igg4 _vishnu_seminar 13 jan 2011
DESCRIPTION
igg4 syndrome,autoimmune pancreatitis, extrapancreatic lesions,immune mediated sialadenitis,role of imaging,reidel thyroiditisTRANSCRIPT

Seminar
IgG4- related diseases
M.Vishnu Vardhan Reddy
Clinical Immunology department
SGPGIMS,Lucknow,IndiaSGPGIMS,Lucknow,India
13 Jan 2011

Format of Presentation
• Introduction
– History
– What is IgG4, special properties
• Clinical features• Clinical features
– Case report
– Clinical spectrum
– Prototype – AIP
– Extrapancreatic lesions

Introduction

Timeline
• 1961 -Autoimmune pancreatitis was first described
• 2001- diagnostic value of serum IgG4 concentrations became
well known
• 2003- Kamisawa et al proposed a new concept of IgG4-related
autoimmune disease around autoimmune pancreatitis,


2003

Ig G types
IgG4 subclass
•Least common in serum•Expressed in conditions of chronic antigenic exposure

IgG4 breaks rules
What we take for granted : But :
IgG antibodies have 2 identical
antigen binding sites-
monospecific
Bispecific-functional
monovalency
monospecific
Antibodies are stable structures
i.e they do not change after
secretion by plasma cell
Posttranslational modification-
dynamic arm exchange

Hinge region makes the difference
Hinge core of IgG1- CPPC:
Interchain disulphide bonds
IgG4- CPSC – Cannot form
interchain disulphide bonds

Dynamic Exchange of IgG4 half molecules
Bispecific but functionally monovalent
Exchange fab arms by swapping a heavy chain and attached light chain
(half-molecule) with a heavy-light chain pair from another molecule

IgG4 is anti-inflammatory :4 Mech
1. low affinity for C1q and Fc receptors
2. half antibody exchange�bi-specific’ and functionally monovalent
for a given antigen. IgG4 anti-bodies in the circulation cannot form
large immune complexes with antigenlarge immune complexes with antigen
3. much reduced binding to the low-affinity Fc-gamma receptors
4. IgG4 antibodies can displace the binding of those IgG1 or IgE
antibodies with related specificities

This antiinflammatory property is
therapeutically exploited
IgG4 constant domain used in recombinant antibodies where effector function is undesirable

Eponyms -IgG4-related systemic disease
IgG4-RSD
• IgG4-related sclerosing disease
• IgG4-related disease
• IgG4 syndrome
• IgG-related systemic sclerosing disease• IgG-related systemic sclerosing disease
• IgG4-related autoimmune disease
• Hyper-IgG4 disease
• Systemic IgG4-related plasmacytic syndrome (SIPS)
• IgG4-postive Multiorgan Lymphoproliferative Syndrome
[MOLPS]

Japan leads in IgG4 RSD reports

Clinical Spectrum

IgG4 -RSD presents as a mimic
IgG4 RSD Mimic
Autoimmune Pancreatitis Ca Pancreas
Igg4-associated Cholangitis P S C/Cholangiocarcinoma
Isd-lung Involvement Interstitial Pneumonia/Lung Cancer
Hepatopathy Autoimmunehepatitis
Lymphadenopathy Lymphoproliferative Neoplasms
Sialadenitis-mikulicz Disease,kuttners Sjogren Syndrome,sarcoid
Aortitis With Or Without Aneurysm Takayasu/Gaint Cell/Atherosclerosis
Retroperitoneal Fibrosis Ormonds Disease
Orbital Pseudotumor Wegeners/Lymphoma
Igg4 Thyroiditis/Reidels Hashimoto/Ca Thyroid

Increasing list-not exhaustive
• Inflammatory masses-of Pituitary-prostate-breast-skin
• Constrictive pericarditis
• Cervical fibrosis
• Meninges -pachymeningitis
• Tubulointerstitial nephritis- increasingly reported
• Gallbladder- acalculous lymphoplasmacytic cholecystitis

