i the current status of tooth crèmes for enamel...
TRANSCRIPT
DEN
TAL
INC
. Jul
y/A
ugus
t 200
9D
ENTA
L IN
C.J
uly/
Aug
ust 2
009
The current status of tooth crèmes for enamel remineralization
MICA (P) No. 116/05/2009 I KDN: PPS 1681/03/2009 (020069) I JUL/AUG 2009 • Vol 2, No. 6
38
n recent years it has become easy for the dental practitioner to become confused regarding the bona fi des of the many agents which have
been promoted as agents for remineralizing enamel. This article looks at the process of remineralization, and from that examines some current products and therapies, to try to make sense of the fruit salad of “apples, oranges and pears.” The characteristics of an ideal remineralizing agent are summarized in Table 1 [1], and this gives a useful measure of how the available materials and technologies perform.
Enamel minerals: back to natureThe mineral in human enamel is not pure hydroxyapatite, but rather a mixture of compounds including a number of carbonated apatites, which together occupy up to 98 weight per cent and up to 96 volume per cent, when constitutional water is included. Of these various apatites, fl uorapatite is less acid soluble than hydroxyapatite, which in turn is less soluble than carbonated apatite. While it is somewhat simplistic, looking at the major apatites makes it clear that the ratio of components required for remineralization is 10 calcium ions to 6 phosphate ions to either 2 fl uoride or 1 hydroxyl ions or 1carbonate ion, a ratio of 5:3:1. It is also clear that calcium availability remains the singular limiting
I factor in enamel remineralization, and herein lies the problem, since the majority of calcium compounds are very insoluble. If we want remineralization then we will need calcium and phosphate ions (ideally assisted by fl uoride) to rebuild a new surface on existing crystal remnants – and this must occur in subsurface lesions, and not simply precipitate onto the surface.
Making it realIf one is going to assess potential remineralization agents, this must be done in realistic conditions, such as by using in situ models where enamel slabs are carried in patients mouth and removed in order to measure mineral changes. This aproach is necessary to take into account the effects of saliva, particularly its glycoproteins (which adsorb onto tooth structure to form pellicle) and its phosphoproteins (which regulate calcium saturation). The early pellicle glycoproteins, acidic proline-rich proteins and statherin, promote remineralization of the enamel by attracting and binding calcium ions, attaching strongly to hydroxyapatite, and inhibiting crystal growth and precipitation of calcium phosphate salts. [2] In situ studies which examine enamel slabs that have been in the mouth of patients allow full expression of the impacts of saliva. In contrast, some “laboratory
DEN
TAL IN
C. July/A
ugust 2009D
ENTA
L INC
.July/August 2009
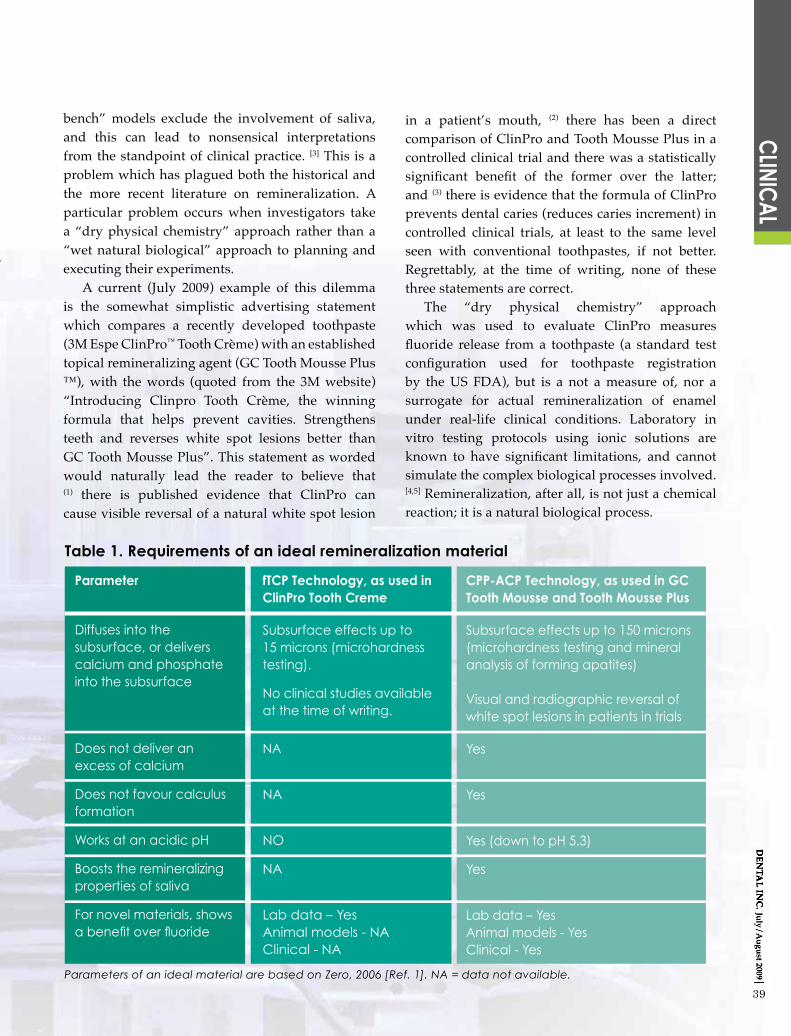
Table 1. Requirements of an ideal remineralization material
Parameter
