hypophosphatemia and rhabdomyolysis - jci
TRANSCRIPT

Hypophosphatemia and Rhabdomyolysis
J. P. KNOCHEL, C. BARCENAS,J. R. COTTON,T. J. FULLER, R. HALLER, andN. W. CARTER, Veterans Administration Hospital, Dallas, Texas 75216 andThe University of Texas Health Science Center at Dallas, SduthwesternMedical School, Dallas, Texas 75235
A B S T RA C T Clinical observations suggest thatovert rhabdomyolysis may occur if severe hypophos-phatemia is superimposed upon a pre-existing sub-clinical myopathy. To examine this possibility, a sub-clinical muscle cell injury was induced in 23 dogs byfeeding them a phosphorus- and calorie-deficient dietuntil they lost 30% of their original weight. To induceacute, severe hypophosphatemia in the animals afterpartial starvation, 17 of the dogs were given large quan-tities of the same phosphorus-deficient diet in conjunc-tion with an oral carbohydrate supplement, which to-gether provided 140 kcal/kg per day.
After phosphorus and caloric deprivation, serumphosphorus and creatine phosphokinase (CPK) activ-ity were normal. Total muscle phosphorus content fellfrom 28.0±1.3 to 26.1+2.5 mmol/dg fat-free dry solids.Sodium, chloride, and water contents rose. Thesechanges resembled those observed in patients with sub-clinical alcoholic myopathy. Whenstudied after 3 daysof hyperalimentation, the animals not receiving phos-phorus showed weakness, tremulousness, and in somecases, seizures. Serum phosphorus fell, the averagelowest value was 0.8 mgJdl (P < 0.001). CPKactivityrose from 66+357 to 695+1,288 IU/liter (P <0.001).Muscle phosphorus content fell further to 21.1+7.7mmol/dg fat-free dry solids (P < 0.001). Muscle Na andCl contents became higher (P < 0.01). Sections of gracilismuscle showed frank rhabdomyolysis.
6 of the 23 phosphorus- and calorie-deprived dogswere also given 140 kal/kg per day but in addition,each received 147 mmol of elemental phosphorus.These dogs consumed their diet avidly and displayedno symptoms. They did not become hypophosphatemic,their CPKremained normal, and derangements of cel-lular Na, Cl, and H20 were rapidly corrected. Thegracilis muscle appeared normal histologically in theseanimals.
Presented at plenary session of the Annual Meeting of theAssociation of American Physicians, San Francisco, Calif.,April 1978.
Received for publication 12 May 1978 and in revised form17 July 1978.
1240
These data suggest that a subclinical myopathy mayset the stage for rhabdomyolysis if acute, severe hy-pophosphatemia is superimposed. Neither acute hy-pophosphatemia nor rhabdomyolysis occur if abundantphosphorus is provided during hyperalimnentation.
INTRODUCTION
Recent observations have shown that most severe al-coholics with either clinical or laboratory evidence ofalcoholic myopathy have abnormally low total phos-phorus content in skeletal muscle (1). Many of thesepatients demonstrate normal or slightly subnormalvalues for serum phosphorus concentration. when theyare admitted to the hospital. However, during the firstfew hospital days, hypophosphatemia appears and maybecome progressively more severe. It generally occursas nutrients are administered and from all evidence,results from phosphorus movement into cells (2). Atleast in some patients, this decline of serum phosphorusis associated with a sharp rise of serum creatine phos-phokinase (CPK)1 activity (1), suggesting that severehypophosphatemia may be responsible for convertinga subclinical myopathy into acute rhabdomyolysis.
In previous reports, we have shown an abnormallylow total phosphorus content of muscle tissue in pa-tients with alcoholic myopathy. They also demonstratedelevated muscle content of sodium, chloride, and water.Directly measured transmembrane electrical potentialdifference of skeletal muscle cells was abnormally low(1). Such abnormalities suggest a defect in ion trans-port. Subsequent studies in dogs (3) showed that ex-perimental phosphorus deficiency led to weakness,anorexia, and an electrochemical disturbance of musclecells closely resembling that observed in patients withalcoholic myopathy. This was reversible upon phos-phorus repletion. Of interest, hypophosphatemia de-veloped gradually and did not become severe in theseexperimental animals. In addition, CPK activity re-
'Abbreviations used in this paper: CPK, creatine phos-phokinase; FFDS, fat-free dry solids.
