illinois regional integrated behavioral health network region reports
TRANSCRIPT
Illinois Regional Integrated
Behavioral Health Network
Region Reports

45
Illinois Regional Integrated
Behavioral Health Network
Region 1
Draft Report

2
Table of Contents
Topics Page #
Region 1 Plan Introduction 3
Background 4
Key Priorities 5
Unique Characteristics and Needs of Region 1:
The Chicago Metropolitan Area 6
Recommendations of Region 1 Stakeholders 6
Innovative Suggestions 9
Measures of Success 10
Conclusion 11
Meetings Letter of Invitation 12
Agenda October 5 13
Minutes October 5 14
Small Group Responses October 5 16
Agenda October 31 22
Minutes October 31 23
Small Group Responses October 31 26
Agenda November 14 29
Minutes November 14 30 Appendices PA 97-0381 32
Institute of Medicine’s Six Aims of Healthcare Quality 36
Questionnaire 37
Region 1 Participation List 39
Psychiatric & Licensed Staffed Beds 41
Statewide & Behavioral Health Primary
Diagnoses Discharges 44
State Operated Hospitals Inpatient Discharges 45
ILHFB Bed Totals 46
Hospital Statistics 47

3
Illinois Regional Behavioral Health Networks
For hospital, primary care, mental health, substance abuse,
and other community-based providers.
Note: The content of this report does not reflect the opinion or position of the Illinois Hospital
Association.
Region 1 Introduction
The Region 1 planning process began and likely will continue during a time of paradox.
Seemingly intractable challenges have been balanced by great opportunities that are unfolding
daily. Consumers, parents, and providers alike have been discouraged by tough times and bad
news. Yet, our understanding of behavioral health and substance abuse issues has never been
greater, and our willingness to think creatively and collaboratively about new models of care is
refreshing and profound.
As we enter 2013, health reform is a reality. Among the many positive opportunities presented
by national health reform legislation is the recognition that mental health and substance abuse
issues should be treated like any other illnesses. We must view persons holistically. This
legislation affirmed what we already knew and provided the structure and incentives to
significantly transform health care. It will integrate general health care with behavioral health
care; it will reward positive performance and outcomes; and it will encourage collaboration
across existing provider entities. These opportunities are presented to us at time in which the
mental health and substance abuse services systems are broken.
In 2012, the behavioral health system in Illinois is inadequate to meet the needs of persons with
mental health and substance abuse issues. It is underfunded, fragmented, inaccessible in some
locales, and inconsistent in nature, scope and quality. It is not a system. Rather, it is an amalgam
of loosely organized services. Our state’s fiscal crisis has translated into facility closures,
program reductions and waiting lists. A person with a mental health illness is more likely to
receive services in a jail than in a psychiatric facility; more likely to seek treatment in an
emergency department, in crisis, than to obtain treatment in a less-intensive setting. A person
with a substance abuse illness, in numbers disproportionate to the rest of the population, is
homeless, waiting for one of the few residential treatment slots. Those with a criminal
background do not have many housing options.
Despite a legitimate concern by participants that this planning process will be one more exercise
in futility, close to 100 consumers, parents, providers, agency staff, and advocates gathered on
three occasions to articulate a vision for a system in which every person, regardless of his or her
diagnosis, will receive the right treatment, at the right time, in the right place. Every person will
have access to safe, high quality, effective, efficient, timely, and respectful care. Every person
will have the opportunity to be well, to experience health, to have a life of meaning however he
or she defines it.
“Pie in the sky” dreams? Perhaps. However, is it unrealistic to organize, manage, and finance a
behavioral health care system that works? The participants developing the Region 1 Regional

4
Integrated Behavioral Health Network think it is not only possible, they are ready to achieve it.
Following is a compilation of their ideas and recommendations.
Background
On August 15, 2011, Governor Pat Quinn signed into law House Bill 2982 as Public Act 97-
0381, which creates the Regional Integrated Behavioral Health Networks Act. The act provides
a platform to establish Regional Integrated Behavioral Health Networks. Its purpose is to ensure
and improve access to appropriate mental health and substance abuse services throughout Illinois
by: organizing systematically all relevant health, mental health, substance abuse, and other
community resources among regional providers; developing a mechanism to use regional
resources efficiently and effectively; and serving as a catalyst for innovation and collaboration.
Under the act, each Behavioral Health Regional Network is required to develop a strategic plan
for its respective region that addresses the inventory of existing services, identifies community
needs, and defines opportunities to improve access to care. The act contemplates a broad-cross
section of the mental health, substance abuse, general health, and social services community that
will be involved in the development and implementation of the plan. Collaboration among all of
the relevant community resources will be essential to accomplish the purposes of the act, and to
build effective, coordinated and comprehensive systems of care.
In partnership with the Illinois Department of Human Services (DHS), Division of Mental Health
(DMH) and Division of Alcoholism and Substance Abuse (DASA), the Illinois Hospital
Association (IHA) and others convened a group of behavioral health providers in the state’s DHS
Region 1 to begin to identify existing services in the region; strategies for improving the
behavioral health services delivery system, including timely and appropriate access to medical as
well as behavioral health services; and ways in which providers can begin working together to
improve not only access to services but importantly, patient outcomes.
This plan outlines the priorities and recommendations for DHS Region 1, articulated by
participating service providers in three Region 1 meetings. At the first meeting held at the State
of Illinois Center, in Chicago, on October 12, participants defined their vision for behavioral
health care services in the future, identified short- term system needs and measures of success.
During the second meeting, held on October 31, participants identified priorities among their
recommendations. In the third meeting on November 14, the group reviewed and provided input
on the first draft of a regional plan. They also provided additional feedback on data sources and
trends they have experienced over the past 12 months.
This plan is a template that recognizes the shortcomings and inefficiencies of the present system,
but also embraces partnerships that promise better coordination of care, across primary medical
and behavioral care, using technology and research to improve outcomes. It is an interactive
process and one that will evolve with a changing health care and economic landscape. It will
depend on the continued commitment of all stakeholders—state agencies, primary medical,
hospitals, human and social service, and behavioral health providers. It builds on community
strengths to achieve a system of care that delivers the right care, at the right time, in the right
place. It is the first of many steps.

5
Key Priorities
There should be no wrong door into the system of care for any person, whether a person
enters the general medical door or the psychiatric or substance abuse door.
The system should be coordinated and integrated and include a continuum of care—from
prevention to acute to outpatient to rehabilitative to housing. Clinical protocols, legal and
regulatory policies and requirements, and infrastructure such as financing, information
technology, billing and records, should be designed to support the seamless movement of
an individual—regardless of his or her diagnosis—to the appropriate level of care.
Make the system easy to understand and to navigate for patients/consumers and
providers. Remove redundant processes, simplify billing and reporting, and standardize
administrative requirements, when possible, while allowing flexibility, when necessary.
Establish a system of care that is designed and financed to achieve good outcomes.
Remove incentives to use more expensive levels of care than are necessary.
Appropriately finance the level of acuity and intensity of care necessary to support
treatment and recovery. Remove financing silos that make it difficult for collaboration
and that force patients/consumers into narrowly defined categories that don’t meet their
complex needs.
Develop models for crisis and emergency services that more effectively treat mental
health and substance abuse illnesses in these settings.
Demand the use of evidence-based/ informed practices that reflect scientific knowledge
and research. Demand a commitment to continuous learning and performance consistent
with evidence-based/informed standards. Accept nothing less than the best. Be willing to
pay for the best.
Educate and train the health and behavioral health workforces to practice in an integrated
environment in which patients are treated holistically. Begin with schools and
universities; include medical residencies and traditional health professions such as
nursing; include persons who interact with children and adults in their natural settings
such as teachers or pastors.
Demonstrate to our elected leaders how they can support an effective, efficient,
accountable, high quality, accessible, culturally competent, recovery-oriented system of
care.
6
Unique Characteristics and Needs of Region 1: The Chicago Metropolitan Area
Region 1 encompasses the Chicago metropolitan area. It represents a relatively small geographic
portion of Illinois but a majority of the state’s population. It is diverse: economically, socially,
culturally, racially, and religiously. Whereas rural Illinois regions have limited access defined by
geography, financial resources, and the availability of services and health care professionals, the
Chicago’s access challenges are more about financial, social-economic and cultural barriers.
And, they are about volume; more seek care than what is available. Moreover, for many
Chicagoans, English is their second language. Some are not citizens and are unable to reach out
for services. Some hold cultural and religious beliefs that stigmatize addiction or mental health
illness.
Chicago children are growing up in some neighborhoods where friends and relatives are lost due
to gang violence. Lack of jobs and high drop-out rates contribute to cycles of poverty and unrest.
Crime is an unfortunate, but not unexpected, side-effect of these factors. Chicago-area substance
abuse, community mental health, social service providers and hospitals are operating within this
tumultuous environment as well.
Recommendations of Region 1 Stakeholders
Delivery System Innovation to Improve Access
There was consensus that there is value in focusing on the whole person. Integrating and
coordinating care across systems, including medical and behavioral health, supports this
principle. Moreover, a holistic, person-centered system must consider and attend to a person’s
multi-dimensional needs, i.e., medical, rehabilitative, social, spiritual, housing, vocational and
educational. This holistic approach is necessary if we are going to support the wellness of
consumers/clients/patients. The centerpiece of an integrated system of care is that every door will
be the right door to enter the system.
Recommendations:
The “no wrong door” approach will require articulation of a single vision by all relevant
state agencies, organization of the system of care around consistent policies, financing
and payment rules, and performance objectives.
Specifically, it will require revisions to funding and administrative regulations, which
reflect and support preservation of care delivery silos.
Licensing rules will need to be revised to achieve a unified system.
A coherent system of care must also accommodate differences. Attention must be paid to
cultural and linguistic differences and needs of a culturally diverse population as that
found in the Chicago area.
Innovative models of care should be encouraged—support behavioral health homes;
support medical homes that co-locate behavioral health clinicians in primary care
settings.

7
The integrated system of care must be designed so that everyone is on the same team—
the consumer/patient’s team. Teamwork must be rewarded. Every link must be
accountable to other members of the team and to the patient. For example, in an
integrated system, there cannot be a handoff to another level of care unless this level of
care is appropriate for the patient’s condition, is accessible and is available within an
appropriate timeframe.
Financing/Payment
Emerging delivery and payment constructs are anticipated, but there is little concrete
understanding of what it will mean for behavioral health providers. There is limited
understanding of the nature and scope of services that will be offered through the Illinois health
insurance exchange, what will be the scope of Medicaid benefits, benefits for persons who will
be insured under an “essential benefits package,” and who will remain uninsured and dependent
on the state for services. To this point, there is significant concern that persons who do not
qualify for Medicaid or Medicare, and have no insurance, are being left with too few options or
none at all. This group of persons has been disenfranchised by funding cuts in recent years. As a
consequence, they present in acute care settings or in our jails.
Recommendations:
The payment system must be flexible.
It must be adequate.
It must be timely.
It must reward the performance expected and desired.
Funding must be driven by clinical need not by eligibility for a funding category. It must
be designed to support persons who may not meet Medicaid eligibility but present with a
mental health or substance use illness and need treatment.
Providers are embarking on new models of care that will require them to assume risk.
They will need support that will vary according to their size, capitalization and expertise.
There is value in supporting the provider community’s ability to manage the care they
provide rather than have proprietary companies assume the risks and management.
Funding should be available for innovative models that represent collaboration across
general medical and behavioral care.
Eliminate the DHS contractor used to process bills. Use savings for services. Establish a
data-driven system as a replacement.

8
Quality
The President’s New Freedom Commission on Mental Health recognized in its landmark report
that there is a disconnect between what we know scientifically about mental health illness and
what is practiced. The Institute of Medicine has observed that there is a lag in the behavioral
health community in adopting evidence-based practices. It also has found that the principles that
apply to general medical care also apply to behavioral health care—care must be safe, effective,
efficient, timely, patient-centered, and equitable.
Recommendations:
Scarce resources must be reallocated to address programs that work using evidence-
informed and-based practices. Use of evidence-based/informed practices must cross all
providers and all levels of care. We should be measuring outcomes and incentivize
programs that demonstrate good or improved outcomes.
Examples of evidence-based practices for inpatient care: reduction and elimination of the
use of restraint and seclusion; limiting use of multiple antipsychotics without clinical
justification; and good discharge planning.
Outpatient care evidence-based practices include ACT Teams, WRAP or recovery action
plans.
Workforce
There are service desserts in Illinois–places where there are no psychiatrists or mental health or
substance abuse professionals, and where there are no hospitals, or mental health centers or
substance abuse providers. In Chicago, the issue is not as much the absence of professionals as it
is access to the professional. It is not as much the absence of mental health centers as it is
waiting lists for services in mental health centers that have lost funding and the capacity to serve
all who present to them.
And, we are not training a sufficient number of psychiatrists to meet current and expected need.
The primary care physician is already treating a large number of persons with psychiatric
conditions, but primary care physicians are also in short supply. After implementation of the
Affordable Care Act in 2014, the models supported under that Act depend on a large number of
primary care physicians to support it. There are not and will not be enough PCPs to support it.
In addition to a shortage of physicians trained to treat mental illness and addictive disorders,
there also is a shortage of nurses that will grow as the needs of an aging population requires more
health care. Shortages exist for all mental health professionals.
The shortage of professionals specifically trained to serve persons with mental and substance use
disorders is an issue.

9
Recommendations:
The shortage of psychiatrists to attend to the growing number of persons who need
evaluation and medication management could be addressed in part by expanding the use
or telemedicine/technology.
There should be a centralized server supported by the state to permit Chicago-area
psychiatrists to treat persons who otherwise may not have access to a psychiatrist.
State law must be reviewed to remove any barriers to the use of telemedicine. For
example, psychiatrists are not paid the same amount for a telepsychiatry service as a face-
to-face encounter. With protections in place, we may want to permit physicians licensed
in another state to provide psychiatric services to a patient in Illinois. Medicaid payment
should adequately reimburse providers at both the host and the receiving site.
Technology
Technology, specifically, the electronic health record, will be a necessary ingredient in the
integrated health system and will be necessary to accomplish the clinical goals of integration,
which include timely, accurate information about the patient’s care. Electronic billing, and
computerized systems that simplify the reporting and billing systems, also will be necessary to
reduce costs and support communication and service delivery across systems. Consumers should
have access to electronic clinical information as well.
Recommendations:
Use technology such as telemedicine to expand access, not only to rural areas but also to
patients/consumers who may have language barriers or hearing or other disabilities that
limit mobility.
Support adoption by the behavioral health community of the electronic medical record to
enable sharing of relevant clinical information about a patient/consumer across general
medical and behavioral health providers.
Establish a centralized telemedicine server that is secure. Provide local
connections/machines to providers in underserved areas.
Innovative Suggestions
There were a few innovative suggestions that can be implemented immediately or in the short
term. They include the following:
Provide a dedicated fund for acute care (defined as emergency crisis and/or inpatient
care) of persons who do not have public or private insurance. This could be similar to the
original Emergency Psychiatric Services (EPS) funds DMH administered in the past.

10
These funds had been eliminated when CHIPs was originally established, but there is not
a dedicated line item for EPS funds that are available statewide.
Establish a central data base of information about services available and their capacity.
Provide a mechanism (electronic) to ensure the information on the database is timely and
providers can easily access information when attempting to find a service for a
client/consumer/patient. Something akin to a LinkedIn page may work for this purpose. A
regional newsletter or page may also work.
Provide cross training to clinicians in health and behavioral health disciplines to support
communication across systems, identification of symptoms and timely intervention.
Measures of Success
Region 1 participants also identified measures of success for the system they were
recommending. They include the following:
Fewer presentations by persons with mental health and substance use illness in hospital
emergency departments, which would reflect an improvement of access to community
services, psychiatrists, or primary care.
Fewer admissions to a level of care that is more acute than needed, e.g. inpatient care, or
inappropriate, for patient/consumer needs, e.g. nursing homes.
Fewer readmissions to hospitals when a lower level of care would appropriately meet
patient needs, if available.
System can be accessed by any person through any door, i.e., primary care, mental health,
substance abuse, are all doors to a comprehensive, coordinated system.
The system is not organized around funding streams, but is available to every person,
regardless of funding source.
And, this “system” has consistent and rational administrative requirements (regulations)
across all provider groups, including medical and behavioral health; electronic medical
records that are accessible to all care givers; professionals in each system are trained to
recognize symptoms of health or behavioral health issues; the education system provides
cross training.
Fewer persons waiting for mental health and substance abuse services. Shorter waits for
these services when there is a list with the ultimate goal of no waiting lists.
New delivery models integrate primary and behavioral care, incorporate evidence-based
practices, measure and reward improved patient/consumer outcomes, involve provider
collaboration appropriate for the community they serve.
There will be fewer persons with either a mental or substance use condition in jail or
prison.
There will be less homeless persons with mental health or substance use conditions.

11
Conclusion
These recommendations reflect the expertise and experience of clinicians and consumers of
mental health and/or substance abuse services. They reflect their concerns that the behavioral
health system in Illinois is fragile to the point of breaking. These recommendations must now be
translated into an action plan that includes measurable objectives. Some of the recommendations
will require legislation, some regulatory changes, some additional funding, and some flexible
thinking. All of these recommendations will require the collective leadership of everyone—from
the state’s leaders to every provider to every person who interacts with the health and behavioral
health systems.

12
August 20, 2012
Name
Title
Organization
Address
City, State Zip
Dear:
Persons with mental and substance use illnesses in Illinois must navigate a complex amalgam of services
that are inconsistently available and accessible. Many seek care in crisis because they cannot obtain
timelier, appropriate care. Our state and federal fiscal crises have translated into the loss of essential
behavioral health services throughout the state, but particularly in rural Illinois. Yet, despite these
challenging circumstances, we can also identify opportunities to improve care. Some of these
opportunities stem from health reform; others are being generated by our own strategies to serve our
patients and communities. One such opportunity is being presented to us by the enactment of House Bill
2982 – Public Act 97-0381, which creates the Regional Integrated Behavioral Health Networks Act.
The purpose of the Regional Integrated Behavioral Health Networks Act is to ensure and improve access
to appropriate, high quality mental health and substance abuse services throughout Illinois. Recognizing
regional characteristics, the Act provides a platform to systematically organize all relevant health, mental
health, substance abuse, and other community resources among regional providers. And, it provides a
mechanism through which providers may integrate behavioral and other health care. To use resources
wisely, it defines each region to be consistent with existing Department of Human Services regions.
Under the Act, each respective Behavioral Health Regional Network must develop a strategic plan that
addresses the inventory of existing services, identifies community needs and defines opportunities to
improve access to care. The Act contemplates a broad-cross section of the mental health, substance abuse,
health, and social services community will be involved in the development –and implementation—of the
plan. Collaboration among all of the relevant community resources will be essential to accomplish the
purposes of the Act and to build effective, coordinated and comprehensive systems of care.
We would like to invite you to participate in the first Behavioral Health Regional Network meeting for
DHS Region 1. The meeting will take place Friday, October 5, 2012 at the Michael Bilandic Building,
5th
Floor, Room C-500 at 160 N. LaSalle, Chicago, IL. The meeting will take place from 9:00 am to
12:00 Noon.
If you have any questions or concerns, please contact: MaryLynn Clarke at 217-541-1154 or
[email protected] or Dan Wasmer at 773-908-6267 or [email protected].
To confirm your attendance, please contact Stacey Dunlap at 217-541-1152 or email your response to
Thank you,
MaryLynn McGuire Clarke
Sr. Director, Health Policy & Regulation Illinois Hospital Association
Dan Wasmer Associate Director Region Services Illinois Department of Human Services, DMH
13
Illinois Behavioral Health Network Meeting – Region 1
October 5, 2012, 9:00 am – 12:00 pm
Michael Bilandic Building
160 N. LaSalle
5th
Floor, Room C-500
Chicago, IL
Agenda
I. WELCOME.......9:00 am................Dan Wasmer, Associate Director Region Services,
DHS Division of Mental Health &
Rick Nance, Administration Bureau of Program Management,
DHS Division of Alcoholism and Substance Abuse
II. OVERVIEW OF INTEGRATED REGIONAL BEHAVIORAL HEALTH
NETWORKS ACT (HB 2982/PA 97-0381)........9:10 am................MaryLynn Clarke,
Senior Director, Illinois Hospital Association
III. DEVELOPING A PLAN FOR REGION 1…9:20 am............Maureen Slade, Director,
Stone Institute of Psychiatry, Northwestern Memorial Hospital
IV. REGIONAL PLAN DISCUSSION GROUPS…9:35 am ................................ Groups
A. Defining your vision for the behavioral health system in Illinois:
o What should the behavioral health system look like three years from now?
o What would be the key components of the new behavioral health system?
o Are there immediate actions that could be taken to improve access to
behavioral health services in this region? If so, what are they?
IV. SMALL GROUP REPORTS ...............................10:45 am............ Group Facilitators
V. SETTING PRIORITIES & NEXT STEPS .........11:45 am................. Maureen Slade
o Provider Questionnaire
VI. ADJOURNMENT & NEXT MEETING ............12:00 pm ................ Maureen Slade

14
Illinois Behavioral Health Network Meeting – Region 1
October 5, 2012, 9:00 am – 12:00 pm
Michael Bilandic Building
160 N. LaSalle
5th Floor, Room C-500
Chicago, IL
Meeting Minutes
I. Welcome
Dan Wasmer, deputy director for regions, Department of Human Services, Division of
Mental Health (DMH) and Rick Nance, administrator, bureau of program management,
DHS Division of Alcoholism and substance Abuse (DASA) welcomed meeting
participants to the first Region 1 meeting, at 9:00 a.m. They described the purpose of the
meeting: to convene a broad cross- section of the health, social service, and behavioral
health communities in Region 1, to develop a plan for that region that reflects its unique
resources and needs. This Region meeting is one of five DHS Regions that have met to
develop plans for their areas, pursuant to legislation creating the Regional Integrated
Behavioral Health Networks Act, which became effective on January 1, 2012.
There were approximately 99 participants in the meeting. See attached list.
II. Overview of HB 2982 (PA 97-0381) - The Regional Integrated Behavioral Health
Networks Act
MaryLynn Clarke, senior director, Illinois Hospital Association, provided an overview of
the Regional Integrated Behavioral Health Networks Act (P.A. 97-0381), which requires
the Department of Human Services to facilitate the development of Regional Behavioral
Health Networks in each DHS region. The Act creates a platform for providers and
community interests to improve access to behavioral health services by identifying
resources as well as needs. The Act supports collaboration among providers, and it
supports integration of general health and behavioral health services. It contemplates new
delivery models that will develop under federal health reform legislation and state
initiatives. In addition to regional planning efforts, the legislation also created the
Regional Integrated Behavioral Health Networks Steering Committee, which must be
comprised of state agencies. This statewide steering committee must support the work of
the regional planning groups by providing technical expertise and coordinating efforts
among planning regions. The Regional Plans will be communicated to the Governor and
to the Illinois General Assembly annually.
III. Regional Plan Discussion Groups
Maureen Slade, director, Stone Institute of Psychiatry, Northwestern Memorial Hospital,
served as the facilitator for Region 1. She directed participants to divide into four groups,
each of which would address four questions related to their vision for the behavioral
health and health systems in Illinois:
15
(1) What should the behavioral health system look like three years from now? (2) What
would be the key components of the new behavioral health system? (3) Are there
immediate actions that could be taken to improve access to behavioral health services in
this region? If so, what are they? (4) And, how is success defined? i.e., what are the
measures of success?
IV. Small Group Reports
The four groups reported on their findings. The information from the break-out groups is
included in the attached document.
V. Setting Priorities & Next Steps
The information collected at the meeting will be assembled by IHA. A focus on priorities
and developing specifics of the plan will be examined at the next meeting. A more
detailed summary of the meeting and a list of participants are attached.
VI. Adjournment & Next Meeting
Ms. Slade noted that the next meeting will be held Oct. 31 at 8:30 a.m. She adjourned the
meeting at 12:00 pm.

16
Small Group Responses
Region 1 October 5, 2012
Question 1: What should the behavioral health system look like three years from now?
No wrong door for any person; one entry for mental health and substance abuse and
general health care patient
Access for all people, regardless of funding ability or source; do not disenfranchise
unfunded by eliminating funding for them
Serve the “whole” individual, necessitating revisions to current providers’ eligibility
criteria
Integration of and seamlessness across types and levels of care: substance abuse, mental
health and physical health
o An example would include a multi-specialty practice
o One Site or Virtual
o Seamless transitions child/adult/geriatric
Strong community-based system
o Staff – trained, professional, quality, adequate number of staff
o Housing – safe, affordable, accessible, partnership with CAEH
o Heightened awareness of resources; service connections in neighborhood of
choice
o Technology to connect linkages and slot availability
Single system – paperwork, EHRs, eligibility
Care coordination: proper “handoffs” from different provider systems
Define system’s continuum of care to include a range of providers
Shift focus to wellness and sustenance of recovery
Incentivize hospitals to be able to provide care to non-funded patients
Medical Detox, NMRO – lack of coordination of care for these folks or lack of money?
Prevention money
LOC – how do we get a patient in one “system” connected to other systems? Care
coordination?
Need to develop “community health workers”
“Prosumers” – don’t forget the value they bring – redefine this term to include
community health workers
Gaps in connecting to other systems, LOC, “step downs”, first responder EMS
Expand system providers to include CJs, schools, EMS, housing. Lessen the gap of
disparate systems.
Adequate transition; need for new laws
Identify all sources of funding such as counties and townships, private foundations;
coordinate all types of funders. Bring all to the same table
Longer range planning – state contracts for multi-years, rather than annual.
Money – timely payments, adequate rates, proper incentives, payment systems
recognizing outcomes, efficient processing (clear definitions) of claims.
Medicaid payment continues to be an issue

17
Rates – need to be increased for Behavioral health, especially capacity grants, and
primary care
Regional HUD continuum decides what new requests/awards are submitted.
Collaborative decisions, Peer decisions.
Referral to EP MH without ER
o Direct referral to Cook County Mental Health Center
o Unfunded population
Common document/communication
Electronic record and referral
Redefine mindset of clinical professionals
Care Coordination Entities
o CCE’s
o Demonstration Projects
o Creation of Health Homes
Hub & Spokes
Care for Special population
o Children/Adolescent
o Language
o Geriatrics
Financial Support for Peer mentors and Rec. Support Specialty
More Providers with medical detox and treatment capability
More options for dually diagnosed
o Developmentally Disabled
Individualized and Holistic wrap around and funding to support this type of delivery
Birth to Death – Prenatal – special population
Evidence-based and informed
o Paid for outcome
o Assistance in implementation
Care coordinators
o Access to provider to understand MH + SA + DD
Cross training with provider & auxiliary settings, e.g., housing
Family support, treatment and involvement
Prevention
o Proactive vs. reactive
Access to care
o Lower threshold/non-acute
Med/MD education re: pharmacology – Protocol
o Include substance abuse and mental health in screenings in Primary Health
Payment incentive to do screening for MD
Education of Medical/Nurse/MD
o Univ./Med to educate
Tracking compliance of patient – quick re-entry
Protocol for ER services – pre acute admission/waiting
Team integration
Best practice models

18
Housing
o Choice of where to live
o Social determinates of health – supportive services – housing nutrition,
employment
Adolescent
Integrated Data (EMRs, Criminal Health/BH)
Electronic Records – Funding to enhance technology
Trained workforce
Peer driven services
State system that works (responsive, billing system, streamline)
Multilingual, culturally appropriate/diverse systems
Supportive employment
Evidence-based practices (long term – ongoing – continuum of services)
Managed care – Aetna vs. Illini Care
Issues with authorizations
Health information exchange
Question 2: What would be the key components of the new behavioral health system?
Recognition of everyone’s level of expertise
Financial investment in outcomes
Community based care with proper supports is more fiscally sound. Adequate money for
each level of care
Appropriate “assignment” of care to appropriate provider type or level of care
What mechanism do we need to bring it all together?
Rethink multi-disciplinary teams to multi-provider type teams; reimbursement needs to
catch up with our patient’s needs.
Transportation
Home-based behavioral health care; providers go to the patient
Consumer choice, preference, involvement
Increase available choices, recognizing geographic disparities not by funder-defined
areas
Telehealth for specialty care (psych and PCS) so much more to do with technology
Open up availability for students, fellowship – increase scholarships
Multi-cultural, lingual providers lacking
Infrastructures...look at what funding does not pay for but need to run a business. Can
jobs for consumers help in this?
Stigma – wellness – the system currently forces people to fit into LOC
Increase screenings
Care Coordination; co-location to have staff (the right staff) available
Single claim submission (one clearinghouse)
Standardize rules, including MCO, reduce redundancy
Inter-disciplinary training
More options for treatment

19
o Spectrum
o More options for insured/not insured
More bilingual services
Early intervention and prevention
Funding Source (federal/state) to implement an effective integrated network – payer
system that works
Relationship between funding and outcomes
Wellness as a family systems approach not just “identified patient”
Creative re-allocation of state services/funding
Workforce development, training, universities
Psychiatry resources limited in some communities – telemedicine – physician/nurse
practitioners/psychologists
Physician numbers to handle Medicaid expansion are low; will require concerted
attention
“Community” oriented service models – Community Health Workers
Training of physicians on mental health issues
More Robust model of training for employment development
Behavioral Health Care homes (e.g. community mental health center)
Children/Adolescent services integrated – if primary issues are chronic mental illness
Consumer involvement – peer support – designed for specific population
Outreach/education of public around behavioral health
Creative Partnering between providers
o Care Coordination Entities
Family Unit Planning
Access to health information exchange
Increase Medicaid rate to at least national median
Streamline coordination of care – equal funding
Coordinate substance use treatment with mental health through contracting or other ways
Lack of Leadership – be able to coordinate with Department of Corrections and
corrections-related agencies
Leader of mental health & substance abuse should be a cabinet position
Money for Department of Corrections
Question 3: Are there immediate actions that could be taken to improve access to
behavioral health services in this region? If so, what are they?
Fund projects to measure success
Service package for Medicaid Rehab Option services needs total revamp
o Utilization criteria, more in pot
Resource (housing) availability for Suburbs and City
Legislation to more form with more expansion
IMD rule and how it affects hospitals
Develop stronger relationship between providers to foster care coordination
Archaic regulations need to be outlawed
Break state silos between DASA/DMH and HFS
20
Eliminate Medicaid 4 prescription limit
Strong media campaign on impact (of funding inadequacy on access)
Decide core more services to be funded
Telepsychiatry; telehealth
Prompt Payment for Services
Broaden unfunded requirements
o Eligibility criteria
o Wiser expenditures – not just acute
Integrating children and DCFS – start coordination
Redefine/change payment and systematic incentives
Develop resource network
o By region – call 1-800-Help
Break down barriers to agency partnerships – joint projects – meetings – leadership
Regional Newsletter
Linked in Group
Communicate with Associations, trade support, legislatures, move to use regional
network as political force
Break down barriers between agencies and hospitals
Terminate Value Options
Integrate Systems (MH, SA, DD, etc.)
Obtain data from HFS to assist in systems design and planning
Bridge Subsidy program expansion
EPSDT Expansion
Increase services for non-Medicaid population
BH providers in similar areas collaborate, share resources, cross-training
Re-open back of the yard clinic
Ensure communication (documentation) with primary care every time a patient is seen by
behavioral health
Add public mental health services (e.g. criminal justice)
Integrated Care Philosophy
o Psych Issues
o Substance Abuse
Case Manger to have access to all
Accountability to have people follow up for integration
Updated database
Funding flexibility
Fund several community based
Managed care entity to coordinate case management and medical necessity
Universal expectations – consistency
Administrative cost covered – regardless of changes
Flexible money
Comprehensive care – OB, ER, SA, Psych
Common list of services available to all regions
Reinstate emergency funds for unfunded people

21
Expand capacity for inpatient treatment
Increase standard rates
Increase alcohol tax to support/strengthen behavioral health success
Central server – accessmydoc.com – “Tele-Anything”
Affordable medications
Question 4: How do we measure success?
Decrease in homelessness
Improved participant experience; consumer and patient satisfaction
Lower number of hospital and other services readmissions, fewer number of inpatient
bed days (of patients who could be treated in another setting appropriate for his or her
needs)
Fewer ED presentations; shorter wait times in ED
Increased Access to appropriate level of care; no or shorter wait lists
More Prosumer (CRSS) involvement
Improved population and individual health outcomes
Lower Number of behavioral health consumers in jails and corrections; and fewer
persons with mental illness in IMD nursing homes.
24-7 Access to Care (non-acute, integrated med/BH/SA-Med Rec. individualized service
net program, seamless client)
Non-acute based
Individualized – access, service delivery
Quick re-entry from acute
Seamless/portable medical record
Reasonable, consistent, timely payment
co-efficient – wise spending
“Group ownership” of clients – multidisciplinary
SMIs don’t die 25 years younger than general population
Reduction in cost of state operated facilities
Reduced wait times/improved access to appropriate level of care
A single state-wide vision/plan for behavioral healthcare
Service delivery that results in cost containment
Reduction of stigma/improved understanding acceptance of mental health
Integration of trade organizations

22
Behavioral Health Regional Network Meetings – Region 1
October 31, 2012, 8:30am-11:00am
Michael Bilandic Building
160 N. LaSalle
5th
Floor, Room C-500
Chicago, IL
Agenda
I. WELCOME...................................................8:30…...Dan Wasmer & Rick Nance
II. SUMMARY OF FIRST MEETING...........8:35 ....................... MaryLynn Clarke
III. FOCUS ON PRIORITIES………………...8:45 ............................. Maureen Slade
Small Group Priority Setting
IV. SMALL GROUP REPORTS.....................10:00 ....................... Group Facilitators
V. PRIORITIES & NEXT STEPS ................10:45 ...................................... Ms. Slade
VI. ADJOURNMENT......................................11:00…......Mr. Wasmer & Mr. Nance
Next Meeting:
November 14, 2012
Webinar

23
Illinois Behavioral Health Network Meeting – Region 1
October 31, 2012, 8:30 am – 11:00 pm
Michael Bilandic Building
160 N. LaSalle
5th Floor, Room C-500
Chicago, IL
Meeting Minutes
I. Welcome
Dan Wasmer, DHS Division of Mental Health (DMH) and Rick Nance, DHS Division of
Alcoholism and Substance Abuse (DASA), welcomed participants to the second planning
meeting of Region 1 stakeholders.
II. Summary of First Meeting
MaryLynn Clarke, IHA, provided a summary of the first meeting, during which participants
articulated their vision for the health and behavioral health systems of care. These vision
statements were defined in terms of a three year time frame and included the components of
the system. Participants also identified short term, immediate needs of the mental health and
substance abuse systems of care. And, they articulated measures of success: how they would
know when they achieved their goals and vision. A summary of these recommendations was
shared with the group.
III. Focus on Priorities
Maureen Slade, Northwestern Memorial Hospital and facilitator of the meeting, asked
participants to reconvene in the same groups in which they had convened at the October 12
meeting. Each group was directed to prioritize their recommendations in to their top ten.
IV. Small Group Reports
The four groups reported on their prioritized recommendations. These are attached to these
minutes and made a part thereof. In addition, the group as a whole engaged in a discussion of
themes that crossed all of the groups’ priorities. Among them are the following:
Provide the services the patient/consumer needs, i.e., patient-centered services.
To improve access, blend funding and eliminate silos.
Develop a user-friendly payment system, including billing, processes for submission,
methodology.
Involve more consumers in the system of care.
Provide services across the lifespan, and include the entire continuum from prevention to
acute to wrap around services.

24
Develop an information system that works: integrates patient records across settings,
respects patient rights, permits providers to talk to each other about relevant things, is
timely, accessible.
Adopt a public health model that is less medical and more recovery focused.
Failures in access to a system of care that meets patient needs by providing care in the
most appropriate level of care for the patient’s condition shifts the locus of care to the
criminal justice system. Our jails and prisons are the largest mental health facilities in
Illinois.
Shift from an emergency access dominated system.
Focus on outcomes.
Develop workforce to meet needs of emerging integrated system of care. push the
boundaries of what disciplines can do; encourage professionals to practice to the full scope
of their licenses; train workers who are able to work in multidisciplinary settings,
including behavioral health and medical care.
Empower front line staff: pay them adequately.
Dan Wasmer described the Division of Mental Health’s Strategic Planning Task Force, which
has been meeting pursuant to legislation also requiring the development of a plan for mental
health services that will be submitted to the governor and the General Assembly. This
legislation is HB 2084. The five Region Plans, including that of Region 1, will be reported to
a Statewide Steering Committee that will serve as the statewide steering committee for both
legislative enactments. There is a meeting tentatively scheduled for November 29, in which a
representative of this Region will join representatives of the other regions to present their
recommendations to the Statewide Steering Committee. These reports will be incorporated
into a plan that is submitted to the governor and to the General Assembly in 2013.
Dan noted the value of the collaborative process such as that occurring in this planning work.
Rick Nance and Dan have agreed to combine meetings with substance abuse and mental
health regional providers. At the provider level, much can be done. We don’t have to wait to
work together. We are not without the ability to get things done. This legislation happened
because someone drafted a bill and got it passed. It may take additional bills to take this work
to another level. This planning effort permits everyone—at the state and provider level—to
get beyond the annual budget cycle and to think strategically.
The discussion concluded with an admonition to all participants by a father of a consumer and
his guest, the mayor of Lincolnwood, to translate the recommendations in the plan to tangible
goals that need funding. Then, find the funding. We need a champion. As a strategy, providers
and advocates should involve their local community leaders, who can be our champions at
home. They, in turn can introduce our needs to elected representatives. We should also
demonstrate ways in which these plans will save money by being more cost-effective,
reducing redundancies, getting the right person into the right milieu.
25
V. Setting Priorities & Next Steps
We will prepare a summary of our meeting and a draft plan. This will be shared with meeting
participants before the next meeting, November 14, during which we will comment on the
draft and finalize it.
VI. Adjournment & Next Meeting
Ms. Slade noted that the next meeting will be held Nov. 14 at 2:00 p.m. She adjourned the
meeting at 11:00 a.m.

26
Small Group Responses
Region 1 October 31, 2012
GROUP ONE:
Care
Holistic/Person centered
Coordinated/integrated
Eliminate barriers
o Language
o Special Needs – Child/Adolescent
Non-Acute Based – Full Spectrum
Prevention Wellness/Recovery
Easy Access – No wrong door
Family/Client Support System
Community?
Funding
Funding for Basic Needs – Housing and Transportation
Wrap Around Support – Non Medicaid Transportation
Improve Medicaid Rates
Timely Payments
Services for Un-funded
Pro-assessing efficient
Communication/Admin
Standardize Claim Process
Single System
Efficient Processing of claims
U-Mgmt. – Single Claims Submission
Provider Communication Integration
Standardize Set of Data
Electronic Health Record
GROUP TWO:
What about DHS Providers not DIV Contractors Open Door – No Wrong Door
Improve capacity to diagnose and treat
Service Deserts
o Psychiatrist
o Telemedicine
o APN & Clinical Psychologist
Technology to Improve Information Sharing across Silos (CJ/MH) Law Change?
Access to Outpatient Directly from ED or Acute Care (Inpatient)
Medications post ED or Inpatient

27
Rates
Flex Rules at provider level to ease silos impact
Repurpose money to target outcomes
CHIPS for ED overcrowding (Pay for what works)
Vocational and Housing needs to be streamed into BH approaches
Prepare for Health care Reform
Compress with Integrated Health & BH
Look at purchasing differently
Flexibility and provider/consumer level
o Blend from silos
o Across life span
Let providers “re-purpose” contract resources
Buy outcomes more than services or service packages. Such as:
o Stable housing
o Job
o School
o Etc.
GROUP THREE:
BH Homes/CCEs providing integrated/seamless care
Single Claim Submission
Access to Health Information Exchange
Break Down Silos
Prompt Payment
Increase Services for Non-Medicaid Population
Fewer ED Use
Lower # of BH Consumers in Jail; Fewer BH Consumers in IMDs
Reduced Wait Times/Improved Access to Appropriate Level of Care
GROUP FOUR:
Improve Medicaid Rate
Timely Payment
Single Claims System
Services for Unfunded
o Regardless of Ability to Pay/Fewer Restrictions
Eliminate Structure/System
o Silos in DHS & DOC – Cooperation in programs/services/deflection/discharges
from jail at all levels
Cooperation/Communication
o Between Providers/Electronic Medical Records – Development of Coalition,
Partnerships
Full Funding for Spectrum of Care, including:
o Prevention/Recovery/Support

28
Funding Medicaid Streams for breaking barriers to care:
o Transportation
o Housing
o Translation/language/cultural
Consumer, Family, Support System Involvement in Services, Feedback regarding
services and services development.
GROUP FIVE:
Better explanation of planning process and how this process fits.
Access for all people (especially un/under insured) – Inclusive of Rule 132/Rule 2060
Timely Payments and Adequate Rates
Strong Community Based System (Prevent inappropriate placement for services, i.e. jails,
prisons, ER)
Integrated systems including CRSS credentialed consumers, cook county waiver
Workforce development training university = meeting increased demands.
Prevention Money
Eliminate the 4 prescription Drug limit
Effective Integrated Network
o Electronic
o Documentation
o Claims
o Sharing information
o Consistency
o Telemedicine
o Telehealth
Care Coordination; proper hand off to next level of care (continuum of care from
prevention to reintegration)
A common vision for a spectrum of services from engagement to recovery for mental
health and substance abuse
Strong Media Campaign
Recommendation: Region 1 Manage this.
29
Behavioral Health Regional Network Meetings – Region 1
November 14, 2012, 2:00 pm - 3:30 pm
Webinar
Agenda
I. WELCOME..............................................2:00 ..…...Dan Wasmer & Rick Nance
II. SUMMARY OF SECOND MEETING.......2:10.........................MaryLynn Clarke
III. REVIEW OF PLAN/PRIORITIES………...2:30.............................Maureen Slade
IV. DISCUSSION..................................................2:45.......................................Everyone
V. NEXT STEPS .................................................3:15.......................................Ms. Slade
VI. ADJOURNMENT......................................3:30...............Mr. Wasmer & Mr. Nance

30
Illinois Behavioral Health Network Meeting – Region 1
November 14, 2012, 2:00 pm – 3:30 pm
Webinar
Meeting Minutes
I. Welcome
Rick Nance, administrator, DHS/ DASA and Dan Wasmer, associate director, DHS/
DMH, welcomed participants to the third Region 1 meeting. They noted meeting
materials had been sent to them in advance of the meeting. These included a draft Region
1 Plan, which reflects many of their discussions during the first two meetings. They
explained that the purpose of this meeting was to review, comment upon, and contribute
to this Plan.
II. Review of Second Region 1 Meeting
MaryLynn Clarke, IHA, reviewed the second Region 1 meeting. She noted that, during
that meeting, participants resumed participation into small groups, and they prioritized
the recommendations they had made in the first meeting. A copy of these small group
prioritized recommendations had been provided to them in their meeting materials. She
indicated that the Region 1 Plan under discussion today incorporated these
recommendations.
III. Region 1 Plan Priorities
Maureen Slade, Region 1 facilitator and director, Stone Institute of Psychiatry,
Northwestern Memorial Hospital, opened the discussion about the Plan by presenting
priorities of the group. Mr. Nance then reviewed recommendations regarding delivery
system innovations; Mr. Wasmer reviewed financing and payment priorities and
challenges; Ms. Clarke presented workforce and with Ms. Slade quality
recommendations; Mr. Nance presented technology recommendations.
IV. Data
Ms. Clarke reviewed data that had been provided. These data included information about
the number of acute, inpatient hospital psychiatric beds in Region 1; the number of
hospital discharges for persons with behavioral health diagnoses for the years 2007-2012;
and state-operated hospital statistics. Data about community mental health centers and
substance abuse providers will be added to the Plan.
V. Discussion
Participants in the webinar were invited to ask questions or make suggestions. Among the
issues discussed was:
Emergency departments differ in their capacity to provide emergency services tailored to
persons with psychiatric disorders and as a consequence in the level of care they are

31
providing. Can we survey Chicago-area emergency departments about the psychiatric
care they are providing?
Will the current fee-for-service payment model for community services continue in a
managed care payment model? It appears that this is the direction in which payment is
moving.
It was recommended that DHS provide data from FY08 to the present documenting the
budgeted funds and reductions made in each of these years in order to demonstrate the
actual dollars lost to the system. We should also document the number of community
mental health centers and substance abuse programs that have closed.
Cross training of professionals in either and both the behavioral and general health care
sectors should occur.
There should be performance-based contracting.
A defining characteristic of Region 1 is the volume of persons who need behavioral
health services. The large numbers of persons in this urban environment who present for
treatment often experience waiting lists from over-burdened providers. Access is a
function of the capacity to serve the numbers of persons presenting for care.
We should add “prevention” to the continuum of care recommended in the plan. Include
various kinds of prevention activities that should be available. Funding for prevention
services has been reduced; yet it is so important.
Housing also must be included in the continuum of care. An evidence-based practice is
the combination of housing with mental health and substance abuse services.
Support the integration of FQHCs and CMHCs.
VI. Adjournment
The webinar concluded at 3:25 PM.

32
Appendix
Regional Integrated Behavioral Health Networks Act
Public Act 097-0381
An Act concerning health.
Be it enacted by the People of the State of Illinois, represented in the General Assembly:
Section 1. Short title.
This Act may be cited as the Regional Integrated Behavioral Health Networks Act.
Section 5. Legislative Findings.
The General Assembly recognizes that an estimated 25% of Illinoisans aged 18 years or older
have experienced a mental or substance use disorder, an estimated 700,000 Illinois adults aged
18 years or older have a serious mental illness and an estimated 240,000 Illinois children and
adolescents have a serious emotional disturbance. And on any given day, many go without
treatment because it is not available or accessible. Recent federal and State fiscal crises have
exacerbated an already deteriorating mental health and substance abuse (behavioral health)
treatment system that is characterized by fragmentation, geographic disparities, inadequate
funding, psychiatric and other mental health workforce shortages, lack of transportation, and
overuse of acute and emergency care by persons in crisis who are unable to obtain treatment
from less intensive community alternatives. The failure to treat mental and substance use
illnesses has human and financial consequences: human suffering and loss of function; increased
use of hospital emergency departments; increased use of all medical services; increased
unemployment, and lack of productivity; lack of meaningful engagement in family and
communities; school failure; homelessness; incarceration; and, in some instances, death. The
citizens of Illinois with mental and substance use illnesses need an organized and integrated
system of care that recognizes regional differences and is able to deliver the right care to the
right person at the right time.
Section 10. Purpose.
The purpose of this Act is to require the Department of Human Services to facilitate the creation
of Regional Integrated Behavioral Health Networks (hereinafter "Networks") for the purpose of
ensuring and improving access to appropriate mental health and substance abuse (hereinafter
"behavioral health") services throughout Illinois by providing a platform for the organization of
all relevant health, mental health, substance abuse, and other community entities, and by
providing a mechanism to use and channel financial and other resources efficiently and
effectively. Networks may be located in each of the Department of Human Services geographic
regions.
Section 15. Goals.
Goals shall include, but not be limited to, the following: enabling persons with mental and
substance use illnesses to access clinically appropriate, evidence-based services, regardless of
where they reside in the State and particularly in rural areas; improving access to mental health
and substance abuse services throughout Illinois, but especially in rural Illinois communities, by

33
fostering innovative financing and collaboration among a variety of health, behavioral health,
social service, and other community entities and by supporting the development of regional-
specific planning and strategies; facilitating the integration of behavioral health services with
primary and other medical services, advancing opportunities under federal health reform
initiatives; ensuring actual or technologically-assisted access to the entire continuum of
integrated care, including the provision of services in the areas of prevention, consumer or
patient assessment and diagnosis, psychiatric care, case coordination, crisis and emergency care,
acute inpatient and outpatient treatment in private hospitals and from other community providers,
support services, and community residential settings; identifying funding for persons who do not
have insurance and do not qualify for State and federal healthcare payment programs such as
Medicaid or Medicare; and improving access to transportation in rural areas.
Section 20. Steering Committee and Networks.
(a) To achieve these goals, the Department of Human Services shall convene a Regional
Integrated Behavioral Health Networks Steering Committee (hereinafter "Steering Committee")
comprised of State agencies involved in the provision, regulation, or financing of health, mental
health, substance abuse, rehabilitation, and other services. These include, but shall not be limited
to, the following agencies:
(1) The Department of Healthcare and Family Services.
(2) The Department of Human Services and its Divisions of Mental Illness and
Alcoholism and Substance Abuse Services.
(3) The Department of Public Health, including its Center for Rural Health.
The Steering Committee shall include a representative from each Network. The agencies of the
Steering Committee are directed to work collaboratively to provide consultation, advice, and
leadership to the Networks in facilitating communication within and across multiple agencies
and in removing regulatory barriers that may prevent Networks from accomplishing the goals.
The Steering Committee collectively or through one of its member Agencies shall also provide
technical assistance to the Networks.
(b) There also shall be convened Networks in each of the Department of Human Services'
regions comprised of representatives of community stakeholders represented in the Network,
including when available, but not limited to, relevant trade and professional associations
representing hospitals, community providers, public health care, hospice care, long term care,
law enforcement, emergency medical service, physicians trained in psychiatry; an organization
that advocates on behalf of federally qualified health centers, an organization that advocates on
behalf of persons suffering with mental illness and substance abuse disorders, an organization
that advocates on behalf of persons with disabilities, an organization that advocates on behalf of
persons who live in rural areas, an organization that advocates on behalf of persons who live in
medically underserved areas; and others designated by the Steering Committee or the Networks.
A member from each Network may choose a representative who may serve on the Steering
Committee.
Section 25. Development of Network Plans.
Each Network shall develop a plan for its respective region that addresses the following:
34
(a) Inventory of all mental health and substance abuse treatment services, primary health
care facilities and services, private hospitals, State-operated psychiatric hospitals, long
term care facilities, social services, transportation services, and any services available to
serve persons with mental and substance use illnesses.
(b) Identification of unmet community needs, including, but not limited to, the following:
(1) Waiting lists in community mental health and substance abuse services.
(2) Hospital emergency department use by persons with mental and substance use
illnesses, including volume, length of stay, and challenges associated with
obtaining psychiatric assessment.
(3) Difficulty obtaining admission to inpatient facilities, and reasons therefore.
(4) Availability of primary care providers in the community, including Federally
Qualified Health Centers and Rural Health Centers.
(5) Availability of psychiatrists and mental health professionals.
(6) Transportation issues.
(7) Other.
(c) Identification of opportunities to improve access to mental and substance abuse
services through the integration of specialty behavioral health services with primary care,
including, but not limited to, the following:
(1) Availability of Federally Qualified Health Centers in community with mental
health staff.
(2) Development of accountable care organizations or other primary care entities.
(3) Availability of acute care hospitals with specialized psychiatric capacity.
(4) Community providers with an interest in collaborating with acute care
providers.
(d) Development of a plan to address community needs, including a specific timeline for
implementation of specific objectives and establishment of evaluation measures. The
comprehensive plan should include the complete continuum of behavioral health
services, including, but not limited to, the following:
(1) Prevention.
(2) Client assessment and diagnosis.
(3) An array of outpatient behavioral health services.
(4) Case coordination.
(5) Crisis and emergency services.
(6) Treatment, including inpatient psychiatric services in public and private
hospitals.
(7) Long term care facilities.
(8) Community residential alternatives to institutional settings.
(9) Primary care services.
Section 30. Timeline.
The Network plans shall be prepared within 6 months of establishment of the Network. The
Steering Committee shall assist the Networks in the development of plans by providing technical
expertise and in facilitating funding support and opportunities for the development of services
identified under each of the plans.

35
Section 35. Report to Governor and General Assembly.
The Steering Committee shall report to the Governor and General Assembly the status of each
regional plan, including the recommendations of the Network Councils to accomplish their
goals and improve access to behavioral health services. The report shall also contain
performance measures, including changes to the behavioral health services capacity in the
region; any waiting lists for community services; volume and wait times in hospital emergency
departments for access to behavioral health services; development of primary care-behavioral
health partnerships or barriers to their formation; and funding challenges and opportunities. This
report shall be submitted on an annual basis.
Section 99. Effective date.
This Act takes effect January 1, 2012.
HB2982 Enrolled LRB097 10532 KTG 51304 b
Public Act 097-0381

36
The Institute of Medicine’s Six Aims of Healthcare Quality:
1. Safe: Care should be as safe for patients in health care facilities as in their homes;
2. Effective: The science and evidence behind health care should be applied and serve as the
standard in the delivery of care;
3. Efficient: Care and service should be cost effective, and waste should be removed from
the system;
4. Timely: Patients should experience no waits or delays in receiving care and service;
5. Patient centered: The system of care should revolve around the patient, respect patient
preferences, and put the patient in control; and
6. Equitable: Unequal treatment should be a fact of the past; disparities in care should be
eradicated.
Recognizing that aims must be accompanied by observable metrics, the IOM defined sets of
measurements for each aim. For example:
Safe: Overall mortality rates or the percentage of patients receiving safe care;
Effective: How well evidenced-based practices are followed, such as the percentage of
time diabetic patients receive all recommended care at each visit;
Efficient: Analysis of the costs of care by patient, provider, organization, and community;
Timely: Waits and delays in receiving care, service, or results;
Patient centered: Patient and family satisfaction; and
Equitable: Differences in quality measures by race, gender, income, and other
population-based demographic and socioeconomic factors.
Institute of Medicine. (2006). “Improving the Quality of HealthCare for Mental and
Substance-Use Conditions”. Crossing the Quality Charm: Adaptation for Mental
Health and Addictive Disorders. A. Daniels, M.J. England, Ann Page, J.M. Corrigan.
(Eds.) Washington, DC: National Academy Press.
37
Regional Behavioral Health Network – Region 1
Provider Questionnaire
1. Wait Times
Over the past year, has your facility experienced longer wait times for patients to
receive services due to transportation, available placements, etc.? If so, what
primary factors contribute to the delays?
On a scale of 1-5 how big a problem are wait times for your facility? (1= very
important – 5 = not important at all) ______
Have you documented these delays?______ If so, what data do you have?
2. Security Concerns
Have you had to utilize security to maintain patients who are at your facility
waiting for a transfer? ______
On a scale of 1-5 how big a problem is security concerns related to delayed
transfers? (1 = very important, 5 = not important at all) ____ What data do you
have to document security issues? ______
If so, what data do you have?
3 Patient Volume
Have you seen an increase in the number of mentally ill and or substance abusing
patients being served at your facility in the past year?
On a scale of 1-5 how important is this issue to your facility?
What data do you have available to demonstrate these increases?
4. Transportation
Is transportation to appropriate care for unfunded patients a problem in your area?
On a scale of 1-5 how big a problem do you believe this is? ______
What data is available to document this problem?
5. Admissions

38
Over the past year have you had to admit more patients with mental illness or
substance abuse problems to non-behavior health units in your hospital because
you could not locate appropriate care elsewhere either inside or outside your
facility? _____
On a scale of 1-5 how big a problem do you believe this is? _______
What data do you have available to document this issue?
6. Please add any additional issues or trends experienced at your facility over the
past year and what data you have to document the issue.
7. Would you be interested in continuing to dialogue with other behavioral health
providers in your region through meetings, trainings, and workshops?
8. Would you be interested in working with other providers in the region on
common network issues such as transportation, regulatory barriers and other
system design issues? Please indicate which issues would be helpful to you.
9. Any other items (including data) you would like to share about this planning
process or materials that are related to this effort?

