ihi expedition 6 sli… · ihi expedition expedition: ... demonstrate examples of how to engage...
TRANSCRIPT
6/1/2015
1
IHI ExpeditionExpedition: Preparing Care Teams for Bundled Payments
Session 6: Case Study - CMS Bundled Payments for Care Improvement Experience
June 2, 2015
Begins at 1:00 PM
Evan Benjamin, MD, FACPStephanie Calcasola, MSN, RN-BCJan Mayforth, CPADouglas Salvador, MD, MPHMolly Bogan, MA
Today’s Host2
Akiera GilbertProject Office Assistant
Institute for Healthcare Improvement

6/1/2015
2
Phone Connection (Preferred)3
To join by phone:
1) Click on the
“Participants” and
“Chat” icons in the top
right hand side of your
screen.
2) Click the
button on the right hand
side of the screen.
3) A pop-up box will
appear with the option
“I will call in.” Click that
option.
4) Please dial the phone
number, the event
number and your
attendee ID to connect
correctly .
WebEx Quick Reference
• Please use chat to
“All Participants”
for questions
• For technology
issues only,
please chat to
“Host”
4
Enter Text
Select Chat recipient
Raise your hand
6/1/2015
3
5
Chat
5
Name and the Organization you represent
Example: Sam Jones, Midwest Health
Please send your message to All Participants
Expedition Director6
Molly Bogan, MA
Director
Institute for Healthcare Improvement
6/1/2015
4
Expedition Objectives
At the end of this Expedition, participants will be able to:
Describe the benefit of transitioning to a value-based purchasing model
Understand and apply activity-based cost accounting methodology to at least
one care process
Demonstrate examples of how to engage stakeholders in building a bundle
Describe how to customize care team redesign to deliver optimum care
under value-based purchasing
7
Today’s Agenda8
Introductions
Session 5 Action Period Assignment Debrief
Case Study: CMS Bundled Payments for Care
Improvement Experience
Action Period Assignment
Closing
6/1/2015
5
Expedition Sessions
Session 1: Volume to Value; Describe the benefit of transitioning Value- Based Purchasing
Lead Faculty: Lucy Savitz & Trisha Frick
Session 2: Getting Started with Building a Care Bundle
Lead Faculty: Trisha Frick & Nick Bassett
Session 3: Collecting Data Using Activity-based Costing
Lead Faculty: Nick Bassett & Lucy Savitz
Session 4: Engaging Stakeholders in Bundle Design
Lead Faculty: Trisha Frick & Nick Bassett
Session 5: Care Team Redesign
Lead Faculty: Trisha Frick & Nick Bassett
Session 6: Case Study: CMS Bundled Payments for Care Improvement Experience
Lead Faculty: Stephanie Calcasola, Evan Benjamin, Jan Mayfort and Doug Salvador
9
Action Period Assignment Debrief10
• Build an outline for designing optimum care team end-to-end based
on data collected in sessions 1, 2, 3 & 4.
Share with others using the chat to All Participants
6/1/2015
6
11
Chat
Please chat in one change to your care
team that you identified.
Please send your message to All Participants
Faculty12
Evan Benjamin,
MD, FACP
Senior Vice
President/Chief
Quality Officer for
Baystate Health
Springfield, MA
Stephanie Calcasola,
MSN, RN-BC
Director of Quality and
Medical Management
Baystate Medical Center
Springfield, MA
Doug Salvador,
MD, MPH,
Vice President of
Medical Affairs
Baystate Medical
Center
Springfield, MA
Jan Mayforth, CPA
Director, Clinical
Financial Planning
and Decision
Support
Baystate Health
Springfield, MA
6/1/2015
7
Baystate Medical Center’s Experience with Bundled Payments
Institute of Healthcare Improvement
June 2nd 2015Evan Benjamin, MD, FACP
Stephanie Calcasola, MSN, RN-BC
Jan Mayforth, CPA
Douglas Salvador, MD, MPH
6/1/2015
8
Award Recognitions
2013
Why Do Bundle Payments?

