the hypertension workup consist of ?
• How should we measure BP?
• Future directions……..personalized medicine and home monitoring !

Historical Trends in HTN
National Health and Nutrition Examination SurveyNational Health and Nutrition Examination Survey
AwarenessAwareness
TreatmentTreatment
ControlControl
1991-19941991-1994
68%68%
54%54%
27%27%
1976-19801976-1980
51%51%
31%31%
10%10%
1988-19911988-1991
73%73%
55%55%
29%29%
1994-20001994-2000
70%70%
59%59%
34%34%
SBP < 140 mmHg and DBP < 90 mmHgSBP < 140 mmHg and DBP < 90 mmHg
Trends in awareness, treatment, and control of high blood Trends in awareness, treatment, and control of high blood pressure in adults ages 18-74pressure in adults ages 18-74
Adapted from:Hajjar I, et al. JAMA. 2003;290:199-206.Ong KL et al Hypertension 2007: 49;69-75
2003-20042003-2004
75%
65%
33%
• Effective blood pressure control, regardless of which (or how Effective blood pressure control, regardless of which (or how many) agents are employed, is paramount to reduce CV many) agents are employed, is paramount to reduce CV endpointsendpoints
• Current control rates, even in idealized study populations, is Current control rates, even in idealized study populations, is sub-par. On a practical level, whatever potential benefits or sub-par. On a practical level, whatever potential benefits or drawbacks occur as a result of a specific property of one agent drawbacks occur as a result of a specific property of one agent vs. another at equivalent blood pressure levels is drowned out vs. another at equivalent blood pressure levels is drowned out by the adverse events of those that remain uncontrolledby the adverse events of those that remain uncontrolled
• At equivalent levels of blood pressure control, newer agents At equivalent levels of blood pressure control, newer agents offer a more appealing biochemical profile… the long-term offer a more appealing biochemical profile… the long-term importance of which remains to be seenimportance of which remains to be seen
Lessons Learned from ALLHAT and ASCOT-BPLA on Lessons Learned from ALLHAT and ASCOT-BPLA on specific antihypertensive agentsspecific antihypertensive agents
10
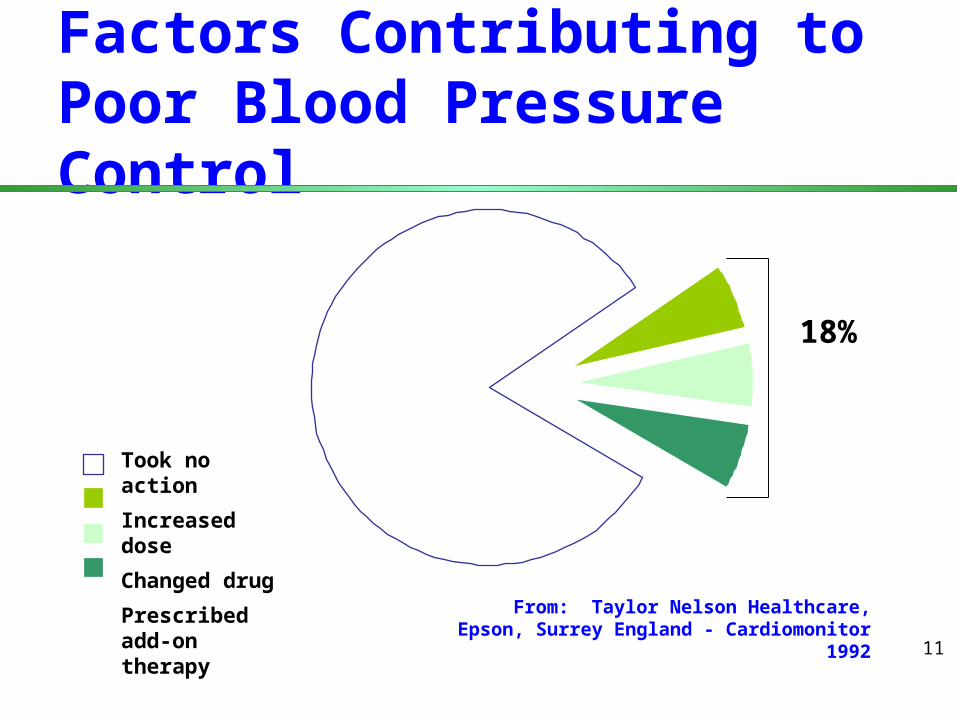
Factors Contributing to Poor Blood Pressure Control
Took no action
Increased dose
Changed drug
Prescribed add-on therapy
18%
From: Taylor Nelson Healthcare, Epson, Surrey England - Cardiomonitor 1992
11