J. Clin Invest. X The American Society for Clinical Investigation, Inc., 0021-9738/78/1201-1240 $1.00Volume 62 December 1978 1240-1246

mained within normal limits despite chemical derange-ments of the muscle cells. These features were quitesimilar to our observations on patients with alcoholicmyopathy before they developed severe hypophospha-temia (1). Therefore, whereas simple phosphorus de-ficiency may lead to a subclinical cellular injury, thedevelopment of acute rhabdomyolysis may requiresuperimposition of an additional insult, such as hy-pophosphatemia.
The purpose of this study was to determine if hy-pophosphatemia induced by hyperalimentation canproduce acute rhabdomyolysis in the dog if it is super-imposed upon an existing electrochemical injury. Asubclinical myopathy was induced by phosphorus de-privation and partial starvation so that severe hypo-phosphatemia would likely occur upon re-feedingwithout phosphorus. The results show that administra-tion of excessive calories to an animal prepared in thismanner causes severe hypophosphatemia and acuterhabdomyolysis. Such hyperalimentation in the sameanimal preparation causes neither hypophosphatemianor rhabdomyolysis if adequate elemental phosphorusis provided in the diet.
METHODS
The dog model used in these studies was developed to stim-ulate certain features of severe, chronic alcoholics found tohave myopathy. These patients commonly have lost bodyweight and are phosphorus deficient.
23 healthy male mongrel dogs weighing from 22 to 25 kgwere each studied on three occasions: (a) control, (b) afterweight loss and phosphorus deprivation, and (c) after hyper-alimentation with and without supplemental phosphorus.Control studies were conducted after the animals hadreceived a synthetic, phosphorus-deficient but otherwisenutritionally adequate diet for 7 days. Before the control study,1.87 g of Na2HPO4was added to the diet each day. The dietwas obtained from ICN Pharmaceuticals Inc., Life SciencesGroup, Cleveland, Ohio. Each 100 g contained 410 calories,20 g of protein, 60 g of carbodhydrate, and 10 g of fat. UpoITchemical analysis, each 100 g of diet contained 26 mg of ele-mental phosphorus, 3 mmol of magnesium, and 36 meq ofpotassium. In other respects the diet contained all vitamins,minerals, and electrolytes in excess of minimum require-ments. For the control study, sufficient diet was fed to pro-vide 30 calories/kg per day. On day 8, when the dogs wereunder sedation with 15 mg/kg body wt pentobarbital, serumCPK, plasma and muscle sodium, potassium, chloride, andtotal phosphorus were measured. Venous blood was alsosampled for pH, carbon dioxide tension, and oxygen tension.For determination of composition, samples of the gracilismuscle were collected with a needle biopsv instrument andanalyzed as previously described (3, 4).
After the control study, the dogs were placed on the samesynthetic diet without added phosphorus but in a reducedquantity to provide 15 calories/kg per day. Aluminum car-bonate gel (Basaljel, Wyeth Laboratories, Philadelphia, Pa.),60 ml, was mixed into the diet each day to bind phosphorusin the gut. The dogs were weighed daily before feeding. Thesecond study, identical to the first, was conducted when theanimals had lost 30% of their initial body weight.
After the effects of weight loss and phosphorus deprivation
were determined, 17 of the animals were begun on 500 gof the same diet without added phosphorus but with suf-ficient added carbohydrate to provide 140 calories/kg per day.The extra carbohydrate was provided as a solution that con-tained 10 g glucose and 40 g of maltose/100 cm3. One-halfof the diet was given in the morning and one-half in the after-noon. Any diet not consumed spontaneously was fed by ga-vage. The remaining six dogs were fed the same diet wvithoutaluminum carbonate. This diet contained phosphorus and pro-vided 140 calories/kg per day. Because both hypophospha-temia and hypokalemia may occur under conditions of suchhyperalimentation, sodium and potassium phosphate were ad-ministered in the following proportions: 3 mmol Na2HPO4,8 mmol NaH2PO4, 3 mmol K2HPO4, and 3.2 mmol KH2PO4. 20 gof this mixture was given to each dog daily. This quantity con-tained 147 mmol of phosphorus and 79 meq of potassium.This quantity contained 147 mmol of phosphorus and 79 meqof potassium. Fasting blood samples were collected on eachmorning during hyperalimentation. Skeletal muscle was ob-tained 72 h after initiation of hyperalimentation unless theanimal appeared seriously ill before that time. For the samereason, some dogs wvere biopsied on the 2nd or 3rd day ofhyperalimentation. For examination of muscle histology,stretched sections of gracilis muscle were removed, fixed inbuffered formalin, and stained with hematoxylin and cosin.
