identifying ovarian tumors at high risk for ovarian cancer frederick r. ueland, m.d. associate...
TRANSCRIPT

Identifying Ovarian Tumors at High Risk for Ovarian Cancer
Frederick R. Ueland, M.D.
Associate Professor Gynecologic Oncology
Vice Chairman, Department of Obstetrics and Gynecology
University of Kentucky Markey Cancer Center

Ovarian CancerEpidemiology
● Fifth leading cause of female cancer death in the United States
● Approximately 21,500 new cases of ovarian cancer and 14,600 deaths in 2009
● Median age at diagnosis: 63 years● Incidence: 13.1 per 100,000 women● Prevalence: 176,000 women alive with a history of
ovarian cancer (2006)● Lifetime risk: 1/71 (1.4%)
American Cancer Society, 2007Surveillance, Epidemiology, and End Results (SEER) Program: National Cancer Institute, 2008

Cancer Incidence Rates 1975-2003
Age-adjusted to the 2000 US standard population and adjusted for delays in reporting.Source: Surveillance, Epidemiology, and End Results Program, 1975-2003, Division of Cancer Control andPopulation Sciences, National Cancer Institute, 2006
0
25
50
1975 1978 1981 1984 1987 1990 1993 1996 1999 2002
Colon and rectum
Rate Per 100,000
Uterine Corpus
Ovary

Cancer Mortality Rates1930-2003
Age-adjusted to the 2000 US standard population.Source: US Mortality Public Use Data Tapes 1960-2003, US Mortality Volumes 1930-1959,National Center for Health Statistics, Centers for Disease Control and Prevention, 2006
0
10
20
30
4019
30
1935
1940
1945
1950
1955
1960
1965
1970
1975
1980
1985
1990
1995
2000
Colon & rectum
UterusStomach
Ovary
Rate Per 100,000
Background
• Advanced stage presentation common (70%)• Poor prognosis (50% 5-year survival)• Slowly improving outcomes
– Annual mortality change: –1.4% (2002-2006)• Treatment
– Comprehensive surgical staging for early disease– Cytoreduction for advanced disease– Combination chemotherapy– Clinical trials
American Cancer Society: Facts & Figures, 2009. Atlanta. www. Cancer.orgHoskins WJ, Perez CA, Young RC, eds. Principles and practice of Gynecologic Oncology, 4 th ed.
Philadelphia: Lippincott Williams & Wilkins: 919-922, 2006

Stage and Outcome
Stage Percent Survival
I 24 95%
II 6 65%
III 55 15-30%
IV 15 0-20%
Overall 50%
American Cancer Society

Ovarian Cancer Symptoms• Symptom awareness
– 95% report symptoms prior to diagnosis– > 12 times monthly– Pelvic and abdominal pain (77%)– Bloating, early satiety, GI symptoms (70%)– Pelvic (26%) and urinary symptoms (34%)
• Physician evaluation– Avoid diagnostic delay– Examination, imaging, laboratory testing as indicated– Sensitivity
• 57% for early stage• 80% for advanced stage
– Specificity• 90% if > 50yo• 86% for premenopausal women
Goff B, et al. JAMA. 291:2705-12:2068-75, 2004Olson S, et al. Obstet Gynecol. 98:212-7, 2001Goff B, et al. JAMA. 291:2705-12:2068-75, 2004Olson S, et al. Obstet Gynecol. 98:212-7, 2001

Challenge of Ovarian Tumors• There are 155 million women in United States
– ~125 million women 13 years of age or older• 90 million are between 13 and 50 years of age• 30 million are over age 50• 40 million women are Baby Boomers (age 41-59)
• How common are ovarian tumors? – Premenopausal women
• 14% annual incidence (13 million) • 30% prevalence (27 million)
– Postmenopausal women• 5% annual incidence (1.5 million)• 16% prevalence (5 million)
– 30% of unilocular and 45% of complex tumors typically persist
• Annually, there are tens of millions of ovarian cystic tumors, but only 22,000 ovarian cancers diagnosed United States Census Bureau, 2008Data from University of Kentucky Ovarian Cancer Screening Program, 2009 (N=27,000)

