ihi open school global chapter webinar: strengthening your ... os... · ihi open school global...
TRANSCRIPT
IHI Open School Global Chapter Webinar: Strengthening Your QI KnowledgeDon Goldmann, MD
Faheem Ahmed, MD
Kirsty McNeil
October 24, 2016
WebEx Quick Reference
• Welcome to today’s session!
• Please use chat to “All
Participants” for questions
• For technology issues only,
please chat to “Host”
• WebEx Technical Support:
866-569-3239
• Dial-in Info: Communicate /
Join Teleconference (in
menu)
Raise your hand
Select Chat recipient
Enter Text
Type into the chat box:
Select “All Participants” as the recipient
1. Name
2. Chapter Name
(University/Organization)
3. How long have you been involved with
your Chapter?
4. Are you a new Chapter?
5. What are you hoping to learn on
today’s call?
Select Chat recipient
Enter Text
Today’s Agenda
Welcome and Introductions
IHI Open School Overview
Tips for getting your Chapter involved in QI work
Back to the Basics: How to apply QI
Questions/Discussion
IHI Open School Announcements
Introductions – Facilitators and Presenters
Kirsty McNeil, UK & Ireland
Regional Leader
Gina Deitz, Community
Manager, IHI Open School
Faheem Ahmed, UK & Ireland
Regional Leader
Introductions – Facilitators and Presenters
Don Goldmann, MD
Chief Scientific and Medical Officer, IHI

Open School
IHI Open School Mission“Advance health care improvement and patient safety
competencies in the next generation of health professionals worldwide.”

• 32+ online courses developed by world-
renowned experts in the following topics:
• Improvement Capability
• Patient Safety
• Person- and Family-Centered Care
• Triple Aim for Populations
• Leadership
• Set of GME courses
• More than 2.9 million courses completed
• More than 400,000 learners have completed a
course
• More than 94,000 learners have earned the
Certificate
• More than 1,000 universities and health care
organizations using the courses
IHI Open School Courses
3 Levels of Learning
100-level courses:
Introductory concepts for all health care audiences
200-level courses:
Intermediate concepts and specialized topic areas