Serum sodium, potassium, and chloride determinationswere performed by conventional laboratory procedures.Serum phosphorus was measured by the colorimetric methodused for the Technicon AutoAnalyzer (Technicon Instru-ments Corp., Tarrytown, N. Y.). Muscle sodium, chloride, andpotassium contents were determined on dilute acetic acid ex-tracts of dried, fat-extracted samples that weighed 10-20 mgas previously described (4). Serum CPK activity was meas-ured spectrophotometrically by a modification of the Rosalkiprocedure (5). After weight loss and hyperalimentation elec-trolytes and total phosphorus in muscle were compared in-dividually to their respective values obtained during the con-trol study by the paired t test. All data are expressed asmean+1 SD.
RESULTS
As noted previously, dogs fed a phosphorus-deficientdiet generally became anorectic and had to be gavagefed w^rhen the diet was not voluntarily consumed. Ex-cept for equivocal weakness and diminished spontane-ous physical activity, the animals displayed no unl-usual symptoms during the period of caloric depriva-tion. From 28 to 40 days vere required for the dogs tolose 30% of their initial weight. During the period ofhyperalimentation those not given a phosphorus sup-plement became extremely ill. They demonstrated trem-ulousness, difficulty in standing, and severe wveak-ness. Somedisplayed convulsive movements. Four diedby the 3rd dav of hyperalimentation. Data on theseanimals were excluded.
Individual values for serum phosphorus concentra-tioin are showin in Fig. 1. The average value in thecontrol study vas 4.4+0.8 mg/dl. After the dogs re-ceived the phosphorus-deficient diet and lost 30% oftheir original body weight, the serum phosphorus was3.9+1.2 mg/dl. This was not significantly different fromthe control value. After 3 days of hyperalimentation,
Hypopphosphvatemii ia (Incd Rhabdomyolysis 1241
mg/dl6
5
SERUM4-
Pi 3-
2-
04
mmol/ liter2.00
11*1.5 --0O-
*1.0
0
80
0
0.5
*0 &
CONTROL PD-S HYPERALIME-NTATIONWITHOUTP
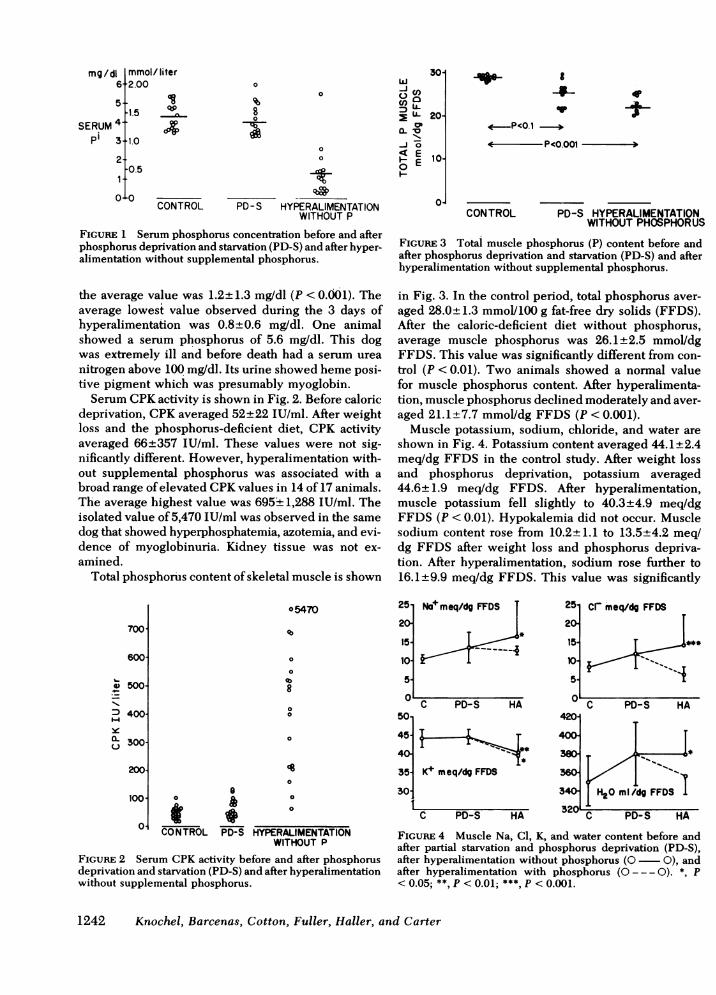
FIGURE 1 Serum phosphorus concentration before and afterphosphorus deprivation and starvation (PD-S) and after hyper-alimentation without supplemental phosphorus.
the average value was 1.2±+1.3 mg/dl (P < 0.001). Theaverage lowest value observed during the 3 days ofhyperalimentation was 0.8±0.6 mg/dl. One animalshowed a serum phosphorus of 5.6 mgldl. This dogwas extremely ill and before death had a serum ureanitrogen above 100 mg/dl. Its urine showed heme posi-tive pigment which was presumably myoglobin.