39
Region 1 Participation List
ACMHAI
Ada S. McKinley Community Services, Inc.
Adapt of Illinois
Advocate Christ Medical Center
Advocate Illinois Masonic Medical Center
Advocate South Suburban Hospital
Advocate Trinity Hospital
Aetna Better Health, Illinois
Alexian Brothers Behavioral Health
Hospital
Alexian Brothers Center for Mental Health
Alternatives, Inc
Asian Human Services, Inc.
Association for Individual Development
Association House of Chicago
Behavioral Services Center
Bremen Youth Services
Caritas
Cathedral Shelter of Chicago
Catholic Charities
Chicago Children's Center for Behavioral
Health Saints Mary & Elizabeth Medical
Center
Chicago Department of Public Health
Chicago Read Mental Health Center
Circle Family HealthCare Network
Claudia & Eddie's Place, NFP
Community Behavioral Healthcare
Association of IL
Community Counseling Centers of Chicago
Community Mental Health Board of Oak
Park Township
Confidential DUI Services
Cook County Adult Probation
Corporation for Supportive Housing
DePaul Family and Community Services
DHS - Elgin Mental Health Center
Doctors Council
Family Guidance Centers
Family Service & Mental Health Center of
Cicero
Gateway Foundation
Grand Prairie Services
Grow In Illinois
Guildhaus Halfway House For Men
Harbor Light Center of the Salvation Army
Hartgrove Hospital
Haymarket Center
Healthcare Alternative Systems
Heartland Health Outreach/Heartland
Alliance
Housing Options
HSI
Human Resources Development Institute,
Inc.
IJEGDA Community, Inc.
Illinois Department of Human Services,
DMH
Illinois Department of Human Services,
DASA
Illinois Dept. of Human Services, DMH
Illinois Health Connect
Illinois Hospital Association
Illinois Psychiatric Society
Ingalls Memorial Hospital
Iroquois Mental Health Center
Josselyn Center
Lester & Rosalie Anixter Center
Leyden Family Service
Leyden Family Service & The SHARE
Program
Loretto Hospital
Loyola Gottlieb Memorial Hospital
Lutheran Social Services of Illinois
Maine Center, Inc.
Mercy Hospital & Medical Center
Metro C & A
Metropolitan Family Services
Mount Sinai Hospital
NAMI of Illinois
NAMI South Suburbs of Chicago
Neumann Family Services
New Foundation Center, Inc.
NorthShore University HealthSystem at
Evanston Hospital
Northwestern Memorial Hospital
PEER Services
Pillars
40
Pilsen Wellness Center, Inc.
Polish American Association
Resurrection Behavioral Health
Rincon Family Services
Saint Bernard Hospital
Solleys' Place
Southwest Community Services, Inc.
Specialist Assistance Services, NFP
Sts. Mary & Elizabeth Medical Center
TASC, Inc.
The Helen Wheeler Center for Community
Mental Health
The Path - Recovery Living for Women
The Salvation Army Harbor Light Center
The South Suburban Council on Alcoholism
& Substance Abuse
The Women's Treatment Center
Thorek Memorial Hospital
Thresholds
Thrive Counseling Center
Trinity Services
Trinity United Church of Christ
Turning Point Behavioral Health Care
Center
University of Chicago
University of Illinois at Chicago
Will County Health Departments, Division
of BH Programs

41
Region 1 Acute Care Hospitals with
Psychiatric Beds
Hospital Name City
Psychiatric
Licensed Beds
Staffed Psych
Beds Oct 1, 2009
Adventist La Grange Mem Hosp La Grange 0 0
Advocate Christ Medical Center Oak Lawn 51 46
Advocate Illinois Masonic MC Chicago 39 35
Advocate Lutheran General Hosp Park Ridge 55 49
Advocate South Suburban Hosp Hazel Crest 0 0
Advocate Trinity Hospital Chicago 0 0
Alexian Brothers Behav Hlth Hsp Hoffman Estates 141 141
Alexian Brothers Medical Ctr Elk Grove Village 0 0
Chicago Lakeshore Hospital Chicago 146 108
Chicago-Read Mental Health Ctr Chicago Children's Memorial Hospital Chicago 18 12
Franciscan St James Hlth/Chi Ht Chicago Heights 0 0
Franciscan St James Hlth/Oly Fl Olympia Fields 0 0
Hartgrove Behavioral Health Sys Chicago 150 150
Holy Cross Hospital Chicago 0 0
Holy Family Medical Center Des Plaines 0 0
Ingalls Memorial Hospital Harvey 68 34
Jackson Park Hospital & Med Ctr Chicago 86 86
Jesse Brown VA Medical Center Chicago John H Stroger, Jr Hsp/Cook Cty Chicago 0 0
John J Madden Mental Hlth Ctr Hines Kindred Chicago Central Hosp Chicago 0 0
Kindred Chicago Lakeshore Chicago 0 Kindred Hosp Chicago Northlake Northlake 0 0
Kindred Hospital Chicago North Chicago 31 26
La Rabida Children's Hospital Chicago 0 0
Little Co of Mary Hosp & HCC Evergreen Park 24 24
Loretto Hospital Chicago 76 60
Loyola Gottlieb Memorial Hosp Melrose Park 12 12
Loyola University Med Center Maywood 0 0
MacNeal Hospital Berwyn 62 52
Maryville Scott Nolan Center Des Plaines 180 56
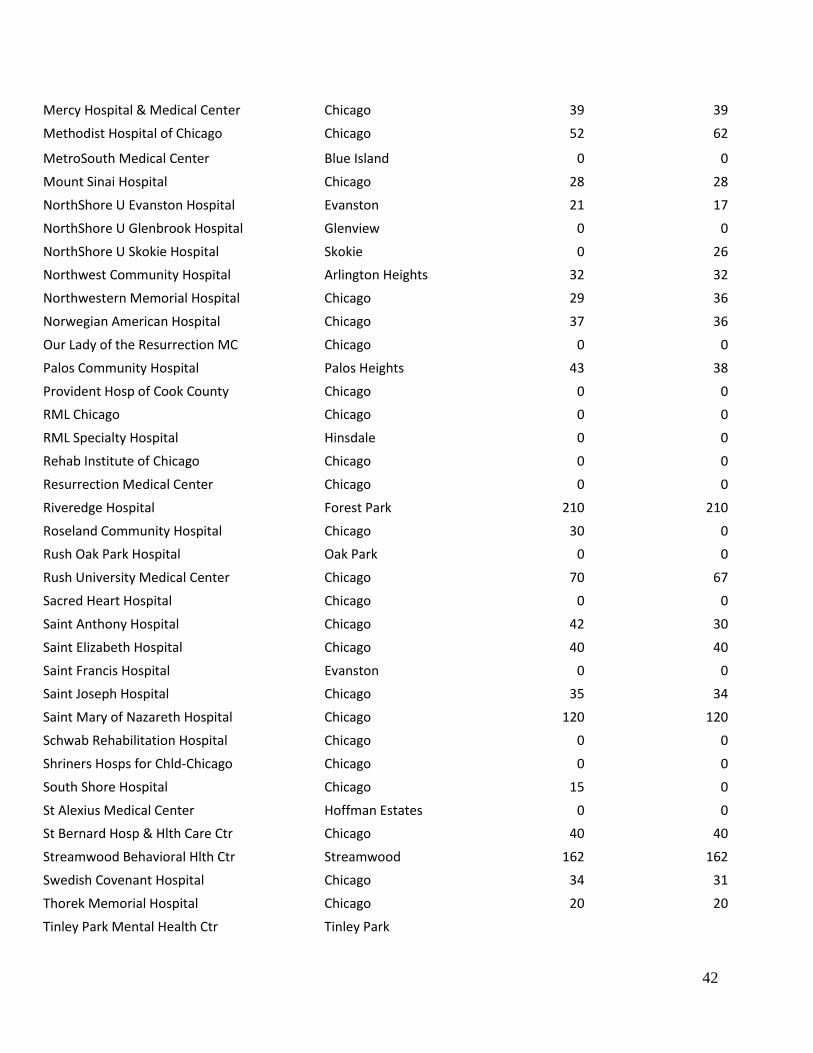
42
Mercy Hospital & Medical Center Chicago 39 39
Methodist Hospital of Chicago Chicago 52 62
MetroSouth Medical Center Blue Island 0 0
Mount Sinai Hospital Chicago 28 28
NorthShore U Evanston Hospital Evanston 21 17
NorthShore U Glenbrook Hospital Glenview 0 0
NorthShore U Skokie Hospital Skokie 0 26
Northwest Community Hospital Arlington Heights 32 32
Northwestern Memorial Hospital Chicago 29 36
Norwegian American Hospital Chicago 37 36
Our Lady of the Resurrection MC Chicago 0 0
Palos Community Hospital Palos Heights 43 38
Provident Hosp of Cook County Chicago 0 0
RML Chicago Chicago 0 0
RML Specialty Hospital Hinsdale 0 0
Rehab Institute of Chicago Chicago 0 0
Resurrection Medical Center Chicago 0 0
Riveredge Hospital Forest Park 210 210
Roseland Community Hospital Chicago 30 0
Rush Oak Park Hospital Oak Park 0 0
Rush University Medical Center Chicago 70 67
Sacred Heart Hospital Chicago 0 0
Saint Anthony Hospital Chicago 42 30
Saint Elizabeth Hospital Chicago 40 40
Saint Francis Hospital Evanston 0 0
Saint Joseph Hospital Chicago 35 34
Saint Mary of Nazareth Hospital Chicago 120 120
Schwab Rehabilitation Hospital Chicago 0 0
Shriners Hosps for Chld-Chicago Chicago 0 0
South Shore Hospital Chicago 15 0
St Alexius Medical Center Hoffman Estates 0 0
St Bernard Hosp & Hlth Care Ctr Chicago 40 40
Streamwood Behavioral Hlth Ctr Streamwood 162 162
Swedish Covenant Hospital Chicago 34 31
Thorek Memorial Hospital Chicago 20 20
Tinley Park Mental Health Ctr Tinley Park

43
Univ of Chicago Medical Center Chicago 0 0
University of IL Med Ctr Chicago 53 47
Veterans Affairs Hines Hospital Hines
Weiss Memorial Hospital Chicago 10 10
West Suburban Medical Center Oak Park 0 0
Westlake Hospital Melrose Park 33 30
Region Total: 2,334 2,046
Source: Licensed Beds-IDPH Addendum to Inventory of Health Care Facilities
Staffed Beds-IDPH Annual Hospital Questionnaire, 2009.

44
Inpatient Discharges Cumulative % Change
SFY
2005
SFY
2006
SFY
2007
SFY
2008
SFY
2009
SFY
2010
From SFY 2005 to SFY 2010
Statewide 1,723,215 1,714,661 1,724,116 1,715,750 1,677,926 1,651,967 -4.1%
Region 3 85,305 85,313 86,099 85,500 85,807 89,970 5.5%
Source: COMPdata
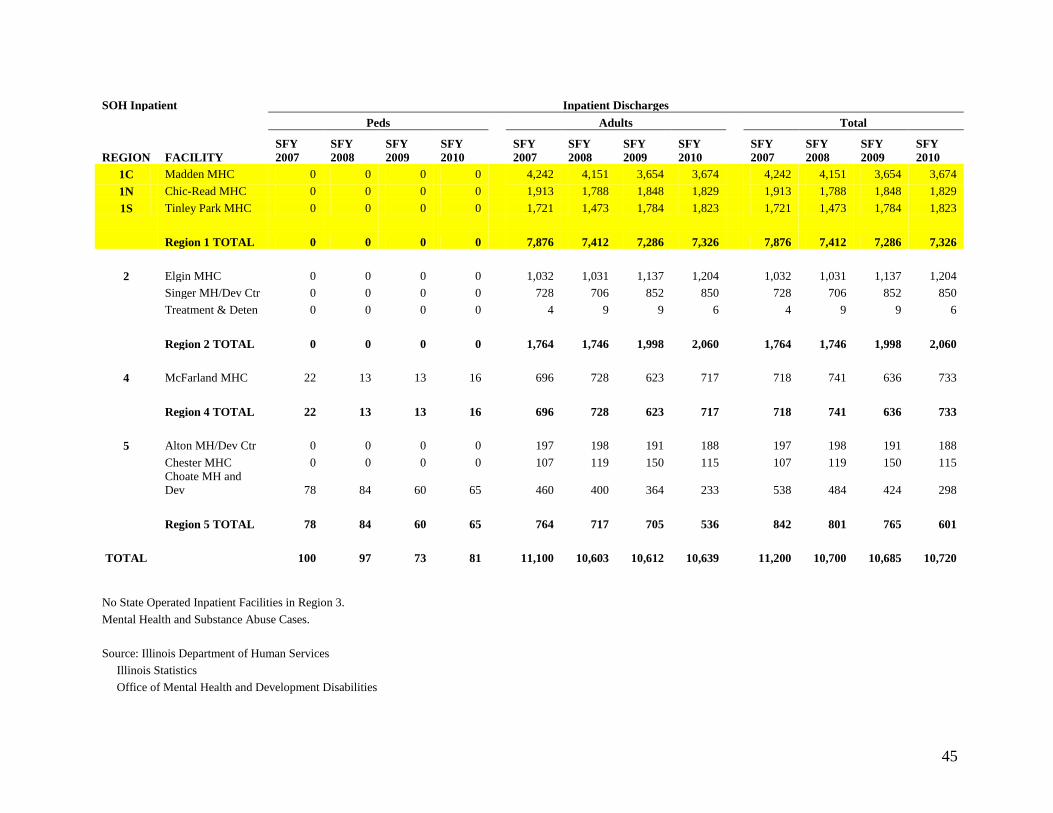
45
SOH Inpatient Inpatient Discharges
Peds
Adults
Total
REGION FACILITY
SFY
2007
SFY
2008
SFY
2009
SFY
2010
SFY
2007
SFY
2008
SFY
2009
SFY
2010
SFY
2007
SFY
2008
SFY
2009
SFY
2010
1C Madden MHC 0 0 0 0
4,242 4,151 3,654 3,674
4,242 4,151 3,654 3,674
1N Chic-Read MHC 0 0 0 0
1,913 1,788 1,848 1,829
1,913 1,788 1,848 1,829
1S Tinley Park MHC 0 0 0 0
1,721 1,473 1,784 1,823
1,721 1,473 1,784 1,823
Region 1 TOTAL 0 0 0 0
7,876 7,412 7,286 7,326
7,876 7,412 7,286 7,326
2 Elgin MHC 0 0 0 0 1,032 1,031 1,137 1,204 1,032 1,031 1,137 1,204
Singer MH/Dev Ctr 0 0 0 0 728 706 852 850 728 706 852 850
Treatment & Deten 0 0 0 0 4 9 9 6 4 9 9 6
Region 2 TOTAL 0 0 0 0
1,764 1,746 1,998 2,060
1,764 1,746 1,998 2,060
4 McFarland MHC 22 13 13 16
696 728 623 717
718 741 636 733
Region 4 TOTAL 22 13 13 16
696 728 623 717
718 741 636 733
5 Alton MH/Dev Ctr 0 0 0 0 197 198 191 188 197 198 191 188
Chester MHC 0 0 0 0 107 119 150 115 107 119 150 115
Choate MH and
Dev 78 84 60 65 460 400 364 233 538 484 424 298
Region 5 TOTAL 78 84 60 65 764 717 705 536 842 801 765 601
TOTAL
100 97 73 81
11,100 10,603 10,612 10,639
11,200 10,700 10,685 10,720
No State Operated Inpatient Facilities in Region 3.
Mental Health and Substance Abuse Cases.
Source: Illinois Department of Human Services
Illinois Statistics
Office of Mental Health and Development Disabilities

46
*The Illinois Health Facilities Planning Board discontinued licensing substance abuse beds as a category of service on April 17, 2000. this
category was converted to medical/surgical beds.

47
Hospital Statistics
DMH Hospital Statistics - FY 03 through FY 09
FY 03 FY 04 FY 05 FY 06 FY 07 FY 08 FY 09
Total Presentations (Civil
only)
10,472 10,759 11,233 11,657 11,654 10,812 10,504
Total Admissions (Civil &
Forensics)
9,625 9,609 10,190 11,421 11,349 10,729 10,677
Civil Total Admissions 8,991 8,975 9,580 10,860 10,747 10,139 10,103
Civil Adult 8,870 8,844 9,462 10,770 10,668 10,063 10,045
Civil Child & Adolescents 121 131 118 90 79 76 58
Forensics total 634 634 610 561 602 590 574
Forensics Adult 611 614 593 546 587 573 565
Forensics Child &
Adolescents
23 20 17 15 15 17 9
Total Triage 1,482 1,784 1,653 797 907 673 401
Total Transfers-in 409 414 466 232 211 246 271
Civil total 365 364 410 166 152 184 200
Civil Adult 365 364 410 166 152 184 200
Civil Child & Adolescents 0 0 0 0 0 0 0
Forensics Total 44 50 56 66 59 62 71
Forensics Adult 43 50 55 66 59 62 71
Forensics Child &
Adolescents
1 0 1 0 0 0 0
Individuals with 3+
admissions Civil only
569 536 592 639 630 585 626
Individuals with 3+
admissions Civil only
forensics
0.0632 0.0597 0.0617 0.059 0.059 0.055 0.059
FY
03
FY
04
FY
05
FY
06
FY
07
FY
08
FY
09
All Admissions/100,000 78 77 82 92 91 86 86
Total Civil Admissions/100,000 72 72 77 87 87 82 81
Adult Civil Admissions/100,000 97 96 103 117 116 110 109
Child & Adolescents Civil
Admissions/100,000
4 0 4 3 2 2 2
Total Forensics Admissions/100,000 5 5 5 5 5 5 5
Adult Forensics Admissions/100,000 7 7 6 6 6 6 6
Child & Adolescents Forensics Admissions/100,000
1 1 1 0 0 1 0
Co-Occurring Disorders 4,613 5,389 5,417 4,916 4,991 4,569 4,491
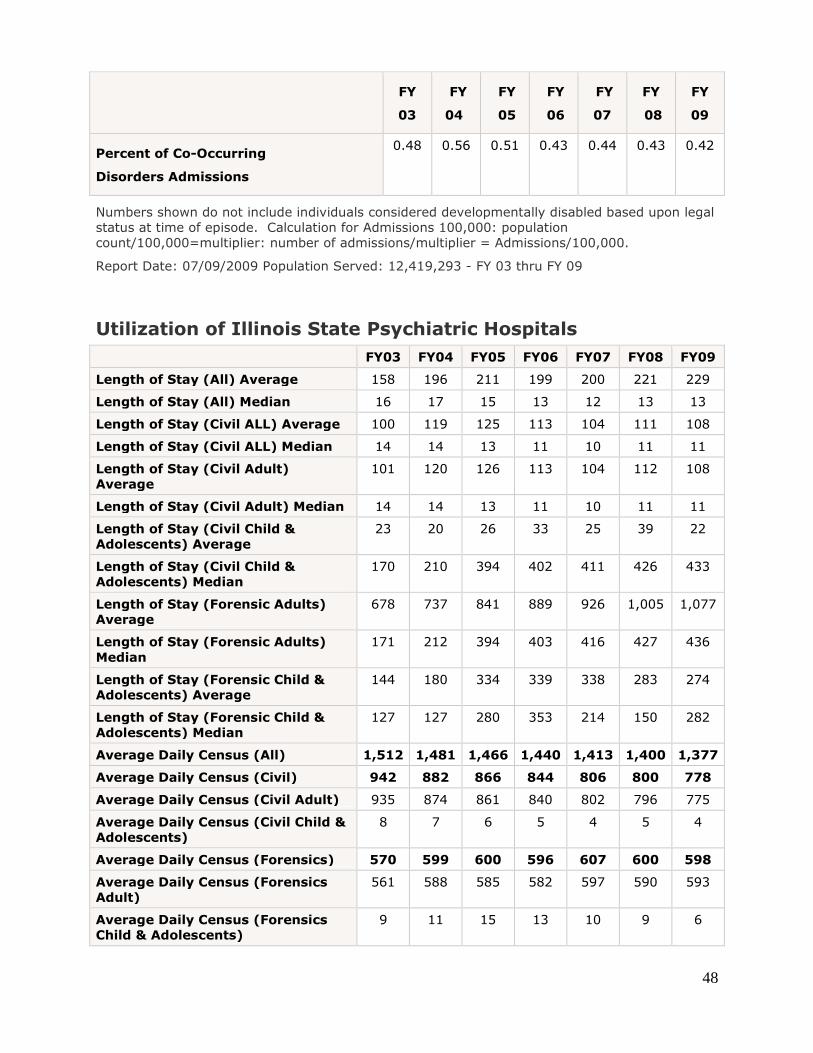
48
FY
03
FY
04
FY
05
FY
06
FY
07
FY
08
FY
09
Percent of Co-Occurring
Disorders Admissions
0.48 0.56 0.51 0.43 0.44 0.43 0.42
Numbers shown do not include individuals considered developmentally disabled based upon legal
status at time of episode. Calculation for Admissions 100,000: population
count/100,000=multiplier: number of admissions/multiplier = Admissions/100,000.
Report Date: 07/09/2009 Population Served: 12,419,293 - FY 03 thru FY 09
Utilization of Illinois State Psychiatric Hospitals
FY03 FY04 FY05 FY06 FY07 FY08 FY09
Length of Stay (All) Average 158 196 211 199 200 221 229
Length of Stay (All) Median 16 17 15 13 12 13 13
Length of Stay (Civil ALL) Average 100 119 125 113 104 111 108
Length of Stay (Civil ALL) Median 14 14 13 11 10 11 11
Length of Stay (Civil Adult)
Average
101 120 126 113 104 112 108
Length of Stay (Civil Adult) Median 14 14 13 11 10 11 11
Length of Stay (Civil Child &
Adolescents) Average
23 20 26 33 25 39 22
Length of Stay (Civil Child &
Adolescents) Median
170 210 394 402 411 426 433
Length of Stay (Forensic Adults)
Average
678 737 841 889 926 1,005 1,077
Length of Stay (Forensic Adults)
Median
171 212 394 403 416 427 436
Length of Stay (Forensic Child &
Adolescents) Average
144 180 334 339 338 283 274
Length of Stay (Forensic Child &
Adolescents) Median
127 127 280 353 214 150 282
Average Daily Census (All) 1,512 1,481 1,466 1,440 1,413 1,400 1,377
Average Daily Census (Civil) 942 882 866 844 806 800 778
Average Daily Census (Civil Adult) 935 874 861 840 802 796 775
Average Daily Census (Civil Child &
Adolescents)
8 7 6 5 4 5 4
Average Daily Census (Forensics) 570 599 600 596 607 600 598
Average Daily Census (Forensics
Adult)
561 588 585 582 597 590 593
Average Daily Census (Forensics
Child & Adolescents)
9 11 15 13 10 9 6

49
FY03 FY04 FY05 FY06 FY07 FY08 FY09
Total Number of Residents & Home
Visits on 7/09/09.
1,410 1,369 1,402 1,322 1,373 1,353 1,319
Total Number of Civil Residents and
Home Visits on 7/09/09.
799 760 791 706 762 742 709
Total Number of Civil Adult
Residents and Home Visits on
7/09/09.
797 757 786 705 757 742 707
Total Number of Civil Child &
Adolescents Residents and Home
Visits on 7/09/09.
2 3 5 1 5 0 2
Total Number for Residential and
Home Visits on 7/09/09
611 609 611 616 611 611 610
Total Number for Adult Residential
and Home Visits on 7/09/09
601 593 595 601 603 601 605
Total Number for Child
& Adolescents Residential and
Home Visits on 7/09/09
10 16 16 15 8 10 5
Utilization of Illinois State Psychiatric Hospitals
FY 03 FY 04 FY 05 FY 06 FY 07 FY 08 FY 09
Total Separations 10,190 10,058 10,625 11,731 11,496 10,988 10,979
Total Discharges (Civil &
Forensics)
9,772 9,641 10,150 11,498 11,286 10,739 10,708
Civil Total Discharge 9,255 9,052 9,584 10,981 10,729 10,211 10,171
Civil Adult 9,122 8,922 9,468 10,888 10,654 10,131 10,115
Civil Child & Adolescents 133 130 116 93 75 80 56
Forensics Total 517 589 566 517 557 528 537
Forensic Adults 502 578 553 506 538 517 525
Forensic Child &
Adolescents
15 11 13 11 19 11 12
Total Transfers-Out (Civil
& Forensic)
418 417 475 233 210 249 271
Civil Total 368 359 408 161 138 173 200
Civil Adult 368 359 408 161 138 173 200
Civil Child & Adolescents 0 2 0 0 0 0 0
Forensics Total 50 58 67 72 72 76 71
Forensics Adult 49 58 65 72 72 76 71
Forensics Child &
Adolescents
1 0 2 0 0 0 0
Report date 07/09/2009 Population Served 12,419,293
http://www.dhs.state.il.us/page.aspx?item=33869
1
Illinois Regional Integrated
Behavioral Health Networks
Region 2
Draft Report
2
Table of Contents Topics Page # Region 2 Plan
Background 3-4
Access 4-5
Funding 5-6
Quality Improvement 6-7
Technology 7-8
Workforce 8-9
Meetings
Letter of Invitation 10
Agenda Nov. 30 11
Minutes Nov. 30 12-13
Small Group Responses Nov. 30 14-16
Agenda Dec. 21 17
Minutes Dec. 21 18-19
Small Group Responses Dec. 21 20-26
Agenda Jan. 11 27
Minutes Jan. 11 28-29
Appendix
PA 97-0381 30-33
Questionnaire 34-40
Region 2 Contact List 41-68
Psychiatric & Licensed Staffed Beds 69-70
Statewide & Behavioral Health Primary
Diagnoses Discharges 71
State Operated Hospitals Inpatient Discharges 72
ILHFB Bed Totals 73
Hospital Statistics 74-76
3
Illinois Regional Behavioral Health Networks
For hospital, primary care, mental health, substance abuse and
other community-based providers
Region 2
Note: The content of this report does not reflect the opinion or position of the Illinois Hospital
Association.
Background
On August 15, 2011, Governor Pat Quinn signed into law House Bill 2982 as Public Act 97-
0381, which creates the Regional Integrated Behavioral Health Networks Act. The act provides
a platform to establish Regional Integrated Behavioral Health Networks. Its purpose is to ensure
and improve access to appropriate mental health and substance abuse services throughout Illinois
by: organizing systematically all relevant health, mental health, substance abuse, and other
community resources among regional providers; developing a mechanism to use regional
resources efficiently and effectively; and serving as a catalyst for innovation and collaboration.
Under the act, each Behavioral Health Regional Network shall develop a strategic plan for its
respective region that addresses the inventory of existing services, identifies community needs
and defines opportunities to improve access to care. The act contemplates a broad-cross section
of the mental health, substance abuse, health, and social services community that will be
involved in the development and implementation of the plan. Collaboration among all of the
relevant community resources will be essential to accomplish the purposes of the act and to build
effective, coordinated and comprehensive systems of care.
In partnership with the Illinois Department of Human Services (DHS), Division of Mental Health
(DMH) and Division of Alcoholism and Substance Abuse (DASA), the Illinois Hospital
Association (IHA)and others convened a group of behavioral health providers in the State’s DHS
Region 2 to begin to identify existing services in the region, strategies for improving the
behavioral health services delivery system, including timely and appropriate access to medical as
well as behavioral health services, and ways in which providers can begin working together to
improve access to services and patient outcomes.
This plan outlines the priorities and recommendations for DHS Region 2, articulated by
participating service providers in three Region 2 meetings. At the first meeting held at FHN
Health System, Freeport, on November 30, 2011, providers defined their vision for behavioral
health care services in the future and outlined priority issues and areas of focus. During the
second meeting at Rosecrance Health Network, Rockford, on December 21, 2011, participants
identified strategies to improve priority areas of concern listed in this plan. In the third meeting
at Family Service and Community Mental Health in McHenry on January 11, 2012, the group
reviewed and provided input on the first draft of a regional plan and provided additional
feedback on data sources and trends they have experienced over the past 12 months.
This plan is a template that recognizes the shortcomings and inefficiencies of the present system,
but also embraces partnerships that promise better coordination of care, across primary medical

4
and behavioral care, using technology and research to improve outcomes. It is an interactive
process and one that will evolve with a changing health care and economic landscape and will
depend on the continued commitment of all stakeholders—state agencies, primary medical,
hospitals, and behavioral health providers. It builds on community strengths to achieve a system
of care that delivers the right care, at the right time, in the right place.
1. Access for All Who Need It
First and foremost, providers were concerned about access to behavioral health services
for all residents of the region. Patients and consumers seeking behavioral health care
currently find long waiting lists for outpatient care, hospital emergency department visits,
admission to state-operated psychiatric hospitals, and substance abuse treatment
programs. Persons who are not covered by programs such as Medicaid or Medicare are
particularly compromised by continuous budget cuts. Patient-centered models of care
that work well offer improved access as well as outcomes integrate primarily medical and
behavioral health services. Integrated care will provide the patient and his/ her family
with health services needed for both physical and behavioral health, while also serving
the uninsured, with a hospital approach to health care and wellness.
Primary care integrated with behavioral health services is currently being implemented in
a couple of rural communities and is being introduced to federally qualified health
centers, rural health clinics and family practice clinics. It will be important for these new
integrated service models to coordinate care across and among community mental health
centers, substance abuse treatment and prevention service providers, hospitals, health
departments, and other community-based service providers. A care coordination
component, along with these integrated models, will help patients and their families
navigate their health care journey as they move from assessment, diagnosis, treatment,
follow-up and pharmaceutical compliance.
In addition to care coordination, Region 2 planning participants indicated a need for crisis
stabilization services and ongoing treatment resources for persons in need of care.
Region 2 would like to explore alternative strategies to expand access to behavioral
health services through more appropriate settings to stabilize patients in crisis, provide
counseling to keep patients out of crisis, assist patients with life challenges, and provide
outreach to patients to improve their quality of life through community resources,
employment, housing, etc. Notwithstanding the value of providing alternative services,
providers emphasized the need to maintain access to the full continuum of care, from
acute care to rehabilitative services.
Region 2 planning participants highlighted the need to eliminate “silo” thinking and
management principles within state agencies that minimize the ability of providers to
work across the spectrum of behavioral health programs and services. Understanding the
unique needs of mental health, substance abuse, prevention, and dual diagnosis clients is
important for providers and state agency leaders. However, there is a need for some level
of cross-training, common definitions and language, and standardization that will help
behavioral health providers work jointly towards a more holistic approach to behavioral
and physical health care for clients in Illinois.
5
Recommendations
Integrate behavioral health services and primary care through the use of patient-
centered entities that are funded to support these new strategies. A patient-centered
navigator could be one possible solution.
Coordinate education, advocacy and support for patients and their families who
navigate through the service delivery system.
Identify a consistent, common patient access system to ensure patients receive the
right level of care at the right time and in the right setting (inpatient, outpatient,
treatment, counseling, and prevention).
Provide direct inpatient services before crisis occurs.
Develop one electronic billing system to integrate administrative functions at the state
level and standardize forms and processes.
Develop more outpatient services, crisis stabilization centers and non-traditional
counseling services to keep patients out of the emergency departments of hospitals
and state-operated facilities.
Utilize community-based mental health centers, substance abuse providers, home
health agencies and others to track and monitor patients with chronic conditions to
keep them out of crisis. Electronic HIE may assist here.
Provide resources to link behavioral and physical health providers through the use of
electronics and technology to ensure access to services through all points of entry into
the behavioral and physical health care systems.
Expand access to inpatient beds in areas with long waiting lists and professional
shortage areas.
Facilitate communication between mental health providers and pharmacists to
coordinate the pharmaceutical needs of the patient with physical health conditions to
improve patient education and compliance with the patient’s pharmacy plan.
2. Funding
There was an in-depth discussion on how funding should be redesigned to support
behavioral health services in the future. There was consensus among providers that
funding needs to follow the patient through the system of care. Providers would like to
work with the department and statewide organizations to plan for the use of state, federal
and commercial insurer funds that better meets the needs of patients and their families.
For example, by decreasing emergency department usage, those resources can be used to
provide additional counseling and prevention services. These funds could be used to

6
create alternative strategies such as crisis stabilization centers and medication
management services. In the future, providers agreed that moving to more outpatient
services will help to reduce the cost of care and provide more timely services for patients
and their families. Capitated funding alternatives would allow more flexibility utilizing
funding for locally identified needs, addressing gaps and developing services where
needed most as determined by local stakeholders.
There is a recognition that multiple providers may need to form a collaborative to address
common needs. For example, multiple providers would work together to fund
transportation services in a region or to create alternative setting for service delivery. If
the state currently provides transportation for the involuntary patients, can multiple
providers pool resources to provide transportation for the voluntary patients?
Recommendations
Lead a performance-based funding redesign initiative to define behavioral health
quality indicators, assessment strategies, data collection, analysis, and reporting
requirements across both mental health and substance abuse providers.
Identify public and private sector funding to pilot non-traditional services in the
region and to provide the necessary equipment to connect behavioral health providers
to the state’s health information exchange (HIE) and telepsychiatry services.
Design funding mechanisms that follow the patient through the behavioral health
system and provide support services to clients as they transition from supported living
services to other community-based systems of care.
Provide coverage for the uninsured population in Illinois.
Create administrative service organizations to support to behavioral health providers
in the region, especially for those common services such as transportation, non-
traditional service models, etc. With existing thin administrative margins, this would
make the service delivery system more effective and efficient to operate.
Create one electronic billing system for behavioral health providers to streamline the
different billing processes currently used by different state agencies.
3. Quality Improvement
The planning participants requested that state agencies work closely with existing
providers in the region to identify quality measures for behavioral health clients, to
improve data collection, analysis and utilization, and to develop funding strategies based
upon quality outcomes. The quality improvement process should be driven by
comprehensive and accurate assessments, self-assessments, shared decision-making and
uniform measures when appropriate. Members pointed to DASA’s use of national
assessment uniform measures that assisted substance abuse providers to collect and
utilize common data. Planning participants need more information on evidence-based,
emerging best practices in other state and regions that have improved patient outcomes.

7
Recommendations
Relevant state agencies should engage in a meaningful dialogue with providers
regarding uniform measures needed to assess patient outcomes across the continuum
of behavioral health care service providers.
Encourage use of core measures across the continuum, including outpatient
behavioral health.
Develop training curriculum for behavioral health providers on existing core
measures and best practices to implement a quality improvement program.
Appropriate state and federal should continue to identify best practices and evidence-
based strategies to improve the delivery of quality care.
The Department of Human Services, in partnership with its state partners, should host
training sessions for behavioral health providers to provide a consistent message on
rules related to Emergency Medical Treatment and Active Labor Act (EMTALA) and
patient confidentiality.
4. Technology
Region 2 providers would like the state to assist them in utilizing technology to improve
access to care and create efficiencies in the system. Providers would like to integrate
behavioral health services into the patient’s electronic medical records and have access to
the patient’s complete health record when caring for the patient. Creating an
authorization form for patients to allow their behavioral health provider to have access to
their electronic medical record will assist providers in assessing and treating the
behavioral health needs of their patients.
Providers would also like to better utilize technology to reduce duplication in the
behavioral health system. Patients receive numerous assessments as they move from the
community mental health center to the specialist office to the hospital and back to the
community mental health center. This requirement creates redundancy in the process,
utilizes resources that are unnecessary and delays access to care for the patient and their
family. Providers would like to utilize technology to record assessment information at
the point of entry and build the patient record as they move among health care providers.
Providers would like to work with state leaders to develop standardized forms when
appropriate to collect reliable and consistent data on basic information that is common
across behavioral health providers. Standardized forms will simplify the administrative
process and streamline the data available to providers and the state.
Providers also would like to work with the state and its partners to expand access to
psychiatrists and other specialty providers through telemedicine and telephonic services,
especially in the rural parts of the region. Telepsychiatry is currently working in
8
several communities to provide assessment, treatment, counseling, and follow-up
services. However, the cost of equipment ($20,000) can be a barrier to implementation,
especially in rural community mental health centers and substance abuse centers.
Recommendations
Work with the Office of Health Information Technology (OHIT) and the state HIE
Advisory Committee to integrate behavioral health services into the state’s HIE
planning and implementation strategies.
Convene a network of providers to explore innovative strategies to reduce duplication
in assessments, patient forms, and provider reporting requirements, through
technology programs and software. This duplication increases cost to the behavioral
health system and delays patient care.
Work with state, federal and private funders to identify resources to expand access to
health information and telemedicine equipment.
Create a bed availability central depository system to manage patient intake and
referral process. It is expected that a centralized system will help providers avoid
EMTALA concerns.
5. Workforce
Region 2 providers recognized a need to develop the workforce to manage care in the
new service delivery system. There will be a need for new workers such as care
coordinators and patient navigators, information technology specialists, home health
services, and family and patient educators. Staff from the different specialty care
providers will need to be cross-trained to understand the needs of patients as they move
from one type of behavioral health provider to another, especially for those with multiple
chronic conditions.
Providers continue to struggle with workforce shortages especially in the rural parts of
the region. Utilizing vocational and community college training programs, providers will
work to identify new members of the behavioral health workforce, and in some rural
areas, utilize telemedicine services to access specialty services.
As the workforce changes, the group agreed that new information and professional skills
will be needed by those in the future workforce to address patient care such as: growing
quality measures, cross-training across specialty services, interactions with law
enforcement, primary care integrations, electronic medical records, new billing and
coding data, and ongoing evidence-based practice training. Linkages with higher
education will continue to be a priority as these new members of the workforce are
developed.
The planning participants recommended education services be made available to family
members who can act as first responders to persons in need of behavioral health services.
Current programs designed to train family members should be analyzed and expanded

9
where appropriate. Mental health agencies should have first aid toolkits for families who
serve as first responders.
The group also discussed the need for providers to reach out to other community-based
organizations that link services for patients and families like housing and transportation
services to ensure educational services are available.
Recommendations
Identify new skills needed by the workforce of the future and design payment systems
to fund those provider services (care coordinators, patient navigators, etc.).
Remove regulatory barriers that limit the existing workforce from transitioning to the
new system of behavioral health services.
Work with community colleges and vocational schools to recruit and train new
behavioral health service providers.
Train emergency department physicians, especially in hospitals that do not provide
psychiatric services, to ensure best practices for behavioral health patients are known
and utilized.
Assess current staff salaries and reform reimbursement rates to attract a skilled
workforce.
Provide a forum for providers to discuss the changing workforce needs, identify
existing education resources, discuss potential workforce barriers, and develop a plan
to expand educational services for behavioral health providers.
Develop and provide incentives for workforce shortage areas of the state.
10
November 15, 2011
Name
Title
Organization
Address
City, State Zip
Dear:
As providers, we know that persons with mental and substance use illnesses in Illinois must navigate a
complex amalgam of services that are inconsistently available and accessible. Many seek care from us in
crisis because they could not obtain more timely or appropriate care. Our state and federal fiscal crises
have translated into the loss of essential behavioral health services particularly in rural Illinois. Yet,
despite these challenging circumstances, we can also identify opportunities to improve care. Some of
these opportunities stem from health reform; others are being generated by our own strategies to serve our
patients and communities. One such opportunity is being presented to us by the recent enactment of
House Bill 2982 – Public Act 97-0381, which creates the Regional Integrated Behavioral Health
Networks Act.
The bill establishes Regional Integrated Behavioral Health Networks to ensure and improve access to
appropriate mental health and substance abuse services throughout Illinois by systematically organizing
all relevant health, mental health, substance abuse, and other community resources among regional
providers, to develop a mechanism to use regional resources efficiently and effectively.
Under the Act, each Behavioral Health Regional Network shall develop a strategic plan for its respective
region that addresses the inventory of existing services, identifies community needs and defines
opportunities to improve access to care. The Act contemplates a broad-cross section of the mental health,
substance abuse, health, and social services community will be involved in the development –and
implementation—of the plan. Collaboration among all of the relevant community resources will be
essential to accomplish the purposes of the Act and to build effective, coordinated and comprehensive
systems of care.
We would like to invite you to participate in the first Behavioral Health Regional Network meeting for
DHS Region 2. The meeting will take place Wednesday, November 30 from 10:00 am to 1:00 pm at
FHN Memorial Hospital in Freeport, IL.
If you have any questions or concerns, please contact IHA Staff: Lori Williams, at 217-541-1164 or
[email protected] or MaryLynn M. Clarke at 217-541-1154 or [email protected].
To confirm your attendance, please contact Abby Radcliffe at 217-541-1178 or email your response to
Thank you,
MaryLynn McGuire Clarke
Sr. Director, Health Policy & Regulation
Lori Williams
V.P. Small & Rural Hospital Affairs
11
Illinois Behavioral Health Network Meeting – Region 2
November 30, 2011, 10:00 a.m. – 1:00 p.m.
FHN Memorial Hospital, 1045 W. Stephenson Street, Freeport, IL
Agenda
I. WELCOME & INTRODUCTIONS ................10:00 ............................... Dan Neal
II. OVERVIEW OF HB 2982 (PA 97-0381) .........10:20..MaryLynn McGuire Clarke
III. REGIONAL PLAN DISCUSSION GROUPS..10:25 ................................. Groups
What should the behavioral health system look like 3 years from now?
What would be the key components of the new behavioral health system?
Are there immediate actions that could be taken to improve access to behavioral
health services in this region? If so, what are they?
IV. SMALL GROUP REPORTS ............................11:30 ..................... Abby Radcliffe
V. SETTING PRIORITIES & NEXT STEPS ....12:15 ............................... Dan Neal
VI. ADJOURNMENT & NEXT MEETING ........1:00 ................................. Dan Neal

12
Illinois Behavioral Health Network Meeting – Region 2
November 30, 2011
FHN Memorial Hospital, 1045 W. Stephenson Street, Freeport, IL
MaryAnn Abate, Rosecrance
Jennifer Avrand, FHN-Family Counseling Center
Susan Ayers-Krause, Pioneer Center
Eric Benink, OSF SHMC
Karen Beyer, Ecker Center for Mental Health
Barbara Brooks, DHS
David Deopere, Robert Young Center
Emily Dykstra, CGH
Michael Flora, Ben Gordon Center
Michael Freda, Robert Young Center
Ann Gantzer, SwedishAmerican
Robin Garvey, State
David Gomel, Rosecrance
Filiz Gunay, DuPage County Health Department
Karen Hines, Nicasa
Patricia Kates-Collins, DASA
Deb Keaschall, CGH
Patti Kimbel, Vista Medical Center West
Rodger J. Kinard, PhD, Willowglen Academy
Teddi Kruchman, Elmhurst Hospital
Amparo Lopez, DHS Region 2
MaryLynn McGuire Clarke, IHA
Nancy Monroe, RMH
Pamela Morzos, McHenry County Dept. of Health
Deanna Murray, RMH
Diane Murray, Delnor
Dan Neal, FHN
Larry Prindaville, Sinnissippi
Abby Radcliffe, IHA
Linda Rice, Morris Hospital
Jim Sarver, Sinnissippi Centers
Sue Schroeder, Stepping Stones
Rob Schwichow, Sherman
Linda Snelten, Nicasa
Eldon Wigget, State
I. Welcome & Introductions
Dan Neil called the meeting to order at 10:00 a.m. and those in attendance introduced
themselves.
II. Overview of HB 2982 (PA 97-0381)
MaryLynn McGuire Clarke gave an overview of the legislation which requires the
Department of Human Services to create Regional Behavioral Health Networks in each
DHS region to ensure and improve access to behavioral health services. The networks
will work collaboratively to develop region-specific plans. The legislation also created
the Regional Integrated Behavioral Health Networks Steering Committee comprised of
state agencies to coordinate efforts among planning regions.
III. Regional Plan Discussion Groups
Participants were divided into groups to discuss three questions: 1) What should the
behavioral health system look like three years from now? ; 2) What would be the key
components of the new behavioral health system? ; and 3) Are there immediate actions
that could be taken to improve access to behavioral health services in this region? If so,
what are they?

13
IV. Small Group Reports
The four small groups reported on their findings. Information from the break-out groups
is included in the attached document.
V. Setting Priorities & Next Steps
Information collected at the meeting will be assembled by IHA. A focus on priorities and
developing specifics of the plan will be examined at the next meeting.
VI. Adjournment & Next Meeting
Dan noted that the next meeting will be held Dec. 21 at 10:00 a.m. He adjourned the
meeting at 1:00 p.m.
14
Nov. 30 Small Group Responses
Question 1: What should the behavioral health system look like three years from now?
Network is large, need smaller groups, all medical providers linked to mental health
systems within that local region for all patients
Uninsured population should be included, no disparity
Care coordination, individual primary care coordination
Strong partnerships, collaboration, continuum of care meetings, agreements with all
levels (eliminate silos)
Improved communication capability, including access to data, re: patient clinical data
Reduction of duplication
Behavioral health access for all, payers for all seeking care/services
Medical homes include all behavioral health
Plenty of crisis stabilization beds
Federally Qualified Health Centers (FQHCs) need to be a big part of the picture
Demonstrate outcomes better
More community mental health and substance abuse money, state funding
Integrated set of rules, re: confidentiality and have laws align with access needs
EMTALA compliance for all
Allocate resources to region
Open access-service on demand
Interstate agreements established
Increase outpatient services for meds/counseling, etc.
Uniform Screening and Referral Form (USARF) requirements, resource intensive
Merge public policy, licensure mergers
Emergency Department not appropriate holding area, triage crisis establishment needed
Improve med student/med prof education
Distribute mental health professionals proportionately and have enough providers for all
ages to have the capacity to support timely access
Streamline mental health P & C process
No wrong door for persons with behavioral health
Fully integrated approach
Colocation
Stigma reduction
Consumer and family driven care, shared decision making
Not driven by funding sources, driven by medical necessity
Increase in community programming at every level
Increase in crisis, residential innovation, other models
Comprehensive
Explore telepsych laws
Increase in mental health services to intellectual and developmental disabilities
population
Increase in private, local psych beds

15
Question 2: What would be the key components of the new behavioral health system?
More home care, more coordination, more long term care for the chronically ill
Increased use of telepsych, telesocial work
Access to needed medication
Central access, criteria the same, continuity
More Standardization is needed
Colocation of entities
More use of evidence-based practices including use of innovative emergency department
behavioral health models
More substance abuse centers
More inpatient beds, residential, housing, and outpatient facilities
Use of crisis stabilization, solution focused
Community education for all (police, EMS, etc.) as first responders are the key
Money should follow clients
Full continuum, prevention, education, assessment, treatment
Outpatient-counseling for all, psychiatry, case management, pre-screener, etc.
Community triage should be used
Question 3: Are there immediate actions that could be taken to improve access to
behavioral health services in this region? If so, what are they?
Make sure that all are involved and there is an incentive to participate
Need for more local partnerships and stronger collaboration, network meetings
Working on electronic medical health records
Look at DCFS area networks/structures and integrate with children services
Use RIN numbers, have central access, local level
Not shifting money away from existing mental health resources
Know resources available
Continuum of care meetings
Fund raising, foundation resources
State should evaluate public spending, misuse of state funds
Incentives for mental health prevention and care
EMTALA adherence
Initiate triage center approach to effectively direct patients to appropriate level of care
Submission of proposals ASAP
No closure of seven state facilities until alternatives/options established
Encourage clients to become registered voters
Governor needs to hear voice of community, let areas of state tell him, and Legislative
reps need to hear voices as well
More community provider representation /state behavioral health strategic planning
process
Funding, uninsured, redefine eligible criteria for services
Suggest pilots for consumers/uninsured, data information to support those pilots and
expand current demonstration projects
Allow providers to manage care and funding for consumers at local level
Information system-interoperability, shared, privacy protections, integrate across system

16
Work on the shortage of psychiatrists
Cooperation program with FQHCs
Medical home for behavioral health
Fund telepsychiatry

17
Illinois Behavioral Health Network Meeting – Region 2
December 21, 2011, 10:00 a.m. – 1:00 p.m.
Rosecrance Griffin Williamson Campus, Community Room,
1601 North University Drive, Rockford, IL
Agenda
I. WELCOME ........................................................10:00 ............................... Dan Neal
II. SUMMARY OF FIRST MEETING.................10:20 ............................. ..Dan Neal
III. FOCUS ON PRIORITIES…………………….10:25 .................................. Groups
WORKFORCE:
What specific training is needed for existing workforce?
What are the new skills that are needed?
What are regulatory barriers to workforce utilization?
What are the specific training needs for dual diagnosis patients?
PREVENTION:
What are the current prevention services?
What new prevention services are needed?
DELIVERY SYSTEM:
How would you recommend we fill the gaps in the service delivery system?
Are there new models that would be effective in this region?
TRANSPORTATION:
Where are the transportation gaps (unfunded, Medicaid, others)?
What alternatives can you suggest in your community to provide
transportation?
PAYMENT DESIGN:
What services are not currently reimbursed that should be?
How should the payment system by redesigned to better meet the client’s needs?
IV. SMALL GROUP REPORTS ............................11:30 .............................. Everyone
V. SETTING PRIORITIES & NEXT STEPS ....12:15 ....................... Lori Williams
VI. ADJOURNMENT & NEXT MEETING ........1:00 ................................. Dan Neal
January 11, 2011: 10:00 a.m.-1:00 p.m.

18
Illinois Behavioral Health Network Meeting – Region 2
December 21, 2011
Rosecrance Griffin Williamson Campus, Community Room,
1601 North University Drive, Rockford, IL
Mary Ann Abate, Rosecrance
Susan Ayers-Krause, YSB/Pioneer Center
Carolyn Bengston, Rockford Memorial Hospital
Karen Beyer, Ecker Center for Mental Health
Hugh Brady, NAMI, IL
Robin Cabral, IL Children’s Mental Health Part.
Laura Crain, Woodstock School District #200
Phil Eaton, Rosecrance
Robin Garvey, NAMI, IL
David Gomel, Rosecrance
Ann Guild, Illinois Hospital Association
Filiz Gunay, DuPage County Health Dept.
Gary Halbach, Remedies Renewing Lives
Erin Harsevoort, NAMI IL
Karen Hines, Nicasa
Abby Hornbogen, Provena St. Joe’s-Joliet
Lisa Johnson, Independence Center
Doug Jones, Provena St. Mary’s Hospital
Patti Kimbel, Vista Medical Center West
Betty Kinard, Willowglen Academy
Rodger Kinard, Willowglen Academy
Lorraine Kopczynski, Pioneer Center
Sandy Lewis, McHenry County MHB
Bob Lesser, McHenry Co. MHB
Patricia Lindquist, DHS/DMH Region 2
Amparo Lopez, DHS/DMH Region 2
Michelle McMullin, AID
Pamela Morzos, McHenry Co. Dept. of Health
Deanna Murray, Rockford Memorial Hospital
Dan Neal, FHN
Lori Nelson, Family Service & CMH Center
Larry Prindaville, Sinnissippi
Faye Redmond, Advocate Good Shepherd Hosp.
Abby Radcliffe, Illinois Hospital Association
Cassie Reese, Provena St. Joe’s-Joliet
Linda Rice, Morris Hospital
Sue Schroeder, Stepping Stones
Rob Schwichow, Sherman Hospital
Sheila Senn, Centegra Health System
Linda Snelten, Nicasa
Gail Stickle, KSB Hospital
Ted Testa, Lake County Health Department
Eldon Wigget, MDH
Lori Williams, Illinois Hospital Association
I. Welcome & Introductions
Dan Neal called the meeting to order at 10:00 a.m. and those in attendance introduced
themselves.
II. Summary of First Meeting
Dan gave an overview of the last meeting. He thanked the group and the state for
participating in these meetings. The purpose of the group is to outline a plan for
behavioral health services in this region. The goal of the plan is to improve access to
behavioral health services in the region and work with the state steering committee to
implement changes to the system.
III. Focus on Priorities
Participants were divided into groups to discuss five topic areas: 1) Workforce; 2)
Prevention; 3) Delivery System; 4) Transportation; and 5) Payment Design. These
priority issues were identified in the first meeting. The questions on these topics will help
identify provider needs in each of the areas.
19
IV. Small Group Reports
The four small groups reported on their findings. The information from the break-out
groups is included in the attached document.
V. Setting Priorities & Next Steps
The information collected at the meeting will be assembled by IHA. A focus on a draft
plan will be discussed at the next meeting.
VI. Adjournment & Next Meeting
Dan noted that the next meeting will be held Jan. 11 at 10:00 a.m. He adjourned the
meeting at 1:00 p.m.