Ovarian TumorsPremenopausal Women
• 15% of ovarian neoplasms in premenopausal women are malignant
• Non-inflammatory ovarian tumors– 70% functional cysts– 20% neoplastic– 10% endometriomas
• Other– Inflammatory process, bowel

Ovarian TumorsPostmenopausal Women
• 50% of ovarian neoplasms in postmenopausal women are malignant
• Benign epithelial tumor • Stromal tumor
– Granulosa cell – Fibroma– Thecoma
• Epithelial ovarian cancer• Metastatic cancer

Guidelines and Algorithms•NIH Consensus Statement, 1994
– “Women with ovarian masses identified preoperatively having a significant risk of cancer should be given the option of surgery performed by a gynecologic oncologist”
•Clinical algorithms– Examination, imaging, patient history, and
laboratory tests– Infrequently utilized, not standardized– Challenging to evaluate

Biopsy of Ovarian Tumors
• Percutaneous FNA cytology of cystic ovarian tumors has low cancer sensitivity, ranging from 25% to 82%
• Approximately 25-50% of ovarian cystic tumors aspirated in perimenopausal women will recur within 1 year
• Aspiration of a malignant cystic tumor may disseminate the cancer, increase the stage and worsen the prognosis
ACOG Practice Bulletin no 83, 2006. Mizuno M, et al. Oncology. 65:29, 2003Sainz de la Cuesta R, et al. Obstet Gyn. 84:1, 1994

Evaluation
• Physical examination– Pelvic, abdominal, and lymph node survey
• Imaging study– Transvaginal ultrasonography– CT scan
• CA-125– Not FDA-approved as a diagnostic test– Low sensitivity and specificity

Pelvic ExaminationDetecting Ovarian Tumors
1. Ovarian detection on pelvic examination is infrequent in women ≥ 55 years old (30%)
2. Ovarian detection is exceedingly difficult in women weighing at least 200 lb (9%)
3. A large uterus (weight ≥ 200 g) makes ovarian palpation unlikely (16%)
Ueland et al. Gyn Oncol, 2005

Pelvic Exam vs. Ultrasound
Pelvic Exam Ultrasound P value
Age ≥ 55 0.30 0.74 < 0.001
Patient wt ≥ 200 lb
0.09 0.73 < 0.001
Uterine wt ≥ 200 g
0.16 0.80 < 0.001
Ueland et al. Gyn Oncol, 2005

Sonographic CharacteristicsOvarian Tumors
• Unilateral• Simple, unilocular• Septated (MI < 5)• No ascites• Resolution
• Bilateral• Complex (MI ≥ 5)
– Solid wall abnormalities– Internal papillations
• Ascites• Persistence or growth
Benign Malignant

Ovarian Tumor Imaging
Type of Cyst Patients %Regressed under observation 205 72
Required exploratory laparotomy
81 28
Ovarian neoplasms 46 16
Benign epithelial 32 11
Benign teratoma 9 3
Malignant epithelial 4 1.4
Dysgerminoma 1 0.3
Endometriosis 28 10
Para-ovarian cyst 4 1.4
Hydrosalpinx 3 1
Functional cysts 0 0
Spanos W. Am J Obstet Gynecol, 1973

Ovarian Tumor Imaging
Modesitt et al, Gyn Oncol, 2003
Type of Cyst Patients %
Resolution 2261 69%
Cyst + septum 537 17%
Persistent cyst 220 7%
Cyst + solid area 180 5%
Solid mass 21 0.7%
Removed by surgery 40 1.3%
Total 3259 100%

Kentucky Morphology IndexMI Score = 6
Ueland et al. Gyn Oncol, 2003Ascites

Kentucky Morphology IndexHigh Risk Score (5-10)
20
3238
92
7783
Ueland et al. Gyn Oncol, 2003

Morphology IndexPredicting Malignancy
• Sensitivity 0.98
• Specificity 0.81
• Positive predictive value 0.41
• Negative predictive value0.99
• Accuracy 0.83
Ueland et al. Gyn Oncol, 2003