Serum CPKactivity is shown in Fig. 2. Before caloricdeprivation, CPKaveraged 52+22 IU/ml. After weightloss and the phosphorus-deficient diet, CPK activityaveraged 66+357 IU/ml. These values were not sig-nificantly different. However, hyperalimentation with-out supplemental phosphorus was associated with abroad range of elevated CPKvalues in 14 of 17 animals.The average highest value was 695+ 1,288 IU/ml. Theisolated value of 5,470 IU/ml was observed in the samedog that showed hyperphosphatemia, azotemia, and evi-dence of myoglobinuria. Kidney tissue was not ex-amined.
Total phosphorus content of skeletal muscle is shown
30-w-Ic'0 a
i- 20-
of
0 g 10-
0^
I-
00
84-
CONTROL
4*
PD-S HYPERALIMENTATIONWITHOUTPHOSPHORUS
FIGURE 3 Total muscle phosphorus (P) content before andafter phosphorus deprivation and starvation (PD-S) and afterhyperalimentation without supplemental phosphorus.
in Fig. 3. In the control period, total phosphorus aver-aged 28.0±1.3 mmol/100 g fat-free dry solids (FFDS).After the caloric-deficient diet without phosphorus,average muscle phosphorus was 26.1±2.5 mmol/dgFFDS. This value was significantly different from con-trol (P < 0.01). Two animals showed a normal valuefor muscle phosphorus content. After hyperalimenta-tion, muscle phosphorus declined moderately and aver-aged 21.1± 7.7 mmol/dg FFDS (P < 0.001).
Muscle potassium, sodium, chloride, and water areshown in Fig. 4. Potassium content averaged 44.1±2.4meq/dg FFDS in the control study. After weight lossand phosphorus deprivation, potassium averaged44.6±1.9 meq/dg FFDS. After hyperalimentation,muscle potassium fell slightly to 40.3±4.9 meq/dgFFDS (P < 0.01). Hypokalemia did not occur. Musclesodium content rose from 10.2±1.1 to 13.5±4.2 meq/dg FFDS after weight loss and phosphorus depriva-tion. After hyperalimentation, sodium rose further to16.1±9.9 meq/dg FFDS. This value was significantly
700
600
e 500I.
:D 400y
X 300
200
o5470 2512011511015-
0
0
8
00
0
0
100. o i 00101 * ___
° CONTROL PD-S HYPERALIMENTATIONWITHOUTP
FIGURE 2 Serum CPKactivity before and after phosphorusdeprivation and starvation (PD-S) and after hyperalimentationwithout supplemental phosphorus.
50
45
40
35.30
N+meq/dg FFDS T
T*
251201
15S
10i
S
420-
400-
360-
C PD-S HA
K :meq/dg FFDSK+ meq/dg FFDS
C PD-S HA
cr meq/dg FFDS
C PD-S HA
I H20 m /dg FFDS
C PD-S HA
FIGURE 4 Muscle Na, Cl, K, and water content before andafter partial starvation and phosphorus deprivation (PD-S),after hyperalimentation without phosphorus (O 0), andafter hyperalimentation with phosphorus (O --- 0). *, P< 0.05; **, P <0.01; ***, P <0.001.