Spectrum of IgG4-RSD

4 histological hallmarks of IgG4 RSD
Lymphoplasmacytic infiltration
IgG4 plasma staining on IHC
Storiform fibrosis
Phlebitis with unremarkable
artery
Clinical Spectrum
Autoimmune PancreatitisPrototype of IgG4 RSD
Autoimmune pancreatitis
clinical presentation
• Pancreatic manifestations
• Acute– painless obstructive jaundice (80%)
– [D/D panccreatic CA]
– Acute/recurrent pancreatitis –rare– Acute/recurrent pancreatitis –rare
• Subacute /late:
• Persistent pancreatic mass
• Atrophic pancreas +/- calcifications
• Unexplained steatorrhea
• Extrapancreatic manifestations
• -simultaneous; precede;years later

AIP 2 types
AIP otherwise implies type 1 –IgG4 related

GCNA2008;37:439-60

Extrapancreatic lesions

Pathogenesis

Autoimmune origin suggested but never proved
YES
• Autoantigen distribution matches disease distribution
• Response to immunosuppressive therapy
POSSIBLY
• Autoreactive immune response to defined autoantigens
• Production of disease by adoptive transfer of autoreactive cells • Production of disease by adoptive transfer of autoreactive cells and/or antibody
• HLA association
• Induction of disease by sensitisation with autoantigen
• Spontaneous animal model with identical antigen specificity
NO
• Female predisposition
• Both children and adults affected


Definitive Autoantigen not established
• Antilactoferrin (ALF)
• Anticarbonic anhydrase II or IV (ACA-II, IV)
• Antipancreatic Secretory Trypsin Inhibitor (PSTI) in 30–40%
Genetic factors• DRB1*0405-DQB1*0401 in Japanese patients
• SNP in CTLA-4 gene in Taiwanese patients

Tregs are increased in IgG4 RSD!
• number of Tregs increased – in both tissue and blood ofpatients with IgG4-related disease
• Animal Models –Treg deficiency leads to spontaneous IgG4RSD
1. WBN/Kob rats –congentially decreased peripheral Tregs
2. Treg-deficient NODmouse
3. CD28KOmice-closely resembles the human disease—autoantigen-pancreatic amylase
• Hypothesis--Treg depletion may initiate AIP,whileprogression of disease is mediated by Tregs and itsmodulation of Th1/th2 balance towards Th2

Link between IgG4 RSD and Allergic Diathesis-
Th2-dominant reaction
• IgG4-related disease commonly develops in people with a
predisposition to allergy
• serum eosinophilia and high serum IgE levels are frequently
seen
• histologically shows eosinophilic infiltration
• IgG4 class switching depends on interleukin-4 and/or
interleukin-13 mainly secreted by T-helper 2 cells

Biphasic model

Histology–Immunology correlation

IgG4 elevation is a secondary response
• IgG4 type autoantibodies have not been detected in IgG4-
related disease!!
• whether IgG4 is an autoantibody in IgG4-related disease or is
overexpressed secondarily in response to an unknown
primary inflammatory stimulus??primary inflammatory stimulus??

Molecular mimicry with H pylori
• Evidence 1:homology between human CA-II and a-CA of H
pylori--the homologous segments contain the binding motif of
DRB1*0405
• possession of the HLA DRB1*0405-DQB1*0401 genotype
confers a risk for AIP developmentconfers a risk for AIP development
• Evidence 2: Antibodies to Plasminogen-binding Protein
Peptide