Ovarian Tumor Ultrasound
Definition of (+) US varied with each author
Author Number Prevalence Sens(%) Spec (%) PPV(%)PPV
(at 20%)
Kobayashi, 1976
406 15 70 73 31 39
Hermann, 1987
241 21 82 93 75 73
Finkler, 1988
102 36 62 95 88 75
Benacerraf, 1990
100 30 80 87 72 62
Granberg, 1990
180 22 82 92 74 73
Sassone, 1991
143 10 100 83 37 59
Ueland, 2003
442 12 98 81 41 56

CA-125• Antigen derived from:
– coelomic epithelium (pericardium, pleura, peritoneum)– mullerian epithelium (tubal, endometrial, endocervical)
• Two different assays– Assay I < 35 U/ml– Assay II < 20 U/ml
• Expressed by 80% non-mucinous EOC• FDA-approved to monitor cancer treatment
– Neither a screening nor a diagnostic test
• False negative CA-125 values (low sensitivity)– 50% of early stage ovarian cancers– 20-25% of advanced stage ovarian cancers– Mixed mullerian tumors, clear cell cancers

CA-125Non-specific
• Benign ovarian cysts• Uterine leiomyomata• Pelvic inflammatory
disease• Endometriosis• Adenomyosis• Pregnancy • Menstruation• Ascites
• Heart failure• Liver failure• Renal failure• Peritoneal tuberculosis• Diverticulitis• Pancreatitis• Recent abdominal or
thoracic surgery• Other malignancies

Role Surgery
• Proper staging for early disease– Determine adjuvant therapy
• Cytoreduction for advanced disease– Radical surgery as indicated– “Optimal” ≤ 1cm
• Reassessment laparotomy
• Secondary debulking

Staging by Specialty
• Women with early stage ovarian cancer– 291 subjects
• Complete surgical staging performed:– 97% gynecologic oncologists– 52% general obstetrician/gynecologists– 35% general surgeons
McGowan L, et al. Obstet Gynecol;65:568-72, 1985

Surgical CytoreductionAdvanced Stage Ovarian Cancer
Slide courtesy of Gynecologic Cancer Foundation

Surgical CytoreductionAdvanced Stage Ovarian Cancer
• Meta-analysis of 53 studies
– 6,885 stage III/IV patients
• Cytoreduction– High volume centers have higher
rates of “optimal” surgery
– “Optimal” improved survival by 11 months (50% increase)
– Each 10% increment in cytoreduction = 5.5% improvement in survival
20
22
24
26
28
30
32
34
36
38
40
0 10 20 30 40 50 60 70 80 90 100
% Cytoreduction
Med
ian
Sur
viva
l (m
onth
s)
Bristow, J Clin Oncol 20:1248, 2002

Improved Survival
• Utah Cancer Registry– 848 new ovarian cancers, 1992-1998
• Only 39% were ever seen by a gyn onc
• Patients with advanced disease had significant survival advantage when managed by gynecologic oncologist– median survival 26 mo vs. 15 mo, p < 0.01
Carney ME, et al. Gynecol Oncol;84:36-42, 2002

Improved Survival
• Medicare claims by physician specialty– SEER database– 65 years or older– 3067 surgeries for ovarian cancer
• Only 33% of patients with ovarian cancer were treated by gynecologic oncologist
• Improved outcomes and overall survival when managed by gynecologic oncologistEarle C.C, et al. JNCI 98:3, 2006


Value of Specialists
• Meta-analysis (18 studies) concluded marked benefit with gynecologic oncologist (Giede 2005)
– Complete surgical staging with early stage disease– Optimal cytoreductive surgery with advanced disease– Improved median and overall survival
• Others supporting GO involvement: – NCCN guidelines– SGO, ACOG– SOGC clinical practice guidelines– NIH consensus statement– London Medical Advisory statement

33
NCCN Guidelines
●Cytoreductive surgery●all patients with stage II, III or IV ovarian cancer●“optimal” cytoreduction (no residual disease > 1 cm)
●Gynecologic oncologist ●perform the initial surgical procedure●Improved overall survival●Category I recommendation
●Combination adjuvant chemotherapy●Most patients (>70%) relapse after 1st line therapy●Clinical trials
NCCN Clinical Practice Guidelines in Oncology, 2008Ozols et al. J Clin Oncol. 21: 3194-3200, 2003

