hypomyelinating hypomyelinating · pathologic classification of white matttt didi ddtter disorders...
TRANSCRIPT
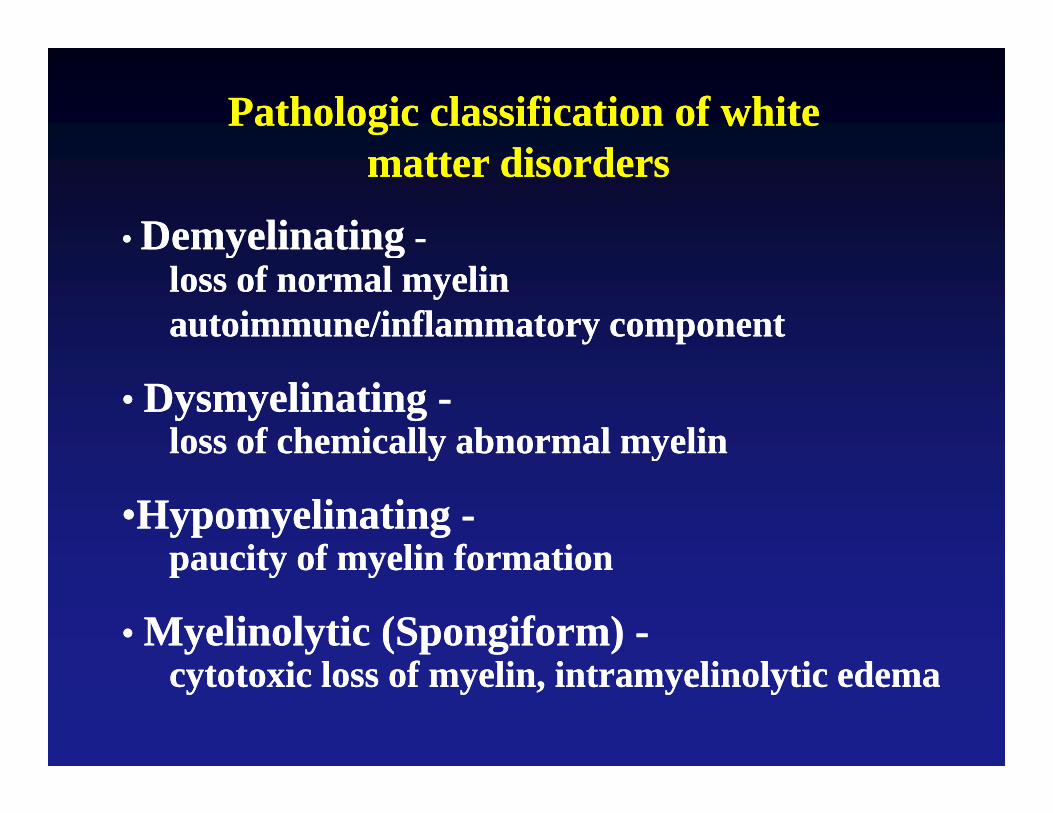
Pathologic classification of white Pathologic classification of white tt di dtt di dmatter disordersmatter disorders
•• DemyelinatingDemyelinating --y gy gloss of normal myelinloss of normal myelinautoimmune/inflammatory componentautoimmune/inflammatory component
•• Dysmyelinating Dysmyelinating --loss of chemically abnormal myelinloss of chemically abnormal myeliny yy y
••Hypomyelinating Hypomyelinating --paucity of myelin formationpaucity of myelin formationpaucity of myelin formationpaucity of myelin formation
•• Myelinolytic (Spongiform) Myelinolytic (Spongiform) --i l f li i li l i di l f li i li l i dcytotoxic loss of myelin, intramyelinolytic edemacytotoxic loss of myelin, intramyelinolytic edema
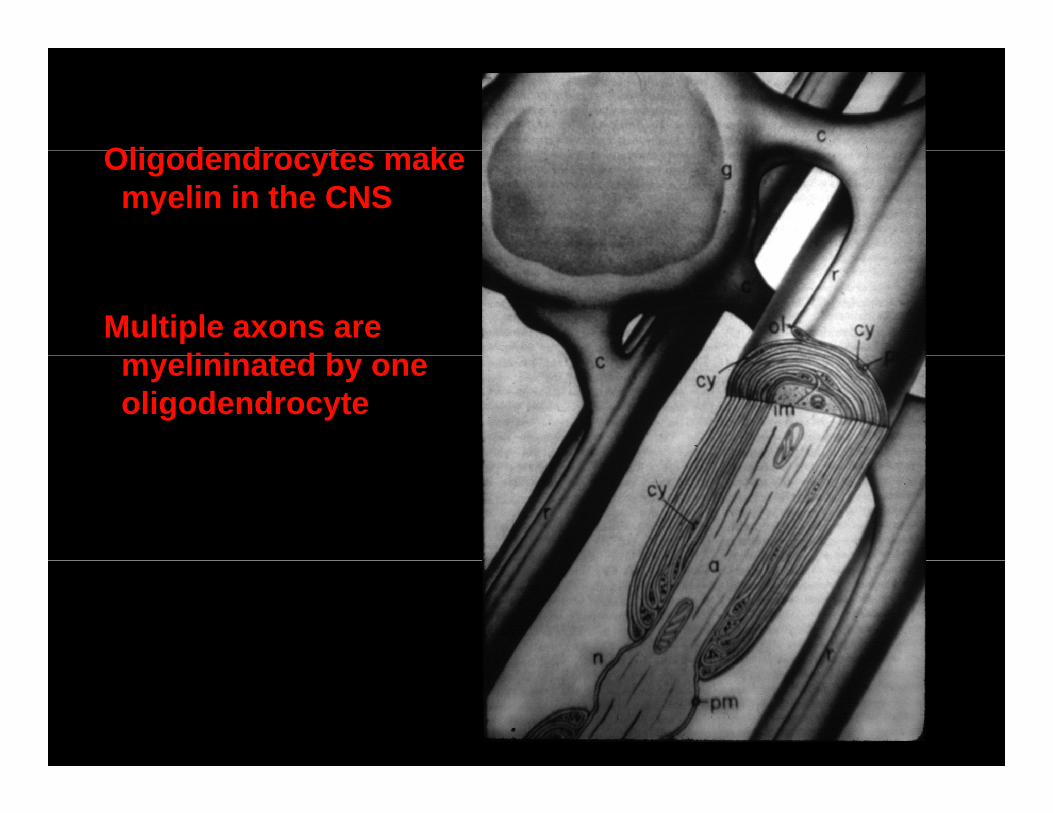
Oli d d t kOligodendrocytes makemyelin in the CNS
Multiple axons areli i t d bmyelininated by one
oligodendrocyte
Demyelinating DiseasesDemyelinating Diseasesy gy g
•• Multiple SclerosisMultiple SclerosisMultiple SclerosisMultiple Sclerosis
•• Acute Disseminated EncephalomyelitisAcute Disseminated Encephalomyelitis
•• Acute Hemorrhagic LeukoencephalitisAcute Hemorrhagic Leukoencephalitis
•• Progressive Multifocal LeukoencephalopathyProgressive Multifocal Leukoencephalopathy
•• Subacute Sclerosing PanencephalitisSubacute Sclerosing Panencephalitis•• Subacute Sclerosing PanencephalitisSubacute Sclerosing Panencephalitis
•• Idopathic Polyneuritis (LandryIdopathic Polyneuritis (Landry--GuillainGuillain--Barre)Barre)

Multiple SclerosisMultiple Sclerosis
•• Episodic neurologic signs and symptoms referable to differentEpisodic neurologic signs and symptoms referable to differentEpisodic neurologic signs and symptoms referable to differentEpisodic neurologic signs and symptoms referable to differentparts of the neuraxis (“disseminated in time and space”)parts of the neuraxis (“disseminated in time and space”)
Att k f ll d b l t ti l i iAtt k f ll d b l t ti l i i•• Attacks followed by complete or partial remissionAttacks followed by complete or partial remission
•• Peak age of onset is 20Peak age of onset is 20--40 years; more common in women40 years; more common in women
•• Chronic relapsing (“classical”) and rapidly progressing formsChronic relapsing (“classical”) and rapidly progressing forms