AIP serology
• Serum IgG4
• >140mg/dl—sensitivity 76% ;specificity 93% PPV 36%
• > 280mg/dl—sensitivity 53% ;specificity 99% PPV 75%
• Elevated in 7-10 % of CA pancreas (usually mild) & 5% of
normal population
• unsuitable single marker for diagnosis but when combined • unsuitable single marker for diagnosis but when combined
with other features of AIP, it is diagnostic
• Methods to detect IgG4 : Nephelometry & RID
• Other Autoantibodies-
• Lactoferrin & carbonic anhydrase2
• disadv--sensitivity –only 50% and not widely available,
• Pancreatic Secretory Trypsin Inhibitor(PSTI),
• ANA, RF
•
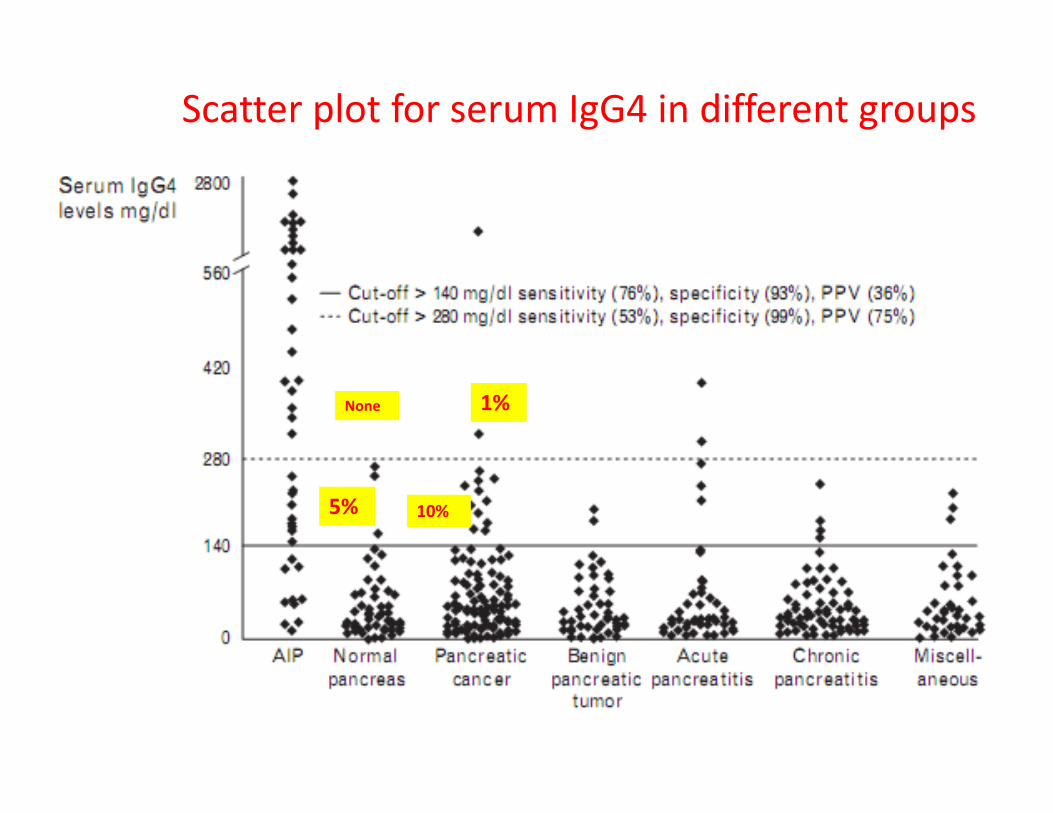
Scatter plot for serum IgG4 in different groups
None 1%
5%
None 1%
10%

94%-AIP
PBP - Plasminogen-binding Protein-H.Pylori
UBR2-- Ubiquitin-protein Ligase E3 Component N-recognin 2—
acinar cells of pancreas
94%-AIP
5%- pancreatic cancer
NEJM,2009

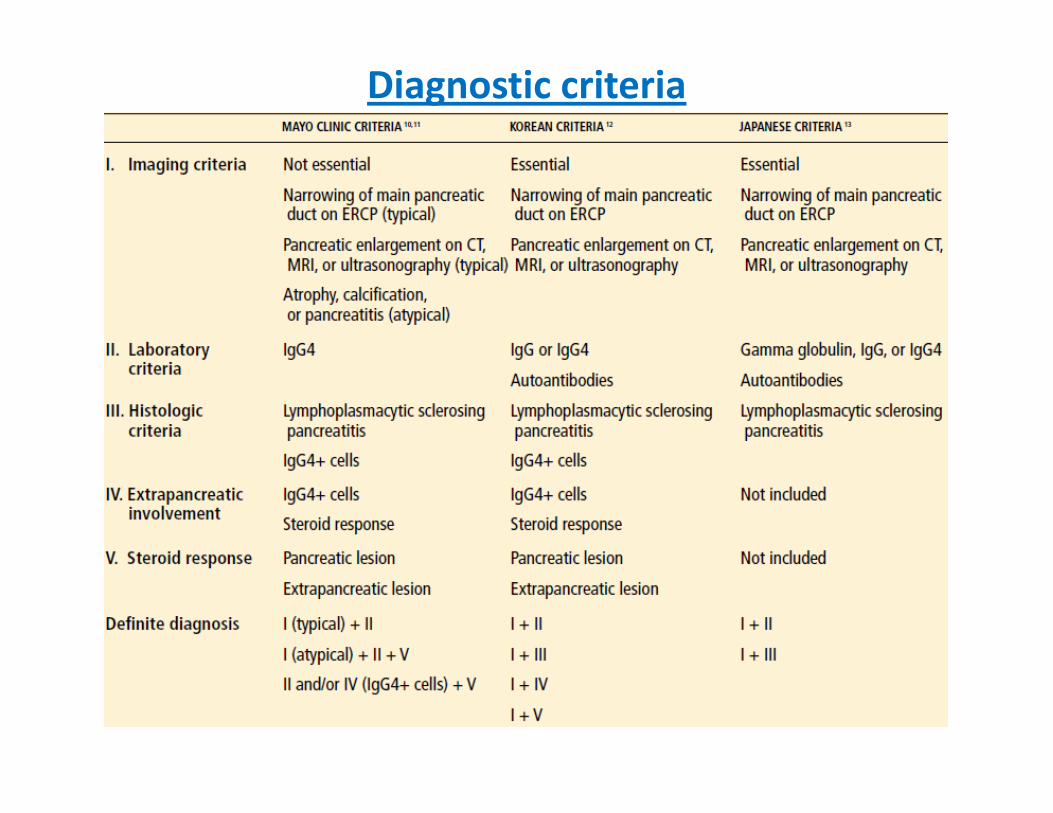
Diagnostic criteria
• Japan Pancreas Society (JPS I, JPS II)
• Mayo Clinic (HISORt criteria)
• South Korea criteria• South Korea criteria
• Asian consensus criteria-latest