SBP=systolic BP, DBP=diastolic BP; HYTN=hypertension, ACEI=Angiotensin-converting enzyme inhibitor, ARB=angiotensin, CCB=calcium channel blocker
* Treatment determined by highest BP categorya Treat patients with chronic kidney disease or diabetes to BP goal of <130/80 mm Hgb Thiazide-type diuretics for most; may consider ACEI, ARB, -blocker, CCB or combinationc Other antihypertensive drugs (diuretics, ACEI, ARB,-blocker, CCB) as neededd Two-drug combination for most (usually thiazide-type diuretic and ACEI or ARB or b-blocker of CCB.
Initiation of combined therapy should be used cautiously in those at risk for orthostatic hypotension.e Other antihypertensive drugs (diuretics, ACEI, ARB, -blocker, CCB) as needed.
Blood Pressure (BP) Classification and Management*
Normal <120 and <80 encourage
Pre HYTN 120-139 or 80-89 Yes No Yesa
Stage 1 HYTN 140-159 or 90-99 Yes Yesb Yesc
Stage 2 HYTN >160 or >100 Yes Yesd Yese
Life- Initial Drug Therapy BP SBP, DBP, style Compelling Indications Classification mm Hg* mm Hg* Changes Without With
Life- Initial Drug Therapy BP SBP, DBP, style Compelling Indications Classification mm Hg* mm Hg* Changes Without With
JNC VII. JAMA 2003;289:2560.
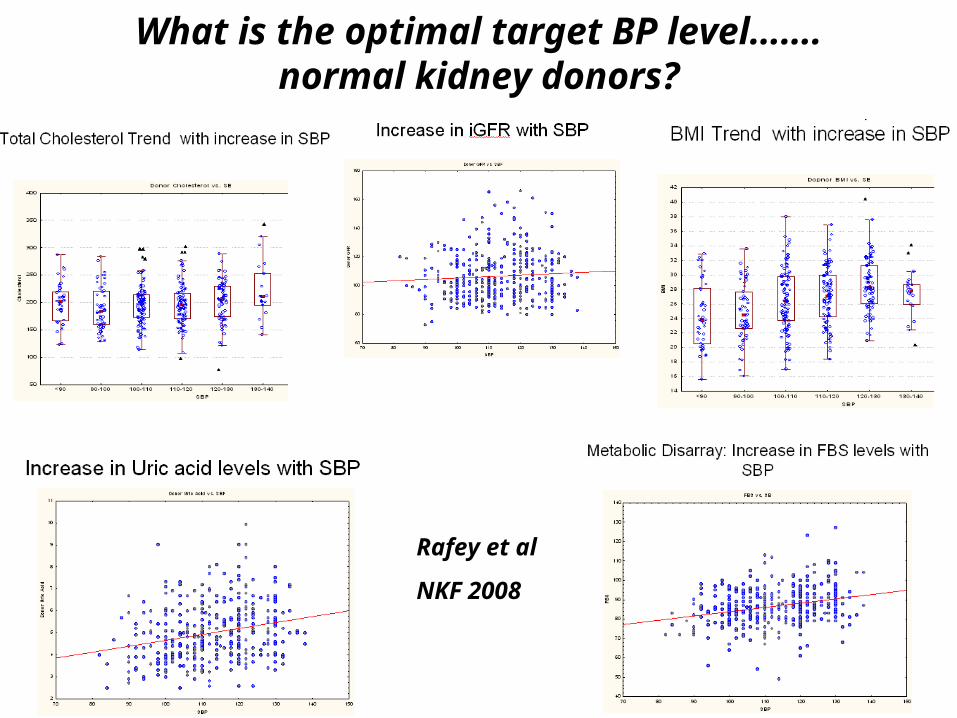
What is the optimal target BP level…….normal kidney donors?
Rafey et al
NKF 2008

Goals of the Hypertensive Goals of the Hypertensive EvaluationEvaluation
• Does the patient have primary or Does the patient have primary or secondary (reversible) hypertension? secondary (reversible) hypertension?
• Is target organ damage present?Is target organ damage present?
• Are other cardiovascular (CV) risk Are other cardiovascular (CV) risk factors present?factors present?
14
JNC 7 Recommendations for Routine Work-up of Hypertensive Patients
Routine Tests• Electrocardiogram • Urinalysis • Blood glucose, and hematocrit • Serum potassium, creatinine, or the corresponding estimated GFR,
and calcium• Lipid profile, after 9- to 12-hour fast, that includes high-density and
low-density lipoprotein cholesterol, and triglycerides
Optional tests • Measurement of urinary albumin excretion or albumin/creatinine ratio
More extensive testing for identifiable causes is not generally indicated unless BP control is not achieved
JNC 7 Recommendations for Routine Work-up of Hypertensive Patients
Routine Tests• Electrocardiogram • Urinalysis • Blood glucose, and hematocrit • Serum potassium, creatinine, or the corresponding estimated GFR,
and calcium• Lipid profile, after 9- to 12-hour fast, that includes high-density and
low-density lipoprotein cholesterol, and triglycerides
Optional tests • Measurement of urinary albumin excretion or albumin/creatinine ratio
More extensive testing for identifiable causes is not generally indicated unless BP control is not achieved

Secondary Causes of Hypertension: Secondary Causes of Hypertension: Renovascular DiseaseRenovascular Disease
Clinical CluesAbrupt onsetAbrupt onset<30 or >55 years of age<30 or >55 years of ageRefractory to 3-drug regimenRefractory to 3-drug regimenEvidence of diffuse vascular Evidence of diffuse vascular
diseasediseaseARF with ACEIARF with ACEIAccelerated retinopathyAccelerated retinopathyEpigastric bruitEpigastric bruit
DiagnosisDuplex renal Duplex renal
arteriesarteriesCaptopril Captopril
renographyrenographyMRAMRAAngiogramAngiogramRenal vein reninRenal vein renin
TreatmentAngioplasty/stentAngioplasty/stentSurgerySurgeryMedical treatmentMedical treatment
17
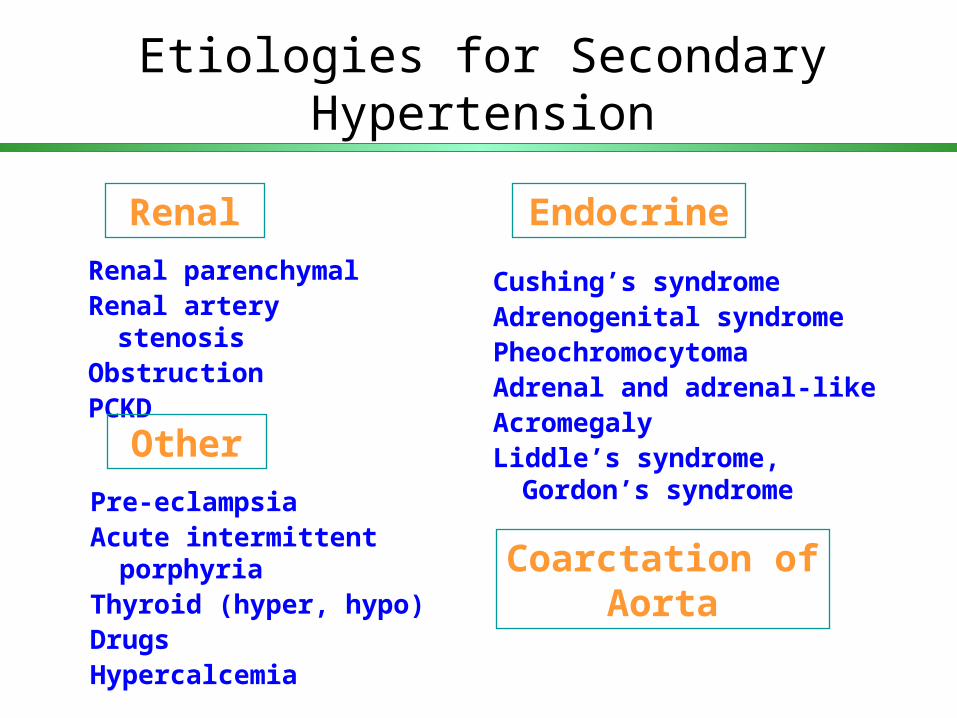
Etiologies for Secondary Hypertension
Renal parenchymalRenal artery stenosisObstructionPCKD
Renal
Cushing’s syndromeAdrenogenital syndromePheochromocytomaAdrenal and adrenal-like AcromegalyLiddle’s syndrome, Gordon’s
syndrome
Endocrine
Other
Pre-eclampsiaAcute intermittent porphyriaThyroid (hyper, hypo)DrugsHypercalcemia
Coarctation of Aorta
Secondary Hypertension
Chronic Kidney Disease and hypertension:
• Present in more than 80% of patients
• Mechanism: Excessive salt retention and increased peripheral resistance– Exacerbates proteinuria– Accelerated progression of CKD
• ACEI and ARBs slow progression of CKD