•• Diagnosis established by clinical history, MRI, Diagnosis established by clinical history, MRI, CSF analysis (oligoclonal bands)CSF analysis (oligoclonal bands)
“Classical” Multiple Sclerosis“Classical” Multiple SclerosisClassical Multiple SclerosisClassical Multiple Sclerosis
•• Prevalence:Prevalence:•• 3030--120/100,000 in Northern Latitudes120/100,000 in Northern Latitudes
•• Etiology:Etiology:G iG i•• Genetic FactorsGenetic Factors
•• Environmental FactorsEnvironmental Factors•• Immunologic PathogenesisImmunologic Pathogenesis•• Immunologic PathogenesisImmunologic Pathogenesis
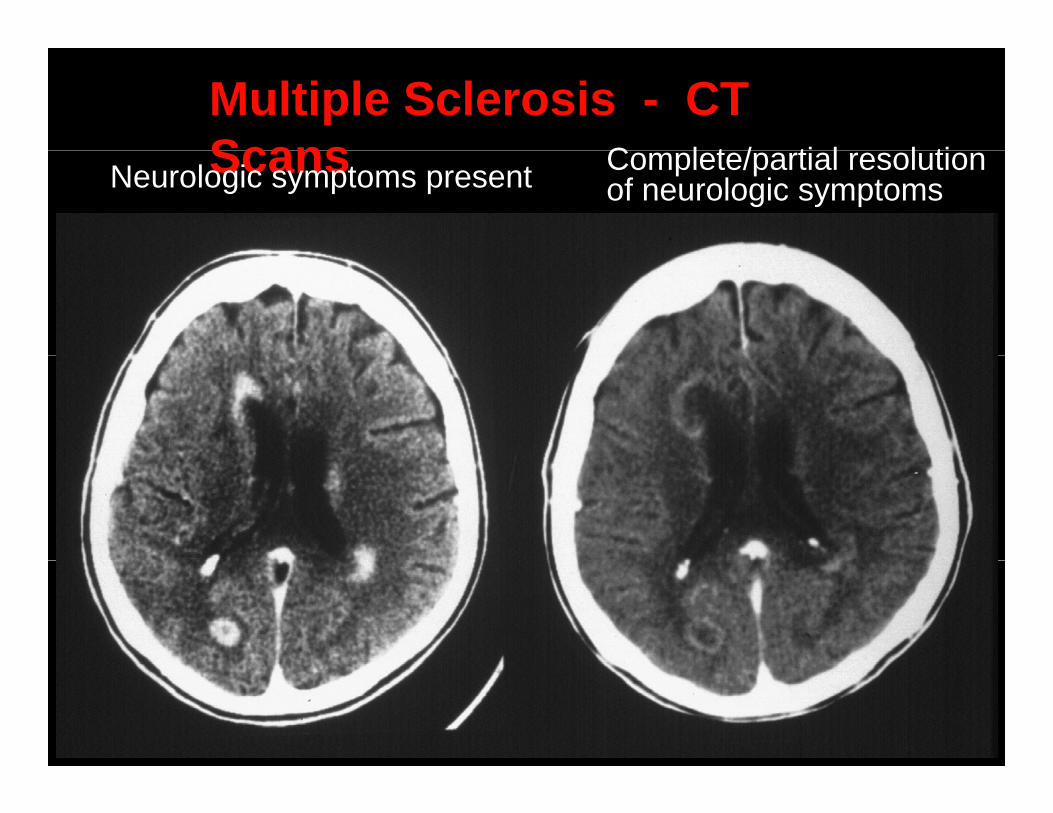
Multiple Sclerosis - CT Scans C l t / ti l l tiScansNeurologic symptoms present Complete/partial resolution
of neurologic symptoms
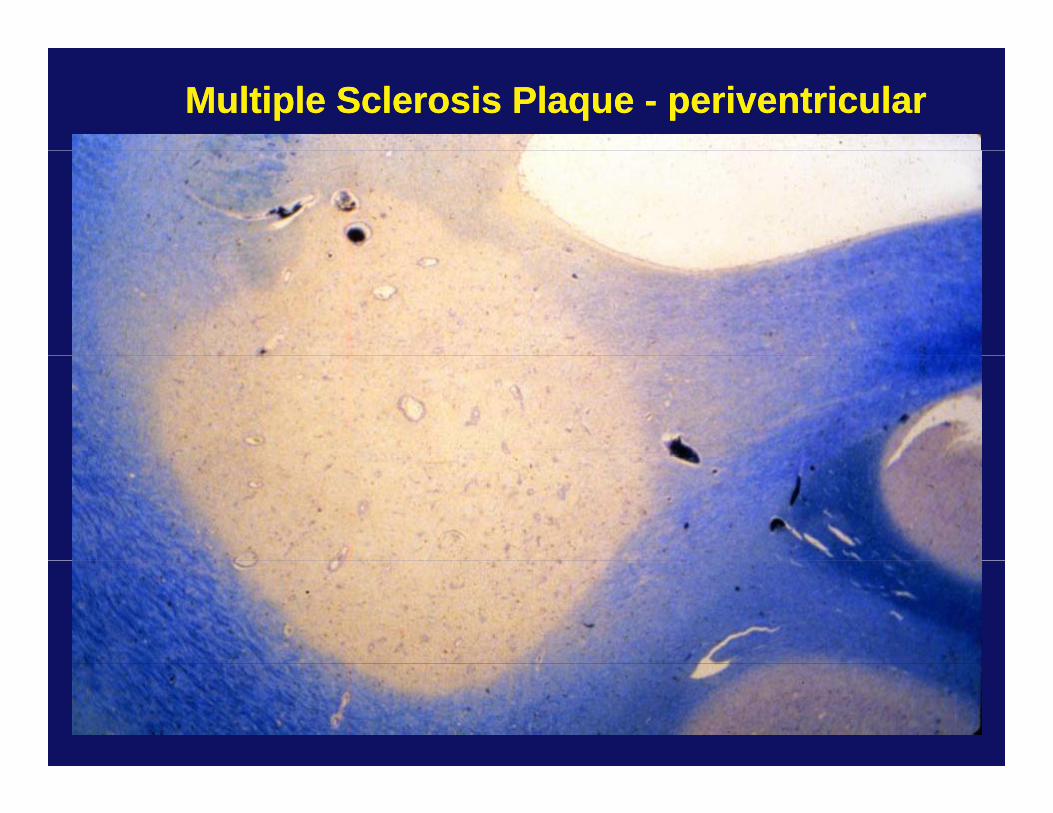
Multiple Sclerosis Plaque Multiple Sclerosis Plaque -- periventricularperiventricular
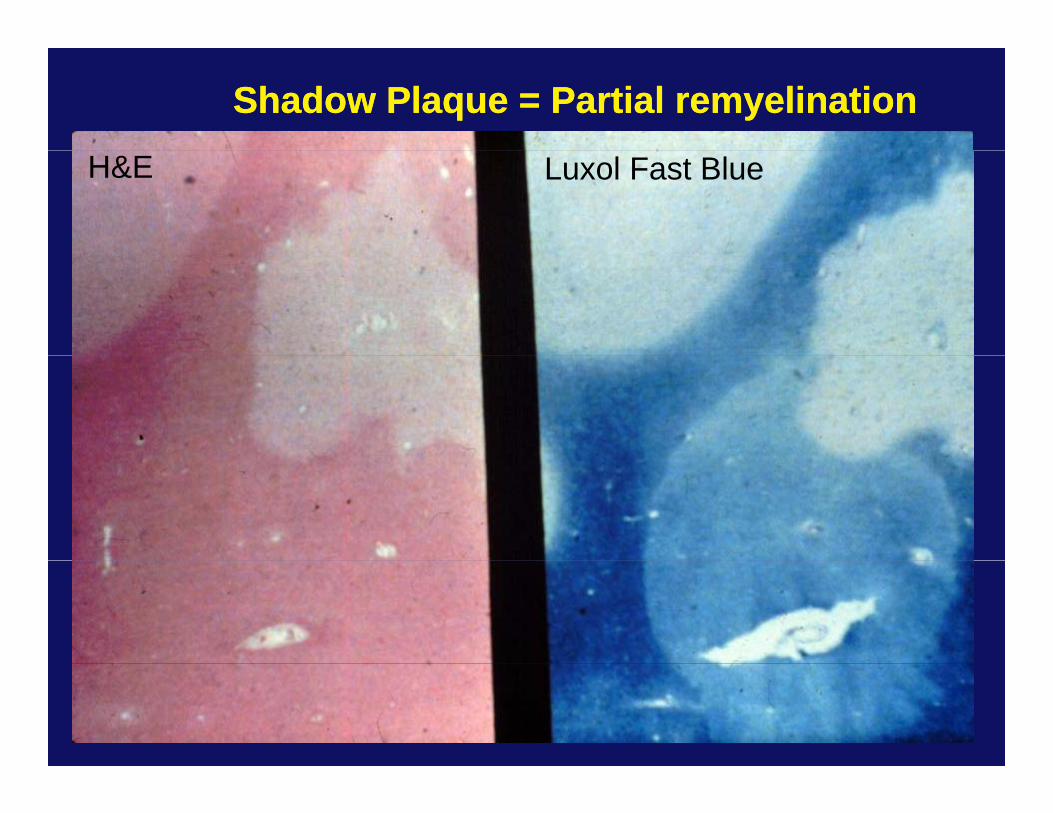
Shadow Plaque = Partial remyelinationShadow Plaque = Partial remyelination
H&E Luxol Fast Blue
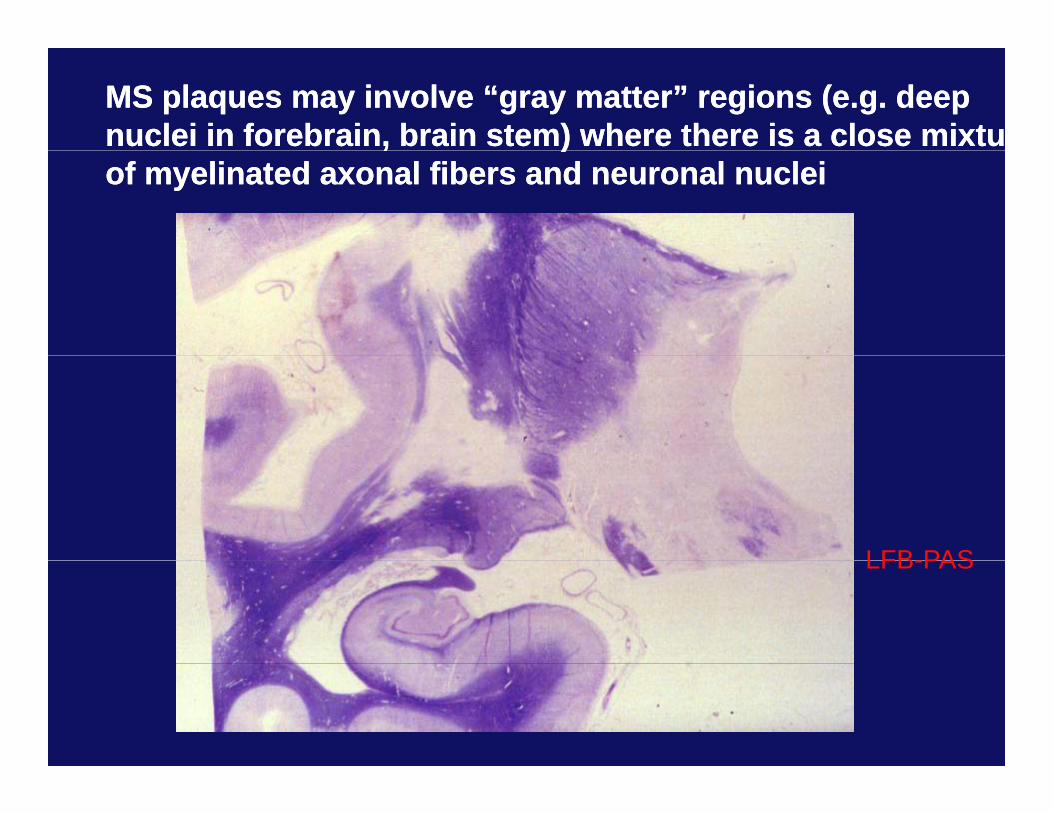
MS plaques may involve “gray matter” regions (e.g. deepMS plaques may involve “gray matter” regions (e.g. deepnuclei in forebrain, brain stem) where there is a close mixtunuclei in forebrain, brain stem) where there is a close mixtu, ), )of myelinated axonal fibers and neuronal nucleiof myelinated axonal fibers and neuronal nuclei
LFB-PASLFB-PAS
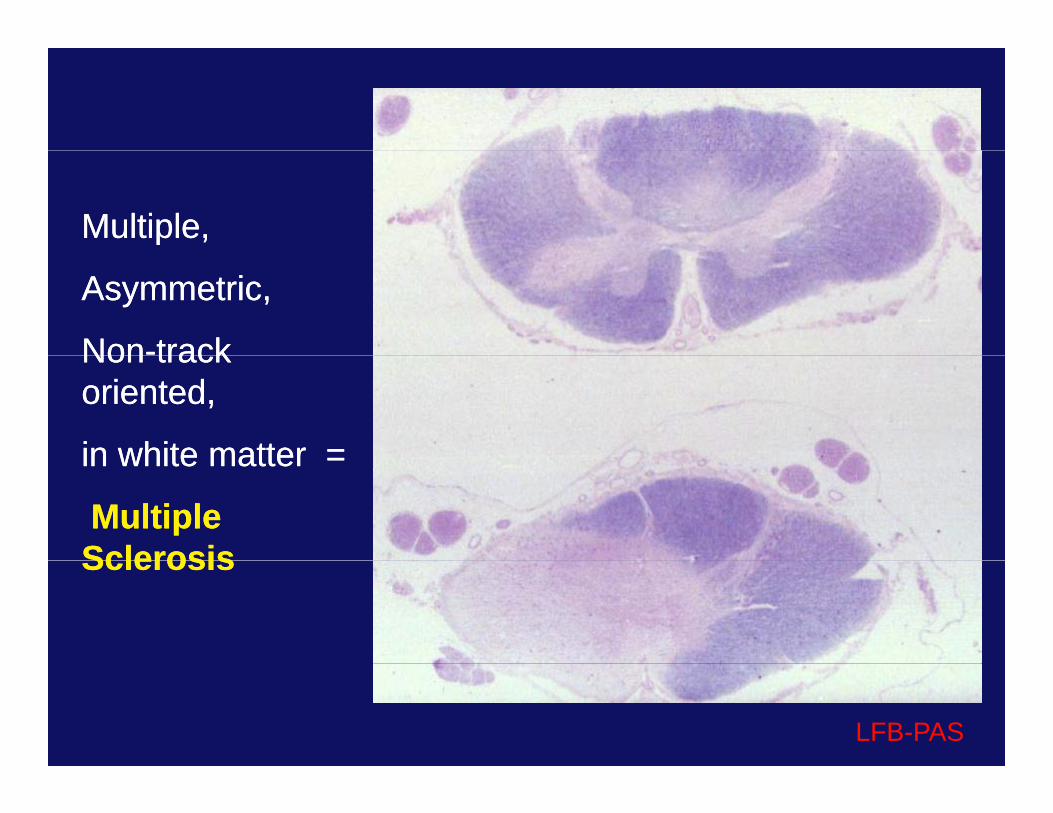
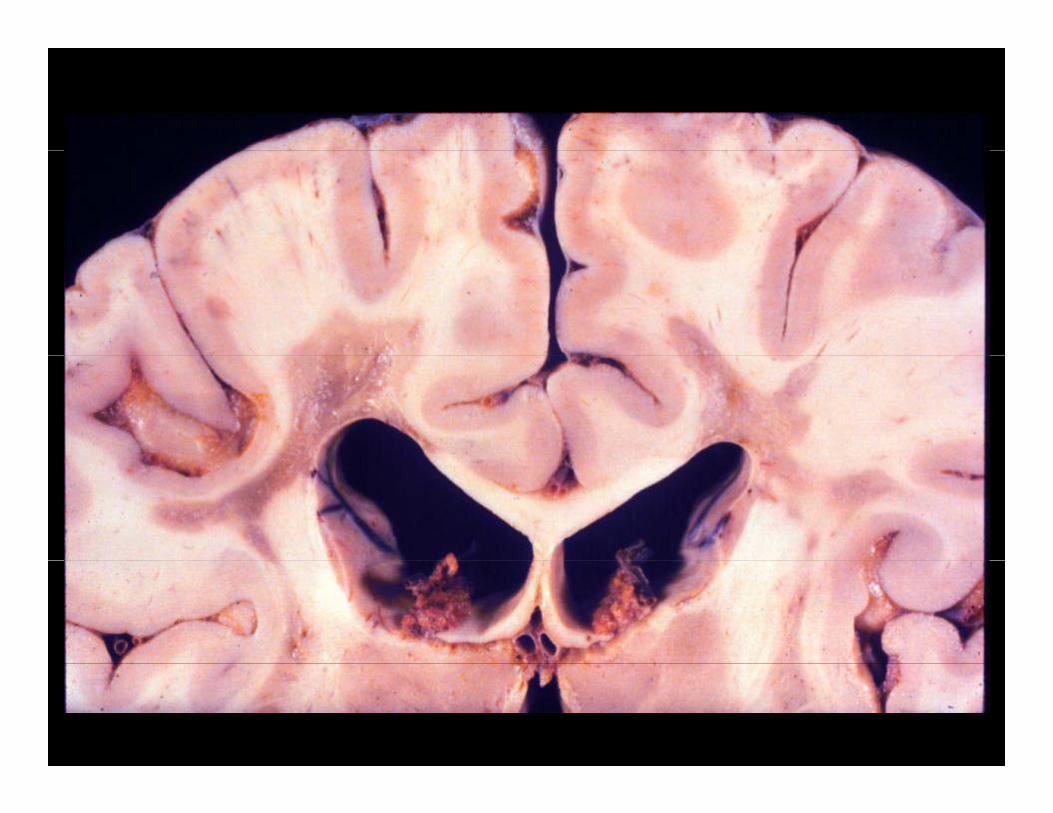
Multiple, Multiple,
Asymmetric,Asymmetric,
NonNon--tracktrackNonNon track track oriented,oriented,
in white matter =in white matter =in white matter = in white matter =
Multiple Multiple SclerosisSclerosisSclerosisSclerosis
LFB-PAS
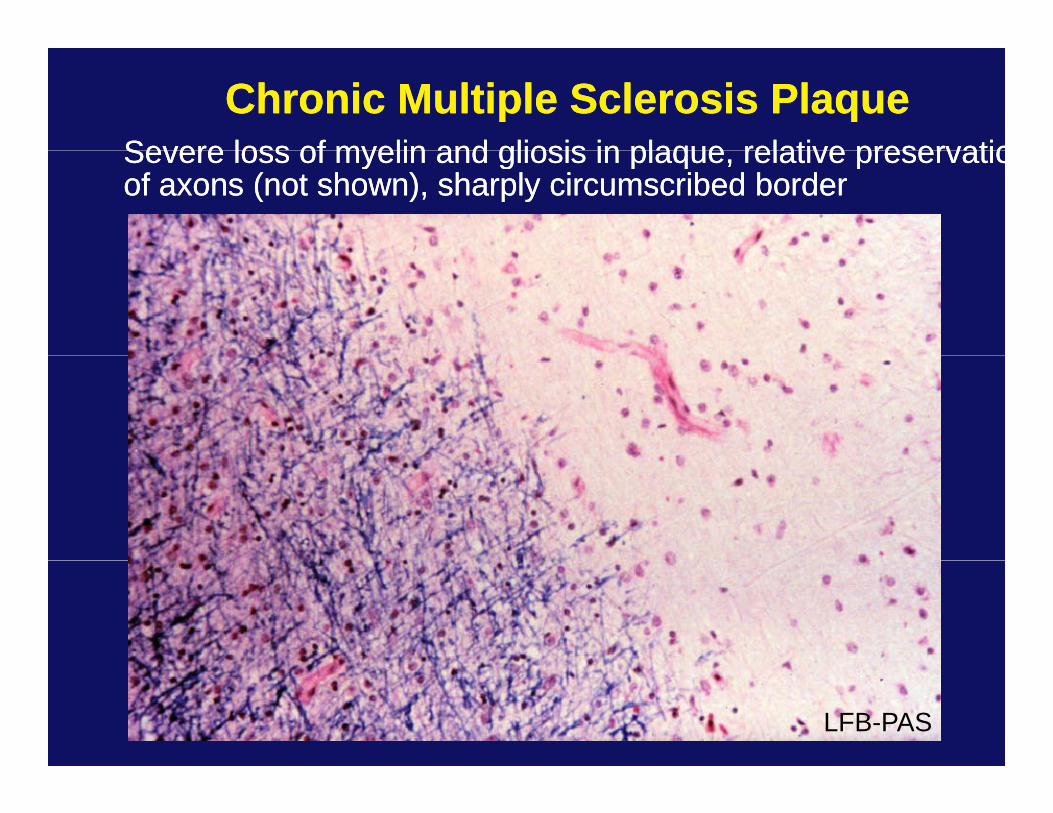
Chronic Multiple Sclerosis PlaqueChronic Multiple Sclerosis PlaqueSevere loss of myelin and gliosis in plaque relative preservatioSevere loss of myelin and gliosis in plaque relative preservatioSevere loss of myelin and gliosis in plaque, relative preservatioSevere loss of myelin and gliosis in plaque, relative preservatioof axons (not shown), sharply circumscribed borderof axons (not shown), sharply circumscribed border
LFB-PAS
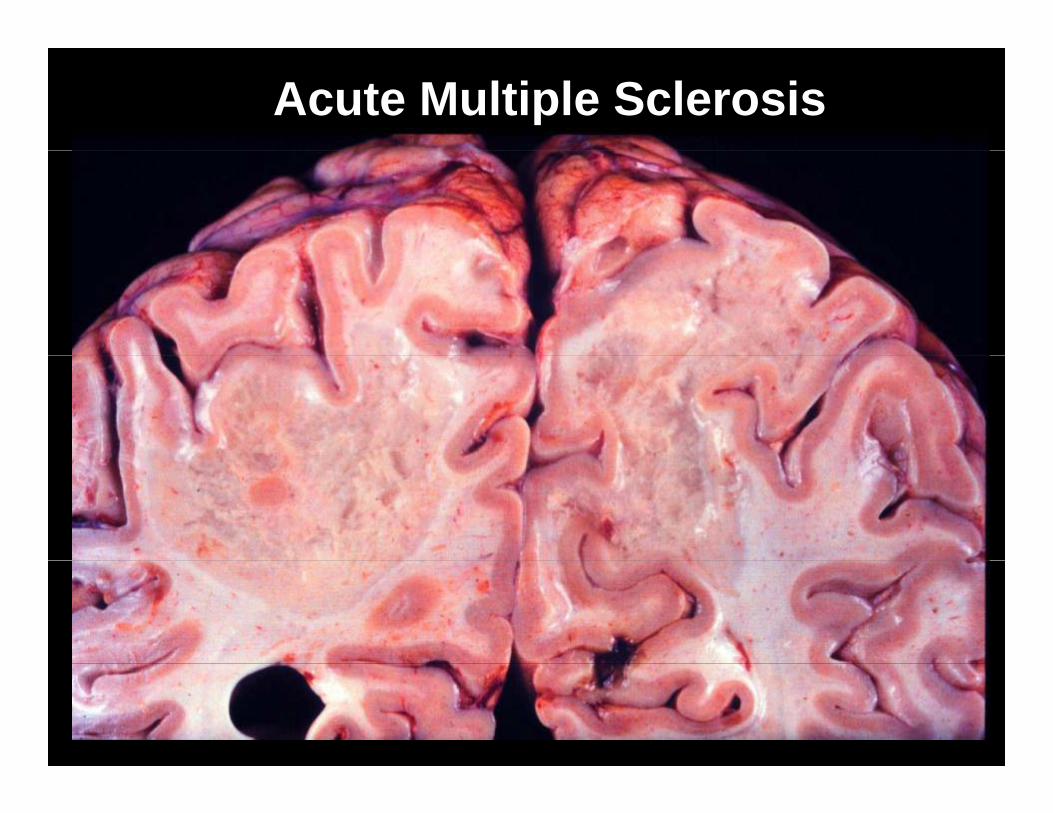
Acute Multiple Sclerosis
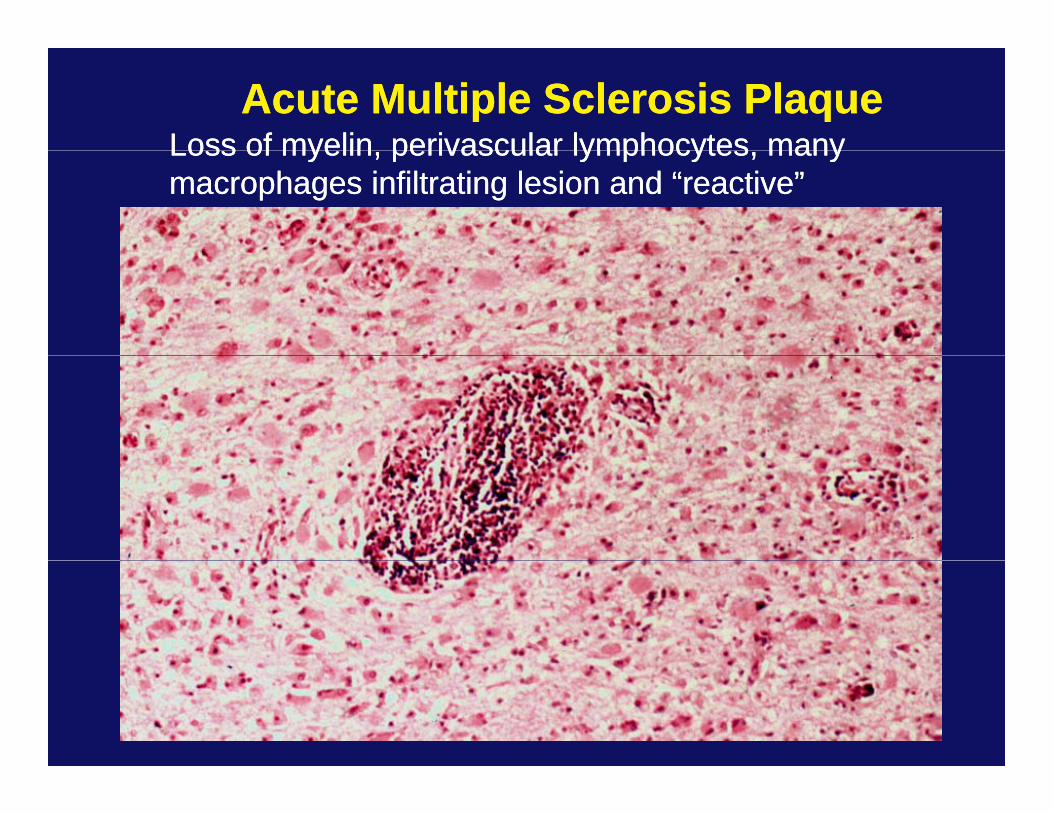