3 ways to establish AIP diagnosis1.Typical imaging + serology or compatible histology
• If IgG4 levels not available ,then less specific autoimmune serological markers, such as high titres of ANAs and rheumatoid factor, may also be used
2.Diagnostic histology/immunostaining
• pancreatic histology showing all three features of LPSP-• pancreatic histology showing all three features of LPSP-but seen in only 20%
• IgG4 immunostaining, if there are >10 IgG4-positive cells per high power field.
• Isolated IgG4 immunostaining is not diagnostic
3.Response to steroids
• Steroid trials are both diagnostic and reassuring
Diagnostic criteria

Pancreatobiliary Imaging
• Enlargement of the pancreas, diffuse or focal
• Irregular narrowing of main pancreatic duct on ERCP
• Calcifications and cysts are rare
• Stenosis of the distal common bile duct

Typical imaging features
•diffusely enlarged gland with loss of lobulation (‘‘sausage-shaped’’)•diffusely enlarged gland with loss of lobulation (‘‘sausage-shaped’’)
•rim-like enhancement (arrows)
pancreatic duct with multiple strictures BUT not associated with ductal dilatation

serum IgG4 levels for monitoring therapy
and predicting relapse
• IgG4 levels failed to normalize in 115/182 (63%) of the
patients treated with steroids
• Only 30% of patients with persistent IgG4 elevation relapsed,
• relapse was also seen in 10% of patients who normalized IgG4
levelslevels
• utility of serial IgG4 levels- not convincing at present
Gut 2009,Kamisawa

Treatment
• Natural history -less known
• Steroid responsive only before dense sclerosis sets in
• Aim of Rx- to prevent organ damage and to prevent the involvement of other organ systems
• Indications for steroids: Obstructive jaundice, abdominal
pain, and back pain, and the presence of symptomatic extrapancreatic lesionsextrapancreatic lesions
• Symptomatic improvement in AIP occurs within 2 weeks
• Benefit of GCs
� higher remission rate
� Less time to remission
� improve pancreatic exocrine function

2 GC regimens
Japanese
• initially with prednisolone,
0.6mg/kg/day for 2–4 weeks
• taper over a period of 3–6
months to a dose of 5mg/day,
Mayo clinic
• Start with prednisone
40mg/day -4 weeks
• 7-week prednisone taper -
5mg/week, --stops by the end months to a dose of 5mg/day,
• continue at a dose between
2.5–5mg/day for up to 3 years
• 25% -disease flares despite
receiving maintenance GCs
5mg/week, --stops by the end
of 11 weeks
• more than 50% of AIP patients
relapsed within a median of 3
months (range: 0–14 months)
after discontinuing GCs