6/1/2015
9
What is a Bundle
● An integrated model to deliver to patients, families, referring physicians and payers substantially improved quality and value for a defined set of health care services by:
Redesign of complex systems to embed evidence based best practices reliably;
everyday patient flow => better outcomes cheaper
Activating patients and families to be engaged in the care processes;
Aligning the interests of the patient, provider, payor and purchaser.
6/1/2015
10
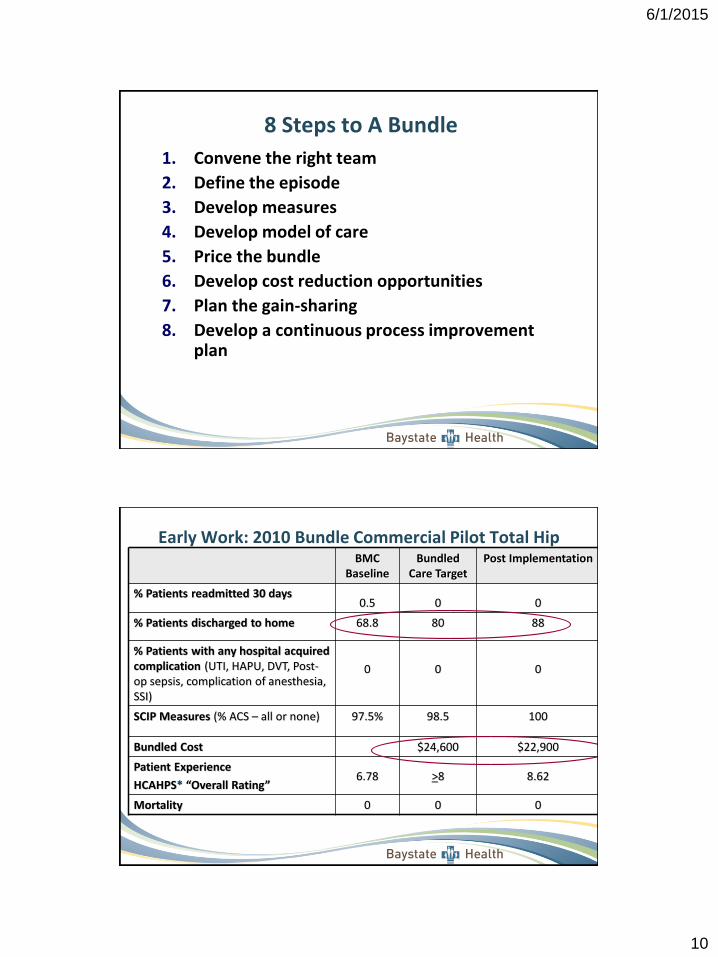
8 Steps to A Bundle
1. Convene the right team
2. Define the episode
3. Develop measures
4. Develop model of care
5. Price the bundle
6. Develop cost reduction opportunities
7. Plan the gain-sharing
8. Develop a continuous process improvement plan
BMC Baseline
Bundled Care Target
Post Implementation
% Patients readmitted 30 days0.5 0 0
% Patients discharged to home 68.8 80 88
% Patients with any hospital acquired complication (UTI, HAPU, DVT, Post-op sepsis, complication of anesthesia, SSI)
0 0 0
SCIP Measures (% ACS – all or none) 97.5% 98.5 100
Bundled Cost $24,600 $22,900
Patient Experience
HCAHPS* “Overall Rating”6.78 >8 8.62