Acute Multiple Sclerosis PlaqueAcute Multiple Sclerosis PlaqueLoss of myelin perivascular lymphocytes manyLoss of myelin perivascular lymphocytes manyLoss of myelin, perivascular lymphocytes, many Loss of myelin, perivascular lymphocytes, many macrophages infiltrating lesion and “reactive” macrophages infiltrating lesion and “reactive” astrocytesastrocytes
LFB-PAS
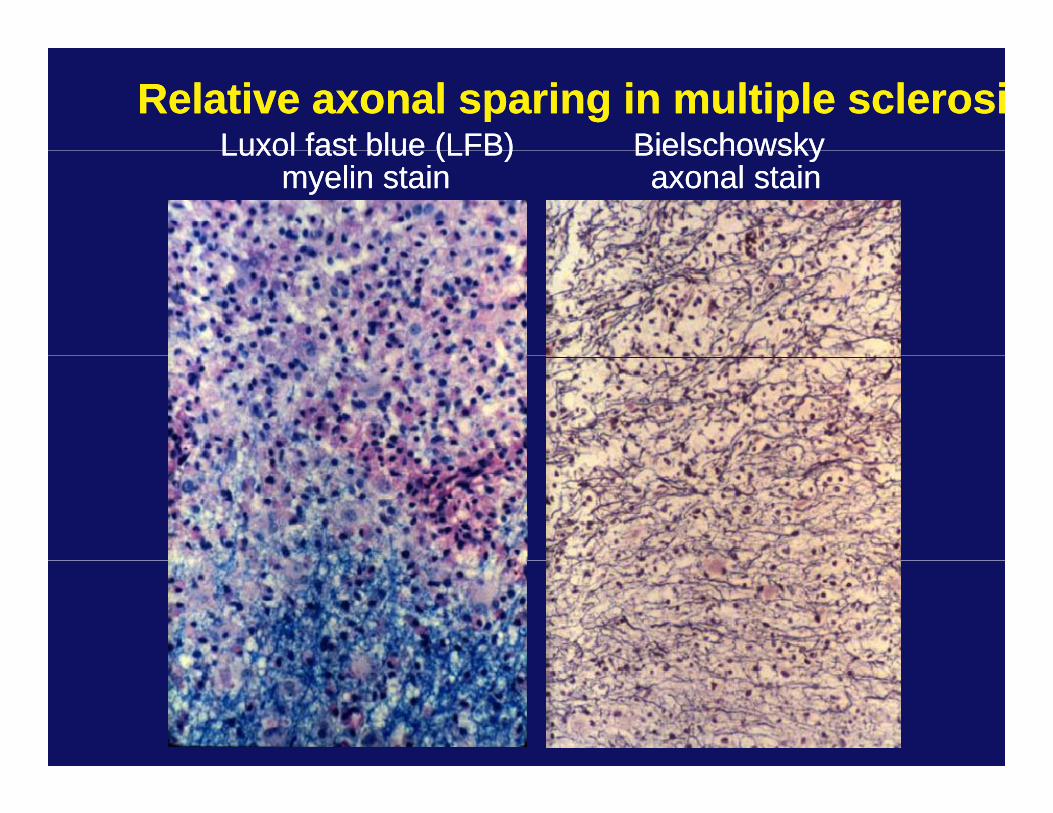
Relative axonal sparing in multiple sclerosiRelative axonal sparing in multiple sclerosiLuxol fast blue (LFB)Luxol fast blue (LFB) BielschowskyBielschowskyLuxol fast blue (LFB) Luxol fast blue (LFB)
myelin stain myelin stain Bielschowsky Bielschowsky axonal stainaxonal stain
Acute Disseminated EncephalomyelitisAcute Disseminated EncephalomyelitisAcute Disseminated EncephalomyelitisAcute Disseminated Encephalomyelitis
•• Monophasic illness, lasting ~2 to 4 weeks Monophasic illness, lasting ~2 to 4 weeks p , gp , g
•• Affects predominantly children and young adultsAffects predominantly children and young adults
•• Usually follows an infection also immunizationsUsually follows an infection also immunizations•• Usually follows an infection, also immunizationsUsually follows an infection, also immunizations•• Immune mediated complicationImmune mediated complication
•• Acute onset of multifocal neurologic disturbancesAcute onset of multifocal neurologic disturbances•• Acute onset of multifocal neurologic disturbancesAcute onset of multifocal neurologic disturbances
•• Most patients recover (early recognition andMost patients recover (early recognition andsteroid treatment)steroid treatment)steroid treatment)steroid treatment)
•• Perivenous inflammation and demyelination, Perivenous inflammation and demyelination, punctate to confluent, widespread in neuraxispunctate to confluent, widespread in neuraxisp pp p
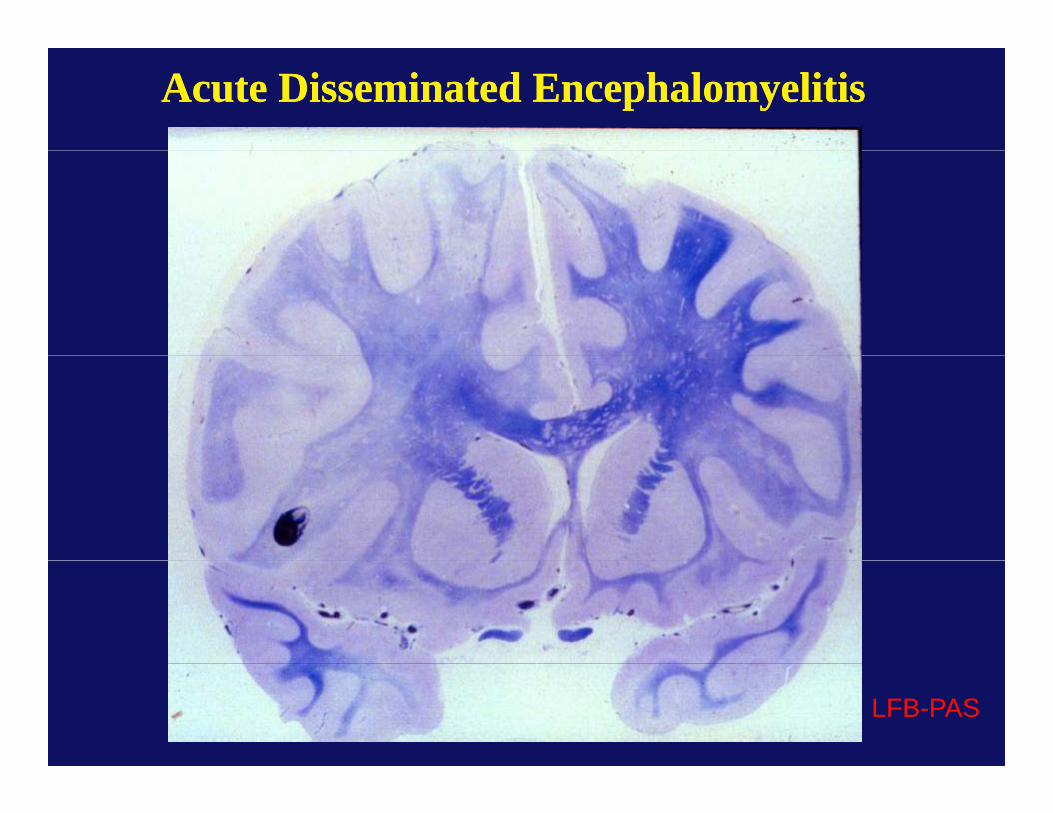
Acute Disseminated EncephalomyelitisAcute Disseminated Encephalomyelitis
LFB-PAS
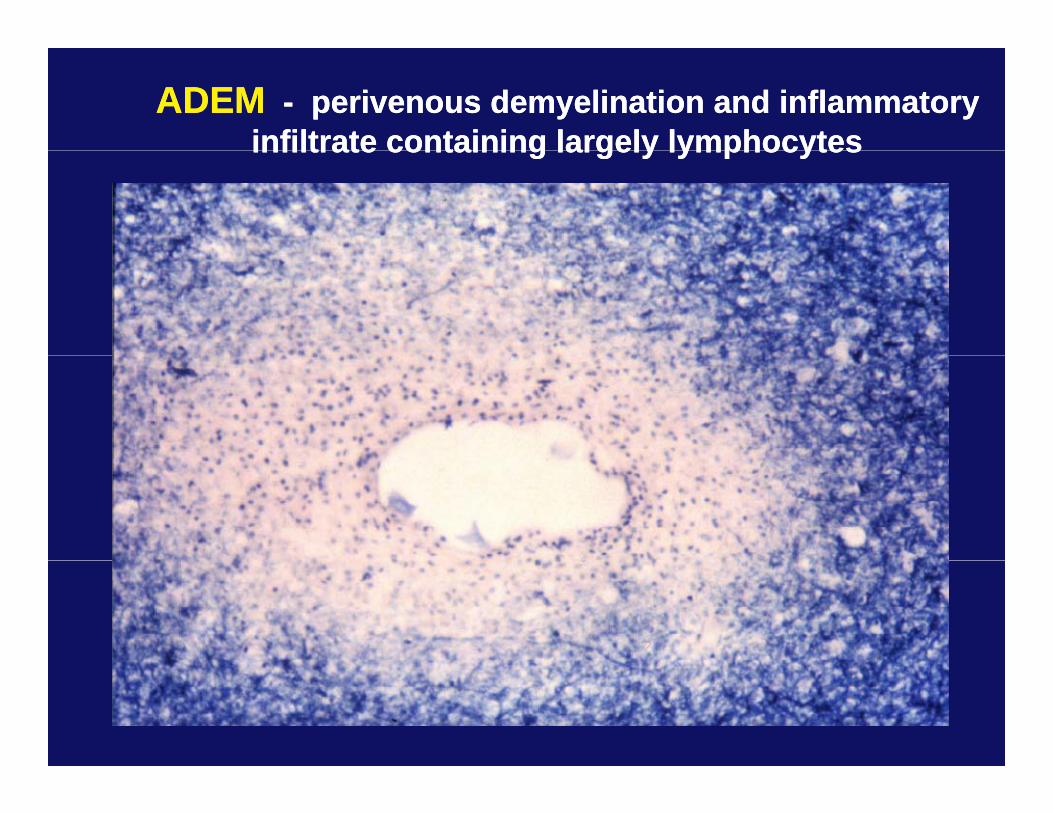
ADEMADEM -- perivenous demyelination and inflammatory perivenous demyelination and inflammatory infiltrate containing largely lymphocytesinfiltrate containing largely lymphocytesinfiltrate containing largely lymphocytesinfiltrate containing largely lymphocytes
Dysmyelinating DiseasesDysmyelinating Diseases•• inherited disordersinherited disordersinherited disordersinherited disorders•• chemically abnormal myelinchemically abnormal myelin