300-level courses:
Project-based learning
Basic Certificate in Quality & Safety
• 94,000+ Certificates earned
• Formal recognition for
participation
• Proves commitment to
employers
• Required by many university
& GME faculty
• Requires completion of 13
courses
IHI Open School Video Library
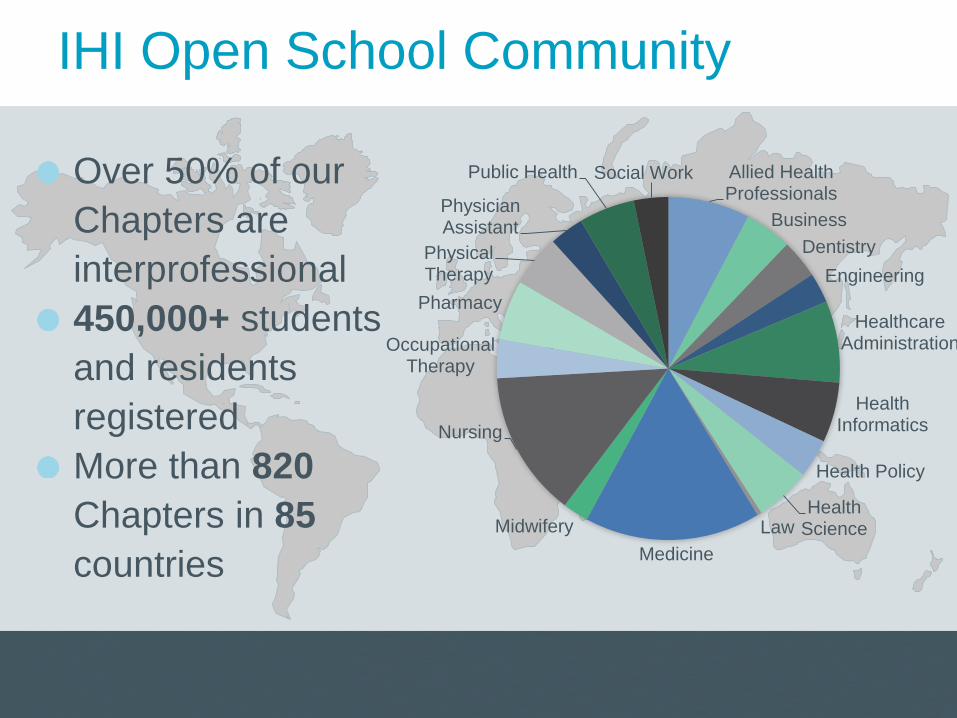
IHI Open School Community
Over 50% of our
Chapters are
interprofessional
450,000+ students
and residents
registered
More than 820
Chapters in 85
countries
Allied Health Professionals
Business
Dentistry
Engineering
Healthcare Administration
Health Informatics
Health Policy
Health ScienceLaw
Medicine
Midwifery
Nursing
Occupational Therapy
Pharmacy
Physical Therapy
Physician Assistant
Public Health Social Work
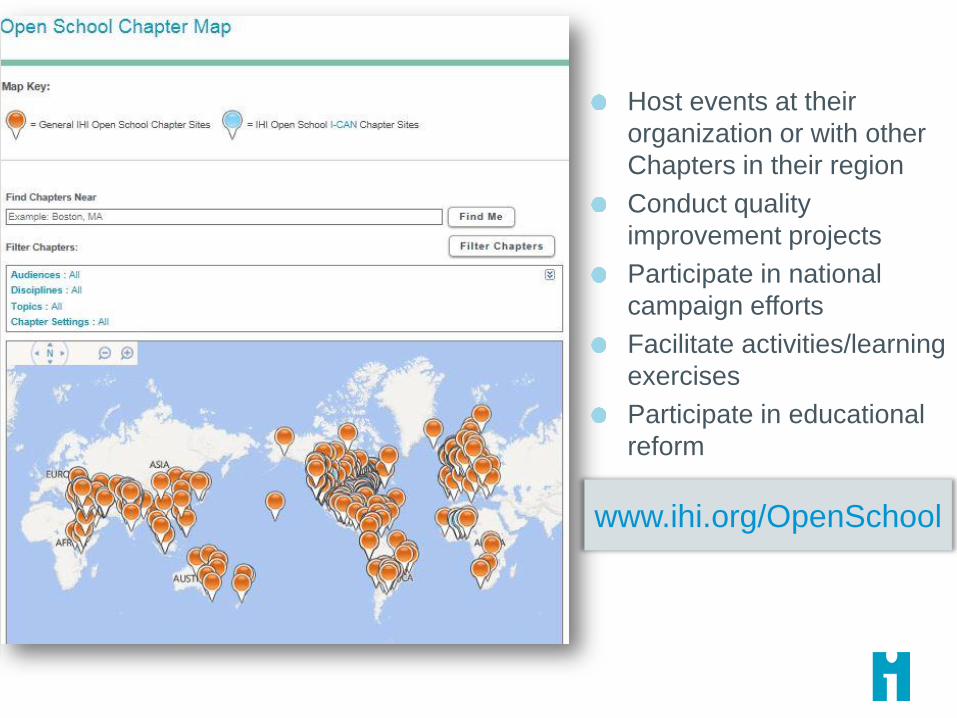
www.ihi.org/OpenSchool
Host events at their
organization or with other
Chapters in their region
Conduct quality
improvement projects
Participate in national
campaign efforts
Facilitate activities/learning
exercises
Participate in educational
reform
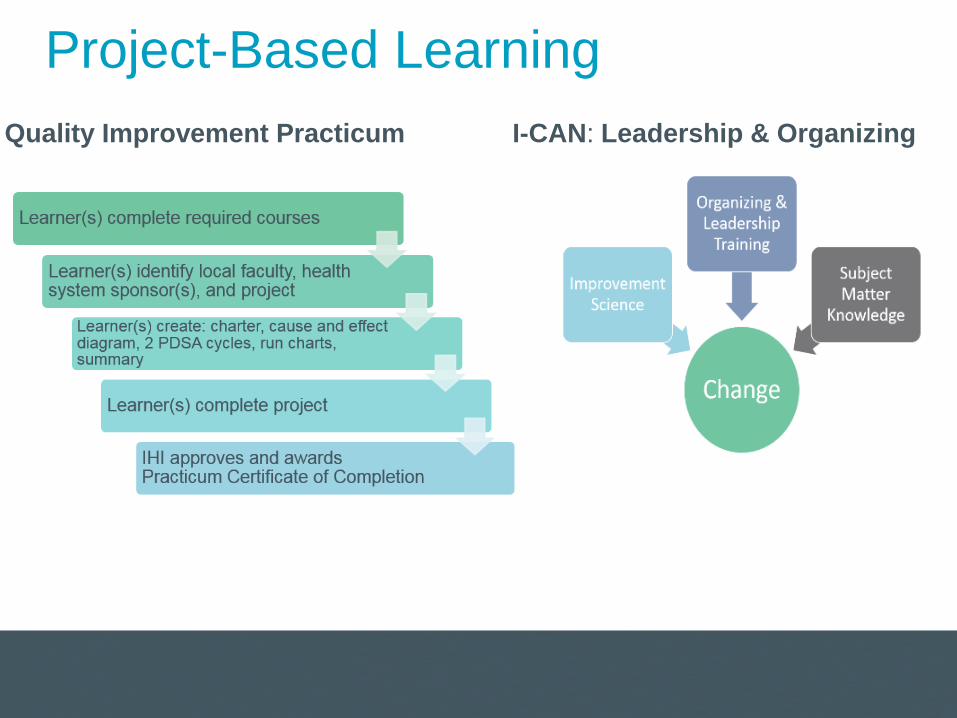
Project-Based Learning
I-CAN: Leadership & Organizing Quality Improvement Practicum
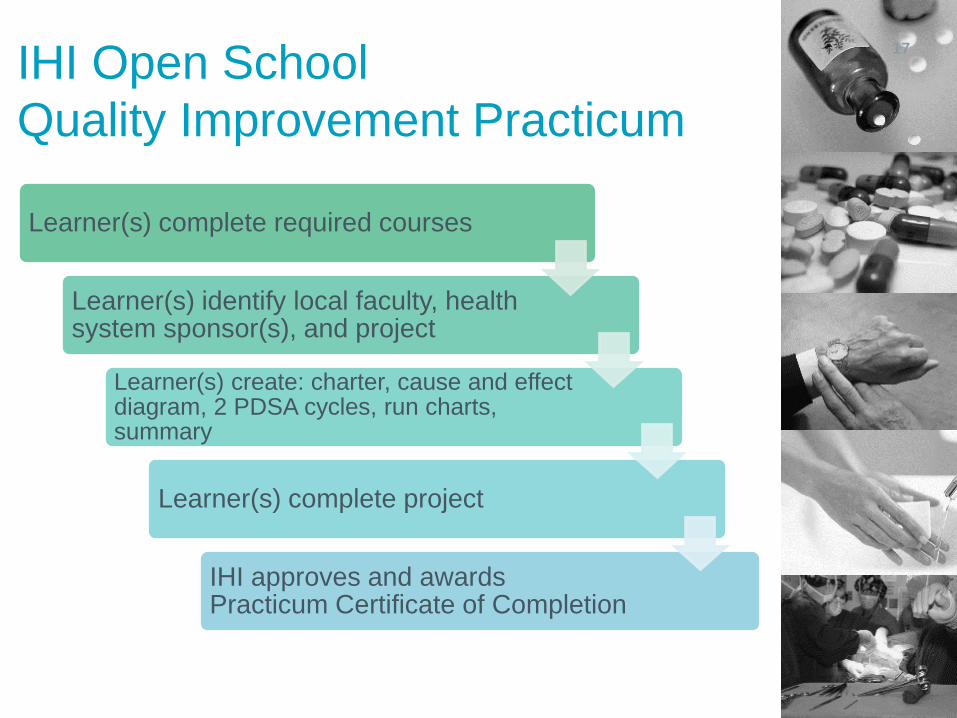
IHI Open School
Quality Improvement Practicum
Learner(s) complete required courses
Learner(s) identify local faculty, health system sponsor(s), and project
Learner(s) create: charter, cause and effect diagram, 2 PDSA cycles, run charts, summary
Learner(s) complete project
IHI approves and awards Practicum Certificate of Completion
17
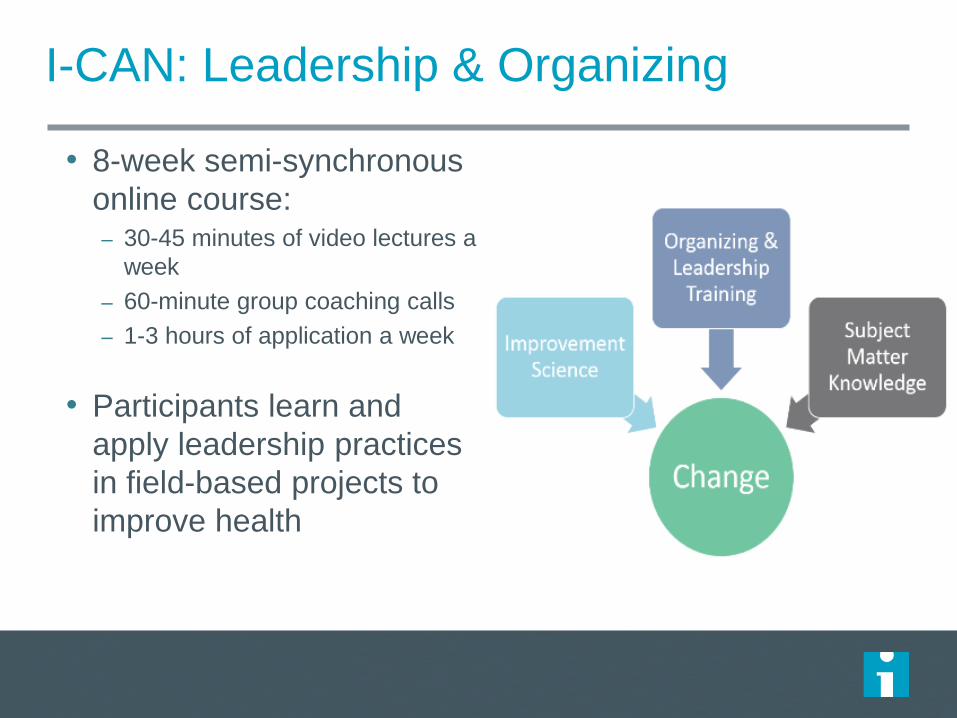
I-CAN: Leadership & Organizing
• 8-week semi-synchronous
online course:– 30-45 minutes of video lectures a
week
– 60-minute group coaching calls
– 1-3 hours of application a week
• Participants learn and
apply leadership practices
in field-based projects to
improve health
Tips for getting your Chapter involved in Quality Improvement work in your local setting
Team
Planning
Skills
Support
Projects
Projects Identify potential projects in your area
Are there projects already set up that your Chapter can get involved in?