Angioplasty and Stent for Renal Artery Lesions
ASTRAL
Cardiovascular Outcomes in Renal Atherosclerotic Lesions
CORAL

www.coralclinicaltrial.govwww.coralclinicaltrial.gov 23

New Features New Features and Key Messagesand Key Messages
JNC VIIJNC VII
• For persons over age 50, SBP is a more important than For persons over age 50, SBP is a more important than DBP as CVD risk factor.DBP as CVD risk factor.
• Persons who are normotensive at age 55 have a 90% Persons who are normotensive at age 55 have a 90% lifetime risk for developing HTN.lifetime risk for developing HTN.
• Starting at 115/75 mm Hg, CVD risk doubles with each Starting at 115/75 mm Hg, CVD risk doubles with each increment of 20/10 mm Hg throughout the BP range. increment of 20/10 mm Hg throughout the BP range.
• Those with SBP 120–139 mmHg or DBP 80–89 mm Hg Those with SBP 120–139 mmHg or DBP 80–89 mm Hg should be considered prehypertensive who require should be considered prehypertensive who require health-promoting lifestyle modifications to prevent CVD.health-promoting lifestyle modifications to prevent CVD.
24

JNC VIIJNC VII
New Features and New Features and Key Messages Key Messages (Continued)(Continued)
• Thiazide-type diuretics should be initial drug therapy for Thiazide-type diuretics should be initial drug therapy for most, either alone or combined with other drug classes. most, either alone or combined with other drug classes.
• Certain high-risk conditions are compelling indications for Certain high-risk conditions are compelling indications for other drug classes.other drug classes.
• Most patients will require two or more antihypertensive Most patients will require two or more antihypertensive drugs to achieve goal BP.drugs to achieve goal BP.
• If BP is >20/10 mmHg above goal, initiate therapy with two If BP is >20/10 mmHg above goal, initiate therapy with two agents, one usually should be a thiazide-type diuretic.agents, one usually should be a thiazide-type diuretic.
25

Combination Therapy Needed to Achieve Target SBP Goals
Updated from Bakris GL et al. Am J Kidney Dis. 2000;36:646-661.
Number of BP meds
Trial/SBP Achieved
1 2 3 4
UKPDS (144 mm Hg)
RENAAL(141 mm Hg)
ALLHAT (135 mm Hg)
IDNT (138 mm Hg)
HOT (138 mm Hg)
INVEST (133 mm Hg)
ABCD (132 mm Hg)
MDRD (132 mm Hg)
AASK (128 mm Hg)

RAS Inhibitor use in Hypertensive Blacks
• ACEIs/ARBs should be considered first line in patients (including blacks) with nephropathy (esp. with proteinuria) and or heart failure
• Available data suggest that RAS inhibitors are less effective in lowering BP in black hypertensives in the absence of adequate
doses of a diuretic or CCB (and in preventing clinical outcomes)• ACEI also carry increased risk of angioedema , esp. in blacks• In the absence of HF or CKD, particularly in Black hypertensives,
beta blockers, ACEI,and ARBs(and presently renin inhibitors) should be prescribed only in combination with thiazide-type diuretics or calcium channel blockers

Blood pressure measurement…
• Recognize the diagnostic limitations of traditional office blood pressure measurement..
• 24hr ambulatory BP measurement: diagnostic utility and clinical correlations…
• Understand the physiology of the arterial waveform, central BP measurement, vascular stiffness indices and pulsology in clinical practice

Center for Blood Pressure Disorders
Clinical Program: Goals
• Accurate BP Measurement
• Comprehensive Vascular Evaluation

180 –
170 –
160 –
150 –
140 –
130 –
120 –
110 –
100 –
90 –
80 –
0 –
152
140
132 134
8780 75 77
FamilyPhysician
ResearchTechnician
BpTRU Ambulatory BP
Blo
od
Pre
ssu
re (
mm
Hg
)
Myers M, et al, Journal of Hypertension 2009 27(2) 280-286 n=309
Reduction of WCE in Clinical Practice