34
Ovarian Cancer Dilemma
● Ovarian tumors are very common, particularly in young women
● Women with benign tumors prefer to have their surgery close to home with their established gynecologist
● Women with ovarian cancer are best managed by a gynecologic oncologist
● Current methods are unreliable in differentiating benign from malignant ovarian tumors, particularly in young women and early stage disease

ACOG Referral Guidelines
• CA125 >200 U/mL• Ascites• Evidence of abdominal or
distant metastases• Family history one or
more first-degree relatives with ovarian or breast cancer
• CA125 >35 U/mL• Nodular or fixed mass• Ascites• Evidence of abdominal or
distant metastases• Family history one or
more first-degree relatives with ovarian or breast cancer
Premenopausal Women Postmenopausal Women

Validation of Guidelines• Im, 2005
– Chart review with 7 tertiary centers: 1035 patients– 95% had imaging, 68% had preop CA-125, 24% had both– “SGO and ACOG referral guidelines effectively separate
women with pelvic masses into two risk categories for malignancy”
• Dearking, 2007– Prospective, single-institutional trial: 837 patients– Guidelines performed well in predicting advanced-stage
disease, but “poorly” in early-stage disease, and premenopausal women
– Recommended modifications:• CA-125 <67 U/mL (pre), exclude FH of breast, ovarian cancer

A Multi-institutional Evaluation of ACOG and SGO Referral
Guidelines for an Ovarian Mass
Rachel Ware, Alan Smith, Chris Desimone, Leigh Seamon, Scott Goodrich, Iwona
Podzielinski, Lori Sokoll, Joseph Santoso, J.R. van Nagell Jr., Zhen Zhang,
Frederick Ueland.
Presented at the Society of Gynecologic Oncology Annual Meeting, 2010Presented at the Society of Gynecologic Oncology Annual Meeting, 2010

Results
ACOG Criteria
Modified ACOG Criteria
Sensitivity, % 77 80 95% CI 70 to 83 73 to 85
Specificity, % 68 71 95% CI 63 to 72 66 to 75
PPV, % 52 55 95% CI 46 to 58 49 to 61
NPV, % 87 88 95% CI 82 to 90 84 to 92

ACOG Results
Premenopausal (N= 235)
Postmenopausal (N= 281)
ACOG Criteria ACOG Criteria
Modified ACOG Criteria
ACOG Criteria
Modified ACOG Criteria
Sensitivity, % 58 76 84 81 95% CI 43 to 71 61 to 86 77 to 90 73 to 87
Specificity, % 77 70 56 71 95% CI 71 to 83 64 to 77 49 to 64 64 to 77
PPV, % 38 38 58 66 95% CI 27 to 50 28 to 48 50 to 65 58 to 74
NPV, % 89 92 84 84 95% CI 83 to 92 87 to 96 76 to 90 77 to 89

ACOG Results
ACOG CriteriaPremenopausal women
Cancer Stage
Early Late
Sensitivity, % 47 10095% CI 26 to 69 72 to 100
Specificity, % 77 7795% CI 71 to 83 71 to 83
PPV, % 16 1995% CI 8 to 28 11 to 31
NPV, % 94 10095% CI 89 to 97 98 to 100

FDA NEWS RELEASE
For Immediate Release: Sept. 11, 2009
Media Inquiries: Peper Long, 301-796-4671, [email protected] Inquiries: 888-INFO-FDA
FDA Clears a Test for Ovarian CancerTest can help identify potential malignancies, guide surgical decisions
The U.S. Food and Drug Administration today cleared a test that can help detect ovarian cancer in a pelvic mass that is already known to require surgery. The test, called OVA1, helps patients and health care professionals decide what type of surgery should be done and by whom.