•• Metachromatic LeukodystrophyMetachromatic Leukodystrophy
•• Globoid Cell LeukodystrophyGloboid Cell Leukodystrophy
•• AdrenoleukodystrophyAdrenoleukodystrophy
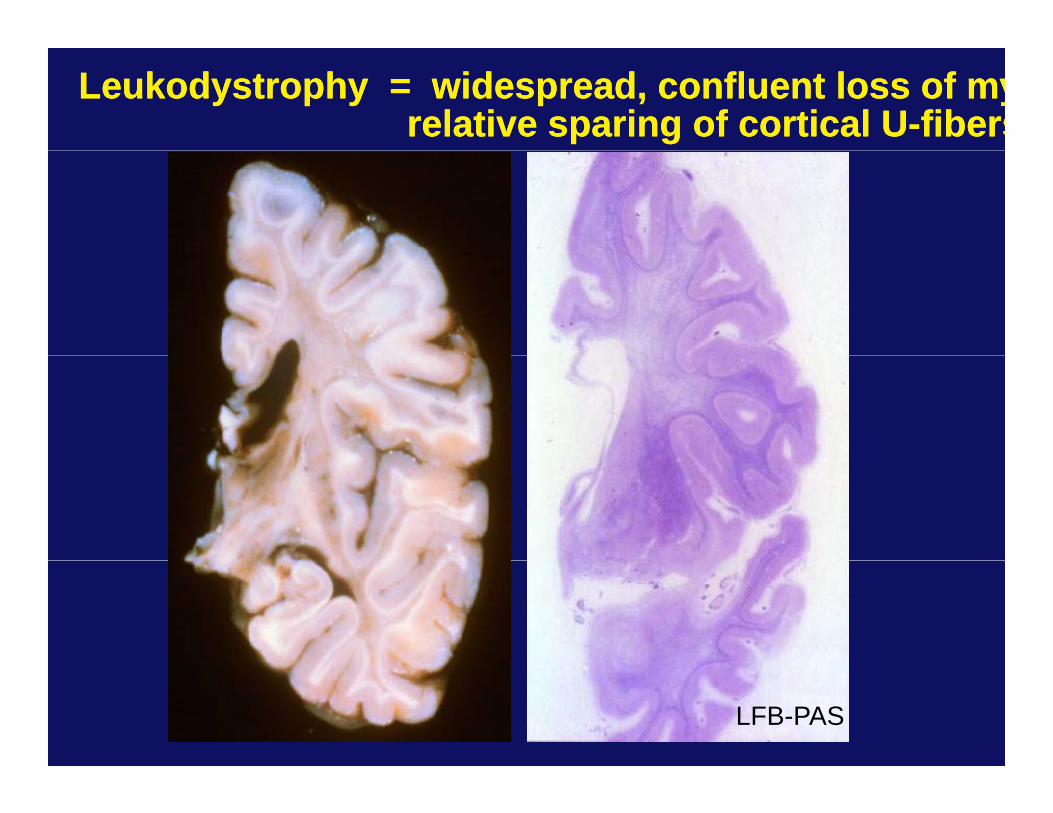
Leukodystrophy = widespread, confluent loss of myLeukodystrophy = widespread, confluent loss of myrelative sparing of cortical Urelative sparing of cortical U--fibersfibers
LFB-PAS
Metachromatic LeukodystrophyMetachromatic Leukodystrophy
•• Deficiency of the lysosomal enzyme arylsulfatase A;Deficiency of the lysosomal enzyme arylsulfatase A;autosomal recessiveautosomal recessiveautosomal recessiveautosomal recessive
•• Late infantile form most common, onset 1Late infantile form most common, onset 1--2 years;2 years;i t di bilit i t ll t l d lii t di bilit i t ll t l d liprogressive motor disability, intellectual decline,progressive motor disability, intellectual decline,
rapid demiserapid demise
•• “Metachromatic” deposits of sulfatide in CNS, PNS,“Metachromatic” deposits of sulfatide in CNS, PNS,and kidneyand kidney
•• Diagnosis made by measurement of enzyme activity, Diagnosis made by measurement of enzyme activity, urinary sulfatide excretion; prenatal diagnosis isurinary sulfatide excretion; prenatal diagnosis is
ibliblpossiblepossible
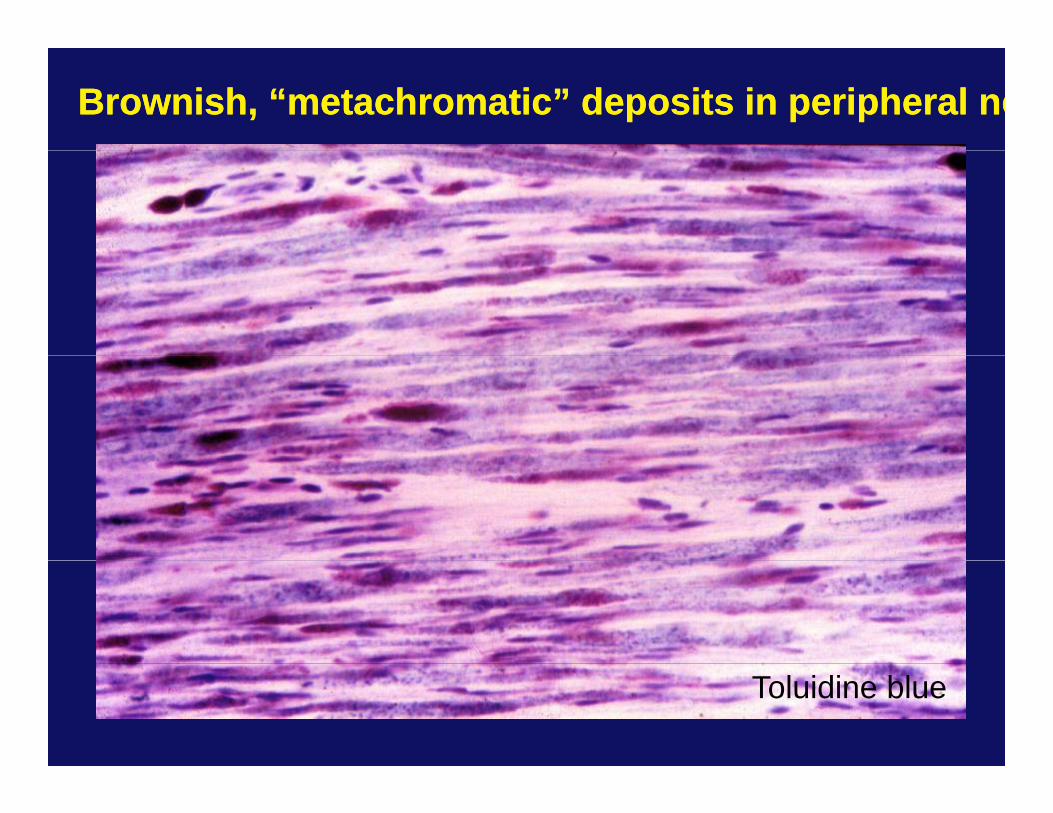
Brownish, “metachromatic” deposits in peripheral neBrownish, “metachromatic” deposits in peripheral ne
Toluidine blue
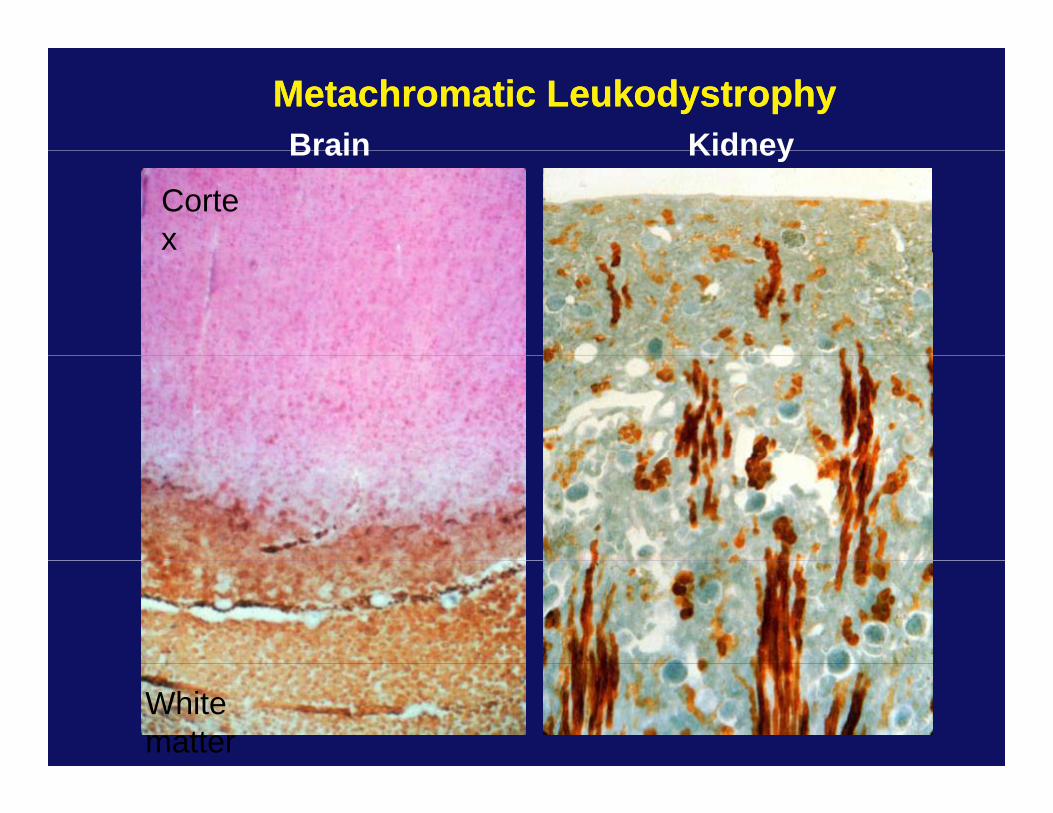
Metachromatic LeukodystrophyMetachromatic LeukodystrophyBrain KidneyBrain
Cortex
Kidney
White matter
Globoid cell Leukodystrophy (Krabbe’s disease)Globoid cell Leukodystrophy (Krabbe’s disease)
• Deficiency of the lysosomal enzyme betaDeficiency of the lysosomal enzyme beta--galactocerebrosidase;galactocerebrosidase;autosomal recessiveautosomal recessive
•• Onset and symptoms: Onset and symptoms: •• Late infancy most common (80%), usually before 6 monthsLate infancy most common (80%), usually before 6 months
•• developmental arrestdevelopmental arrest•• extreme irritability and crying followed by rigidity extreme irritability and crying followed by rigidity
and tonic spasms;and tonic spasms;and tonic spasms;and tonic spasms;•• frequent episodes of pyrexiafrequent episodes of pyrexia•• death by 1death by 1--2 years with continued seizures 2 years with continued seizures yy yy