BpTRU
• White coat effect
• Work in progress
BpTRU
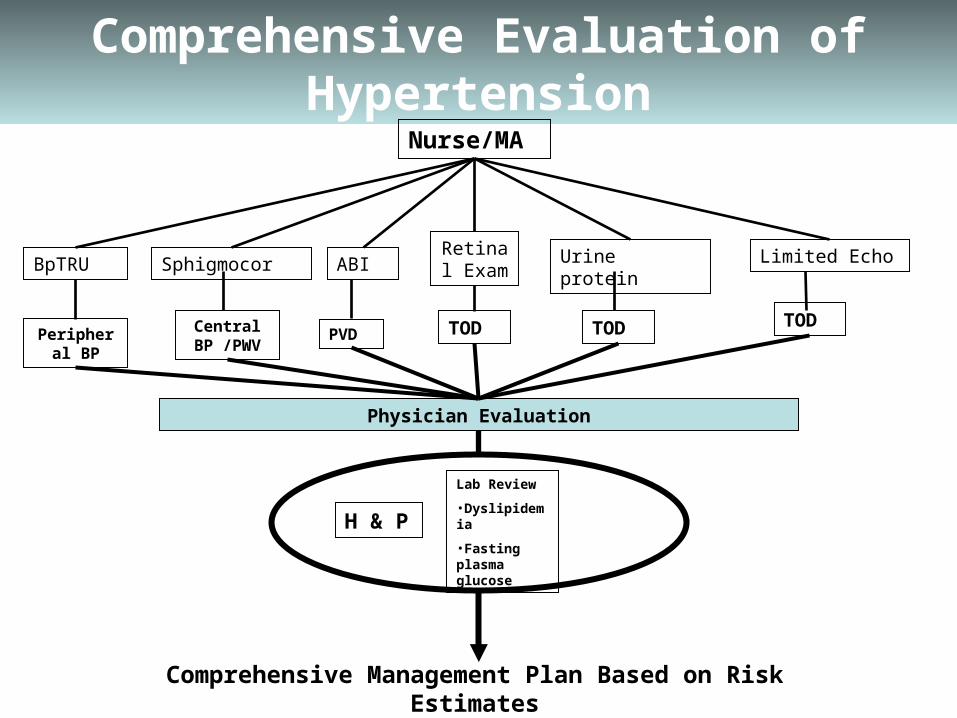
Comprehensive Evaluation of Hypertension
SphigmocorRetinal ExamABI
Nurse/MA
Limited EchoUrine protein
Peripheral BP
Lab Review
•Dyslipidemia
•Fasting plasma glucose
H & P
Physician Evaluation
Central BP /PWV
PVD TOD TOD TOD
Comprehensive Management Plan Based on Risk Estimates

