igf-1 insulin-like growth factor 1 matthew klinka
TRANSCRIPT
IGF-1Insulin-Like Growth Factor 1Matthew Klinka
BackgroundPrimarily produced in the liverHowever is also a paracrine
hormone◦Present in many cell types in a wide
range of tissue types.Typically bound to proteins when
both intra or extracellular◦98% of IGF-1 is protein bound◦IGFBP-3 most common

http://www.ncbi.nlm.nih.gov/Structure/mmdb/mmdbsrv.cgi?uid=20049

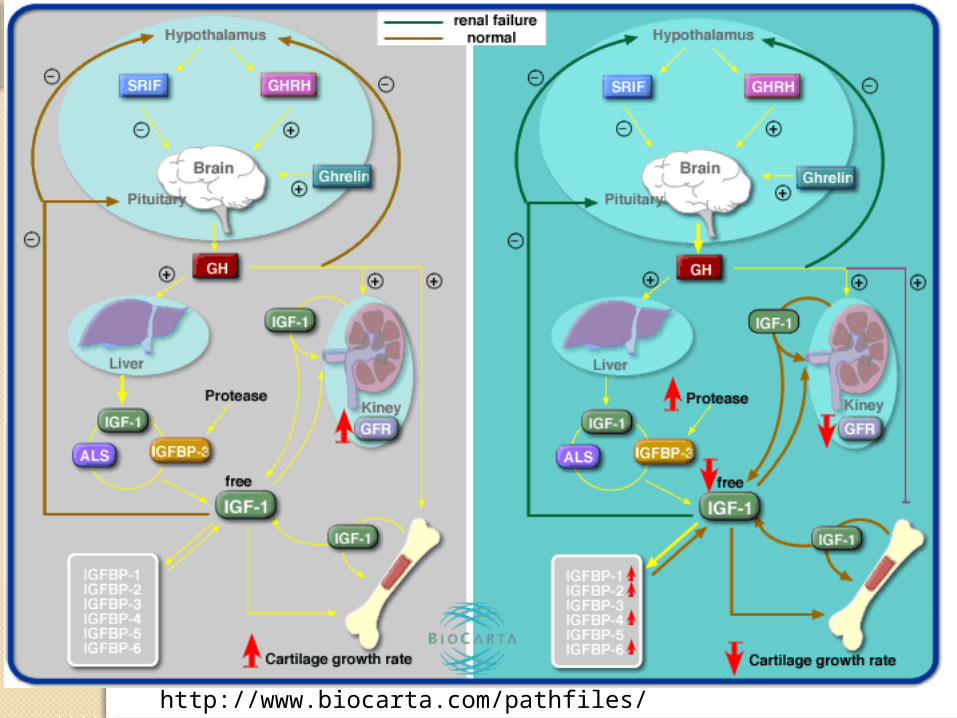
ProductionProduction of IGF-1 is linked to
dietary protein intake◦Especially casein◦Protein free diet can result in IGF-1
deficiencyMade in response to growth
hormone signalling
FunctionAnabolic Hormone
◦IGF-1 triggers growth until adulthood◦After adulthood triggers hypertrophy
in skeletal muscleRegulates kidney function and
growth

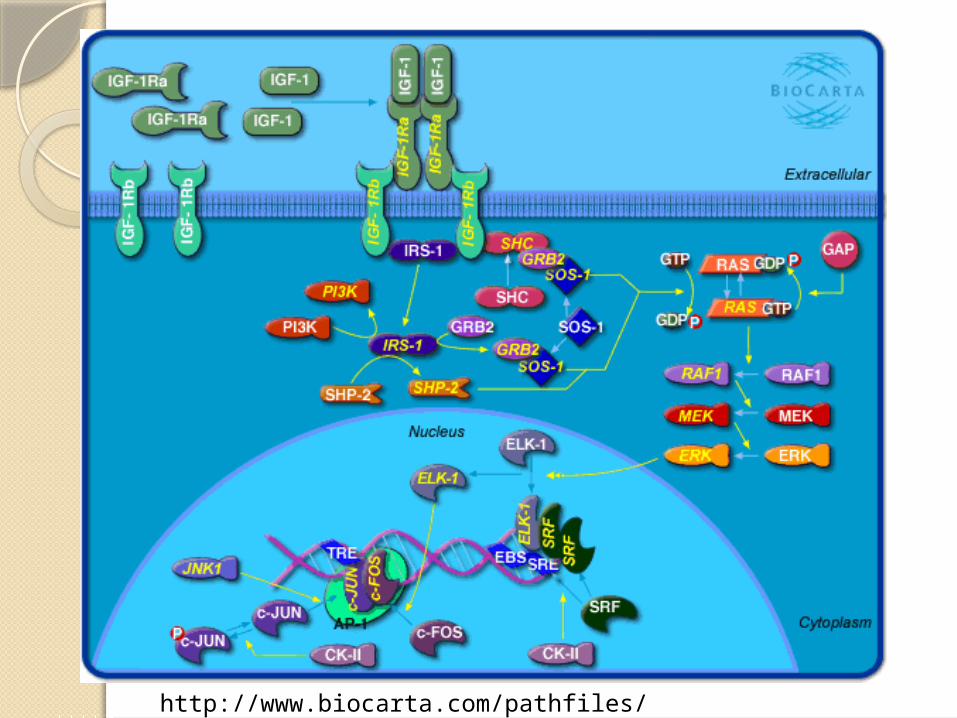
ReceptorReceptor is IGF1R
◦“Insulin-like growth factor 1 receptorTyrosine Kinase receptor
◦Dimeric◦Two sets of Alpha & Beta subunits◦320 Kda◦Member of the Insulin receptor
family◦Beta subunits contain the catalytic
tyrosine residues