and opisthotonusand opisthotonus•• CNS pathology due to accumulation of psychosineCNS pathology due to accumulation of psychosine
•• May also affect the peripheral nervous systemMay also affect the peripheral nervous system
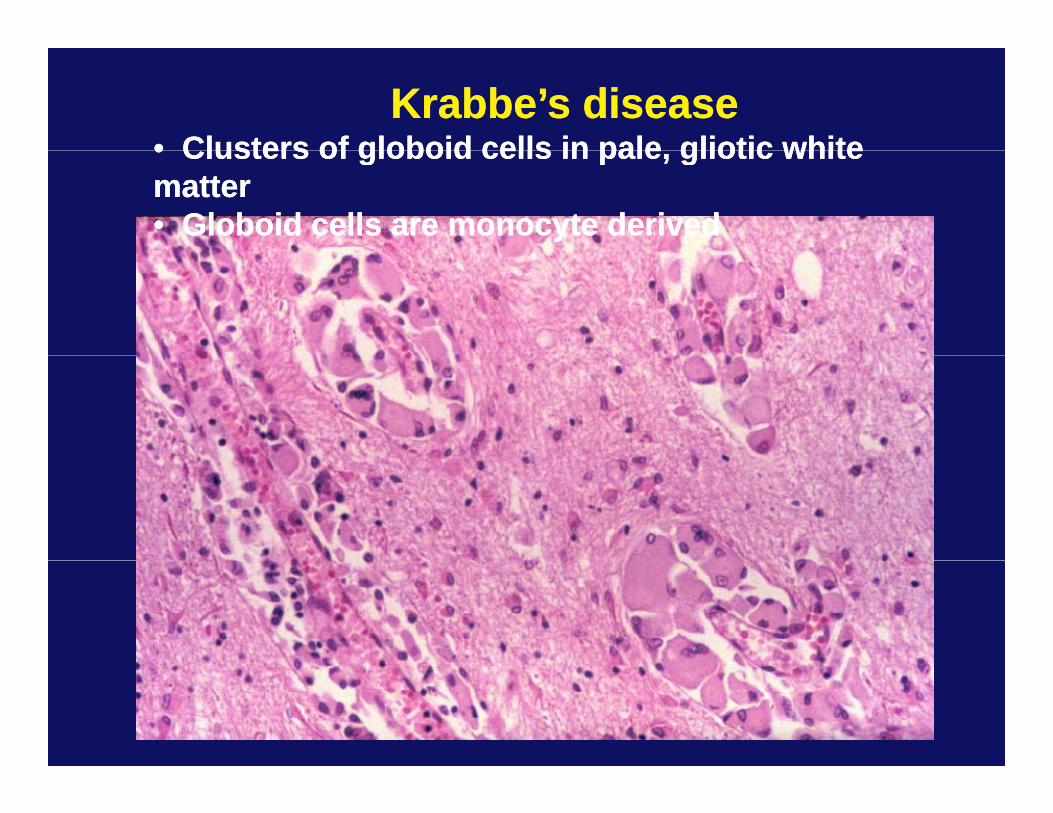
Krabbe’s diseaseKrabbe’s disease•• Clusters of globoid cells in pale gliotic whiteClusters of globoid cells in pale gliotic white•• Clusters of globoid cells in pale, gliotic white Clusters of globoid cells in pale, gliotic white mattermatter•• Globoid cells are monocyte derivedGloboid cells are monocyte derived
AdrenoleukodystrophyAdrenoleukodystrophy
•• INHERITANCE:INHERITANCE: XX--linked recessive (Xq28)linked recessive (Xq28)
•• ONSET:ONSET: 44--8 years (childhood cerebral form)8 years (childhood cerebral form)
•• SYMPTOMOTOLOGY:SYMPTOMOTOLOGY: Disturbances in affective behaviorDisturbances in affective behaviorN l i d fi itN l i d fi itNeurologic deficitsNeurologic deficitsAdrenal insufficiency Adrenal insufficiency
•• AVG AGE AT DEATH:AVG AGE AT DEATH: 10 years10 years•• AVG AGE AT DEATH:AVG AGE AT DEATH: 10 years10 years
•• BIOCHEMICAL DEFECT:BIOCHEMICAL DEFECT: Peroxisomal disorderPeroxisomal disorderAccumulation of VLCFA (>C22:0)Accumulation of VLCFA (>C22:0)( )( )
due to defective betadue to defective beta--oxidation oxidation Mutations in ALDP gene, anMutations in ALDP gene, an
ABC transporterABC transporter
AdrenoleukodystrophyAdrenoleukodystrophyChildh d b lChildh d b lChildhood cerebralChildhood cerebral (peak age of onset 4(peak age of onset 4--8 years)8 years)
Age of onset and extent of lesions at presentationAge of onset and extent of lesions at presentation(by MRI scans) are predictive of clinical course(by MRI scans) are predictive of clinical course
AdrenomyeloneuropathyAdrenomyeloneuropathy (peak age of onset 20(peak age of onset 20--30 years)30 years)Slowly progressive (over decades) spastic paraparesis,Slowly progressive (over decades) spastic paraparesis,y p g ( ) p p p ,y p g ( ) p p p ,sphincter disturbance due to spinal cord involvement;sphincter disturbance due to spinal cord involvement;variable cerebral involvementvariable cerebral involvement
Adult cerebralAdult cerebralCerebral symptoms after age 21, no spinal involvementCerebral symptoms after age 21, no spinal involvement
Adrenal insufficiency onlyAdrenal insufficiency only (“Addison disease” in men)(“Addison disease” in men)