1242 Knochel, Barcenas, Cotton, Fuller, Haller, and Carter
If P<0.001 30
L-
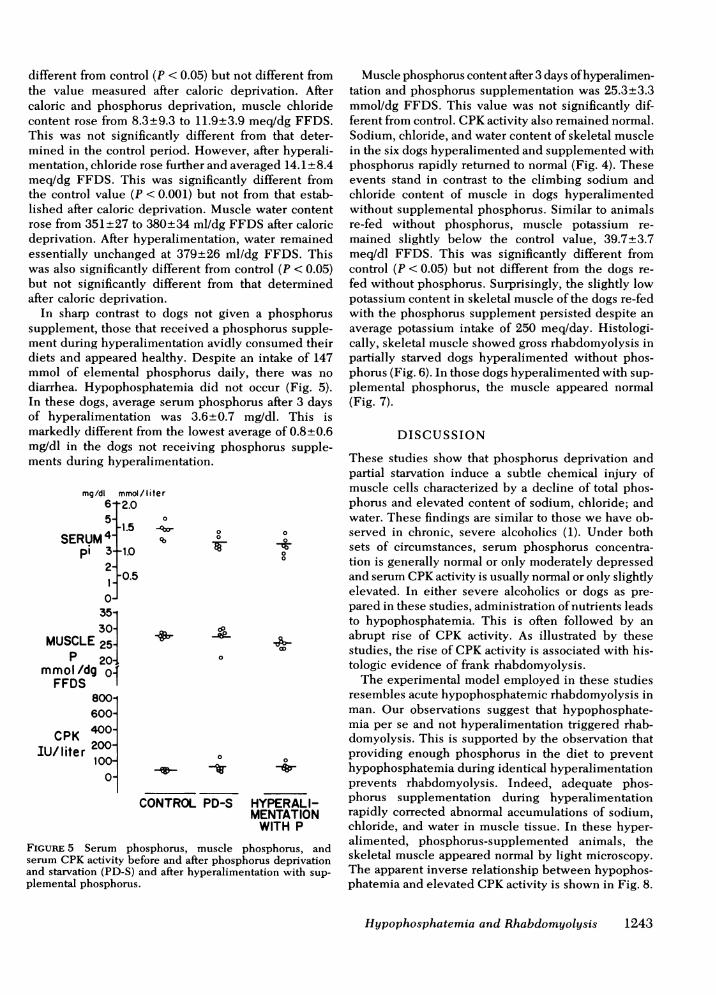
different from control (P < 0.05) but not different fromthe value measured after caloric deprivation. Aftercaloric and phosphorus deprivation, muscle chloridecontent rose from 8.3±9.3 to 11.9±3.9 meq/dg FFDS.This was not significantly different from that deter-mined in the control period. However, after hyperali-mentation, chloride rose further and averaged 14.1±8.4meq/dg FFDS. This was significantly different fromthe control value (P < 0.001) but not from that estab-lished after caloric deprivation. Muscle water contentrose from 351±27 to 380±34 ml/dg FFDS after caloricdeprivation. After hyperalimentation, water remainedessentially unchanged at 379±26 ml/dg FFDS. Thiswas also significantly different from control (P < 0.05)but not significantly different from that determinedafter caloric deprivation.
In sharp contrast to dogs not given a phosphorussupplement, those that received a phosphorus supple-ment during hyperalimentation avidly consumed theirdiets and appeared healthy. Despite an intake of 147mmol of elemental phosphorus daily, there was nodiarrhea. Hypophosphatemia did not occur (Fig. 5).In these dogs, average serum phosphorus after 3 daysof hyperalimentation was 3.6±0.7 mg/dl. This ismarkedly different from the lowest average of 0.8±0.6mg/dl in the dogs not receiving phosphorus supple-ments during hyperalimentation.
mg/di mmol/liter6-2.05-15 -
SERUM4 %pi 3- 1.0
2 0.5
35-301
MUSCLE251P 20-,4