Mortality 0 0 0
Early Work: 2010 Bundle Commercial Pilot Total Hip
6/1/2015
11
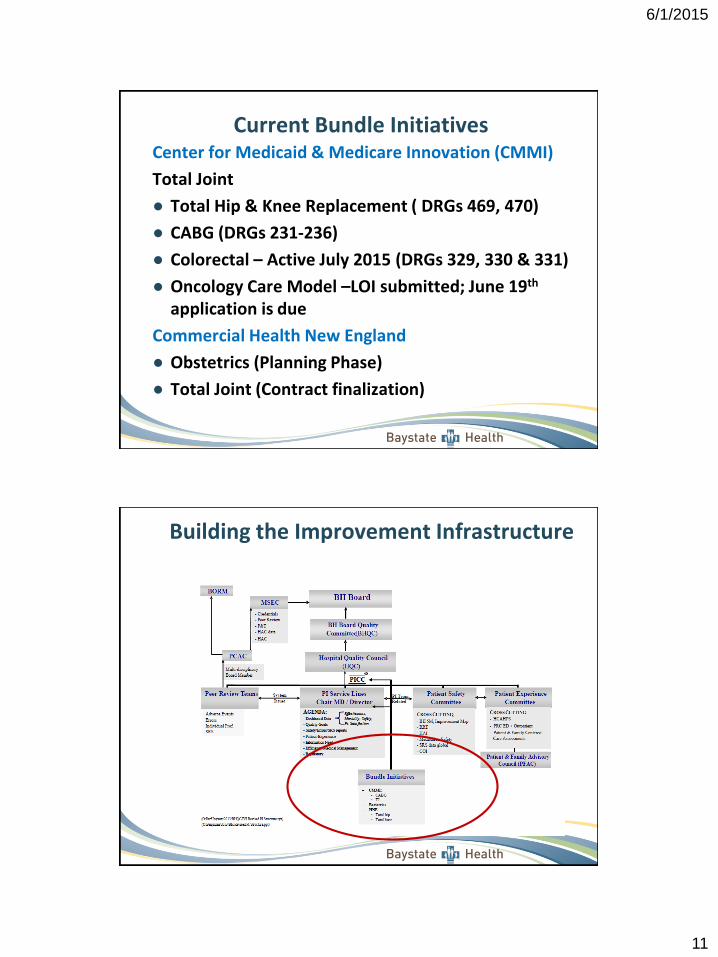
Current Bundle InitiativesCenter for Medicaid & Medicare Innovation (CMMI)
Total Joint
● Total Hip & Knee Replacement ( DRGs 469, 470)
● CABG (DRGs 231-236)
● Colorectal – Active July 2015 (DRGs 329, 330 & 331)
● Oncology Care Model –LOI submitted; June 19th
application is due
Commercial Health New England
● Obstetrics (Planning Phase)
● Total Joint (Contract finalization)
Building the Improvement Infrastructure
6/1/2015
12
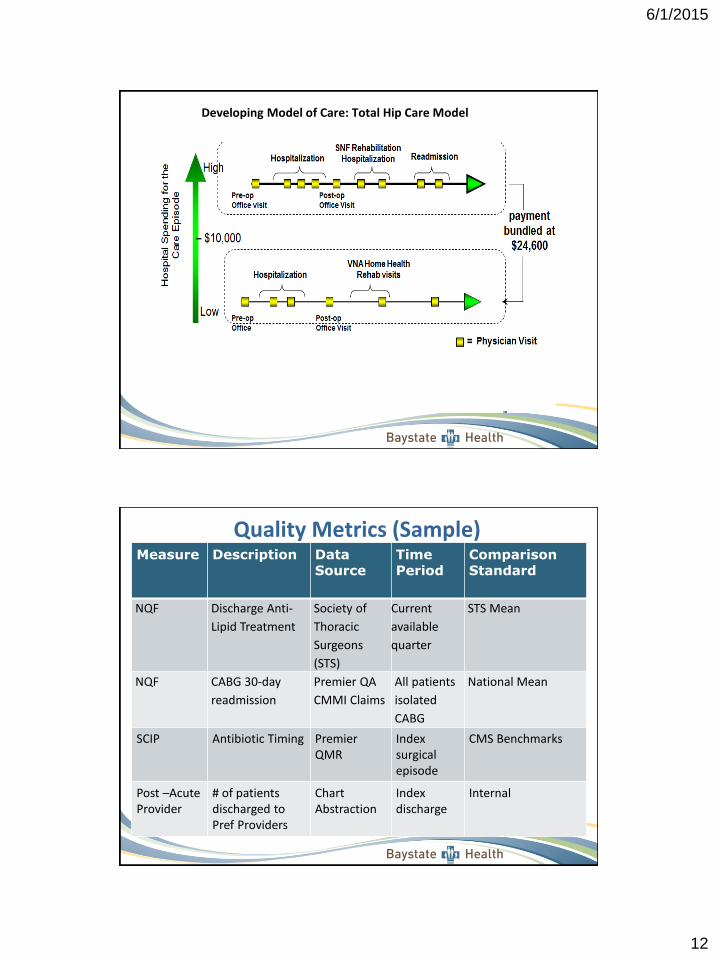
Developing Model of Care: Total Hip Care Model
Measure Description Data Source
Time Period
Comparison Standard
NQF Discharge Anti-
Lipid Treatment
Society of
Thoracic
Surgeons
(STS)
Current
available
quarter
STS Mean
NQF CABG 30-day
readmission
Premier QA
CMMI Claims
All patients
isolated
CABG
National Mean
SCIP Antibiotic Timing PremierQMR
Indexsurgical episode
CMS Benchmarks
Post –Acute Provider
# of patients discharged to Pref Providers
ChartAbstraction
Index discharge
Internal
Quality Metrics (Sample)
6/1/2015
13
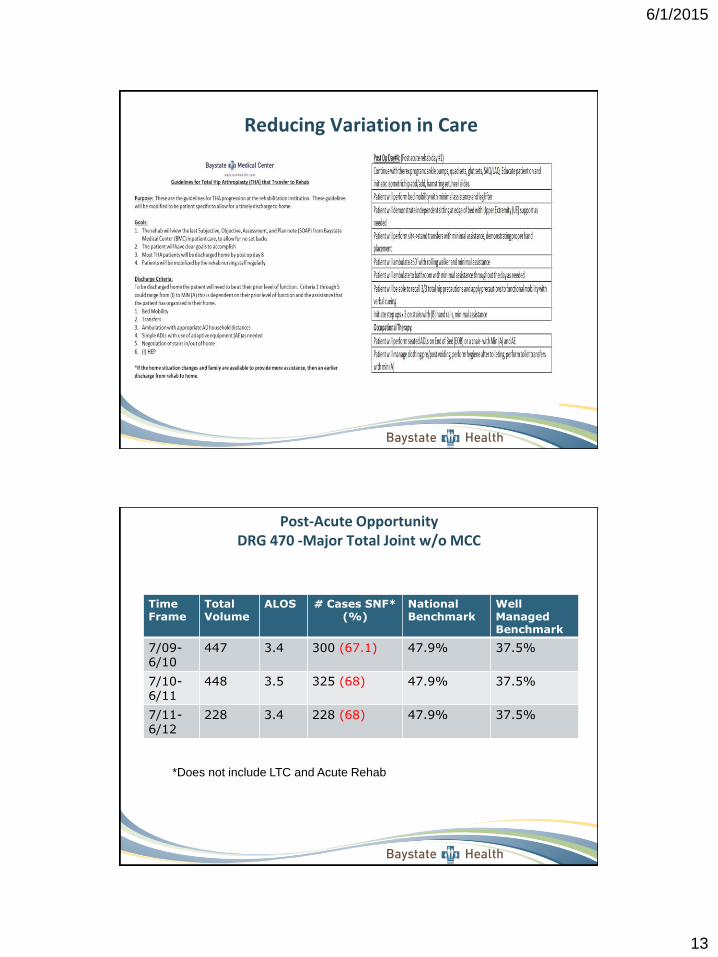