20
Dec. 21 Small Group Responses
WORKFORCE
Question 1: What specific training is needed for existing workforce?
Trauma informed care
Case management and medical services
Cross training
National Alliance on Mental Illness (NAMI)-partner family to family training
Recovery resilience, philosophy
Family members/clients as partners, looking from their perspective
Learning to mend bridges
De-escalation skills (not just for mental health)
Residential or vocational specialist training at community colleges including physical
education in nursing
More training in mental health for primary degree care docs, emergency department, and
other health care providers
Standardized evaluation tool
More education on IL Mental Health Code
Supervision of peer specialists to develop skills-peer supervisors come from clinical
backgrounds
Billing/support data-documentation/coding/billing, etc. Including Billing Medicaid for
wrap. Billable under Rule 132.
Clinical-short term evidence based practice training
Electronic Medical Records (EMRs)
Practice management
Sharing information-community resources, etc.
Increased knowledge and competency for clients with multiple intellectual and
developmental disabilities: triple axis syndrome, mental health, dual diagnosis
More psychiatrists/nurse practitioners that can prescribe-medication management
Education on “new structure”
Primary care integration
Department of Corrections & law enforcement
Fewer health providers for mental health and other disabilities
Training consumers to assist with management of illness, consumer empowerment
Address shortages
Evidence-based practices, evidence-informed practices, best practices (academic partners,
research, training of professionals, dual-diagnosis, co-occurring, co-morbidity)
Technology needs, EMR, meaningful use, e-training, data sharing, telepsychiatry
Family support groups
Question 2: What are the new skills that are needed?
Community-based in home care
Coaching/teaching
Empathy skills, customer service
Cultural competency
Interagency awareness

21
Assessing for suicide
Treating behavioral health as health
Preventing and dealing with violent situations
Parity-pay scale social worker, physician assistant, psychiatric, med intern, residents
Secondary education
Attraction/retention
Existing workforce—train on new system and evidence-based practices
Education for staff to see family perspective
Primary care linkage/engagement
Medical assessment, medication
Empower clients on self-care
Collaboration through networks
Question 3: What are regulatory barriers to workforce utilization?
Allied professionals being able to prescribe
Regulatory issues with home health care
Clarity on what schools can bill for Medicaid
Substance abuse/mental health rules
More family advocate services being billable
Financial barriers, state is too prescriptive
State paperwork requirements, uniform intake forms, etc.
Fear of guardianship and advocacy commission
Office of Investigator General
Credentials needed for Medicaid reimbursements and Medicaid formulary list prior-
authorization times
Ability to share patient information across settings
Stigma among peers/community/workforce
Rates for counseling—hard to get high-quality (qualified) staff. Existing: no raises, leave
Prompt payments from state
Cross train staff
FFS 2060 Rules-132 Rules (grant model moved to fee for services without fee for service
flexibility)-two separate rules make it difficult to bill- plus commercial rates. Duplication
is costly
Family Nurse Practitioner vs. Psychiatric Nurse Practitioner-Peer source payment
impacts billing and prescription differences
Collaboration by departments, regulatory requirements
Standardized assessments
Question 4: What are the specific training needs for dual diagnosis patients?
Assertive Community Treatment (ACT) funding for therapy, teams/too much regulation
Motivational enhancements, stages of change
Dual credentials, cross training
Also refers to developmental disabilities
Tool that addresses mental health and substance abuse
State agencies funding—silos

22
More wrap facilitators trained for wrap
Integrated dual diagnosis model
Number of professionals trained to address population client needs
Question 5: Extra thoughts on workforce shortages
Advance practice nurses, psychiatrists , social workers, and physician assistants are
needed
In home behavioral interventionists
Parent/peer advocates
IT specialists who understand things from a behavioral health level
Collaborative business models to build efficiencies
Resource availability
PREVENTION
Question 1: What are the current prevention services?
Victim’s services
NAMI offerings, education
Mental health first aid
Continued crisis intervention training, Critical Incident Stress Management
Community wide-destabilization
Child adolescent-prevention money gone
Community education-clients and families
School based programs-substance abuse, suicide prevention, early-intervention grants
City prevention programs-RFP
Almost all substance abuse. providers have a prevention arm
Reduction of stigma
Mental health or suicide prevention month
Secondary education services-more connections
Transitions funding would be expanded
Public health-maternal child health screenings
Legal counsel-guardianship issues
Hotline/Crisis Lines-substance abuse & suicide
Crisis intervention training for police
Providing Access to Health (PATH), Assertive Community Treatment, Community
Support Team
Family resource center, family engagement
Partners for success
Perinatal screenings
Wellness Recovery Action Plan (WRAP)
Self-help community support mentoring
Research/training brought into treatment re: co-occurring/co-morbid diagnoses through
screening and training—postpartum , cardiac, chronic conditions
Peer support
23
Question 2: What new prevention services are needed?
Schools social and emotional learning standards-making sure they are doing it, consistent
school based models
Workplaces need stress management
Whole health
Parenting classes
Partnership with faith institutions
Adult and community family
Expanded and integrated screenings-early and periodical
Need for help for those outside of diagnosis
More advocates in court system
Financial resources
Education re: successful prevention models-why are they important
Empirical evidence of success
Stigma-consumer participation
Education for school leaders, teachers, and parents
Engaged Consumer advisory committees (regional/local)
Task force developed to target consumer groups
Convener groups for providers to cut duplication
708 BDS-County Board-for Winnebago Co.
377 Board for development disabilities services
More on mental health side
Community education and data
Health plan coverage of behavioral health and substance abuse prevention
Existing screening tools to address MH
Training on what to do with tool results
Early identification
Access to care
Student education through health classes
DELIVERY SYSTEM
Question 1: How would you recommend we fill the gaps in the service delivery system?
Reauthorization issues-streamline
Medically necessity systems
Fill the gaps
Substance abuse and mental health under one umbrella-shouldn’t be unique to combine
both
Group homes are needed
Illinois should pay for needed care and assist in accessing resources
Restore non-Medicaid funding
Centralized case management-more than substance abuse and mental health-family
advocacy
Avoid duplication in systems- mental health, substance abuse, development disabilities
different providers, cuts have limited service providers, consumer choice
Access-uninsured, prompt payment

24
Record keeping-electronic medical records
More crisis beds-more short term acute care
Child plus AD-90 day window of services Screening, Assessment and Support Services
(SASS), need longer window for SASS for adults
More short term counseling services
Case management services
Integrated care models require change in providers-difficult to navigate; for Medicaid
consumers
Enroll the eligible clients into Medicaid. DHS has one point person to work with at
facility. One person at entrance of facility to get patients enrolled
Speed up Medicaid enrollment process (Elgin model)
Need pharma access-bring meds to client
New psychiatrist changes meds/cost
Home visits (home health-psych follow-up), need to promote
Living room model
Triage center-peer and non-acute model
Triage center model-stabilization, licensed behavioral health care professionals to staff
Safe place-crisis plus brief services
Licensed social worker, nurse
Hospital diversion
CMS funding for triage center
Small comparative studies (pilots-AZ)
Intake needs improved-crisis worker meets with hospital
Continuity of care from triage center to service providers
Capacity in system after hospital
Respite care will keep patients out of emergency department (DuPage County
government pays for respite)
Capacity grants-cutting
Misdiagnosis for development disabilities and mental illness-learned behavior vs.
undiagnosed mental illness
Community integrated living arrangement (CILA’s) to address dual and triple diagnosis-
specialized CILA’s
Focus on employment for adults-stigma
Delivery system is not fully integrated across the behavioral health continuum
Effective continuity of care (referral source vested in successful outcome)
More collaboration, need integration with primary care
Delivery system (agreed upon components)
Question 2: Are there new models that would be effective in this region?
System of care approach-care locally
Coordinated care models- co-locating etc...computers sharing information
Communities mentoring others
Clients need choice
Drive change through evaluation process, evidence based practices
Emergency room-different pathway for psych patients respite, crisis beds

25
Acute care needs, diversion, adult SASS model
Community triage center
Community mental health center liaison to hospital
State Operated Hospitals (SOH’s)-short length of stay, no follow-up-counseling, family
therapy, medication, no alternatives
Integrated services across continuum of service providers, including primary care
Evidence-based practice models are in silos
Early identification, prevention, service delivery, specific services
Managed care/care coordination
Crisis management, efficiencies, single access or multiple points?
Technology use-electronic medical record/telepsychiatry/meaningful use
TRANSPORTATION
Question 1: Where are the transportation gaps (unfunded, Medicaid, others)?
Billing transportation for staff time, etc.
Liability/risk issues
Funding cuts, Medicaid payment
Flexible hours
Some ambulances will not transport mental health patients
Transport can be limited by geography, inadequate bus stops, limited hours
Some local options-hospital community foundation funds but not violent patients
Transportation for children
Abuse of involuntary paperwork
Use EMTALA form instead for transport
Train lines
Public access
Patients to hospital
Trained workers for transit providers
Specific training-like seniors-paratransit senior centers
Barriers to service; hospital, ambulance, outpatient access, co-morbidity e.g. homebound
Options for transportation, identify needs in rural, urban and suburban areas
Funding; legislative barrier, transport restrictions, identify sustainable options
Service delivery; in home, home health
Question 2: What alternatives can you suggest in your community to provide
transportation?
Local solutions, county models
B.H. taxi system/community transport system/van transport, paratransit
Use of stipends (broader)
Transport plus bed broker
Videoconference-telepsychiatry , e-therapy
Transit funding
Use community supports that currently transport, e.g. EMTS/taxi and ambulances;
destigmatize
26
PAYMENT DESIGN
Question 1 and 2: What services are not currently reimbursed that should be? How should
the payment system by redesigned to better meet the client’s needs?
Wellness packages
Medical necessity system plus necessary supports, driven by need of client
Prevention
Global contracting
Flexibility
How large regions manage, how does it work
Community-based waivers
Medically indigent with same access to services
Make payments (30/90 days)
Multiple points of entry with different expectations
Streamline funding system
Pay for non-Medicaid and increase rates, model includes state in some risk
Address eligibility criteria for community services
Services based on need, not funding source
Modify Medicaid prior approval review for medications
Pay for behavioral health homes- not based on capitation, if capitation- monitor to make
sure care not withheld
Global payment that is provider centered to align incentives
Home visit payment
Many services not reimbursed/increased rates
Unfunded/charity care
Peer support
Supported employment teams
Maintenance-stabilization
Recovery based services
Transportation
Psychiatric rates increase
Medical advocacy pay
Linkage case management
Capitated risk based system
Support infrastructure (Administrative Service Organizations, compliance, HR)
Affiliations
Cost efficiencies in community based service; quantify cost to system in “unmanaged”
system-transferred to emergency room, police, jails, etc.; demands on primary care—
repeat access via crisis
Address charity care absorbed by community
Redesign funding strategy; remove silos from DMH/DASA/DCFS, etc. (other states
transferred DOC money to mental health/substance abuse, etc.)
Inform legislators re: cost/benefits-performance based

27
Illinois Behavioral Health Network Meeting – Region 2
January 11, 2012, 10:00 a.m. – 1:00 p.m.
Family Service & Community Mental Health Center, Community Room,
4100 Veterans Parkway, McHenry, IL 60050
Agenda
I. WELCOME ........................................................10:00 ............................... Dan Neal
II. SUMMARY OF SECOND MEETING ............10:20 ............................. ..Dan Neal
III. REVIEW OF PLAN/PRIORITIES………… ..10:25 ....................... Lori Williams
IV. REGION INFORMATION...............................11:30 .............................. Everyone
V. NEXT STEPS ....................................................12:15 ....................... Lori Williams
VI. ADJOURNMENT ..............................................1:00 ................................. Dan Neal

28
Illinois Behavioral Health Network Meeting – Region 2
January 11, 2012
Family Service & Community Mental Health Center, Community Room
4100 Veterans Parkway, McHenry, IL 60050
Susan Ayers-Krause, YSB/Pioneer Center
Eric Benink, OSF Saint Anthony
Karen Beyer, Ecker Center
Jayne Braden, Braden Counseling Center
Donna Buss, McHenry County MHB
James Carpenter, Pioneer Center
Andrea Gargani, Hinsdale Hospital
Robin Garvey, NAMI, IL
Ann Guild, Illinois Hospital Association
Filiz Gunay, DuPage County Health Department
Gary Halbach, Remedies Renewing Lives
Craig Harling, Provena St. Joseph, Elgin
Pat Henningsen, Ada S. McKinley
Alison Herrdejs, Consumer
Karen Hines, Nicasa
Doug Jones, Provena St. Mary’s Hospital
Patti Kimbel, Vista Medical Center West
Rodger Kinard, Willowglen Academy
Mark Klocek, McHenry Co. MHB
Teddi Krochman, Elmhurst Memorial Hospital
Arthur Krzyzanowski, Thresholds
Lisa LaForge, Family Serv. Assoc. of Elgin
Noel Lemke, Advocate Good Shepherd Hospital
Teri Lindahl, Families Etc.
Patricia Lindquist, State
Amparo Lopez, DMH
Ann May, Family Alliance
Catherine McBride, Advocate Good Shep. Hosp.
Michelle McMullin, AID
Doug Milliman, Professional Consultant
Pamela Morzos, McHenry Co. Dept. of Health
Deanna Murray, Rockford Memorial Hospital
Dan Neal, FHN
Lori Nelson, Family Service & CMH Center
Elias Palacios, Global Behavioral Health, Inc.
Abby Radcliffe, Illinois Hospital Association
Todd Schroll, McHenry Co. MHB
Sheila Senn, Centegra Health System
Jerry Skogmo, Renz Center
Ronald Smith, Consumer
Linda Snelten, Nicasa
Ted Testa, Lake County Health Department
Elizabeth Thrun, Morris Hospital
Deb Wagner, SwedishAmerican
Charla Waxman, Linden Oaks at Edward
Eldon Wigget, DMH
Lori Williams, Illinois Hospital Association
I. Welcome & Introductions
Dan Neal called the meeting to order at 10:00 a.m. and those in attendance introduced
themselves.
II. Summary of Second Meeting
Dan gave an overview of the second meeting. He thanked the group and the state for
participating in these meetings. The purpose of these three meetings is to outline a plan
for behavioral health services in this region. The goal is to develop a plan to improve
access to behavioral health services in the region and work with a state steering
committee to implement changes to the system.
III. Review of Plan/Priorities
Lori Williams noted that today’s meeting will take the priority issues that were identified
in the first two meetings and begin to craft recommendations to be part of this region’s
29
plan. Comments will be recorded and added to the plan. Lori went through each section
of the draft plan and the group made recommendations for any changes.
IV. Region Information
Some region specific data was collected. This was included in the packets and any
feedback on additional data needed would be appreciated.
V. Next Steps
The information collected at the meeting will be assembled by IHA. The updated draft
plan will be sent to the group for any other changes. This plan will then be submitted to
the State Steering Committee when they begin to meet.
VI. Adjournment
Dan adjourned the meeting at 1:00 p.m.
30
Appendix
Regional Integrated Behavioral Health Networks Act
Public Act 097-0381
An Act concerning health.
Be it enacted by the People of the State of Illinois, represented in the General Assembly:
Section 1. Short title.
This Act may be cited as the Regional Integrated Behavioral Health Networks Act.
Section 5. Legislative Findings.
The General Assembly recognizes that an estimated 25% of Illinoisans aged 18 years or older
have experienced a mental or substance use disorder, an estimated 700,000 Illinois adults aged
18 years or older have a serious mental illness and an estimated 240,000 Illinois children and
adolescents have a serious emotional disturbance. And on any given day, many go without
treatment because it is not available or accessible. Recent federal and State fiscal crises have
exacerbated an already deteriorating mental health and substance abuse (behavioral health)
treatment system that is characterized by fragmentation, geographic disparities, inadequate
funding, psychiatric and other mental health workforce shortages, lack of transportation, and
overuse of acute and emergency care by persons in crisis who are unable to obtain treatment
from less intensive community alternatives. The failure to treat mental and substance use
illnesses has human and financial consequences: human suffering and loss of function; increased
use of hospital emergency departments; increased use of all medical services; increased
unemployment, and lack of productivity; lack of meaningful engagement in family and
communities; school failure; homelessness; incarceration; and, in some instances, death. The
citizens of Illinois with mental and substance use illnesses need an organized and integrated
system of care that recognizes regional differences and is able to deliver the right care to the
right person at the right time.
Section 10. Purpose.
The purpose of this Act is to require the Department of Human Services to facilitate the creation
of Regional Integrated Behavioral Health Networks (hereinafter "Networks") for the purpose of
ensuring and improving access to appropriate mental health and substance abuse (hereinafter
"behavioral health") services throughout Illinois by providing a platform for the organization of
all relevant health, mental health, substance abuse, and other community entities, and by
providing a mechanism to use and channel financial and other resources efficiently and
effectively. Networks may be located in each of the Department of Human Services geographic
regions.
Section 15. Goals.
Goals shall include, but not be limited to, the following: enabling persons with mental and
substance use illnesses to access clinically appropriate, evidence-based services, regardless of
where they reside in the State and particularly in rural areas; improving access to mental health
and substance abuse services throughout Illinois, but especially in rural Illinois communities, by
fostering innovative financing and collaboration among a variety of health, behavioral health,

31
social service, and other community entities and by supporting the development of regional-
specific planning and strategies; facilitating the integration of behavioral health services with
primary and other medical services, advancing opportunities under federal health reform
initiatives; ensuring actual or technologically-assisted access to the entire continuum of
integrated care, including the provision of services in the areas of prevention, consumer or
patient assessment and diagnosis, psychiatric care, case coordination, crisis and emergency care,
acute inpatient and outpatient treatment in private hospitals and from other community providers,
support services, and community residential settings; identifying funding for persons who do not
have insurance and do not qualify for State and federal healthcare payment programs such as
Medicaid or Medicare; and improving access to transportation in rural areas.
Section 20. Steering Committee and Networks.
(a) To achieve these goals, the Department of Human Services shall convene a Regional
Integrated Behavioral Health Networks Steering Committee (hereinafter "Steering Committee")
comprised of State agencies involved in the provision, regulation, or financing of health, mental
health, substance abuse, rehabilitation, and other services. These include, but shall not be limited
to, the following agencies:
(1) The Department of Healthcare and Family Services.
(2) The Department of Human Services and its Divisions of Mental Illness and
Alcoholism and Substance Abuse Services.
(3) The Department of Public Health, including its Center for Rural Health.
The Steering Committee shall include a representative from each Network. The agencies of the
Steering Committee are directed to work collaboratively to provide consultation, advice, and
leadership to the Networks in facilitating communication within and across multiple agencies
and in removing regulatory barriers that may prevent Networks from accomplishing the goals.
The Steering Committee collectively or through one of its member Agencies shall also provide
technical assistance to the Networks.
(b) There also shall be convened Networks in each of the Department of Human Services'
regions comprised of representatives of community stakeholders represented in the Network,
including when available, but not limited to, relevant trade and professional associations
representing hospitals, community providers, public health care, hospice care, long term care,
law enforcement, emergency medical service, physicians trained in psychiatry; an organization
that advocates on behalf of federally qualified health centers, an organization that advocates on
behalf of persons suffering with mental illness and substance abuse disorders, an organization
that advocates on behalf of persons with disabilities, an organization that advocates on behalf of
persons who live in rural areas, an organization that advocates on behalf of persons who live in
medically underserved areas; and others designated by the Steering Committee or the Networks.
A member from each Network may choose a representative who may serve on the Steering
Committee.
Section 25. Development of Network Plans.
Each Network shall develop a plan for its respective region that addresses the following:
(a) Inventory of all mental health and substance abuse treatment services, primary health
care facilities and services, private hospitals, State-operated psychiatric hospitals, long
32
term care facilities, social services, transportation services, and any services available to
serve persons with mental and substance use illnesses.
(b) Identification of unmet community needs, including, but not limited to, the following:
(1) Waiting lists in community mental health and substance abuse services.
(2) Hospital emergency department use by persons with mental and substance use
illnesses, including volume, length of stay, and challenges associated with
obtaining psychiatric assessment.
(3) Difficulty obtaining admission to inpatient facilities, and reasons therefore.
(4) Availability of primary care providers in the community, including Federally
Qualified Health Centers and Rural Health Centers.
(5) Availability of psychiatrists and mental health professionals.
(6) Transportation issues.
(7) Other.
(c) Identification of opportunities to improve access to mental and substance abuse
services through the integration of specialty behavioral health services with primary care,
including, but not limited to, the following:
(1) Availability of Federally Qualified Health Centers in community with mental
health staff.
(2) Development of accountable care organizations or other primary care entities.
(3) Availability of acute care hospitals with specialized psychiatric capacity.
(4) Community providers with an interest in collaborating with acute care
providers.
(d) Development of a plan to address community needs, including a specific timeline for
implementation of specific objectives and establishment of evaluation measures. The
comprehensive plan should include the complete continuum of behavioral health
services, including, but not limited to, the following:
(1) Prevention.
(2) Client assessment and diagnosis.
(3) An array of outpatient behavioral health services.
(4) Case coordination.
(5) Crisis and emergency services.
(6) Treatment, including inpatient psychiatric services in public and private
hospitals.
(7) Long term care facilities.
(8) Community residential alternatives to institutional settings.
(9) Primary care services.
Section 30. Timeline.
The Network plans shall be prepared within 6 months of establishment of the Network. The
Steering Committee shall assist the Networks in the development of plans by providing technical
expertise and in facilitating funding support and opportunities for the development of services
identified under each of the plans.
Section 35. Report to Governor and General Assembly.
The Steering Committee shall report to the Governor and General Assembly the status of each
regional plan, including the recommendations of the Network Councils to accomplish their
goals and improve access to behavioral health services. The report shall also contain
performance measures, including changes to the behavioral health services capacity in the

33
region; any waiting lists for community services; volume and wait times in hospital emergency
departments for access to behavioral health services; development of primary care-behavioral
health partnerships or barriers to their formation; and funding challenges and opportunities. This
report shall be submitted on an annual basis.
Section 99. Effective date.
This Act takes effect January 1, 2012.
HB2982 Enrolled LRB097 10532 KTG 51304 b
Public Act 097-0381

34
Regional Behavioral Health Network – Region 2
Provider Questionnaire (28 Completed)
1. Wait Times
Over the past year, has your facility experienced longer wait times for patients to
receive services due to transportation, available placements, etc.? If so, what
primary factors contribute to the delays?
Staff reductions
Less state hospital beds available and overall psych beds
Inpatient for kids
Population, high medical activity, intellectual and developmental
disabilities diagnosis, availability
Lack of available transport services, nobody wanting to admit uninsured
patients
Placement issues
On a scale of 1-5 how big a problem are wait times for your facility? (1= very
important – 5 = not important at all)
#5 - 6
#4 - 2
#3 - 2
#2 - 2
#1 - 13
Have you documented these delays?
NO- 6
YES- 14
If so, what data do you have?
In agency record keeping system
Social service log of Services to Children and Family (SCF) transfers, data
available at hospital
Numbers of transfers, denials, and delays to SOH(s).
There is a waiting list and not all incoming clients have insurance
Crisis program documents amount of time consult talks to disposition a
patient to the needed level of service
Internally in specific client case records
Adults-intensive services if urgent, 15 days if non-urgent; orientation
group formed. Child and adolescent-seven days if non-urgent, referral to
family night. Psychiatry over two months if non-urgent. Once assessed,
second appointment is delayed in some programs. Non-Medicaid/
uninsured is a challenge.
35
Availability of services (output), particularly psychiatry
Rosecrance Berry campus may have data related to child/adolescent waits
Resource and referral, department documents, all related information
Length of time on wait list, Services for Spanish-speaking families is very
difficult to provide
Clinical case notes, emergency room records, email
No waiting lists, client access all levels of care in one to three days
It is documented on individual evaluations, but not collected or
documented in summary form
Emergency department documents length of stay
We keep data that provides wait times to transfer patients from our
emergency department to outside providers or our own unit
Demand is getting worse
Not documented consistently
2. Security Concerns
Have you had to utilize security to maintain patients who are at your facility
waiting for a transfer?
NO- 8
YES- 12
N/A- 5
We do not have security and that increases our risk
1:1 coverage
Sometimes
Security utilized for all psych patients in our emergency department
No, but had a couple of incidents; we are not a residential hospital
On a scale of 1-5 how big a problem is security concerns related to delayed
transfers? (1 = very important, 5 = not important at all)
#5 - 2
#4 - 3
#3 - 3
#2 - 3
#1 - 4
What data do you have to document security issues?
Sitter and/or security standby hours. Need of the hospital to develop a
“behavioral response team” to address patient issues/concern especially
safety (completed in 2011).
We document number of security watches and injuries that occur in the
emergency department
Security documentation/logs

36
Incident reports, client waiting for ambulance to go to hospital may run or
become physically aggressive
Security may keep data, not sure
911 calls for assistance
Critical incident reporting. Increased evidence of higher activity due to
shorter length of stay inpatient/reduced funding; discharges from State
Operated Facilities/Chester, etc.
Not sure if security has documented length of stay or wait times
Clinical assessments, 1:1 documentation
Quality measures, risk department. Director of quality documents
Data is documented on individual patients but is not collated at this time
Our emergency department/security would have this information related to
this
Crisis management at program level
3. Patient Volume
Have you seen an increase in the number of mentally ill and or substance abusing
patients being served at your facility in the past year?
Yes- 14
No- 3
Staff reductions has resulted in fewer being served
We focus on mental illness/intellectual and developmental disabilities
Minor increase
There is an increase in uninsured volumes of patients which effects the
bottom line and causes hospitals to want to close psych units
Not significantly
Increase by 1/3 in terms of behavioral health presentations from 2nd
to 3rd
quarter
On a scale of 1-5 how important is this issue to your facility?
#5 - 6
#4 - 2
#3 - 1
#2 - 2
#1 - 8
What data do you have available to demonstrate these increases?
Service data statistics
Number of admissions turned away due to bed availability
Not sure
Social service documentation, statistics available at hospital

37
Number of people served are declining due to withdraw of state funding
for unfunded people and the inability of local resources to fund their care
at our community mental health center
Screening
Client member counts (non-duplicated) from 6,000 to 6,500. Client calls
increased to 900 a month
Number of patients seen in emergency department for behavioral health
issues
Number of intake phone calls, number of clients that have to wait for
services
Intake/referral data, capacity limitations
Daily/monthly inquiry, client roster logs
Not collected consistently
Further assessment revealing the underlying diagnosis or misdiagnosis of
Axis I and Axis III diagnosis
Logs, but not consistent date only primary if DX (diagnosis)loss without
transfer
Census always documented
Statistics on length of stay, payer source, referral source information
We have data on numbers of psych evaluations completed and admissions
and discharges, etc.
We are suspending our inpatient services pending State Board approval
None recorded
4. Transportation
Is transportation to appropriate care for unfunded patients a problem in your area?
NO- 2
YES- 7
It is a concern that there can be long delays in using the transportation
company vs. local ambulance
Public transportation is not sufficient, PACE is limited
At times
For patients that cannot get to appointments it is high
On a scale of 1-5 how big a problem do you believe this is?
#5 - 7
#4 - 4
#3 - 6
#2 - 3
#1 - 7
38
What data is available to document this problem?
Lock, Northern IL, data
Not sure
Morris has hospital transportation services that provide free transportation
and medical/counseling needs in Grundy county
Limited bus routes (cities with no coverage) and times/days they run
Community analysis 2010, new transportation model began 1-1-12 in
McHenry County but only serves three largest areas, but does not reach
outlying areas
Occasionally have issues, more so the last 9 months
Use of $27,000 in unfunded transportation costs in excess of $10,000 in
funded transportation (Taxi, PACE bus, gas cards)
Crisis reports
Anecdotal data, utilization of agency van service
None
Lack of public transportation systems-no vehicles that people own-no
money to pay for it
We have expense reports documenting how much we have had to pay for
patients who are unfunded and live far away to get home
5. Admissions
Over the past year have you had to admit more patients with mental illness or
substance abuse problems to non-behavior health units in your hospital because
you could not locate appropriate care elsewhere either inside or outside your
facility?
YES- 5
NO- 4
N/A- 6
Not sure
Not an increase, but it is an issue
They wait in the emergency room for days
Try hard to keep them in the emergency department
No effort to place patients from the emergency department in priority
Will only admit to medical units if there is a medical issue
On a scale of 1-5 how big a problem do you believe this is?
#5 - 1
#4 - 1
#3 - 3
#2 - 1
#1 - 5

39
What data do you have available to document this issue?
Unsure, but I know that this is an issue and the hospital does keep data on
this
Data could be drawn from patient census on admitting
Clinical files
No data on this
Social service documentation, statistics available
The emergency room has statistics and we have documented the cases
Overcrowding in the emergency department is more of a problem
Not consistently
6. Please add any additional issues or trends experienced at your facility over the
past year and what data you have to document the issue.
Funding reduction-staff reduction-fewer clients being served
Placement (long-term) for those suffering from mental health issues.
Continue to have extended length of stay in the emergency departments
Waiting lists, not sure about documentation
Continuing huge wait lists to be paid by State of IL
State funding has been drastically reduced and delayed resulting in cash
flow issues
Electronic records
Morris does not have a behavioral health unit. In addition to increase wait
times for non-funded patients we are also seeing increase wait times for
patients with insurance due to inpatient psych units running full
Increase in stress related to lack of funding, finances, etc.
Referrals for Community Integrated Living Arrangements, schools, and
Child and Adolescent providers. Group home services presenting with
high-activity behavioral issues with grossly inadequate funding
Increase of heroin admits, higher patient acuity
An ongoing issue has been lack of adequate referrals/placement for
patients with substance abuse. Also, our local county respite program
denies a good number of patients solely based on their medical issues,
which are generally long standing.
Lack of funding, coordination of services
Need to incorporate the peer specialist roles in planning, strategizing and a
part of the whole process to help as change agents
Increase in primary substance abuse services
Increase in length of stay in emergency department, increase in number of
patients without a payer source, increase in difficulty in accessing
community services due to decrease in resources
Lack of child psychiatrists, lower reimbursement
40
7. Would you be interested in continuing to dialogue with other behavioral health
providers in your region through meetings, trainings, and workshops?
YES - 24
We need to have a presentation for legislators to hear some individual, and
family stories, and successes and challenges
8. Would you be interested in working with other providers in the region on
common network issues such as transportation, regulatory barriers and other
system design issues?
YES - 21
Please indicate which issues would be helpful to you:
Systems funding, reductions
Bed availability log for input psych beds would be very helpful
Regulatory issues
Access
Only if the state divisions and department will act on our work
All issues
Development/training
Coordination with services for patients with substance abuse and patients
with high readmission rates
Transportation and regulatory barriers
System design issues
I would be interested in strengthening the collaboration between providers
and family members
Barriers, design, hierarchy (democratic leadership for the human service
model) for better outcomes of staff
9. Any other items you would like to share about this planning process or materials
that are related to this effort?
Would just like to play a part if I have the time
Include representatives from Council on Accreditation, Commission on
Accreditation Rehabilitation Facilities, and Joint Commission. The
accrediting representatives have a national and global perspective on
issues we have discussed.
It was great
Illinois Psychological Association workers should be involved in the
authorizations for hospitalization as opposed to hospitals accepting a
referral under the belief they need to and then finding out they were not
accessed appropriately.
Nice effort, glad to hear what you have done in region 2
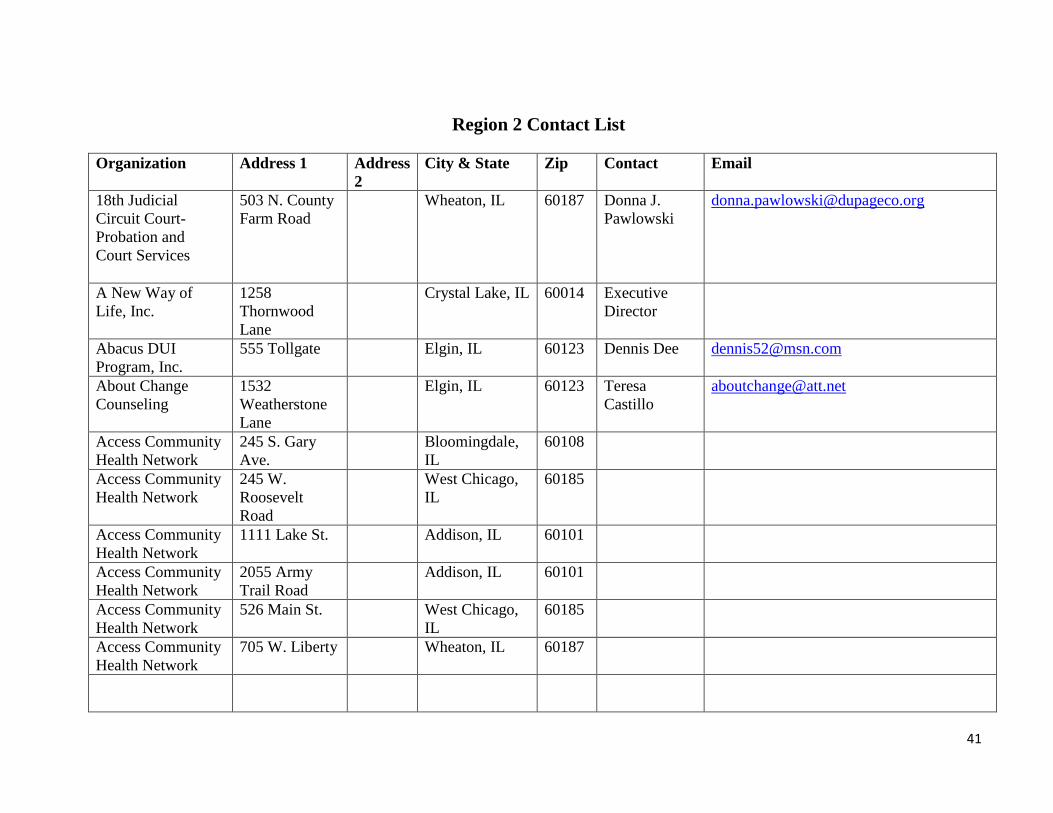
41
Region 2 Contact List
Organization Address 1 Address
2
City & State Zip Contact Email
18th Judicial
Circuit Court-
Probation and
Court Services
503 N. County
Farm Road
Wheaton, IL
60187
Donna J.
Pawlowski
A New Way of
Life, Inc.
1258
Thornwood
Lane
Crystal Lake, IL 60014 Executive
Director
Abacus DUI
Program, Inc.
555 Tollgate Elgin, IL 60123 Dennis Dee [email protected]
About Change
Counseling
1532
Weatherstone
Lane
Elgin, IL 60123 Teresa
Castillo
Access Community
Health Network
245 S. Gary
Ave.
Bloomingdale,
IL
60108
Access Community
Health Network
245 W.
Roosevelt
Road
West Chicago,
IL
60185
Access Community
Health Network
1111 Lake St. Addison, IL 60101
Access Community
Health Network
2055 Army
Trail Road
Addison, IL 60101
Access Community
Health Network
526 Main St. West Chicago,
IL
60185
Access Community
Health Network
705 W. Liberty Wheaton, IL 60187
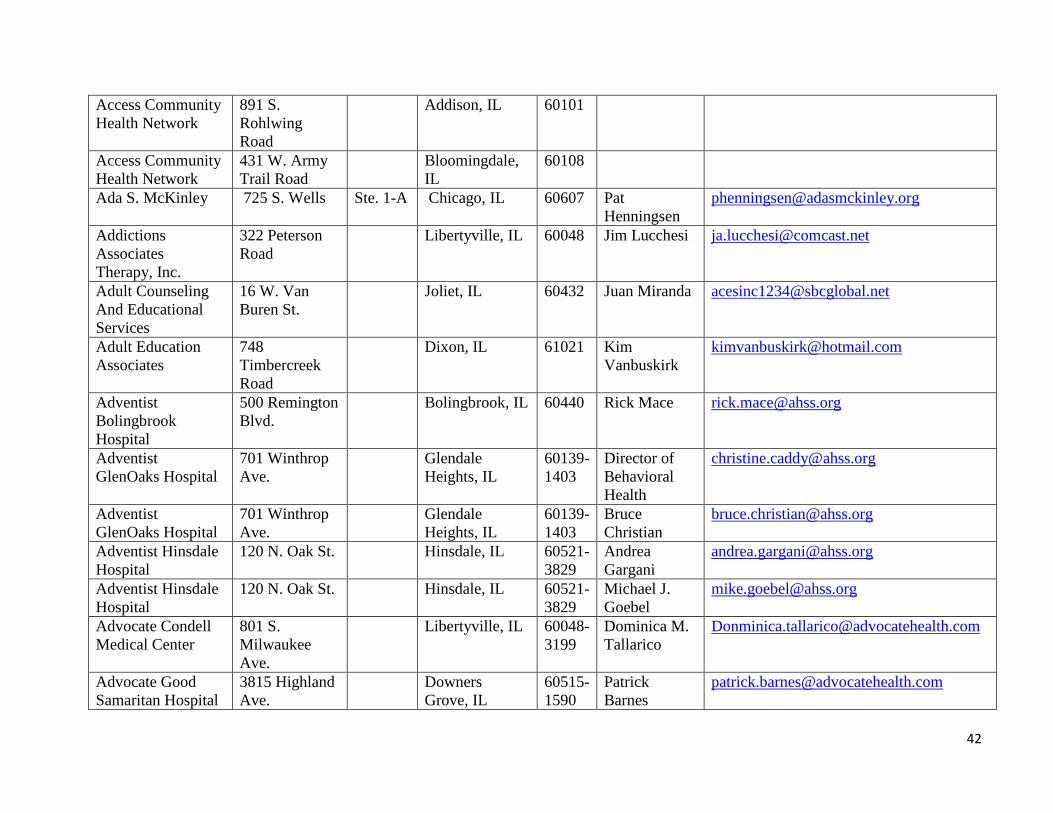
42
Access Community
Health Network
891 S.
Rohlwing
Road
Addison, IL 60101
Access Community
Health Network
431 W. Army
Trail Road
Bloomingdale,
IL
60108
Ada S. McKinley 725 S. Wells Ste. 1-A Chicago, IL 60607 Pat
Henningsen
Addictions
Associates
Therapy, Inc.
322 Peterson
Road
Libertyville, IL 60048 Jim Lucchesi [email protected]
Adult Counseling
And Educational
Services
16 W. Van
Buren St.
Joliet, IL 60432 Juan Miranda [email protected]
Adult Education
Associates
748
Timbercreek
Road
Dixon, IL 61021 Kim
Vanbuskirk
Adventist
Bolingbrook
Hospital
500 Remington
Blvd.
Bolingbrook, IL 60440 Rick Mace [email protected]
Adventist
GlenOaks Hospital
701 Winthrop
Ave.
Glendale
Heights, IL
60139-
1403
Director of
Behavioral
Health
Adventist
GlenOaks Hospital
701 Winthrop
Ave.
Glendale
Heights, IL
60139-
1403
Bruce
Christian
Adventist Hinsdale
Hospital
120 N. Oak St. Hinsdale, IL 60521-
3829
Andrea
Gargani
Adventist Hinsdale
Hospital
120 N. Oak St. Hinsdale, IL 60521-
3829
Michael J.
Goebel
Advocate Condell
Medical Center
801 S.
Milwaukee
Ave.
Libertyville, IL 60048-
3199
Dominica M.
Tallarico
Advocate Good
Samaritan Hospital
3815 Highland
Ave.
Downers
Grove, IL
60515-
1590
Patrick
Barnes

43
Advocate Good
Samaritan Hospital
3815 Highland
Ave
Downers
Grove, IL
60515-
1590
David S. Fox [email protected]
Advocate Good
Shepherd Hospital
450 W.
Highway 22
Barrington, IL 60010-
1901
Karen A.
Lambert
Advocate Good
Shepherd Hospital
450 W.
Highway 22
Barrington, IL 60010-
1901
Faye
Redmond
Advocate Good
Shepherd Hospital
450 W.
Highway 22
Barrington, IL 60010-
1901
Noel Lemke [email protected]
Advocate Good
Shepherd Hospital
450 W.
Highway 22
Barrington, IL 60010-
1901
Catherine
McBride
Affordable DUI
Counseling
570 W.
Broadway St.
Bradley, IL 60915 Michael
Regas
Alexander Zubenko
and Associates
4699 Auvergne
Ave.
Lisle, IL 60532 Alexander
Zubenko
Allendale
Association
P.O.
Box
1088
Lake Villa, IL 60046 Sue Gaddy [email protected]
Allied
Psychological
Services, LTC
501 W.
Peterson Road
Libertyville, IL 60048 Janice
Prepura
Alpha Counseling
Center, Inc.
1112 S.
Washington St.
Naperville, IL 60540 Mary
Kullman
Al-Tech Services,
Inc.
2233 Charles
St.
Rockford, IL 61104 E. Taylor
Reynolds IV
Alternative
Behavior Treatment
Centers
27255 N.
Fairfield Road
Mundelein, IL 60060 Robin
McGinnis,
MSW
Amanecer, Inc. 25W560
Geneva Road
Carol Stream,
IL
60188 Roberto
Almeida
Arlington Center
for Recovery, LLC
1655 S.
Arlington
Heights Road
Arlington
Heights, IL
60005 Donna
Johnson

44
Associates in BH
Care
309 Pheasant
Trl
Lake in the
Hills, IL
60156 Mary Crick [email protected]
Association of
Community Mental
Health Authorities
P.O.
Box 935
Aurora, IL 60507 Maureen
Mulhall
Association of
Community Mental
Health Authorities
P.O.
Box 935
Aurora, IL 60507 Phyllis
Russell
Association for
Individual
Development
309 W. New
Indian Trail
Court
Aurora, IL 60506 Lynn O'Shea [email protected]
Association for
Individual
Development
309 W. New
Indian Trail
Court
Aurora, IL 60506 Michelle
McMullin
Aunt Martha's
Youth Service
Center, Inc.
101 S.
Broadway St.
Aurora, IL 60505
Aunt Martha's
Youth Service
Center, Inc.
3003
Wakefield
Carpentersville,
IL
60110
Aunt Martha's
Youth Service
Center, Inc.
1777 E. Court
St.
Kankakee, IL 60901
Aunt Martha's
Youth Service
Center, Inc.
317 E. Indian
Trail
Aurora, IL 60506
Aunt Martha's
Youth Service
Center, Inc.
76 S. LaSalle Aurora, IL 60505
Aunt Martha's
Youth Service
Center, Inc.
1515 E. Lake
St.
Hanover Park,
IL
60133

45
AVP Counseling &
DUI Services, Inc.
336 W. Maple
St.
New Lenox, IL 60451 Arnold
Pilmonas
Aztec Counseling
Agency, Inc.
231 Ruby St.
Joliet, IL
60435
Karina
Ramirez
Bam House, inc. 431 N.
Genesee St.
Waukegan, IL 60085 Kevin A.
Means
Behavioral
Education and
Treatment, Inc.
1415 W. Lake
St.
Addison, IL 60101 Marsha
Murphy
Ben Gordon Center 12 Health
Services Drive
DeKalb, IL 60115 Michael Flora [email protected]
Boone County
Department of
Health
1204 Logan
Ave.
Belvidere, IL 61008 Executive
Director
Braden Counseling
Center
2580 DeKalb
Ave.
Sycamore, IL 60178 Jayne A.
Braden
Breaking Free, Inc. 120 Gale St. Aurora, IL 60506 Mike Moran [email protected]
Bridges Counseling
& DUI Services
215 N. Main
St.
Algonquin, IL 60102 Sheila
Schmidt
Cap of Downers
Grove, Inc.
4954 Main St. Downers
Grove, IL
60515 Marie
Angelico
Care Clinics, Inc. 522 N. Lake
St.
Aurora, IL 60506 Scott A.
Rocush
Carroll County
Department of
Health
822 S. Mill St. Mt. Carroll, IL 61053 Executive
Director
Centegra Health
Systems
527 W. South
St.
Woodstock, IL 60098 Laura
Walczak
Centegra Health
Systems
527 W. South
St.
Woodstock, IL 60098 Astrid Larsen [email protected]
Centegra Hospital-
McHenry
4201 Medical
Center Drive
McHenry, IL 60050-
8499
Michael S.
Eesley

46
Centegra Hospital-
Woodstock
3701 Doty
Road
P.O.
Box
1990
Woodstock, IL 60098-
3797
Sheila Senn,
PhD
Centegra Hospital-
Woodstock
3701 Doty
Road
PO Box
1990
Woodstock, IL 60098-
3797
Michael S.
Eesley
Central DuPage
Hospital
25 N. Winfield
Road
Winfield, IL 60190-
1295
Mike Tinken [email protected]
Central DuPage
Hospital
25 N. Winfield
Road
Winfield, IL 60190-
1295
Brian Lemon [email protected]
Central DuPage
Hospital
25 N. Winfield
Road
Winfield, IL 60190-
1295
Alison
Johnson
CGH Medical
Center
100 E. LeFevre
Road
Sterling, IL 61081-
1279
Edward
Andersen
CGH Medical
Center
100 E. LeFevre
Road
Sterling, IL 61081-
1279
Emily
Dykstra
CGH Medical
Center
100 E. LeFevre
Road
Sterling, IL 61081-
1279
Deb
Keaschall
Challenge
Behavioral
Healthcare, Nic.
15 Spinning
Wheel Road
Hinsdale, IL 60521 Richard
Kelling
Changes Place 264 N. Phelps
Ave.
Rockford, IL 61108 Jack Phillips [email protected]
Comgraph, Inc. 105 Warwick
St.
Park Forest, IL 60466 Victor
Needham
Community
Behavioral
Healthcare
Association
3085 N.
Stevenson
Drive
#308 Springfield, IL 62703 Sheryl Turpin [email protected]
Community Health
Partnership of
Illinois
157 S. Lincoln
Ave.
Aurora, IL 60505
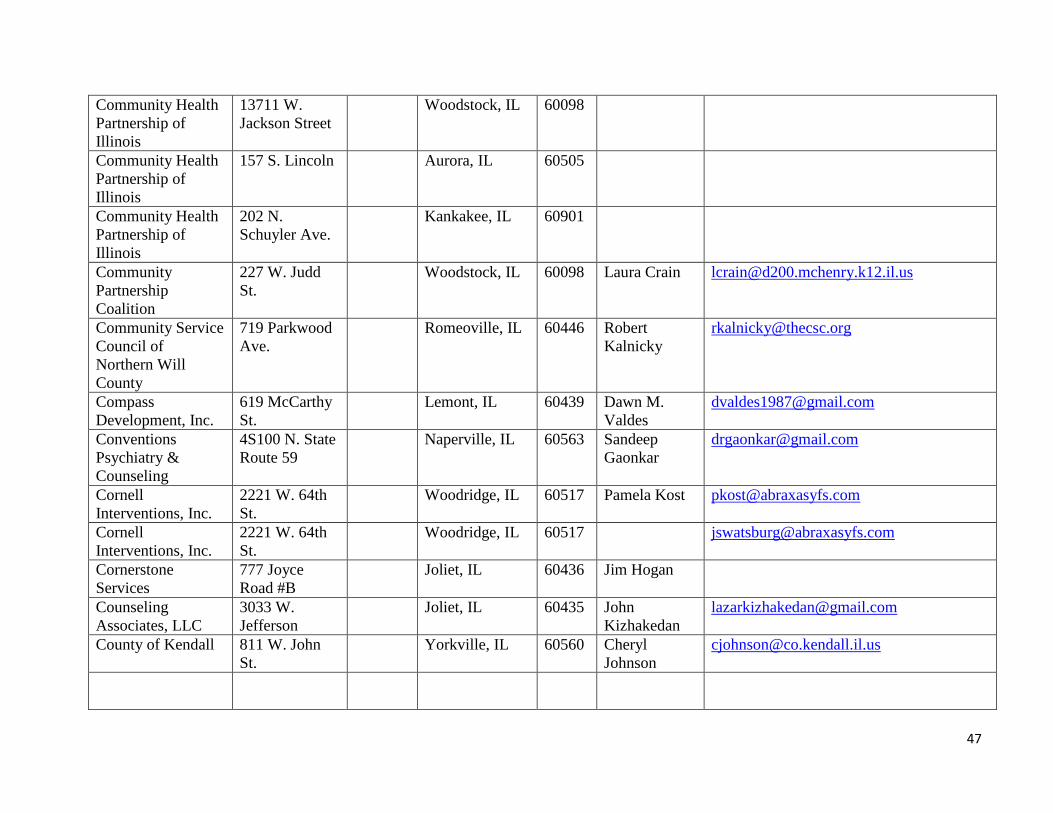
47
Community Health
Partnership of
Illinois
13711 W.
Jackson Street
Woodstock, IL 60098
Community Health
Partnership of
Illinois
157 S. Lincoln Aurora, IL 60505
Community Health
Partnership of
Illinois
202 N.
Schuyler Ave.
Kankakee, IL 60901
Community
Partnership
Coalition
227 W. Judd
St.
Woodstock, IL 60098 Laura Crain [email protected]
Community Service
Council of
Northern Will
County
719 Parkwood
Ave.
Romeoville, IL 60446 Robert
Kalnicky
Compass
Development, Inc.
619 McCarthy
St.
Lemont, IL 60439 Dawn M.
Valdes
Conventions
Psychiatry &
Counseling
4S100 N. State
Route 59
Naperville, IL 60563 Sandeep
Gaonkar
Cornell
Interventions, Inc.
2221 W. 64th
St.
Woodridge, IL 60517 Pamela Kost [email protected]
Cornell
Interventions, Inc.
2221 W. 64th
St.
Woodridge, IL 60517 [email protected]
Cornerstone
Services
777 Joyce
Road #B
Joliet, IL 60436 Jim Hogan
Counseling
Associates, LLC
3033 W.
Jefferson
Joliet, IL 60435 John
Kizhakedan
County of Kendall 811 W. John
St.
Yorkville, IL 60560 Cheryl
Johnson

48
Criminal Justice
Advocacy for
People M.I.
Gertrude
Rodig
Crossroads
Counseling
Services, LLC
1802 N.
Division St.
Morris, IL 60450 Angela Solis [email protected]
Crossroads
Counseling
Services, LLC
1802 N.
Division St.
Morris, IL 60450 Amanda
Jessie
Crusader
Community Health
1200 W. State
St.
Rockford, IL 61102 Executive
Director
Crusader
Community Health
1100
Broadway
Rockford, IL 61102
Crusader
Community Health
730 W. State
St.
Rockford, IL 61102
Crusader
Community Health
1720 18th St. Rockford, IL 61104
Crusader
Community Health
516 Green St. Rockford, IL 61102
Crusader
Community Health
715 W. State
St.
Rockford, IL 61102
Crusader
Community Health
412 N. Church
St.
Rockford, IL 61103
Crusader
Community Health
809 Cedar St. Rockford, IL 61102
Crusader
Community Health
1149 Railroad
Ave.
Rockford, IL 61104
Crusader
Community Health
10 W. Linden Freeport, IL 61032
Crusader
Community Health
1050 Logan
Ave.
Belvidere, IL 61008
Crusader
Community Health
714 Third Ave. Rockford, IL 61104

49
DeKalb County
Department of
Health
2550 N. Annie
Glidden Road
DeKalb, IL 60115 Executive
Director
DeKalb County
Mental Health
(708) Board
2500 N. Annie
Glidden Road
Suite B DeKalb, IL 60115 Donna
Moulton
Delnor Hospital 300 Randall
Road
Geneva, IL 60134-
4202
Robert
Friedberg
Delnor Hospital 300 Randall
Road
Geneva, IL 60134-
4202
Diane Murray [email protected]
DHS 100 W.
Randolph,
Suite 5-600
Chicago, IL 60601 Barbara J.
Brooks
DHS Patricia
Kates-Collins
Direct Counseling,
Nic.
400 Russell
Court
Woodstock, IL 60098 William L.
Blaul
DMH Eldon Wigget [email protected]
Duane Dean
Behavioral Health
Center
700 E. Court
St.
Kankakee, IL 60901 Herbert
Delaney
DUI & Addiction
Counseling Center,
Inc.
333 E. Route
83
Mundelein, IL 60060 Christine M.
Hinkeldey
DUI and Addiction
Counseling
2210 Dean St. St. Charles, IL 60175 Rita Gennusa [email protected]
DUI Associates 1826 E.
Belvedere
Road
Grayslake, IL 60030 Randy
Edwards
DUI Counseling
Center, Inc/Bayrach
Counseling
Services
9933 N.
Lawler Ave.
Skokie, IL 60077 Scott K.
Bayrach

50
DUI Solutions 129 Phelps
Ave.
Rockford, IL 61108 Norbert J.
Wick
DuPage County
Health Department
111 N. County
Farm Road
Wheaton, IL 60187 Filiz Gunway,
MSW
DuPage County
Psychological
Services/Comm.
Resources
505 N. County
Farm Road
Wheaton, IL 60187 Thomas
Sayers
Ecker Center for
Mental Health, Inc.
1845
Grandstand
Place
Elgin, IL 60123 Karen Beyer [email protected]
Edward Hospital 801 S.
Washington St.
Naperville, IL 60540-
7430
Pam Davis [email protected]
El Puente Latino,
Inc.
2415 N.
Butrick St.
Waukegan, IL 60087 Narcisco Diaz [email protected]
Elgin MH Center,
DHS Region 2
750 S. State St. Elgin, IL 60120 Amparo
Lopez
Elmhurst Memorial
Hospital
155 E. Brush
Hill Road
Elmhurst, IL 60126 Pamela
Dunley
Elmhurst Memorial
Hospital
155 E. Brush
Hill Road
Elmhurst, IL 60126 W. Peter
Daniels
Elmhurst Memorial
Hospital
155 E. Brush
Hill Road
Elmhurst, IL 60126 Teddi
Kruchman
Ely, Patricia &
Associates
2625
Butterfield
Oak Brook, IL 60523 Patricia Ely [email protected]
Employee Health
Consultants, Inc.
101 N.
Virginia
Crystal Lake, IL 60014 Richard S.
Atwater
Family Alliance,
Inc.
2028 N.
Seminary Ave.
Woodstock, IL 60098 Carol Louise
RN-BC
Family Alliance,
Inc.
2028 N.
Seminary Ave.
Woodstock, IL 60098 Ann May [email protected]
Family Counseling
Services of Aurora
70 South River
St.
Aurora, IL 60506 Eric Ward [email protected]

51
Family Etc. 2028 N.
Seminary Ave.
Woodstock, IL 60098 Teri Lindahl [email protected]
Family Service and
Community Mental
Health
4100 Veterans
Parkway
McHenry, IL 60050 Lori A.
Nelson
Family Service and
Community Mental
Health
4100 Veterans
Parkway
McHenry, IL 60050 Chris Gleason [email protected]
Family Service
Association of
Greater Elgin
22 S. Spring
St.
Elgin, IL 60120 Lisa LaForge [email protected]
FHN Family
Counseling
300 Summit St. Galena, IL 61036 Executive
Director
FHN Memorial
Hospital
421 W.
Exchange St.
Freeport, IL 61032 Dan Neal [email protected]
FHN Memorial
Hospital
1045 W.
Stephenson St.
Freeport, IL 61032-
4899
Michael R.
Perry, M.D.
FHN Memorial
Hospital
421 W.
Exchange St.
Freeport, IL 61032 Jennifer
Aurand, PsyD
Foundations
Center, Inc.
5592 Spring
Brook Road
Rockford, IL 61114 Carol Wick [email protected]
Galena Clinic, Inc. 9567 W. US
Highway 20
Galena, IL 61036 Kenneth
Davis
Geneva Community
Mental Health
(708) Board
22 S. First St. Geneva, IL 60134 Greg
Torrence
Global Behavioral
Health, Inc.
303 N. Second
St.
Suite
23A
St. Charles, IL 60174 Elias A.
Palacios
Greater Elgin
Family Care Center
370 Summit St.
#A
Elgin, IL 60120 Executive
Director
Greater Elgin
Family Care Center
1770 Spartan
Drive
Elgin, IL 60123

52
Greater Elgin
Family Care Center
37 S. Geneva
Street
Elgin, IL 60121
Greater Elgin
Family Care Center
510 Franklin
Blvd.
Elgin, IL 60120
Greater Elgin
Family Care Center
190 N. Melrose
Ave.
Elgin, IL 60123
Greater Elgin
Family Care Center
420 May St. Elgin, IL 60120
Greater Elgin
Family Care Center
240 S. Clifton
Ave.
Elgin, IL 60123
Greater Elgin
Family Care Center
949 Van St. Elgin, IL 60123
Greater Elgin
Family Care Center
225 S. Liberty
St.
Elgin, IL 60120
Greater Elgin
Family Care Center
665 Dundee
Ave.
Elgin, IL 60120
Greater Elgin
Family Care Center
1475 Larkin
Ave.
Elgin, IL 60123
Greater Elgin
Family Care Center
450 Dundee
Ave.
Elgin, IL 60120
Greater Elgin
Family Care Center
1730 Berkley
St.
Elgin, IL 60123
Greater Elgin
Family Care Center
901 Center St. Elgin, IL 60120
Greater Elgin
Family Care Center
4100 Veterans
Parkway
McHenry, IL 60050
Greater Elgin
Family Care Center
264 Oak St. Elgin, IL 60123
Greater Elgin
Family Care Center
63 S. Channing
St.
Elgin, IL 60120
Grundy County
Health Department
1320 Union Morris, IL 60450 Kay Lynn
Shoemaker,
BSN, RN

53
Guiding Light
Counseling, Inc.
538 E.
Boughton
Road
Bolingbrook, IL 60440 Kimberly
Duris
Hope for
Tomorrow, Inc.
479 N. Lake
St.
Aurora, IL 60506 Jeffrey S.
Gilbert
ILDS/DHM Region
2
Patricia
Lindquist
Illinois Association
of Rehab Facilities
206 S. Sixth St. Springfield, IL 62701 Janet Stover [email protected]
Illinois Association
of Rehab Facilities
206 S. Sixth St. Springfield, IL 62701 Josh Evans [email protected]
Illinois Children's
Mental Health
Partnership
Robin Cabral [email protected]
INC Board, NFP A
Community Mental
Health Funding
Alliance
P.O.
Box 935
Aurora, IL 60506 Jerry J.
Murphy
Independence
Center
2025
Washington St.
Waukegan, IL 60085 Lisa Johnson [email protected]
Inroads Counseling
and DUI Center,
Inc.
150 S.
Kennedy Drive
Carpentersville,
IL
60110 Donna
Beichel
Institute for
Personal
Development
1401
Lakewood
Drive
Morris, IL 60450 Elizabeth M.
Varnes
Janet Wattles
Center
526 W. State
St.
Rockford, IL 61101 Executive
Director
Jem Treatment, Inc. 2424
Washington St.
Waukegan, IL 60085 Darlene
Maloney
JoDaviess County
Department of
Health
9483 U.S. Rt.
20 West
P.O.
Box 318
Galena, IL 61036 Executive
Director

54
JoDaviess County
Mental Health
(708) Board
330 N. Bench
St.
Galena, IL 61036 Ben Anderson [email protected]
Kane County
Department of
Health
1240 N.
Highland St.
Aurora, IL 60506 Executive
Director
Kankakee County
Department of
Health
2390 W.
Station
Kankakee, IL 60901 Executive
Director
Katherine Shaw
Bethea Hospital
403 E. First St. Dixon, IL 61021-
3116
Gail Stickle [email protected]
Katherine Shaw
Bethea Hospital
403 E. First St. Dixon, IL 61021-
3116
David L.
Schreiner,
FACHE
Kelly's Accurate
DUI
Evaluations/Risk
Education Services
81 N. Chicago
St.
Joliet, IL 60432 Renee Kelly [email protected]
Kendall County
Department of
Health
811 W. John
St.
Yorkville, IL 60560 Executive
Director
Kenneth Young
Centers
1001 Rohlwing
Road
Elk Grove
Village, IL
60007 Mitchell
Bruski
Kevin & Associates 257 N. West
Ave.
Elmhurst, IL 60126 Maureen
Kevin
Kindred Hospital-
Sycamore
225 Edward St. Sycamore, IL 60178-
2197
Cindy Smith [email protected]
Kishwaukee
Community
Hospital
One Kish
Hospital Drive
P.O.
Box 707
DeKalb, IL 60115-
0707
Brad Copple [email protected]
Kishwaukee
Community
Hospital
One Kish
Hospital Drive
P.O.
Box 707
DeKalb, IL 60115-
0707
Laura Desilva [email protected]

55
KP Counseling Inc. 461 N.
Mulford Road
Rockford, IL 61107 Thomas G.
Mlodzik
L.S. Berkley And
Associates
1207 Old
McHenry Road
Buffalo Grove,
IL
60089 Leslie St.
Berkley
Lake County
Health Department
914 Eighth St. Waukegan, IL 60085
Lake County
Health Department
285 E.
Washington St.
Grayslake, IL 60030
Lake County
Health Department
3601 N. Lewis Waukegan, IL 60087
Lake County
Health Department
54 S. Whitney Grayslake, IL 60030
Lake County
Health Department
22333 W.
Erhart Road
Mundelein, IL 60060
Lake County
Health Department
3001 Green
Bay Road
North Chicago,
IL
60064
Lake County
Health Department
2400 Belvidere
Road
Waukegan, IL 60085
Lake County
Health Department
2215 14th St. North Chicago,
IL
60064
Lake County
Health Department
1819 27th St. Zion, IL 60099
Lake County
Health Department
224 W.
Clarendon
Drive
Round Lake
Beach, IL
60073
Lake County
Health Department
3010 Grand
Ave.
Waukegan, IL 60085
Lake County
Health Department
1840 Green
Bay Road
Highland Park,
IL
60035
Lake County
Health Department,
Behavioral Health
Services
3012 Grand
Ave
Waukegan, IL 60085 Ted Testa [email protected]

56
Larkin Center 1212 Larkin
Ave.
Elgin, IL 60123 Dennis L.
Graf, MS
Latino Intervention
Center
54 S. Grove
Ave.
Elgin, IL 60120 Ernest Pujals [email protected]
Lee County
Department of
Health
309 S. Galena
Avenue
Suite
100
Dixon, IL 61021 Executive
Director
Linden Oaks at
Edward
801 S.
Washington
Naperville, IL 60540-
7430
Mary Lou
Mastro
Linden Oaks at
Edward
801 S.
Washington
Naperville, IL 60540-
7430
Charla
Waxman
Marianjoy
Rehabilitation
Hospital & Clinics
26 W. 171
Roosevelt
Road
Wheaton, IL 60187 Kathleen C.
Yosko
Mathers Clinic,
LLC
6180 E. State
St.
Rockford, IL 61108 Ramesh
Vemuri
McHenry County
Department of
Health
2200 N.
Seminary Ave.
Woodstock, IL 60098 Patrick J.
McNulty
McHenry County
Department of
Health
2200 N.
Seminary Ave.
Woodstock, IL 60098 Pamela
Morzos
McHenry County
MHB &ACMHAI
620 Dakota Crystal Lake, IL 60012 Sandy Lewis [email protected]
McHenry County
MHB &ACMHAI
620 Dakota Crystal Lake, IL 60012 Bob Lesser [email protected]
McHenry County
MHB
620 Dakota Crystal Lake, IL 60012 T. Schroll [email protected]
McHenry County
MHB
620 Dakota Crystal Lake, IL 60012 Mark Klocek [email protected]
McHenry County
MHB
620 Dakota Crystal Lake, IL 60012 Donna Buss [email protected]