24 Hour Ambulatory Blood Pressure Monitoring

HBPM: New Recommendations May 2008

Indications for 24 Hour ABPM
Clinical situations in which ABPM may be helpful:
• Rule out white-coat HTN • Apparent drug resistance (office resistance)• To better define resistant HTN• Hypotensive symptoms with antihypertensives• Episodic hypertension• Autonomic dysfunction
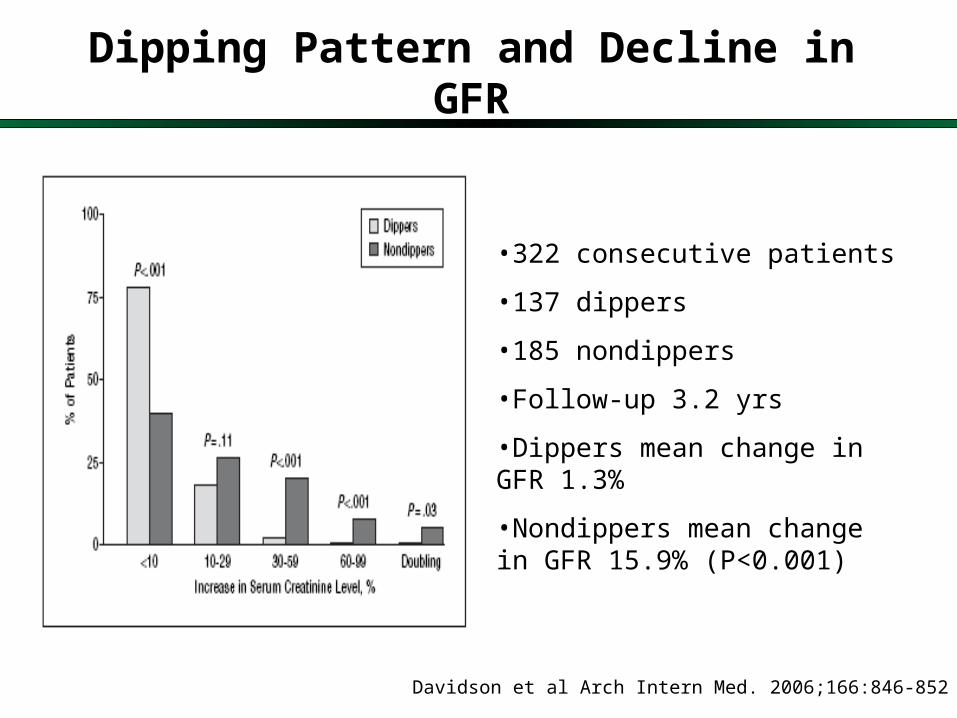
Dipping Pattern and Decline in GFR
Davidson et al Arch Intern Med. 2006;166:846-852
•322 consecutive patients
•137 dippers
•185 nondippers
•Follow-up 3.2 yrs
•Dippers mean change in GFR 1.3%
•Nondippers mean change in GFR 15.9% (P<0.001)
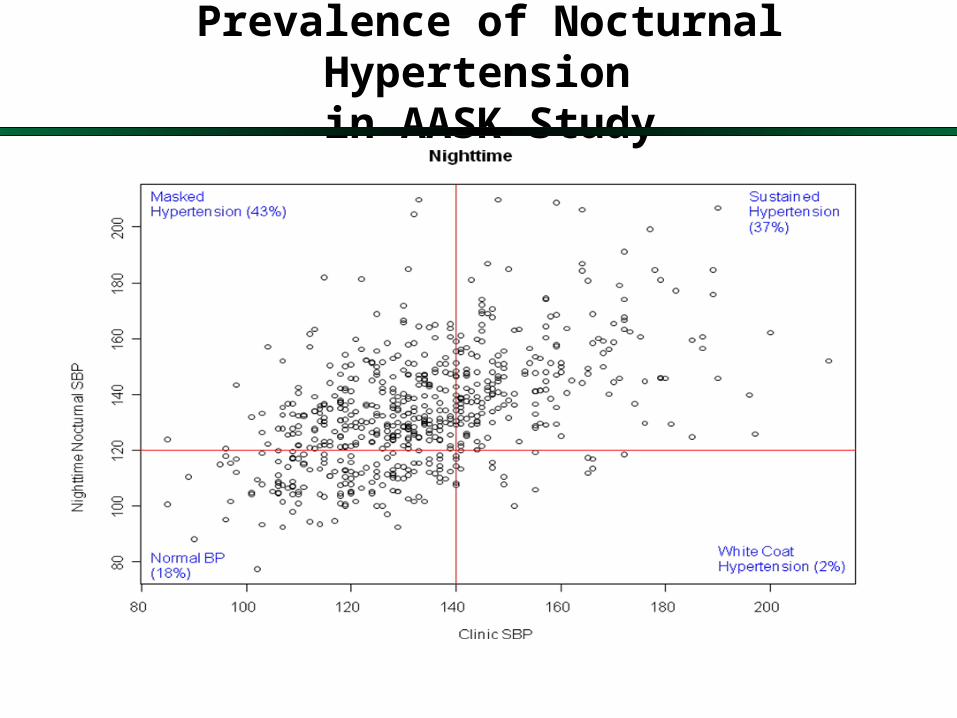
Prevalence of Nocturnal Hypertension in AASK Study
24 Hour Ambulatory Blood Pressure Monitoring
• Central Aortic Pressure
• Pulse Wave Velocity (PWV)
• Augmentation Index (AIx)
Measures of Arterial Stiffness
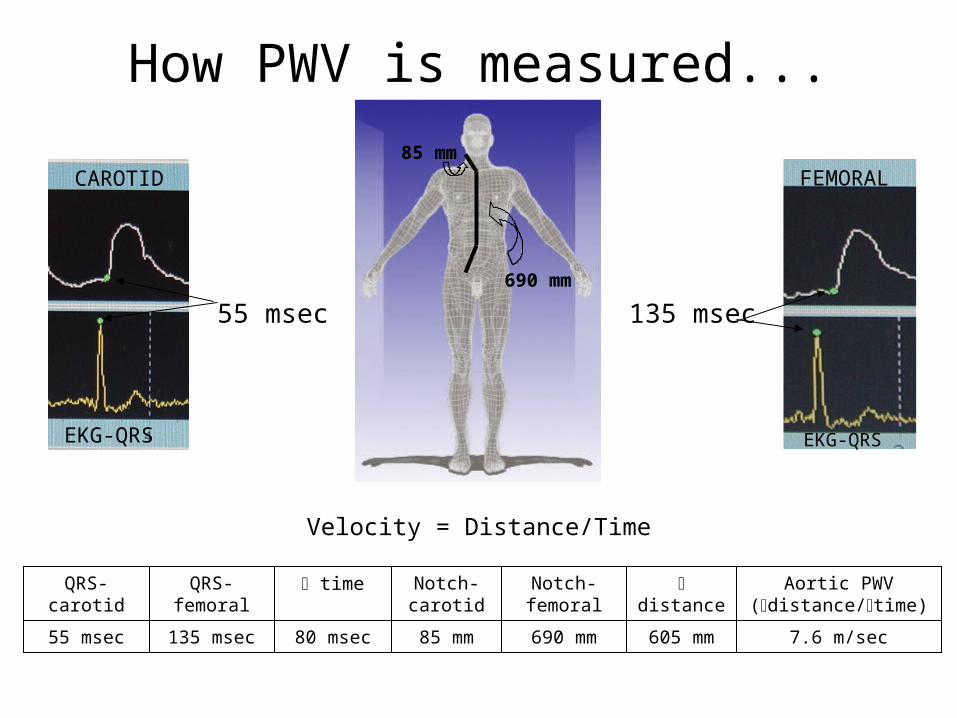