IGF-2 BindingIGF1R may also bind IGF-2Key differences:
◦IGF-2 functions primarily in fetal development During gestation aids neural
development
◦IGF-1 functions in adults During gestation deals with physical
development

http://www.ncbi.nlm.nih.gov/Structure/mmdb/mmdbsrv.cgi?uid=68828
Primary ResultIGF1R triggering often results in
cell proliferation or growthHowever still a cell specific
response◦Ie: may trigger growth in size of an
adult’s skeletal muscle cells, or may trigger growth and subsequent division of embryonic cells
◦May even trigger growth (hypertrophy) of heart muscle cells
Role in reproductionIGF1R plays a role in the
development of limb buds in an embryo
IGF1R serves to facilitate lactation in pregnant and nursing females◦Differentiates breast cells into duct
and glandular tissue◦Prevents apoptosis of duct and
glandular tissue during pregnancy and nursing

CancerBecause of it’s anti-apoptotic
action, IGF1R may contribute to some cancers◦Prostate◦Breast◦Cervical
All of the above have been observed to contain cells with heightened levels of IGF1R

CraniosynostosisPremature ossification of sutures
in an infant cranium◦Results in oddly shaped skull and in
most cases brain damage if not corrected
Caused by a number of different single nucleotide polymorphisms in IGF1R

Secondary ReceptorIGF-1 Can also bind insulin
receptor◦Also a tyrosine Kinase receptor◦Much lower binding affinity than
IGF1R◦IGF-1 binds at 10% of the rate of
insulin◦May form a heterodimer with IGF1R
RegulationIn serum may be bound by
certain IGFBPs◦IGF-1 has a higher affinity for some
of these than it does for its receptor◦IGF1R may be targeted with tyrosine
kinase inhibitors◦miRNA thought to play a role in
regulation as well
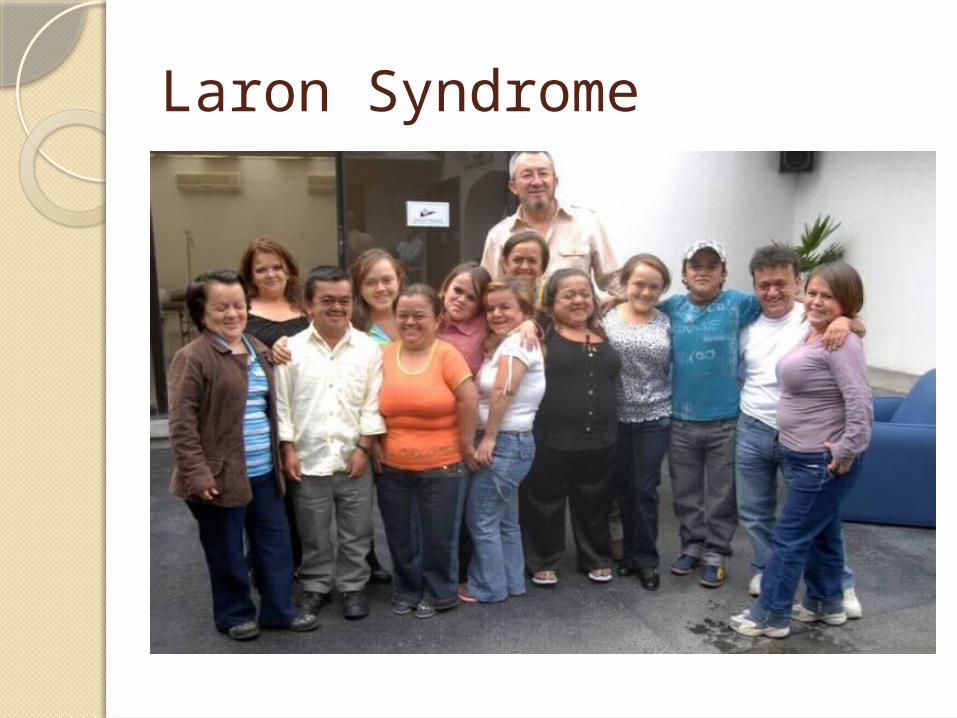
Laron Syndrome
Laron SyndromeAutosomal recessiveResults from low levels or low
efficacy of IGF-1◦Most cases are due to a lack of GH
receptor◦Some due to mutation in genes
coding for IGF-1 or IGF1R
SymptomsNormal GH levelsVery low IGF-1 levelsShort statureProminent foreheadObesity in the trunk of the bodyLack of response to GH therapy
◦Typically used to treat other forms of dwarfism

TreatmentSynthetic IGF-1Must be taken before pubertyNot effective if there are other
mutations further along the signaling pathway
Cancer, Diabetes, and agingInterestingly, people with Laron
syndrome are nearly immune to cancer and diabetes.◦Two theories for cancer protection
1. IGF-1 has anti-apoptotic function Reduced IGF-1 results in more normal apoptosis
2. Lack of IGF-1 somehow results in more protection from oxidative DNA damage
Diabetes protectionLaron syndrome sufferers have
high insulin sensitivity despite being obese◦Most likely reason is because IGF-1
can bind insulin receptor◦In the absence of a competitor, a
smaller amount of insulin can have great effect
AgingIn mice, mutations reducing IGF-
1 levels resulted in longer lifespans on average◦In nematodes IGF-1 deficiency
resulted in doubling of lifespanMechanism is not understood
◦Unknown if this property occurs in humans Only ~300 people with Laron Syndrome
worldwide Difficult to establish a baseline because
incidence of accidental death is relatively common
http://www.biocarta.com/pathfiles/h_ghrelinPathway.asp
http://www.biocarta.com/pathfiles/h_igf1pathway.asp