57
McHenry County
Youth Service
Bureau
101 S.
Jefferson St.
Woodstock, IL 60098 Susan A.
Krause, B.D.
Ed., M.S. Ed,
MBA
MCM Substance
Abuse Center
135 Robert
Palmer Drive
Elmhurst, IL 60126 Martin C.
Manion
Memorial Medical
Center, Chemical
Dependency
Services
527 W. South
St.
Woodstock, IL 60098 Executive
Director
Mercy Harvard
Hospital
901 Grant St. PO Box
850
Harvard, IL 60033-
0850
Jeni Hallatt [email protected]
Midwest Medical
Center
One Medical
Center Drive
Galena, IL 61036 Tracy Bauer [email protected]
Morris Hospital &
Healthcare Centers
150 W. High
St.
Morris, IL 60450-
1463
Mark B.
Steadham
Morris Hospital &
Healthcare Centers
150 W. High
St.
Morris, IL 60450-
1463
Linda Rice [email protected]
Morris Hospital &
Healthcare Centers
150 W. High
St.
Morris, IL 60450-
1463
Elizabeth
Thrun
Morrison
Community
Hospital
303 N. Jackson
St.
Morrison, IL 61270-
3042
Kent
Jorgensen
Motivating
Individuals
3445 Elmwood
Rd.
Rockford, IL 61101 Executive
Director
NAMI, IL Robin Garvey [email protected]
NAMI, IL Erin
Harsevoort
NAMI, IL Hugh Brady [email protected]
Naperville
Psychiatric
Ventures
801 S.
Washington
Naperville, IL 60540 Mary Lou
Mastro

58
NASA Education
Corporation
3305 S. IL
Route 31
Crystal Lake, IL 60012 Donna
McCafferty
New Hope
Counseling Center
275 E. Court
St.
Kankakee, IL 60901 K.A.
Abraham
New Hope
Recovery Center,
LLC
201 N. Third
St.
Geneva, IL 60134 Greg Simpson [email protected]
New Visions
Counseling
Services, Inc.
6912 Main St. Downers
Grove, IL
60516 Gina
Pattermann
Nicasa 31979 N. Fish
Lake Road
Round Lake, IL 60073 Linda Snelten [email protected]
Nicasa 31979 N. Fish
Lake Road
Round Lake, IL 60073 Karen Hines [email protected]
Nicasa 2031 Dugdale
Road
North Chicago,
IL
60064 Tricia
Bowdidge
N. IL Council on
Alcoholism & SA
31979 N. Fish
Lake Road
Round Lake, IL 60073 Linda Snelten [email protected]
Northpointe
Resources, Inc.
3441 Sheridan
Road
Zion, IL 60099 Karl Kopp
NorthShore
University
HealthSystem
Highland Park
Hospital
777 Park Ave.
W.
Highland Park,
IL
60035-
2497
Deborah
Taber
NorthShore
University
HealthSystem
Highland Park
Hospital
777 Park Ave.
W.
Highland Park,
IL
60035-
2497
Jesse Peterson
Hall
Northwestern Lake
Counseling
17 W. Grand
Ave.
Fox Lake, IL 60020 Darlene
Kreiger
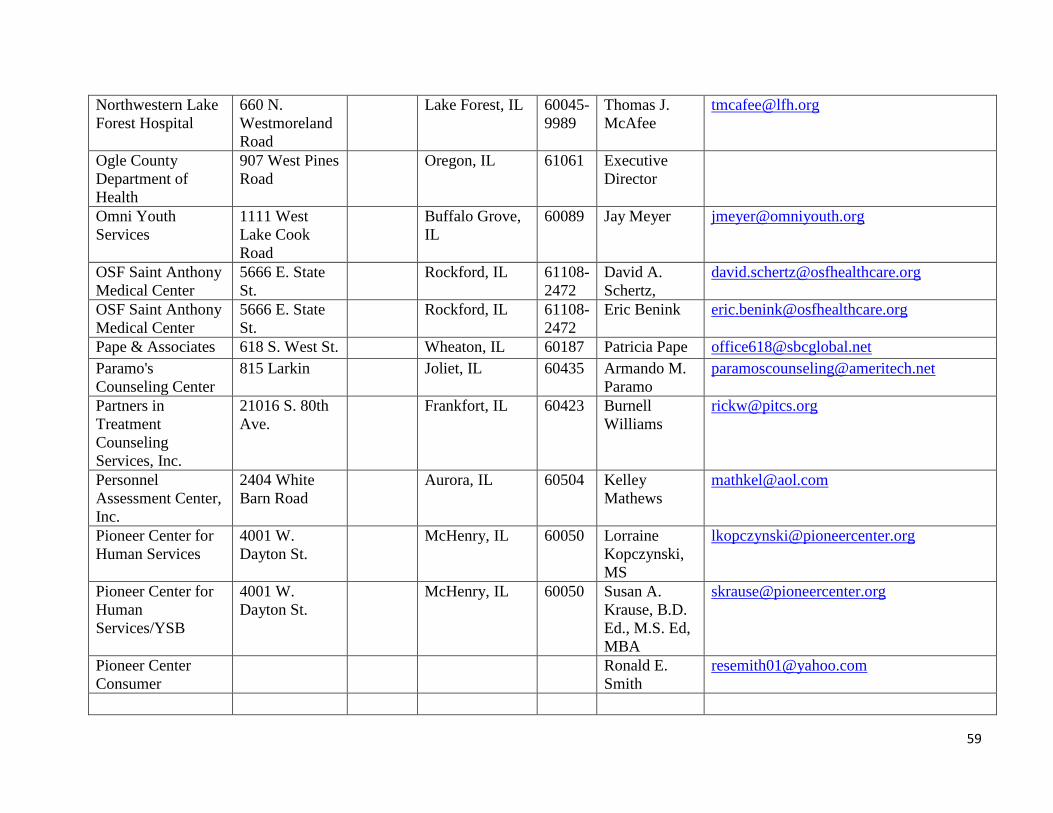
59
Northwestern Lake
Forest Hospital
660 N.
Westmoreland
Road
Lake Forest, IL 60045-
9989
Thomas J.
McAfee
Ogle County
Department of
Health
907 West Pines
Road
Oregon, IL 61061 Executive
Director
Omni Youth
Services
1111 West
Lake Cook
Road
Buffalo Grove,
IL
60089 Jay Meyer [email protected]
OSF Saint Anthony
Medical Center
5666 E. State
St.
Rockford, IL 61108-
2472
David A.
Schertz,
OSF Saint Anthony
Medical Center
5666 E. State
St.
Rockford, IL 61108-
2472
Eric Benink [email protected]
Pape & Associates 618 S. West St. Wheaton, IL 60187 Patricia Pape [email protected]
Paramo's
Counseling Center
815 Larkin Joliet, IL 60435 Armando M.
Paramo
Partners in
Treatment
Counseling
Services, Inc.
21016 S. 80th
Ave.
Frankfort, IL 60423 Burnell
Williams
Personnel
Assessment Center,
Inc.
2404 White
Barn Road
Aurora, IL 60504 Kelley
Mathews
Pioneer Center for
Human Services
4001 W.
Dayton St.
McHenry, IL 60050 Lorraine
Kopczynski,
MS
Pioneer Center for
Human
Services/YSB
4001 W.
Dayton St.
McHenry, IL 60050 Susan A.
Krause, B.D.
Ed., M.S. Ed,
MBA
Pioneer Center
Consumer
Ronald E.
Smith

60
Pioneer Center
Consumer
Alison
Herrdejs
Pioneer Center 4001 W.
Dayton St.
McHenry, IL 60050 James
Carpenter
Professional
Consultations, Inc.
745 S. Eighth
St.
West Dundee,
IL
60118 Carole
Milliman
Professional
Consultations, Inc.
745 S. Eighth
St.
West Dundee,
IL
60118 Doug
Milliman
Provena Mercy
Medical Center
1325 N.
Highland Ave.
Aurora, IL 60506-
1461
Diane
McLaughlin
Provena Mercy
Medical Center
1325 N.
Highland Ave.
Aurora, IL 60506-
1461
Maureen
Bryant
Provena Saint
Joseph Hospital
77 N. Airlite
St.
Elgin, IL 60123-
4998
Craig Harling [email protected]
Provena Saint
Joseph Hospital
77 N. Airlite
St.
Elgin, IL 60123-
4998
Eugene
McMahon,
MD
Provena Saint
Joseph Medical
Center
333 N.
Madison St.
Joliet, IL 60435-
6595
Jane Mitchell [email protected]
Provena Saint
Joseph Medical
Center
333 N.
Madison St.
Joliet, IL 60435-
6595
Beth Hughes [email protected]
Provena Saint
Joseph Medical
Center
333 N.
Madison St.
Joliet, IL 60435 Cassie Reese [email protected]
Provena Saint
Joseph Medical
Center
333 N.
Madison St.
Joliet, IL 60435 Abby
Hornbogen
Provena St. Mary's
Hospital
500 W. Court
St.
Kankakee, IL 60901-
3661
Douglas Jones [email protected]
Provena St. Mary's
Hospital
500 W. Court
St.
Kankakee, IL 60901-
3661
Amy LaFine [email protected]

61
R.O.P.E., Inc. 424 10th Street Waukegan, IL 60085 Patricia L.
White
Regional Care
Association
72 N. Chicago
St.
Joliet, IL 60432 Patricia L.
Langehenning
Remedies
Renewing Lives
516 Green St. Rockford, IL 61101 Gary Halbach [email protected]
Renacer Latino,
Inc.
620
Washington St.
Waukegan, IL 60085 Luz R. Gvero [email protected]
Renz Addiction
Counseling Center
Two American
Way
Elgin, IL 60120 Jerry Skogmo [email protected]
Resolve Center 411 W.
Division
Manteno, IL 60952 Dr. James
Simone
Resurrection
Behavioral Health
2001
Butterfield
Road, #320
Downers
Grove, IL
60515 Executive
Director
Right Direction
Services
1415 Pate
Plaza Drive
South Beloit, IL 61080 Monkia T.
Dougherty
Rita's Ministry
(Restoring Inmates
To America's
Society)
150 S.
Lincolnway
North Aurora,
IL
60542 Linda Martin [email protected]
Riverside Medical
Center
350 North Wall
St.
Kankakee, IL 60901-
2901
Christine
Anthony
Christine-
Riverside Medical
Center
350 N. Wall St. Kankakee, IL 60901-
2901
Phillip
Kambic
Riverside Resolve
Center
350 N. Wall
St.
Kankakee, IL 60901 James Simone [email protected]
Riverview
Counseling Center
705 Dodge St. Galena, IL 61036 Executive
Director
Robert A. Moylan 3333
Warrenville
Road
Lisle, IL 60532 Robert A.
Moylan
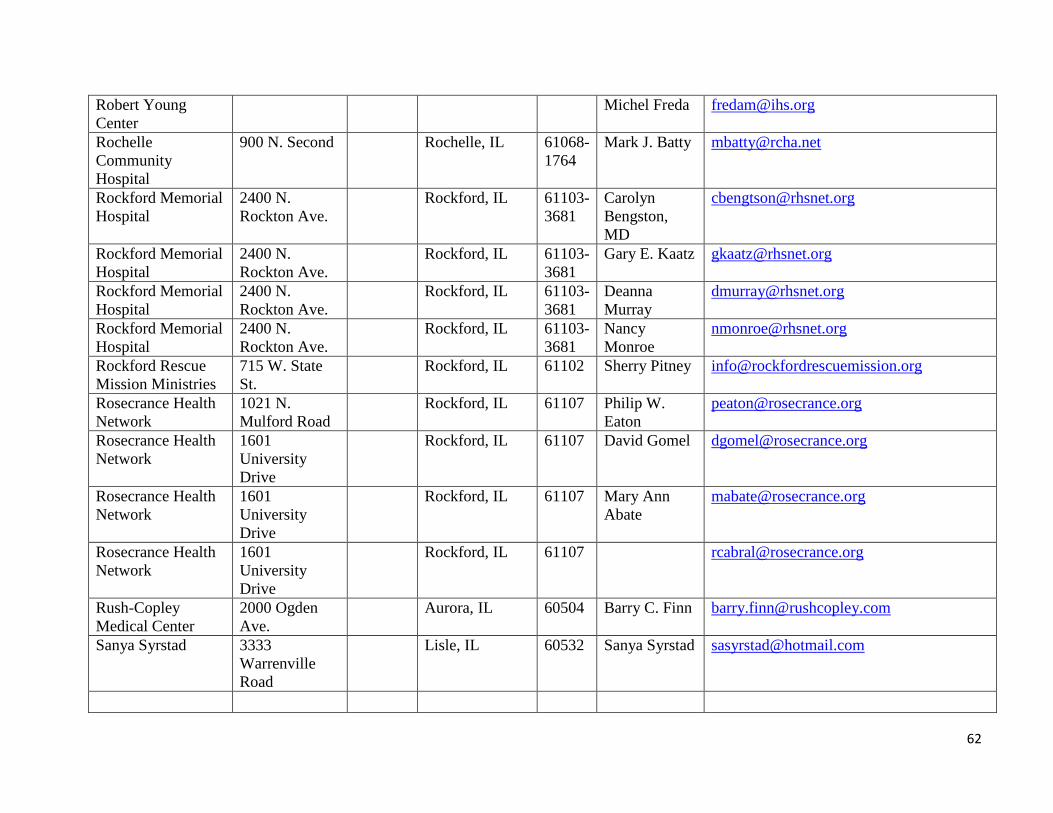
62
Robert Young
Center
Michel Freda [email protected]
Rochelle
Community
Hospital
900 N. Second Rochelle, IL 61068-
1764
Mark J. Batty [email protected]
Rockford Memorial
Hospital
2400 N.
Rockton Ave.
Rockford, IL 61103-
3681
Carolyn
Bengston,
MD
Rockford Memorial
Hospital
2400 N.
Rockton Ave.
Rockford, IL 61103-
3681
Gary E. Kaatz [email protected]
Rockford Memorial
Hospital
2400 N.
Rockton Ave.
Rockford, IL 61103-
3681
Deanna
Murray
Rockford Memorial
Hospital
2400 N.
Rockton Ave.
Rockford, IL 61103-
3681
Nancy
Monroe
Rockford Rescue
Mission Ministries
715 W. State
St.
Rockford, IL 61102 Sherry Pitney [email protected]
Rosecrance Health
Network
1021 N.
Mulford Road
Rockford, IL 61107 Philip W.
Eaton
Rosecrance Health
Network
1601
University
Drive
Rockford, IL 61107 David Gomel [email protected]
Rosecrance Health
Network
1601
University
Drive
Rockford, IL 61107 Mary Ann
Abate
Rosecrance Health
Network
1601
University
Drive
Rockford, IL 61107 [email protected]
Rush-Copley
Medical Center
2000 Ogden
Ave.
Aurora, IL 60504 Barry C. Finn [email protected]
Sanya Syrstad 3333
Warrenville
Road
Lisle, IL 60532 Sanya Syrstad [email protected]

63
Serenity House
Counseling
Services, Inc.
891 S. Route
53
Addison, IL 60101 Tom Stamas [email protected]
Sherman Hospital 1425 N.
Randall Road
Elgin, IL 60123-
2300
Richard B.
Floyd,
FACHE
Sherman Hospital 1425 N.
Randall Road
Elgin, IL 60123-
2300
Rob
Schwichow
Silver Cross
Hospital
1200 Maple
Road
Joliet, IL 60432-
1497
Lisa Smith [email protected]
Silver Cross
Hospital
1200 Maple
Road
Joliet, IL 60432-
1497
Paul Pawlak [email protected]
Singer Mental
Health & Dev
Center
4402 N. Main
St.
Rockford, IL 61103-
1278
Amparo
Lopez
Sinnissippi Centers,
Inc.
325 IL Route 2 Dixon, IL 61021 Jim Sarver [email protected]
Sinnissippi Centers,
Inc.
325 IL Route 2 Dixon, IL 61021 Larry
Prindaville
Soft Landing
Interventions
1S224 Summit
Ave.
Oakbrook
Terrace, IL
60181 Abdel Fahmy [email protected]
Sojourn House, Inc. 565 North
Turner Ave.
Freeport, IL 61032 Dave Manson [email protected]
Southern Illinois
University, School
of Medicine
P.O.
Box
19604
Springfield, IL 62794-
9604
Robert
Wesley
Spillie and
Associates
1802 N.
Division St.
Morris, IL 60450 Anthony
Spillie
Stephenson County
Department of
Health
10 W. Linden
St.
Freeport, IL 61032 Executive
Director
Stepping Stones
Inc.
1621 Theodore
St.
Joliet, IL 60435 Paul
Lauridsen

64
Stepping Stones,
Inc.
1621 Theodore
St.
Joliet, IL 60435 Peter
McLenighan
Stepping Stones of
Rockford, Inc.
706 N. Main
St.
Rockford, IL 61103 Sue Schroeder [email protected]
Stepping Stones of
Rockford, Inc.
706 N Main St. Rockford, IL 61103 Stephen
Langley
Stonybrook Center,
Inc.
27W281
Geneva Road
Winfield, IL 60190 Frances M.
Walter
SwedishAmerican
Hospital
1401 E. State
St.
Rockford, IL 61104-
2298
William
Gorski, MD
SwedishAmerican
Hospital
1401 E. State
St.
Rockford, IL 61104-
2298
Ann Gantzer [email protected]
SwedishAmerican
Hospital
1401 E. State
St.
Rockford, IL 61104-
2298
Deb Wagner [email protected]
The Advantage
Group Foundation,
LTD
422 Tag Way Crystal Lake, IL 60014 Patrice Owens [email protected]
The Counseling
Center, Inc.
735 Mcardle
Drive
Crystal Lake, IL 60014 Donna
Schmidt-Baer
The Family
Connection
1548 Bond St. Naperville, IL 60563 Liberty Braun [email protected]
The Helen Wheeler
Center for CMH
275 E Court Suite
102
Kankakee, IL 60901 Jackie Haas
The IDS Group,
Inc.
1706 N.
Farnsworth
Aurora, IL 60505 Jim Fisher [email protected]
The Recovery Zone 707 First
Avenue
Rock Falls, IL 61071 Martin
Huntley
Thresholds 4101 N.
Ravenswood
Ave.
Chicago, IL 60613 Debbie
Pavick,
LCSW

65
Thresholds 4101 N.
Ravenswood
Avenue
Chicago, IL 60613 [email protected]
Tools for Life, Ltd. 35 S. Stolp
Ave.
Aurora, IL 60506 Shelley
Simmons-
Fiorito
Traffic School for
Behavior Change,
Inc.
54 N. Ottawa
St.
Joliet, IL 60432 Tamara
Santagelo
Transitional
Alternative Reentry
Initiative, Inc.
19 S.
Broadway
Aurora, IL
0505
Keith Knazze [email protected]
Transitions Mental
Health Rehab
805 19th St. P.O.
Box
4238
Rock Island, IL 61204 Executive
Director
Tricity Family
Services
1120 Randall
Court
Geneva, IL 60134 James R.
Otepka, MS,
LMFT
Tricon Counseling
Centers
380 S. Schmale
Road
Carol Stream,
IL
60188 Richard
Ordlook
Trinity David
Deopere
Trinity Services,
Inc.
100 N. Gouger
Road
Joliet, IL 60432 Art Dykstra [email protected]
Turning Point
Behavioral Health
Care Center
8324 Skokie
Blvd.
Skokie, IL 60077 Ann Fisher
Raney,
LCSW, BCD
Tylers Justice
Center
400 Front St. Stockton, IL 61085 Executive
Director
Valley West
Community
Hospital
11 E. Pleasant
Ave.
Sandwich, IL 60548-
1100
Brad Copple [email protected]

66
Van Matre
HealthSouth
Rehabilitation
Hospital
950 S. Mulford
Road
Rockford, IL 61108-
4274
Kenneth
Bowman
Virginia M. Mejia 1275 W.
Roosevelt
Road
West Chicago,
IL
60185 Virginia M.
Mejia
Visiting Nurse
Association of Fox
Valley
400 N.
Highland Ave.
Aurora, IL 60506 Executive
Director
Visiting Nurse
Association of Fox
Valley
157 S. Lincoln
Ave.
Aurora, IL 60505
Visiting Nurse
Association of Fox
Valley
1130 Sheffer
Road
Aurora, IL 60505
Visiting Nurse
Association of Fox
Valley
500 Tomcat
Lane
Aurora, IL 60505
Visiting Nurse
Association of Fox
Valley
620 Wing St. Elgin, IL 60123
Visiting Nurse
Association of Fox
Valley
56 Jackson Aurora, IL 60505
Visiting Nurse
Association of Fox
Valley
441 N.
Farsnworth
Ave.
Aurora, IL 60505
Vista Medical
Center East
1324 N.
Sheridan Road
Waukegan, IL 60085-
2199
Patricia
Kimbel
Vista Medical
Center East
1324 N.
Sheridan Road
Waukegan, IL 60085-
2199
Barbara J.
Martin
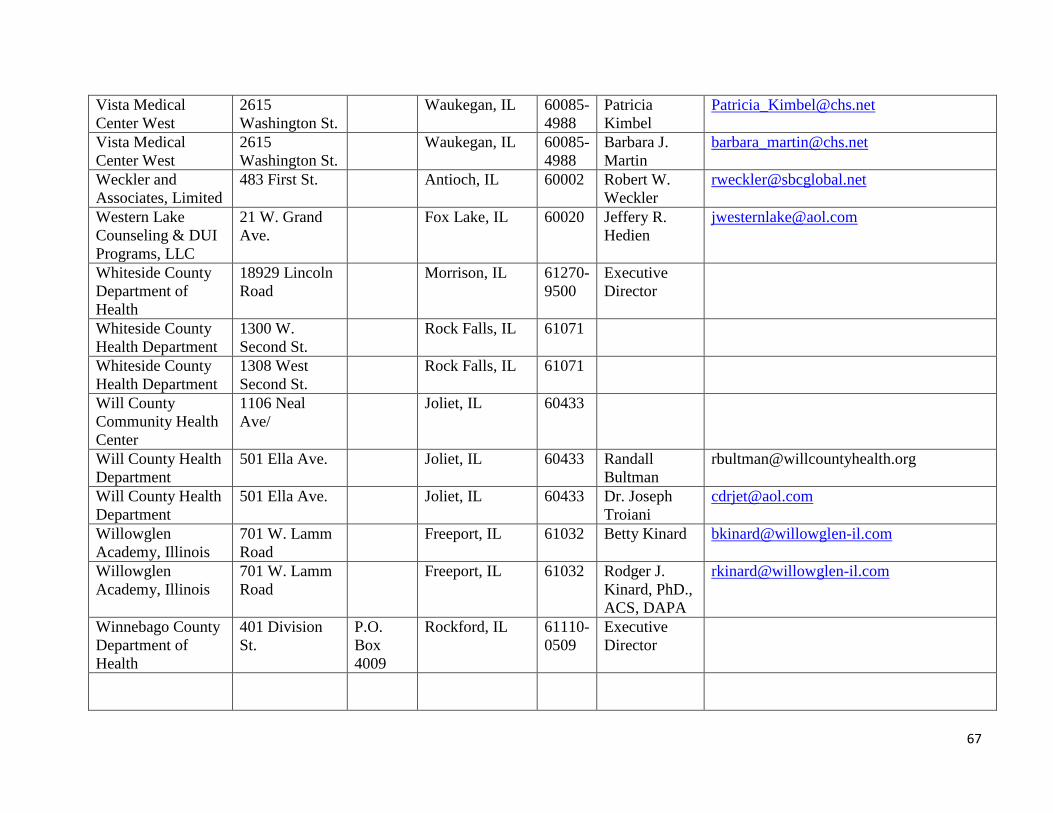
67
Vista Medical
Center West
2615
Washington St.
Waukegan, IL 60085-
4988
Patricia
Kimbel
Vista Medical
Center West
2615
Washington St.
Waukegan, IL 60085-
4988
Barbara J.
Martin
Weckler and
Associates, Limited
483 First St. Antioch, IL 60002 Robert W.
Weckler
Western Lake
Counseling & DUI
Programs, LLC
21 W. Grand
Ave.
Fox Lake, IL 60020 Jeffery R.
Hedien
Whiteside County
Department of
Health
18929 Lincoln
Road
Morrison, IL 61270-
9500
Executive
Director
Whiteside County
Health Department
1300 W.
Second St.
Rock Falls, IL 61071
Whiteside County
Health Department
1308 West
Second St.
Rock Falls, IL 61071
Will County
Community Health
Center
1106 Neal
Ave/
Joliet, IL 60433
Will County Health
Department
501 Ella Ave. Joliet, IL 60433 Randall
Bultman
Will County Health
Department
501 Ella Ave. Joliet, IL 60433 Dr. Joseph
Troiani
Willowglen
Academy, Illinois
701 W. Lamm
Road
Freeport, IL 61032 Betty Kinard [email protected]
Willowglen
Academy, Illinois
701 W. Lamm
Road
Freeport, IL 61032 Rodger J.
Kinard, PhD.,
ACS, DAPA
Winnebago County
Department of
Health
401 Division
St.
P.O.
Box
4009
Rockford, IL 61110-
0509
Executive
Director
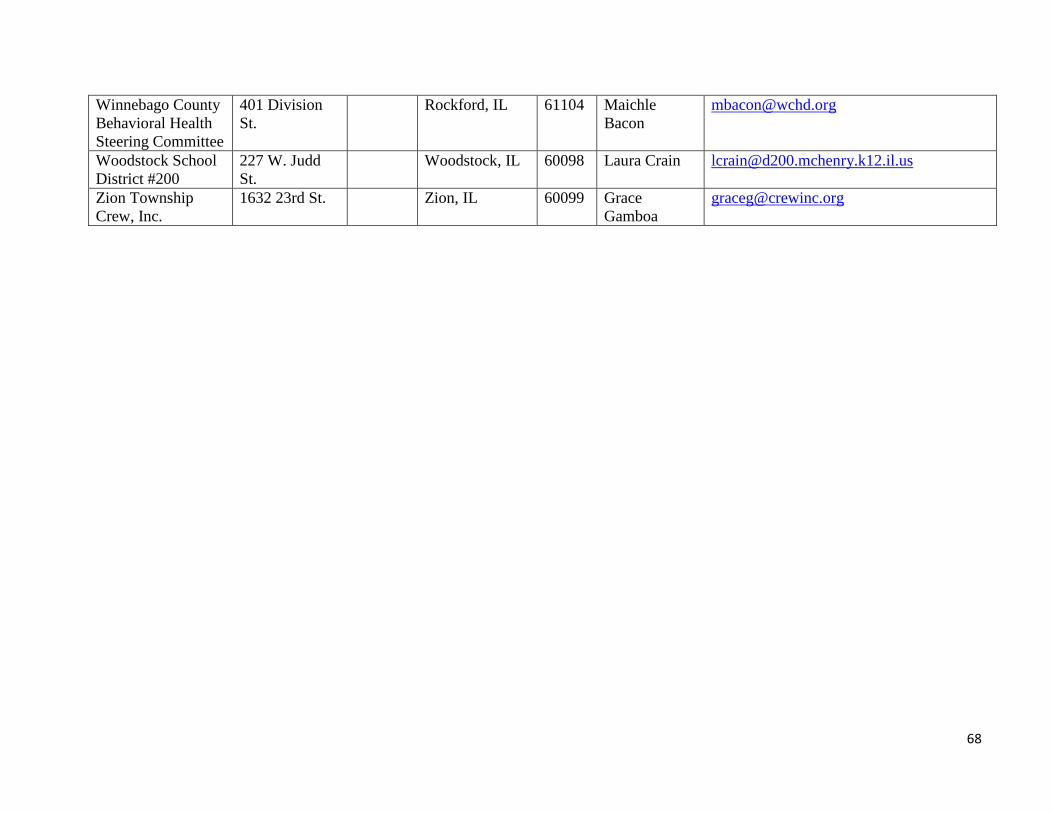
68
Winnebago County
Behavioral Health
Steering Committee
401 Division
St.
Rockford, IL 61104 Maichle
Bacon
Woodstock School
District #200
227 W. Judd
St.
Woodstock, IL 60098 Laura Crain [email protected]
Zion Township
Crew, Inc.
1632 23rd St. Zion, IL 60099 Grace
Gamboa
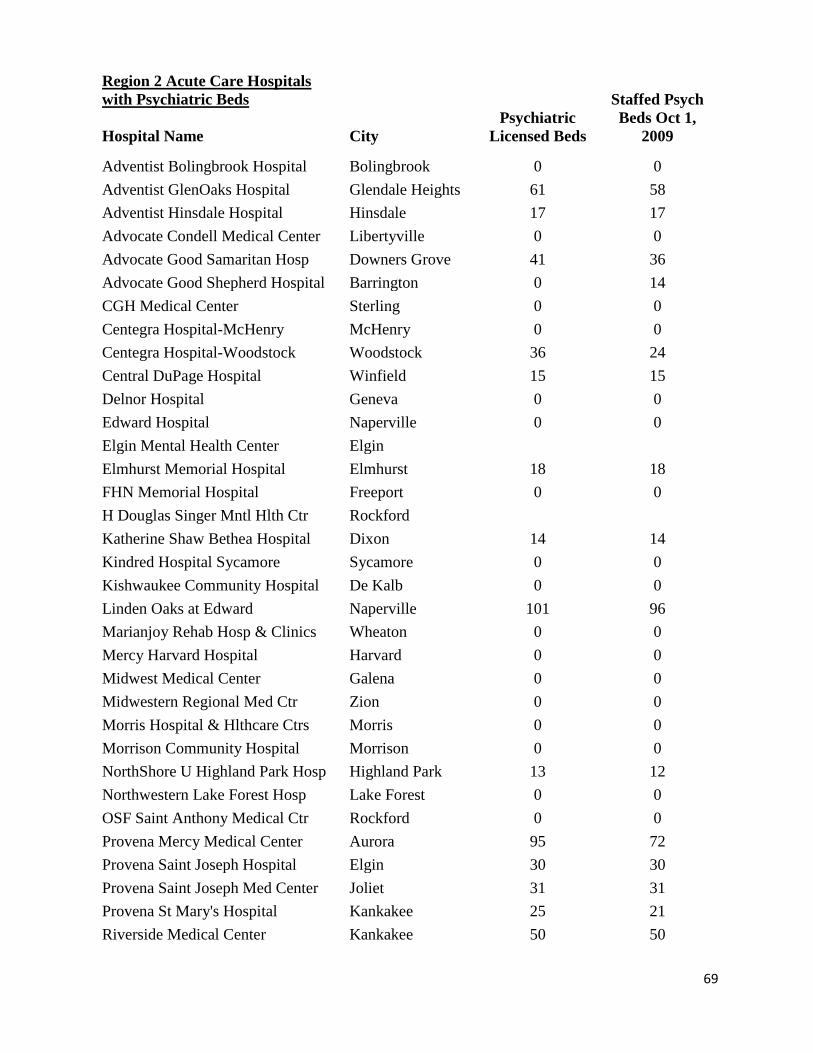
69
Region 2 Acute Care Hospitals
with Psychiatric Beds
Hospital Name City
Psychiatric
Licensed Beds
Staffed Psych
Beds Oct 1,
2009
Adventist Bolingbrook Hospital Bolingbrook 0 0
Adventist GlenOaks Hospital Glendale Heights 61 58
Adventist Hinsdale Hospital Hinsdale 17 17
Advocate Condell Medical Center Libertyville 0 0
Advocate Good Samaritan Hosp Downers Grove 41 36
Advocate Good Shepherd Hospital Barrington 0 14
CGH Medical Center Sterling 0 0
Centegra Hospital-McHenry McHenry 0 0
Centegra Hospital-Woodstock Woodstock 36 24
Central DuPage Hospital Winfield 15 15
Delnor Hospital Geneva 0 0
Edward Hospital Naperville 0 0
Elgin Mental Health Center Elgin
Elmhurst Memorial Hospital Elmhurst 18 18
FHN Memorial Hospital Freeport 0 0
H Douglas Singer Mntl Hlth Ctr Rockford
Katherine Shaw Bethea Hospital Dixon 14 14
Kindred Hospital Sycamore Sycamore 0 0
Kishwaukee Community Hospital De Kalb 0 0
Linden Oaks at Edward Naperville 101 96
Marianjoy Rehab Hosp & Clinics Wheaton 0 0
Mercy Harvard Hospital Harvard 0 0
Midwest Medical Center Galena 0 0
Midwestern Regional Med Ctr Zion 0 0
Morris Hospital & Hlthcare Ctrs Morris 0 0
Morrison Community Hospital Morrison 0 0
NorthShore U Highland Park Hosp Highland Park 13 12
Northwestern Lake Forest Hosp Lake Forest 0 0
OSF Saint Anthony Medical Ctr Rockford 0 0
Provena Mercy Medical Center Aurora 95 72
Provena Saint Joseph Hospital Elgin 30 30
Provena Saint Joseph Med Center Joliet 31 31
Provena St Mary's Hospital Kankakee 25 21
Riverside Medical Center Kankakee 50 50

70
Rochelle Community Hospital Rochelle 0 0
Rockford Memorial Hospital Rockford 20 12
Rush-Copley Medical Center Aurora 0 0
Sherman Hospital Elgin 0 0
Silver Cross Hospital Joliet 20 14
SwedishAmerican Hospital Rockford 32 32
SwedishAmerican MC/Belvidere Belvidere 0 0
Valley West Community Hospital Sandwich 0 0
Van Matre HealthSouth Rehb Hsp Rockford 0 0
Veterans Affairs Medical Ctr North Chicago
Vista Medical Center East Waukegan 0 0
Vista Medical Center West Waukegan 46 42
Region Total: 665 608
Source: Licensed Beds-IDPH Addendum to Inventory of Health Care Facilities
Staffed Beds-IDPH Annual Hospital Questionnaire, 2009.

Inpatient Discharges Cumulative % Change
SFY 2005 SFY 2006 SFY 2007 SFY 2008 SFY 2009 SFY 2010 From SFY 2005 to SFY 2010
Statewide 1,723,215 1,714,661 1,724,116 1,715,750 1,677,926 1,651,967 -4.1%
Region 2 25,654 23,318 27,005 27,484 27,741 28,116 9.6%
Source: COMPdata

72
SOH Inpatient Inpatient Discharges
Peds
Adults
Total
REGION FACILITY SFY 2007
SFY 2008
SFY 2009
SFY 2010
SFY 2007
SFY 2008
SFY 2009
SFY 2010
SFY 2007
SFY 2008
SFY 2009
SFY 2010
1C Madden MHC 0 0 0 0
4,242 4,151 3,654 3,674
4,242 4,151 3,654 3,674
1N Chic-Read MHC 0 0 0 0
1,913 1,788 1,848 1,829
1,913 1,788 1,848 1,829
1S Tinley Park MHC 0 0 0 0
1,721 1,473 1,784 1,823
1,721 1,473 1,784 1,823
Region 1 TOTAL 0 0 0 0
7,876 7,412 7,286 7,326
7,876 7,412 7,286 7,326
2 Elgin MHC 0 0 0 0 1,032 1,031 1,137 1,204 1,032 1,031 1,137 1,204
Singer MH/Dev Ctr 0 0 0 0 728 706 852 850 728 706 852 850
Treatment & Deten 0 0 0 0 4 9 9 6 4 9 9 6
Region 2 TOTAL 0 0 0 0
1,764 1,746 1,998 2,060
1,764 1,746 1,998 2,060
4 McFarland MHC 22 13 13 16
696 728 623 717
718 741 636 733
Region 4 TOTAL 22 13 13 16
696 728 623 717
718 741 636 733
5
Alton MH/Dev Ctr 0 0 0 0 197 198 191 188 197 198 191 188
Chester MHC 0 0 0 0 107 119 150 115 107 119 150 115
Choate MH and Dev 78 84 60 65 460 400 364 233 538 484 424 298
Region 5 TOTAL 78 84 60 65 764 717 705 536 842 801 765 601
TOTAL
100 97 73 81
11,100 10,603 10,612 10,639
11,200 10,700 10,685 10,720
No State Operated Inpatient Facilities in Region 3.
Mental Health and Substance Abuse Cases.
Source: Illinois Department of Human Services
Illinois Statistics
Office of Mental Health and Development Disabilities

73
*The Illinois Health Facilities Planning Board discontinued licensing substance abuse beds as a category of service on April 17, 2000.
this category was converted to medical/surgical beds.
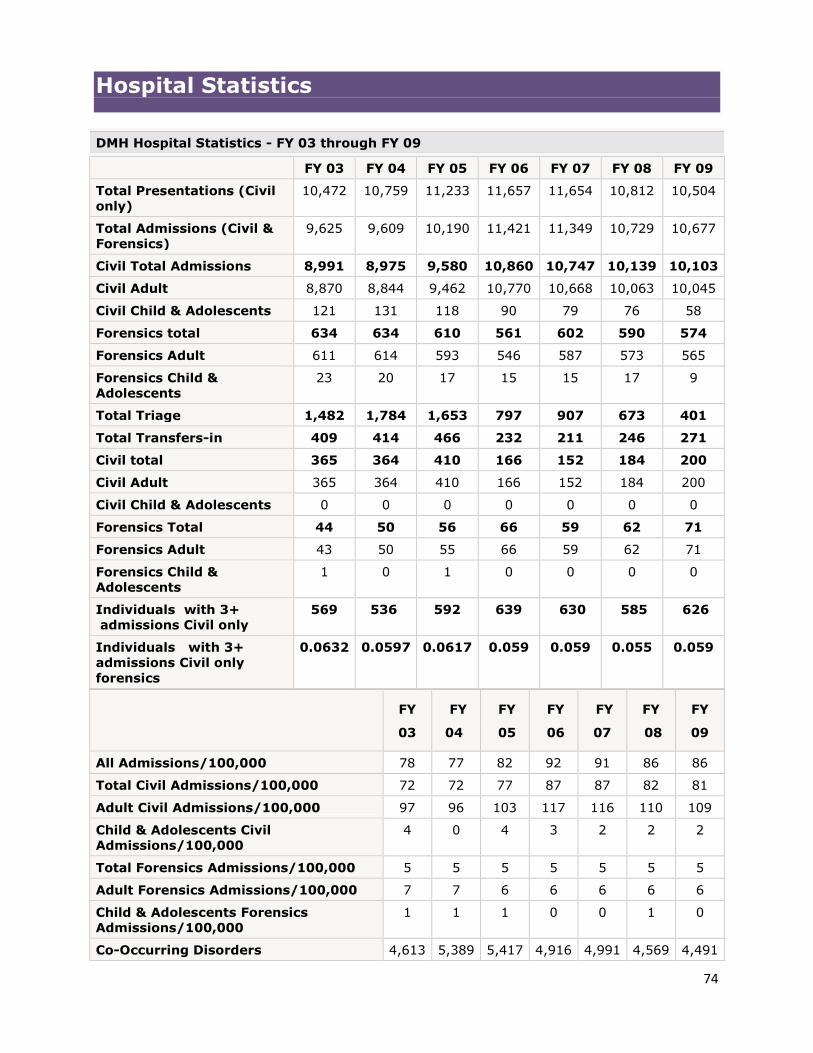
74
Hospital Statistics
DMH Hospital Statistics - FY 03 through FY 09
FY 03 FY 04 FY 05 FY 06 FY 07 FY 08 FY 09
Total Presentations (Civil
only)
10,472 10,759 11,233 11,657 11,654 10,812 10,504
Total Admissions (Civil &
Forensics)
9,625 9,609 10,190 11,421 11,349 10,729 10,677
Civil Total Admissions 8,991 8,975 9,580 10,860 10,747 10,139 10,103
Civil Adult 8,870 8,844 9,462 10,770 10,668 10,063 10,045
Civil Child & Adolescents 121 131 118 90 79 76 58
Forensics total 634 634 610 561 602 590 574
Forensics Adult 611 614 593 546 587 573 565
Forensics Child &
Adolescents
23 20 17 15 15 17 9
Total Triage 1,482 1,784 1,653 797 907 673 401
Total Transfers-in 409 414 466 232 211 246 271
Civil total 365 364 410 166 152 184 200
Civil Adult 365 364 410 166 152 184 200
Civil Child & Adolescents 0 0 0 0 0 0 0
Forensics Total 44 50 56 66 59 62 71
Forensics Adult 43 50 55 66 59 62 71
Forensics Child &
Adolescents
1 0 1 0 0 0 0
Individuals with 3+
admissions Civil only
569 536 592 639 630 585 626
Individuals with 3+
admissions Civil only
forensics
0.0632 0.0597 0.0617 0.059 0.059 0.055 0.059
FY
03
FY
04
FY
05
FY
06
FY
07
FY
08
FY
09
All Admissions/100,000 78 77 82 92 91 86 86
Total Civil Admissions/100,000 72 72 77 87 87 82 81
Adult Civil Admissions/100,000 97 96 103 117 116 110 109
Child & Adolescents Civil
Admissions/100,000
4 0 4 3 2 2 2
Total Forensics Admissions/100,000 5 5 5 5 5 5 5
Adult Forensics Admissions/100,000 7 7 6 6 6 6 6
Child & Adolescents Forensics Admissions/100,000
1 1 1 0 0 1 0
Co-Occurring Disorders 4,613 5,389 5,417 4,916 4,991 4,569 4,491

75
FY
03
FY
04
FY
05
FY
06
FY
07
FY
08
FY
09
Percent of Co-Occurring
Disorders Admissions
0.48 0.56 0.51 0.43 0.44 0.43 0.42
Numbers shown do not include individuals considered developmentally disabled based upon legal
status at time of episode. Calculation for Admissions 100,000: population
count/100,000=multiplier: number of admissions/multiplier = Admissions/100,000.
Report Date: 07/09/2009 Population Served: 12,419,293 - FY 03 thru FY 09
Utilization of Illinois State Psychiatric Hospitals
FY03 FY04 FY05 FY06 FY07 FY08 FY09
Length of Stay (All) Average 158 196 211 199 200 221 229
Length of Stay (All) Median 16 17 15 13 12 13 13
Length of Stay (Civil ALL) Average 100 119 125 113 104 111 108
Length of Stay (Civil ALL) Median 14 14 13 11 10 11 11
Length of Stay (Civil Adult)
Average
101 120 126 113 104 112 108
Length of Stay (Civil Adult) Median 14 14 13 11 10 11 11
Length of Stay (Civil Child &
Adolescents) Average
23 20 26 33 25 39 22
Length of Stay (Civil Child &
Adolescents) Median
170 210 394 402 411 426 433
Length of Stay (Forensic Adults)
Average
678 737 841 889 926 1,005 1,077
Length of Stay (Forensic Adults)
Median
171 212 394 403 416 427 436
Length of Stay (Forensic Child &
Adolescents) Average
144 180 334 339 338 283 274
Length of Stay (Forensic Child &
Adolescents) Median
127 127 280 353 214 150 282
Average Daily Census (All) 1,512 1,481 1,466 1,440 1,413 1,400 1,377
Average Daily Census (Civil) 942 882 866 844 806 800 778
Average Daily Census (Civil Adult) 935 874 861 840 802 796 775
Average Daily Census (Civil Child &
Adolescents)
8 7 6 5 4 5 4
Average Daily Census (Forensics) 570 599 600 596 607 600 598
Average Daily Census (Forensics
Adult)
561 588 585 582 597 590 593
Average Daily Census (Forensics
Child & Adolescents)
9 11 15 13 10 9 6
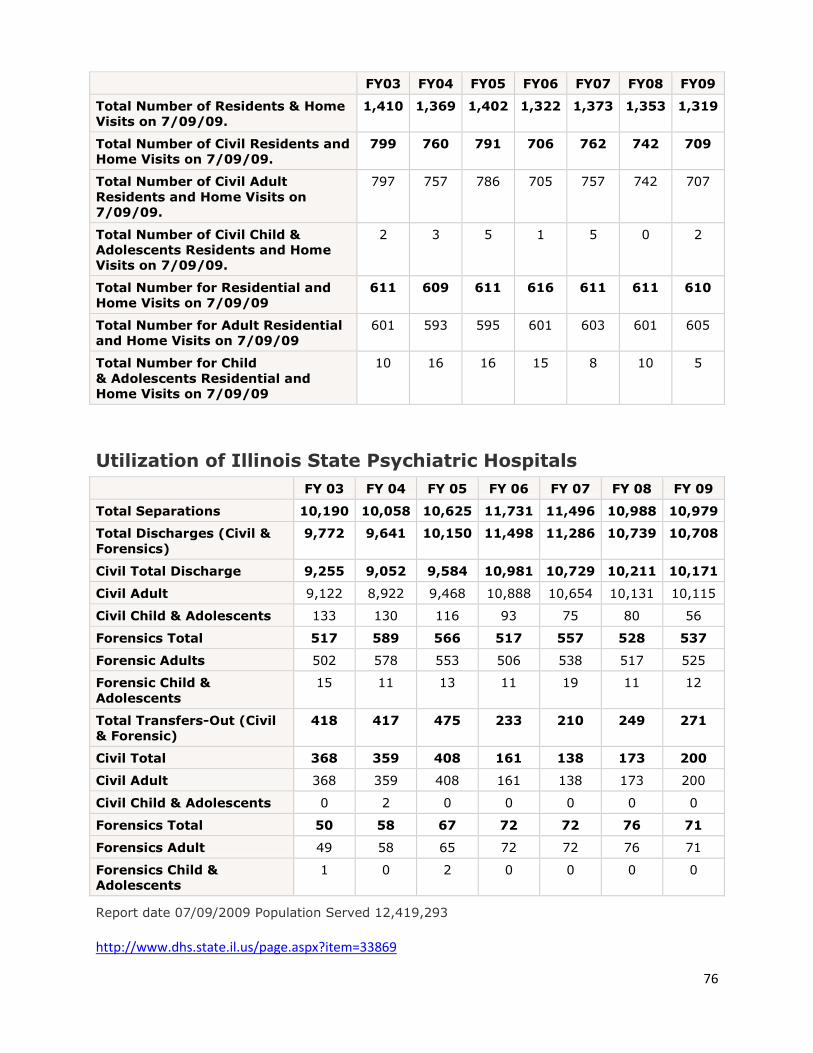
76
FY03 FY04 FY05 FY06 FY07 FY08 FY09
Total Number of Residents & Home
Visits on 7/09/09.
1,410 1,369 1,402 1,322 1,373 1,353 1,319
Total Number of Civil Residents and
Home Visits on 7/09/09.
799 760 791 706 762 742 709
Total Number of Civil Adult
Residents and Home Visits on
7/09/09.
797 757 786 705 757 742 707
Total Number of Civil Child &
Adolescents Residents and Home
Visits on 7/09/09.
2 3 5 1 5 0 2
Total Number for Residential and
Home Visits on 7/09/09
611 609 611 616 611 611 610
Total Number for Adult Residential
and Home Visits on 7/09/09
601 593 595 601 603 601 605
Total Number for Child
& Adolescents Residential and
Home Visits on 7/09/09
10 16 16 15 8 10 5
Utilization of Illinois State Psychiatric Hospitals
FY 03 FY 04 FY 05 FY 06 FY 07 FY 08 FY 09
Total Separations 10,190 10,058 10,625 11,731 11,496 10,988 10,979
Total Discharges (Civil &
Forensics)
9,772 9,641 10,150 11,498 11,286 10,739 10,708
Civil Total Discharge 9,255 9,052 9,584 10,981 10,729 10,211 10,171
Civil Adult 9,122 8,922 9,468 10,888 10,654 10,131 10,115
Civil Child & Adolescents 133 130 116 93 75 80 56
Forensics Total 517 589 566 517 557 528 537
Forensic Adults 502 578 553 506 538 517 525
Forensic Child &
Adolescents
15 11 13 11 19 11 12
Total Transfers-Out (Civil
& Forensic)
418 417 475 233 210 249 271
Civil Total 368 359 408 161 138 173 200
Civil Adult 368 359 408 161 138 173 200
Civil Child & Adolescents 0 2 0 0 0 0 0
Forensics Total 50 58 67 72 72 76 71
Forensics Adult 49 58 65 72 72 76 71
Forensics Child &
Adolescents
1 0 2 0 0 0 0
Report date 07/09/2009 Population Served 12,419,293 http://www.dhs.state.il.us/page.aspx?item=33869

Illinois Regional Integrated
Behavioral Health Network
Region 3
Draft Report

2
Table of Contents
Topics Page #
Region 3 Plan Introduction 3
Background 4
Characteristics of Region 3 5
Overarching themes in Region 3 5
Recommendations for Region 3 6
Meetings Letter of Invitation 11
Agenda July 18 12
Minutes July 18 13
Small Group Responses July 18 15
Agenda August 8 20
Minutes August 8 22
Small Group Responses August 8 24
Agenda August 22 28
Minutes August 22 29
Appendices PA 97-0381 31
Questionnaire 35
Region 3 Contact List 37
Psychiatric & Licensed Staffed Beds 40
Statewide & Behavioral Health Primary
Diagnoses Discharges 41
State Operated Hospitals Inpatient Discharges 42
ILHFB Bed Totals 43
Hospital Statistics 44

3
Illinois Regional Behavioral Health Networks
For hospital, primary care, mental health, substance abuse,
and other community-based providers
Region 3 Note: The content of this report does not reflect the opinion or position of the Illinois Hospital
Association.
Introduction
Budget cuts to human services, on top of a structurally weak and over-burdened behavioral
health system, have seriously compromised access to mental health and substance abuse services
in Illinois, as evidenced by the large and growing number of persons with these conditions.
Many are homeless and incarcerated. Others seek care from hospital emergency rooms.
Communities across Illinois, but especially in our rural communities, are attempting to address a
growing need with few available options. Limited resources, however, have never stood in the
way of a determined community willing to work together to solve a problem. Recognizing the
desire of our rural communities to improve not only access to mental health and substance abuse
services but also their ability to do so well, the Illinois Hospital Association worked with
members of the Illinois Legislature and other advocates to craft legislation that would provide a
platform for communities to act, proactively, to solve a serious problem for their communities.
The Regional Integrated Behavioral Health Act (HB2982/PA-98-0381) was enacted in 2011 both
as a response to a serious deterioration in the mental health system and as a proactive effort to
channel human and financial resources towards the creation of an effective and accessible system
of care. It also sought to capitalize on the opportunities that were being presented by federal
health reform, emerging clinical practices, and new models of care. In 2011, state budget cuts
had decimated many community mental health and substance abuse services. All but a few
programs for the uninsured were eliminated. Hospital emergency departments were overflowing
with persons with mental and substance use conditions in crisis. Our patients were in crisis. The
system within which they sought care was in crisis. There was no clear plan or vision in sight. By
calling for collaboration across providers, innovation, and creative thinking, HB2982 sought to
be a step towards building a system of care. The first step is to identify a vision, goals, and a plan
to achieve them.
The Regional Integrated Behavioral Health Networks Act (HB2982/P.A.98-0381) provides a
platform for the establishment of regional behavioral health networks in each of the five Illinois
Department of Human Services regions and for a DHS-facilitated statewide steering committee
comprised of relevant state agencies and stakeholders. It requires each region to identify existing
relevant mental health, substance abuse, social service and health resources; gaps in services,
including areas in which access to care is seriously limited; and services that are needed to serve
the needs of the regions’ people. This information will be compiled as a regional plan and will be
shared with the statewide steering committee and ultimately with the Illinois General Assembly.

4
This legislation recognizes the urgency of the need to improve access to care and the corollary
need to use community resources wisely and creatively. It establishes a process and forum within
which a variety of community stakeholders can assess what is needed to serve persons with
mental and substance use illnesses within their respective communities and develop a plan to
address these needs. It recognizes that what is needed in one region may not necessarily be true
for another.
It identifies a consultative, supportive role for the Illinois Department of Human Services that
will be executed through a statewide steering committee comprised of several state agencies
responsible for funding or regulating mental health, substance abuse, and health care services.
The state wide and regional committees will interact synergistically to identify opportunities not
only to address current services deficiencies but most importantly to identify ways in which to
integrate behavioral and primary health care and thereby build the health system of the future.
Integration of services is cost effective, and it improves patient outcomes.
A copy of the legislation is contained in the appendices of this report.
Background
Region 3 Planning Process
The Region 3 planning meetings have followed similar such planning meetings in Regions 2, 4,
and 5. Each region has brought together a cross section of the medical, mental health, substance
abuse, social services, and other community entities to identify the nature and scope of the
challenges facing persons who need services for a mental or substance use condition in their
respective areas. They have convened to identify solutions both in the short term and long term,
drawing upon the collective resources of their communities and their commitment to improve
access to high quality health care.
Each region has specific and unique characteristics which are addressed in their respective plans.
The Region 3 likewise, will reflect the unique features, challenges, and opportunities of central
and western Illinois. However, there are themes that run through all of the regions. These
include: a general lack of sufficient resources to meet demand, especially in rural Illinois; use of
crisis and acute services to a large and growing extent because so many less intensive
community services have been reduced or lost; a willingness to embrace integration of care
across primary and specialty behavioral health but little experience doing so; varying degrees of
success and experience adopting technology such as telemedicine/psychiatry to expand
availability of specialty psychiatric services; a shortage of psychiatrists, especially child
psychiatrists; and uncertainty of funding now and in the future.
Providers and community stakeholders all have demonstrated a “can do” commitment to their
patients/consumers and communities through their participation in the planning process, by
sitting at a common table to brainstorm ideas and develop concrete solutions to pressing
community and patient/consumer needs.