Have the teams within your local setting identified any potential projects?
Construct a QI team
Identify members for your QI team Get “buy-in” Students as change agents
Team
Plan your QI project carefully
Set clear aims, objectives and measures Set “SMART” goals: Specific, Measurable,
Achievable, Realistic and Timely
Planning
Ensure Chapter members know who they can go to for support
Chapter Leaders/ Faculty/ Regional leaders/ Other Chapters
Share your experience to help support and learn from others
Support
Ensure members of your Chapter have the skills to carry out their own QI projects
Online IHI Open School modules Chapter workshops Teach
Skills
Practical, Scientific Methods for Improving Health, Healthcare, and Your Life
Don Goldmann, MD
Chief Medical and Scientific Officer
Institute for Healthcare Improvement
Clinical Professor of Pediatrics
Harvard Medical School
@DAGoldmann
October 24, 2016
IHI Open School Global Chapter Call
My Personal Take on the “Science of
Improvement”
• Scientific regardless of name:– Science of improvement
– Health care delivery science
– Implementation science
– Systems strengthening
– Systems engineering
• Scientific methods include– “Model for Improvement” promulgated by IHI
– Lean
– Six Sigma
– Lean Six Sigma – DMAIC (Design, Measure, Analyze, Improve and Control)
– Value stream maps
• And it can be explained in under 7 minutes, so here goes!
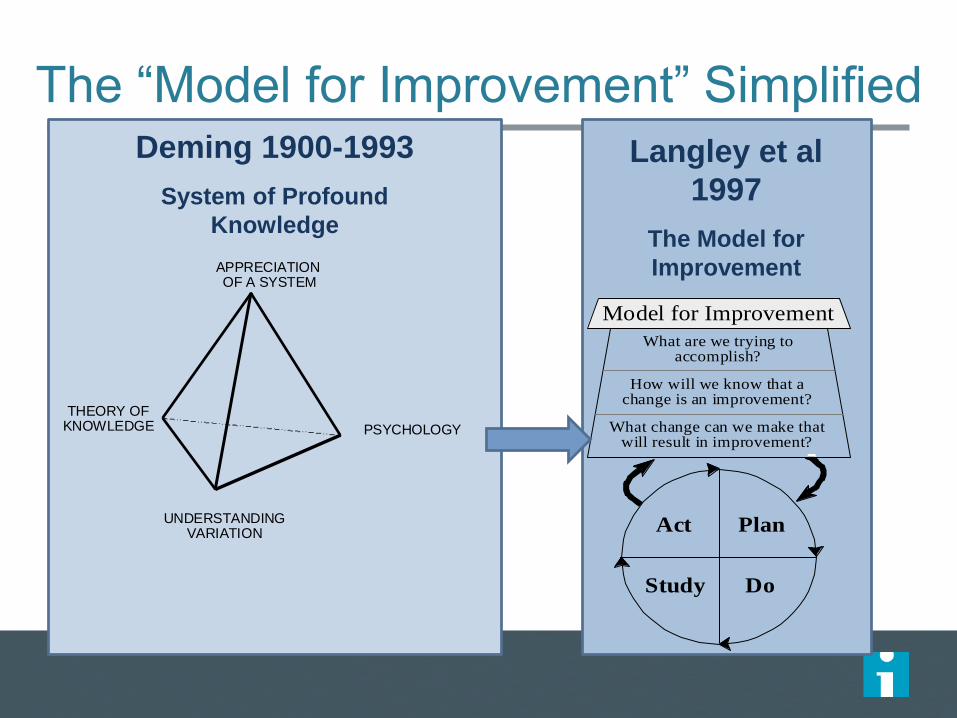
The “Model for Improvement” Simplified
APPRECIATION OF A SYSTEM
PSYCHOLOGY
UNDERSTANDINGVARIATION
THEORY OFKNOWLEDGE
Deming 1900-1993
System of Profound
Knowledge
What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Model for Improvement
PlanAct
DoStudy
Langley et al
1997
The Model for
Improvement
In Summary
• Specify a clear, measurable aim and state when you hope to achieve it (“how much by when”)
• Understand the system in which you are trying to reach your goal –precisely where it can fail, where there is inefficiency and waste, and where it needs to be improved and monitored
• Be clear about the expected (predicted) impact of the changes you are testing on the outcomes you want to achieve
• Be clear about your implementation plan and the expected outputs of your planned activities