Reducing Variation in Care
Post-Acute OpportunityDRG 470 -Major Total Joint w/o MCC
Time Frame
TotalVolume
ALOS # Cases SNF* (%)
National Benchmark
Well ManagedBenchmark
7/09-6/10
447 3.4 300 (67.1) 47.9% 37.5%
7/10-6/11
448 3.5 325 (68) 47.9% 37.5%
7/11-6/12
228 3.4 228 (68) 47.9% 37.5%
*Does not include LTC and Acute Rehab
6/1/2015
14
Post-Acute Model Redesign
Post-Acute Work Summary
BH Strategic Post-Acute Care Committee
Post-Acute Preferred Partnerships
Bundle Navigator Role
Post-Acute Care Oversight Work Group
Transitions in Care/Cross Continuum Collaboration/Readmission Prevention
Goals of Strategic Partnerships
BH Strategic Post-Acute Care Committee
● Creating the overarching strategy for Post-acute care (PAC) for the BH hospitals
● Providing a single point of decision making around PAC relationships
● Assuring that the strategy is consistent with other BH approaches to PAC
● Creating a Preferred Provider Partnership Network
6/1/2015
15
Post-Acute Preferred PartnershipsQuality and Operational Performance
Collaborative Partner Facility Profiles
● Facility demographics
● Quality performance (star rating, readmissions, falls, etc.)