Diffuses into the subsurface, or delivers calcium and phosphate into the subsurface
Does not deliver an excess of calcium
Does not favour calculus formation
Works at an acidic pH
Boosts the remineralizing properties of saliva
For novel materials, shows a benefi t over fl uoride
fTCP Technology, as used inClinPro Tooth Creme
Subsurface effects up to 15 microns (microhardness testing).
No clinical studies available at the time of writing.
NA
NA
NO
NA
Lab data – YesAnimal models - NAClinical - NA
CPP-ACP Technology, as used in GC Tooth Mousse and Tooth Mousse Plus
Subsurface effects up to 150 microns (microhardness testing and mineral analysis of forming apatites)
Visual and radiographic reversal of white spot lesions in patients in trials
Yes
Yes
Yes (down to pH 5.3)
Yes
Lab data – YesAnimal models - YesClinical - Yes
Parameters of an ideal material are based on Zero, 2006 [Ref. 1]. NA = data not available.
CLINIC
AL
39
bench” models exclude the involvement of saliva, and this can lead to nonsensical interpretations from the standpoint of clinical practice. [3] This is a problem which has plagued both the historical and the more recent literature on remineralization. A particular problem occurs when investigators take a “dry physical chemistry” approach rather than a “wet natural biological” approach to planning and executing their experiments. A current (July 2009) example of this dilemma is the somewhat simplistic advertising statement which compares a recently developed toothpaste (3M Espe ClinPro™ Tooth Crème) with an established topical remineralizing agent (GC Tooth Mousse Plus ™), with the words (quoted from the 3M website) “Introducing Clinpro Tooth Crème, the winning formula that helps prevent cavities. Strengthens teeth and reverses white spot lesions better than GC Tooth Mousse Plus”. This statement as worded would naturally lead the reader to believe that (1) there is published evidence that ClinPro can cause visible reversal of a natural white spot lesion
in a patient’s mouth, (2) there has been a direct comparison of ClinPro and Tooth Mousse Plus in a controlled clinical trial and there was a statistically signifi cant benefi t of the former over the latter; and (3) there is evidence that the formula of ClinPro prevents dental caries (reduces caries increment) in controlled clinical trials, at least to the same level seen with conventional toothpastes, if not better. Regrettably, at the time of writing, none of these three statements are correct. The “dry physical chemistry” approach which was used to evaluate ClinPro measures fl uoride release from a toothpaste (a standard test confi guration used for toothpaste registration by the US FDA), but is a not a measure of, nor a surrogate for actual remineralization of enamel under real-life clinical conditions. Laboratory in vitro testing protocols using ionic solutions are known to have signifi cant limitations, and cannot simulate the complex biological processes involved. [4,5] Remineralization, after all, is not just a chemical reaction; it is a natural biological process.