• Learn continuously from testing (experimentation) to determine if the changes you predict will lead to improvement actually do lead to improvement
• Use data to track improvement over time to see if you actually are getting closer to achieving your aim
• Understand how to change human behavior (for example, through behavioral economics)
Why Research Scientists and Academics
Should be Comfortable With These Methods
• My ten years working with a PhD scientist to
develop a staph vaccine…..
‒ Mice, PDSAs, and laboratory culture
Personal Journey
Personal Improvement Projects
• Sometimes the system needs major change, not
tinkering
– “Watching the tele… A nightmare without end”
• PDSA tests made simple – how to grow cucumbers
Personal Improvement Projects
• Sometimes the system needs major change, not
tinkering
– “Watching the tele…”
• PDSA tests made simple – how to grow cucumbers
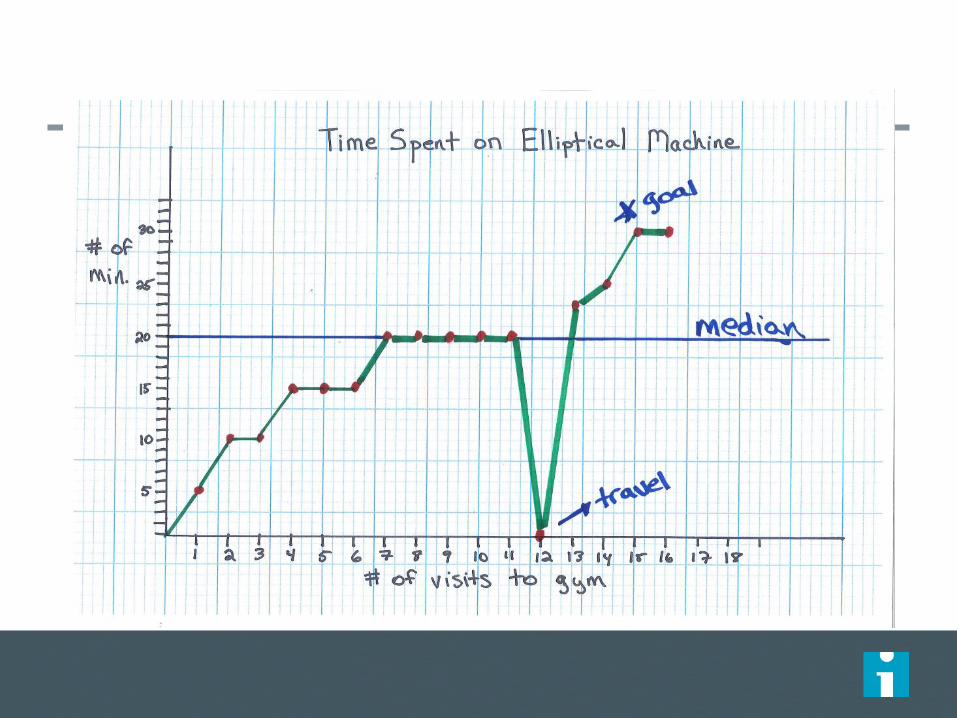
• Aerobic exercise at the gym
– 20 minutes on the elliptical and level 10 at least two times per
week
– “balancing measure” – completion of free weights and machine
routine
Be Clear about Cause and Effect
• We must have a theory, or prediction, that the change(s)
we are testing and implementing will have a impact on
the outcome we are trying to improve
• “Driver diagrams” are very useful in displaying your
theory of cause and effect
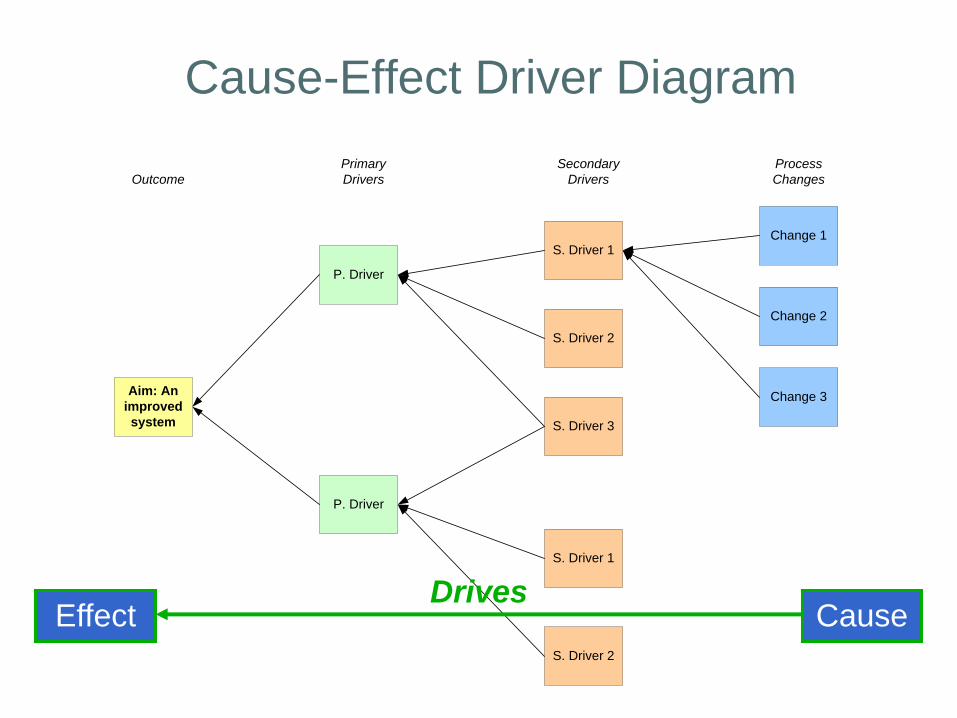
Cause-Effect Driver Diagram
Primary
DriversOutcome
Secondary
Drivers
Process
Changes
Aim: An
improved
system
P. Driver
S. Driver 1Change 1
P. Driver
S. Driver 2
S. Driver 3
S. Driver 1
S. Driver 2
Change 2
Change 3
CauseEffectDrives
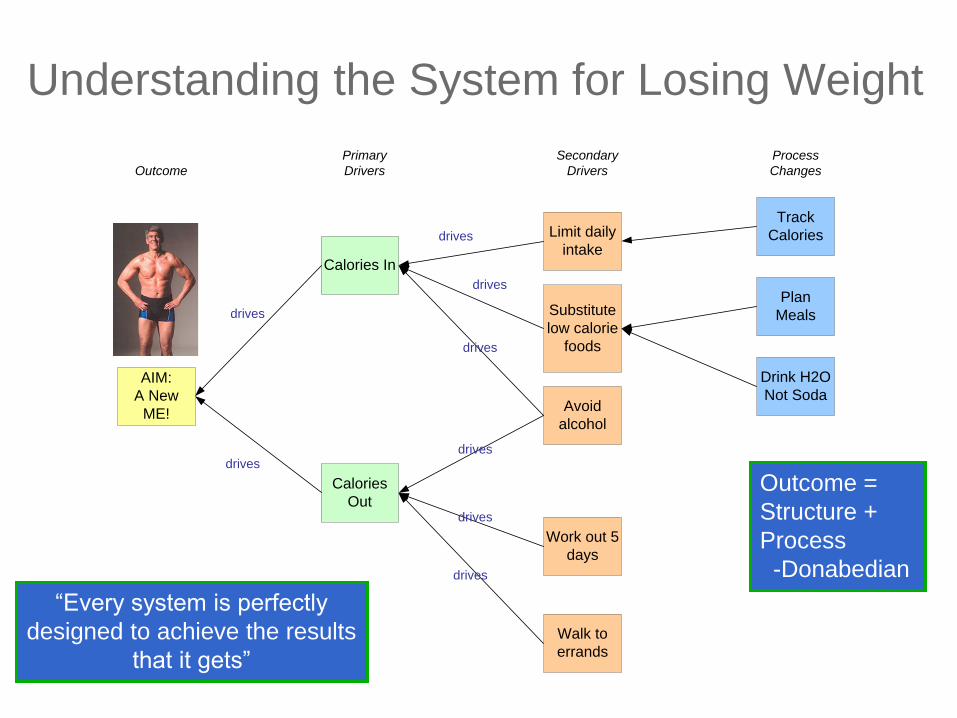
Primary
DriversOutcome
Secondary
Drivers
Process
Changes
AIM:
A New
ME!
Calories In
Limit daily
intake
Track
Calories
Calories
Out
Substitute
low calorie
foods
Avoid
alcohol
Work out 5
days
Walk to
errands
Plan
Meals
Drink H2O
Not Soda
drives
drives
drives
drives
drives
drives
drives
drives
Understanding the System for Losing Weight
“Every system is perfectly
designed to achieve the results
that it gets”
Outcome =
Structure +
Process
-Donabedian
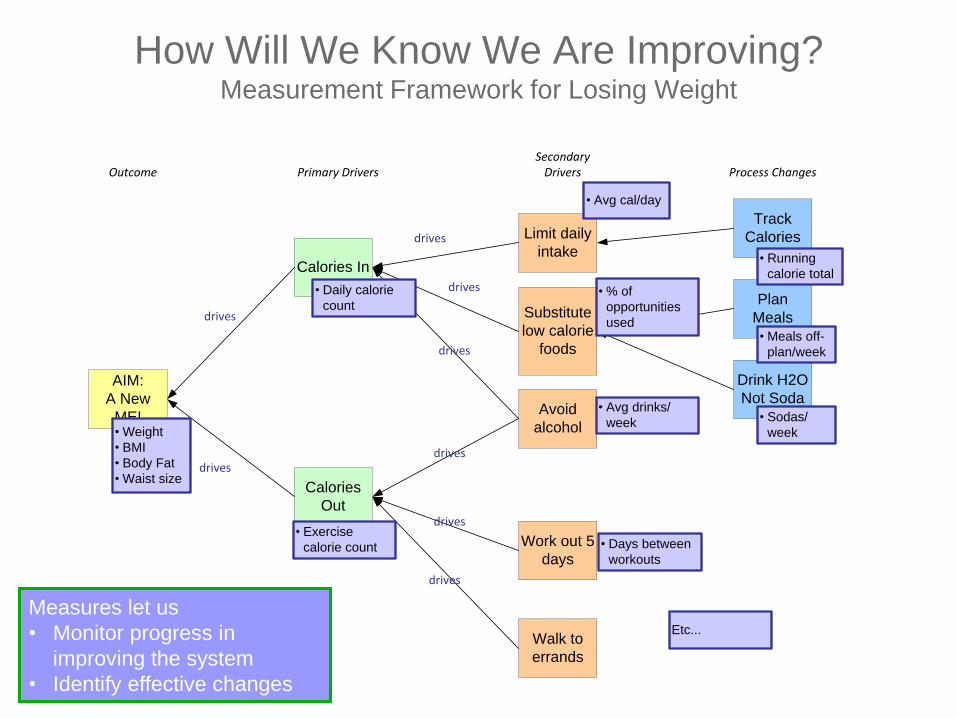
How Will We Know We Are Improving?Measurement Framework for Losing Weight
Primary DriversOutcomeSecondary
Drivers Process Changes
AIM:
A New
ME!