● Provider model
● Services (dietitian, rehab, 24/7 access)
● Citizenship
● Patient satisfaction
● Staffing
● Professional Development (certification)
● Environment aesthetics
Bundle Navigator Role
● Provide oversight of care coordination and quality monitoring working in partnership with case management, post-acute partnerships.
● Work to develop and ensure streamlined operations, patient satisfaction and care navigation in the episodes of care bundle model.
● Knowledge around national best practice standards, transitions of care, regulatory rules and requirements for post-acute care; skilled in improvement methods and project management; proficient in data management (excel, access, database mining)
6/1/2015
16
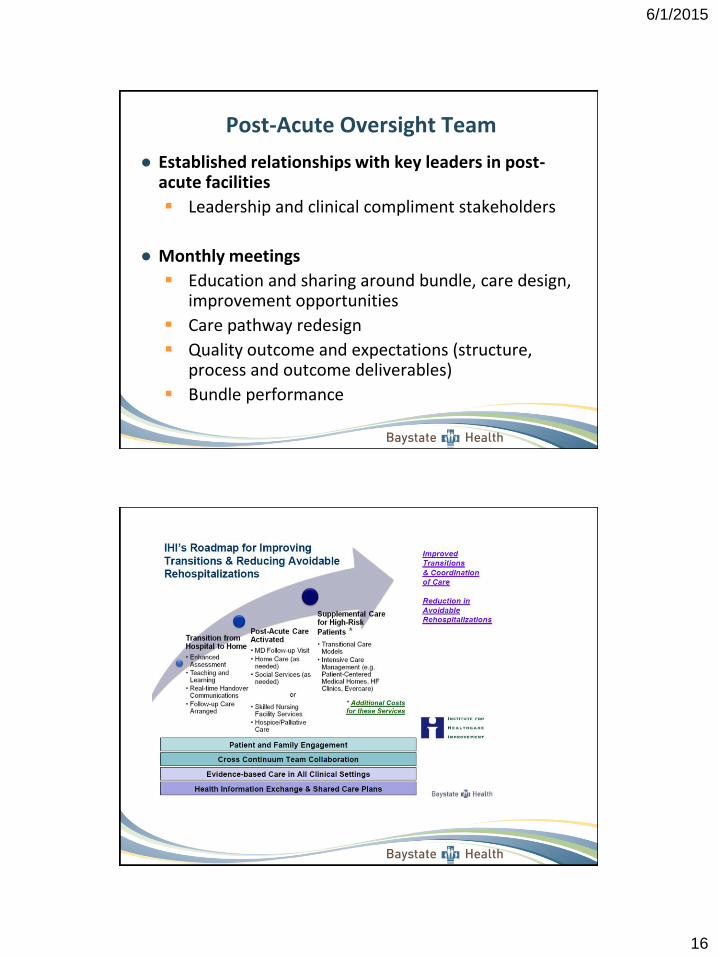
Post-Acute Oversight Team
● Established relationships with key leaders in post-acute facilities
Leadership and clinical compliment stakeholders
● Monthly meetings
Education and sharing around bundle, care design, improvement opportunities
Care pathway redesign
Quality outcome and expectations (structure, process and outcome deliverables)
Bundle performance
6/1/2015
17
Transitions in Care
● Risk screening on index admission
● Targeted intervention for high risk patients
● Standardized education tools
● Medication reconciliation
● Follow up phone calls
● Appointments made before discharge
● Active cross continuum teams
● Automated readmission notification EMR
● PAC Performance Improvement Teams
● Savings from 2 sources
Over entire bundle episode – savings would accrue 100% to insurer without gainsharing arrangement
• Based on reducing cost through better management of in-hospital services billed outside the DRG (MD consultations), reduced readmissions and reduction in post-acute services (both % of patient receiving service and cost of services received)
Costs incurred while patient is in hospital – savings would accrue to hospital without a gainsharing arrangement
● Use benchmarking to identify areas of opportunity
Premier Bundled Payment Collaborative provided benchmarks on readmissions and post-acute services
Premier Quality Advisor – DRG LOS and Cost benchmarks
Internal data from decision support system – comparisons between providers and service item level detail comparisons.