mmol /dg O.fFFDS
9 0
800-600-
CPK 4001
IU/liter 200-100-
O-
00
00
0
-v- -W
CONTROLPD-S HYPERALI-MENTATION
WITH P
FIGURE 5 Serum phosphorus, muscle phosphorus, andserum CPKactivity before and after phosphorus deprivationand starvation (PD-S) and after hyperalimentation with sup-plemental phosphorus.
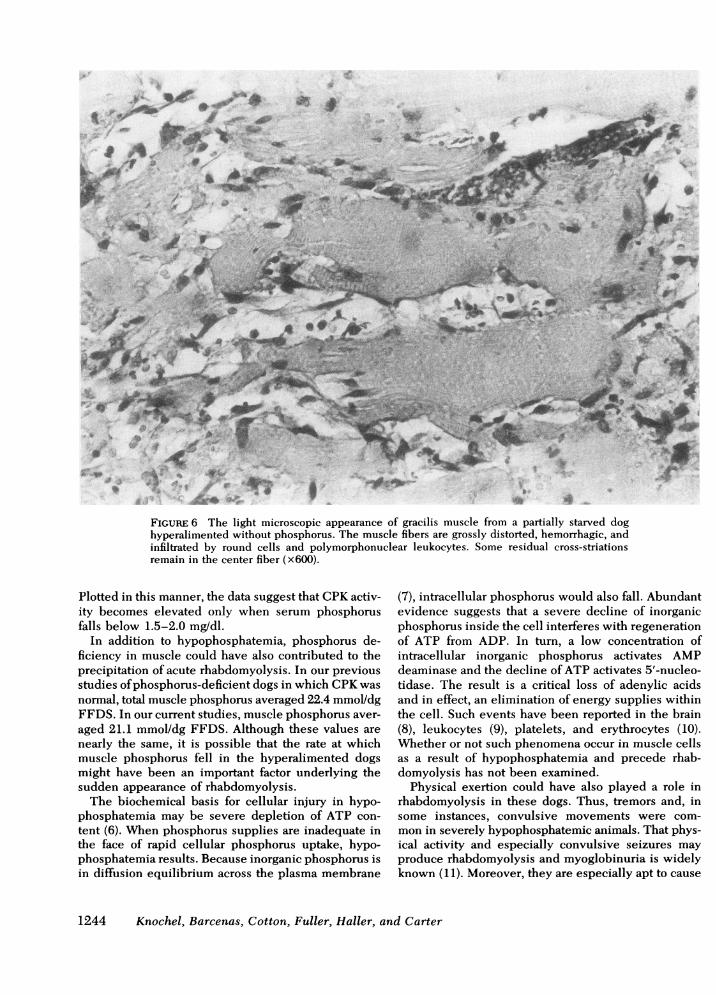
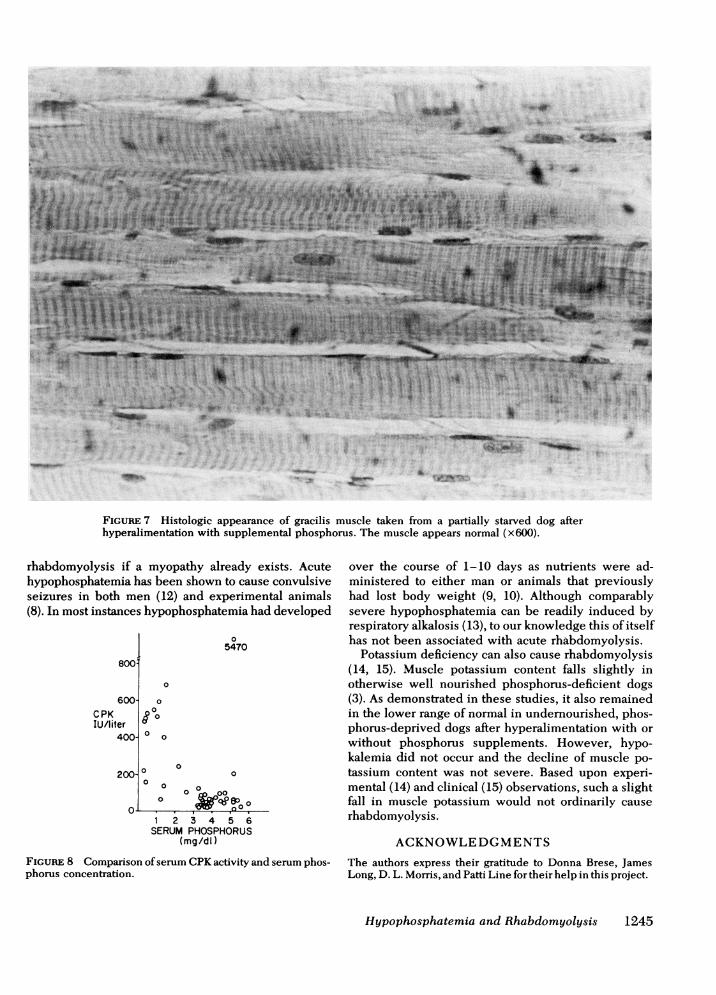
Muscle phosphorus content after 3 days of hyperalimen-tation and phosphorus supplementation was 25.3±3.3mmol/dg FFDS. This value was not significantly dif-ferent from control. CPKactivity also remained normal.Sodium, chloride, and water content of skeletal musclein the six dogs hyperalimented and supplemented withphosphorus rapidly returned to normal (Fig. 4). Theseevents stand in contrast to the climbing sodium andchloride content of muscle in dogs hyperalimentedwithout supplemental phosphorus. Similar to animalsre-fed without phosphorus, muscle potassium re-mained slightly below the control value, 39.7±3.7meq/dl FFDS. This was significantly different fromcontrol (P < 0.05) but not different from the dogs re-fed without phosphorus. Surprisingly, the slightly lowpotassium content in skeletal muscle of the dogs re-fedwith the phosphorus supplement persisted despite anaverage potassium intake of 250 meq/day. Histologi-cally, skeletal muscle showed gross rhabdomyolysis inpartially starved dogs hyperalimented without phos-phorus (Fig. 6). In those dogs hyperalimented with sup-plemental phosphorus, the muscle appeared normal(Fig. 7).