Calories In
Limit daily
intake
Track
Calories
Calories
Out
Substitute
low calorie
foods
Avoid
alcohol
Work out 5
days
Walk to
errands
Plan
Meals
Drink H2O
Not Soda
drives
drives
drives
drives
drives
drives
drives
drives
• Weight
• BMI
• Body Fat
• Waist size
• Daily calorie
count
• Exercise
calorie count • Days between
workouts
• Avg drinks/
week
• Running
calorie total
• % of
opportunities
used
• Sodas/
week
• Meals off-
plan/week
• Avg cal/day
Etc...
Measures let us
• Monitor progress in
improving the system
• Identify effective changes
Five Simple Examples of
Interprofessional QI Involving Trainees
• Do you know who your doctor is?
• “Tinkering” with a teenagers blood pressure medication
• Understanding drug usage and reducing unnecessary
prescriptions
‒ A million $ discovery by the medical residents
• Learning how to look for medical errors as part of routine
work
• “He’s always late for rounds”
If They Can Do It in Bogotá during
Civil Conflict with Constrained
Resources…
Reducing Post-Caesarian Infections
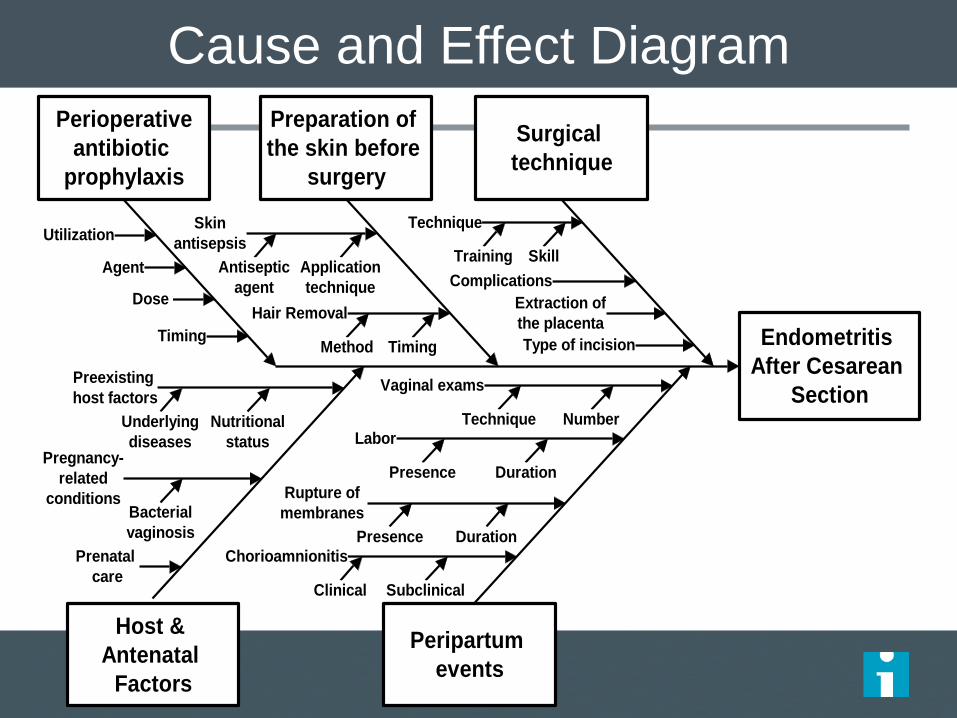
Cause and Effect Diagram
Endometritis
After Cesarean
Section
Peripartum
events
Host &
Antenatal
Factors
Preparation of
the skin before
surgery
Perioperative
antibiotic
prophylaxis
Skin
antisepsis
Hair Removal
Utilization
Timing
Nutritional
statusPregnancy-
related
conditions
Preexisting
host factors
Labor
Chorioamnionitis
Rupture of
membranes
Surgical
technique
Antiseptic
agent
Application
technique
TimingMethod
Complications
Extraction of
the placenta
Technique
Training
Prenatal
care
Vaginal exams
SubclinicalClinical
Number
Skill
Type of incision
Agent
Technique
Dose
Underlying
diseases
Bacterial
vaginosis
DurationPresence
DurationPresence
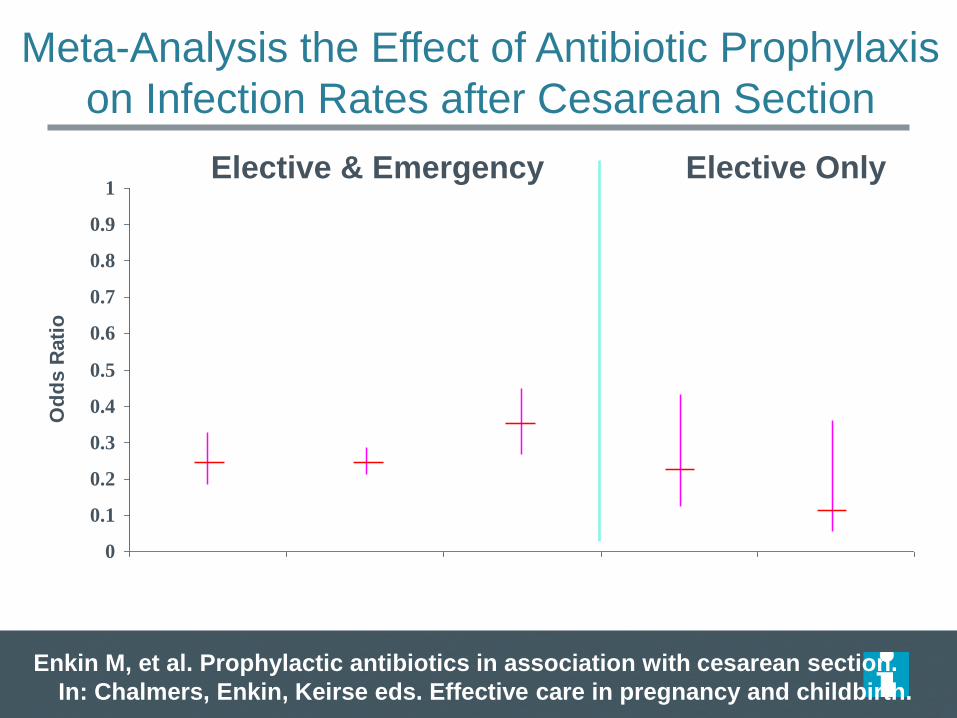
Meta-Analysis the Effect of Antibiotic Prophylaxis
on Infection Rates after Cesarean Section
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Od
ds R
ati
o
Enkin M, et al. Prophylactic antibiotics in association with cesarean section.
In: Chalmers, Enkin, Keirse eds. Effective care in pregnancy and childbirth.