Determine Opportunities for Cost Savings
6/1/2015
18
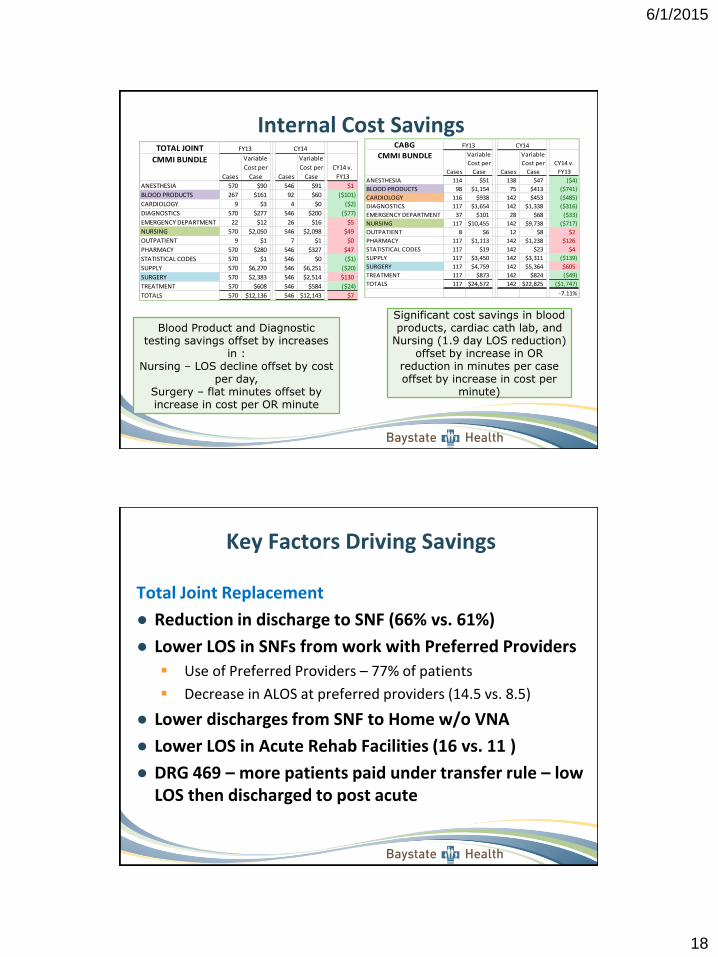
Internal Cost SavingsTOTAL JOINT
CMMI BUNDLE
Cases
Variable
Cost per
Case Cases
Variable
Cost per
Case
CY14 v.
FY13
ANESTHESIA 570 $90 546 $91 $1
BLOOD PRODUCTS 267 $161 92 $60 ($101)
CARDIOLOGY 9 $3 4 $0 ($2)
DIAGNOSTICS 570 $277 546 $200 ($77)
EMERGENCY DEPARTMENT 22 $12 26 $16 $5
NURSING 570 $2,050 546 $2,098 $49
OUTPATIENT 9 $1 7 $1 $0
PHARMACY 570 $280 546 $327 $47
STATISTICAL CODES 570 $1 546 $0 ($1)
SUPPLY 570 $6,270 546 $6,251 ($20)
SURGERY 570 $2,383 546 $2,514 $130
TREATMENT 570 $608 546 $584 ($24)
TOTALS 570 $12,136 546 $12,143 $7
CY14FY13 CABG
CMMI BUNDLE
Cases
Variable
Cost per
Case Cases
Variable
Cost per
Case
CY14 v.