Other treatment options
• MMF and AZA-
• Rituximab
• Bortezomib

IgG4 Related Sialadenitis

Mikulicz’s disease-IgG4-related plasmacytic
exocrinopathy
• 1888-- Johann von Mikulicz–Radecki reported a case exhibiting
bilateral, painless and symmetrical swellings of the lacrimal, parotid
and submandibular gland
• 1953- Morgan and Castleman - 18 cases diagnosed as having MD--
found both MD and SS were histologically similar;
• Concluded that most cases reported as MD could be included in
SS.– thus MD became a part of SS
• Present Criterion- persistent (>3 months) symmetrical swelling of
atleast two glands:lacrimal /parotid/SM glands

• Less female predominance[2.5:1]
• Persistent but not intermittent swelling of lacrimal and
salivary glands
• 50% lack KCS, &Sialogrphy was normal• 50% lack KCS, &Sialogrphy was normal
• no anti-SS-A or SS-B antibodies
• All had elevated igg4
• Abundant plasmacytes with IgG4 are detected in the lacrimal
glands, salivary glands and lymph nodes
• frequency of apoptosis in glands of MD patients is lower
• Excellent response to steroids and rituximab

Serum IgG4 levels were significantly higher and serum IgG1 levels
were significantly lower in Mikulicz’s disease than in Sjogren’s
syndrome

Anti-IgG4 antibody staining:minor salivary glands
MD- abundant IgG4-bearing
plasmacytes infiltrating around
acinar and ductal cells
SS- no infiltrating cell
with IgG4

IgG4-associated
chronic sclerosing sialadenitis,
Küttner’s tumor

Chronic sclerosing sialadentis (Kuttner tumor)
• middle-aged to elderly patients (mean 61 years) with a slight male
predominance
• a unilateral or bilateral, largely symmetrical hard enlargement of
the submandibular salivary glands
• One fourth have other manifestations of IgG4-RSD• One fourth have other manifestations of IgG4-RSD
• Salivary functions are normal
• serum IgG4 variably elevated
Summary of Immune Mediated Sialadenitis
IgG4 related:
1. IgG4-associated sialadenitis-(Mikulicz’s disease) –
lacrimal/parotid/SM glands-symmetrical-atleast 2 , for >3
months
2. Chronic sclerosing sialadenitis[Kuttner tumor]-hard u/l or b/l2. Chronic sclerosing sialadenitis[Kuttner tumor]-hard u/l or b/l
SM gland swelling
Non IgG4
1. Sjogren
2. Lymphoma
3. Sarcoidosis

• Compared with 31 typical SS patients
• the numbers of patients with symptoms of xerostomia, xerophthalmia andarthralgia were significantly lower
• Allergic rhinitis and autoimmune pancreatitis were significantly morecommon
• Interstitial pneumonitis was significantly rarer
• Not only IgG4 but also total IgG, IgG2 and IgE levels were significantly• Not only IgG4 but also total IgG, IgG2 and IgE levels were significantlyhigher
• IgG1, IgG3, IgA and IgMlevels were significantly lower
• Lymphocytic infiltration into the ducts (formation of lymphoepitheliallesions) was rare
• good response to glucocorticoid treatment
• Suspect -IgG4+MOLPS should therefore be suspected in patients with symptoms of SS but without auto antibodies, and IgG subclasses should be examined in such patients

Effect of glucocorticoid therapy on swollen lacrimal glands.
Masaki Y et al. Ann Rheum Dis 2009;68:1310-1315

Clinical Spectrum
Other diseases

Systemic IgG4-related Lymphadenopathy
• CLINICAL PRESENTATION
• Systemic lymphadenopathy
• Lymph node are not very large (usually up to 2cm)
• Exocrine or extranodal lesions may precede,follow, or present together with the lymph node swelling
• Absence of fever
• ABNORMAL LABORATORY FINDINGS:
• Polyclonal hyperimmunoglobulinemia
• Raised serum IgG and IgE levels
• Elevation of serum soluble interleukin-2 Receptor
• Presence of autoantibodies
• Normal laboratory findings-- IL-6 level,CRP,LDH

IgG4-related lymphadenopathy
4 histologic patterns
Pattern Histological subtype
Distribution pattern of
IgG4-positive cells
1
Castleman’s disease-like
morphology Interfollicular
2 Reactive follicular hyperplasia Interfollicular2 Reactive follicular hyperplasia Interfollicular
3
Interfollicularplasmacytosis
and immunoblastosis Interfollicular
4
Progressive transformation of
germinal center-like
Intra-germinal
center
5
Inflammatory pseudotumor-like
morphology Interfollicular