Elective & Emergency Elective Only
Any serious
infection
Endometritis Wound
infection
Endometritis Wound
infection
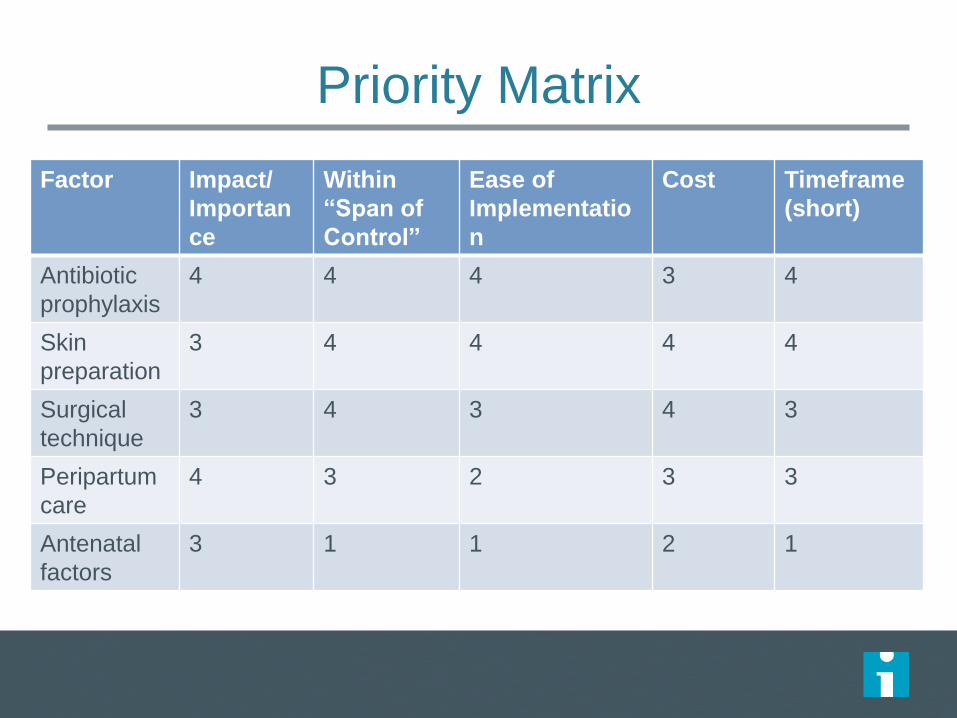
Priority Matrix
Factor Impact/
Importan
ce
Within
“Span of
Control”
Ease of
Implementatio
n
Cost Timeframe
(short)
Antibiotic
prophylaxis
4 4 4 3 4
Skin
preparation
3 4 4 4 4
Surgical
technique
3 4 3 4 3
Peripartum
care
4 3 2 3 3
Antenatal
factors
3 1 1 2 1
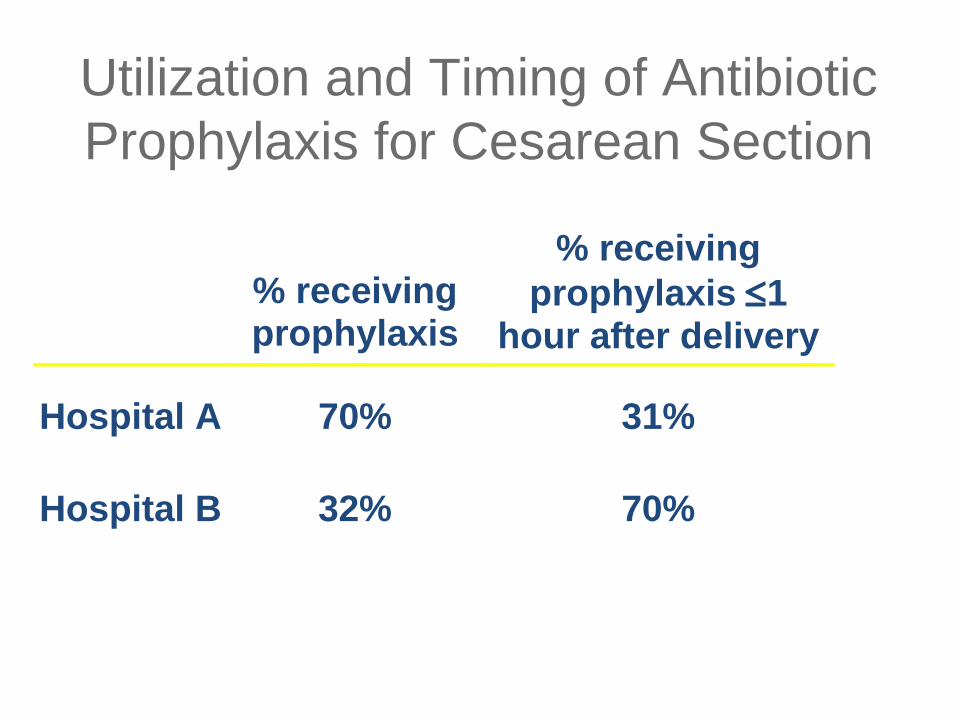
Utilization and Timing of Antibiotic
Prophylaxis for Cesarean Section
% receiving prophylaxis
% receiving
prophylaxis 1 hour after delivery
Hospital A 70% 31%
Hospital B 32% 70%
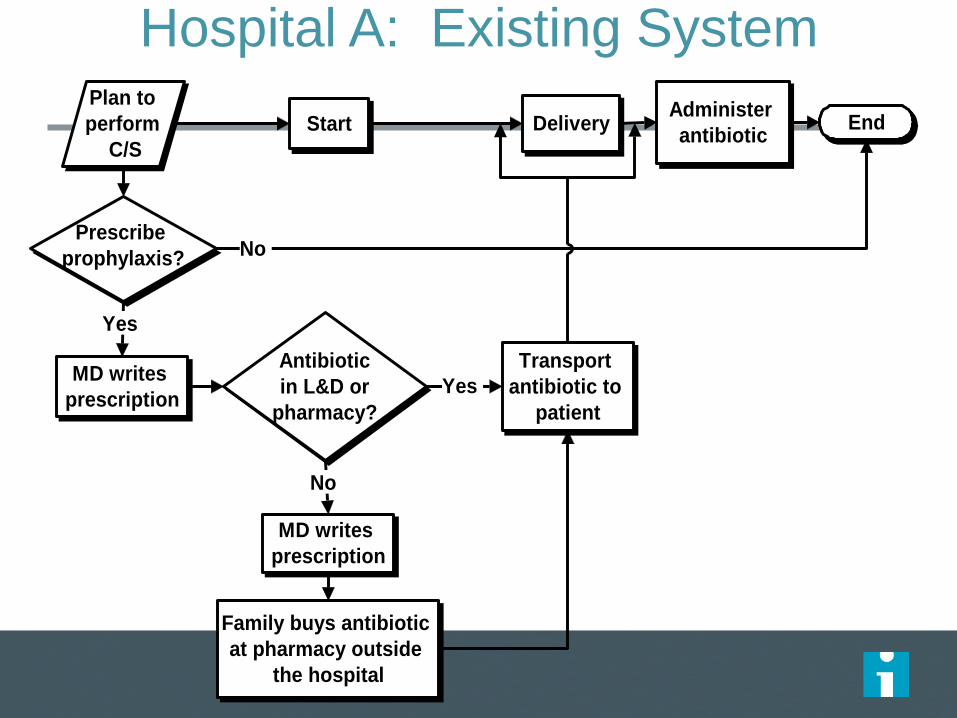
Hospital A: Existing System
Family buys antibiotic
at pharmacy outside
the hospital
Antibiotic
in L&D or
pharmacy?