5
Characteristics of Region 3
Region 3 is located in central and western Illinois. The region includes four “other urban” cities:
Peoria, Bloomington, Champaign, and Rock Island/Moline. The remainder of the region is rural.
Refer to the Appendices for a description of acute psychiatric beds and services and other data.
Overarching themes in Region 3:
There was consensus around and support of region-specific planning, noting that a
statewide plan will fail to capture the unique characteristics and needs of a specific
region. Consideration also should be given to sub-regions that will have a different
constellation of services, resources, and needs. In Region 3, there are distinct sub-
regions, e.g., Peoria, Champaign, Bloomington, quad Cities, rural.
The lack of psychiatric capacity, particularly for children and adolescents, thwarts the
development of new models of care and use of technology to enhance access. There are
not enough psychiatrists in the pipeline to improve the situation. Use of non-physician
professionals such as APNs or PAs for persons who need medication management, and
other mental health and substance abuse professionals for persons with conditions that do
not require medication or for conditions that may be appropriately addressed by these
professionals is one strategy to address the shortage of psychiatrists. Other ideas may
include easing J1 visa requirements, loan forgiveness for physicians going into child
psychiatry, improving payment rates for psychiatrists.
Telepsychiatry and telemedicine are being used by some; all recognize the value of using
this technology to improve access to care in rural areas of Illinois. There is a range of
experience and understanding of the technology. One hospital is using a software
package that is affordable ($1,000 for license per station) and easy to use. Others are
struggling with the technology and expense. Information about the variety of hardware
and software packages available would be helpful. Staff training and necessary IT
supports needed are also important considerations in implementing telepsychiatry. As
noted above, the biggest challenge with telepsychiatry is finding psychiatrists to do it.
Crisis services are needed for all, but especially for the psychotic patient and the person
with a substance abuse condition. Children have access to SASS services, but there are
limited acute care and psychiatric services available to these children. As a consequence,
they are cycling in and out of the SASS crisis system.
With the closure of Singer Mental Health Center, the region will have fewer inpatient
resources than they have currently. What is currently available is not sufficient to meet
demand. The loss of acute services will shift demand to other venues such as hospital
EDs, community providers, and law enforcement. The loss of capacity in one region also
shifts services demands onto other areas of the state. This occurred when the Zeller
Mental Health Center closed in Peoria.
6
Loss of the SOH also reduces a level of care for patients who require longer lengths of
stay. Private hospitals have experienced an increase in the numbers of patients who
require longer stays than are customary, for these settings and which ordinarily are not
allowed /approved by utilization and quality entities reviewing inpatient care in behalf of
Medicaid, Medicare and others. Use of beds by a long-term patient in a unit designed for
acute stabilization also limits access to this level of care by patients in crisis.
The loss of facilities for persons with developmental and intellectual disabilities also
further strains hospital EDs and inpatient psychiatric units. Other community resources
frequently do not have the staff or expertise to manage a person who is acting out. The
system is not designed to provide ready access to the level of care these persons need.
Rural hospitals are caring for a large and growing number of persons with mental and
substance use conditions, straining the resources of organizations that were not designed
to provide this level of specialized care. The growing use of the ED and hospital beds is
symptomatic of the lack of other community resources. These hospitals appreciate any
and all assistance that supports their efforts to care for persons with mental and substance
use conditions and are eager to collaborate with specialty behavioral health organizations
to improve access to appropriate behavioral health care.
Recommendations
Access to Care: Delivery System Innovation
Region 3 is predominantly a rural region in which services are not consistently available in every
community. Recent budget cuts to the substance abuse and mental health and child care
providers have caused programs to close or to reduce their size and scope. Acute care services
also are limited—there is one state-operated psychiatric hospital where there once had been two;
there is one freestanding private psychiatric hospital providing services to children and
adolescents as well as adults; there are two psychiatric units in acute care hospitals providing
services to adolescents; and there are a handful of acute hospital inpatient psychiatric units in the
region serving adults. Examples of patients waiting days and weeks for an inpatient bed in a
state hospital or any hospital abound.
Access to care is defined by poverty, geographic distances separating consumers and providers,
and shortages of healthcare and behavioral health professionals. Although persons in this region
experience difficulty finding many services, they have almost no substance abuse residential
services available in the region, and they are experiencing waiting lists for child psychiatrists that
are far too long to meet the need of the region’s children.
Recommendations:
Care should be coordinated and integrated across settings. It should include the full
continuum of care, including prevention, early intervention, acute and rehabilitative
services, and wrap around services such as housing, and case/care management. Care
management is essential to support access in a timely manner to the appropriate level of
7
care, to support adherence to a treatment regimen, and to intervene when a person is
unable to obtain services because of family issues or lack of transportation. Care
management is an essential and necessary component of services package for persons
with a serious, chronic illness such as a mental illness.
Crisis capacity needs to be built into the system—either by building a crisis center,
adding crisis beds to a hospital or a residential treatment program. Capital is needed to
support the development of these services.
Observation beds/units in either a hospital or residential treatment center need to be
expanded and developed for those persons who need up to 48 hours of observation. This
is an opportunity for collaboration across systems of care, using community providers
and hospitals, and Emergency medical services (EMS) services. (Note that our laws may
need to be revised to support new crisis models of care.)
The EMS system provides information about the availability of ICU beds in a respective
system. A hospital ED can call the EMS system to determine whether or not an
appropriate ICU or trauma service is available. Explore similar capabilities for
psychiatric beds. This would be challenging, given the different types of patients
facilities and providers are able to treat, but it will provide an additional communications
vehicle for providers and should reduce wait times for persons in hospital EDs.
Inpatient beds are inadequate to meet demand. They should be expanded. No additional
civil beds should be removed from the public system. Attention should be paid to
policies that undermine the continued viability of the private acute inpatient beds.
There needs to be a place and accommodation for the unmanageably violent patient.
Care of such a patient requires one-on-one or more staff 24/7. This is a role the SOH has
assumed in the past. With the closure of SOHs, private hospitals will not have the
physical space to accommodate the violent patient, and they will not have the staff to
provide one-to-one care. The state has been unwilling to pay for this level of staffing. If
the state psychiatric hospital is closed and the private hospital is unable to care for the
violent patient, the person will be directed to the criminal justice system. This puts the
patient in a compromised position because law enforcement is not always willing to take
the patient who may be assaulting staff because they are not equipped to manage the
person. Law enforcement oftentimes sees the ED as the best place for such individuals.
This is an example of the “hot potato” syndrome, in which our patients are unwitting
participants.
Services for Veterans are needed to serve a large Veteran population in the Peoria and
Bloomington communities
Children’s services should follow the EPSDT model.
There is an urgent need to develop specialized services for persons with
intellectual/developmental disabilities.
8
Substance abuse services are limited in this region and should be enhanced. Level I and
II services (ASAM) are not funded sufficiently and are only available on a limited basis.
There are waiting lists for these services. Residential services are no longer available in
this region. There is no medical detoxification. Rural hospitals lack the expertise to
manage a patient who needs specialized detoxification care. Partnerships between
hospitals and DASA providers should be developed to address this population.
Financing/Payment
The uninsured and underinsured patients are the most disenfranchised in the system. State
funding cuts to grants and funding of services for person who do not qualify for Medicaid and do
not have any other insurance have been drastic, leaving these persons with little or no access to
community services. Substance abuse providers have eliminated complete product lines in the
wake of funding cuts; community providers have also eliminated or limited services that are no
longer funded. Non-institutional providers such as psychiatrists and other mental health
professionals may not accept Medicaid let alone those who lack any means of payment. These
persons either do not receive treatment or they receive it in crisis, in an emergency department or
other crisis setting.
Recommendations:
Funding must remain available for persons who do not qualify for Medicaid and have no
other means of funding their health or behavioral health care. The Medicaid domination
of the system is leaving many with no options except emergency departments, the streets,
or jail.
Research and pursue opportunities to obtain federal grants to support innovative services,
children’s services, and other Medicaid options.
Medicaid rule 132 services are defined too narrowly for children, making it very difficult
to find outpatient services for kids.
Eliminate the financing rules that limit specific services to a setting licensed by one
agency. This limits flexibility and choices and adds administrative complexity and costs.
Protect critical access hospital funding which is under threat. They are on the front lines
in many rural communities.
Support agreements between hospitals to provide psychiatric care to patients; support
agreements between hospitals and other community providers. Flexibility is necessary to
address unique characteristics and needs of the rural communities developing such
relationships.
9
Workforce
Integration of behavioral and medical care is good for patients/consumers. To advance
integration between behavioral and other medical care, staff in both sectors needs training.
Primary care physicians need training to enable them to treat patients with psychiatric or
substance use conditions in conjunction with behavioral health specialists and psychiatrists.
Areas in which the PCP can provide traditionally behavioral services: identification of a
psychiatric or substance use disorder, monitoring of a stable patient, prescribing medication for
certain conditions such as depression. Pediatricians can play similar roles.
Recommendations:
Health professionals across the spectrum of medicine, mental health and
substance abuse will need to be cross-trained in each other’s disciplines.
Use non-physician medical professionals to expand the reach of the physicians:
Advanced practice nurses (APNs) are valuable resources especially in delivering
services to children. They also are able to monitor medication and other physical
health needs.
Consider loan forgiveness and other incentives to encourage medical students to
go into psychiatry and to practice in a rural community.
Train all medical students about mental health and addiction issues.
Provide incentives such as scholarships, grants or loan forgiveness for persons to
enter any of the health and behavioral health professions that are not available to
rural communities.
Educate first responders about appropriate ways in which to care for a person
experiencing a mental health crisis.
Educate teachers and others in schools to recognize behavioral health conditions
in their students. Provide resources to the schools to refer students appropriately.
Quality of Care
The right care should be delivered in the right place, at the right time, to every patient.
Recommendations:
Accredit care managers. Standards exist.
Take the American Academy of Pediatrics assessment tool kit to the next level. This
should facilitate care integration across primary and behavioral care.

10
Use evidence-based/–informed practices at every level of care. Fund the use of these
services; disseminate those practices that are available (e.g., SAMSHA has a list of EBPs
on their web site.)
The ACES study provides a predictive model that many in primary care and behavioral
health care could use.
Apply the current Illinois DOC Assist model, which provides phone access for Medicaid
kids to a primary care physician, to adults.
Technology
Telepsychiatry and telemedicine are tools to improve access to all health care in rural Illinois,
including and especially psychiatric care. We are not going to meet the current and growing need
for specialized psychiatric services in rural communities without reaching out to other
geographic areas in which these professionals live and practice. Moreover, our medical schools
are not training enough primary care and psychiatrists to meet current and future demand.
Recommendations:
Medicaid in Illinois should pay a psychiatrist the same amount for a telepsychiatry
encounter as they do for a face-to-face encounter.
Current law requires that a physician be credentialed by an Illinois hospital in order to
provide telemedicine services. If a physician is credentialed by an accredited and licensed
hospital in another state, or he or she is a licensed physician in Illinois, this hospital
privileges issues should not be necessary.
Transportation
Transportation to behavioral health and other healthcare services is frequently a function of a
person’s ability to get to them. Some communities relay on public ambulance services, a few
have a private ambulance company, all have limited options—especially in circumstances
involving a mentally ill person who may be difficult to manage. The Division of Mental Health
pursuant to statute provides transportation to persons with mental illness who are being
transferred to a mental health facility on an involuntary admission status. These services are not
available to an adult who seeks treatment willingly, i.e., is a voluntary patient, or for children and
adolescents. For voluntary adults, this policy may force an individual to choose a status he or she
does not wish; there may be stigma associated with involuntary status; there are legal
consequences to being admitted on an involuntary status (e.g., FOID card denial or revocation).
Recommendation:
Transportation services should be available for the voluntary adult and for children and
adolescents under certain circumstances.

11
June 29, 2012
Name
Title
Organization
Address
City, State Zip
Dear:
As providers, we know that persons with mental and substance use illnesses in Illinois must navigate a
complex amalgam of services that are inconsistently available and accessible. Many seek care from us in
crisis because they could not obtain more timely or appropriate care. Our state and federal fiscal crises
have translated into the loss of essential behavioral health services particularly in rural Illinois. Yet,
despite these challenging circumstances, we can also identify opportunities to improve care. Some of
these opportunities stem from health reform; others are being generated by our own strategies to serve our
patients and communities. One such opportunity is being presented to us by the 2011 enactment of House
Bill 2982 – Public Act 98-031, which creates the Regional Integrated Behavioral Health Networks Act.
The bill establishes Regional Integrated Behavioral Health Networks to ensure and improve access to
appropriate mental health and substance abuse services throughout Illinois by systematically organizing
all relevant health, mental health, substance abuse, and other community resources among regional
providers, to develop a mechanism to use regional resources efficiently and effectively.
Under the Act, each Behavioral Health Regional Network shall develop a strategic plan for its respective
region that addresses the nature and scope of existing services, identifies community needs and defines
opportunities to improve access to care. The Act contemplates a broad-cross section of the mental health,
substance abuse, health, and social services community will be involved in the development –and
implementation—of the plan. Collaboration among all of the relevant community resources will be
essential to accomplish the purposes of the Act and to build effective, coordinated and comprehensive
systems of care.
You are invited to participate in the Behavioral Health Regional Network meetings for DHS Region 3.
The first meeting will take place Wednesday, July 18 from 10:00 am to 1:00 pm, in the Methodist
Atrium Building, 900 Main Street, on the campus of Methodist Medical Center of Illinois, in Peoria.
(Please park toward the back of the lot across from the Atrium.)
Please note that the second meeting is scheduled for Wednesday, August 8, at Bridgeway, Inc, in
Galesburg. The third meeting will be held on Wednesday, August 22, at The Center for Children’s
Services, in Danville. You will receive separate invitations to these meetings.
If you have any questions or concerns, please contact IHA Staff: MaryLynn M. Clarke at 217-541-1154
Please confirm your attendance for the July 18 meeting by contacting Stacey Dunlap at 217-541-1151 or
email your response to [email protected].
Thank you,
MaryLynn M. Clarke
Senior Director, Health Policy & Regulation

12
Illinois Behavioral Health Network Meeting – Region 3
July 18, 2012, 10:00 am – 1:00 pm
Methodist Medical Center of Illinois
221 NE Glen Oak Avenue
Peoria, IL 61636-0002
Agenda
I. WELCOME & INTRODUCTIONS ................10:00 ........................ Dean Steiner
II. OVERVIEW OF HB 2982 (PA 97-0381) .........10:20 ............. ..MaryLynn Clarke
III. REGIONAL PLAN DISCUSSION GROUPS..10:25 ................................. Groups
o What should the behavioral health system look like 3 years from now?
o What would be the key components of the new behavioral health system?
o Are there immediate actions that could be taken to improve access to behavioral
health services in this region? If so, what are they?
IV. SMALL GROUP REPORTS ............................11:30 ............... MaryLynn Clarke
V. SETTING PRIORITIES & NEXT STEPS ....12:15 ........................ Dean Steiner
o Provider Questionnaire
VI. ADJOURNMENT & NEXT MEETING ........1:00 .......................... Dean Steiner
Next Meeting: August 8, 2012
Bridgeway, Inc.
2323 Windish Drive, Galesburg, IL
13
Illinois Behavioral Health Network Meeting – Region 3
July 18, 2012
Methodist Medical Center, Peoria
Stephanie Barisch, The Center for Youth & Family Srvs
Melissa Black, Carle Foundation Hospital
Terry Carmichael, CBHA
Greg Chance, Peoria County Health Department
MaryLynn Clarke, Illinois Hospital Association
Joe Croegaert, DHS/DMH
Laurelyn Cropek, Community Resource & Counseling Ctr, Inc.
Sally Davidson, DHS/DMH
Dennis Duke, Robert Young Center
Sheila Ferguson, Community Elements, Inc.
Carol Flessner, Livingston County 708 Board
Michael Freda, Robert Young Center
Charlene Guldbrandsen, GROW in Illinois
Nancy Greenwalt, Promise Healthcare
Christine Kahl, South Side Office of Concern
Gail Koch, OSF Medical Group
Dietra Kulicke, Chestnut Health Systems
Erin Laytham, Illinois Association of Rehab Facilities
Jordan Litvak, DHS/DMH
Michelle Locke, Graham Hospital
Victor Martino, Rose Medical Association, Inc.
Adam Meuser, Community Health Care, Inc.
Ed Michaels, Center or Children Services
Don Miskowiec, North Central Behavioral Health Systems
Rhonda Nelson, Bridgeway, Inc.
Fred Nirde, Human Service Center
Patrick Phelan, Children’s Home Association of IL
Arlin Pinto, Human Service Center
Thom Pollack, Crosspoint Human Services
John Reinert, North Central Behavioral Health Systems
Caterina Richardson, Tazwood Mental Health Center
Dennis Rodeghero, OSF St. Elizabeth Medical Center
Ernest C. Rose, Rose Medical Association, Inc.
Don Russell, New Directions
Melvia Russell, New Directions
DeeAnn Ryan, Vermillion County MH 708 Board
Amber Sturgeon, Galesburg Cottage Hospital
Bruce Suardini, Prairie Center Health System
Tom Troe, DHS/DMH
Joe Vaughan, Institute for Human Resources
Gary Weinstein, Transitions Mental Health Services
Micky Will, Community Elements, Inc
Rick Zehr, Institute of Physical Medicine & Rehab
I. Welcome & Introductions
Dean Steiner called the meeting to order at 10:00 a.m., and those in attendance
introduced themselves. Mr. Steiner provided a snapshot of the environmental issues
challenging the delivery of behavioral health services in Illinois. Notwithstanding these,
he noted that the group was not there to focus on problems but, rather, to find solutions.
II. Overview of HB 2982 (PA 97-0381)
MaryLynn McGuire Clarke provided an overview of HB2982/PA 97-0382, legislation
which requires the Department of Human Services to facilitate the creation of Regional
Behavioral Health Networks in each DHS region to ensure and improve access to
behavioral health services. The legislation provides a platform for providers across the
continuum of care to collaborate, build on existing community resources, identify needed
services, and work collaboratively to develop region-specific plans. Region 3 is the fourth
DHS regional group to meet in 2012. The legislation also created the Regional Integrated

14
Behavioral Health Networks Steering Committee, which will be comprised of state
agencies, advocacy and trade associations, and a representative of each of the five DHS
regions.
III. Regional Plan Discussion Groups
Participants were divided into groups to discuss three questions: (1) What should the
behavioral health system look like three years from now? (2) What would be the key
components of the new behavioral health system? (3) Are there immediate actions that
could be taken to improve access to behavioral health services in this region? If so, what
are they?
IV. Small Group Reports
Mr. Steiner asked a representative of each of the break-out groups to report on their
findings and recommendations. The information from the break-out groups is included in
the attached document.
V. Setting Priorities & Next Steps
The recommendations collected at the meeting will be shared with participants before the
next planning meeting. Participants in the second meeting will set priorities and develop
specifics of their regional plan.
VI. Adjournment & Next Meeting
Mr. Steiner noted that the next meeting will be held August 8, at Bridgeway, Inc. in
Galesburg, at 10:00 a.m.
15
July 18 Small Group Notes
Group 1
System Components - 3 Years
Integrated – bidirectional for (high utilizers of care)
- MH/SA patients
- Older adults
- DD/MR
Need managed integration
Medical Home
- B.H. Home
Need standard vehicle to reach this
Need community points of access
Intercept model which will ensure quality and lower costs
Need integration of providers (medical, B.H., S.A., DD/MR, Public Health)
Need to reduce regulatory and financial silos
Need Consistency of funding
Development of interceptor points that can deflect from an ED admission
Improved technology and use of it
Telemedicine
Integrated EMR
Key Components
Incentivize integrated organizations with shared risk reward
Education
- Prevention
- Organization cooperation
- Community
- Cross Integration
Balancing regulatory requirements with reality of available resources
Education process of all stakeholders
Health care Navigator
Strategic planning process in local communities throughout region
Immediate Actions
Expand mental health first aid in communities
Include higher education institutions, re: internships
Utilizing recovery model across all settings
Embrace all evidence based models that demonstrate fidelity
16
Group 2
System Components- 3 years
Access/capacity for all (i.e., uninsured)
Cost effective delivery system that is outcome-based, evidenced-based
Enhanced crisis service – Deflection from ED - No cuts
Improved outpatient treatment continuum
Primary Behavioral Integration (MH, CD)
- Reimbursement structure - Parity
- Learning collaborative – Bidirectional
- Screening – CD, MH – (Reimbursement)
Prevention/screening – CD, MH
Reimbursement for consultation between PCP and MH providers
Integrated Medical Record – Access for all providers
Increased use of peer services/community support groups
Reimbursement structure that support full treatment continuum including employment
services (IPS) and housing
Follow-up care
Alternative funding services (i.e., drug companies)
Key Components
Integration– PC/BH
Consistent reliable funding – Update reimbursement rate
Evidence/outcome based
Single regulatory body/streamline regulations
Practical workforce development
ED training that supports integrated delivery model
Timely access to treatment and medications
Community collaboration
Immediate Actions
“Show me the money” Dr. Pinto…
Community education forums – All stakeholders:
Providers
Courts
State Agencies
Law
Schools
Service directory by community
Enhanced crisis services
17
Group 3
System Components - Three Years
Integrated
Interdisciplinary Teams
Funded – Blended pay system
Uninsured compensated
Immediate access
Comprehensive
Integrated medical records
Public policy commit to managed care vs. cost
Preventative vs. reactive
Community agencies funding for EMR
Evidenced based
Aligning clinician to payer
Cohesive language
Easier to access Medicaid and other funding
Key Components
Technology as asset
EPSDT
Person centered/individualized
Ready access
Care Coordination
Structured
Integrated and human services
Community support
Training and education
Salary/compensation
Regulatory regs
Workforce
Consumer accountability
Transportation
Immediate Actions
Telehealth and 3rd
party reimbursement
Consents
Blended funding
Resource link (OSF)
Training
Advocacy
Parity implementation
Pharmacy
- Access to 340B

18
Access to National Health Service Corp
Identifying value
- Common definition
Improve outcomes for clients
Conversations with non-traditional payers
Group 4
System Components - Three Years
On-time payments
Consumer and provider input and participation at all stages of development
More accountability tied to resource allocation (budgeting for outcomes)
Less silos
More consistency in requirements
Access to a full spectrum of services (levels of intensity)
- Expand continuum of services
- Pager issues resolved
- Severity getting care
- Adequate transportation
Valid mean of determining levels of care consistently
Care coordination teams – including all providers
- Conflict-free care coordination
- Consumer oriented
- Flexibility based on specific community needs
- Role of health homes
- Defined referral from primary HC
- Communication back and forth
Common IT system (EMR)
- Appropriate confidentiality safeguards
Workforce expansion
- Peer and para-professional
- Training and curriculum
- Allowing more home based services and community based services (natural
environments)
Community educations
- ER diversion
- Planned health care access
Sustainable financial model (support prevention and early intervention)
- Infrastructure capacity grants
- Government payers (fed, state, county, local)
- Private insurers
- Fed block grant utilized for non-Medicaid services
Unified goal, unified approach
- Direction

19
- Legislation
- Finances/budgeting
- Funding streams that support the whole system
Adult specific vs. child specific services (unique, need recognized)
- Less emphasis on medical treatment model
- More emphasis on global treatment model
Key Components
Care coordination – communication at all levels (funding, providers, accountability)
Health Information Technology (telemed – telepsy)
Adequate funding – sustainable financial modeling – systemic
Integration between state and local planners
Health homes
Less institutional care settings
Full continuum of services
Focus on prevention and early intervention (wellness)
Regional flexibility
Standardized outcome metrics
Recognition of co-occurring treatment
Confidence in state leadership – at department level
ER diversion projects – statewide
Workforce expansion – workforce support
Consumer and provider participation at all levels
Trauma — informed treatment
Evidence – informed treatment
Adequate transportation system to enable access
Immediate Actions
Borrow money to pay down Medicaid backlog
Seek to inform our legislative officials
Establish a coherent vision for behavioral health within Health Care Reform
Immediate coordination between state agencies (DASA, DMH, HFS, Gov, DCFS)
Establish a regional consortium with all key stakeholders (seek to maintain)
Coordination between various planning groups
20
Behavioral Health Regional Network Meetings – Region 3
August 8, 2012, 10:00 am – 1:00 pm
Bridgeway, Inc.
2323 Windish Drive Galesburg, IL
Agenda
I. WELCOME ........................................................10:00 ............................ Bill Nelson
II. SUMMARY OF FIRST MEETING.................10:20 ...................... ..Dean Steiner
III. FOCUS ON PRIORITIES…………………….10:25 .................................. Groups
A. DELIVERY SYSTEM IMPROVEMENT & INNOVATION
1. Define components of an integrated system of care, i.e., one that integrates
behavioral health and primary care and includes the full continuum of care.
What examples of integration currently exist in your region? What models
may work in your region, given your demographics, resources, and needs?
What are next steps to be taken to implement integrated models of care?
2. What behavioral and medical services are available in your region? What
services are not available in your region? In terms of priorities, what services
are urgently needed? What services should be built or developed in the next
few years?
3. What crisis behavioral health services are needed? What crisis services are
available?
4. What transportation is available in your region, for what patients? What is
needed?
B. TECHNOLOGY
1. What is the penetration of electronic medical record, by agency type and
geographic area? What is needed to bring all providers into the electronic
system?
2.Telemedicine and telepsychiatry. Are you using this technology? Would you
like to use it? What do you need to do to use it?
C. QUALITY OF CARE/BEST PRACTICES/EVIDENCE-BASED &
EVIDENCE-INFORMED PRACTICES
1. What EB/best practices are you currently using, for what services or consumer
groups?
2. What EB/ best practices do you plan to implement?
3. What resources would assist you in implementing EBPs?
4. What efforts are you making to ensure and improve quality of care?

21
D. PAYMENT ISSUES
1. What payment policies, models and incentives are necessary to improve
access to the most appropriate levels of care for the patient/consumer’s
condition?
2. What payment incentives and/or models are necessary to support integrated
models of care?
3. What services should be available to a consumer/patient that is not reimbursed
at all or adequately?
E. WORKFORCE 1. What mental health, substance abuse, and healthcare professionals are in short
supplies in your region?
2. What are the training and educational needs of your existing workforce?
3. Are you currently cross training behavioral and other medical professionals?
If so, what tools are you using? What resources do you need to accomplish
this integration?
4. What resources do you need to expand workforce in your region?
IV. SMALL GROUP REPORTS ............................11:30 ............... Group Facilitators
V. SETTING PRIORITIES & NEXT STEPS ....12:15 ........................... Mr. Steiner
VI. ADJOURNMENT & NEXT MEETING ........1:00 ............................. Ms. Clarke
Next Meeting: August 22, 2012
Center for Children’s Services - Danville, IL

22
Illinois Behavioral Health Network Meeting – Region 3
August 8, 2012
Bridgeway, Inc, Galesburg
Stephanie Barisch, The Center for Youth & Family Srvs
Karen Brauer, Mason District Hospital: Havana Medical
Jennifer Chiras, Children’s Home Association of IL
MaryLynn Clarke, Illinois Hospital Association
Vivian Coeur, Western IL University
Joe Croegaert, DHS/DMH
Laurelyn Cropek, Community Resource & Counseling Ctr, Inc.
Julie Darnell, Children’s Home Association of IL
Renee Donaldson, Advocate BroMenn Medical Center
Laura Domino, Hammond-Henry Hospital
Dennis Duke, Robert Young Center
Carol Evans, OSF Holy Family
Deb Fritz, Knox County Health Department
Carrie Hagen, OSF St. Mary’s Medical Center
Hillary Haggertt, Woodford County Health Department
Joan Hartman, Chestnut
Kimberly Hasselbach, OSF St. Mary’s Medical Center
Gail Koch, OSF Medical Group
Wayne Kubasak, McDonough District Hospital
Denise Jackson, Perry Memorial Hospital
Erin Laytham, Illinois Association of Rehab Facilities
Delinda Leopold, Perry Memorial Hospital
Marlin Livingston, Cunningham Children’s Home
Michelle Locke, Graham Hospital
Wendy Navarro, OSF St. Elizabeth
Bill Nelson, Bridgeway, Inc.
Rhonda Nelson, Bridgeway, Inc.
Fred Nirde, Human Service Center
Linda Parsons, Illinois Valley Community Hospital
Arlin Pinto, Human Service Center
Gretchen Robbins, Carle Foundation Hospital
Ernest C. Rose, Rose Medical Association, Inc.
Don Russell, New Directions
Melvia Russell, New Directions
Patricia Sampson, OSF St. Mary’s Medical Center
John Smith, Western IL University
Alice Snyder, OSF St. Mary’s Medical Center
Amber Sturgeon, Galesburg Cottage Hospital
Amy Tippey, Tazewell County Health Department
Tom Troe, DHS/DMH
Gary Weinstein, Transitions Mental Health Services
Robert Wesley, SIU School of Medicine
Melinda Whiteman, Eagle View Community Health Sys
I. Welcome & Summary of First Meeting
Bill Nelson, chief operating officer, Bridgeway, Inc., welcomed the group to Bridgeway,
at 10 a.m. He then turned the meeting over to Dean Steiner who provided a summary of
the first meeting and the agenda for the current meeting. Mr. Steiner reminded the group
that the goal of the meeting is to develop a plan to improve access to behavioral health
services in the region.
II. FOCUS ON PRIORITIES
Mr. Steiner asked the group to divide into small groups to discuss the following topics:
(1) Delivery system improvement and innovation; (2) technology; (3) Quality of
care/best practices/evidence-based and evidence-informed practices; (4) payment issues;
and (4) workforce.

23
III. Small Group Reports
Mr. Steiner asked a representative of each of the break-out groups to report on their
findings and recommendations. The information from the break-out groups is included in
the attached document.
IV. Setting Priorities & Next Steps
The recommendations collected at the meeting will be shared with participants before the
next planning meeting. Participants in the third meeting will develop the draft of their
regional plan.
V. Adjournment & Next Meeting
Mr. Steiner noted that the next meeting will be held August 22, at Center for Children’s
Services, in Danville, at 10:00 a.m. the meeting adjourned at 1:00 p.m.

24
August 8 Small Group Notes
Group #1
Facilitator: Alice Snyder
1. Increase Telemedicine – ABC
2. Funding – Streams – D
3. Physician extenders – A, D & E
4. Examine PCP training curriculum – E
5. Examine APN training curriculum – E
6. Licensing should be extended to younger range (↓15 years) for APNs – E
7. LCPC, CAADC (A, E) and LCSW
8. Incentivize Evidence Based Practices – C, D & E
9. Education – A & B
*Safe transport of violently psychotic patients
*AMT – Peoria – throughout state
*Expand emergency transport to younger patients. Need more services.
B. Technology
1. OSF – has EHR
2. Improve communication between referring and consulting practitioners
3. All electronic health records should connect w/HIE as it develops
4. Secure method of patient info electric transfer
C. Evidence Based
1. Wrap – Wellness Recovery Action Plans are EBPs
2. Telehealth
3. Employment Assistance programs
Q1 – Now in Region
a. Peoria - MHC and SA
Work with FQHC → soon two days/week
Psych accredited with FQHC
Hope to expand
b. FQHC work with another medical center – Rock Island
c. FQHC – Eagle view
Piecemeal with Bridgeway and others
Need a psychiatrist at least once a week
d. In Tennessee – Cherokee HCT System
MHC w/BH consultant
Incorporate Telehealth
Similar one in OR
e. Wyoming works with EDs (safe rooms)
f. A number of informal becoming formal relationships
g. Need for service Ls already forcing cooperation → need formal descriptions
h. Shopping for available services/modes of cooperation – should be formalized

25
i. Fee-for-service/private grd/now offer integrated services and have for some time
j. Private practice – Letters of Understanding for referrals – contract with reviewing
physicians
k. Chronic D/S patients have tough time getting into pays practices 0 OSF trying to provide
intermediate care to this population
Q2
*Psychiatric care for children is very difficult to acquire. This is true throughout much of the
state.
*Funding streak necessary
*Perhaps more training for PCPs
*Train MORS physician extender
Q3
a. SA is major issue in emergency situations → #1 issue
b. Detox is medical problem
Group #2
A. Delivery Systems/Models of Care
1. Education
2. Motivation/Costs
3. Access/response
4. Develop protocol
5. Strategies
B. Technology
1. Using Telehealth (efficient)
2. Electronic records linking with other providers
C. Evidence Based
1. Outcomes
2. Evidence/performance-based contracting
D. Payment Issues
1. Cost of Telehealth
2. Lack of psychiatry resources/cost
3. Lack of funding for prevention
E. Workforce
1. Psychiatry is limited
2. Acute children’s services are scarce

26
Group #3
A. Delivery Systems
1. Increased volume of BH in EDs brings need for increased inpatient beds
Local communities focus on collaboration and integration, care coordination
Development of workforce
Integration needs to include community services, police, transportation, basic
needs, and education
In-service/training of law enforcement
Support for caregivers
2. Availability to licensed BH professionals
3. Transportation needs increased.
Expand utilization of HAN network to include inpatient BH beds
Create handbook of services (update)
B. Technology
1. Developing EMR or HIE portal
BH behind in EMR
No consistency between chosen EMR
Need strong control over who has access to record and where it goes
2. Utilize available technology to increase services
Technology to provide “instant” access to patients
Bridgeway offers Telemedicine/Telepsych (cannot bill for it)
Incentives for Telepsych
C. Evidence Informed Practices
1. Health department is working with BH to assist with expectations/quality of care
2. Creating a “safe room” in ED with additional staff training
3. Training in mental health first aid
4. Using EBP in Employment Services
5. Using Health Matters
6. Proposal to develop “BH Homes”
D. Payment Issues
1. Observation care not paid beyond 48 hours
2. Re-admission not to be reimbursed
3. Medicaid limiting services – 1*
4. Timeliness of payments
5. Access to affordable meds – 1*
6. Dental care – 1*
7. No services access for unfunded population – 1*
*Top priority
E. Workforce
1. All Psychiatrist
Nurse Practitioners

27
Interventional strategies (training)
Financial resource to pay
Incentive exists to enter field but retention is problem
Recruitment and retention
Group 4
A. Delivery System
1. Integrated care (person centered) with ED diversion component (explore various
models/options
2. $/emphasis in school system and early intervention
3. Allowance of regional planning decision making – empower us to direct resources
– knowing what our regional needs are.
4. Merge affordable housing/transportation
Hard for hospital to get people back to community
Collaboration between in/outpatient settings
5. Post-discharge capability for clients – psych, meds, and counseling
B. Technology
1. Regional telecrisis, telepsychiatry) telemedicine access (e.g.., Iowa services being
provided by Chicago-based psychiatrists)
Assist with ED DC (reimbursement)
Assist hospitals with no psychiatrists to provide appropriate patient care
2. Financial incentive for paperless system, shared access
C. Evidence Based
1. Support funding at lower levels of care to keep people from inpatient, especially
for persons with substance use conditions
2. Need lots of training to support EBP
3. Lack of support for EBP from state. Where’s monitoring for quality? – no data
reporting required
4. Inpatient will be required to implement psychiatric core measures – need
quality/process improvement tracking
5. Expansion and support of WRAP
E. Workforce
1. More e-learning access
2. MH 1st aid curriculum – for front-line responder
3. Critical access hospital grants to trim
4. CIT training
5. Short of APNs and psychiatrists
6. Education of medical community (IHA can be an advocate here)
7. Residency program at Methodist
8. Collaboration of projects/integrated care with/I region for EB practice (best
practice)
28
Behavioral Health Regional Network Meetings – Region 3
August 22, 2012, 10:00 am – 12:30 pm
Center for Children’s Services
702 Logan Avenue, Danville, IL 61832
Agenda
I. WELCOME ........................................................10:00 ......................... Ed Michaels
II. SUMMARY OF SECOND MEETING ............10:05 ....................... Dean Steiner/
MaryLynn Clarke
III. REVIEW OF PLAN/PRIORITIES………… ..10:15.. ............ MaryLynn Clarke/
Jordan Litvak
IV. DISCUSSION .....................................................11:30 .............................. Everyone
V. NEXT STEPS ....................................................12:15 .............. MaryLynn Clarke/
Jordan Litvak
VI. ADJOURNMENT ..............................................12:30 ......................... Ed Michaels

29
Behavioral Health Regional Network Meetings – Region 3
August 22, 2012, 10:00 am – 12:30 pm
Minutes
Center for Children’s Services
702 Logan Avenue, Danville, IL 61832 I. WELCOME
Edward Michaels, Ph.D., president, The Center for Children’s Services, and host for the
meeting, welcomed everyone to the Region 3 planning meeting.
II. SUMMARY OF SECOND MEETING/REVIEW OF PLAN & PRIORITIES
MaryLynn Clarke, Illinois Hospital Association, asked the participants to review the Region
3 draft plan that had been provided to them and to indicate areas of agreement as well as
suggested revisions. During their discussion about the plan, they made the following
recommendations:
In addition to referencing the shortage of psychiatrists in the area, there are also shortages
of many licensed professionals. Community mental health centers experience difficulty
recruiting and retaining staff because they are not able to pay them as much as other
entities such as a hospital or school.
Telepsychiatry is being used in the region by North Central Mental health Center. They
use telepsychiatry in multiple sites, for psychosocial rehabilitation, intensive outpatient
therapy, Level I addiction services, and for group therapy (after obtaining a waiver for
such from the Division of Alcoholism and Substance abuse). To expand the use of
telepsychiatry in Illinois, Bob Wesley, SIU School of Medicine, recommended that
Illinois pass legislation that payers reimburse the physician the same for telemedicine as
for a face-to-face interaction. He also added that Medicaid payment is low and slow for
all services, including telemedicine. And, many insurers don’t pay for telemedicine.
Legislation is also needed to remove the requirement that a physician, in order to practice
using telemedicine, must both have admitting privileges at an Illinois hospital and be
licensed in Illinois. Every state, including Illinois, has different requirements for a
physician to use telemedicine. These are barriers to its use.
Children’s services are in short supply in Region 3. All outpatient services for kids have a
waiting list, some for up to six months. The only way to access services is through the
crisis SASS system. There is a lack of sub-acute services for kids such as partial hospital
or intensive outpatient services.
Integration between general medical and behavioral health presents opportunities to
improve access and outcomes for persons with mental illness. An example of a Region 3
integrated system of care is the Human Services Center in Peoria, which provides
behavioral health services in collaboration with a FQHC. The group endorsed as a model
to emulate the Human Services Center in Peoria. They offer 8 crisis beds that are open 24
hours a day, seven days a week that is staffed by a registered nurse, a recovery specialist
and other professionals. They also had housing that was funded by a federal grant that has
since expired. Other examples of integrated models of care included St. Mary’s Hospital
and Heritage community mental health center. Integration must be include care
management in order to work. It was observed that integrated care works best with
30
medical homes and mental health services work best with care managers. There is an
array of services in all communities that are not connected and this is a role for the
electronic medical record. Several noted that information goes to the primary care
physician but information seldom is directed to the behavioral health client.
The group recommended blended funding to support these models. The block grant permitted
providers to offer a full range of services and to use the block grant funding to support it. The
loss of grant funding has also reduced provider’s flexibility to develop comprehensive services.
Funding needs to be stable and predictable. A provider should be able to take all comers, not just
those who qualify for Medicaid. They recommended funding that provides a lump sum (e.g., a
grant) that can be used according to the unique needs of the particular community. The Mental
Health Block Grant should be changed in two ways: first, the application should include
integration of medical and mental health and substance abuse. Second, money should be
available for the non-Medicaid population.
Hospitals are caring for many persons with mental and substance use illnesses in crisis. One
recommendation to shore up their ability to meet these demands is for hospitals to have
agreements with each other. Another idea is to adults the Doc Assist phone consultation program
currently available for kids.
The group recommended the addition of early intervention and prevention to the continuum of
care. Examples include family education, suicide prevention in the schools, depression
screening. Some of these services can be provided by a primary care physician including
pediatricians. Funding limitations do not support these services for the non- Medicaid client,
unfortunately.
There are excellent evidence-based screening tools available that can be used in the primary care
setting. The ACES Study provides a predictive model for substance abuse or mental illness that
can be used in medical setting. The American Academy of Pediatricians has a tool kit that can be
sued and enhanced.
Substance abuse services in Region 3 are in crisis. There is an absence of many types or levels of
care: medical and medically managed or monitored detoxification, Level I and II outpatient
services, and residential services. There should be a capacity study done in the region to
determine what exists and what is needed. SBIRT may screen a person but there are not
programs to which to refer the individual.
Priorities for Region 3 include the following:
Education of first responders about mental health and suicide prevention;
Funding related to the patient/client’s need rather than their source of or eligibility
for funding;
This collaborative, region-based and –centric planning process should continue as
an on-going effort;
It should be coordinated with the other planning efforts underway, as well.
The meeting adjourned at 12:30 pm.

31
Appendix
Regional Integrated Behavioral Health Networks Act
Public Act 097-0381
An Act concerning health.
Be it enacted by the People of the State of Illinois, represented in the General Assembly:
Section 1. Short title.
This Act may be cited as the Regional Integrated Behavioral Health Networks Act.
Section 5. Legislative Findings.
The General Assembly recognizes that an estimated 25% of Illinoisans aged 18 years or older
have experienced a mental or substance use disorder, an estimated 700,000 Illinois adults aged
18 years or older have a serious mental illness and an estimated 240,000 Illinois children and
adolescents have a serious emotional disturbance. And on any given day, many go without
treatment because it is not available or accessible. Recent federal and State fiscal crises have
exacerbated an already deteriorating mental health and substance abuse (behavioral health)
treatment system that is characterized by fragmentation, geographic disparities, inadequate
funding, psychiatric and other mental health workforce shortages, lack of transportation, and
overuse of acute and emergency care by persons in crisis who are unable to obtain treatment
from less intensive community alternatives. The failure to treat mental and substance use
illnesses has human and financial consequences: human suffering and loss of function; increased
use of hospital emergency departments; increased use of all medical services; increased
unemployment, and lack of productivity; lack of meaningful engagement in family and
communities; school failure; homelessness; incarceration; and, in some instances, death. The
citizens of Illinois with mental and substance use illnesses need an organized and integrated
system of care that recognizes regional differences and is able to deliver the right care to the
right person at the right time.
Section 10. Purpose.
The purpose of this Act is to require the Department of Human Services to facilitate the creation
of Regional Integrated Behavioral Health Networks (hereinafter "Networks") for the purpose of
ensuring and improving access to appropriate mental health and substance abuse (hereinafter
"behavioral health") services throughout Illinois by providing a platform for the organization of
all relevant health, mental health, substance abuse, and other community entities, and by
providing a mechanism to use and channel financial and other resources efficiently and
effectively. Networks may be located in each of the Department of Human Services geographic
regions.
Section 15. Goals.
Goals shall include, but not be limited to, the following: enabling persons with mental and
substance use illnesses to access clinically appropriate, evidence-based services, regardless of
where they reside in the State and particularly in rural areas; improving access to mental health
and substance abuse services throughout Illinois, but especially in rural Illinois communities, by

32
fostering innovative financing and collaboration among a variety of health, behavioral health,
social service, and other community entities and by supporting the development of regional-
specific planning and strategies; facilitating the integration of behavioral health services with
primary and other medical services, advancing opportunities under federal health reform
initiatives; ensuring actual or technologically-assisted access to the entire continuum of
integrated care, including the provision of services in the areas of prevention, consumer or
patient assessment and diagnosis, psychiatric care, case coordination, crisis and emergency care,
acute inpatient and outpatient treatment in private hospitals and from other community providers,
support services, and community residential settings; identifying funding for persons who do not
have insurance and do not qualify for State and federal healthcare payment programs such as
Medicaid or Medicare; and improving access to transportation in rural areas.
Section 20. Steering Committee and Networks.
(a) To achieve these goals, the Department of Human Services shall convene a Regional
Integrated Behavioral Health Networks Steering Committee (hereinafter "Steering Committee")
comprised of State agencies involved in the provision, regulation, or financing of health, mental
health, substance abuse, rehabilitation, and other services. These include, but shall not be limited
to, the following agencies:
(1) The Department of Healthcare and Family Services.
(2) The Department of Human Services and its Divisions of Mental Illness and
Alcoholism and Substance Abuse Services.
(3) The Department of Public Health, including its Center for Rural Health.
The Steering Committee shall include a representative from each Network. The agencies of the
Steering Committee are directed to work collaboratively to provide consultation, advice, and
leadership to the Networks in facilitating communication within and across multiple agencies
and in removing regulatory barriers that may prevent Networks from accomplishing the goals.
The Steering Committee collectively or through one of its member Agencies shall also provide
technical assistance to the Networks.
(b) There also shall be convened Networks in each of the Department of Human Services'
regions comprised of representatives of community stakeholders represented in the Network,
including when available, but not limited to, relevant trade and professional associations
representing hospitals, community providers, public health care, hospice care, long term care,
law enforcement, emergency medical service, physicians trained in psychiatry; an organization
that advocates on behalf of federally qualified health centers, an organization that advocates on
behalf of persons suffering with mental illness and substance abuse disorders, an organization
that advocates on behalf of persons with disabilities, an organization that advocates on behalf of
persons who live in rural areas, an organization that advocates on behalf of persons who live in
medically underserved areas; and others designated by the Steering Committee or the Networks.
A member from each Network may choose a representative who may serve on the Steering
Committee.
Section 25. Development of Network Plans.
Each Network shall develop a plan for its respective region that addresses the following:

33
(a) Inventory of all mental health and substance abuse treatment services, primary health
care facilities and services, private hospitals, State-operated psychiatric hospitals, long
term care facilities, social services, transportation services, and any services available to
serve persons with mental and substance use illnesses.
(b) Identification of unmet community needs, including, but not limited to, the following:
(1) Waiting lists in community mental health and substance abuse services.
(2) Hospital emergency department use by persons with mental and substance use
illnesses, including volume, length of stay, and challenges associated with
obtaining psychiatric assessment.
(3) Difficulty obtaining admission to inpatient facilities, and reasons therefore.
(4) Availability of primary care providers in the community, including Federally
Qualified Health Centers and Rural Health Centers.
(5) Availability of psychiatrists and mental health professionals.
(6) Transportation issues.
(7) Other.
(c) Identification of opportunities to improve access to mental and substance abuse
services through the integration of specialty behavioral health services with primary care,
including, but not limited to, the following:
(1) Availability of Federally Qualified Health Centers in community with mental
health staff.
(2) Development of accountable care organizations or other primary care entities.
(3) Availability of acute care hospitals with specialized psychiatric capacity.
(4) Community providers with an interest in collaborating with acute care
providers.
(d) Development of a plan to address community needs, including a specific timeline for
implementation of specific objectives and establishment of evaluation measures. The
comprehensive plan should include the complete continuum of behavioral health
services, including, but not limited to, the following:
(1) Prevention.
(2) Client assessment and diagnosis.
(3) An array of outpatient behavioral health services.
(4) Case coordination.
(5) Crisis and emergency services.
(6) Treatment, including inpatient psychiatric services in public and private
hospitals.
(7) Long term care facilities.
(8) Community residential alternatives to institutional settings.
(9) Primary care services.
Section 30. Timeline.
The Network plans shall be prepared within 6 months of establishment of the Network. The
Steering Committee shall assist the Networks in the development of plans by providing technical
expertise and in facilitating funding support and opportunities for the development of services
identified under each of the plans.

34
Section 35. Report to Governor and General Assembly.
The Steering Committee shall report to the Governor and General Assembly the status of each
regional plan, including the recommendations of the Network Councils to accomplish their
goals and improve access to behavioral health services. The report shall also contain
performance measures, including changes to the behavioral health services capacity in the
region; any waiting lists for community services; volume and wait times in hospital emergency
departments for access to behavioral health services; development of primary care-behavioral
health partnerships or barriers to their formation; and funding challenges and opportunities. This
report shall be submitted on an annual basis.
Section 99. Effective date.
This Act takes effect January 1, 2012.
HB2982 Enrolled LRB097 10532 KTG 51304 b
Public Act 097-0381

35
Regional Behavioral Health Network – Region 3
Provider Questionnaire
1. Wait Times
Over the past year, has your facility experienced longer wait times for patients to
receive services due to transportation, available placements, etc? If so, what
primary factors contribute to the delays?
On a scale of 1-5 how big a problem are wait times for your facility? (1= very
important – 5 = not important at all) ______
Have you documented these delays?______ If so, what data do you have?
2. Security Concerns
Have you had to utilize security to maintain patients who are at your facility
waiting for a transfer? ______
On a scale of 1-5 how big a problem is security concerns related to delayed
transfers? (1 = very important, 5 = not important at all) ____ What data do you
have to document security issues? ______
If so, what data do you have?
3 Patient Volume
Have you seen an increase in the number of mentally ill and or substance abusing
patients being served at your facility in the past year?
On a scale of 1-5 how important is this issue to your facility?
What data do you have available to demonstrate these increases?
4. Transportation
Is transportation to appropriate care for unfunded patients a problem in your area?
On a scale of 1-5 how big a problem do you believe this is? ______
What data is available to document this problem?

36
5. Admissions
Over the past year have you had to admit more patients with mental illness or
substance abuse problems to non-behavior health units in your hospital because
you could not locate appropriate care elsewhere either inside or outside your
facility? _____
On a scale of 1-5 how big a problem do you believe this is? _______
What data do you have available to document this issue?
6. Please add any additional issues or trends experienced at your facility over the
past year and what data you have to document the issue.
7. Would you be interested in continuing to dialogue with other behavioral health
providers in your region through meetings, trainings, and workshops?
8. Would you be interested in working with other providers in the region on
common network issues such as transportation, regulatory barriers and other
system design issues? Please indicate which issues would be helpful to you.
9. Any other items (including data) you would like to share about this planning
process or materials that are related to this effort?
37
Region 3 Invitation List
A & L Counseling Services, P.C.
Accent Counseling, LLC
Action Consultants
Advocate BroMenn Medical Center
Advocate Eureka Hospital
Alcohol and Drug Education Clinic, Inc.
Alcohol and Drug Educational Services
Alcohol and Drug Professionals
Alcohol Chemical Evaluation Services,
DBA A.C.E.S., LTD
Alcohol Education and Intervention
Services, Inc.
Allied Counseling Resources, LTD
Association of Community Mental Health
Authorities
Association of Community MH Authorities
of IL
Aunt Martha's Youth Service Center, Inc. -
Vermillion Area Community Health Center
Aunt Martha's Youth Service Center, Inc. -
Great River Community Health Center
Aunt Martha's Youth Service Center, Inc. -
Iroquois Community Health Center
Bridgeway, Inc.
Bureau County Health Department
Carle Foundation Hospital
Carle Health Care Incorporated
Catholic Charities
Center for Alcohol and & Drug Services,
Inc.
Center for Children's Services
Center for Human Services
Central Counties Health Centers, Inc. -
Francis Nelson Health Center
Central Counties Health Centers, Inc. -
Urbana School Health Center
Champaign County Mental Health (708) and
DD (377) Boards
Champaign-Urbana Public Health District
Chestnut Health Systems
Children's Home Association of IL
Community Behavioral Healthcare
Association
Community Elements, Inc.
Community Elements/Mental Health Center
of Champaign, Co.
Community Health Care Inc., Christian
Family Care Center HomelessClinic
Community Health Care, East Moline Clinic
Community Health Care, Inc.
Community Health Care, Inc. - Rock Island
Clinic
Community Health Centers of Southeastern
Iowa, Inc. - KHS
Community Health Improvement Center
Community Health Partnership of Illinois
Community Health Care, Inc. Robert Young
Center
Community Resource & Counseling Ctr.,
Inc.
Community Workshop and Training Center
Countermeasures, Inc.
Crosspoint Human Services
Cunningham Children's Home, Inc.
Custom Counseling Services
DHS/DMH
DUI Assessments & Services
DUI Services
Eagle View Community Health System
East Central Illinois Humanistic, Inc.
Ford-Iroquois County Health Department
Frances Nelson Health Center
Fulton County Health Department
Fulton County Mental Health (708) Board
Gage & Associates, Inc.
Galesburg Cottage Hospital
Genesis Medical Center, Illini Campus
Gibson Area Hospital & Health Services
Good Shepherd Foundation of Henry
County, Inc.
Graham Hospital
Great River Community Health Center
GROW in Illinois
Hammond-Henry Hospital
Havana Medical Associates
Heartland Community Health Clinic - East
Bluff

38
Heartland Community Health Clinic -
Integrated Health Center
Heartland Community Health Clinic -
Carver Clinic
Heartland Community Health Clinic
Henderson County Health Department
Henry County Health Department
Hoopeston Regional Health Center
Hopedale Medical Complex
Human Service Center, Fayette Companies
Illinois Alcohol and Drug Evaluation
Services
Illinois Association of Rehab Facilities
Illinois Drop In-MLK Center-Homeless
Illinois Drug and Alcohol Counseling
Services, IDAACS, Inc
Illinois Hospital Association
Illinois United for Youth
Illinois Valley Community Hospital
Institute for Human Resources
Institute of Physical Medicine &
Rehabilitation
Iroquois Community Health Center
Iroquois Memorial Hospital & Resident
Home
Iroquois Mental Health Center
Jesus is the Way Prison Ministry
Joann C. Milani, PHD, PC
Kewanee Hospital
Kindred Hospital, Peoria
Knox County Health Department
LaSalle County Health Department
LaSalle County Mental Health (708) Board
LaSalle Outpatient
Livingston County Health Department
Livingston County Mental Health Board
Marshall County Health Department
Mason County Health Department
Mason District Hospital
McDonough County Health Department
McDonough District Hospital
McFarland Mental Health Center
McLean County Ctr. for Human Svcs., Inc.
McLean County Health Department
McLean County Mental Health (553) Board
and McLean County Board for the Care and
Treatment of Persons with a Developmental
Disability (377) Board
Mendota Community Hospital
Mercer County Health Department
Mercer County Hospital
Methodist Medical Center of Illinois
New Directions Counseling Center
Nexus, Inc.-Onarga Academy
North Central Behavioral Health Systems
Occupational Development Center
OSF Holy Family Medical Center
OSFMG Community Behavioral Health
Services
OSF Saint Francis Medical Center
OSF Saint James-John W. Albrecht Medical
Center
OSF St. Joseph Medical Center
OSF St. Mary Medical Center
OSF Saint Elizabeth Medical Center
P.A.T.S. Prevention and Treatment Services
Pekin Hospital
Peoria County Health Department
Perry Memorial Hospital
Prairie Center Health Systems
Proctor Hospital
Promise Healthcare
Provena Covenant Medical Center
Provena United Samaritans Medical Center
Psychological Services in the Quad Cities,
PC
Putnam County Helath Department c/o
Bureua County HD
RICCA
Richardson Counseling Center, LLC
River Bend Christian Counseling, Inc.
Rock Island County Health Department
Rock Island County Mental Health (708)
Board
Robert Young Center
Rose Medical Association, Inc.
Rosecrance Health Network
Siefert Counseling Center
South Side Office of Concern
Southern Illinois University, School of
Medicine
St. Margaret's Health

39
St. Mary's Hospital, Streator
Stark County Health Department
TAP Resources, Inc.
Tazewell County Health Department
Tazwood Mental Health Center
The Baby Fold
The Center for Youth and Family Solutions
The Consultants
The Pavilion
Transitions NFP
Tri-County Alcoholism and Drug Services,
LLC
Trinity Regional Health System
United In Jesus Outreach Ministries
Vermillion County Health Department
Vermillion County Mental Health 708
Board
Warren County Health Department
Western Illinois University/Beu Health
Center
Woodford County Health Department
Youth Service Bureau of Illinois Valley
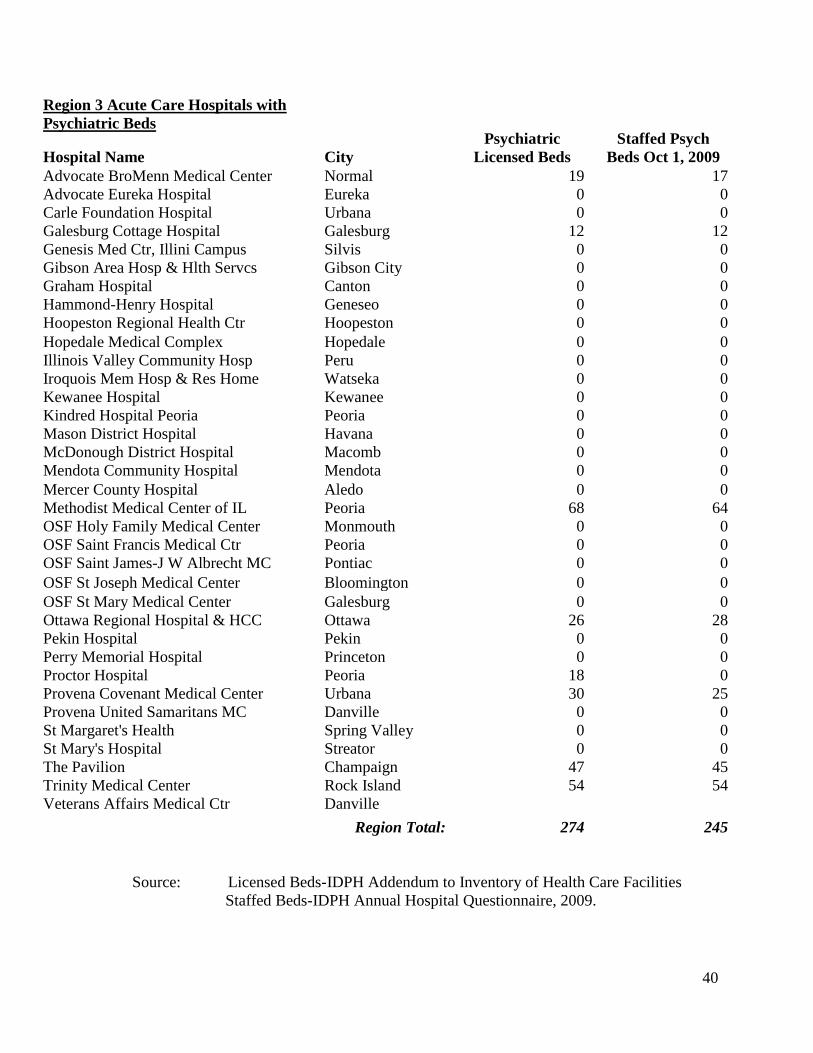
40
Region 3 Acute Care Hospitals with
Psychiatric Beds
Hospital Name
City
Psychiatric
Licensed Beds
Staffed Psych
Beds Oct 1, 2009
Advocate BroMenn Medical Center Normal 19 17
Advocate Eureka Hospital Eureka 0 0
Carle Foundation Hospital Urbana 0 0
Galesburg Cottage Hospital Galesburg 12 12
Genesis Med Ctr, Illini Campus Silvis 0 0
Gibson Area Hosp & Hlth Servcs Gibson City 0 0
Graham Hospital Canton 0 0
Hammond-Henry Hospital Geneseo 0 0
Hoopeston Regional Health Ctr Hoopeston 0 0
Hopedale Medical Complex Hopedale 0 0
Illinois Valley Community Hosp Peru 0 0
Iroquois Mem Hosp & Res Home Watseka 0 0
Kewanee Hospital Kewanee 0 0
Kindred Hospital Peoria Peoria 0 0
Mason District Hospital Havana 0 0
McDonough District Hospital Macomb 0 0
Mendota Community Hospital Mendota 0 0
Mercer County Hospital Aledo 0 0
Methodist Medical Center of IL Peoria 68 64
OSF Holy Family Medical Center Monmouth 0 0
OSF Saint Francis Medical Ctr Peoria 0 0
OSF Saint James-J W Albrecht MC Pontiac 0 0
OSF St Joseph Medical Center Bloomington 0 0
OSF St Mary Medical Center Galesburg 0 0
Ottawa Regional Hospital & HCC Ottawa 26 28
Pekin Hospital Pekin 0 0
Perry Memorial Hospital Princeton 0 0
Proctor Hospital Peoria 18 0
Provena Covenant Medical Center Urbana 30 25
Provena United Samaritans MC Danville 0 0
St Margaret's Health Spring Valley 0 0
St Mary's Hospital Streator 0 0
The Pavilion Champaign 47 45
Trinity Medical Center Rock Island 54 54
Veterans Affairs Medical Ctr Danville
Region Total: 274 245
Source: Licensed Beds-IDPH Addendum to Inventory of Health Care Facilities
Staffed Beds-IDPH Annual Hospital Questionnaire, 2009.