DEN
TAL
INC
. Jul
y/A
ugus
t 200
9D
ENTA
L IN
C.J
uly/
Aug
ust 2
009
USER
REPO
RTUS
ERRE
PORT
TEC
HNO
LOG
YC
LINIC
AL
40
The argument could also be made that a comparison of the two is an apples versus organs situation, since ClinPro is a fl uoride toothpaste and therefore should release some fl uoride; whilst Tooth Mousse Plus is a pH-response long acting remineralizing crème which should not release much of its bound fl uoride or calcium or phosphate until triggered by acidic pH conditions to do so. Details of product composition and other points of information regarding these products are presented in Table 2. With ClinPro, it is unclear how much of the calcium contained in the product is bio-available, and how much would be expectorated along with toothpaste at the completion of toothbrushing. Assuming a best case scenario where similar amounts of each product are used, ClinPro could only deliver a small amount of unbound, non-stabilized calcium in the 2 minutes of brushing before being expectorated from the mouth, whilst Tooth Mousse Plus delivers large amounts of stabilized calcium over an extended time period. One would expect therefore rather different clinical effects because of the different levels of calcium release and from the stability or otherwise of this released calcium, but not from the fl uoride levels which would likely be similar. So, is there any clinical evidence of visible reversal of a natural white spot lesion in a patient’s mouth? There is published work showing this with GC Tooth Mousse, with the fi rst of these perhaps being an early clinical case of a patient treated by this author in 2004 over a period of 12 weeks [6]. Of much greater importance than this anecdote is the recent controlled clinical trial which documented visible reversal of white spot lesions in orthodontic patients over 12 weeks. Tooth Mousse was shown to be achieve this, and to be superior to a conventional 1000 ppm fl uoride toothpaste. [7,8] Tooth Mousse and Tooth Mousse Plus differ in that the latter has 900 ppm fl uoride within its composition (gained from the addition of 0.2% sodium fl uoride). At the present time there has been limited research on the TCP technology used in ClinPro [9-10] and thus it would be premature to make assertions of superiority, one way or the other, until proper clinical trials are conducted.
Nature thought of it fi rstThe problem of stabilizing calcium ions so that bio-available calcium can be delivered when needed is a major biological challenge which impacts on all dental and other hard tissues in the body. Within milk, the casein phosphopeptides (CPP) stabilize calcium and phosphate ions through the formation of complexes. The calcium phosphate in these complexes is biologically available for intestinal absorption, and the same concept has now been applied to create materials with bio-available calcium and phosphate in the appropriate form and molecular ratio for remineralization of subsurface lesions in enamel. Clusters of phosphorylated seryl residues are responsible for the interaction which occurs in bovine milk between the caseins and calcium phosphate. [12]
Understanding this natural process of calcium stabilization, transport, and delivery and applying it to dentistry resulted in the development of CPP-ACP technology by Professor Eric Reynolds and co-workers at the University of Melbourne, and its inclusion into chewing gums (such as Recaldent gum™ and Trident White™) as well as into the Tooth Mousse crèmes. There is extensive clinical as well as laboratory evidence for the effects of CPP-ACP as a remineralizing agent, as well as a truly anti-cariogenic agent, with the latter being demonstrated in both animal and in situ human caries models [2,3,6-8,
12-22]. The material is pH responsive, with increasing pH increasing the level of bound ACP and stabilizing free calcium and phosphate, so that spontaneous precipitation of calcium phosphate does not occur. This is also inherently an anti-calculus action, as well as evidence that CPP-ACP may infl uence the properties and behaviour of dental plaque through (1)
binding to adhesin molecules on mutans streptococci and thus impairing their incorporation into dental plaque, (2) elevating plaque calcium ion levels to inhibit plaque fermentation; and (3) providing protein and phosphate buffering of plaque fl uid pH, to suppresses overgrowth of aciduric species under conditions where fermentable carbohydrate is in excess.