The OVA1 Test
• Biomarker panel– CA125, transthyretin (prealbumin),
apolipoprotein A1, beta 2 microglobulin, transferrin
• OvaCalc software algorithm• OVA1 risk index, range 0-10
Premenopausal Postmenopausal
Low Risk < 5.0 < 4.4
High Risk ≥ 5.0 ≥ 4.4

OVA1 Indications
• Known pelvic mass or ovarian tumor
• Complete physician assessment– Examination, imaging, history, labs
• Decision for surgery
• OVA1– Low risk OVA1 reassuring– High risk OVA1 referred to gyn oncologist

The OVA1 Test Improves the Preoperative Assessment of
Ovarian Tumors
Frederick Ueland, Chris Desimone, Leigh Seamon, Rachel Ware, Scott Goodrich,
Iwona Podzielinski, Lori Sokoll, Alan Smith, Joseph Santoso, J.R. van Nagell Jr., Zhen
Zhang.
Presented at the Society of Gynecologic Oncology Annual Meeting, 2010Presented at the Society of Gynecologic Oncology Annual Meeting, 2010

Methods• 27 primary care, specialty sites throughout U.S.• Preoperative evaluation
– imaging to confirm ovarian tumor– serum collection for CA125– physician assessment (Is it malignant? “yes or no”)
• Centralized assay at Quest Diagnostics• Validation assays
– Johns Hopkins Biomarker Discovery Center– Specialty Laboratories
• Independent data analysis– Applied Clinical Intelligence

Study Population All Subjects
Non-GO Physicians
GO Physicians
Patients 516 269 247Mean age, yr (sd) 52 (14) 50 (14) 55 (14)Median age, yr 52 48 54Range (min, max) 18 to 92 19 to 90 18 to 92
Menopausal Status, n (%)Pre 235 (46%) 144 (54%) 91 (37%)Post 281 (54%) 125 (46%) 156 (63%)
Pathology Diagnosis, n (%)Benign ovarian condition 355 (69%) 197 (73%) 158 (64%)Epithelial ovarian cancer (EOC) 96 (19%) 45 (17%) 51 (21%)Other primary ovarian malignancy 9 (2%) 5 (2%) 4 (2%)Low malignant potential (borderline) 28 (5%) 12 (4%) 16 (6%)
Non-primary ovarian malignancy with involvement of the ovaries
18 (4%) 5 (2%) 13 (5%)
Non-primary ovarian malignancies with no involvement of ovaries
10 (2%) 5 (2%) 5 (2%)
OVA1 Trial

0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Tru
e p
osi
tive
rate
(S
en
siti
vit
y)
False positive rate (1-Specificity)
Premenopausal, AUC= 0.80 (95% CI: 0.73-0.88)Postmenopausal, AUC=0.82 (95% CI: 0.77-0.87)
OVA1 Test Alone
Sensitivity 92%
Specificity 43%
PPV 42%
NPV 93%