Symptomatic ALD HeterozygotesSymptomatic ALD Heterozygotes (women age 25(women age 25 55 years)55 years)Symptomatic ALD Heterozygotes Symptomatic ALD Heterozygotes (women age 25(women age 25--55 years)55 years)61% with “neurologic abnormality”, widely varying severity61% with “neurologic abnormality”, widely varying severity
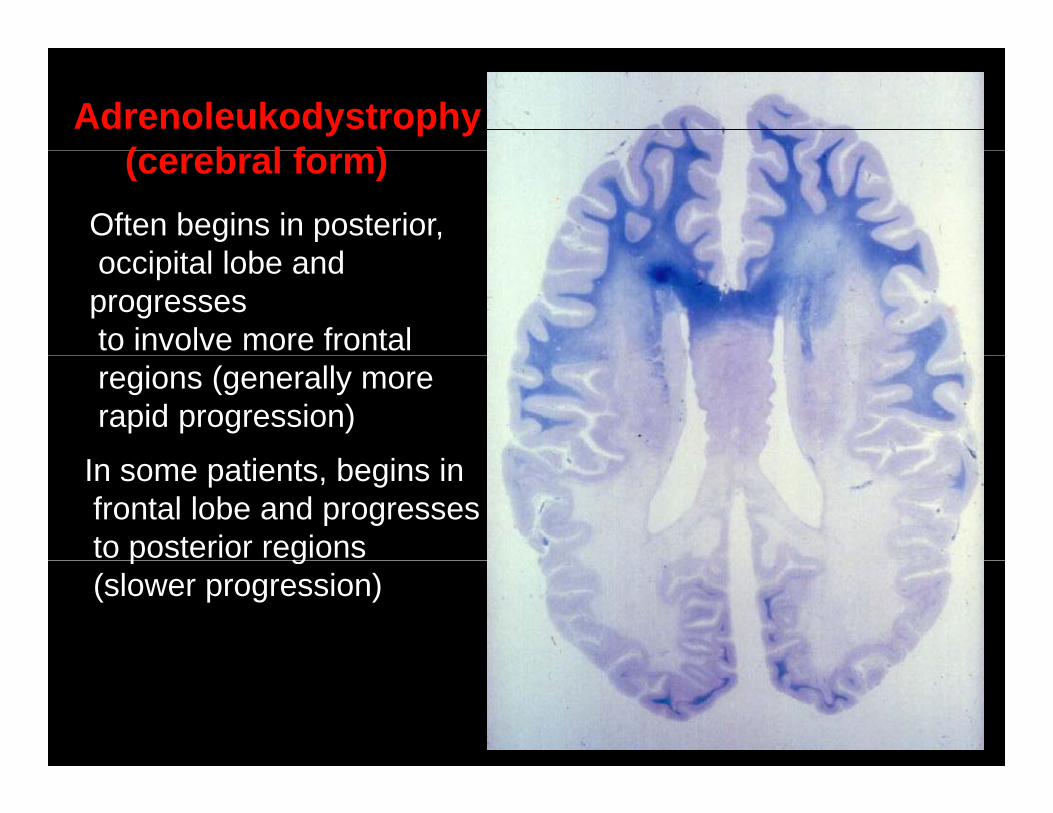
Adrenoleukodystrophy( b l f )(cerebral form)
Often begins in posterior, i it l l b doccipital lobe and
progressesto involve more frontal regions (generally morerapid progression)
In some patients, begins infrontal lobe and progressesto posterior regionsp g(slower progression)
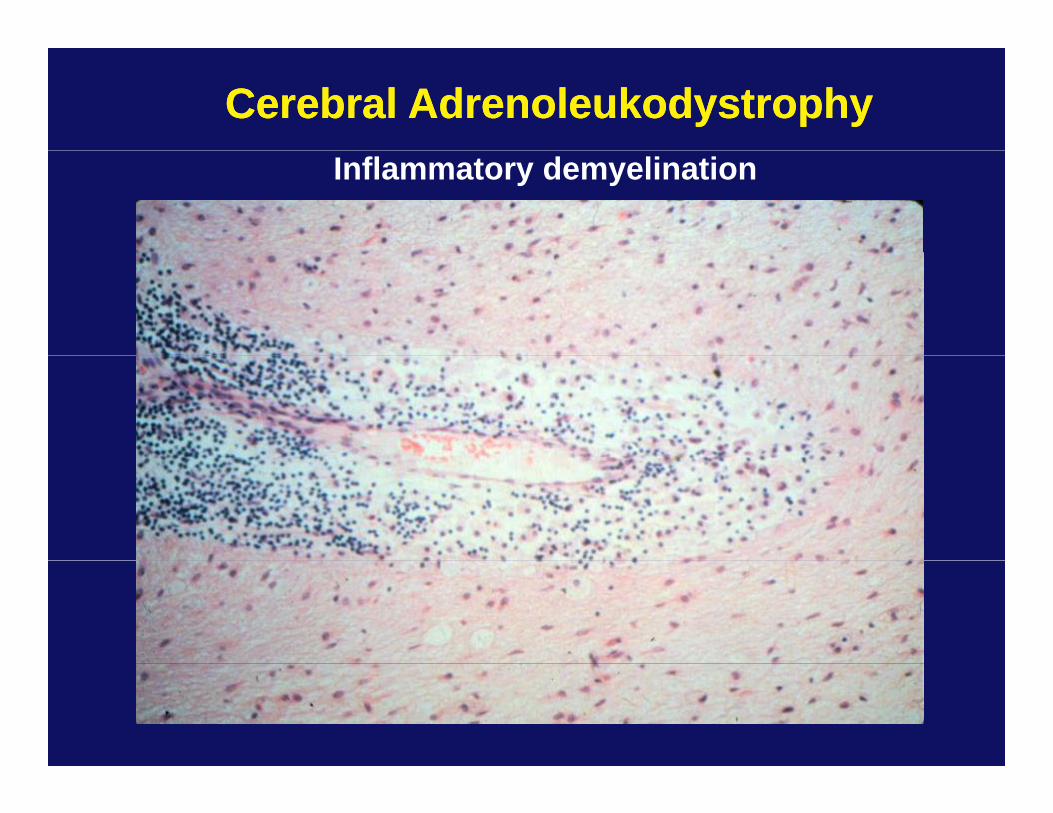
Cerebral AdrenoleukodystrophyCerebral AdrenoleukodystrophyInflammatory demyelination
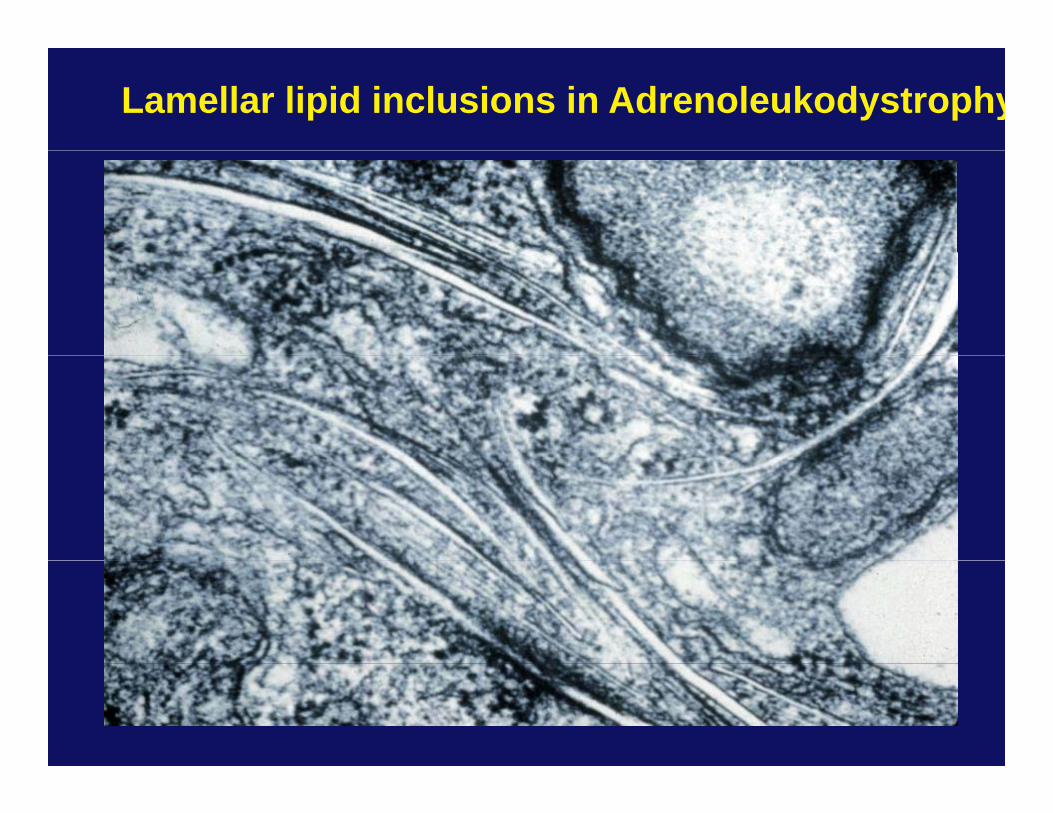
Lamellar lipid inclusions in Adrenoleukodystrophy
Treatment options in leukodystrophyTreatment options in leukodystrophy
•• Palliative measuresPalliative measures
•• Lorenzo’s oil for ALD may slow progression of childhood cerebralLorenzo’s oil for ALD may slow progression of childhood cerebraly p gy p gform when started before symptomatic; debate about utility in form when started before symptomatic; debate about utility in AMN patientsAMN patients
••Bone marrow transplantation, used in childhood cerebral ALD,Bone marrow transplantation, used in childhood cerebral ALD,Bone marrow transplantation, used in childhood cerebral ALD, Bone marrow transplantation, used in childhood cerebral ALD, globoid cell leukodystrophy and metachromatic leukodystrophygloboid cell leukodystrophy and metachromatic leukodystrophy
•• early transplantation and careful selection of patientsearly transplantation and careful selection of patients•• successfully treated patients have shown arrest and/orsuccessfully treated patients have shown arrest and/orsuccessfully treated patients have shown arrest and/or successfully treated patients have shown arrest and/or
reversal of CNS pathologyreversal of CNS pathology
•• Many experimental protocols:Many experimental protocols:•• peroxisome proliferator drugs in ALD: 4peroxisome proliferator drugs in ALD: 4--phenylbutyratephenylbutyrate•• combining gene transfer with bone marrow transplantationcombining gene transfer with bone marrow transplantation•• gene transfer to the nervous system, stem cells (!!!)gene transfer to the nervous system, stem cells (!!!)