DISCUSSION
These studies show that phosphorus deprivation andpartial starvation induce a subtle chemical injury ofmuscle cells characterized by a decline of total phos-phorus and elevated content of sodium, chloride; andwater. These findings are similar to those we have ob-served in chronic, severe alcoholics (1). Under bothsets of circumstances, serum phosphorus concentra-tion is generally normal or only moderately depressedand serum CPKactivity is usually normal or only slightlyelevated. In either severe alcoholics or dogs as pre-pared in these studies, administration of nutrients leadsto hypophosphatemia. This is often followed by anabrupt rise of CPK activity. As illustrated by thesestudies, the rise of CPKactivity is associated with his-tologic evidence of frank rhabdomyolysis.
The experimental model employed in these studiesresembles acute hypophosphatemic rhabdomyolysis inman. Our observations suggest that hypophosphate-mia per se and not hyperalimentation triggered rhab-domyolysis. This is supported by the observation thatproviding enough phosphorus in the diet to preventhypophosphatemia during identical hyperalimentationprevents rhabdomyolysis. Indeed, adequate phos-phorus supplementation during hyperalimentationrapidly corrected abnormal accumulations of sodium,chloride, and water in muscle tissue. In these hyper-alimented, phosphorus-supplemented animals, theskeletal muscle appeared normal by light microscopy.The apparent inverse relationship between hypophos-phatemia and elevated CPKactivity is shown in Fig. 8.
Hypophosphatemia and Rhabdomyolysis 1243
90o
/4.. S.. -
w: _ 8
t -t ,.. w LLis ,< .§ s
.. Si
.. ,^ . 4J _ e _,-.... r rS __ .:E XF 1i P rS ! s X
#A..r )_§*: :. jZ
4||X ^' t' _S w}'t5'v'< a ^
or ;&
& / _ss _,_w}
_.-" i r j.,
.4 .. ..j s J- t
-I4
FIGURE 6 The light microscopic appearance of gracilis muscle from a partially starved doghyperalimented without phosphorus. The muscle fibers are grossly distorted, hemorrhagic, andinfiltrated by round cells and polymorphonuclear leukocytes. Some residual cross-striationsremain in the center fiber (x600).
Plotted in this manner, the data suggest that CPKactiv-ity becomes elevated only when serum phosphorusfalls below 1.5-2.0 mg/dl.
In addition to hypophosphatemia, phosphorus de-ficiency in muscle could have also contributed to theprecipitation of acute rhabdomyolysis. In our previousstudies of phosphorus-deficient dogs in which CPKwasnormal, total muscle phosphorus averaged 22.4 mmol/dgFFDS. In our current studies, muscle phosphorus aver-aged 21.1 mmol/dg FFDS. Although these values arenearly the same, it is possible that the rate at whichmuscle phosphorus fell in the hyperalimented dogsmight have been an important factor underlying thesudden appearance of rhabdomyolysis.
The biochemical basis for cellular injury in hypo-phosphatemia may be severe depletion of ATP con-tent (6). When phosphorus supplies are inadequate inthe face of rapid cellular phosphorus uptake, hypo-phosphatemia results. Because inorganic phosphorus isin diffusion equilibrium across the plasma membrane
(7), intracellular phosphorus would also fall. Abundantevidence suggests that a severe decline of inorganicphosphorus inside the cell interferes with regenerationof ATP from ADP. In turn, a low concentration ofintracellular inorganic phosphorus activates AMPdeaminase and the decline of ATP activates 5'-nucleo-tidase. The result is a critical loss of adenylic acidsand in effect, an elimination of energy supplies withinthe cell. Such events have been reported in the brain(8), leukocytes (9), platelets, and erythrocytes (10).Whether or not such phenomena occur in muscle cellsas a result of hypophosphatemia and precede rhab-domyolysis has not been examined.
Physical exertion could have also played a role inrhabdomyolysis in these dogs. Thus, tremors and, insome instances, convulsive movements were com-mon in severely hypophosphatemic animals. That phys-ical activity and especially convulsive seizures mayproduce rhabdomyolysis and myoglobinuria is widelyknown (11). Moreover, they are especially apt to cause
1244 Knochel, Barcenas, Cotton, Fuller, Haller, and Carter
3e'r 'a .,.
*~~~WI9*jMFMv
.:.l A_ s
-si
-
41 ; *
99..... r
FIGuRE 7 Histologic appearance of gracilis muscle taken from a partially starved dog afterhyperalimentation with supplemental phosphorus. The muscle appears normal (x600).
rhabdomyolysis if a myopathy already exists. Acutehypophosphatemia has been shown to cause convulsiveseizures in both men (12) and experimental animals(8). In most instances hypophosphatemia had developed
8001
600-CPKIU/Iiter
400-
200- c
05470
0
0
? 0
0
00
1 2 3 4 5 6SERUMPHOSPHORUS
(mg/dl)
FIGuRE 8 Comparison of serum CPKactivity and serum phos-phorus concentration.
over the course of 1-10 days as nutrients were ad-ministered to either man or animals that previouslyhad lost body weight (9, 10). Although comparablysevere hypophosphatemia can be readily induced byrespiratory alkalosis (13), to our knowledge this of itselfhas not been associated with acute rhabdomyolysis.