41
Inpatient Discharges Cumulative % Change
SFY
2005
SFY
2006
SFY
2007
SFY
2008
SFY
2009
SFY
2010
From SFY 2005 to SFY 2010
Statewide 1,723,215 1,714,661 1,724,116 1,715,750 1,677,926 1,651,967 -4.1%
Region 3 10,353 10,128 9,649 10,025 10,277 10,738 3.7%
Source: COMPdata

SOH Inpatient Inpatient Discharges
Peds
Adults
Total
REGION FACILITY
SFY
2007
SFY
2008
SFY
2009
SFY
2010
SFY
2007
SFY
2008
SFY
2009
SFY
2010
SFY
2007
SFY
2008
SFY
2009
SFY
2010
1C Madden MHC 0 0 0 0
4,242 4,151 3,654 3,674
4,242 4,151 3,654 3,674
1N Chic-Read MHC 0 0 0 0
1,913 1,788 1,848 1,829
1,913 1,788 1,848 1,829
1S Tinley Park MHC 0 0 0 0
1,721 1,473 1,784 1,823
1,721 1,473 1,784 1,823
Region 1 TOTAL 0 0 0 0
7,876 7,412 7,286 7,326
7,876 7,412 7,286 7,326
2 Elgin MHC 0 0 0 0 1,032 1,031 1,137 1,204 1,032 1,031 1,137 1,204
Singer MH/Dev Ctr 0 0 0 0 728 706 852 850 728 706 852 850
Treatment & Deten 0 0 0 0 4 9 9 6 4 9 9 6
Region 2 TOTAL 0 0 0 0
1,764 1,746 1,998 2,060
1,764 1,746 1,998 2,060
4 McFarland MHC 22 13 13 16
696 728 623 717
718 741 636 733
Region 4 TOTAL 22 13 13 16
696 728 623 717
718 741 636 733
5 Alton MH/Dev Ctr 0 0 0 0 197 198 191 188 197 198 191 188
Chester MHC 0 0 0 0 107 119 150 115 107 119 150 115
Choate MH and
Dev 78 84 60 65 460 400 364 233 538 484 424 298
Region 5 TOTAL 78 84 60 65 764 717 705 536 842 801 765 601
TOTAL
100 97 73 81
11,100 10,603 10,612 10,639
11,200 10,700 10,685 10,720
No State Operated Inpatient Facilities in Region 3.
Mental Health and Substance Abuse Cases.
Source: Illinois Department of Human Services
Illinois Statistics
Office of Mental Health and Development Disabilities

43
*The Illinois Health Facilities Planning Board discontinued licensing substance abuse beds as a category of service on April 17, 2000. this
category was converted to medical/surgical beds.
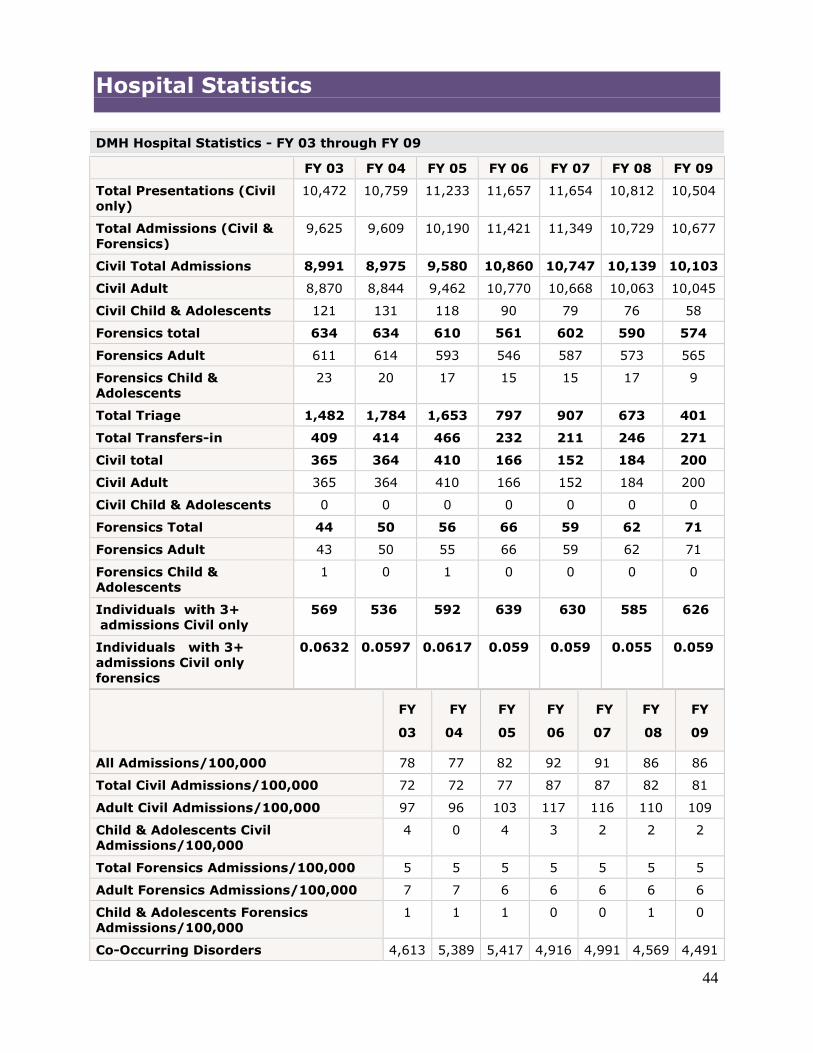
44
Hospital Statistics
DMH Hospital Statistics - FY 03 through FY 09
FY 03 FY 04 FY 05 FY 06 FY 07 FY 08 FY 09
Total Presentations (Civil
only)
10,472 10,759 11,233 11,657 11,654 10,812 10,504
Total Admissions (Civil &
Forensics)
9,625 9,609 10,190 11,421 11,349 10,729 10,677
Civil Total Admissions 8,991 8,975 9,580 10,860 10,747 10,139 10,103
Civil Adult 8,870 8,844 9,462 10,770 10,668 10,063 10,045
Civil Child & Adolescents 121 131 118 90 79 76 58
Forensics total 634 634 610 561 602 590 574
Forensics Adult 611 614 593 546 587 573 565
Forensics Child &
Adolescents
23 20 17 15 15 17 9
Total Triage 1,482 1,784 1,653 797 907 673 401
Total Transfers-in 409 414 466 232 211 246 271
Civil total 365 364 410 166 152 184 200
Civil Adult 365 364 410 166 152 184 200
Civil Child & Adolescents 0 0 0 0 0 0 0
Forensics Total 44 50 56 66 59 62 71
Forensics Adult 43 50 55 66 59 62 71
Forensics Child &
Adolescents
1 0 1 0 0 0 0
Individuals with 3+
admissions Civil only
569 536 592 639 630 585 626
Individuals with 3+
admissions Civil only
forensics
0.0632 0.0597 0.0617 0.059 0.059 0.055 0.059
FY
03
FY
04
FY
05
FY
06
FY
07
FY
08
FY
09
All Admissions/100,000 78 77 82 92 91 86 86
Total Civil Admissions/100,000 72 72 77 87 87 82 81
Adult Civil Admissions/100,000 97 96 103 117 116 110 109
Child & Adolescents Civil
Admissions/100,000
4 0 4 3 2 2 2
Total Forensics Admissions/100,000 5 5 5 5 5 5 5
Adult Forensics Admissions/100,000 7 7 6 6 6 6 6
Child & Adolescents Forensics Admissions/100,000
1 1 1 0 0 1 0
Co-Occurring Disorders 4,613 5,389 5,417 4,916 4,991 4,569 4,491
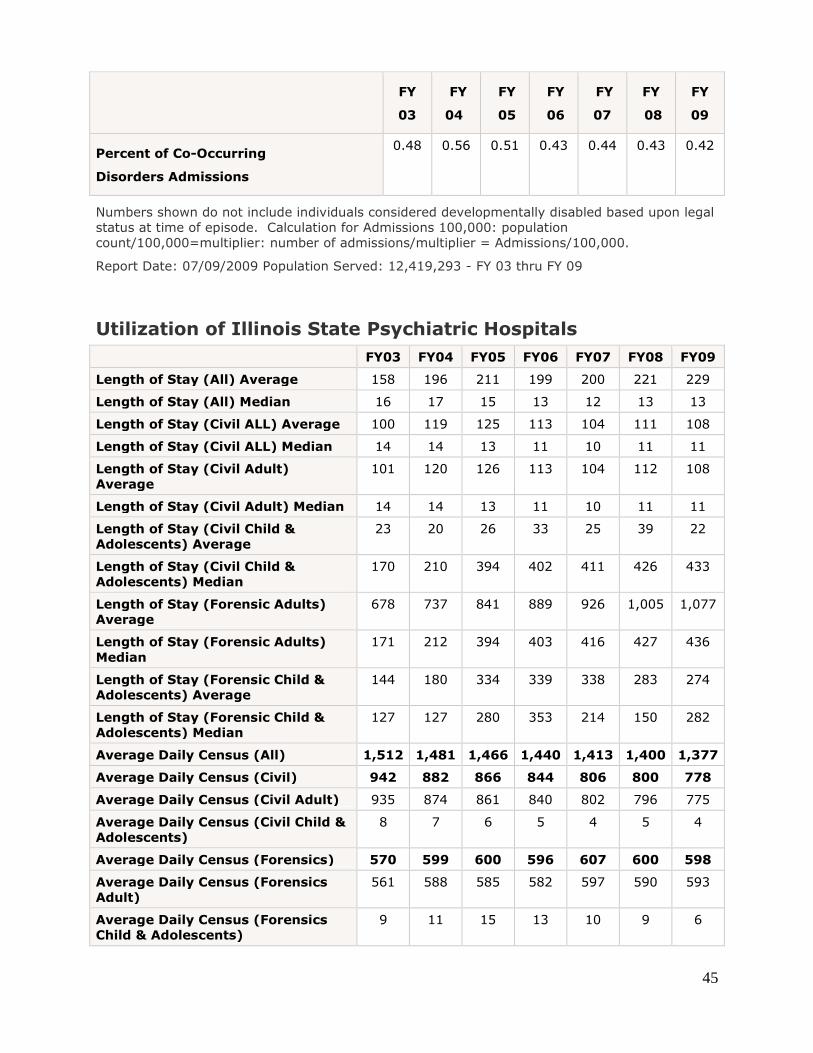
45
FY
03
FY
04
FY
05
FY
06
FY
07
FY
08
FY
09
Percent of Co-Occurring
Disorders Admissions
0.48 0.56 0.51 0.43 0.44 0.43 0.42
Numbers shown do not include individuals considered developmentally disabled based upon legal
status at time of episode. Calculation for Admissions 100,000: population
count/100,000=multiplier: number of admissions/multiplier = Admissions/100,000.
Report Date: 07/09/2009 Population Served: 12,419,293 - FY 03 thru FY 09
Utilization of Illinois State Psychiatric Hospitals
FY03 FY04 FY05 FY06 FY07 FY08 FY09
Length of Stay (All) Average 158 196 211 199 200 221 229
Length of Stay (All) Median 16 17 15 13 12 13 13
Length of Stay (Civil ALL) Average 100 119 125 113 104 111 108
Length of Stay (Civil ALL) Median 14 14 13 11 10 11 11
Length of Stay (Civil Adult)
Average
101 120 126 113 104 112 108
Length of Stay (Civil Adult) Median 14 14 13 11 10 11 11
Length of Stay (Civil Child &
Adolescents) Average
23 20 26 33 25 39 22
Length of Stay (Civil Child &
Adolescents) Median
170 210 394 402 411 426 433
Length of Stay (Forensic Adults)
Average
678 737 841 889 926 1,005 1,077
Length of Stay (Forensic Adults)
Median
171 212 394 403 416 427 436
Length of Stay (Forensic Child &
Adolescents) Average
144 180 334 339 338 283 274
Length of Stay (Forensic Child &
Adolescents) Median
127 127 280 353 214 150 282
Average Daily Census (All) 1,512 1,481 1,466 1,440 1,413 1,400 1,377
Average Daily Census (Civil) 942 882 866 844 806 800 778
Average Daily Census (Civil Adult) 935 874 861 840 802 796 775
Average Daily Census (Civil Child &
Adolescents)
8 7 6 5 4 5 4
Average Daily Census (Forensics) 570 599 600 596 607 600 598
Average Daily Census (Forensics
Adult)
561 588 585 582 597 590 593
Average Daily Census (Forensics
Child & Adolescents)
9 11 15 13 10 9 6

46
FY03 FY04 FY05 FY06 FY07 FY08 FY09
Total Number of Residents & Home
Visits on 7/09/09.
1,410 1,369 1,402 1,322 1,373 1,353 1,319
Total Number of Civil Residents and
Home Visits on 7/09/09.
799 760 791 706 762 742 709
Total Number of Civil Adult
Residents and Home Visits on
7/09/09.
797 757 786 705 757 742 707
Total Number of Civil Child &
Adolescents Residents and Home
Visits on 7/09/09.
2 3 5 1 5 0 2
Total Number for Residential and
Home Visits on 7/09/09
611 609 611 616 611 611 610
Total Number for Adult Residential
and Home Visits on 7/09/09
601 593 595 601 603 601 605
Total Number for Child
& Adolescents Residential and
Home Visits on 7/09/09
10 16 16 15 8 10 5
Utilization of Illinois State Psychiatric Hospitals
FY 03 FY 04 FY 05 FY 06 FY 07 FY 08 FY 09
Total Separations 10,190 10,058 10,625 11,731 11,496 10,988 10,979
Total Discharges (Civil &
Forensics)
9,772 9,641 10,150 11,498 11,286 10,739 10,708
Civil Total Discharge 9,255 9,052 9,584 10,981 10,729 10,211 10,171
Civil Adult 9,122 8,922 9,468 10,888 10,654 10,131 10,115
Civil Child & Adolescents 133 130 116 93 75 80 56
Forensics Total 517 589 566 517 557 528 537
Forensic Adults 502 578 553 506 538 517 525
Forensic Child &
Adolescents
15 11 13 11 19 11 12
Total Transfers-Out (Civil
& Forensic)
418 417 475 233 210 249 271
Civil Total 368 359 408 161 138 173 200
Civil Adult 368 359 408 161 138 173 200
Civil Child & Adolescents 0 2 0 0 0 0 0
Forensics Total 50 58 67 72 72 76 71
Forensics Adult 49 58 65 72 72 76 71
Forensics Child &
Adolescents
1 0 2 0 0 0 0
Report date 07/09/2009 Population Served
12,419,293http://www.dhs.state.il.us/page.aspx?item=33869

1
Illinois Regional Integrated
Behavioral Health Networks
Region 4
Draft Report

2
Table of Contents Topics Page # Region 4 Plan
Background 3-4
Access 4-5
Funding 5-6
Technology 7-8
Quality Improvement 8
Workforce 8-9
Regulatory Barriers 10
Meetings
Letter of Invitation 11
Agenda Dec. 7 12
Minutes Dec. 7 13-14
Small Group Responses Dec. 7 15-18
Agenda Jan. 6 19
Minutes Jan. 6 20-21
Small Group Responses Jan. 6 22-28
Agenda Jan. 17 29
Minutes Jan. 17 30-31
Appendix
PA 97-0381 32-35
Questionnaire 36-40
Region 4 Contact List 41-58
Psychiatric & Licensed Staffed Beds 59
Statewide & Behavioral Health Primary
Diagnoses Discharges 60
State Operated Hospitals Inpatient Discharges 61-62
ILHFB Bed Totals 63
Hospital Statistics 64-66

3
Illinois Regional Behavioral Health Networks
For hospital, primary care, mental health, substance abuse and
other community-based providers
Region 4
Note: The content of this report does not reflect the opinion or position of the Illinois Hospital
Association.
Background
On August 15, 2011, Governor Pat Quinn signed House Bill 2982 as Public Act 97-0381, which
created the Regional Integrated Behavioral Health Networks Act. The act provides a platform to
establish Regional Integrated Behavioral Health Networks. Its purpose is to ensure and improve
access to appropriate mental health and substance abuse services throughout Illinois by:
organizing systematically all relevant health, mental health, substance abuse, and other
community resources among regional providers; developing a mechanism to use regional
resources efficiently and effectively; and serving as a catalyst for innovation and collaboration.
Under the Act, each Behavioral Health Regional Network shall develop a strategic plan for its
respective region that addresses the inventory of existing services, identifies community needs
and defines opportunities to improve access to care. The act contemplates a broad, cross-section
of the mental health, substance abuse, health, and social services community that will be
involved in the development and implementation of the plan. Collaboration among all of the
relevant community resources will be essential to accomplish the purposes of the act and to build
effective, coordinated and comprehensive systems of care.
In partnership with the Illinois Department of Human Services (DHS), Division of Mental Health
(DMH) and Division of Alcoholism and Substance Abuse (DASA), the Illinois Hospital
Association (IHA), and others, convened a group of behavioral health providers in the State’s
DHS Region 4 to begin to identify existing services in the region, strategies for improving the
behavioral health services delivery system, including timely and appropriate access to medical
and behavioral health services, and ways in which providers can begin working together to
improve access to services and patient outcomes.
This plan outlines the priorities and recommendations for DHS Region 4, articulated by
participating service providers in three Region 4 meetings. At the first meeting held at the
Mental Health Center of Central Illinois (MHCCI), Springfield, on December 7, 2011, providers
defined their vision for behavioral health care services and outlined priority issues and areas of
focus. In the second meeting at MHCCI on January 6, 2012, participants identified strategies to
improve priority areas of concern listed in this plan. In the third meeting held on January 17,
2012 at MHCCI, the group reviewed and provided input on the first draft of a regional plan and
provided additional feedback on data sources and trends they have experienced over the past 12
months.

4
This plan is a template that recognizes the shortcomings and inefficiencies of the present system,
but also embraces partnerships that promise better coordination of care, across primary medical
and behavioral care, using technology and research to improve outcomes. It is an interactive
process and one that will evolve with a changing health care and economic landscape and will
depend on the continued commitment of all stakeholders-state agencies, primary medical,
hospitals, and behavioral health providers. It builds on community strengths to achieve a system
of care that delivers the right care, at the right time, in the right place.
1. Access
First and foremost, providers were concerned about access to behavioral health services
for all residents of the region. Providers defined the continuum of care to include a
regional and community-based approach to prevention, assessment, coordinated care, and
the necessary follow-up and transition services needed for patients moving from acute
care to community-based services. Providers in this region would like to work with state
and local agencies to develop a regional and community-based collaborative to design the
continuum of care at the community and regional level. Providers indicated that access to
inpatient beds is a priority for this region.
Providers in this region indicated that there is a need to provide alternative services to
acute and crisis care currently being provided by hospital emergency departments.
Region 4 participants would like to explore alternative strategies to provide behavioral
health services in a more appropriate setting to stabilize patients in crisis, provide
counseling to keep patients out of crisis, assist patients with life challenges, and provide
outreach to patients to improve their quality of life through community resources,
employment, housing, etc. Notwithstanding the value of providing alternative services,
providers emphasized the need to maintain access to the full continuum of care, from
acute care to rehabilitative services. This concept of Urgent Care for Behavioral Health
centers would offer more wrap-around services for clients and their families in a more
cost effective manner.
Providers in this region also agreed that a more patient-centered, holistic approach to
health and wellness for patients is a priority. An integrated behavioral and physical
health care system would allow physicians and behavioral health providers to work
together to enhance patient outcomes. In Quincy, the Patient-Centered Medical Home
(PCMH) model is being piloted at the Southern Illinois University (SIU) School of
Medicine Family Practice Clinic where Licensed Clinical Social Workers (LCSW) are
co-located with primary care physicians. This PCMH model is currently being
introduced to federally qualified health centers, rural health clinics, and family practice
clinics around the country and has shown positive outcomes.
However, these models will need to connect with community mental health centers,
substance abuse treatment and prevention service providers, and other community-based
services through a care coordination program. A care coordination program will help

5
patients and their families navigate through health care as they move from assessment,
diagnosis, treatment, follow-up and pharmaceutical compliance.
Recommendations
Develop criteria for the development of alternative settings for behavioral health
services. Providers will need to maintain existing capacity while designing new
system of care.
Develop psychiatric crisis observation beds in hospitals.
Provide treatment in the least restrictive environment.
Expand access to behavioral health crisis teams with consulting physician when
needed.
Develop a regional planning committee to work with DHS as it explores changes to
the behavioral health system in Region 4.
Provide care coordination services for patients and their families who navigate
through the health care delivery system.
Utilize community-based mental health centers, substance abuse providers, home
health agencies and others, to track and monitor patients with chronic conditions to
keep them out of crisis (within federal law).
Facilitate coordination through electronic medical records, patient tracking
technology and compliance data.
Identify best practices for care coordination at the local level.
Develop linkage agreements to expand coverage of existing services.
2. Funding
There was a lot of conversation regarding future funding strategies for behavioral health
services. There was agreement that existing cuts to the behavioral health system have
resulted in a shift of payments away from community-based services towards more
expensive hospital and long-term care services. Providers would like cuts to mental
health and substance abuse providers restored, so that planning for a more efficient
system of care can be implemented. Long-term funding for behavioral health services
will need to focus on prevention, treatment and follow-up services, based upon patient
outcomes.
6
There was consensus among providers that funding needs to be flexible enough to follow
the patient through the health care delivery system. Providers would like to work with
DHS and statewide organizations to plan for the use of state, federal and commercial
insurer funds that better meet the needs of patients and their families. Over the past few
years, cuts to non-acute care providers have resulted in more acute care patients (or
patients presenting to acute care settings), which increases the cost of care. A serious
plan to provide community-based services will help reduce care costs and provide more
timely services for patients and their families. Funding alternatives are needed that
would allow more flexibility, utilizing funding for locally identified needs, addressing
gaps and developing services where needed most as determined by local stakeholders
Providers would like to work with DHS to identify areas of cost savings to the system,
including lower cost service centers, lower cost transportation options, etc. The cost of
transporting involuntary patients by car is one-third the cost of an ambulance. How do
we transition to a lower cost system using these types of examples?
There is also a recognition that multiple providers may need to collaborate to address
common needs. For example, multiple providers working together to develop training
webinars for providers, recruitment strategies to meet workforce shortages, or to set up
alternative funding and lower cost service options are of interest to this group.
Recommendations
Convene a group of providers to work with DHS to identify lower cost options for
service delivery in the region.
Create behavioral health collaboratives around common needs such as transportation,
alternative service models, etc., to pool resources and implement new models for
patient services.
Explore private and federal funding opportunities to pilot new alternative strategies to
support behavioral health services in the region (crisis centers, care coordinators,
etc.).
Providers need to receive timely payments for services.
Create credentialing opportunities that reflect scope of work for Licensed Clinical
Professional Counselors (LCPC).
Identify accreditation standards for all behavioral health providers.
Provide funding for current unfunded patients.

7
3. Technology
Region 4 providers would like the state to assist them in utilizing technology to improve
access to care and create efficiencies in the system. Providers would like to integrate
behavioral health services into the patient’s electronic medical records and have access to
the patient’s complete health record when caring for the patient. Creating an
authorization form for patients to allow their behavioral health provider to have access to
their electronic medical record will assist providers in assessing and treating the
behavioral health needs of their patients.
Providers would also like to better utilize technology to reduce duplication in the
behavioral health system. Patients receive numerous assessments as they move from the
community mental health center to the specialist office to the hospital and back to the
community mental health center. This process creates redundancy in the process, utilizes
resources that are unnecessary and delays access to care for the patient and their family.
Providers would like to utilize technology to record assessment information at the point
of entry and build the patient record as they move through the health care services.
Providers indicated that patient confidentiality rules and regulations need to be followed
throughout the process.
Providers would also like to work with the state and its partners to expand access to
psychiatrists and other specialty providers through telemedicine services, especially
telepsychiatry in the rural parts of the region. Telepsychiatry is currently working in
several communities to provide assessment, treatment, counseling, and follow-up
services. However, the cost can be prohibitive especially in rural community mental
health centers and substance abuse centers.
Recommendations
Continue to work with the Office of Health Information Technology and the state
Health Information Exchange (HIE) Advisory Committee to integrate behavioral
health data into the state’s HIE planning and implementation strategies.
Support behavioral health providers as they link to the state’s HIE, especially small,
non-profit organizations.
Standardize electronic forms and coding to create efficiencies in reporting standards.
Convene a network of providers to explore innovative strategies to reduce duplication
in assessments, patient forms, and provider reporting requirements through
technology programs and software. This duplication increases cost to the behavioral
health system and delays patient care.
Work with state, federal and private funders to identify resources to expand access to
telemedicine equipment, especially for rural providers in the region.

8
Link telemedicine equipment to new crisis stabilization centers to access specialty
services if needed.
Review existing billing practices to identify areas where standardized forms would
provide efficiency in the system.
4. Quality Improvement
The group discussed the need to improve data collection, analysis and utilization to
provide more effective and efficient services in the region. With an increasing need to
identify patient needs and deliver high-quality patient outcomes, providers need to
develop quality measures that assess patient outcomes as they move through the
continuum of behavioral health services. There is a real need to develop consistent
outcomes measures for patients regardless of where they enter the system of care.
Providers would like more information on evidence-based practices that improve patient
outcomes and best practice strategies to improve care.
Recommendations
Cross-train providers on key patient measures needed to assess patient outcomes
across the continuum of behavioral health care service providers.
Establish the patient outcomes that will be measured and reported and which
Healthcare Effectiveness Data and Information Set (HEDIS) measures should be used
across the continuum of care.
Develop core measures to be used by the behavioral health care stakeholders to
demonstrate inpatient and outpatient outcomes.
DHS and its state partners should host training sessions for behavioral health
providers to provide a consistent message on rules related to Emergency Medical
Treatment and Active Labor Act (EMTALA) and patient confidentiality.
Establish performance measures to be consistent between departments of DHS
(mental health and substance abuse).
5. Workforce
Region 4 providers recognized a need to develop the workforce that will provide care in
the existing and developing delivery system. There will be a need for new workers such
as care coordinators and patient navigators, information technology specialists, home
health services and family and patient educators. Staff from the different specialty care
providers will need to be cross-trained to understand the needs of patients as they move
9
from one type of behavioral health provider to another, especially for those with multiple
chronic conditions. Providers would like to establish a pipeline to create a consistent
supply of qualified workers for the industry in the future.
Providers continue to struggle with workforce shortages, especially in the rural parts of
the region. Utilizing higher education training programs, providers will work to identify
new members of the behavioral health workforce. Providers will need to utilize
telemedicine services to access specialty services in rural communities. Providers also
indicated that the industry must also prepare for retirements through succession planning.
The group agreed that new information and professional skills will be needed by those in
the future workforce to address patient care such as: growing quality measures, cross-
training across specialty services, interactions with law enforcement, primary care
integrations, electronic medical records, new billing and coding data, and ongoing
evidence-based practice training. Linkages with higher education will continue to be a
priority as these new members of the workforce are developed.
The group also discussed the need for providers to reach out to other community-based
organizations that link services for patients and families like housing and transportation
services.
Recommendations
Identify new skills needed by the workforce of the future and design payment systems
to fund those provider services (recovery service specialists, care coordinators, patient
navigators, etc.).
Identify workforce incentives for professional shortage areas to attract providers to
those regions.
Identify core competencies needed for all providers and develop consistent training
for providers.
Provide succession planning training and resources for providers.
Develop locally-based interdisciplinary training for providers.
Remove regulatory barriers that limit the existing workforce from transitioning to the
new system of behavioral health services.
Work with higher education to recruit and train new behavioral health service
providers.
Expand the role of advance practice nurses (APN) in the behavioral health system.

10
6. Regulatory Barriers
This group identified several regulatory rules that prevent patients from receiving
comprehensive and timely services. The group is willing to work with DHS to update
these rules to meet the needs of the behavioral health system moving forward. There
needs to be a review and analysis of rules and regulations across behavioral health
services at both the state and federal levels.
Recommendations
Review Medicare rules that prevent multiple billing for a patient on the same day. It
prevents the coordinated and timely delivery of services for a patient.
The Rule 132 provides licensure inconsistencies that need to be addressed.
The group would like to work with DHS to address inconsistencies related to rules
132, 2090, and 150.
LCPCs should have same privileges and credentialing as LCSWs for billing purposes.

11
November 11, 2011
Name
Title
Organization
Address
City, State Zip
Dear:
As providers, we know that persons with mental and substance use illnesses in Illinois must navigate a
complex amalgam of services that are inconsistently available and accessible. Many seek care from us in
crisis because they could not obtain more timely or appropriate care. Our state and federal fiscal crises
have translated into the loss of essential behavioral health services particularly in rural Illinois. Yet,
despite these challenging circumstances, we can also identify opportunities to improve care. Some of
these opportunities stem from health reform; others are being generated by our own strategies to serve our
patients and communities. One such opportunity is being presented to us by the recent enactment of
House Bill 2982 – Public Act 97-0381, which creates the Regional Integrated Behavioral Health
Networks Act.
The bill establishes Regional Integrated Behavioral Health Networks to ensure and improve access to
appropriate mental health and substance abuse services throughout Illinois by systematically organizing
all relevant health, mental health, substance abuse, and other community resources among regional
providers, to develop a mechanism to use regional resources efficiently and effectively.
Under the Act, each Behavioral Health Regional Network shall develop a strategic plan for its respective
region that addresses the inventory of existing services, identifies community needs and defines
opportunities to improve access to care. The Act contemplates a broad-cross section of the mental health,
substance abuse, health, and social services community will be involved in the development –and
implementation—of the plan. Collaboration among all of the relevant community resources will be
essential to accomplish the purposes of the Act and to build effective, coordinated and comprehensive
systems of care.
We would like to invite you to participate in the first Behavioral Health Regional Network meeting for
DHS Region 4. The meeting will take place Wednesday, December 7 from 11:00 am – 2:00 pm at
Mental Health Centers of Central Illinois in Springfield, IL.
If you have any questions or concerns, please contact IHA Staff: Lori Williams, at 217-541-1164 or
[email protected] or MaryLynn M. Clarke at 217-541-1154 or [email protected].
To confirm your attendance, please contact Abby Radcliffe at 217-541-1178 or email your response to
Thank you,
MaryLynn McGuire Clarke
Sr. Director, Health Policy & Regulation
Lori Williams
V.P. Small & Rural Hospital Affairs

12
Illinois Behavioral Health Network Meeting – Region 4
December 7, 2011, 11:00 a.m. – 2:00 p.m.
MHCCI, 710 N. 8th Street, Springfield, IL 62702
Agenda
I. WELCOME & INTRODUCTIONS ................11:00 ....................... Jan Gambach
II. OVERVIEW OF HB 2982 (PA 97-0381) .........11:20..MaryLynn McGuire Clarke
III. REGIONAL PLAN DISCUSSION GROUPS..11:25 ................................. Groups
What should the behavioral health system look like three years from now?
What would be the key components of the new behavioral health system?
Are there immediate actions that could be taken to improve access to behavioral
health services in this region? If so, what are they?
IV. SMALL GROUP REPORTS ............................12:30 ....................... Lori Williams
V. SETTING PRIORITIES & NEXT STEPS ....1:15 ......................... Jan Gambach
VI. ADJOURNMENT & NEXT MEETING ........2:00 ......................... Jan Gambach

13
Illinois Behavioral Health Network Meeting – Region 4
December 7, 2011
MHCCI Conference Room, 710 N. 8th Street, Springfield, IL 62702
Lynette Ashmore, LifeLinks Mental Health
Jan Aten, Douglas County MHC
Cory Baxter, DeWitt County Human Res. Center
Jeff Bloemker, Heartland Human Services
Patty Bryant, Passavant Area Hospital
Candace Clevenger, Heritage Behav. Health, Inc.
Vickie Coen, Pana Community Hospital
David Cole, Moultrie County MHC
Debby Cook, LifeLinks Mental Health
Joe Croegaert, DMH
Dolan Dalpoas, Abraham Lincoln Mem. Hospital
Carol Davis, Douglas County MHC
Florine Dixon, Memorial Hospital, Carthage
Jan Gambach, MHCCI
Greg Hager, Pana Community Hospital
Randy Hodgson, Christian County MHA
Chuck Johnson, Blessing Hospital
Doug Kilberg, Locust Street Resource Center
Melissa G. Kulp, Jersey Community Hospital
Roger A. Larson, DeWitt County HRC
Darla Lawson, Sarah Bush Lincoln Health Cent.
Jordan Litvak, DHS
MaryLynn McGuire Clarke, Illinois Hospital Assoc.
Tom Miller, DMH
Sandra Mollahan, St. John’s Hospital
Bruce Morgan, Sarah Bush Lincoln Health Center
Rick Nance, DHS
Ken Polky, Human Resources Center of Edg. & Clark
Matt Obert, Chaddock
Abby Radcliffe, Illinois Hospital Association
Mike Rein, Transitions of Western Illinois
Schlabs, Megan, MHCCI
Susan Shafter, St. Mary’s Hospital, Decatur
Dr. Soltys, SIU School of Medicine
Katherine Suberlak, PCC Community Wellness Cent.
Lora Thomas, NAMI
Susan Weikart, Passavant Area Hospital
Bob Wesley, SIU School of Medicine
Lori Williams, Illinois Hospital Association
Katie Wilson, MHCWI
Orlinda (Speckhart) Workman, Passavant Area Hosp.
I. Welcome & Introductions
Jan Gambach called the meeting to order at 11:00 a.m. and those in attendance introduced
themselves. An overview was given of the current state of problems. Jan noted that the
group was not here to rehash the problems, but to find solutions.
II. Overview of HB 2982 (PA 97-0381)
MaryLynn McGuire Clarke gave an overview of the legislation which requires the
Department of Human Services (DHS) to create Regional Behavioral Health Networks in
each DHS region to ensure and improve access to behavioral health services. The
networks will work collaboratively to develop region-specific plans. The legislation also
created the Regional Integrated Behavioral Health Networks Steering Committee
comprised of state agencies to coordinate efforts among planning regions.
14
III. Regional Plan Discussion Groups
Participants were divided into groups to discuss three questions. 1) What should the
behavioral health system look like three years from now?; 2) What would be the key
components of the new behavioral health system?; and 3) Are there immediate actions
that could be taken to improve access to behavioral health services in this region? If so,
what are they?
IV. Small Group Reports
Lori Williams led the small groups to report on their findings. Information from the
break-out groups is included in the attached document.
V. Setting Priorities & Next Steps
Information collected at the meeting will be assembled by IHA. A focus on priorities and
developing specifics of the plan will be examined at the next meeting.
VI. Adjournment & Next Meeting
Jan noted that the next meeting will be held Jan. 6 at 11:00 a.m.

15
Region 4: Group Discussion Responses
December 7, 2011
What should the behavioral health system look like three years from now?
Adequate inpatient psych beds [no emergency department (ED) boarding]
Adequate substance abuse treatment at all /same levels
o Prevention, outpatient, residential, detox
Coordination, integration, and cooperation between behavioral and medical,
mental health and substance abuse, state agencies, hospitals and health
departments (responsive and flexible structure, better continuity of care)
Establishment of a structure to preserve (ongoing) regional
planning/collaboration/ integration/communication, i.e. build collaborative
planning into state infrastructure, but regional planning/organization must
accommodate local needs; allow national boundaries and relationships to flourish
Electronic health records:
o Adequate compatibility and integration
o Privacy Protections
o HIE and relevant health entities
Universal ‘language’ and formats
Serve those who are under and uninsured and improve access to underinsured
government-funded consumers/patients, and indigent care
Eliminate and reduce stigma
o Increase training across healthcare providers, treat whole person
o Cross-education of behavioral health and medical
Wellness focus and early interventions: recognize, pay, provide
Right care, right time, not in emergency room (ER)
Central data/communication link; access and communication, information sharing
technology, standards to share
Less paperwork, streamlined
Local community having more control, define community integration; community
setting
Adequate payment and cash flow, flexibility in payment system for specific
patient needs, predictable funding from state
Easy access to transportation
Education for providers and law enforcement
o Best practices/evidence-based practices
o Sharing, learning collaboratives
Still having consumer choice
Quality and data, evidence and metric to identify success

16
Urban territory barriers
Follow-up care (pharmacy)
Need assessment services, standardization, access to crisis services, and cross
training for assessments
Nutritional needs
Develop linkage agreements to expand coverage, share resources
Protocols for intake and placements and standardized safety plans
Central regional crisis center and return to community
Adequate workforce
o Psychiatrists to cover needs and for emergencies
o More APNs, mid-level providers
o LCPC same privilege/credential as LCSW – billing, reimbursement
o Funding for employment and psychiatrists and personnel
o Counselors
Telepsychiatry expanded; reimbursement model needed
Crisis stabilization services developed (save acute hospital beds)
Detox: inpatient and outpatient
Resolve regulatory barriers that impeded blended services, i.e., merge substance
abuse, mental health, developmental disabilities (Rule 132), legislation focused on
decreasing repetitious regulations, requirements, paperwork
Address confidentiality barriers across services
More comprehensive children services
Care coordination - - ONE person communication care/ decrease duplication
across services, streamlined services
HIE – care management alert system, universal release of information
Regional (inpatient and outpatient) providers replace individual county providers
o 708 law and ensure coverage for all areas
Medical home:
o Integration behavioral-physical
o Child- Pediatricians: first line of service
o (“no take back’s)
o Utilize federally qualified health centers
Three-legged stool: expand prevention to schools, corrections
Forensic patients competing with chronically mentally ill for money, resources:
o Can there be collaboration and develop system for Mental Health Court
Review group assignments; patient to appropriate services
o Decrease the “not mine” mentality

17
What would the key components of the new behavioral health system?
Resources to deflect ED
o Community services
o Alternative crisis, e.g. detox
ER
o BH resources available to ED
o Peer support/living room model and cross training
Substance Abuse services
o Detox
o Residential
Note: Decreased funding = unused substance abuse and psych beds
and closure of residential and detox programs (i.e. available, but no
staffing or revenue to support the programs)
Housing: Supported and Supervised
o Full continuum of housing and for uninsured and publicly funded
Preparing for changes, be creative
Telepsychiatry, telemedicine
Credible, patient centered focus of care
Better use of community volunteers
Adequate technology
o IT equipment, software and workforce
Data, outcomes and those to do it
Transportation services
Cross-training
Regional crisis beds, urgent care for behavioral health
Assessments: staff, standardized and streamlined
Psychiatrist: available for follow-up and medication management
Involvement/Integration with primary care, co-locate/hand-offs
EMR
o Regional/State HIEs
More Acute beds: better use, stabilize and long-term needs
Adequate workforce
o Psychiatrists to cover needs
o More APNs, mid-level providers
o LCPCs same privilege/credential as LCSWs – billing, reimbursement
Infrastructure to reduce need for state hospitals and hospital acute beds
Care coordination
Regional (inpatient and outpatient) providers replace individual county providers

18
Are there immediate actions that could be taken to improve access to behavioral health
services in this region? If so, what are they?
Effective Discharge Planning
Certified EHR plans (comp. pt.) with capacity to share with any provider
including community mental health centers and substance abuse agencies
Broadband expansion
Behavioral health training in the ED
Increased peer support
Increased staff
Bring more groups to the table, organizing community, work with health
departments
Services for underinsured, J-1 visa for underserved
More information of funding of transportation
Analyze needs of community: continuity and communication
Know what we do well, willing to give up those things we can’t do well
Sharing information about grants
Programs without walls
Tele-medicine
72 hrs. on a PNC-2nd
cert. has to be done by a psychiatrist
Assess utilization of existing crisis beds
Development of crisis bed services statewide, urgent care
Access issues: ED delays, safe discharge/timely
Regional plan for recruitment of providers:
o Therapists, psychologists, dentists, etc.
o Share resources
LCPC federal rules - - needs to be same privilege/credential as LCSW – billing,
reimbursement
APNs, expanding reimbursement coverage
Review rules; eliminate barriers
Mental Health Center, federal quality health centers access, workforce increase
Enhanced and timely reimbursement: remove barriers for authorization
Care Competency in behavioral health: organized effort, education and liaison

19
Illinois Behavioral Health Network Meeting – Region 4
January 6, 2012, 11:00 a.m. – 2:00 p.m.
MHCCI Conference Room, 710 N. 8th
Street, Springfield, IL 62702
Agenda
I. WELCOME ........................................................11:00 ....................... Jan Gambach
II. SUMMARY OF FIRST MEETING.................11:20 ..................... ..Jan Gambach
III. FOCUS ON PRIORITIES…………………….11:25 .................................. Groups
WORKFORCE:
What specific training is needed for existing workforce?
What are the new skills that are needed?
What are regulatory barriers to workforce utilization?
What are the specific training needs for dual diagnosis patients?
PREVENTION:
What are the current prevention services?
What new prevention services are needed?
DELIVERY SYSTEM:
How would you recommend we fill the gaps in the service delivery system?
Are there new models that would be effective in this region?
TRANSPORTATION:
Where are the transportation gaps (unfunded, Medicaid, others)?
What alternatives can you suggest in your community to provide
transportation?
PAYMENT DESIGN:
What services are not currently reimbursed that should be?
How should the payment system by redesigned to better meet the client’s needs?
IV. SMALL GROUP REPORTS ............................12:30 .............................. Everyone
V. SETTING PRIORITIES & NEXT STEPS ....1:15 ......................... Lori Williams
VI. ADJOURNMENT & NEXT MEETING ........2:00 ......................... Jan Gambach
January 17, 2011: 11:00 a.m.-2:00 p.m.
20
Illinois Behavioral Health Network Meeting – Region 4
January 6, 2012
MHCCI Conference Room, 710 N. 8th Street, Springfield, IL 62702
Lynette Ashmore, LifeLinks Mental Health
Jan Aten, Douglas Co. MH
Patty Bryant, Passavant Area Hospital
Bruce Carter, The Wells Center
Vickie Coen, Pana Community Hospital
David Cole, Moultrie Co. Mental Health Center
Joe Croegaert, DMH
Carol Davis, Douglas Co. Mental Health
Tom Frederick, Elm Center Rehab Center
Janice Gambach, MHCCI
Richard Gloede, Shelby Co. Com. Services
Greg Hager, Pana Community Hospital
Sherry Hendricksen, Kindred Hospital, Spring.
Mark Hilliard, Logan Co. Health Dept.
Randy Hodgson, Christian Co. MHA
Pamela Irwin, Central East Alc. & Drug Council
Chuck Johnson, Blessing Hospital
Rosemary Johnson, Apple Behav. Health Couns.
Doug Kilberg, Locust Street Resource Center
David King, Piatt County Mental Health
Diana Knaebe, Heritage Behavioral Health Inc.
Dietra Kulicke, Chestnut Health Systems, Inc.
Roger A. Larson, DeWitt Co. HRC
Kathy Lee, Memorial Health System
Jordan Litvak, DHS/DMH
Joe Lokaitis, DASA
Trisha Malott, SIU School of Medicine
Tom Miller, DMH
Sandy Mollahan, St. John’s Hospital
Tim Morenz, Macoupin Co. Public Health Dept.
Bruce Morgan, Sarah Bush Lincoln Health Center
Matt Obert, Chaddock
Daniel Perry, Apple Behavioral Health Counseling
Kenneth Polky, Human Res. Center of Ed. & Cl. Co.
Scott Porter, Piatt County Mental Health
Abby Radcliffe, Illinois Hospital Association
J. Michael Rein, Transitions of Western IL
Megan Schlabs, MHCCI
Earl Sheehy, Dr. John Warner Hospital
Randy Simmons, Paris Community Hospital
Kent Tarro, Macoupin Co. Public Health Dept.
Lora Thomas, NAMI
Nancy Weber, Sarah Bush Lincoln Health Center
Susan Weikert, Passavant Area Hospital
Bob Wesley, SIU
Lori Williams, Illinois Hospital Association
Katie Wilson, MHCWI
Orlinda (Speckhart) Workman, Passavant Area Hosp.
I. Welcome & Introductions
Jan Gambach called the meeting to order at 11:00 a.m. and those in attendance introduced
themselves.
II. Summary of First Meeting
Jan gave an overview of the last meeting. She thanked the group and the state for
participating in these meetings. The purpose of the group is to outline a plan for
behavioral health services in this region. The goal of the plan is to improve access to
behavioral health services in the region and work with the state steering committee to
implement changes to the system.
21
III. Focus on Priorities
Participants were divided into groups to discuss five topic areas. 1) Workforce; 2)
Prevention; 3) Delivery System; 4) Transportation; and 5) Payment Design. These
priority issues were identified in the first meeting. The questions on these topics will help
identify provider needs in each of the areas.
IV. Small Group Reports
The four small groups reported on their findings. Information from the break-out groups
is included in the attached document.
V. Setting Priorities & Next Steps
Information collected at the meeting will be assembled by IHA. A focus on a draft plan
will be discussed at the next meeting.
VI. Adjournment & Next Meeting
Jan noted that the next meeting will be held Jan. 17 at 11:00 a.m. She adjourned the
meeting at 2:00 p.m.

22
Jan. 6 Small Group Responses
Workforce:
Specific Training Needs: -
What are other states doing?
Effective use of bed utilization: core competencies – clinical, resource management
Education/Webinars, free; some existing trainings, but only few can participate, someone
to facilitate/maintain
Standardized approaches/ clinical trainings/ evidence based
Related to Rule 132
Compassion and process training
Regulation differences; different departments all regulated differently and pieced together
over 35 years
Recruitment: Need enough workforce
o RN’s in EDs
o LCSWs in community mental health centers – low $
o LCPC = LCSW / reimbursement equality
o Qualified Mental Health Professionals (QMHPs) – master’s level and experience
o Certified alcohol and drug counselors (addiction counselors)
o Training and finding new managers
Evidence based training/ algorithms
Concurrent charting
Document specialty skills in the new and existing system – by provider group, by
specialty
Cross-training to understand integration of roles and skill sets
o Integration training for behavioral health and primary health
o Cross-training on everything – technical and cultural
o Nurse case managers understanding physician process in telepsych (1-2 weeks)
Prevention and intervention strategies
ER, ICU, med/surg, etc.
Counselors need more information – pharmacy and med. aspects
More information for med. com. of referrals
Law enforcement, first responders, teachers
EMR
Training new staff and continuing education, expectations don’t fit reality for new grads
o University-based training: management, social work, etc., real world applications
New Skills
Looking at WHOLE person
Time management
Technology

23
Communication skills (oral and written)
o Specific writing skills
Skills to put together notes, etc., med necessity
o Professionals need to improve communication skills, conflict resolution
Psychiatrists
Understanding of existing resources
Education for funders and evaluators, to understand therapeutic documentation
Tough to find qualified workforce
o As resources tighten, good for employee to have consistent skills & training
(cookie cutter)
Joint commission – suicide assist for everyone who comes to hospital
Mental health centers and hospitals share staff and resources to manage patient loads
Need common language across industries: law enforcement, mental health centers, etc.
Issues surrounding integration
o Health care professionals need to learn to collaborate around industry needs
Need models of communities that have collaborative structures
o Physicians ignoring recommendation from mental health counselors
o Locally based interdisciplinary training
o Cross cultural integration of all specialties, cross-training, break down silos
o What are all the service needs – established initially, what are the resources
available that matches those up
Training needs to be practical, useful, directed
Peer support – unlicensed/certified: cost to obtain certification, issues related to ADA
Navigator. Unlicensed care coordination
Living room model – set up services outside of ED/hospital
Dual/Multiple diagnosis: developmental disabilities – substance abuse – mental illness –
physical health
Everyone to have a voice and be heard
Regulatory Barriers:
Parity among licenses
o LCPCs, APNs, licensed marriage and family therapist: Fed regulations bar them
from billing Medicare, APN prescription limits, and trainings not eligible to all
(barriers)
Recognizing specialties and utilizing them
Medicare won’t allow medical and psych visits on same day, force integration, but won’t
pay for it
Different behavioral health requirements

24
o Rules: 132 (vs.) 2060 (vs.) 150: are counterintuitive/disagree and prevent services
for those who need, inconsistent / inconsistent in interpretation, and substance
abuse and mental health rules don’t match up for integrated approach
o Rules are woven together, nationally too
o HIPAA
o Confidentiality
Dept. changes need to be passed through provider input
Redundant audits (reform), paperwork
Time spending w/ staff rules, etc.
Payers’ governing rules are competing too
Dual diagnosis training needs:
LCSW – doesn’t mean that person understands each specialty; generalist vs. specialist
Competency training on basic level of care in each area
Physicians training on behavioral health services and needs
Do away with dual diagnosis! Means different things, many definitions
Comprehensive health for the whole person and need patient-centered services
Need specialty services – can’t generalize every service and provider, especially
substance abuse
Specialists and cost balance: overall health outcomes vs. individualized care
Knowing what resources to link to, linkage, referral
Cross-training, case management, integration
Moving from acute to community w/ no follow-up (medical model/Medicaid)
o Recovery-oriented model, ongoing support – will reduce costs
Our service delivery system mirrors what we get funded: fragmented
funding=fragmented care
Continuum: Prevention – Care – Maintenance (NOT discharge)
Behavioral health-Medical (Diagnostic Statistic Manual (DSM) vs. International
Statistical Clarification of Diseases (ICD10))
o More exposure on medical side to behavioral health screening tools needed
o Consistency
o How to integrate will determine training needs
o Medical linkage assessment should include behavioral health assessments
o Payment mechanism must support “warm handoffs”
o Input from medical, need ‘same language’
Mental Illness-Developmental Disability: cultural barriers, billing, misdiagnosis frequent
so that services will be funded, “dumping” game, and placement
Behavioral health-substance abuse
o Workforce needed – behavioral health and substance abuse
High education requirements for low pay and high demand job
25
o Educate workforce: “Substance abuse is part of behavioral health” and “Not my
job” is not an option
o Regulatory issues/billing
o Engaging clients in care
Prevention
A. Current services:
Law enforcement programs (jail, probation)
Schools, training counselors: suicide, depression, high schools, youth groups, etc.
ER screening process, inpatient screening
Peer recovery support services
Employees
Biggest loser
Mental health training for parents
Funded in silos (DASA, 708 boards, Health departments, Federal): disconnect, no
funding for early intervention, competitive grants, mental health First Aid (no funding
received)
Money moving away from prevention to treatment: cuts related to outcomes, short term
funding shift is tough, however long-term prevention strategies will bend the cost curve
Money going to urban – larger services
Prevention Needs
Reimbursable services
Education to teachers and counselors and recommendations
Mental health Screenings in school, education to primary care, adding social workers
(Adams County)
Prevention in primary care, early intervention instead or as well, mental health
professional in office
Best practices guide: what programs work, where are best practices, need research-based
strategies related to prevention and interventions
Focused in-services
Reducing stigma, especially parents, family involvement
Regulatory reformation
Develop crisis services (response system), developmental disabilities beds closing
Define prevention process and outcomes (Population-based? Individual management?)
Smoking cessation
Health risk assessments (HRA)
Nutrition/dietary
Integrated models
Transportation, much could be ‘borrowed’ from hospitals
26
Delivery System
Recommendations to fill gaps in service delivery:
Gaps:
o Hospitals set up for psych in ED
o Set up crisis/stabilization unit: enough funding to meet client needs, personnel
o Supervised residential care – decreased funding: how many 24/7 beds needed?
o Front door – back door coordination: what should the system look like?
o Stigma – R/T mental illness, sexual/physical abuse, depression
o Population requirement to propose preventative services (prevention – schools –
parenting): what if we can’t meet the number?
o Prevention disconnected from treatment
o Get others “in the room” for behavioral health
“Glue” care coordination systems, case coordination – link client to services and also
need to broaden/increase to include: uninsured and fall-out population, integration
Tele-medicine/psych (cost, equipment, setup): reimbursement/Payment and service types,
and reimbursement not required by commercial payers
Transportation
Integration (between primary care & behavioral health – especially initial contact point),
breaking down silos between agencies
Thinking outside of the box, in the community, service access (some are going to
schools), co-location of services
Electronic integration/ EHR / HIE (medical health records)
Innovative ideas: recovery service specialist (recovering patients)
Keep safe, education for non-mental health
Basic services for all regardless of payer
New Models
Regions
Patient-centered medical homes
Transportation
Transportation Gaps:
Accessibility
Rural demographics: distance/miles to travel and no money to reach services
(transportation), un/under insured
MCD Funding: MCR offsets, but doesn’t cover
Funding for Case managers to transport
Education for clients
Public transport issues: not tolerating any behavioral health issues, no public transport,
and waiting times
27
Hospitals currently footing bill for transport back home after ambulanced in (could be
states away – even flights)
State transportation for involuntary admits –extend to voluntary
FY2012 – 1.6million by car; triples with ambulance
Telepsych maintenance
More crisis beds: centralized crisis center w/ telepsych, need to expand existing
Emergency vs. non-emergency transports: aging population in rural with increased
demands
Alternatives
Senior citizen volunteers
Able to use transportation that used to get them there (case managers)
New methodology
Local resources
Needs whole range of possibilities
DOT funding– behavioral health & medical
Payment design
Services not currently reimbursed that should be:
Reimbursement period – not being paid for services provided
Care coordination, Case management (true CM), wrap around services
Transportation
Prevention, early intervention
Community and patient education, community outreach
Psychiatry, Tele-psych
Inter-agency coordination
Limited case consultation
HIT/HIE/EHR: transition support and maintenance
Administrative/overhead
Non-Medicaid: allotted payment every month, take lessons from hospitals on Charity
Care
Medicaid – fee for services (antiquated): Go back to bundling, If stay w/ Fee for Service
(FFS), the fee must keep pace with market value/reimbursed cost (esp. Psych’s)
Tuition Reimbursement – continuing education
Accreditation, auditing, association fees
Closures: reinvest money saved into the continuum of care, at least a large percentage
Fund community-based services
May not see cost savings in first year
Accountable care organizations (ACOs) population dependent and costly to hub hospital

28
Transitional support, step-wise
Capacity grants/support
Services to get people a place to go
CHIPS – coverage for uninsured: no services for uninsured, need outpatient services
(outside of ED) to provide care for uninsured
Smoking cessation, Weight control programs
Populations: Veterans, Foster Care
Timely and consistent contracts
Recommendations on redesigning to better meet client needs
Restructuring of access to care
Reduce waste
All reasonable solutions considered, more ability to decide what is best for the patient
Regulatory requirements minimized, tort immunity
Local models of coordinated care
Grouping issues: behavioral health service is behavioral health
At-risk (via collaboration)
Billing systems standardized coding - including medical-behavioral health
More money for integration
Property tax concerns
Creating environment: What kind of model? medical necessity, etc.
Capacity/outcomes, grant
Decapitated
FFS vs. Block payment/grant: need payment flexibility to serve patients, productive use
of money, based on patient/population outcomes, incentivize outcomes, focus on
efficiencies, audits based on outcomes (substance abuse now)

29
Illinois Behavioral Health Network Meeting – Region 4
January 17, 2012, 11:00 a.m. – 2:00 p.m.
MHCCI Conference Room, 710 N. 8th
Street, Springfield, IL 62702
Agenda
I. WELCOME ........................................................11:00 ....................... Jan Gambach
II. SUMMARY OF SECOND MEETING ............11:20 ..................... ..Jan Gambach
III. REVIEW OF PLAN/PRIORITIES………… ..11:25 ....................... Lori Williams
IV. REGION INFORMATION...............................12:30 .............................. Everyone
V. NEXT STEPS ....................................................1:15 ......................... Lori Williams
VI. ADJOURNMENT ..............................................2:00 ......................... Jan Gambach

30
Illinois Behavioral Health Network Meeting – Region 4
January 17, 2012
MHCCI Conference Room
710 N. 8th Street, Springfield, IL 62702
Mike Bach, Macon County MH Board
Cory Baxter, DeWitt County HRC
Jeff Bloemker, Heartland Human Services
Patty Bryant, Passavant Area Hospital
Bruce Carter, The Wells Center
Don Cates, Cass County MHA
Vickie Coen, Pana Community Hospital
David Cole, Moultrie County MHC
Joe Croegaert, DMH
Barbara Dunn, Comm. Health Improv. Centers
Tom Frederick, Elm City Rehab Center
Jan Gambach, MHCCI
Richard Gloede, Shelby County Comm. Serv.
Craig Glover, Central Counties HC
Greg Hager, Pana Community Hospital
Randy Hodgson, Christian CMHA
Pamela Irwin, Central East Alcoh. & Drug
Chuck Johnson, Blessing Hospital
Doug Kilberg, Locust Street Resource Center
David King, Piatt County Mental Health
Diana Knaebe, Heritage Behavioral Health Inc.
Roger A. Larson, DeWitt County HRC
Kathy Lee, Memorial Health System
Paul LeVeque, Ascent Counseling & DUI
Jordan Litvak, DMH
Tom Miller, DMH
Sandy Mollahan, St. John’s Hospital
Tim Morenz, Macoupin County PHD
Rick Nance, DASA
Barbara Nelson, SIU School of Medicine
Roxie Oliver, MHCWI
Scott Porter, Piatt County Mental Health
Abby Radcliffe, Illinois Hospital Association
J. Michael Rein, Transitions of WI
Katie Sarnes, Mason District Hospital
Susan Shafter, St. Mary’s Hospital, Decatur
Lora Thomas, NAMI
Bob Wesley, SIU School of Medicine
Susan Weikert, Passavant Area Hospital
Lori Williams, Illinois Hospital Association
Katie Wilson, MHCWI
I. Welcome & Introductions
Jan called the meeting to order at 11:00 a.m. and those in attendance introduced
themselves.
II. Summary of Second Meeting
Jan gave an overview of the second meeting. She thanked the group and the state for
participating in these meetings. The purpose of these three meetings is to outline a plan
for behavioral health services in this region. The goal is to develop a plan to improve
access to behavioral health services in the region and work with a state steering
committee to implement changes to the system.
III. Review of Plan/Priorities
Lori Williams noted that today’s meeting will take the priority issues that were identified
in the first two meetings and begin to craft recommendations to be part of this region’s
plan. Comments will be recorded and added to the plan. Lori went through each section
of the draft plan and the group made recommendations for any changes.