FY13
ANESTHESIA 114 $51 138 $47 ($4)
BLOOD PRODUCTS 98 $1,154 75 $413 ($741)
CARDIOLOGY 116 $938 142 $453 ($485)
DIAGNOSTICS 117 $1,654 142 $1,338 ($316)
EMERGENCY DEPARTMENT 37 $101 28 $68 ($33)
NURSING 117 $10,455 142 $9,738 ($717)
OUTPATIENT 8 $6 12 $8 $2
PHARMACY 117 $1,113 142 $1,238 $126
STATISTICAL CODES 117 $19 142 $23 $4
SUPPLY 117 $3,450 142 $3,311 ($139)
SURGERY 117 $4,759 142 $5,364 $605
TREATMENT 117 $873 142 $824 ($49)
TOTALS 117 $24,572 142 $22,825 ($1,747)
-7.11%
CY14FY13
Blood Product and Diagnostic testing savings offset by increases
in :Nursing – LOS decline offset by cost
per day, Surgery – flat minutes offset by increase in cost per OR minute
Significant cost savings in blood products, cardiac cath lab, and
Nursing (1.9 day LOS reduction) offset by increase in OR
reduction in minutes per case offset by increase in cost per
minute)
Key Factors Driving Savings
Total Joint Replacement
● Reduction in discharge to SNF (66% vs. 61%)
● Lower LOS in SNFs from work with Preferred Providers
Use of Preferred Providers – 77% of patients
Decrease in ALOS at preferred providers (14.5 vs. 8.5)
● Lower discharges from SNF to Home w/o VNA
● Lower LOS in Acute Rehab Facilities (16 vs. 11 )
● DRG 469 – more patients paid under transfer rule – low LOS then discharged to post acute
6/1/2015
19
● Must have waiver from CMMI/CMS
● Must include quality measures at MD level – no gainsharing if quality targets not met, considered at individual provider level
● Minimum number of cases – don’t want to reward non-participating MDs
● Net Payment Reconciliation Amounts (NPRA) from CMS Amount saved in excess of the 2% discount
Next 2% kept by Awardee hospital to recoup amount withheld by CMS