Potassium deficiency can also cause rhabdomyolysis(14, 15). Muscle potassium content falls slightly inotherwise well nourished phosphorus-deficient dogs(3). As demonstrated in these studies, it also remainedin the lower range of normal in undernourished, phos-phorus-deprived dogs after hyperalimentation with orwithout phosphorus supplements. However, hypo-kalemia did not occur and the decline of muscle po-tassium content was not severe. Based upon experi-mental (14) and clinical (15) observations, such a slightfall in muscle potassium would not ordinarily causerhabdomyolysis.
ACKNOWLEDGMENTS
The authors express their gratitude to Donna Brese, JamesLong, D. L. Morris, and Patti Line for their help in this project.
Hypophosphatemia and Rhabdomyolysis 1245
10
1=61 .-
0 00 000 Lrctp ep o
IUM-W 00
This work was supported by research funds from the UnitedStates Veterans Administration and the National Institute onAlcohol Abuse and Alcoholism, grant 1 ROI AA 02970-01.
REFERENCES
1. Knochel, J. P., G. L. Bilbrey, T. J. Fuller, and N. W. Carter.1975. The muscle cell in chronic alcoholism. The possiblerole of phosphate depletion in alcoholic myopathy. Ann.N. Y'. Acad. Sci. 252: 274-286.
2. Knochel, J. P. 1977. The pathophysiology and clinicalcharacteristics of severe hypophosphatemia. Arch. Intern.Med. 137: 203-220.
3. Fuller, T. J., N. W. Carter, C. Barcenas, and J. P. Knochel.1976. Reversible changes of the muscle cell in experi-mental phosphorus deficiency. J. Clin. Invest. 57: 1019-1024.
4. Bilbrey, G. L., N. W. Carter, M. G., White, and J. P.Knochel. 1973. Potassium deficiency in chronic renal fail-ure. Kidney Int. 4: 423-430.
5. Rosalki, S. B. 1967. An improved procedure for serumcreatine phosphokinase determination.J. Lab. Clin. Med.69: 696-705.
6. Farber, E. 1973. ATP and cell integrity. 1973. Fed. Proc.32: 1534-1539.
7. Woods, H. F., L. V. Eggleston, and H. A. Krebs. Thecause of hepatic accumulation of fructose-1-phosphate onfructose loading. Biochem. J. 119: 501-510.
8. Yawata, Y., P. Craddock, R. Hebbel, and H. S. Jacob. 1973.
Hyperalimentation hypophosphatemia: Hematologic neu-rologic dysfunction due to ATP depletion. Clitn. Res. 31:729.
9. Craddock, P. R., Y. Yawata, L. Van Santen, S. Gilberstadt,S. Silvis, and H. S. Jacob. 1974. Acquired phagocyte dys-function: A complication of the hypophosphatemia ofparenteral hyperalimentation. N. Engl. J. Med. 290: 1403.
10. Yawata, Y., R. P. Hebbel, S. Silvis, R. Howe, and H. S.Jacob. 1974. Blood cell abnormalities complicating thehypophosphatemia of hyperalimentation: Erythrocytesand platelet ATP deficiency associated with hemolyticanemia and bleeding in hyperalimented dogs. J. Lab.Clin. Med. 84: 643-653.
11. Rowland, L. P., and A. S. Penn. 1972. Myoglobinuria.Symposium on Clinical Neurology. Med. Cliiu. N. Am.56: 1233-1256.
12. Silvis, S. E., and P. D. Paragas. 1972. Paresthesias, weak-ness, seizures and hypophosphatemia in patients receiv-ing hyperalimentation. Gastroenterology. 62: 513-520.
13. Mostellar, M. E., and E. P. Tuttle, Jr. 1964. The effectsof alkalosis on plasma concentration and urinary excre-tion of inorganic phosphate in man. J. Clin. Itivest. 43:138-149.
14. Knochel, J. P., and E. M. Schlein. 1972. On the mechanismof rhabdomyolysis in potassium depletion.J. CliGu. Inciest.51: 1750-1758.
15. Knochel, J. P. 1978. Rhabdomyolysis and effects of po-tassium deficiency on muscle structure and function. Car-diovasc. Med. 3: 247-261.
1246 Knochel, Barcenas, Cotton, Fuller, Haller, and Carter