7.6 m/sec605 mm690 mm85 mm80 msec135 msec55 msec
Aortic PWV (distance/time)
distance
Notch-femoral
Notch-carotid
timeQRS-femoral
QRS-carotid
85 mm
690 mm
EKG-QRS
CAROTID
55 msec 135 msec
FEMORAL
EKG-QRS
How PWV is measured...
Velocity = Distance/Time
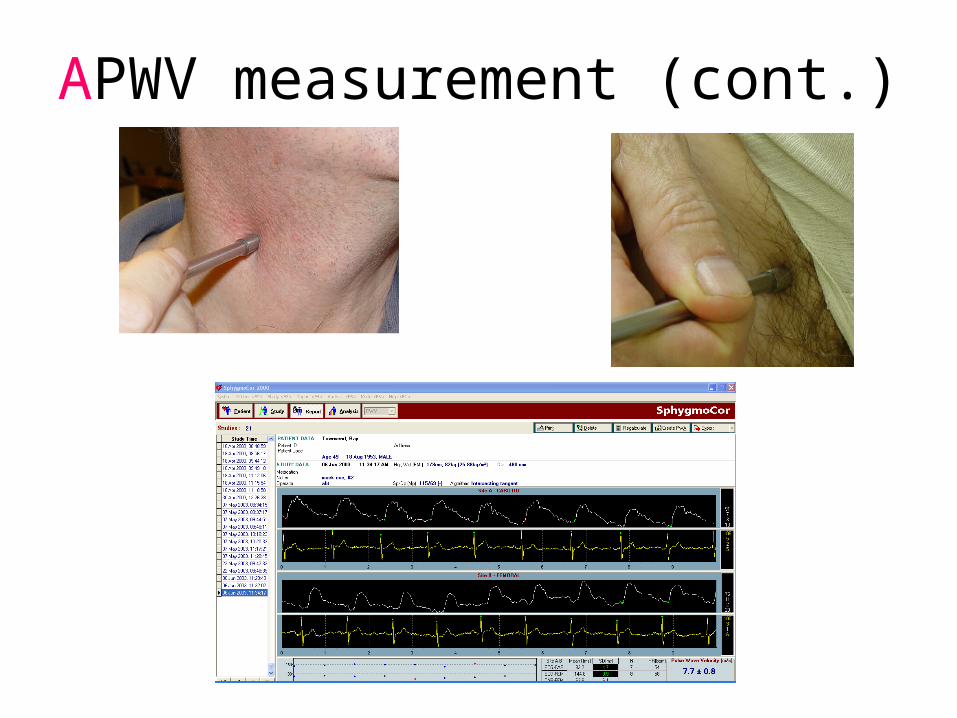
APWV measurement (cont.)
Systole
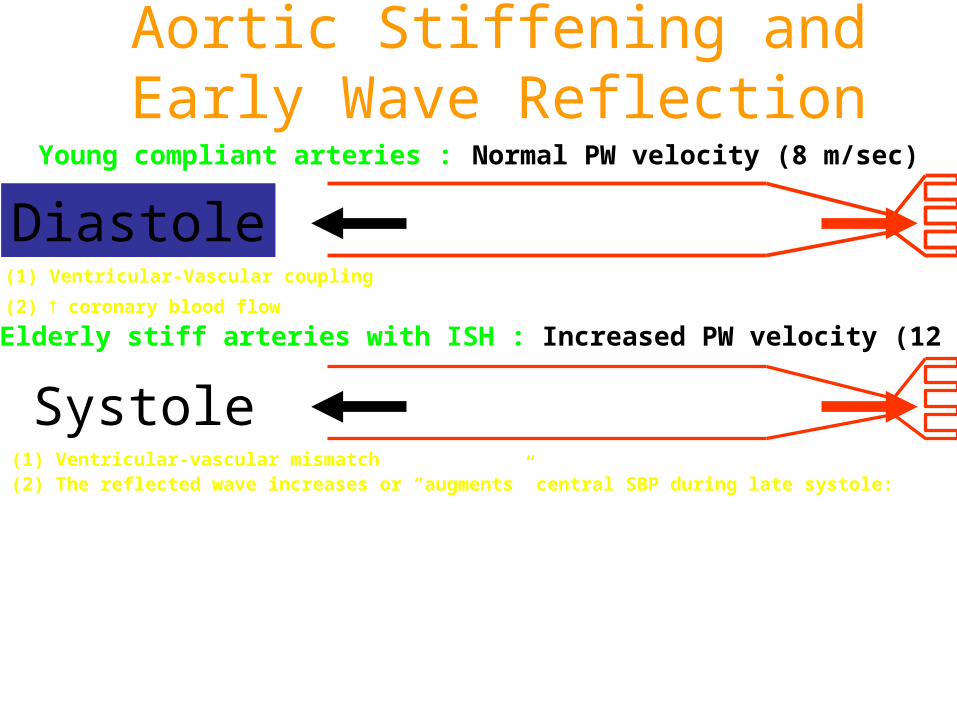
Aortic Stiffening and Early Wave Reflection
Diastole
Systole
Young compliant arteries : Normal PW velocity (8 m/sec)
Elderly stiff arteries with ISH : Increased PW velocity (12 m/sec)
(1) Ventricular-Vascular coupling
(2) coronary blood flow
(1) Ventricular-vascular mismatch(2) The reflected wave increases or “augments” central SBP during late systole:
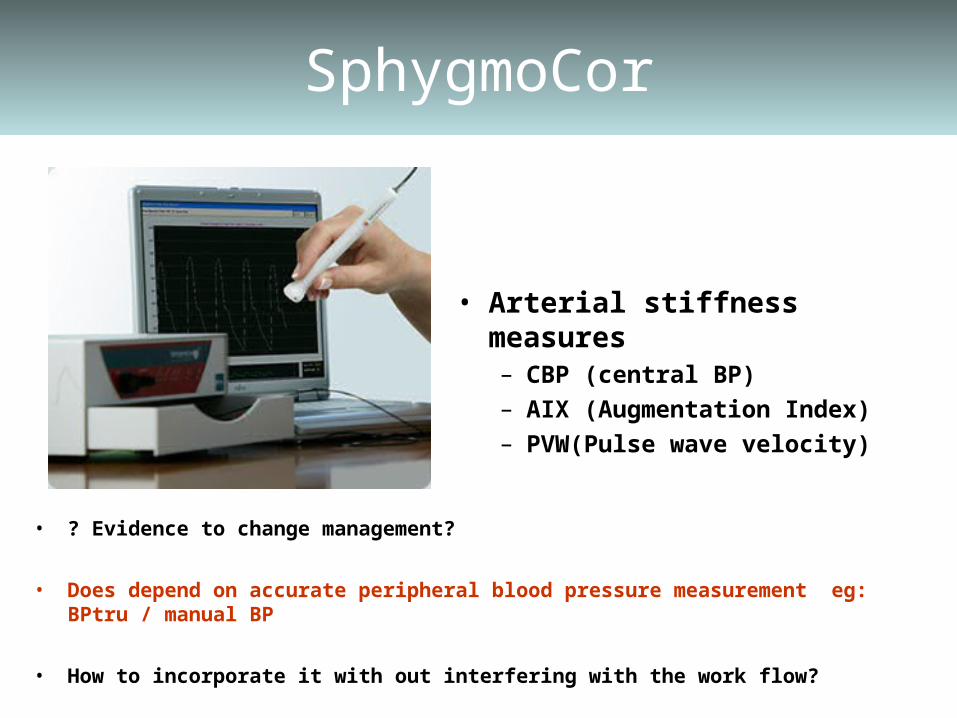
SphygmoCor
• Arterial stiffness measures– CBP (central BP)– AIX (Augmentation Index)– PVW(Pulse wave velocity)
• ? Evidence to change management?