Savings in excess of 2% contributed to gainsharing pool
● Internal Cost Savings – Hospital cost savings identified using internal cost accounting system.
● Commercial bundle shared all savings with MDs
Lessons Learned Around Gain Sharing
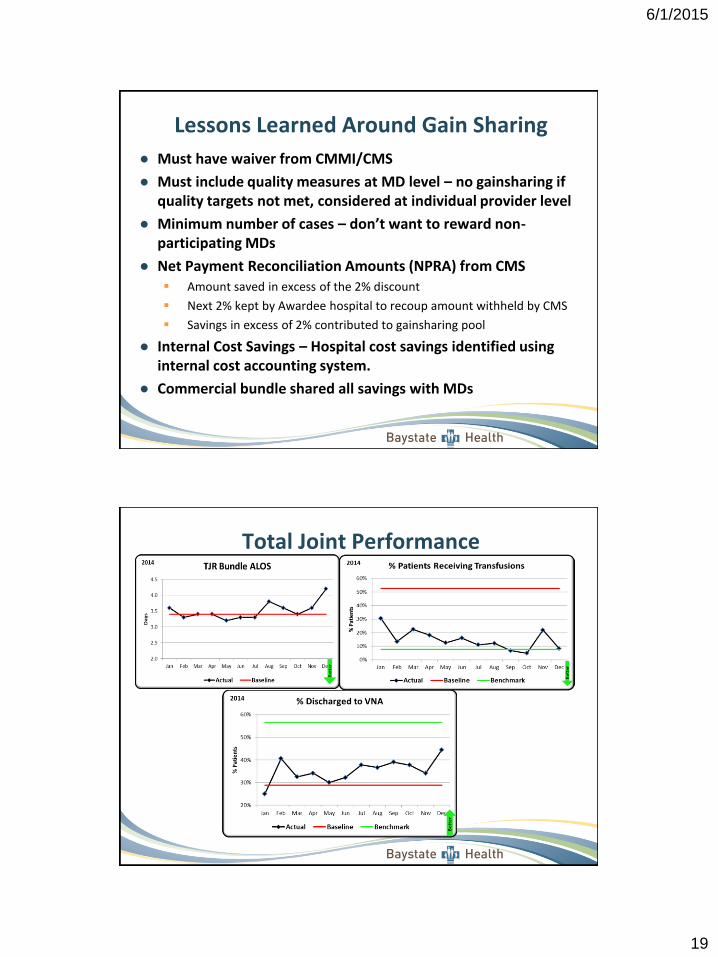
Total Joint PerformanceCMMI Total Joint Replacement Bundle
CY 2014
6/1/2015
20
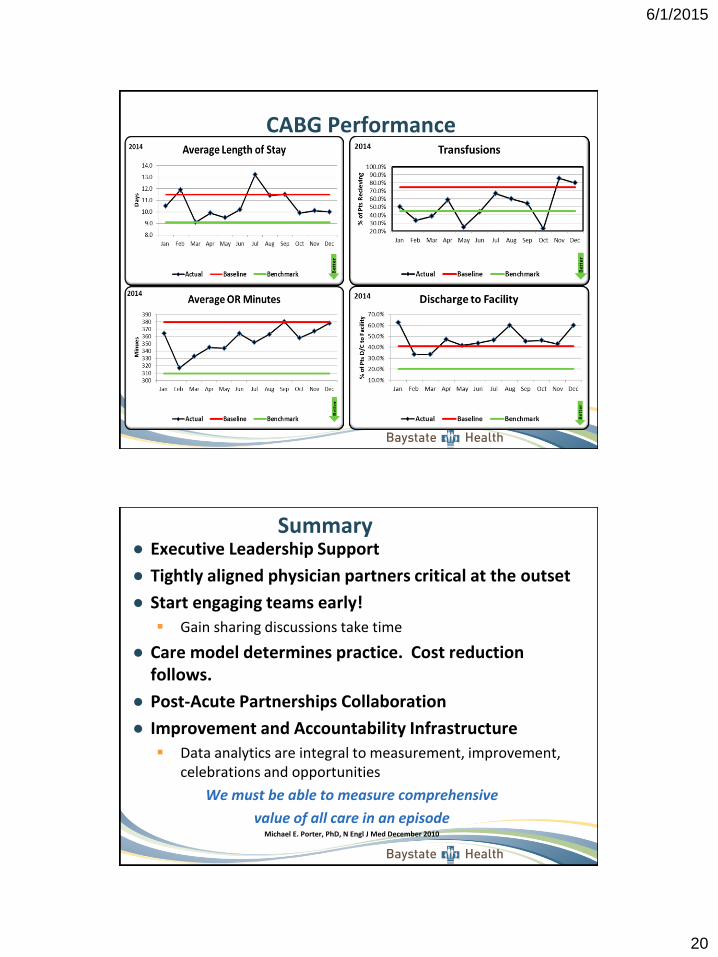
CABG Performance
● Executive Leadership Support
● Tightly aligned physician partners critical at the outset
● Start engaging teams early!
Gain sharing discussions take time
● Care model determines practice. Cost reduction follows.
● Post-Acute Partnerships Collaboration
● Improvement and Accountability Infrastructure
Data analytics are integral to measurement, improvement, celebrations and opportunities
We must be able to measure comprehensive
value of all care in an episode Michael E. Porter, PhD, N Engl J Med December 2010
Summary
6/1/2015
21
Questions/Discussion41
Raise your hand
Use the chat
Action Period Assignment
Take the learning from today’s case study
and test the design from Session 5’s action
period with focus group from your care team
Complete end of program survey – link will
be emailed
Look for the final resources list and
summary slides to be shared on the listserv
6/1/2015
22
Expedition Communications
• All sessions are recorded
• Materials are sent one day in advance
• Listserv address for session communications:
• To add colleagues, email us at [email protected]
43
Thank You!
44
Director: Molly Bogan
Akiera Gilbert
Please let us know if you have any questions or
feedback following today’s Expedition webinar.