MD writes
prescription
Administer
antibiotic
MD writes
prescription
Plan to
perform
C/S
Prescribe
prophylaxis?
Delivery EndStart
Transport
antibiotic to
patient
Yes
No
Yes
No
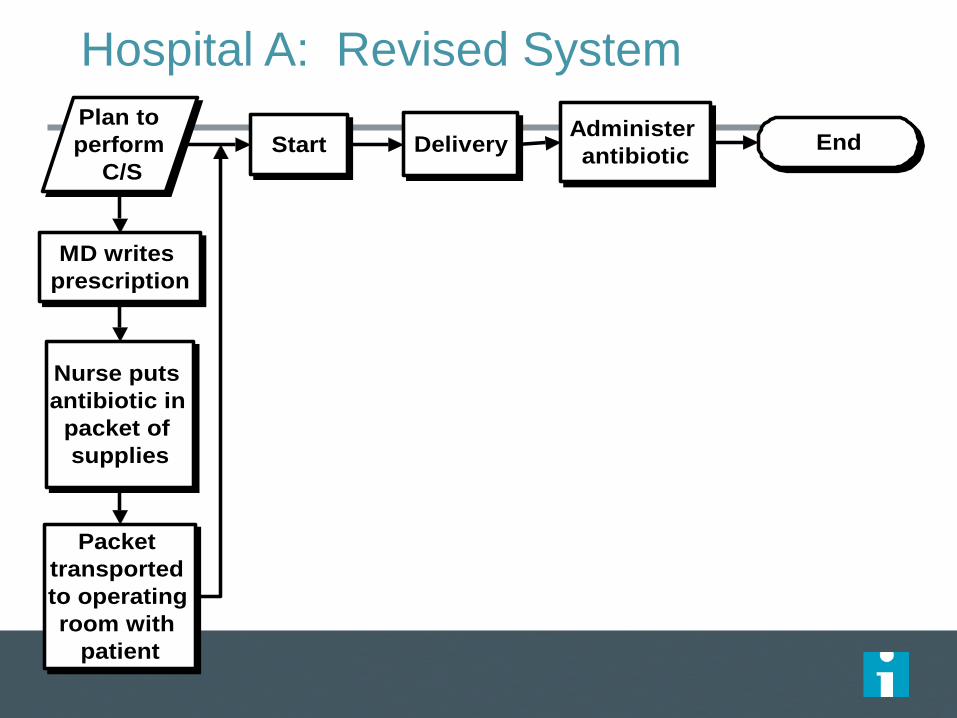
Hospital A: Revised System
Packet
transported
to operating
room with
patient
Administer
antibiotic
MD writes
prescription
Plan to
perform
C/S
DeliveryStart
Nurse puts
antibiotic in
packet of
supplies
End
0
10
20
30
40
50
60
70
80
90
100
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Month
%
0
2
4
6
8
10
12
14
16
18
20
# s
urg
ica
l sit
e in
fec
tio
ns
pe
r 1
00
ce
sa
rea
n s
ec
tio
ns
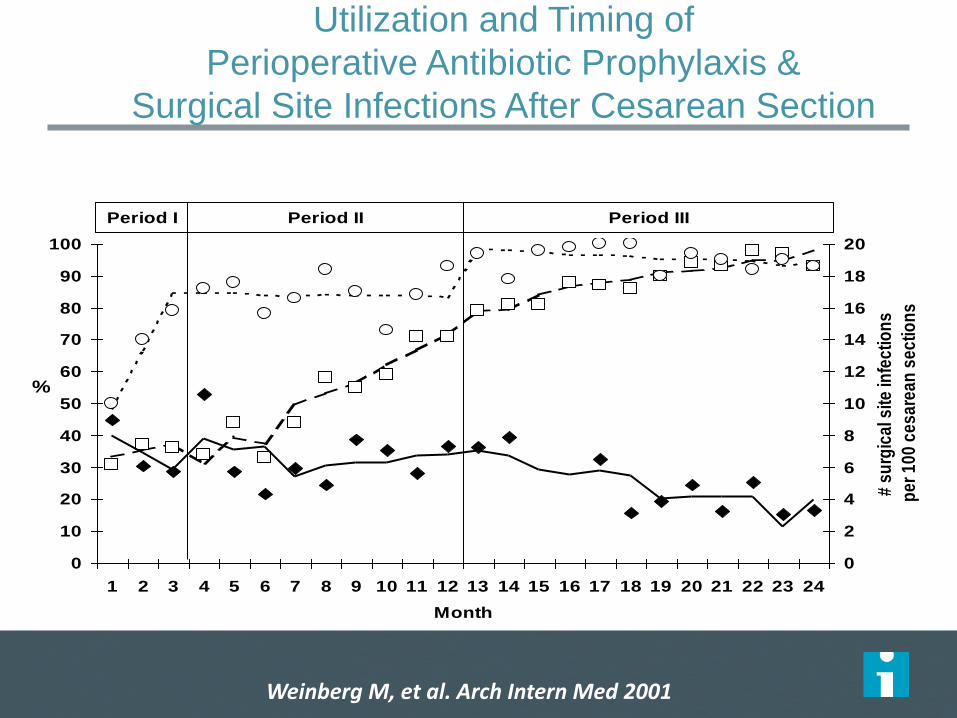
Period I Period II Period III
Utilization and Timing of
Perioperative Antibiotic Prophylaxis &
Surgical Site Infections After Cesarean Section
Receipt of antibiotic Receipt of antibiotic <1 hour after delivery Surgical site infection rate
Weinberg M, et al. Arch Intern Med 2001
Experiential Learning – Making
Rigorous QI Part of Routine Work at
the Point of Care
Monitoring Patient Safety
• Voluntary event reporting
• Morbidity and mortality conferences/reports
• Chart auditing– IHI Global Trigger Tool
• Automated data mining– Patient Safety Indicators (AHRQ PSIs)
– Automated trigger tools
• Random Safety Audit
Random Safety Audit
• Translated from industry (banking and random
process audits via Paul Plesk)
• Real time by the front line
• Data and feedback virtually immediate– Reliability of key safety processes evident immediately
– Motivating, enabling, reinforcing; builds self-efficacy and social norms (key
elements of behavioral change theory)
• Combines audit and feedback with iterative
PDSAs
– Even better than “what can I try by next Tuesday”
Random Safety Audit
• Systematically monitors a subset of error-prone points
in the system that have the potential to harm patients
• Items selected randomly to be addressed either:
– On multi-disciplinary rounds (provider input required)
– At any time during the day (provider input not needed)
• Deck can be “packed”
• 20 items developed by expert consensus for testing in
NICU (21st item added later)
• 4X6 “cards” include yes/no data form; trivia question
on back
Staff Perceptions of the Random Safety
Audit
• 84% of staff participated in rounds on which
audit was performed
• 100% agreed or strongly agreed that this
improved quality and safety
• 95% agreed or strongly agreed that it increased
knowledge of clinical guidelines and safety goals
• 9% agreed with the statement “asking a safety
question of rounds took up too much time”
Why Understanding Systems Is So Important
• Schwan’s ice cream – a terrific Minnesota family
business
• 224,000 cases of Salmonella in 1994
• What happened?