• Does depend on accurate peripheral blood pressure measurement eg: BPtru / manual BP
• How to incorporate it with out interfering with the work flow?
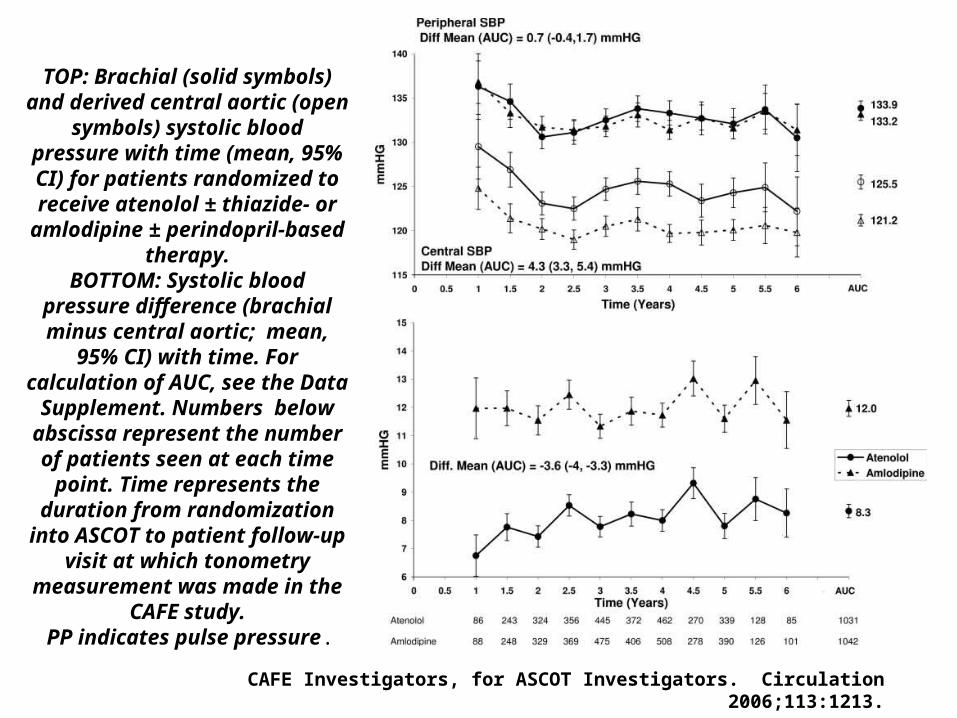
TOP: Brachial (solid symbols) and derived central aortic (open
symbols) systolic blood pressure with time (mean, 95% CI) for patients randomized to receive atenolol ± thiazide- or
amlodipine ± perindopril-based therapy.
BOTTOM: Systolic blood pressure difference (brachial minus central aortic; mean,
95% CI) with time. For calculation of AUC, see the Data Supplement. Numbers
below abscissa represent the number of patients seen at each time point. Time represents the
duration from randomization into ASCOT to patient follow-up
visit at which tonometry measurement was made in the
CAFE study. PP indicates pulse pressure.
CAFE Investigators, for ASCOT Investigators. Circulation 2006;113:1213.
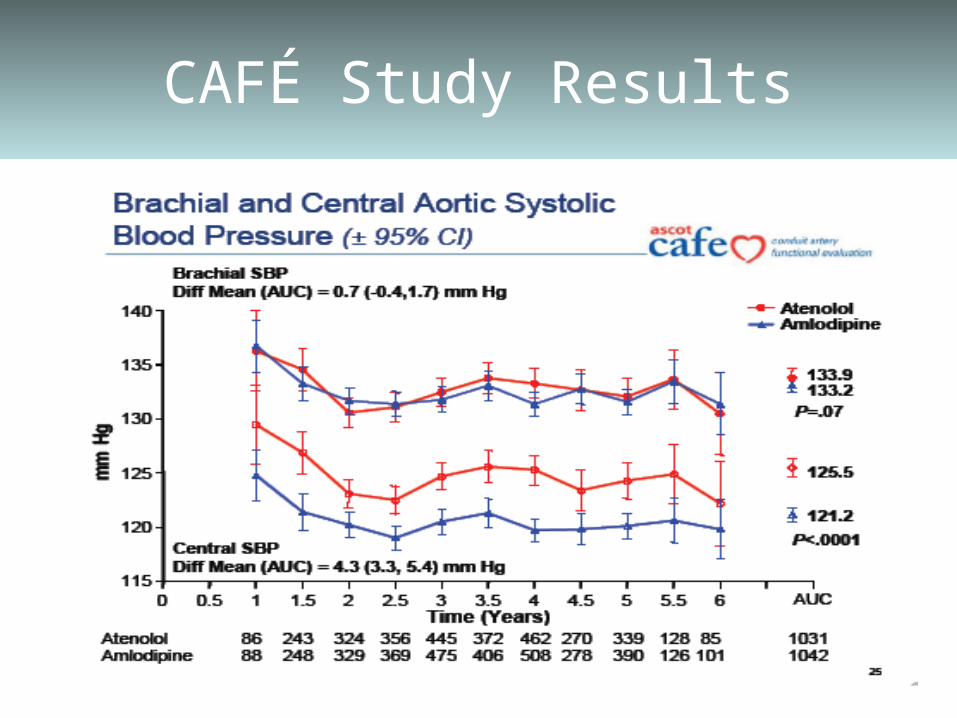
CAFÉ Study Results