Hypomyelinating DiseasesHypomyelinating Diseases
•• PelizaeusPelizaeus--Merzbacher DiseaseMerzbacher Disease
•• Alexander DiseaseAlexander Disease
•• CACH (Vanishing White Matter)CACH (Vanishing White Matter)
Alexander’s DiseaseAlexander’s DiseaseAlexander s DiseaseAlexander s Disease
•• Most often presents in infancy with increased head size, Most often presents in infancy with increased head size, p y ,p y ,psychomotor retardation, spasticity; rapidly progressivepsychomotor retardation, spasticity; rapidly progressive
•• Widespread demyelination in CNS with Rosenthal fibersWidespread demyelination in CNS with Rosenthal fibers•• Widespread demyelination in CNS with Rosenthal fibersWidespread demyelination in CNS with Rosenthal fibersin astrocytic processesin astrocytic processes
•• Usually sporadic; autosomal recessiveUsually sporadic; autosomal recessive
•• Majority of patients have mutations in glial fibrillary acidicMajority of patients have mutations in glial fibrillary acidicj y p g yj y p g yprotein, an intermediate filament protein of astrocytesprotein, an intermediate filament protein of astrocytes
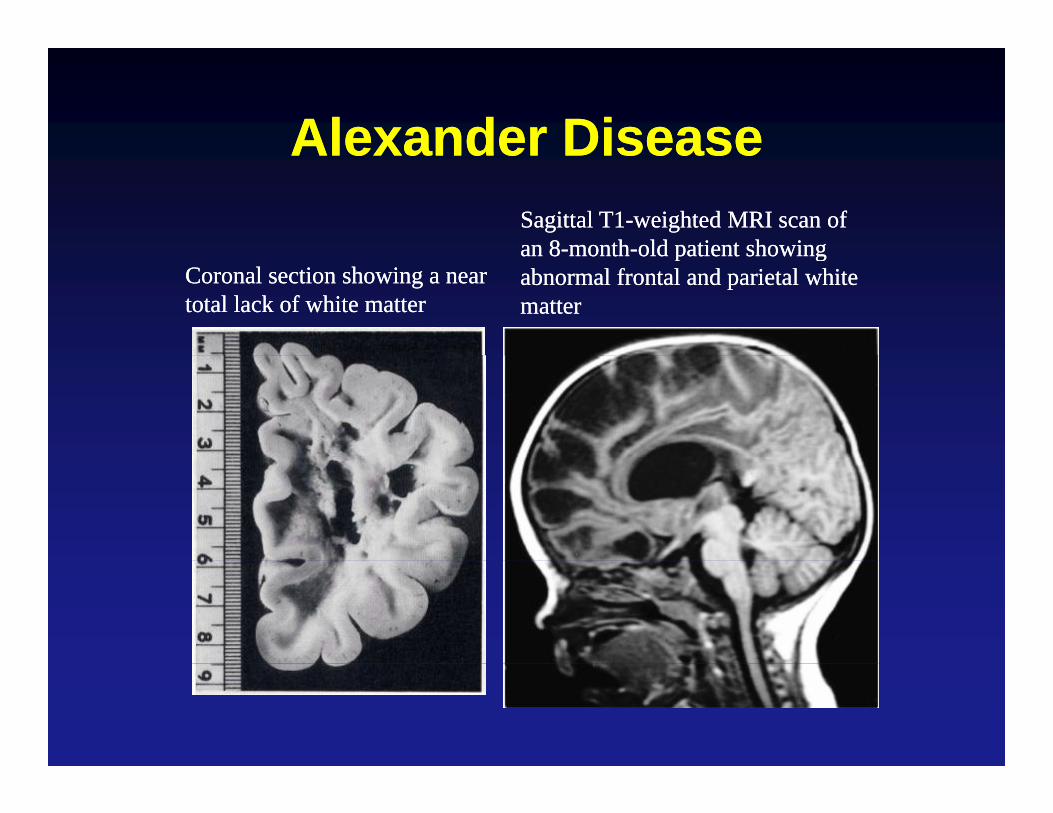
Alexander DiseaseAlexander DiseaseAlexander DiseaseAlexander DiseaseSagittal T1Sagittal T1--weighted MRI scan of weighted MRI scan of an 8an 8--monthmonth--old patient showingold patient showing
Coronal section showing a near Coronal section showing a near total lack of white mattertotal lack of white matter
an 8an 8 monthmonth old patient showingold patient showingabnormal frontal and parietal white abnormal frontal and parietal white mattermatter
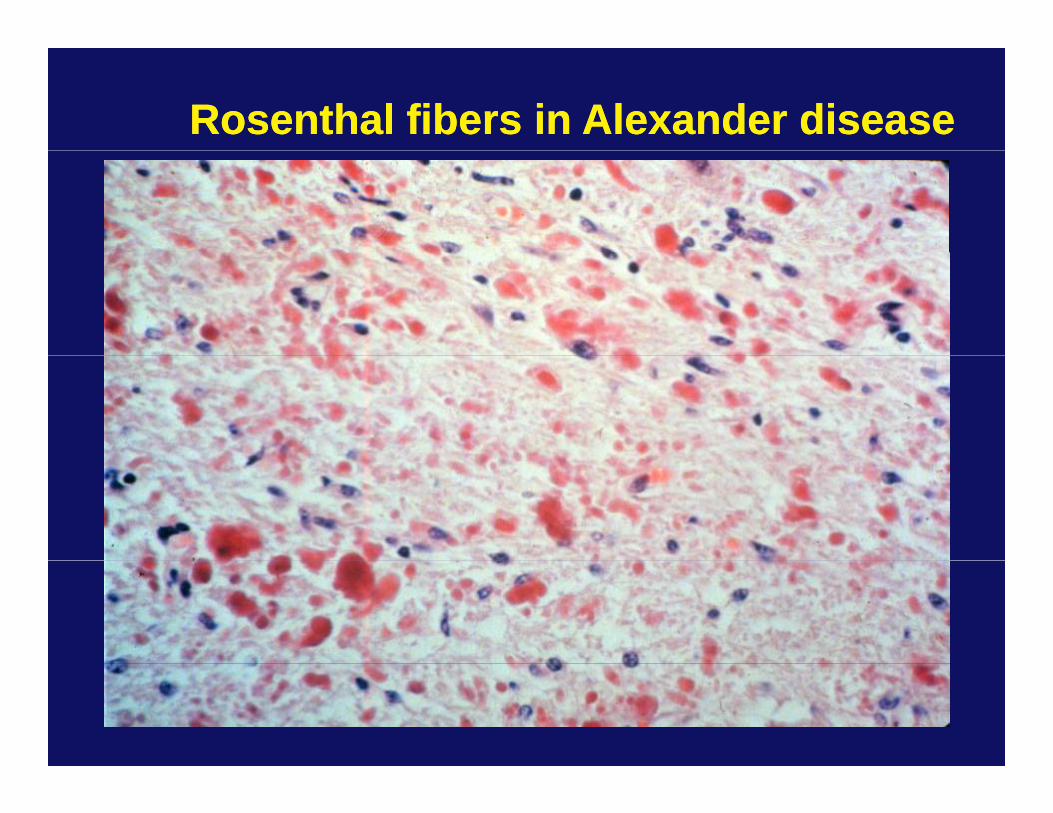
Rosenthal fibers in Alexander diseaseRosenthal fibers in Alexander disease
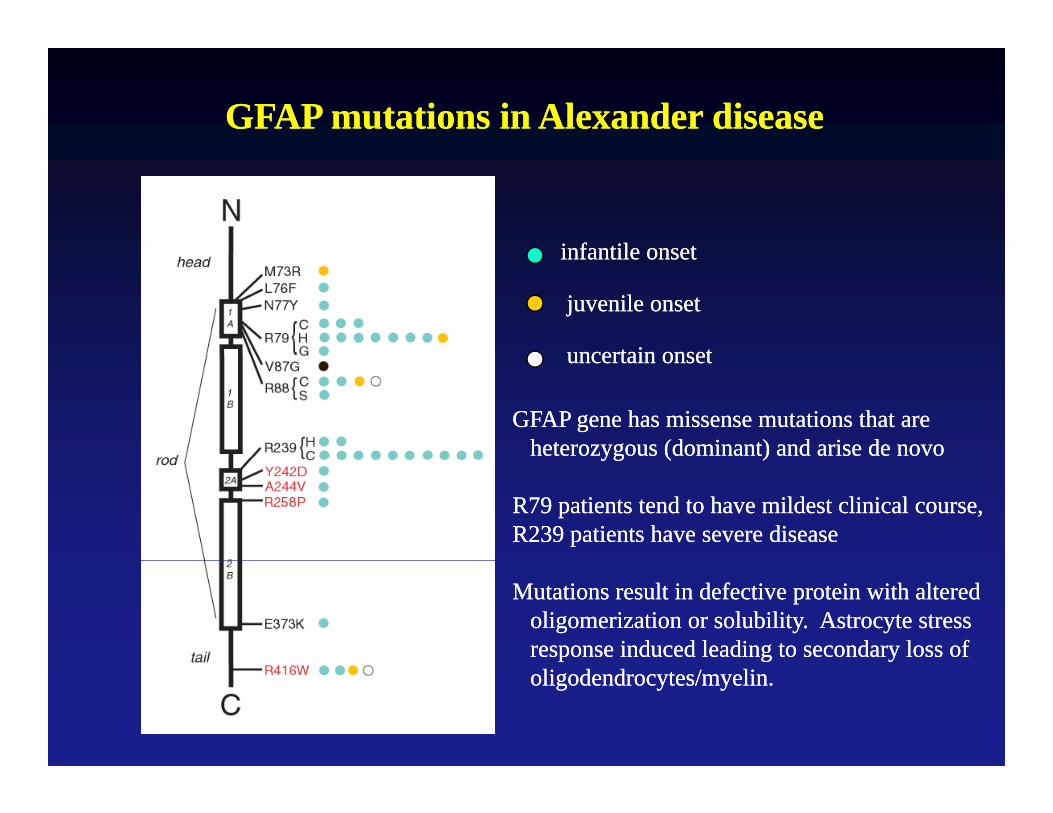
GFAP mutations in Alexander diseaseGFAP mutations in Alexander disease
infantile onsetinfantile onsetinfantile onsetinfantile onset
juvenile onsetjuvenile onset
uncertain onsetuncertain onsetuncertain onsetuncertain onset
GFAP gene has missense mutations that areGFAP gene has missense mutations that areheterozygous (dominant) and arise de novoheterozygous (dominant) and arise de novoyg ( )yg ( )
R79 patients tend to have mildest clinical course,R79 patients tend to have mildest clinical course,R239 patients have severe diseaseR239 patients have severe disease
Mutations result in defective protein with alteredMutations result in defective protein with alteredoligomerization or solubility. Astrocyte stressoligomerization or solubility. Astrocyte stressresponse induced leading to secondary loss of response induced leading to secondary loss of oligodendrocytes/myelin.oligodendrocytes/myelin.