31
IV. Region Information
Some region specific data was collected. This was included in the packets and any
feedback on additional data needed would be appreciated.
V. Next Steps
Information collected at the meeting will be assembled by IHA. The updated draft plan
will be sent to the group for any other changes. This plan will then be submitted to the
State Steering Committee when they begin to meet.
VI. Adjournment
Jan adjourned the meeting at 2:00 p.m.
32
Appendix
Regional Integrated Behavioral Health Networks Act
Public Act 097-0381
An Act concerning health.
Be it enacted by the People of the State of Illinois, represented in the General Assembly:
Section 1. Short title.
This Act may be cited as the Regional Integrated Behavioral Health Networks Act.
Section 5. Legislative Findings.
The General Assembly recognizes that an estimated 25% of Illinoisans aged 18 years or older
have experienced a mental or substance use disorder, an estimated 700,000 Illinois adults aged
18 years or older have a serious mental illness and an estimated 240,000 Illinois children and
adolescents have a serious emotional disturbance. And on any given day, many go without
treatment because it is not available or accessible. Recent federal and State fiscal crises have
exacerbated an already deteriorating mental health and substance abuse (behavioral health)
treatment system that is characterized by fragmentation, geographic disparities, inadequate
funding, psychiatric and other mental health workforce shortages, lack of transportation, and
overuse of acute and emergency care by persons in crisis who are unable to obtain treatment
from less intensive community alternatives. The failure to treat mental and substance use
illnesses has human and financial consequences: human suffering and loss of function; increased
use of hospital emergency departments; increased use of all medical services; increased
unemployment, and lack of productivity; lack of meaningful engagement in family and
communities; school failure; homelessness; incarceration; and, in some instances, death. The
citizens of Illinois with mental and substance use illnesses need an organized and integrated
system of care that recognizes regional differences and is able to deliver the right care to the
right person at the right time.
Section 10. Purpose.
The purpose of this Act is to require the Department of Human Services to facilitate the creation
of Regional Integrated Behavioral Health Networks (hereinafter "Networks") for the purpose of
ensuring and improving access to appropriate mental health and substance abuse (hereinafter
"behavioral health") services throughout Illinois by providing a platform for the organization of
all relevant health, mental health, substance abuse, and other community entities, and by
providing a mechanism to use and channel financial and other resources efficiently and
effectively. Networks may be located in each of the Department of Human Services geographic
regions.
Section 15. Goals.
Goals shall include, but not be limited to, the following: enabling persons with mental and
substance use illnesses to access clinically appropriate, evidence-based services, regardless of
where they reside in the State and particularly in rural areas; improving access to mental health
and substance abuse services throughout Illinois, but especially in rural Illinois communities, by
33
fostering innovative financing and collaboration among a variety of health, behavioral health,
social service, and other community entities and by supporting the development of regional-
specific planning and strategies; facilitating the integration of behavioral health services with
primary and other medical services, advancing opportunities under federal health reform
initiatives; ensuring actual or technologically-assisted access to the entire continuum of
integrated care, including the provision of services in the areas of prevention, consumer or
patient assessment and diagnosis, psychiatric care, case coordination, crisis and emergency care,
acute inpatient and outpatient treatment in private hospitals and from other community providers,
support services, and community residential settings; identifying funding for persons who do not
have insurance and do not qualify for State and federal healthcare payment programs such as
Medicaid or Medicare; and improving access to transportation in rural areas.
Section 20. Steering Committee and Networks.
(a) To achieve these goals, the Department of Human Services shall convene a Regional
Integrated Behavioral Health Networks Steering Committee (hereinafter "Steering Committee")
comprised of State agencies involved in the provision, regulation, or financing of health, mental
health, substance abuse, rehabilitation, and other services. These include, but shall not be limited
to, the following agencies:
(1) The Department of Healthcare and Family Services.
(2) The Department of Human Services and its Divisions of Mental Illness and
Alcoholism and Substance Abuse Services.
(3) The Department of Public Health, including its Center for Rural Health.
The Steering Committee shall include a representative from each Network. The agencies of the
Steering Committee are directed to work collaboratively to provide consultation, advice, and
leadership to the Networks in facilitating communication within and across multiple agencies
and in removing regulatory barriers that may prevent Networks from accomplishing the goals.
The Steering Committee collectively or through one of its member Agencies shall also provide
technical assistance to the Networks.
(b) There also shall be convened Networks in each of the Department of Human Services'
regions comprised of representatives of community stakeholders represented in the Network,
including when available, but not limited to, relevant trade and professional associations
representing hospitals, community providers, public health care, hospice care, long term care,
law enforcement, emergency medical service, physicians trained in psychiatry; an organization
that advocates on behalf of federally qualified health centers, an organization that advocates on
behalf of persons suffering with mental illness and substance abuse disorders, an organization
that advocates on behalf of persons with disabilities, an organization that advocates on behalf of
persons who live in rural areas, an organization that advocates on behalf of persons who live in
medically underserved areas; and others designated by the Steering Committee or the Networks.
A member from each Network may choose a representative who may serve on the Steering
Committee.
Section 25. Development of Network Plans.
Each Network shall develop a plan for its respective region that addresses the following:
34
(a) Inventory of all mental health and substance abuse treatment services, primary health
care facilities and services, private hospitals, State-operated psychiatric hospitals, long
term care facilities, social services, transportation services, and any services available to
serve persons with mental and substance use illnesses.
(b) Identification of unmet community needs, including, but not limited to, the following:
(1) Waiting lists in community mental health and substance abuse services.
(2) Hospital emergency department use by persons with mental and substance use
illnesses, including volume, length of stay, and challenges associated with
obtaining psychiatric assessment.
(3) Difficulty obtaining admission to inpatient facilities, and reasons therefore.
(4) Availability of primary care providers in the community, including Federally
Qualified Health Centers and Rural Health Centers.
(5) Availability of psychiatrists and mental health professionals.
(6) Transportation issues.
(7) Other.
(c) Identification of opportunities to improve access to mental and substance abuse
services through the integration of specialty behavioral health services with primary care,
including, but not limited to, the following:
(1) Availability of Federally Qualified Health Centers in community with mental
health staff.
(2) Development of accountable care organizations or other primary care entities.
(3) Availability of acute care hospitals with specialized psychiatric capacity.
(4) Community providers with an interest in collaborating with acute care
providers.
(d) Development of a plan to address community needs, including a specific timeline for
implementation of specific objectives and establishment of evaluation measures. The
comprehensive plan should include the complete continuum of behavioral health
services, including, but not limited to, the following:
(1) Prevention.
(2) Client assessment and diagnosis.
(3) An array of outpatient behavioral health services.
(4) Case coordination.
(5) Crisis and emergency services.
(6) Treatment, including inpatient psychiatric services in public and private
hospitals.
(7) Long term care facilities.
(8) Community residential alternatives to institutional settings.
(9) Primary care services.
Section 30. Timeline.
The Network plans shall be prepared within 6 months of establishment of the Network. The
Steering Committee shall assist the Networks in the development of plans by providing technical
expertise and in facilitating funding support and opportunities for the development of services
identified under each of the plans.

35
Section 35. Report to Governor and General Assembly.
The Steering Committee shall report to the Governor and General Assembly the status of each
regional plan, including the recommendations of the Network Councils to accomplish their
goals and improve access to behavioral health services. The report shall also contain
performance measures, including changes to the behavioral health services capacity in the
region; any waiting lists for community services; volume and wait times in hospital emergency
departments for access to behavioral health services; development of primary care-behavioral
health partnerships or barriers to their formation; and funding challenges and opportunities. This
report shall be submitted on an annual basis.
Section 99. Effective date.
This Act takes effect January 1, 2012.
HB2982 Enrolled LRB097 10532 KTG 51304 b
Public Act 097-0381

36
Regional Behavioral Health Network – Region 4
Provider Questionnaire (17 Completed)
1. Wait Times
Over the past year, has your facility experienced longer wait times for patients to
receive services due to transportation, available placements, etc.? If so, what
primary factors contribute to the delays?
Reductions in funding have increase delays in access to care
Bed availability, payer
Placement for behavioral health needs patient and IDPA
Concern with safety issues with inclement weather
On a scale of 1-5 how big a problem are wait times for your facility? (1= very
important – 5 = not important at all)
#5 - 3
#4 - 1
#3 - 3
#2 - 1
#1 - 7
Have you documented these delays?
NO - 5
YES - 5
N/A - 1
If so, what data do you have?
ED stats
Documentation, but no data collected
Wait/length of stays can be produced
Emergency department has a log, data has to be hand counted
Patient survey
Funding effects authorization
We are outpatient substance abuse/mental health no state funding so things
work a little different at our agency
Only anecdotal information
2. Security Concerns
Have you had to utilize security to maintain patients who are at your facility
waiting for a transfer?
NO - 7

37
YES - 9
We have increased security coverage within the past year to address the
issue
Use of local police
New electronic medical record may have report capabilities to drill down
to delay in transfers awaiting placements
On a scale of 1-5, how big a problem is security concerns related to delayed
transfers? (1 = very important, 5 = not important at all)
#5 - 2
#4 - 2
#3 - 1
#2 - 4
#1 - 4
What data do you have to document security issues?
Security staff maintain records
On charts of individual patients
Variance reporting system if issue escalates. Believe it is underreported
by ED staff
We don’t have security staff nor have we had that need
Environmental security committee
Elopement of patient
Number of times police have handcuffed violent people
3. Patient Volume
Have you seen an increase in the number of mentally ill and or substance abusing
patients being served at your facility in the past year?
Yes - 11
No - 2
Needs for services have steadily increased over the past three years while
resources have been decreased
On a scale of 1-5, how important is this issue to your facility? (1 = very
important, 5 = not important at all)
#5 - 1
#4 - 2
#3 - 2
#2 - 4
#1 - 6

38
What data do you have available to demonstrate these increases?
Internal census data, patient diagnosis
Client intakes and caseloads
Bed availability census
Report available through county mental health
SS department
Is monitored at least monthly for frequent visitors of substance abuse
Patient numbers tracked by number of visits to emergency
department/Month for years 2009, 2010, 2011
Volume data is tracked and admissions
Many of the local providers at capacity or not taking any more clients at
this time
4. Transportation
Is transportation to appropriate care for unfunded patients a problem in your area?
NO - 4
YES - 3
N/A - 1
On a scale of 1-5 how big a problem do you believe this is? (1 = very important, 5
= not important at all)
#5 - 1
#4 - 1
#3 - 3
#2 - 3
#1 - 4
What data is available to document this problem?
Costs are tallied internally, delay information
No rural transportation for those in crises
Was a significant problem in the past
Individual patient records, social service documents, case management
data
This is more of a problem for child and adolescent patients
Vehicle rider data
5. Admissions
Over the past year have you had to admit more patients with mental illness or
substance abuse problems to non-behavior health units in your hospital because

39
you could not locate appropriate care elsewhere either inside or outside your
facility?
YES - 6
NO - 5
N/A - 3
Even though we are not equipped to care for these patients
We do not admit to medical floors. If the patient has OD’d they go to ICU
Resourced limited and not appropriate
On a scale of 1-5 how big a problem do you believe this is? (1 = very important, 5
= not important at all)
#5 - 0
#4 - 1
#3 - 2
#2 - 0
#1 - 5
What data do you have available to document this issue?
Our social services department has data, psychiatric admissions, and
patient records
We rarely admit to hospital we mostly see community-based people
6. Please add any additional issues or trends experienced at your facility over the
past year and what data you have to document the issue.
Low income, non-Medicaid clients have no payment source for mental
health treatment. It has basically been eliminated, Increase in numbers of
uninsured, long waiting lists, knowledge of resources that are open or
closed
Acute bed availability, fewer community services, no access to facilities
Delay in getting patients transferred once admitted to inpatient and
difficulty placing developmentally disabled patients with several behavior
or medically mental illness patients such as adolescent pregnant patients in
wheelchairs on needing oxygen etc.
ED repeater log, audits
Drug seeking behavior in patients, wanting more medications but not
necessarily waiting for treatments
7. Would you be interested in continuing to dialogue with other behavioral health
providers in your region through meetings, trainings, and workshops?
YES-14
Maybe-
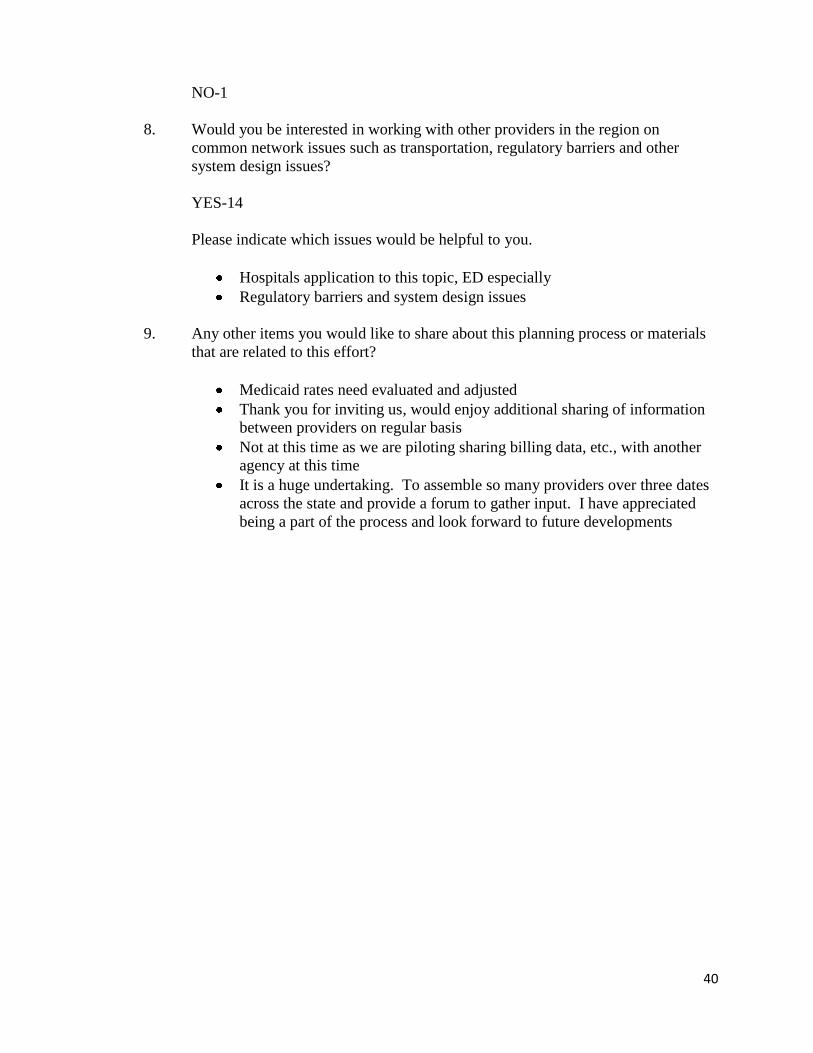
40
NO-1
8. Would you be interested in working with other providers in the region on
common network issues such as transportation, regulatory barriers and other
system design issues?
YES-14
Please indicate which issues would be helpful to you.
Hospitals application to this topic, ED especially
Regulatory barriers and system design issues
9. Any other items you would like to share about this planning process or materials
that are related to this effort?
Medicaid rates need evaluated and adjusted
Thank you for inviting us, would enjoy additional sharing of information
between providers on regular basis
Not at this time as we are piloting sharing billing data, etc., with another
agency at this time
It is a huge undertaking. To assemble so many providers over three dates
across the state and provide a forum to gather input. I have appreciated
being a part of the process and look forward to future developments
41
Region 4 Contact List
Organization Address 1 Addr
ess 2
City & State Zip Contact Email
A & E
Behavioral
Health
Associates
2570 E.
Federal
Drive
Decatur, IL 62526 Kenneth
Veon
Abbcon
Counseling
Corporation
603
Monroe St.
Charleston,
IL
61920 William A.
Epperson
Abraham
Lincoln
Memorial
Hospital
200
Stahlhut
Drive
Lincoln, IL 62656-
2698
Dolan
Dalpoas
Accurate
Evaluations
951 Fairfax
St.
Carlyle, IL 62231 Jessica
Daab
Adams County
Health
Department
330
Vermont
St.
Quincy, IL 62301 Executive
Director
Alcohol &
Addictions
Outpatient
Center
525 S.
Grand Ave.
W.
Springfield,
IL
62704 Ramona L.
Kennedy
ramonak@[email protected]
Apple
Behavioral
Health
Counseling, Inc.
8570 Saint
Lukes
Drive
Beardstown,
IL
62618 Daniel
Perry
Ascent
Counseling
408 S. Fifth
St. #1
Springfield,
IL
62701 Paul
LeVeque

42
Blessing
Hospital
Broadway
at 11th St.
P.O.
Box
7005
Quincy, IL 62305-
7005
Chuck
Johnson
Blessing
Hospital
Broadway
at 11th St.
P.O.
Box
7005
Quincy, IL 62305-
7005
Maureen
Kahn
Brown County
Health
Department
120 E.
Main St.
Mt. Sterling,
IL
62353
Bunker Hill
Health Center
144 N.
Washingto
n St.
Bunker Hill,
IL
62014
Calhoun County
Health
Department
210 French
St.
Hardin, IL 62047 Steve
Shireman
Carlinville Area
Hospital
20733 N.
Broad St.
Carlinville,
IL
62626-
1499
Kenneth
Reid
Cass County
Community
Health Clinic
331 S.
Main Street
Front
Virginia, IL 62691-
1571
Cass County
Health
Department
331 S.
Main St.
Virginia, IL 62691
Cass County
Health
Department
8590 St.
Lukes
Drive
Beardstown,
IL
62618
Cass County
Mental Health
Association
121 E.
Second St.
#1
Beardstown,
IL
62618 Don Cates [email protected]
CEC/Civigenics
Inc.
3300
Honeybend
Ave.
Litchfield, IL 62056 Steven
Bryant
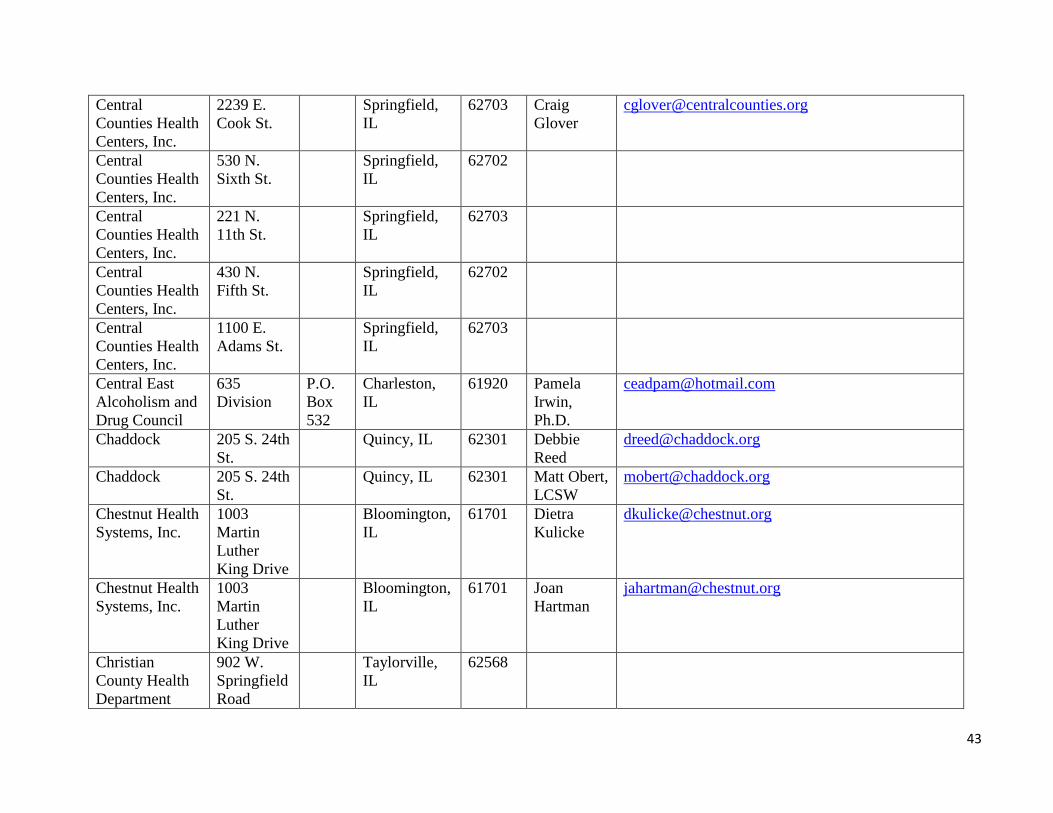
43
Central
Counties Health
Centers, Inc.
2239 E.
Cook St.
Springfield,
IL
62703 Craig
Glover
Central
Counties Health
Centers, Inc.
530 N.
Sixth St.
Springfield,
IL
62702
Central
Counties Health
Centers, Inc.
221 N.
11th St.
Springfield,
IL
62703
Central
Counties Health
Centers, Inc.
430 N.
Fifth St.
Springfield,
IL
62702
Central
Counties Health
Centers, Inc.
1100 E.
Adams St.
Springfield,
IL
62703
Central East
Alcoholism and
Drug Council
635
Division
P.O.
Box
532
Charleston,
IL
61920 Pamela
Irwin,
Ph.D.
Chaddock 205 S. 24th
St.
Quincy, IL 62301 Debbie
Reed
Chaddock 205 S. 24th
St.
Quincy, IL 62301 Matt Obert,
LCSW
Chestnut Health
Systems, Inc.
1003
Martin
Luther
King Drive
Bloomington,
IL
61701 Dietra
Kulicke
Chestnut Health
Systems, Inc.
1003
Martin
Luther
King Drive
Bloomington,
IL
61701 Joan
Hartman
Christian
County Health
Department
902 W.
Springfield
Road
Taylorville,
IL
62568
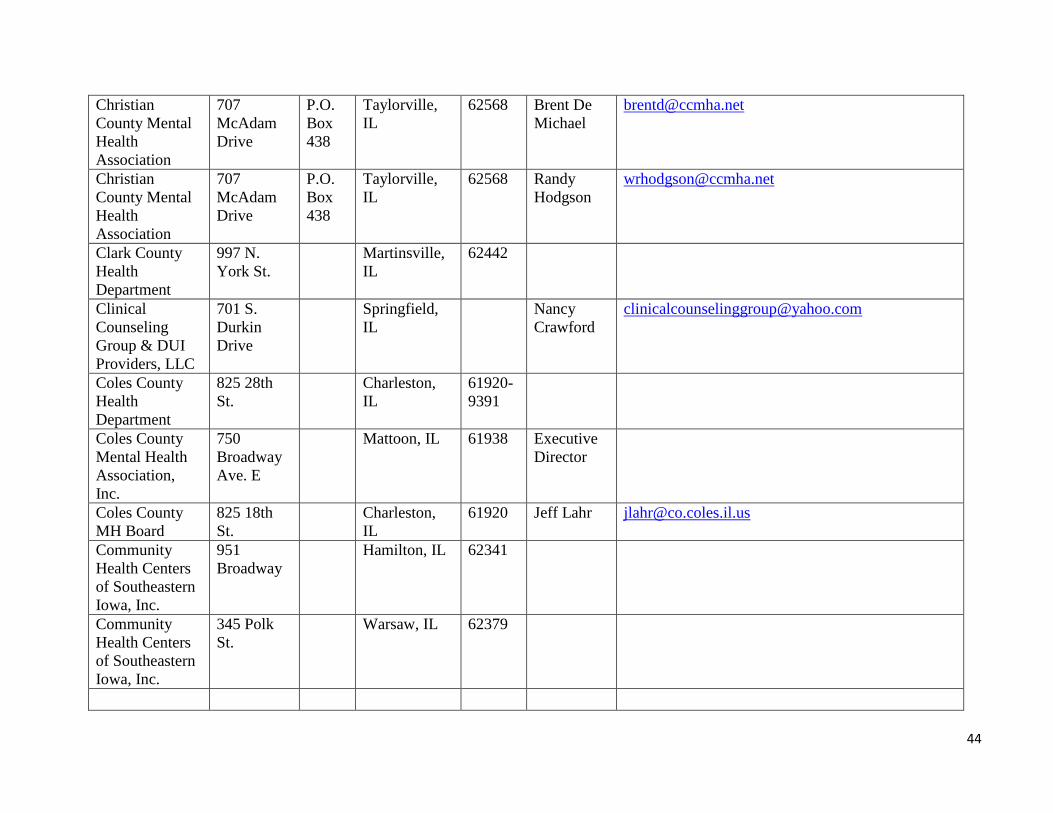
44
Christian
County Mental
Health
Association
707
McAdam
Drive
P.O.
Box
438
Taylorville,
IL
62568 Brent De
Michael
Christian
County Mental
Health
Association
707
McAdam
Drive
P.O.
Box
438
Taylorville,
IL
62568 Randy
Hodgson
Clark County
Health
Department
997 N.
York St.
Martinsville,
IL
62442
Clinical
Counseling
Group & DUI
Providers, LLC
701 S.
Durkin
Drive
Springfield,
IL
Nancy
Crawford
Coles County
Health
Department
825 28th
St.
Charleston,
IL
61920-
9391
Coles County
Mental Health
Association,
Inc.
750
Broadway
Ave. E
Mattoon, IL 61938 Executive
Director
Coles County
MH Board
825 18th
St.
Charleston,
IL
61920 Jeff Lahr [email protected]
Community
Health Centers
of Southeastern
Iowa, Inc.
951
Broadway
Hamilton, IL 62341
Community
Health Centers
of Southeastern
Iowa, Inc.
345 Polk
St.
Warsaw, IL 62379

45
Community
Health
Improvement
Centers
2905 N.
Main St.,
Ste. B
Decatur, IL 62526 Barbara
Dunn
Community
Health
Improvement
Centers
1221 E
Condit St.
Decatur, IL 62521
Community
Health
Improvement
Centers
1221 E.
Condit St.
Decatur, IL 62521
Community
Health
Improvement
Centers
243 W.
Cerro
Gordo
Decatur, IL 62522
Community
Memorial
Hospital
400
Caldwell
Staunton, IL 62088-
1423
Sue
Campbell
Continuing
Recovery
Center
202 W.
Central
Irving, IL 62051 Hugh
Satterlee
Cumberland
Associates, Inc.
120
Courthouse
Square
Toledo, IL 62468 Executive
Director
Cumberland
County Health
Department
132 NE
Courthouse
Square
Toledo, IL 62468
Decatur
Memorial
Hospital
2300 N.
Edward St.
Decatur, IL 62526-
4193
Kenneth
Smithmier

46
DeWitt County
Human
Resource Center
1150 State
Route 54
W.
Clinton, IL 61727 Roger A.
Larson
DeWitt County
Human
Resource Center
1150 State
Route 54
W.
Clinton, IL 61727 Cory
Baxter
DeWitt County
MH Board
121 W.
South St.
Clinton, IL 61727 Edith
Brady
Lunny
DeWitt-Piatt Bi-
County Health
Department
910 Route
54 E.
Clinton, IL 61727
Diel
Counseling, Inc.
444 S.
Willow
Effingham,
IL
62401 Patricia
Diel
Douglas County
Health
Department
1250 E.
U.S.
Highway
36
Tuscola, IL 61953
Douglas County
Mental Health
Center
114 W.
Houghton
Tuscola, IL 61953 Carol
Davis
Douglas County
Mental Health
Center
114 W.
Houghton
Tuscola, IL 61953 Jan Aten [email protected]
Dr. John
Warner Hospital
422 W.
White St.
Clinton, IL 61727-
2199
Earl
Sheehy
DUI Services 301 W.
North St.
Decatur, IL 62522 Joan Lewis [email protected]
DUI Solutions
& Treatment
Alternatives,
Inc.
408 S.
Fifth St.
Springfield,
IL
62701 Delores
Mast
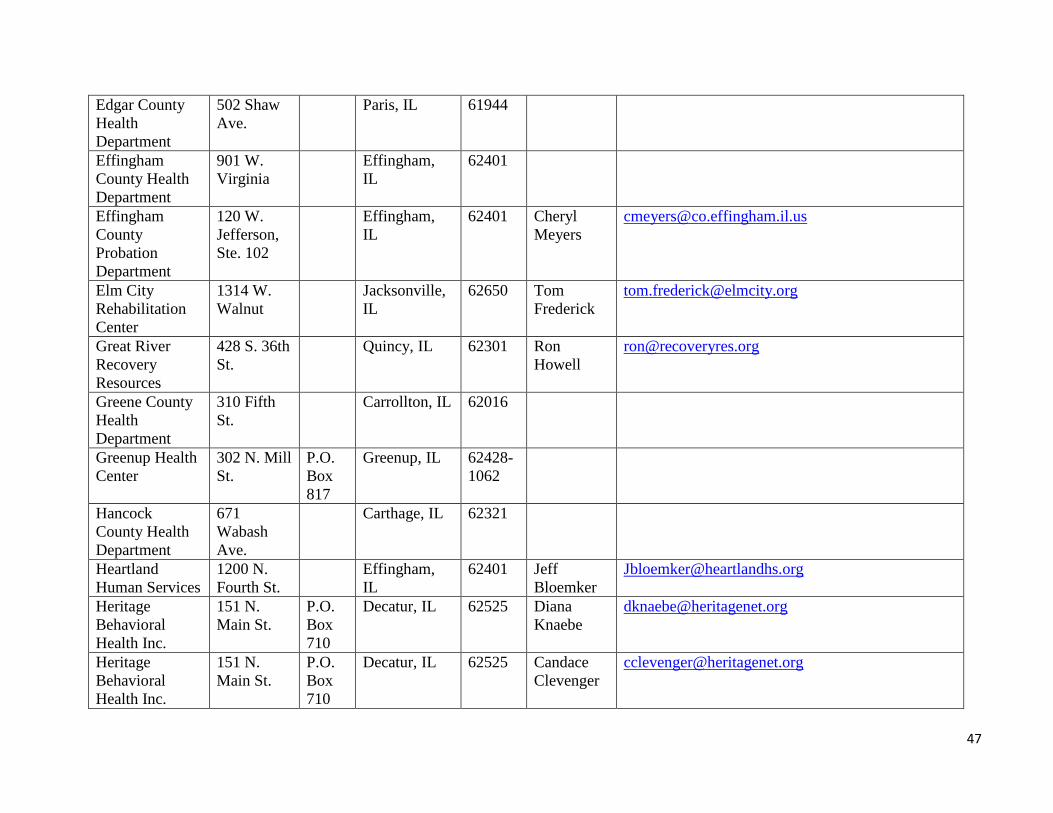
47
Edgar County
Health
Department
502 Shaw
Ave.
Paris, IL 61944
Effingham
County Health
Department
901 W.
Virginia
Effingham,
IL
62401
Effingham
County
Probation
Department
120 W.
Jefferson,
Ste. 102
Effingham,
IL
62401 Cheryl
Meyers
Elm City
Rehabilitation
Center
1314 W.
Walnut
Jacksonville,
IL
62650 Tom
Frederick
Great River
Recovery
Resources
428 S. 36th
St.
Quincy, IL 62301 Ron
Howell
Greene County
Health
Department
310 Fifth
St.
Carrollton, IL 62016
Greenup Health
Center
302 N. Mill
St.
P.O.
Box
817
Greenup, IL 62428-
1062
Hancock
County Health
Department
671
Wabash
Ave.
Carthage, IL 62321
Heartland
Human Services
1200 N.
Fourth St.
Effingham,
IL
62401 Jeff
Bloemker
Heritage
Behavioral
Health Inc.
151 N.
Main St.
P.O.
Box
710
Decatur, IL 62525 Diana
Knaebe
Heritage
Behavioral
Health Inc.
151 N.
Main St.
P.O.
Box
710
Decatur, IL 62525 Candace
Clevenger

48
Hillsboro Area
Hospital
1200 E.
Tremont
St.
Hillsboro, IL 62049-
1912
Rex Brown [email protected]
Hopewell
Clinical
314 N.
Sixth St.
Quincy, IL 62301 Trudy
Myers-
Widmer
Human
Resources
Center of Edgar
& Clark
Counties
118 E.
Court St.
Paris, IL 61944 Kenneth A.
Polky
Illini
Community
Hospital
640 W.
Washingto
n St.
Pittsfield, IL 62363-
1350
Kathy Hull [email protected]
Jersey
Community
Hospital
400 Maple
Summit
Road
P.O.
Box
426
Jerseyville,
IL
62052-
2028
Larry Bear [email protected]
Jersey
Community
Hospital
400 Maple
Summit
Road
P.O.
Box
426
Jerseyville,
IL
62052-
2028
Melissa G.
Kulp
Jersey
Community
Hospital
400 Maple
Summit
Road
P.O.
Box
426
Jerseyville,
IL
62052-
2028
Julie Smith [email protected]
Jersey County
Health
Department
1307 State
Hwy. 109
Jerseyville,
IL
62052
Kemmerer
Village
941 N.
2500 E.
Road
Assumption,
IL
62510 Mike
Havera
Kindred
Hospital,
Springfield
701 N.
Walnut St.
Springfield,
IL
62702 Sally
Hoffman

49
Kirby Medical
Center
1000
Medical
Center
Drive
Monticello,
IL
61856-
1116
Steven
Tenhouse
Liberty
Counseling
Center, Inc.
1429 S.
Main St.,
Ste. A
Jacksonville,
IL
62650 Sandra
Eyman
LifeLinks
Mental Health
750
Broadway
Avenue E.
Mattoon, IL 61938 Debby
Cook
LifeLinks
Mental Health
750
Broadway
Avenue E.
Mattoon, IL 61938 Lynette
Ashmore
Lifeway
Behavioral
Services, Inc.
200 E.
Main St.
Clinton, IL 61727 William
Melton
Lincoln Prairie
Behavioral
Health Center
5230 S.
Sixth St.
Springfield,
IL
62703 Mark
Littrell
Locust Street
Resource Center
320 S.
Locust St.
Carlinville,
IL
62626 Douglas
Kilberg
Logan County
Health
Department
109 Third
St.
Lincoln, IL 62656-
0508
Mark
Hilliard
Macon County
Health
Department
1221 E.
Condit
Street
Decatur, IL 62521-
1405
Julie A.
Aubert
Macon County
MH Board
132 S.
Water St.,
Ste. 604
Decatur, IL 62523 Dennis
Crowley
Macon County
MH Board
132 S.
Water. St.,
Ste. 604
Decatur, IL 62523 Mike Bach [email protected]
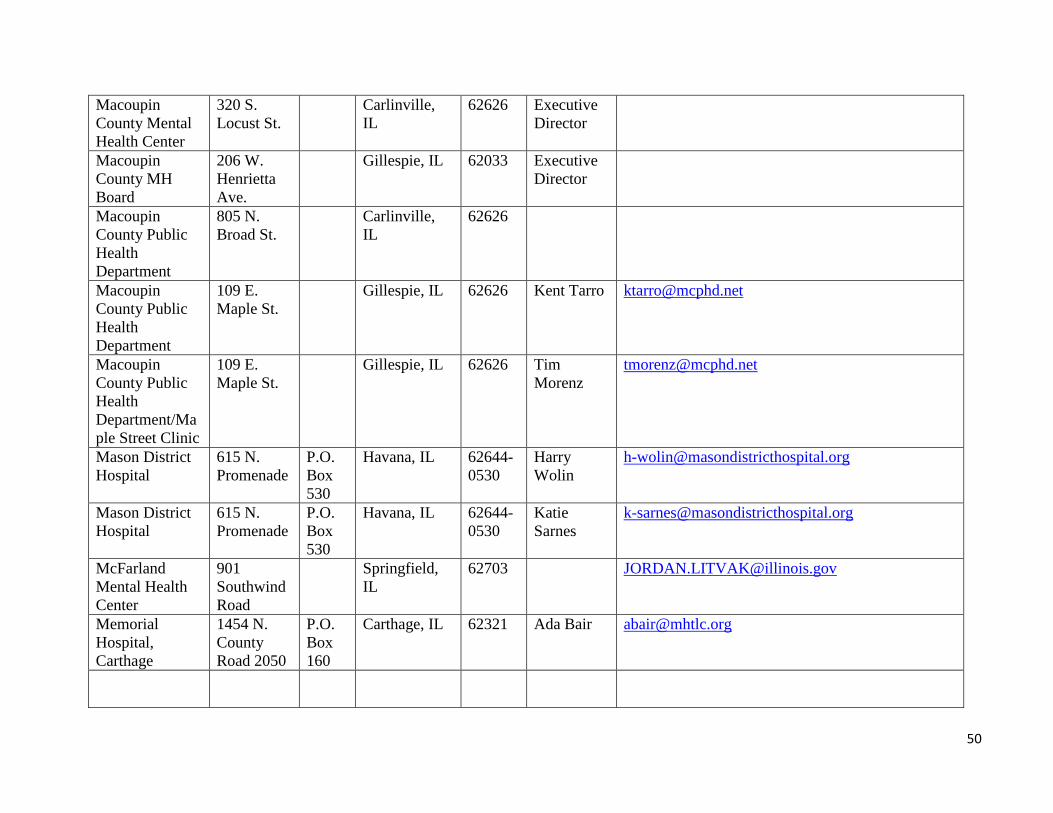
50
Macoupin
County Mental
Health Center
320 S.
Locust St.
Carlinville,
IL
62626 Executive
Director
Macoupin
County MH
Board
206 W.
Henrietta
Ave.
Gillespie, IL 62033 Executive
Director
Macoupin
County Public
Health
Department
805 N.
Broad St.
Carlinville,
IL
62626
Macoupin
County Public
Health
Department
109 E.
Maple St.
Gillespie, IL 62626 Kent Tarro [email protected]
Macoupin
County Public
Health
Department/Ma
ple Street Clinic
109 E.
Maple St.
Gillespie, IL 62626 Tim
Morenz
Mason District
Hospital
615 N.
Promenade
P.O.
Box
530
Havana, IL 62644-
0530
Harry
Wolin
Mason District
Hospital
615 N.
Promenade
P.O.
Box
530
Havana, IL 62644-
0530
Katie
Sarnes
McFarland
Mental Health
Center
901
Southwind
Road
Springfield,
IL
62703 [email protected]
Memorial
Hospital,
Carthage
1454 N.
County
Road 2050
P.O.
Box
160
Carthage, IL 62321 Ada Bair [email protected]
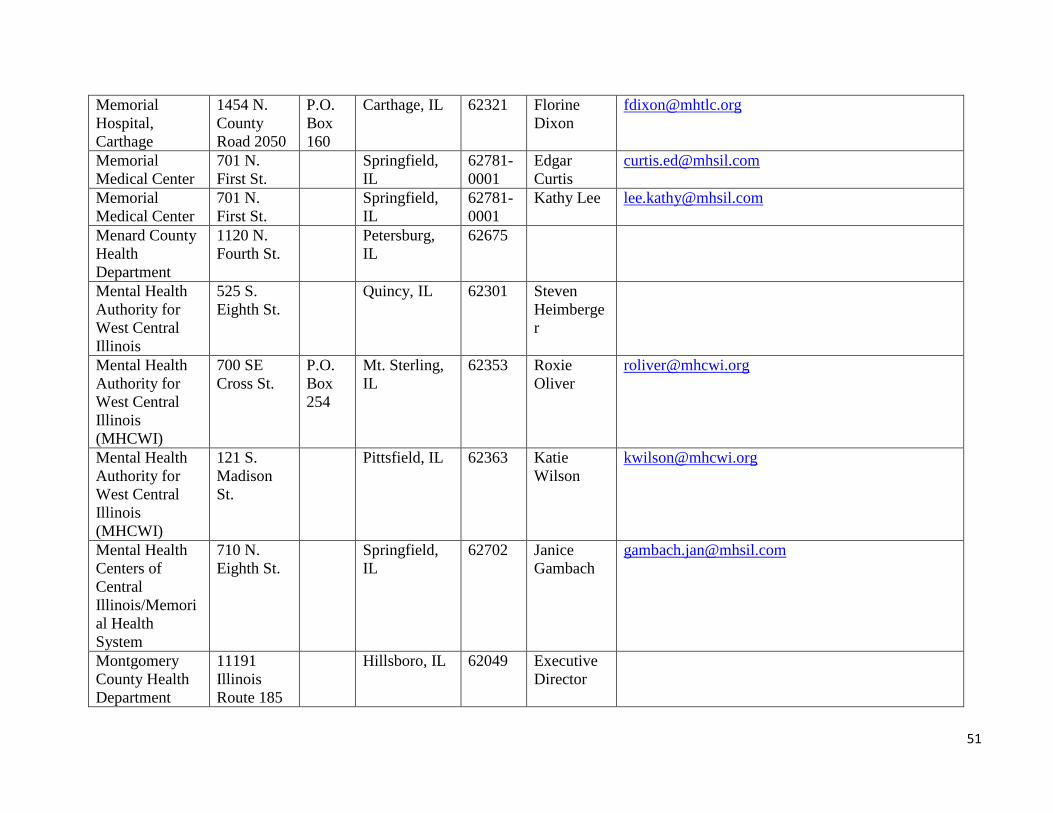
51
Memorial
Hospital,
Carthage
1454 N.
County
Road 2050
P.O.
Box
160
Carthage, IL 62321 Florine
Dixon
Memorial
Medical Center
701 N.
First St.
Springfield,
IL
62781-
0001
Edgar
Curtis
Memorial
Medical Center
701 N.
First St.
Springfield,
IL
62781-
0001
Kathy Lee [email protected]
Menard County
Health
Department
1120 N.
Fourth St.
Petersburg,
IL
62675
Mental Health
Authority for
West Central
Illinois
525 S.
Eighth St.
Quincy, IL 62301 Steven
Heimberge
r
Mental Health
Authority for
West Central
Illinois
(MHCWI)
700 SE
Cross St.
P.O.
Box
254
Mt. Sterling,
IL
62353 Roxie
Oliver
Mental Health
Authority for
West Central
Illinois
(MHCWI)
121 S.
Madison
St.
Pittsfield, IL 62363 Katie
Wilson
Mental Health
Centers of
Central
Illinois/Memori
al Health
System
710 N.
Eighth St.
Springfield,
IL
62702 Janice
Gambach
Montgomery
County Health
Department
11191
Illinois
Route 185
Hillsboro, IL 62049 Executive
Director
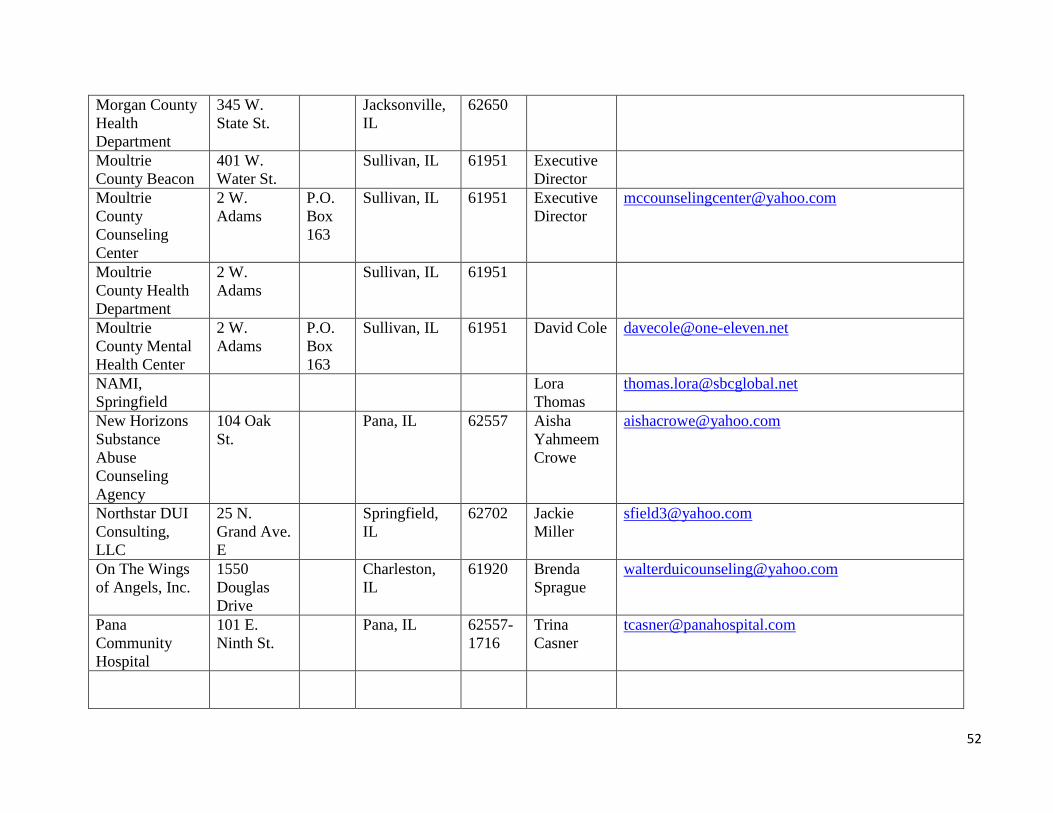
52
Morgan County
Health
Department
345 W.
State St.
Jacksonville,
IL
62650
Moultrie
County Beacon
401 W.
Water St.
Sullivan, IL 61951 Executive
Director
Moultrie
County
Counseling
Center
2 W.
Adams
P.O.
Box
163
Sullivan, IL 61951 Executive
Director
Moultrie
County Health
Department
2 W.
Adams
Sullivan, IL 61951
Moultrie
County Mental
Health Center
2 W.
Adams
P.O.
Box
163
Sullivan, IL 61951 David Cole [email protected]
NAMI,
Springfield
Lora
Thomas
New Horizons
Substance
Abuse
Counseling
Agency
104 Oak
St.
Pana, IL 62557 Aisha
Yahmeem
Crowe
Northstar DUI
Consulting,
LLC
25 N.
Grand Ave.
E
Springfield,
IL
62702 Jackie
Miller
On The Wings
of Angels, Inc.
1550
Douglas
Drive
Charleston,
IL
61920 Brenda
Sprague
Pana
Community
Hospital
101 E.
Ninth St.
Pana, IL 62557-
1716
Trina
Casner

53
Pana
Community
Hospital
101 E.
Ninth St.
Pana, IL 62557-
1716
Greg
Hager, RN
Pana
Community
Hospital
101 E.
Ninth St.
Pana, IL 62557-
1716
Vickie
Coen
Paris
Community
Hospital
721 E.
Court St.
Paris, IL 61944 Randy
Simmons
Park Place
Center, LTD
201 E.
Morgan St.
Jacksonville,
IL
62650 Ed J. Scott [email protected]
Passavant Area
Hospital
1600 W.
Walnut St.
Jacksonville,
IL
62650-
1136
Chester
Wynn
Passavant Area
Hospital
1600 W.
Walnut St.
Jacksonville,
IL
62650-
1136
Orlinda
Speckhart
Workman
Passavant Area
Hospital
1600 W.
Walnut St.
Jacksonville,
IL
62650-
1136
Patty
Bryant,
RN, MS
Passavant Area
Hospital
1600 W.
Walnut St.
Jacksonville,
IL
62650-
1136
Susan
Weikert,
RN
PCC
Community
Wellness Center
Katherine
Suberlak,
LCSW
Personal
Counseling
Services
2659
Farragut
Drive
Springfield,
IL
62704 Vicki
Vandeveer
Piatt County
Mental Health
1921 N.
Market St.
Monticello,
IL
61856 David King [email protected]
Piatt County
Mental Health
1921 N.
Market St.
Monticello,
IL
61856 Scott
Porter

54
Pike County
Health
Department
113 E.
Jefferson
St.
Pittsfield, IL 62363-
1420
Anita
Andress
Pleasant
Counseling
303 E.
Wood St.
Decatur, IL 62523 Diane
Pleasant
Prevention First,
Inc.
2800
Montvale
Drive
Springfield,
IL
62704 Karel
Homrig
Saint Anthony's
Memorial
Hospital
503 N.
Maple St.
Effingham,
IL
62401-
2006
Mark
Reifsteck
Sangamon
County Health
Department
2833 S.
Grand Ave.
E.
Springfield,
IL
62703 Gail
O'Neill
Sarah Bush
Lincoln Health
Center
1000
Health
Center
Drive
P.O.
Box
372
Mattoon, IL 61938-
0372
Bruce
Morgan
Sarah Bush
Lincoln Health
Center
1000
Health
Center
Drive
P.O.
Box
372
Mattoon, IL 61938-
0372
Timothy
Ols
Sarah Bush
Lincoln Health
Center
1000
Health
Center
Drive
P.O.
Box
372
Mattoon, IL
61938-
0372
Darla
Lawson,
RN
Sarah Bush
Lincoln Health
Center
1000
Health
Center
Drive
P.O.
Box
372
Mattoon, IL 61938-
0372
Nancy
Weber, RN

55
Sarah D.
Culbertson
Memorial
Hospital
238 S.
Congress
St.
Rushville, IL 62681-
1465
Lynn
Stambaugh
Schuyler
Counseling and
Health Services
127 S.
Liberty
P.O.
Box
320
Rushville, IL 62681 Trenton
Chockley
Schuyler
County Health
Department
233 N.
Congress
St.
Rushville, IL 62681
Schuyler
County MH
Board
8 Frances
Drive
Rushville, IL 62681 Kip Wilson [email protected]
Scott County
Health
Department
335 W.
Cherry
Winchester,
IL
62694
Shelby County
Community
Services, Inc.
1810 W.S.
Third St.
Shelbyville,
IL
62565 Richard
Gloede
Shelby County
Health
Department
1700 W. S.
Third St.
Shelbyville,
IL
62565
Shelby
Memorial
Hospital
200 S.
Cedar St.
Shelbyville,
IL
62565 Marilyn
Sears
SIU School of
Medicine
P.O.
Box
19620
Springfield,
IL
62794 Executive
Director
SIU School of
Medicine
P.O.
Box
19620
Springfield,
IL
62794 Dr. Soltys [email protected]
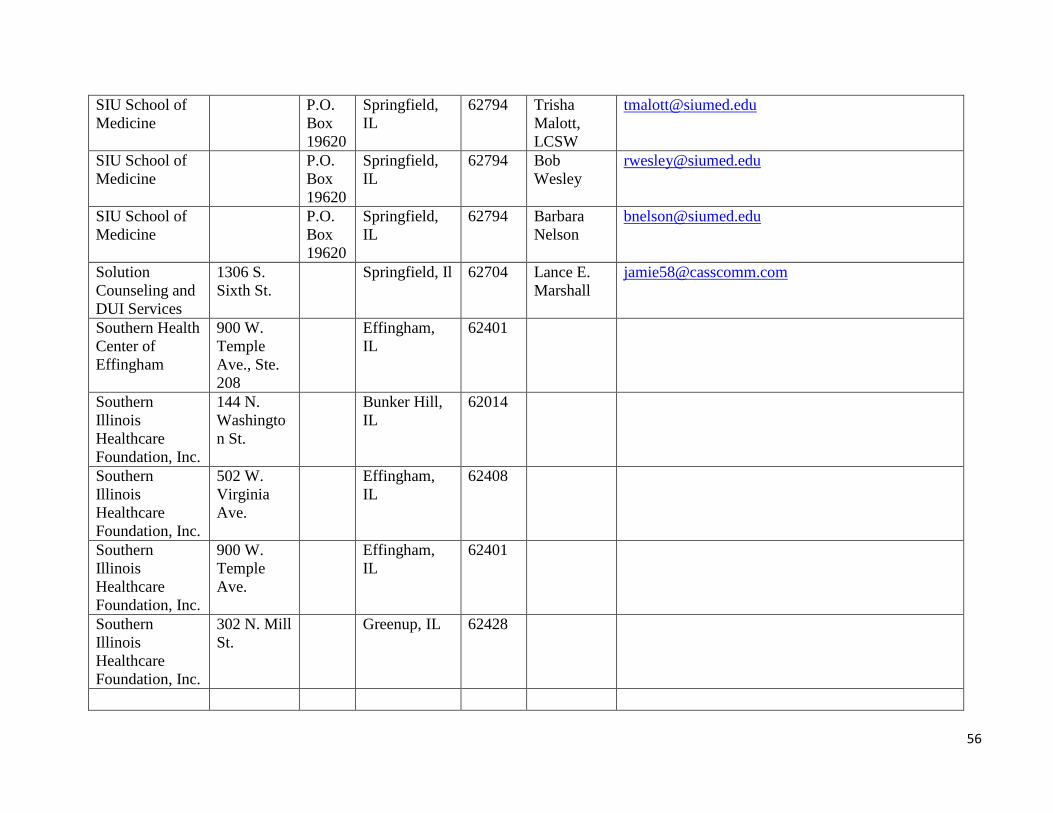
56
SIU School of
Medicine
P.O.
Box
19620
Springfield,
IL
62794 Trisha
Malott,
LCSW
SIU School of
Medicine
P.O.
Box
19620
Springfield,
IL
62794 Bob
Wesley
SIU School of
Medicine
P.O.
Box
19620
Springfield,
IL
62794 Barbara
Nelson
Solution
Counseling and
DUI Services
1306 S.
Sixth St.
Springfield, Il 62704 Lance E.
Marshall
Southern Health
Center of
Effingham
900 W.
Temple
Ave., Ste.
208
Effingham,
IL
62401
Southern
Illinois
Healthcare
Foundation, Inc.
144 N.
Washingto
n St.
Bunker Hill,
IL
62014
Southern
Illinois
Healthcare
Foundation, Inc.
502 W.
Virginia
Ave.
Effingham,
IL
62408
Southern
Illinois
Healthcare
Foundation, Inc.
900 W.
Temple
Ave.
Effingham,
IL
62401
Southern
Illinois
Healthcare
Foundation, Inc.
302 N. Mill
St.
Greenup, IL 62428
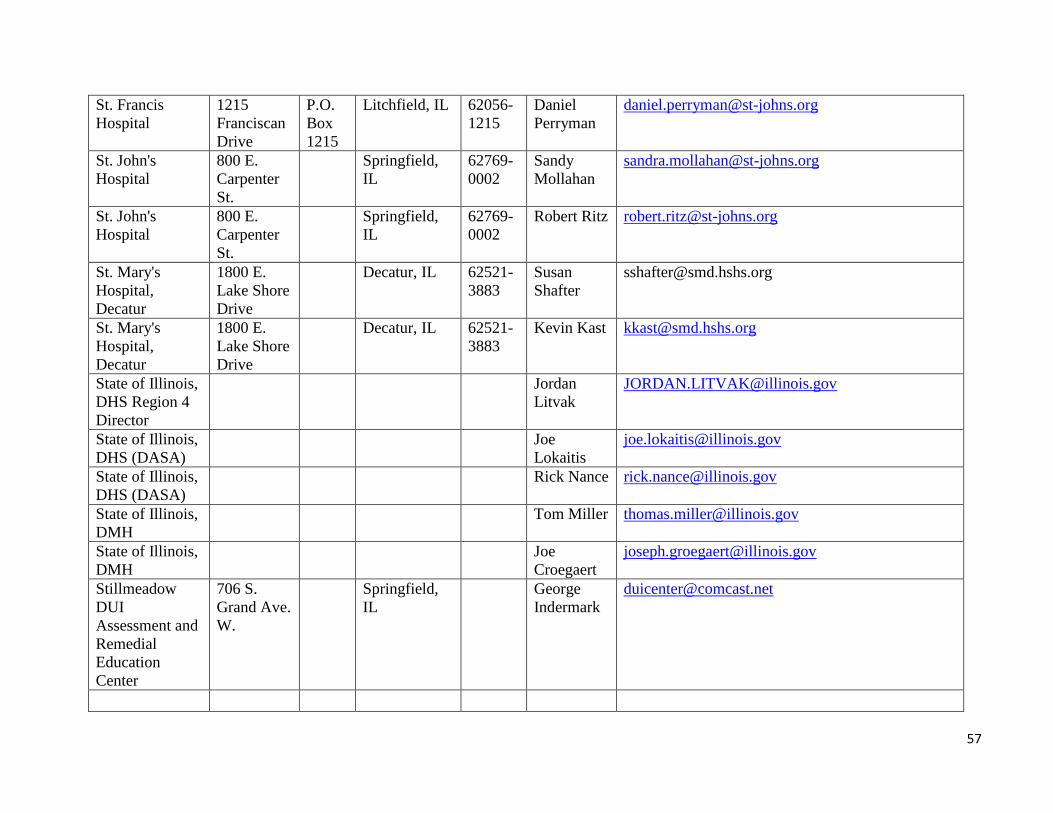
57
St. Francis
Hospital
1215
Franciscan
Drive
P.O.
Box
1215
Litchfield, IL 62056-
1215
Daniel
Perryman
St. John's
Hospital
800 E.
Carpenter
St.
Springfield,
IL
62769-
0002
Sandy
Mollahan
St. John's
Hospital
800 E.
Carpenter
St.
Springfield,
IL
62769-
0002
Robert Ritz [email protected]
St. Mary's
Hospital,
Decatur
1800 E.
Lake Shore
Drive
Decatur, IL 62521-
3883
Susan
Shafter
St. Mary's
Hospital,
Decatur
1800 E.
Lake Shore
Drive
Decatur, IL 62521-
3883
Kevin Kast [email protected]
State of Illinois,
DHS Region 4
Director
Jordan
Litvak
State of Illinois,
DHS (DASA)
Joe
Lokaitis
State of Illinois,
DHS (DASA)
Rick Nance [email protected]
State of Illinois,
DMH
Tom Miller [email protected]
State of Illinois,
DMH
Joe
Croegaert
Stillmeadow
DUI
Assessment and
Remedial
Education
Center
706 S.
Grand Ave.
W.
Springfield,
IL
George
Indermark