AIx in CKD vs. non CKD
• AIx was significantly higher in the non-CKD patients compared to the CKD patients (median AIx 27 % [18, 32] vs. 21 % [14, 29], P = 0.002).
• AIx was similar in the CKD and non-CKD groups after adjusting for age, gender, height, SBP and eGFR
-10
0
10
20
30
40
50
60
AIx
(%
)
0 1
CKD vs. non-CKDNon-CKD CKD

Linear Regression of AIx by SBP
80 100 120 140 160 180 200 220
-10
010
20
30
40
50
60
P_SP
Augm
enta
tion In
dex
FemaleMale
SBP
Aug
men
tatio
n In
dex
(%)
R = 0.24, P <0.0001

Linear Regression of AIx by PPP
20 40 60 80 100 120
-10
01
02
03
04
05
06
0
P_PP
Au
gm
en
tatio
n In
de
x
FemaleMale

Future Developments in Hypertension
Personal medicine
Home BP monitoring

cell membrane
Corin Variants in African-Americans with Hypertension and Heart Disease
enzyme
T555I Q568P
enzyme
Dries et al. Circulation 2005;112:2403 Wang et al. Circ Res 2008;103:502

Home Blood Pressure Monitoring

Graph from the daily readings

Hypertension Clinic Review
Internet Based Hypertension Clinic Program:Achieve individual blood pressure goals
Wireless/USB
Phone/email:
•Titrate medication dose
•Add medications
Secure Data Transfer
CONTROLLED BLOOD PRESSURE
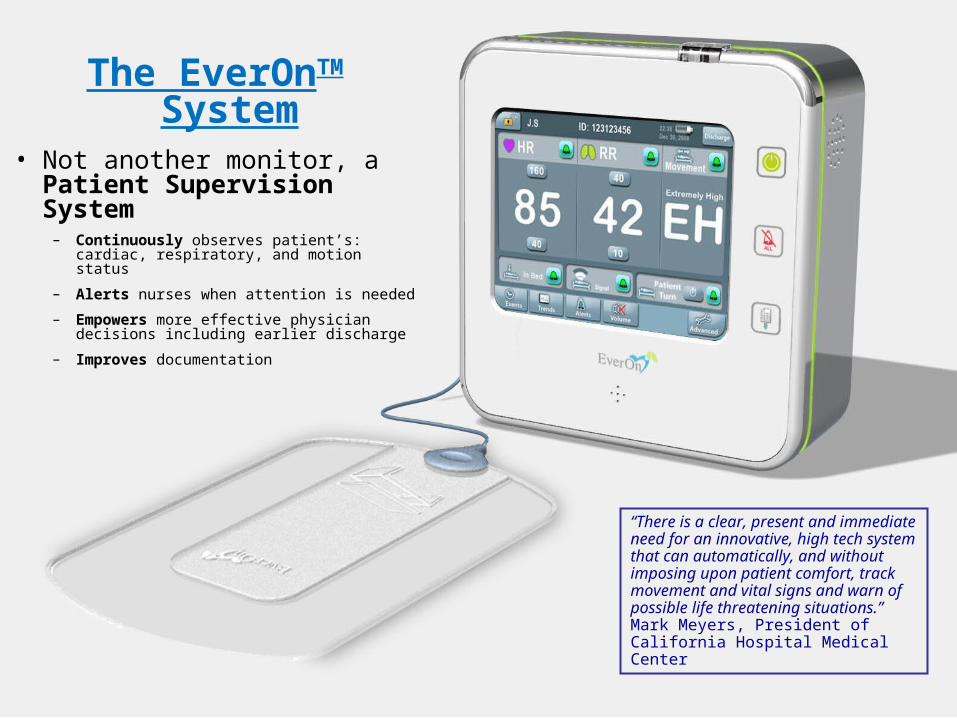
The EverOnTM System
• Not another monitor, a Patient Supervision System
– Continuously observes patient’s: cardiac, respiratory, and motion status
– Alerts nurses when attention is needed
– Empowers more effective physician decisions including earlier discharge
– Improves documentation
“There is a clear, present and immediate need for an innovative, high tech system that can automatically, and without imposing upon patient comfort, track movement and vital signs and warn of possible life threatening situations.” Mark Meyers, President of California Hospital Medical Center

Blood Pressure Monitoring – Preliminary Data
PTT ECG [ms] PTT EverOn[ms]
MAP [mmHg]
SBP [mmHg]
DBP [mmHg]
Baseline (rest)
282.3±17.6 - 81±4.7 123.9±4.4 62.1±6.4
Maximal Effort
264.6±15.3Δ=-17.7±4.4 Δ=-11.9±0.6
95.2±6.5 Δ=+14.2
138.8±9.2 Δ=+14.9
68±4.4Δ=+5.9
Recovery 280.4±15.5Δ=-1.9±5.8 Δ=-0.7±6.8
80.5±6Δ=-0.5
125.8±9.9Δ=+1.9
55.2±5.6Δ=-6.9
240 250 260 270 28080
85
90
95
100
105
110
PTT (ms)
BP (m
mH
g)
Mean Blood PressureVs. PTT from ECG
BaselineMax EffortRecovery
190 200 210 220 23080
85
90
95
100
105
110
PTT (ms)
BP (m
mH
g)
Mean Blood PressureVs. PTT from EverOn
BaselineMax EffortRecovery
240 250 260 270 280190
195
200
205
210
215
220
PTT ECG (ms)
PTT
Ever
On
(ms)
PTT from ECGVs. PTT from EverOn
BaselineMax EffortRecovery

Take Home Points …Hypertension Update 2009
• Hypertension is sub optimally controlled in the US
• Target BP may be lower than traditionally thought
• Resistant hypertension should trigger a workup for secondary causes
• Methods for BP measurement are evolving • Home monitoring is the future for BP
management