DEN
TAL IN
C. July/A
ugust 2009
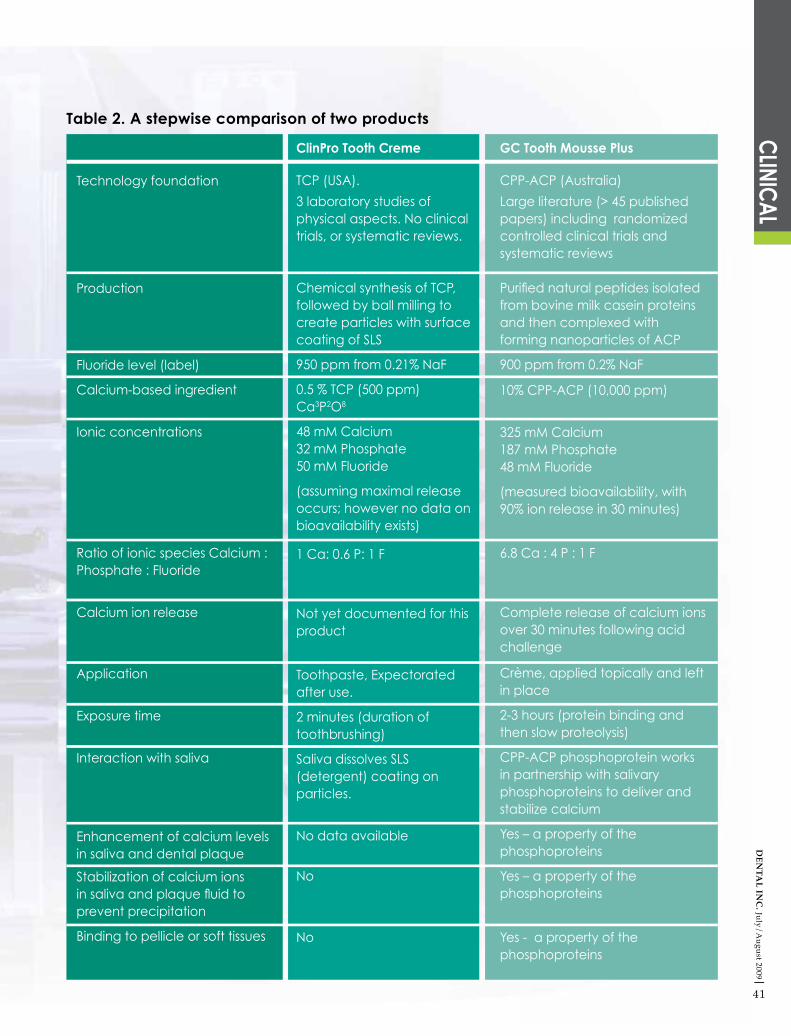
Table 2. A stepwise comparison of two products
Technology foundation
Production
Fluoride level (label)
Calcium-based ingredient
Ionic concentrations
Ratio of ionic species Calcium : Phosphate : Fluoride
Calcium ion release
Application
Exposure time
Interaction with saliva
Enhancement of calcium levels in saliva and dental plaque
Stabilization of calcium ions in saliva and plaque fl uid to prevent precipitation
Binding to pellicle or soft tissues
ClinPro Tooth Creme
TCP (USA).
3 laboratory studies of physical aspects. No clinical trials, or systematic reviews.
Chemical synthesis of TCP, followed by ball milling to create particles with surface coating of SLS
950 ppm from 0.21% NaF
0.5 % TCP (500 ppm)Ca3P2O8
48 mM Calcium32 mM Phosphate50 mM Fluoride
(assuming maximal release occurs; however no data on bioavailability exists)
1 Ca: 0.6 P: 1 F
Not yet documented for this product
Toothpaste, Expectorated after use.
2 minutes (duration of toothbrushing)
Saliva dissolves SLS (detergent) coating on particles.