Even Kids Can Do Rigorous QI
OBESITY PREVENTION
Goal: To eliminate sugar-sweetened beverages and increase water consumption in preschool classrooms
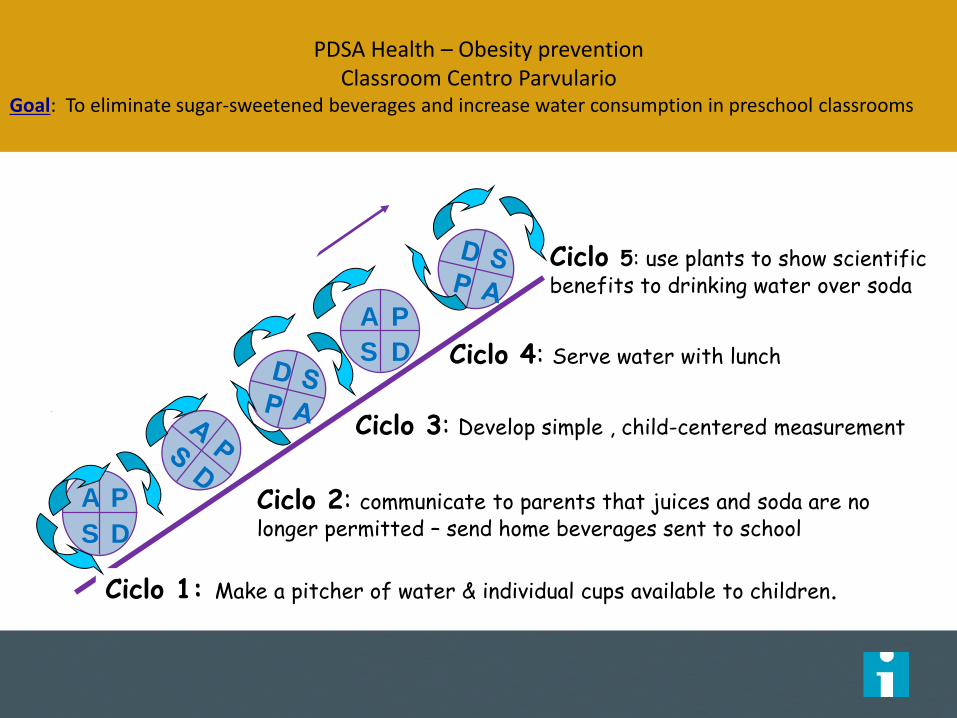
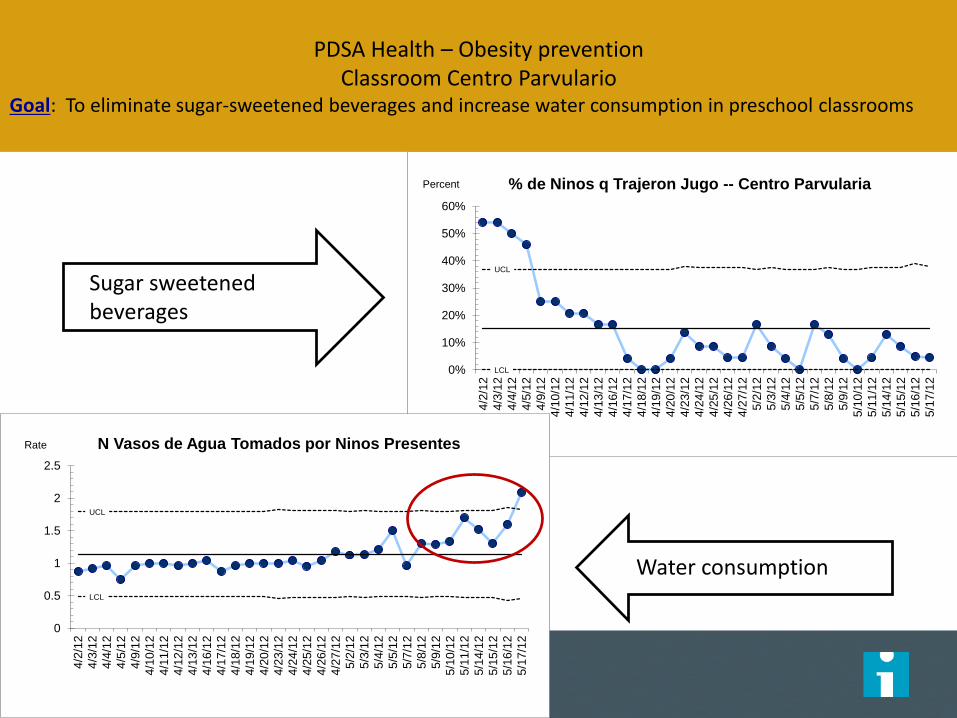
PDSA Health – Obesity preventionClassroom Centro Parvulario
Goal: To eliminate sugar-sweetened beverages and increase water consumption in preschool classrooms
A P
S D
A P
S D
Ciclo 1: Make a pitcher of water & individual cups available to children.
Ciclo 2: communicate to parents that juices and soda are no longer permitted – send home beverages sent to school
Ciclo 4: Serve water with lunch
Ciclo 3: Develop simple , child-centered measurement
Ciclo 5: use plants to show scientific benefits to drinking water over soda


UCL
LCL0%
10%
20%
30%
40%
50%
60%
4/2
/12
4/3
/12
4/4
/12
4/5
/12
4/9
/12
4/1
0/1
2
4/1
1/1
2
4/1
2/1
2
4/1
3/1
2
4/1
6/1
2
4/1
7/1
2
4/1
8/1
2
4/1
9/1
2
4/2
0/1
2
4/2
3/1
2
4/2
4/1
2
4/2
5/1
2
4/2
6/1
2
4/2
7/1
2
5/2
/12
5/3
/12
5/4
/12
5/5
/12
5/7
/12
5/8
/12
5/9
/12
5/1
0/1
2
5/1
1/1
2
5/1
4/1
2
5/1
5/1
2
5/1
6/1
2
5/1
7/1
2
% de Ninos q Trajeron Jugo -- Centro ParvulariaPercent
UCL
LCL
0
0.5
1
1.5
2
2.5
4/2
/12
4/3
/12
4/4
/12
4/5
/12
4/9
/12
4/1
0/1
2
4/1
1/1
2
4/1
2/1
2
4/1
3/1
2
4/1
6/1
2
4/1
7/1
2
4/1
8/1
2
4/1
9/1
2
4/2
0/1
2
4/2
3/1
2
4/2
4/1
2
4/2
5/1
2
4/2
6/1
2
4/2
7/1
2
5/2
/12
5/3
/12
5/4
/12
5/5
/12
5/7
/12
5/8
/12
5/9
/12
5/1
0/1
2
5/1
1/1
2
5/1
4/1
2
5/1
5/1
2
5/1
6/1
2
5/1
7/1
2
N Vasos de Agua Tomados por Ninos PresentesRate
PDSA Health – Obesity preventionClassroom Centro Parvulario
Goal: To eliminate sugar-sweetened beverages and increase water consumption in preschool classrooms
Sugar sweetened beverages
Water consumption
Questions and Open Discussion
• What challenges have you experienced
around applying QI or getting involved
with efforts locally?
• Share your own learning with the group.
What has been helpful to your success?
Raise your hand
Select Chat recipient
Enter Text
When chatting:
• Raise your hand to let us know you have a
question or comment
• Please use chat to “All Participants” for
questions
December 4-7, 2016 in Orlando, FL
• IHI Open School Chapter Congress, Monday, December 5
• Academic Scholarships
o There are scholarships available for student, residents and faculty.
Applications will be accepted on a rolling basis.
o See the Student and Resident section of the IHI Forum website for
details.
www.ihi.org/forum
Join us at the IHI National Forum

Thank you!
Questions? Ideas? Want to connect?
Kirsty and Faheem: [email protected]
IHI Open School Team: [email protected]