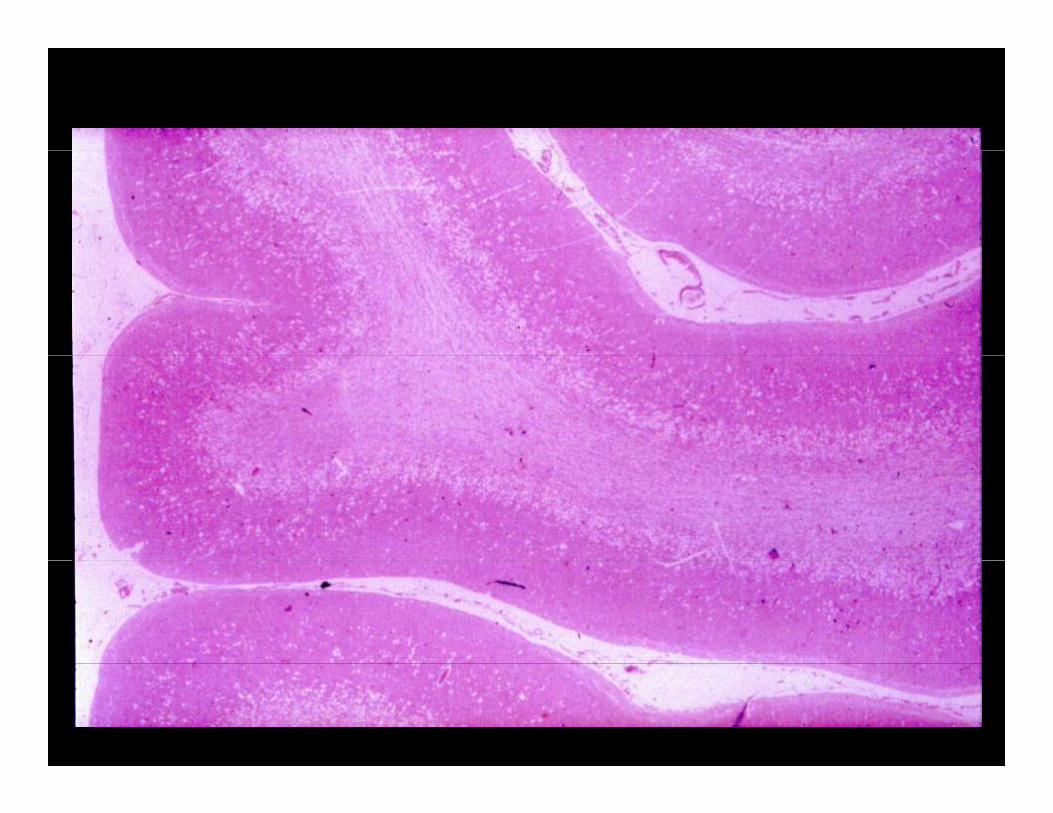
Myelinolytic DiseasesMyelinolytic DiseasesMyelinolytic DiseasesMyelinolytic Diseases
•• Central Pontine MyelinolysisCentral Pontine Myelinolysis
•• MarchiafavaMarchiafava--Bignami DiseaseBignami Disease
•• AminoaciduriasAminoacidurias
S D ti f I f (C )S D ti f I f (C )•• Spongy Degeneration of Infancy (Canavan)Spongy Degeneration of Infancy (Canavan)
•• Vacuolating LeukoencephalopathyVacuolating Leukoencephalopathy
•• Hexachlorophene ToxicityHexachlorophene Toxicity
H i t i it (“ h i th d ”)H i t i it (“ h i th d ”)•• Heroin toxicity (“chasing the dragon”)Heroin toxicity (“chasing the dragon”)
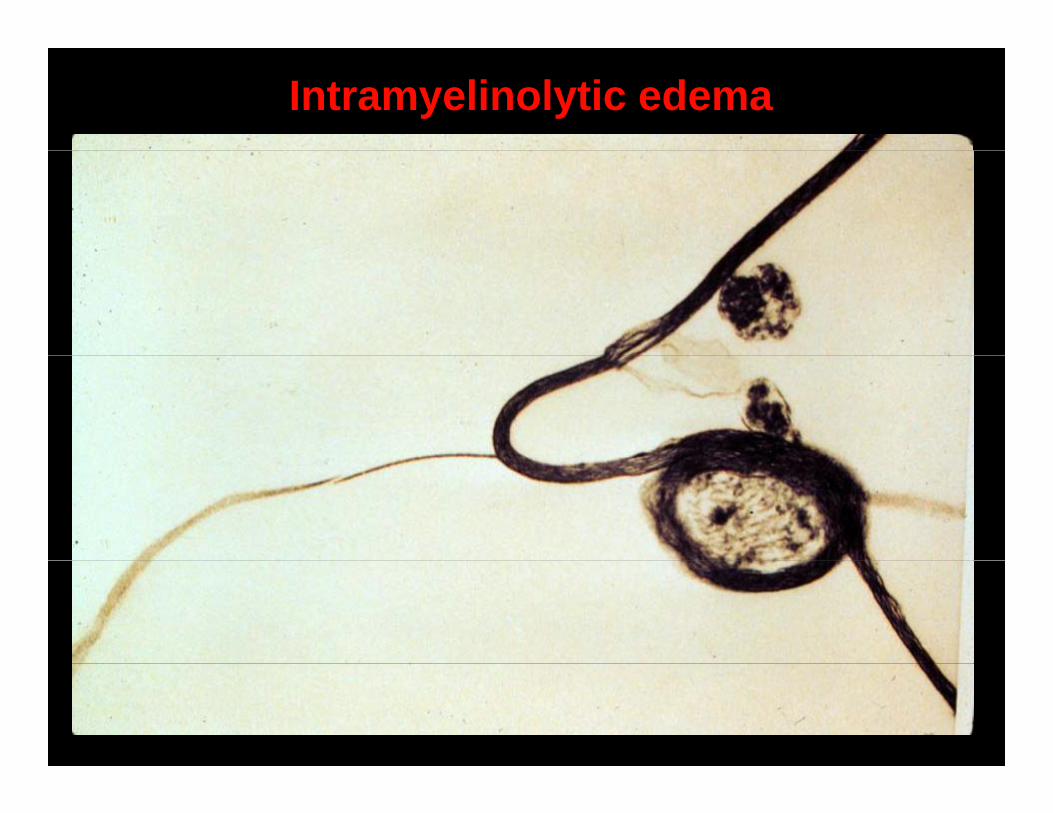
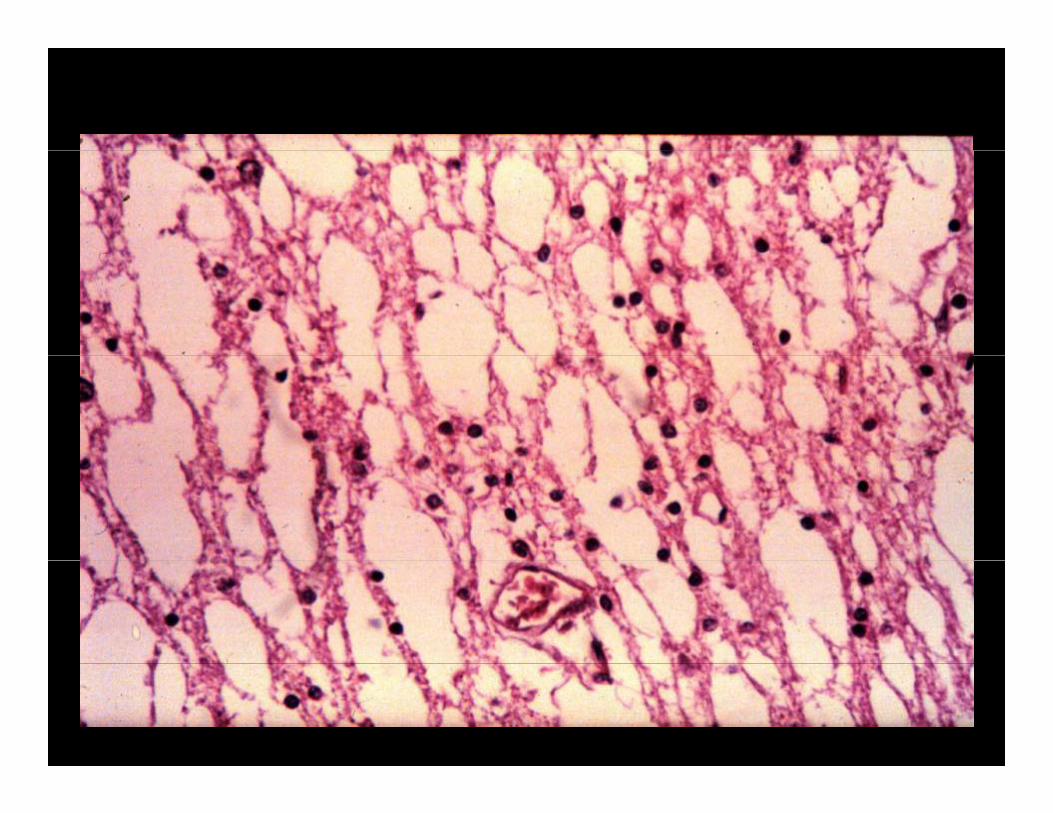
Intramyelinolytic edema
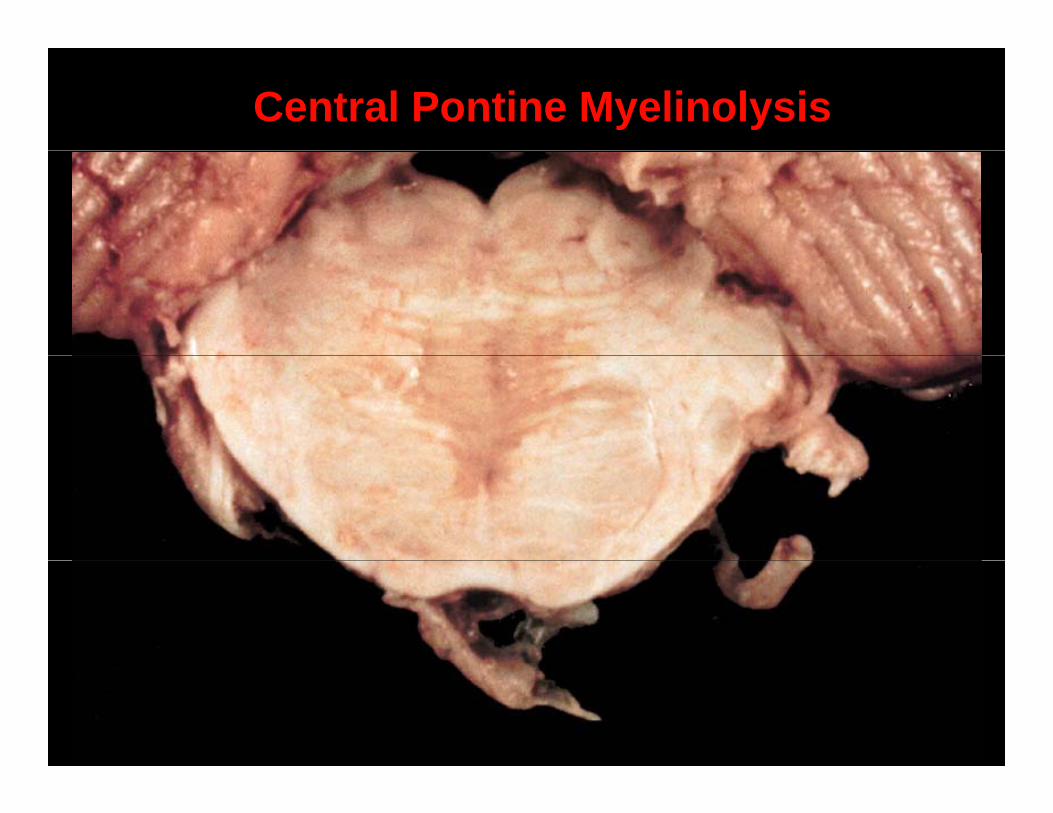
Central Pontine Myelinolysis
CanavanCanavan’’s Diseases DiseaseCanavanCanavan s Diseases Disease
•• Deficiency of the lysosomal enzyme aspartoacylase;Deficiency of the lysosomal enzyme aspartoacylase;•• Deficiency of the lysosomal enzyme aspartoacylase; Deficiency of the lysosomal enzyme aspartoacylase; NN--acetylacetyl--aspartic acid accumulates in brainaspartic acid accumulates in brain
•• Autosomal recessive; most common in Ashkenazi JewsAutosomal recessive; most common in Ashkenazi Jews
•• Presents at 2Presents at 2--6 months of age with psychomotor retardation,6 months of age with psychomotor retardation,Presents at 2Presents at 2 6 months of age with psychomotor retardation, 6 months of age with psychomotor retardation, hypotonia; blindness, megalencephaly, seizures occurhypotonia; blindness, megalencephaly, seizures occur
•• Vacuolar change (Vacuolar change (““spongyspongy””) in CNS due to intramyelinic) in CNS due to intramyelinic•• Vacuolar change (Vacuolar change ( spongyspongy ) in CNS due to intramyelinic ) in CNS due to intramyelinic edema in white matter of cerebrum and cerebellumedema in white matter of cerebrum and cerebellum