No data available
No
No
GC Tooth Mousse Plus
CPP-ACP (Australia)
Large literature (> 45 published papers) including randomized controlled clinical trials and systematic reviews
Purifi ed natural peptides isolated from bovine milk casein proteins and then complexed with forming nanoparticles of ACP
900 ppm from 0.2% NaF
10% CPP-ACP (10,000 ppm)
325 mM Calcium187 mM Phosphate48 mM Fluoride
(measured bioavailability, with 90% ion release in 30 minutes)
6.8 Ca : 4 P : 1 F
Complete release of calcium ions over 30 minutes following acid challenge
Crème, applied topically and left in place
2-3 hours (protein binding and then slow proteolysis)
CPP-ACP phosphoprotein works in partnership with salivary phosphoproteins to deliver and stabilize calcium
Yes – a property of the phosphoproteins
Yes – a property of the phosphoproteins
Yes - a property of the phosphoproteins
CLINIC
AL
41

DEN
TAL
INC
. Jul
y/A
ugus
t 200
9D
ENTA
L IN
C.J
uly/
Aug
ust 2
009
Zero DT. Dentifrices, mouthwashes, and remineralization/caries arrestment strategies. BMC Oral Health. 2006;6 (Suppl 1):S9-S22.Huq L, Cross KJ, Ung M, Reynolds EC. A review of protein structure and gene organization for proteins associated with mineralised tissue and calcium phosphate stabilization encoded on human chromosome 4. Arch Oral Biol. 2005; 50:599-609.Reynolds EC. Calcium phosphate-based remineralization systems: scientifi c evidence? Aust Dent J. 2008;53(3):268-73.White DJ. The application of in vitro models to research on demineralization and remineralization of the teeth. Adv Dent Res. 1995;9(3):175-93.Roberts AJ. Role of models in assessing new agents for caries prevention - non-fl uoride. Adv Dent Res. 1995;9(3):304-11.Walsh LJ. GC Tooth Mousse Portfolio, 4th edn. 2006. Singapore, GC Asia Dental Pte Ltd. pp. 14-15. Morgan MV, Bailey DL, Adams GG, Tsao C, Hyslop A, Escobar K, Manton D, Reynolds EC. A clinical trial measuring white spot lesion progression and regression. J Dent Res (Sp. Iss). IADR 2008 Toronta, Abstract 0112.Clinical trial of Tooth Mousse on white spot lesions. J Dent Res 2009 (In press).Karlinsey RL, Mackey AC. Solid-state preparation and dental application of an organically modifi ed calcium phosphate. J Mater 2009 (In press).Karlinsey RL, Mackey AC, Stookey GK. In vitro remineralisation effi cacy of NaF systems containing unique forms of calcium: a pilot study. Am J Dent (In press). 2009.Karlinsey RL, Mackey AC, Stookey GK, Pfarrer A. In vitro assessments of experimental NaF dentifrices containing a prospective calcium phosphate technology. Am J Dent (In press). 2009.Cross KJ, Huq NL, Palamara JE, Perich JW, Reynolds EC. Physicochemical characterization of casein phosphopeptide-amorphous calcium phosphate nanocomplexes. J Biol Chem. 2005;280(15):15362-9.
1 13
214
15
316
4
175
186
7
198
9
10
21
20
11
2212
REFERENCESWalsh LJ. Tooth Mouse: anthology of applications. 2007, Singapore: GC Asia Pte Ltd.Cross KJ, Huq NL, Reynolds EC. Casein phosphopeptides in oral health - chemistry and clinical applications. Curr Pharm Des. 2007;13(8):793-800.Reynolds EC. Anticariogenic complexes of amorphous calcium phosphate stabilized by casein phosphopeptides: a review. Spec Care Dentist. 1998;18(1):8-16.Reynolds EC. Remineralization of enamel subsurface lesions by casein phosphopeptide-stabilized calcium phosphate solutions. J Dent Res. 1997;76(9):1587-95. Manton DJ, Walker GD, Cai F, Cochrane NJ, Shen P, Reynolds EC. Remineralization of enamel subsurface lesions in situ by the use of three commercially available sugar-free gums. Int J Paediatr Dent. 2008;18(4):284-90. Walker G, Cai F, Shen P, Reynolds C, Ward B, Fone C, Honda S, Koganei M, Oda M, Reynolds E. Increased remineralization of tooth enamel by milk containing added casein phosphopeptide-amorphous calcium phosphate. J Dairy Res. 2006;73(1):74-8. Morgan MV, Adams GG, Bailey DL, Tsao CE, Fischman SL, Reynolds EC. The anticariogenic effect of sugar-free gum containing CPP-ACP nanocomplexes on approximal caries determined using digital bitewing radiography. Caries Res. 2008;42(3):171-84. Reynolds EC, Cai F, Cochrane NJ, Shen P, Walker GD, Morgan MV, Reynolds C. Fluoride and casein phosphopeptide-amorphous calcium phosphate. J Dent Res. 2008 ;87(4):344-8. Cochrane NJ, Saranathan S, Cai F, Cross KJ, Reynolds EC. Enamel subsurface lesion remineralisation with casein phosphopeptide stabilised solutions of calcium, phosphate and fl uoride. Caries Res. 2008;42(2):88-97.Iijima Y, Cai F, Shen P, Walker G, Reynolds C, Reynolds EC. Acid resistance of enamel subsurface lesions remineralized by a sugar-free chewing gum containing casein phosphopeptide-amorphous calcium phosphate. Caries Res. 2004;38(6):551-6.