Lung Disease- 4 patterns

Thyroid disease

IgG4 thyroiditis
Organ specific SystemicOrgan specific
Hashimoto’s disease subtype-more common
Systemic
Reidelsthyroiditis

Hashimoto thyroiditis -IgG4 subtype
• 10% of all patients with Hashimoto’s thyroiditis
• gland is usually larger and more fibrotic
• a recent striking enlargement with severe neckpressure symptoms –confused with malignant disease
• More males but still female predominant
• shorter disease duration of Hashimoto’s thyroiditisbefore surgery
• higher doses of L-T4 needed
• Higher serum titers of the thyroid auto-antibodiesTgAband TPOAb
• Diffuse low echogenicity [c.f. diffuse coarseechogenicity in non IgG4 thyroiditid]

Riedel’s Thyroiditis - Invasive fibrousThyroiditis
• Rare Incidence -0.06% only
• a nonpainful, rapidly growing thyroid mass
• fibroinflammatory mass extends beyond the thyroid capsule
into adjacent anatomic structures
• 1/3 rd have evidence of multifocal fibrosclerosis• 1/3 rd have evidence of multifocal fibrosclerosis

Idiopathic Retroperitoneal Fibrosis
All reported till date are male
Pancreas –mc other organ > salivary
glans>lymph node
Middle aged to elderly male
Low back pain
Obstructive renal failure
ureteral colic-like pain,
constipation, deep vein thrombosis, constipation, deep vein thrombosis,
leg edema, and scrotal swelling due
to varicocele or hydrocele
May or may not be a/w chronic
periaortitis

IgG4-related chronic periaortitis
• Abdominal > Thoracic
• 2 types
– Aneurysmal
– Nonaneurysmal–called IRPF– Nonaneurysmal–called IRPF
• Elderly > 60 years
• Rare


Idiopathic Cervical Fibrosis—latest entry
• rare tumefactive inflammatory-sclerosing lesion involving the soft
tissues of the head and neck
• Also have inflammatory fibrosclerosing lesions in other anatomic
sites
• Presents with an infiltrative, firm cervical mass• Presents with an infiltrative, firm cervical mass
American Journal of Surgical Pathology: Nov 2010,

IgG4- related Tubulo Interstitial Nephritis
• usually has tubular basement membrane (TBM) and interstitial immune complex deposits
• Affects 20-30% of AIP patients
• When to suspect-
presence of a plasma cell rich TIN in a patient with :
• renal mass / enlarged kidneys on imaging studies• renal mass / enlarged kidneys on imaging studies
• hypergammaglobulinemia,
• hypocomplementemia,
• Eosinophilia
• an extrarenal inflammatory mass
• sialadenitis, lymphadenopathy,
• patchy lesion distribution
Anti-PLA2R autoantibodies in serum and
Immunoglobulin subclass in glomerular deposits– IgG4

Myasthenia gravis-MuSK antibodies
• Nowadays ,2 clinicopathologic MG subsets recognised:
1. AChR-MG-IgG1 and IgG3 subclass antibodies
2. MuSK-MG-Antibodies of igg4 subclass to muscle-specific
tyrosine kinase (MuSK)

Take home messages
• IgG4- monovalent, bispecific,antiinflammatory
• Most common presentation- AIP- mimics CA pancreas
• Knowledge of Full spectrum still evolving
• Suspect IgG4 rsd:
• All unexplained tumorous swelling –
• Any Fibrosclerosing lesion-
• Any steroid responsive mass lesion-
• All males with SS,negative autoantibodies
• Generalized lymphadenopathy without constitutional
symptoms

Take home messages
• Once diagnosed in one organ Search actively for e/o other
organ involvement
• Take histories of asthma, eczema, or atopy
• Risk of Lymphoma transformation –only case reports-not
proved
• Elevated serum IgG4 concentrations are neither necessary nor• Elevated serum IgG4 concentrations are neither necessary nor
sufficient for the diagnosis of IgG4-RSDbut when present are
helpful in suggesting the diagnosis
• gold standard for the diagnosis-identification of typical
histopathological features, including the presence of
numerous IgG4þ plasma cells within affected tissue

Suggested readings

IgG4RSD-reminds of Elephant and 5
blind men

Thank you Thank you