OVA1 Sensitivity
Tumor subtype Cancer stage
I 90%
II 100%
III 100%
IV 100%
Epithelial OC 99%
Non EOC 78%
LMP 75%
Metastases 94%
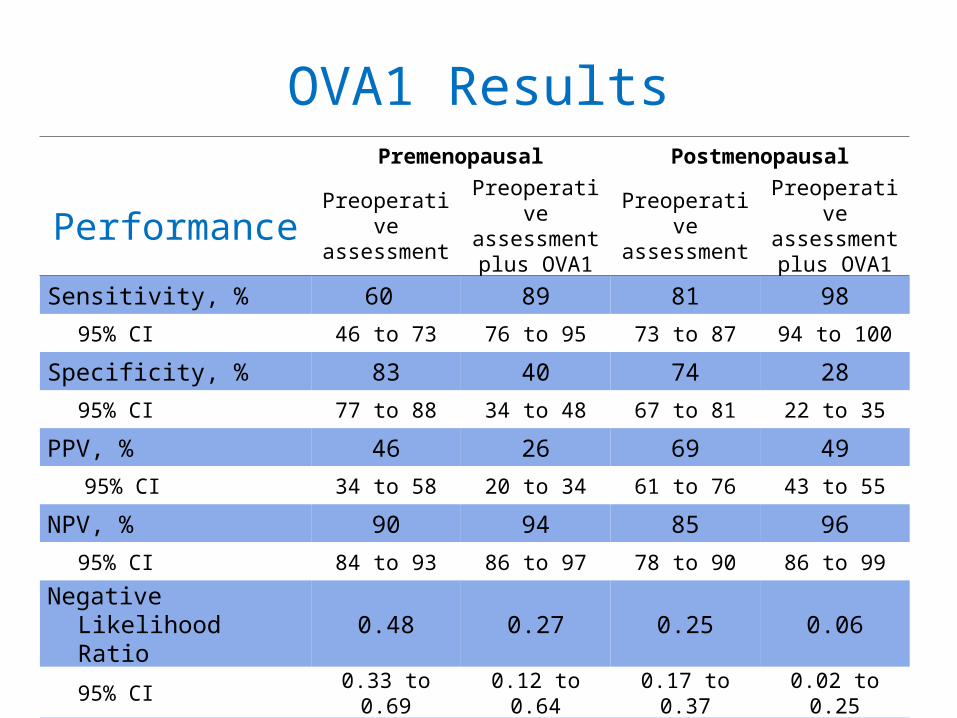
Premenopausal Postmenopausal
PerformancePreoperativ
e assessment
Preoperative assessment plus OVA1
Preoperative
assessment
Preoperative assessment plus OVA1
Sensitivity, % 60 89 81 98
95% CI 46 to 73 76 to 95 73 to 87 94 to 100
Specificity, % 83 40 74 28
95% CI 77 to 88 34 to 48 67 to 81 22 to 35
PPV, % 46 26 69 49
95% CI 34 to 58 20 to 34 61 to 76 43 to 55
NPV, % 90 94 85 96
95% CI 84 to 93 86 to 97 78 to 90 86 to 99
Negative Likelihood Ratio
0.48 0.27 0.25 0.06
95% CI 0.33 to 0.69 0.12 to 0.64 0.17 to 0.37 0.02 to 0.25
Prevalence 19% (45/235) 41% (116/281)
OVA1 Results

non-GO physicians GO physicians
PerformancePreoperativ
e assessment
Preoperative
assessment plus OVA1
Preoperative
assessment
Preoperative assessment plus OVA1
Sensitivity, % 72 92 78 99
95% CI 61 to 81 83 to 96 68 to 85 94 to 100
Specificity, % 83 42 75 26
95% CI 77 to 87 35 to 49 67 to 81 20 to 33
PPV, % 60 36 63 43
95% CI 50 to 70 30 to 44 54 to 72 36 to 50
NPV, % 89 93 86 98
95% CI 84 to 93 86 to 97 79 to 90 88 to 100
Negative Likelihood Ratio
0.34 0.20 0.30 0.04
95% CI 0.23 to 0.49 0.09 to 0.44 0.20 to 0.45 0.01 to 0.31
Prevalence 27% (72/269) 36% (89/247)
OVA1 Results

OVA1 Clinical Utility
1. The OVA1 test successfully classifies patients into high or low probability of malignancy.
2. OVA1 has high sensitivity in pre- and postmenopausal women, all stages of EOC.
3. OVA1 outperforms the ACOG criteria and physician assessment.
4. When combined with other clinical information, the OVA1 test can help determine the risk of malignancy for an ovarian tumor before surgery, and facilitate decisions about referral to a gynecologic oncologist.

Simplified Algorithm
Ovarian Tumor
Physician Assessment
Local surgery
High RiskLow Risk
Referral to GYO for Surgery
OVA1 Blood Test

Summary
• Ovarian tumors are exceedingly common, particularly in premenopausal women
• 5-10% of American women will undergo surgery to evaluate ovarian mass in their life-time
• Ovarian cancer is infrequent but often fatal in advanced stages
• Current algorithms (which combine symptoms, imaging, physical examination, and CA-125) are useful for identifying advanced stage cancer but of limited utility in detecting early stage disease

Summary
• OVA1 is the only FDA-approved blood test for ovarian tumors to assist physicians in making preoperative referral decisions
• Appropriate referral to a gynecologic oncologist for women at high risk for ovarian cancer may lead to improved survival