ABOUT THE EXPERTLaurence J. Walsh is Professor of Dental Science at The University of Queensland in Brisbane, Australia, and has been the Head of the School of Dentistry for the past 6 years. He is a clinical specialist in special needs dentistry, and has been researching preventive agents for the past 25 years. He developed the clinical protocols which are currently used with the Tooth Mousse series of products in his clinical practice. He has served for many years as an advisor to a range of dental companies involved in preventive dentistry. He has no fi nancial interests in either the Tooth Mousse or ClinPro products discussed in this article.
USER
REPO
RTTE
CHN
OLO
GY
CLIN
ICAL
of ClinPro over other common 1000 ppm fluoride toothpastes, to validate the inclusion of TCP into a toothpaste formulation. Dental professionals should remember that it takes significant time (and expense) to establish the bona fides of a new technology, and that a “watching brief” is important in working through the various products and their therapeutic claims.
42
Conclusions: apples and orangesLooking at the evidence base available at the present time, it is important to clearly distinguish between these two products. In fact, one could argue that they share only two features – their nominal fluoride concentrations are similar, and both use vanilla as a flavour. In fact, human in situ and clinical trial data is needed to support the use

DEN
TAL IN
C. July/A
ugust 2009
7
ACTIONRECALDENTTM
CPP-ACPEVIDENCE
OTHERCALCIUM
PHOSPHATESYSTEMS
Inhibition of caries in an animal model √ Reynolds et al., 1995(J Dent Res, 74, 1272-1279) ?
Inhibition of dentine demineralisation in vitro √
Yamaguchi et al., 2007(Caries Res, 41, 204-207)Rahiotis & Vougiouklakis, 2007(J Dent, 35, 695-698)
?Promotion of dentine remineralisation in vitro √ Rahiotis & Vougiouklakis, 2007
(J Dent, 35, 695-698) ?
Inhibition of plaque formation in situ √ Rahiotis et al., 2008(J Dent, 36, 272-280) ?
Inhibition of enamel demineralisation in situ √Reynolds, 1987(J Dent Res, 66, 1120-1127)Reynolds, 1998(Spec Care Dentist, 18, 8-16)
?
Promotion of enamel subsurface lesion remineralisation in situ √
11 publications including Shen et al., 2001
(J Dent Res, 80:2066-2070)Iijima et al., 2004
(Caries Res, 38, 551-556)Manton et al., 2008(Int J Paediatr Dent, 18, 284-290)
?
Inhibition of caries progression andpromotion of regression of caries in a randomised controlled clinical trial
√ Morgan et al., 2008(Caries Res, 42,171-184) ?
Promotion of enamel subsurface lesion remineralisation in a randomised controlled clinical trial
√ Bailey et al., 2009(J Dent Res, Submitted) ?
PROVEN FACTS
No other systemcomes close to matching what
nature has developed
GC Tooth Mousse contains RECALDENTTM (CPP-ACP), an unique ingredient
developed at The School of Dental Science, The University of Melbourne, Victoria, Australia.
RECALDENT and RECALDENT Device are trade marks used under licence.
GC Asia Dental Pte Ltd19 Loyang Way #06-27
Singapore 508724T +65 6546 7588 F +65 6546 7577