58
Synergy
Consulting &
Training LLC
1305
Wabash
Ave.
Springfield, Il 62704 Cynthia
Tubbs
Taylorville
Memorial
Hospital
201 E.
Pleasant St.
Taylorville,
IL
62568-
1597
Daniel
Raab
The Wells
Center
1300
Lincoln
Ave.
Jacksonville,
IL
62650 Bruce
Carter
Thomas H.
Boyd Memorial
Hospital
800 School
St.
Carrollton, IL 62016-
1436
Deborah
Campbell
Transitions of
Western Illinois
4409 Main P.O.
Box
3646
Quincy, IL 62301 J. Michael
Rein, M.S.
Tri-County
Counseling
Center
P.O.
Box
381
Jerseyville,
IL
62052 Executive
Director
Wellspring
Resources
Ann Tyree [email protected]
Youth Advocate
Program
202 E.
Eldorado
St.
Decatur, IL 62523
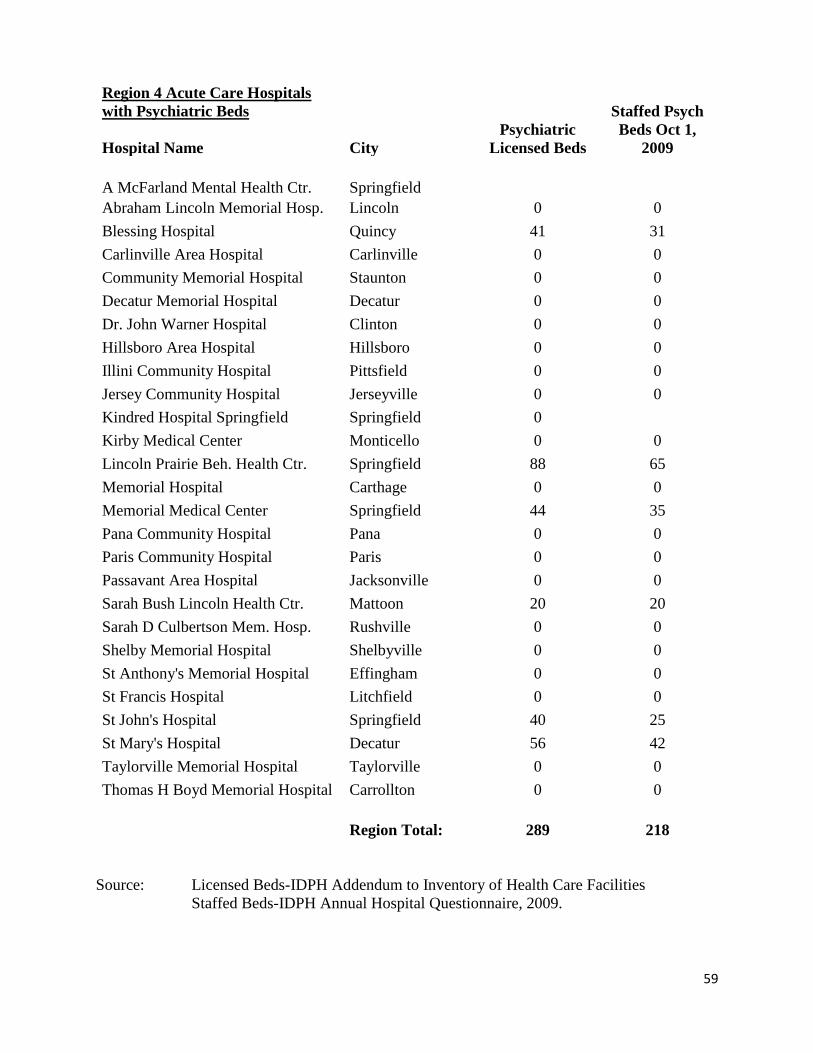
59
Region 4 Acute Care Hospitals
with Psychiatric Beds
Hospital Name City
Psychiatric
Licensed Beds
Staffed Psych
Beds Oct 1,
2009
A McFarland Mental Health Ctr. Springfield
Abraham Lincoln Memorial Hosp. Lincoln 0 0
Blessing Hospital Quincy 41 31
Carlinville Area Hospital Carlinville 0 0
Community Memorial Hospital Staunton 0 0
Decatur Memorial Hospital Decatur 0 0
Dr. John Warner Hospital Clinton 0 0
Hillsboro Area Hospital Hillsboro 0 0
Illini Community Hospital Pittsfield 0 0
Jersey Community Hospital Jerseyville 0 0
Kindred Hospital Springfield Springfield 0
Kirby Medical Center Monticello 0 0
Lincoln Prairie Beh. Health Ctr. Springfield 88 65
Memorial Hospital Carthage 0 0
Memorial Medical Center Springfield 44 35
Pana Community Hospital Pana 0 0
Paris Community Hospital Paris 0 0
Passavant Area Hospital Jacksonville 0 0
Sarah Bush Lincoln Health Ctr. Mattoon 20 20
Sarah D Culbertson Mem. Hosp. Rushville 0 0
Shelby Memorial Hospital Shelbyville 0 0
St Anthony's Memorial Hospital Effingham 0 0
St Francis Hospital Litchfield 0 0
St John's Hospital Springfield 40 25
St Mary's Hospital Decatur 56 42
Taylorville Memorial Hospital Taylorville 0 0
Thomas H Boyd Memorial Hospital Carrollton 0 0
Region Total: 289 218
Source: Licensed Beds-IDPH Addendum to Inventory of Health Care Facilities
Staffed Beds-IDPH Annual Hospital Questionnaire, 2009.
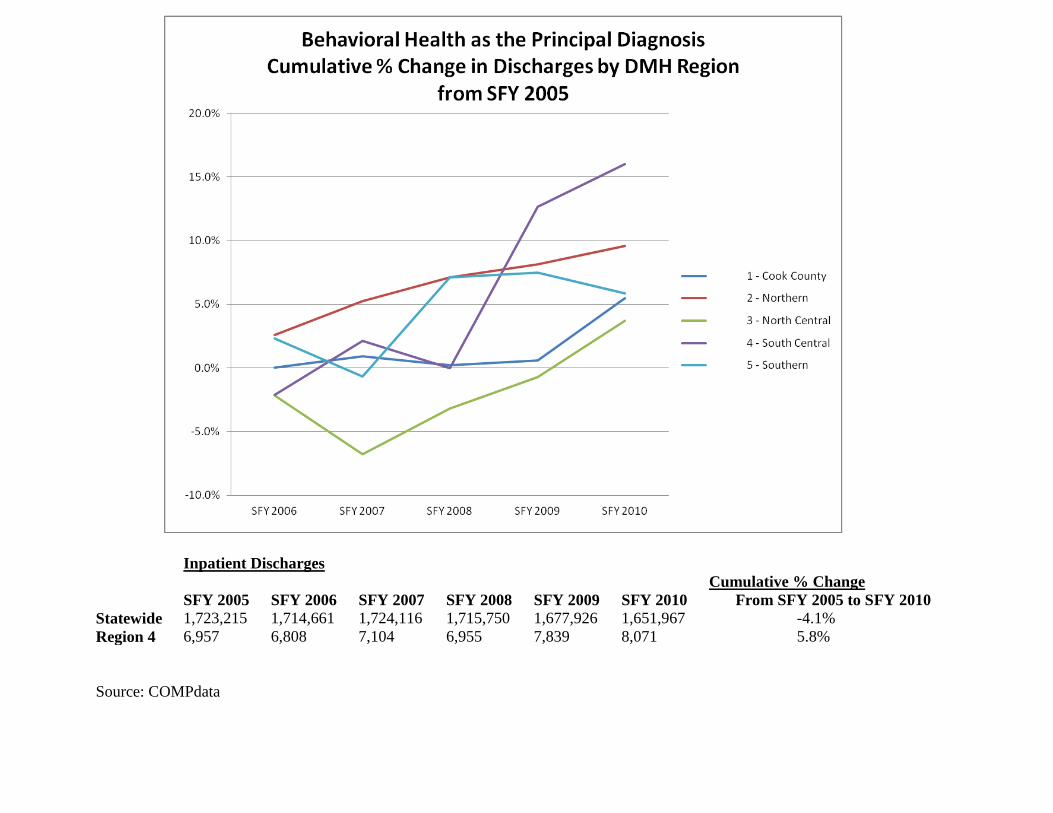
Inpatient Discharges
Cumulative % Change
SFY 2005 SFY 2006 SFY 2007 SFY 2008 SFY 2009 SFY 2010 From SFY 2005 to SFY 2010
Statewide 1,723,215 1,714,661 1,724,116 1,715,750 1,677,926 1,651,967 -4.1%
Region 4 6,957 6,808 7,104 6,955 7,839 8,071 5.8%
Source: COMPdata
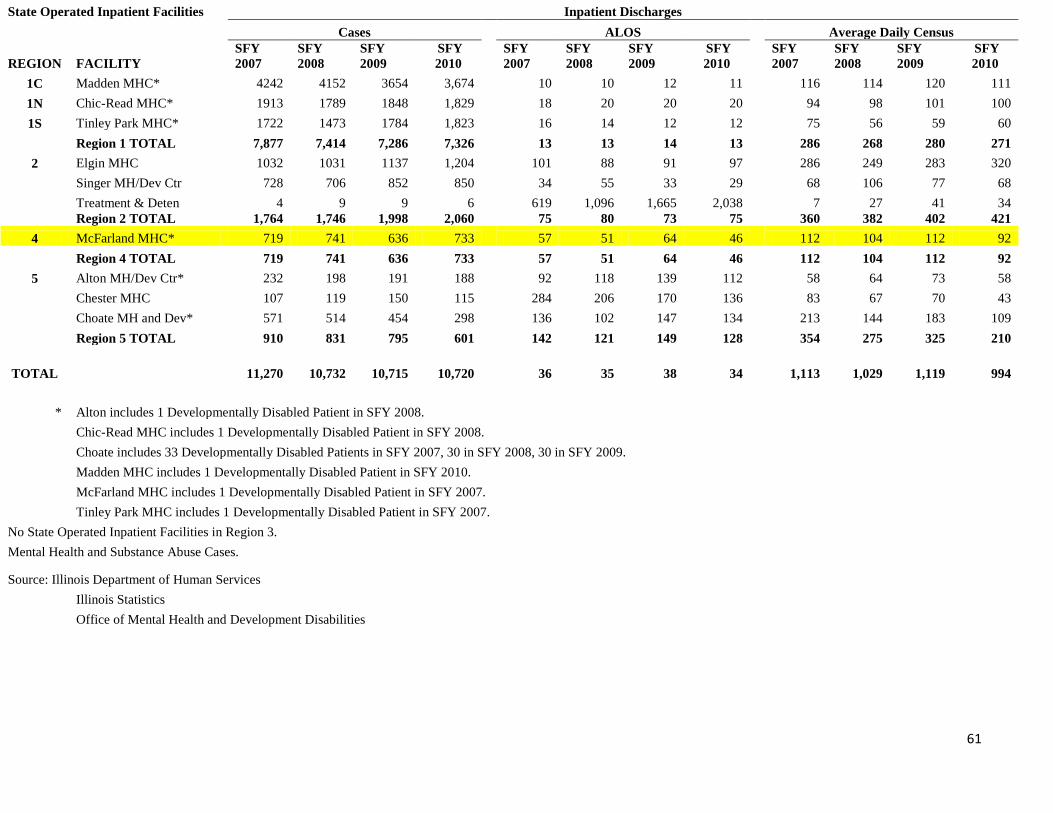
61
State Operated Inpatient Facilities Inpatient Discharges
Cases
ALOS
Average Daily Census
REGION FACILITY
SFY
2007
SFY
2008
SFY
2009
SFY
2010
SFY
2007
SFY
2008
SFY
2009
SFY
2010
SFY
2007
SFY
2008
SFY
2009
SFY
2010
1C Madden MHC* 4242 4152 3654 3,674
10 10 12 11
116 114 120 111
1N Chic-Read MHC* 1913 1789 1848 1,829
18 20 20 20
94 98 101 100
1S Tinley Park MHC* 1722 1473 1784 1,823
16 14 12 12
75 56 59 60
Region 1 TOTAL 7,877 7,414 7,286 7,326
13 13 14 13
286 268 280 271
2 Elgin MHC 1032 1031 1137 1,204
101 88 91 97
286 249 283 320
Singer MH/Dev Ctr 728 706 852 850
34 55 33 29
68 106 77 68
Treatment & Deten 4 9 9 6
619 1,096 1,665 2,038
7 27 41 34
Region 2 TOTAL 1,764 1,746 1,998 2,060
75 80 73 75
360 382 402 421
4 McFarland MHC* 719 741 636 733
57 51 64 46
112 104 112 92
Region 4 TOTAL 719 741 636 733
57 51 64 46
112 104 112 92
5 Alton MH/Dev Ctr* 232 198 191 188
92 118 139 112
58 64 73 58
Chester MHC 107 119 150 115
284 206 170 136
83 67 70 43
Choate MH and Dev* 571 514 454 298
136 102 147 134
213 144 183 109
Region 5 TOTAL 910 831 795 601
142 121 149 128
354 275 325 210
TOTAL 11,270 10,732 10,715 10,720
36 35 38 34
1,113 1,029 1,119 994
* Alton includes 1 Developmentally Disabled Patient in SFY 2008.
Chic-Read MHC includes 1 Developmentally Disabled Patient in SFY 2008.
Choate includes 33 Developmentally Disabled Patients in SFY 2007, 30 in SFY 2008, 30 in SFY 2009.
Madden MHC includes 1 Developmentally Disabled Patient in SFY 2010.
McFarland MHC includes 1 Developmentally Disabled Patient in SFY 2007.
Tinley Park MHC includes 1 Developmentally Disabled Patient in SFY 2007.
No State Operated Inpatient Facilities in Region 3.
Mental Health and Substance Abuse Cases.
Source: Illinois Department of Human Services
Illinois Statistics
Office of Mental Health and Development Disabilities
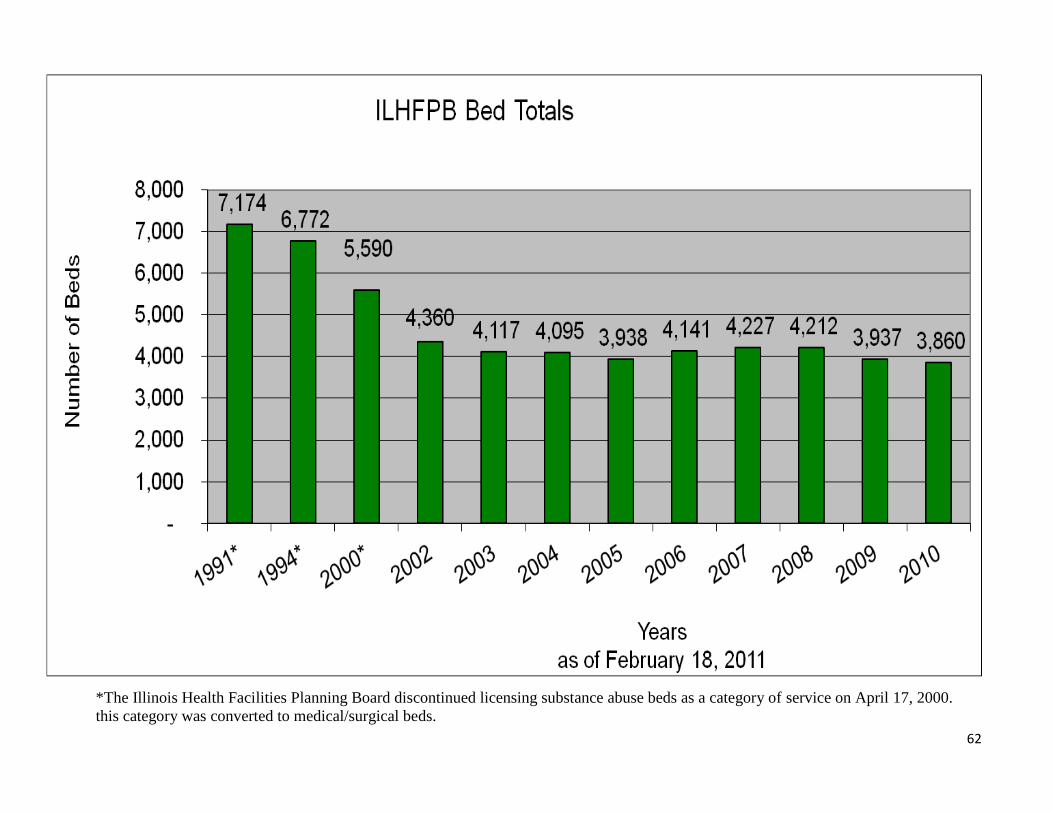
62
*The Illinois Health Facilities Planning Board discontinued licensing substance abuse beds as a category of service on April 17, 2000.
this category was converted to medical/surgical beds.

63
Hospital Statistics
DMH Hospital Statistics - FY 03 through FY 09
FY 03 FY 04 FY 05 FY 06 FY 07 FY 08 FY 09
Total Presentations (Civil
only)
10,472 10,759 11,233 11,657 11,654 10,812 10,504
Total Admissions (Civil &
Forensics)
9,625 9,609 10,190 11,421 11,349 10,729 10,677
Civil Total Admissions 8,991 8,975 9,580 10,860 10,747 10,139 10,103
Civil Adult 8,870 8,844 9,462 10,770 10,668 10,063 10,045
Civil Child & Adolescents 121 131 118 90 79 76 58
Forensics total 634 634 610 561 602 590 574
Forensics Adult 611 614 593 546 587 573 565
Forensics Child &
Adolescents
23 20 17 15 15 17 9
Total Triage 1,482 1,784 1,653 797 907 673 401
Total Transfers-in 409 414 466 232 211 246 271
Civil total 365 364 410 166 152 184 200
Civil Adult 365 364 410 166 152 184 200
Civil Child & Adolescents 0 0 0 0 0 0 0
Forensics Total 44 50 56 66 59 62 71
Forensics Adult 43 50 55 66 59 62 71
Forensics Child &
Adolescents
1 0 1 0 0 0 0
Individuals with 3+
admissions Civil only
569 536 592 639 630 585 626
Individuals with 3+
admissions Civil only
forensics
0.0632 0.0597 0.0617 0.059 0.059 0.055 0.059
FY
03
FY
04
FY
05
FY
06
FY
07
FY
08
FY
09
All Admissions/100,000 78 77 82 92 91 86 86
Total Civil Admissions/100,000 72 72 77 87 87 82 81
Adult Civil Admissions/100,000 97 96 103 117 116 110 109
Child & Adolescents Civil
Admissions/100,000
4 0 4 3 2 2 2
Total Forensics Admissions/100,000 5 5 5 5 5 5 5
Adult Forensics Admissions/100,000 7 7 6 6 6 6 6
Child & Adolescents Forensics
Admissions/100,000
1 1 1 0 0 1 0
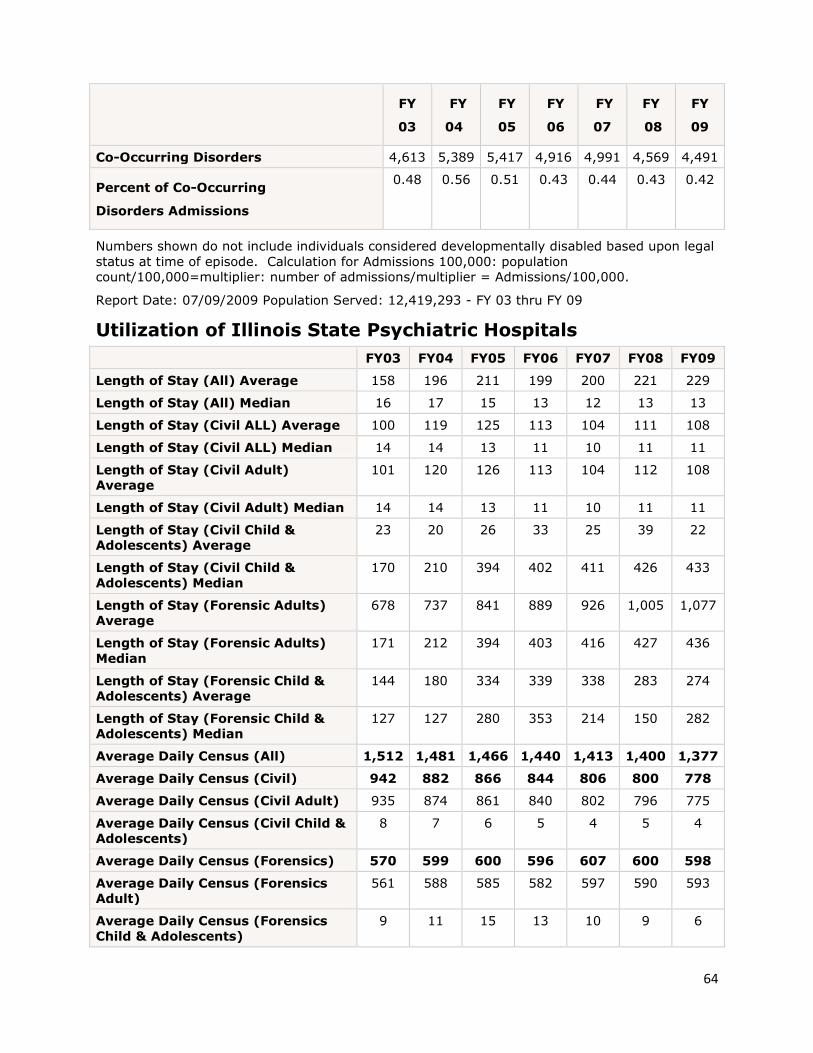
64
FY
03
FY
04
FY
05
FY
06
FY
07
FY
08
FY
09
Co-Occurring Disorders 4,613 5,389 5,417 4,916 4,991 4,569 4,491
Percent of Co-Occurring
Disorders Admissions
0.48 0.56 0.51 0.43 0.44 0.43 0.42
Numbers shown do not include individuals considered developmentally disabled based upon legal
status at time of episode. Calculation for Admissions 100,000: population
count/100,000=multiplier: number of admissions/multiplier = Admissions/100,000.
Report Date: 07/09/2009 Population Served: 12,419,293 - FY 03 thru FY 09
Utilization of Illinois State Psychiatric Hospitals
FY03 FY04 FY05 FY06 FY07 FY08 FY09
Length of Stay (All) Average 158 196 211 199 200 221 229
Length of Stay (All) Median 16 17 15 13 12 13 13
Length of Stay (Civil ALL) Average 100 119 125 113 104 111 108
Length of Stay (Civil ALL) Median 14 14 13 11 10 11 11
Length of Stay (Civil Adult)
Average
101 120 126 113 104 112 108
Length of Stay (Civil Adult) Median 14 14 13 11 10 11 11
Length of Stay (Civil Child &
Adolescents) Average
23 20 26 33 25 39 22
Length of Stay (Civil Child &
Adolescents) Median
170 210 394 402 411 426 433
Length of Stay (Forensic Adults)
Average
678 737 841 889 926 1,005 1,077
Length of Stay (Forensic Adults)
Median
171 212 394 403 416 427 436
Length of Stay (Forensic Child &
Adolescents) Average
144 180 334 339 338 283 274
Length of Stay (Forensic Child &
Adolescents) Median
127 127 280 353 214 150 282
Average Daily Census (All) 1,512 1,481 1,466 1,440 1,413 1,400 1,377
Average Daily Census (Civil) 942 882 866 844 806 800 778
Average Daily Census (Civil Adult) 935 874 861 840 802 796 775
Average Daily Census (Civil Child &
Adolescents)
8 7 6 5 4 5 4
Average Daily Census (Forensics) 570 599 600 596 607 600 598
Average Daily Census (Forensics
Adult)
561 588 585 582 597 590 593
Average Daily Census (Forensics
Child & Adolescents)
9 11 15 13 10 9 6

65
FY03 FY04 FY05 FY06 FY07 FY08 FY09
Total Number of Residents & Home
Visits on 7/09/09.
1,410 1,369 1,402 1,322 1,373 1,353 1,319
Total Number of Civil Residents and
Home Visits on 7/09/09.
799 760 791 706 762 742 709
Total Number of Civil Adult
Residents and Home Visits on
7/09/09.
797 757 786 705 757 742 707
Total Number of Civil Child &
Adolescents Residents and Home
Visits on 7/09/09.
2 3 5 1 5 0 2
Total Number for Residential and
Home Visits on 7/09/09
611 609 611 616 611 611 610
Total Number for Adult Residential
and Home Visits on 7/09/09
601 593 595 601 603 601 605
Total Number for Child
& Adolescents Residential and
Home Visits on 7/09/09
10 16 16 15 8 10 5
Utilization of Illinois State Psychiatric Hospitals
FY 03 FY 04 FY 05 FY 06 FY 07 FY 08 FY 09
Total Separations 10,190 10,058 10,625 11,731 11,496 10,988 10,979
Total Discharges (Civil &
Forensics)
9,772 9,641 10,150 11,498 11,286 10,739 10,708
Civil Total Discharge 9,255 9,052 9,584 10,981 10,729 10,211 10,171
Civil Adult 9,122 8,922 9,468 10,888 10,654 10,131 10,115
Civil Child & Adolescents 133 130 116 93 75 80 56
Forensics Total 517 589 566 517 557 528 537
Forensic Adults 502 578 553 506 538 517 525
Forensic Child &
Adolescents
15 11 13 11 19 11 12
Total Transfers-Out (Civil
& Forensic)
418 417 475 233 210 249 271
Civil Total 368 359 408 161 138 173 200
Civil Adult 368 359 408 161 138 173 200
Civil Child & Adolescents 0 2 0 0 0 0 0
Forensics Total 50 58 67 72 72 76 71
Forensics Adult 49 58 65 72 72 76 71
Forensics Child &
Adolescents
1 0 2 0 0 0 0
Report date 07/09/2009 Population Served 12,419,293 http://www.dhs.state.il.us/page.aspx?item=33869

1
Illinois Regional Integrated
Behavioral Health Networks
Region 5
Draft Report

2
Table of Contents Topics Page # Region 5 Plan
Background 3-4
Access 4-5
Funding 5-6
Quality Improvement 6-7
Technology 7-8
Workforce 8-9
Meetings
Letter of Invitation 10-11
Agenda Nov. 21 12
Minutes Nov. 21 13-14
Small Group Responses Nov. 21 15-17
Agenda Jan. 5 18
Minutes Jan. 5 19-20
Small Group Responses Jan. 5 21-25
Agenda Jan. 31 26
Minutes Jan. 31 27-28
Appendices
PA 97-0381 29-32
Questionnaire 33-37
Region 5 Contact List 38-55
Psychiatric & Licensed Staffed Beds 56-57
Statewide & Behavioral Health Primary
Diagnoses Discharges 58
State Operated Hospitals Inpatient Discharges 59
ILHFB Bed Totals 60
Hospital Statistics 61-64

3
Illinois Regional Behavioral Health Networks
For hospital, primary care, mental health, substance abuse and other community-based providers
Region 5
Note: The content of this report does not reflect the opinion or position of the Illinois Hospital
Association.
Background
On August 15, 2011, Governor Pat Quinn signed into law House Bill 2982 as Public Act 97-
0381, which created the Regional Integrated Behavioral Health Networks Act. The Act provides
a platform to establish 12 Regional Integrated Behavioral Health Networks. Its purpose is to
ensure and improve access to appropriate mental health and substance abuse services throughout
Illinois by: organizing systematically all relevant health, mental health, substance abuse, and
other community resources among regional providers; developing a mechanism to use regional
resources efficiently and effectively; and serving as a catalyst for innovation and collaboration.
Under the act, each Behavioral Health Regional Network shall develop a strategic plan for its
respective region that addresses the inventory of existing services, identifies community needs
and defines opportunities to improve access to care. The act contemplates a broad cross-section
of the mental health, substance abuse, health, and social services community that will be
involved in the development and implementation of the plan. Collaboration among all of the
relevant community resources will be essential to accomplish the purposes of the act and to build
effective, coordinated and comprehensive systems of care.
In partnership with the Illinois Department of Human Services (DHS), Division of Mental Health
and Division of Alcoholism and Substance Abuse, the Illinois Hospital Association and others
convened a group of behavioral health providers in the State’s DHS Region 5 to begin to identify
existing services in the region, strategies for improving the behavioral health services delivery
system including timely and appropriate access to medical and behavioral health services, and
ways in which providers can begin working together to improve access to services and patient
outcomes.
This plan outlines the priorities and recommendations for DHS Region 5, articulated by
participating service providers in three Region 5 meetings. At the first meeting held at Salem
Township Hospital, Salem on November 21, 2011, providers defined their vision for behavioral
health care services and outlined priority issues and areas of focus. During the second meeting at
Centralia Recreational Complex on January 5, 2012, participants identified strategies to improve
priority areas of concern listed in this plan. In the third meeting held at Centralia Recreational
Complex on January 31, 2012, the group reviewed and provided input on the first draft of a
regional plan and provided additional feedback on data sources and trends they have experienced
over the past 12 months.
This plan is a template that recognizes the shortcomings and inefficiencies of the present system,
but also embraces partnerships that promise better coordination of care, across primary medical
4
and behavioral care, using technology and research to improve outcomes. It is an interactive
process and one that will evolve with a changing health care and economic landscape and will
depend on the continued commitment of all stakeholders, state agencies, primary medical,
hospitals, and behavioral health providers. It builds on community strengths to achieve a system
of care that delivers the right care, at the right time, in the right place.
1. Access
First and foremost, providers were concerned about access to behavioral health services
for all residents of the region. Patients and consumers seeking behavioral health care
currently find long waiting lists for outpatient care, long waits in hospital emergency
departments, long waits for admission to state-operated psychiatric hospitals, and long
waits for substance abuse treatment. Providing coverage for all residents in a timely
manner through a Patient-Centered Medical Home (PCMH) model with integrated
behavioral health services provides the patient and his or her family with the consistent
health services needed for both physical and behavioral health with a holistic approach to
health care and wellness.
A PCMH model would provide connections to community mental health centers,
substance abuse treatment and prevention service providers, and other community-based
services through a care coordination program. A care coordination program will help
patients and their families navigate through health care as they move from assessment,
diagnosis, treatment, follow-up and pharmaceutical compliance. The PCMH will also
provide a foundation for the integration of physical and behavioral health services as well
as a coordinated system for patient medical records.
In addition to PCMH’s and care coordination programs, Region 5 participants would like
to explore alternative strategies to provide behavioral health services in a more
appropriate setting to stabilize patients in crisis, provide counseling to keep patients out
of crisis, assist patients with life challenges, and provide outreach to patients to improve
their quality of life through community resources, employment, housing, etc.
Notwithstanding the value of providing alternative services, providers emphasized the
need to maintain access to the full continuum of care, from acute care to rehabilitative
services.
Recommendations
Provide an alternative to the use of hospitals’ emergency departments by developing a
continuum of crisis intervention services, such as crisis stabilization centers and
home-based counseling services.
Improve assessments of emergency department (ED) patients to refer and obtain the
right level and intensity of care for them and effectively facilitate transition to this
care.

5
Coordinate care for patients and their families who navigate through the service
delivery system.
Expand access to patient-centered medical homes with integrated behavioral health
services.
Identify a centralized patient access system to ensure patients receive the right level
of care, at the right time, and in the right setting (inpatient, outpatient, treatment,
counseling, and prevention).
Utilize community-based mental health centers, substance abuse providers, home
health agencies and others to track and monitor patients with chronic conditions to
keep them out of crisis.
Facilitate intake process and care coordination through use of electronics and
technology
Strengthen community mental health centers and bring together mental health,
behavioral health and substance abuse services.
2. Funding
Participants agreed that the funding structure should be redesigned to support flexible,
patient-centered care in the future. There was consensus among providers that funding
needs to follow the patient through the system of care. Providers would like to work with
the department and statewide organizations to plan for the use of state, federal, and
commercial insurer funds that better meet the needs of patients and their families.
Region 5 stakeholders expressed a need to decrease ED usage and create regional crisis
centers where patients can access necessary counseling, crisis interventions and
stabilization services. The creation of more outpatient services will help to reduce the
cost of care and provide more timely services for patients and their families. Members
agreed that regional providers need to work together to develop new strategies and pool
resources when necessary to meet patient needs in a more cost-efficient manner.
There is a recognition that multiple providers may need to collaborate to address common
needs. For example, multiple providers would work together to fund transportation
services in a region or to create alternative settings for service delivery. If the state
currently provides transportation for involuntary patients, can multiple providers pool
resources to provide transportation for voluntary patients?
Recommendations

6
Convene groups of providers to redesign the multiple health and human services
funding streams of providers within the region to support funding that follows the
patient through the behavioral health and health care systems.
Create behavioral health collaboratives around common needs such as transportation,
alternative service models, etc., to pool resources and implement new models for
patient services. Build these partnerships to better serve patients at lower costs.
Identify ways in which Federally Qualified Health Centers (FQHCs), Rural Health
Clinics (RHCs), and mental health providers can bill medical and behavioral health
services to Medicaid on the same day.
Explore private, state and federal funding opportunities to pilot new alternative
strategies to deliver behavioral health services in the region (crisis centers, care
coordinators, etc.). Also, make sure that we are capturing all federal matching dollars.
Explore ways to build capacity funding to keep services available in rural areas.
Review ways in which groups can collaborate to reduce the duplication and extra
paperwork.
Work with the state to enhance transportation funding for voluntary admits, mid-level
providers, and for return trips from hospitals and providers. Large geographic areas
cause great expense to patients and providers.
3. Quality Improvement
The group discussed the need to move towards outcomes-based care and develop a
consistent set of measures across the continuum of care. Participants agreed that
providers need to collect, analyze, and utilize data to provide more effective and efficient
services in the region. With an increasing need to identify patient needs and deliver high-
quality patient outcomes, providers need to develop quality measures that assess patient
outcomes as they move through the continuum of behavioral health services. There is a
real need to develop consistent outcome measures for patients regardless of where they
enter the system of care. Providers would like more information on evidence-based
practices that improve patient outcomes and best practice strategies to improve care.
There is also a need to eliminate the stigma associated with behavioral health issues.
Recommendations
State and local providers need to review existing mental health/behavioral
health/substance abuse core measures to ensure consistency.
Develop core measures to be used by the behavioral health care team to demonstrate
meaningful patient outcomes, not just outcome measures.

7
Cross-train providers on key patient measures needed to assess patient outcomes
across the continuum of behavioral health care service providers.
DHS and its state partners should host training sessions for behavioral health
providers to provide a consistent message on rules related to Emergency Medical
Treatment and Active Labor Act (EMTALA) and patient confidentiality.
Providers and state routinely review measures to make sure they continue to be
appropriate.
Review federal models and innovations.
View interventions, trauma issues and the community as a whole.
4. Technology
Region 5 providers would like the state to assist them in utilizing technology to improve
access to care and create efficiencies in the system. Participants would like the state to
use technology to improve the intake process so that patients can be directed to the right
level of care, at the right time and right place.
Providers would like to integrate behavioral health services into the patient’s electronic
medical records and have access to the patient’s complete health record when caring for
the patient. Creating an authorization form for patients to allow their behavioral health
provider to have access to their electronic medical record will assist providers in
assessing and treating the behavioral health needs of their patients.
Providers would also like to better utilize technology to reduce duplication in the
behavioral health system. Patients receive numerous assessments as they move from the
community mental health center to the specialist office to the hospital and back to the
community mental health center. There is redundancy in the process, which utilizes
resources that are unnecessary and delays access to care for the patient and their family.
Providers would like to utilize technology to record assessment information at the point
of entry and build the patient record as they move through the health care services.
Providers also would like to work with the state and its partners to expand access to
psychiatrists and other specialty providers through telemedicine services, especially
telepsychiatry in the rural parts of the region. Telepsychiatry is currently working in
several communities to provide assessment, treatment, counseling, and follow-up
services. However, the cost of equipment ($20,000) can be a barrier to implementation
especially in rural community mental health centers and substance abuse centers.
Recommendations

8
State agency leaders and providers should meet to discuss reductions in duplication
related to assessments, patient forms and provider reporting requirements through
technology programs and software. This duplication increases cost to the behavioral
health system and delays patient care.
Work with the Office of Health Information Technology and the state Health
Information Exchange (HIE) Advisory Committee to integrate behavioral health
services into the state’s HIE planning and implementation strategies and provide
technical assistance to work together.
Work with state, federal and private funders to identify resources to expand access to
telemedicine equipment, especially for rural providers in the region. Also, work with
providers to provide reliable and consistent delivery.
5. Workforce
The group of providers recognized a need to develop the workforce that will manage care
in the new service delivery system. There will be a need for new workers such as care
coordinators and patient navigators, information technology specialists, home health
services, and family and patient educators. Staff from the different specialty care
providers will need to be cross-trained to understand the needs of patients as they move
from one type of behavioral health provider to another, especially for those with multiple
chronic conditions.
Providers continue to struggle with workforce shortages especially in the rural parts of
the region. Utilizing vocational and community college training programs, providers will
work to identify new members of the behavioral health workforce. However, they will
need to utilize telemedicine services to access specialty services in rural communities.
The group agreed that new information and professional skills will be needed by those in
the future workforce to address patient care such as: growing quality measures, cross-
training across specialty services, interactions with law enforcement, primary care
integration, electronic medical records, new billing and coding data, and ongoing
evidence-based practice training. Linkages with higher education will continue to be a
priority as these new members of the workforce are developed.
The group also discussed the need for providers to reach out to other community-based
organization that provide quality of life services for patients and families like housing
and transportation services.
Recommendations
Identify new skills needed by the workforce of the future and design payment systems
to fund those provider services (care coordinators, patient navigators, data, etc.).
Also, provide incentives for those to work in rural areas.

9
Remove regulatory barriers that limit the existing workforce from transitioning to the
new system of behavioral health services. Focus on building capacity of mid-level
providers to provide care in rural regions experiencing workforce shortages.
Work with universities, community colleges, and vocational schools to recruit and
train new behavioral health service providers.
Develop a forum for a network of regional providers to share current roles and
responsibilities, share changes in regional capacity, and work together to solve
common problems.
Develop a source of consistent training for behavioral health providers to have
common understanding of language, medication, roles, and regulatory boundaries.
Also, provide training for all of those that come in contact with patients.
Disseminate a repository of evidence-based practices for providers to share.
Address reimbursement issues related to licensed clinical social workers (LCSW),
licensed clinical professional counselor (LCPC), licensed social workers, and
certified alcohol and drug counselor workers.
Create collaboration with schools and faith-based organizations.
10
October 27, 2011
Name
Title
Organization
Address
City, State Zip
Dear:
As providers, we know that persons with mental and substance use illnesses in Illinois must
navigate a complex amalgam of services that are inconsistently available and accessible. Many
seek care from us in crisis because they could not obtain more timely or appropriate care. Our
state and federal fiscal crises have translated into the loss of essential behavioral health services
particularly in rural Illinois. Yet, despite these challenging circumstances, we can also identify
opportunities to improve care. Some of these opportunities stem from health reform; others are
being generated by our own strategies to serve our patients and communities. One such
opportunity is being presented to us by the recent enactment of House Bill 2982 – Public Act 98-
031, which creates the Regional Integrated Behavioral Health Networks Act.
The bill establishes Regional Integrated Behavioral Health Networks to ensure and improve
access to appropriate mental health and substance abuse services throughout Illinois by
systematically organizing all relevant health, mental health, substance abuse, and other
community resources among regional providers, to develop a mechanism to use regional
resources efficiently and effectively.
Under the Act, each Behavioral Health Regional Network shall develop a strategic plan for its
respective region that addresses the inventory of existing services, identifies community needs
and defines opportunities to improve access to care. The Act contemplates a broad-cross section
of the mental health, substance abuse, health, and social services community will be involved in
the development –and implementation—of the plan. Collaboration among all of the relevant
community resources will be essential to accomplish the purposes of the Act and to build
effective, coordinated and comprehensive systems of care.
We would like to invite you to participate in the first Behavioral Health Regional Network
meeting for Region 5. The meeting will take place Monday, November 21 from 10:00 am to
1:00 pm at Salem Township Hospital in Salem, IL.
Many of you attended the Southern Illinois Behavioral Health Consortium meeting hosted by the
SIUC Center for Rural Health and Social Service Development on October 7. Not only are the
goals for the Behavioral Health Regional Network in line with the vision expressed by those in
attendance at the first Consortium meeting, but the stakeholders are almost identical. Let’s build
11
on the ideas generated by the consortium to develop our Behavioral Health Regional Network
strategic plan for Region 5.
If you have any questions or concerns, please contact IHA Staff: Lori Williams, at 217-541-
1164 or [email protected] or MaryLynn M. Clarke at 217-541-1154 or
To confirm your attendance, please contact Abby Radcliffe at 217-541-1178 or email your
response to [email protected].
Thank you,
MaryLynn M. Clarke
Sr. Director,
Health Policy & Regulation,
Illinois Hospital Association
Lori Williams
V.P. Small & Rural Hospital Affairs,
Illinois Hospital Association
Kim Sanders
Director, Center for Rural Health
& Social Service Development

12
Illinois Behavioral Health Network Meeting – Region 5
November 21, 2011, 10:00 a.m. – 1:00 p.m.
Salem Township Hospital, 1201 Ricker Drive, Salem, IL
Agenda
I. WELCOME & INTRODUCTIONS ................10:00 ............................ Dave Allen
II. OVERVIEW OF HB 2982 (PA 97-0381) .........10:20 ....................... Lori Williams
III. REGIONAL PLAN DISCUSSION GROUPS..10:25 ................................. Groups
What should the behavioral health system look like three years from now?
What would be the key components of the new behavioral health system?
Are there immediate actions that could be taken to improve access to behavioral
health services in this region? If so, what are they?
IV. SMALL GROUP REPORTS ............................11:30 ........................ Kim Sanders
V. SETTING PRIORITIES & NEXT STEPS ....12:15 ............................ Dave Allen
VI. ADJOURNMENT & NEXT MEETING ........1:00 .............................. Dave Allen
13
Illinois Behavioral Health Network Meeting – Region 5
November 21, 2011
Salem Township Hospital, 1201 Ricker Drive, Salem, IL 62881-6250
Sharon Adams, The H Group
Dave Allen, Richland Memorial Hospital
Vince Ashley, Harrisburg Medical Center
Dan Boehmer, Jefferson Co. Comp. Services
Georgianne Broughton, Com. Resource Center
Gary L. Buatte, Human Service Center
Robert Cole, Human Support Services
John Cooley, Touchette Regional Hospital
Lisa Crouch, SMGSMG
Randall Dauby, Hamilton Memorial Hospital
Denise Daum, Community Resource Center
Sulbrena Day, Touchette Regional Hospital
Tom Duff, United Methodist Children’s Home
Diane Duft, Bond Co. Health Department
Joann Emge, Sparta Hospital
Susan Englehardt, Perry County Counseling
Mickey Finch, The Fellowship House
Cynthia K. Flamm, Rural Health Inc.
Sharon Fradelos, JeffersonCo. Comp. Services
Amy Gibbar, Chestnut Health Systems
Ann Guild, Illinois Hospital Association
Angie Hampton, Egyptian Health
Joan Hartman, Chestnut Health Systems
Ruth Heitkamp, SIU
Wendy Ice, Delta Center
Beth Inman, Pinckneyville Hospital
Jeannie Johnson, Jasper Co. Health Dept.
Laurie Kellerman, Marshall Browning Hospital
Dietra Julieke, Chestnut Health Systems
John Markley, The H Group
Kate Mays, Delta Center
Mary McMahan, Union Co. Counseling Services
Gajif McNeill, IDHS/DASA
Kelly Medlin, WellSpring Resources
Donna Meyers, St. Elizabeth Hospital
Nancy Newby, Washington County Hospital
Jim Novelli, DHS/DMH
Deborah Page, The H Group
Cindy Poland, Wabash Co. Health Department
Abby Radcliffe, Illinois Hospital Association
Kim Sanders, SIU
Wanda Scates, Egyptian Health
Lori Schmider, Jefferson Co. Comp. Services
Greg Sims, St. Mary’s Good Samaritan
Loretta Stevens, SMGSMG
Michele Sturm, Gateway Regional Medical Center
Sharon Szatkowski, Salem Medical Center, SIHC
Woody Thorne, Southern Illinois Healthcare
Deborah Vogel, St. Elizabeth Hospital
Bob Wesley, SIU School of Medicine
Lori Williams, Illinois Hospital Association
Art Zaitz, DHS/DMH
I. Welcome & Introductions
Dave Allen called the meeting to order at 10:00 a.m. and those in attendance introduced
themselves. An overview was given of the current state of problems. Dave noted that the
group was not here to rehash the problems, but to find solutions.
II. Overview of HB 2982 (PA 97-0381)
Lori Williams gave an overview of the legislation which requires the Department of
Human Services (DHS) to create Regional Behavioral Health Networks in each DHS
region to ensure and improve access to behavioral health services. The networks will
work collaboratively to develop region-specific plans. The legislation also created the
Regional Integrated Behavioral Health Networks Steering Committee comprised of state
agencies to coordinate efforts among planning regions.

14
III. Regional Plan Discussion Groups
Participants were divided into groups to discuss three questions: 1)What should the
behavioral health system look like three years from now?; 2)What would be the key
components of the new behavioral health system?; and 3)Are there immediate actions
that could be taken to improve access to behavioral health services in this region? If so,
what are they?
IV. Small Group Reports
Kim Sanders led the small groups to report on their findings. Information from the
break-out groups is included in the attached document.
V. Setting Priorities & Next Steps
Information collected at the meeting will be assembled by IHA. A focus on priorities and
developing specifics of the plan will be examined at the next meeting.
VI. Adjournment & Next Meeting
Dave noted that the next meeting will be held Dec. 14 at 10:00 a.m.
15
Nov. 21 Small Group Responses
Question 1: What should the behavioral health system look like three years from now?
Timely access to care, staffed adequately
Quality measured with outcomes, overall program evaluation system
Continuum of care
Funding based on cost, standard for payments, payment for uninsured and underinsured
Standardization of assessment, treatment
Electronic health records (EHRs), shared information technology, information follows
the patient
Increased reimbursement for medical, transportation and mental health centers
Integration of rules and regulations, possible waivers
Case management system for follow-up
Comprehensive Coordinated care
Crisis assessment, urgent care psych
State thorough evaluation of new ideas and get more input from providers
Streamline record keeping, reviews
Better training in schools for social workers, etc.
Laws regarding transportation, also transportation to follow-up care
Education to primary care providers and community
Cost of medicine and open access to medical formularies
Collaborative approach with government, law enforcement, and others
Funding of all evidence-based practices, modify for rural
Salaries to attract
One stop shop for patients
Free standing specialty sites
More consistent regional approach, less local
Local flexibility
Less redundancy, more fluidity
More psychiatrist availability
Alternatives to hospitalizations, ED, crisis support outside of ED
Real time information on service availability, bed, etc.
Behavioral health home
Telehealth access using advanced practice nurses (APNs), more use of telehealth
Tort immunity for psychiatrists in community mental health centers
Expand Federally Qualified Health Centers (FQHCs)
Support for physicians, to handle more psych
Education of hospital workforce, how to deal
Patient navigators
Simplify telehealth rules for patients
Community based services
Integration of behavioral health and substance abuse systems and regulations
State and private payer not consistent and federal
Alternative sites for medical clearance

16
Medical care and behavioral health/substance abuse on same day
Early identification of need for services and intervention, prevention
Screening, Assessment, and Support Services (SASS)
Impact of the Adverse Childhood Experiences (ACE) and are there resources to help
Consolidation of resources
New role of health care providers
Risk based contract
Change of rules made by payment sources
Question 2: What would be the key components of the new behavioral health system?
Supportive housing, less residential for young and more crisis residential
Support for indigents
Planning and communication with all players, evidence-based treatments
Attracting younger workforce in rural areas
Education, full picture for students, part-time programs, grants or loan repayment
programs
Programs in rural areas for psych services for students
Reimbursement for those not licensed and LCPC billing
Internal accounting and billing changes
Integration include schools and Department of Corrections (DOC)
Prevention, early intervention/assessment, wellness
Communication/information exchange/EHRs/HIE: system and patient
Fiscal responsibility across all stakeholders, including patients, central pot of funds
System to prevent no shows
Technology for self-assessment, data across continuum
Transportation
Connection between hospital and community particularly for heavy users-care
coordination
Integration between medical and behavioral health/substance abuse
Community services, continuity of care
Case management at community level, pull resources around individuals, consumer
friendly
Telemedicine
School system, universities, student clinics, seniors
Tax for cigarette and alcohol
Ambulance
Laws: transportation
Full assessment at each provider
Set of evaluations
Care coordination per person, patient-centered, one stop integrated behavioral health
More psychiatrists, therapists, psych nurses, mid-level capacity, new workforce roles,
innovative staffing
Stabilization
Alternative options to ED on psych beds
Ease of access

17
Change in payment system from production based to patient-centered medical home
Medication must be accessible
Children should be included instead of adult driven
Resources to make it financially viable
Robust crisis system
Question 3: Are there immediate actions that could be taken to improve access to
behavioral health services in this region? If so, what are they?
Coordination, communication, networking, best practices, evidence-based care
Relaxation of some requirements, redundancy, less micro management of non-Medicaid
funding
Looking outside the box, finding other referral sources, other states even
Start in crisis intervention services
Urgent care for psych patients
Money to improve access, money in the right place
Continuous Quality Improvement (CQI)
Shared list of training resources (CPI) in region, shared staff, information.
Facilitate wrap around services, family
Identify a model of care
Care coordination release form
Sharing or pooling of resources, prevent loss of services
Wellness recovery action plan ( WRAP) services, prevention, screening
Stronger legislative voice
Strategic planning across region
Coordination of data regionally, decide on metrics
Influence client choice
Better follow-up after discharge
Track patients better
Robust crisis system-build rather than reduce
Training for law enforcement
Support groups for high ED users
One set of standardized paperwork across hospitals
Telepsych
HFS waiver

18
Illinois Behavioral Health Network Meeting – Region 5
January 5, 2012, 10:00 a.m. – 1:00 p.m.
Centralia Recreation Complex
115 E. Second Street, Centralia, IL 62801
Agenda
I. WELCOME ........................................................10:00 ........................ Kim Sanders
II. SUMMARY OF FIRST MEETING.................10:20 ...................... ..Kim Sanders
III. FOCUS ON PRIORITIES…………………….10:25 .................................. Groups
WORKFORCE:
What specific training is needed for existing workforce?
What are the new skills that are needed?
What are regulatory barriers to workforce utilization?
What are the specific training needs for dual diagnosis patients?
PREVENTION:
What are the current prevention services?
What new prevention services are needed?
DELIVERY SYSTEM:
How would you recommend we fill the gaps in the service delivery system?
Are there new models that would be effective in this region?
TRANSPORTATION:
Where are the transportation gaps (unfunded, Medicaid, others)?
What alternatives can you suggest in your community to provide
transportation?
PAYMENT DESIGN:
What services are not currently reimbursed that should be?
How should the payment system by redesigned to better meet the client’s needs?
IV. SMALL GROUP REPORTS ............................11:30 .............................. Everyone
V. SETTING PRIORITIES & NEXT STEPS ....12:15 ....................... Lori Williams
VI. ADJOURNMENT & NEXT MEETING ........1:00 .......................... Kim Sanders
19
Illinois Behavioral Health Network Meeting – Region 5
January 5, 2012
Centralia Recreation Complex, 115 E. Second Street, Centralia, IL 62801
Attendees
Kelly Medlin, WellSpring Resources
Lisa Tolbert, Delta Center
Gajif McNeill, IDHS/DASA
Mary McMahan, VCCS
Jim Novelli, DHS/DMH
Lisa Crouch, SMGSMG
Loretta Stevens, SMGSMG
Susan Engelhardt, Perry County Counseling
Dave Allen, Richland Memorial Hospital
Keith Suedmeyer, SSMHC
Virginia Telford, St. Mary’s Hospital
Wanda Scates, Egyptian Health Department
Angie Hampton, Egyptian Health
Department
Susan Grace, HMC
Bernstein, CHESI
Dan Boehmer, JCCS
Vince Ashley, Harrisburg Medical Center
Cheryl Colwell, Lawrence Co. Health Dept.
Robert J. Cole, Human Support Services
Lyn Gartke, Center for Senior Renewal
Mickey Finch, The Fellowship House
Bob Wesley, SIU School of Medicine
Jim Flynn, Heartland Regional
Melisa Adkins, Heartland Regional
Rachael Belford, Massac Memorial Hospital
Tom Barry, Ferrell Hospital
Denise Daum, Community Resource Center
Beverly Vokes, SIHF
Dana Shantel Taylor, FMH
Gary L. Buatte, Human Service Center
Kim Abell, Massac Memorial Hospital
Georgianne Broughton, Com. Res. Center
Donna Meyers, St. Elizabeth’s Hospital
Deborah Vogel, St. Elizabeth’s Hospital
Woody Thorne, Southern IL. Health Care
Chris Larrison, U of I
Larry Mizell, Family Counseling Center
Nancy Newby, Washington County Hospital
Sulbrena Day, Touchette Regional Hospital
Randy Dauby, Hamilton Memorial Hospital
Roger Hanna, IRC
Judy Wissel, Wabash County Health Dept.
Debby Page, The H Group
John Markley, The H Group
Mike McManus, Touchette Regional
Hospital
Amy Whipple, St Mary’s
Sharon Szatkowski, Southern IL HC Found.
Carole Hannan, Hardin Co. General
Hospital
Jennie Johnson, Jasper Co. Health
Department
Kim Sanders, SIU
Ruth Heitkamp, SIU
Lori Williams, IHA
Abby Radcliffe, IHA
Ann Guild, IHA
I. Welcome & Introductions
Kim Sanders called the meeting to order at 10:00 a.m. and those in attendance introduced
themselves. Kim reviewed the purpose of this series of three meetings being to outline a
plan for behavioral health services in the region and work with a state steering committee
20
to implement changes to the system. Kim outlined that in today’s meeting the group will
take the priority issues identified in the first meeting and drill down into the details in
each of the following areas: workforce, transportation, payment system redesign, service
delivery system, and prevention.
II. Regional Plan Discussion Groups
Participants were divided into groups to discuss questions in five categories:
1)Workforce; 2)Prevention; 3) Delivery System; 4)Transportation; and 5)Payment
Design. These priority issues were identified in the first meeting. The questions on these
topics will help identify provider needs in each of the areas.
III. Small Groups Reports
Kim Sanders led the small groups to report on their findings. The compiled information
from the break-out groups is included in the attached document.
IV. Next Steps
Information collected at the meeting will be used by IHA to develop a draft plan and
recommendation for a viable Behavioral Health System.
V. Adjournment & Next Meeting
IHA will communicate the next meeting date, time and place when scheduled.
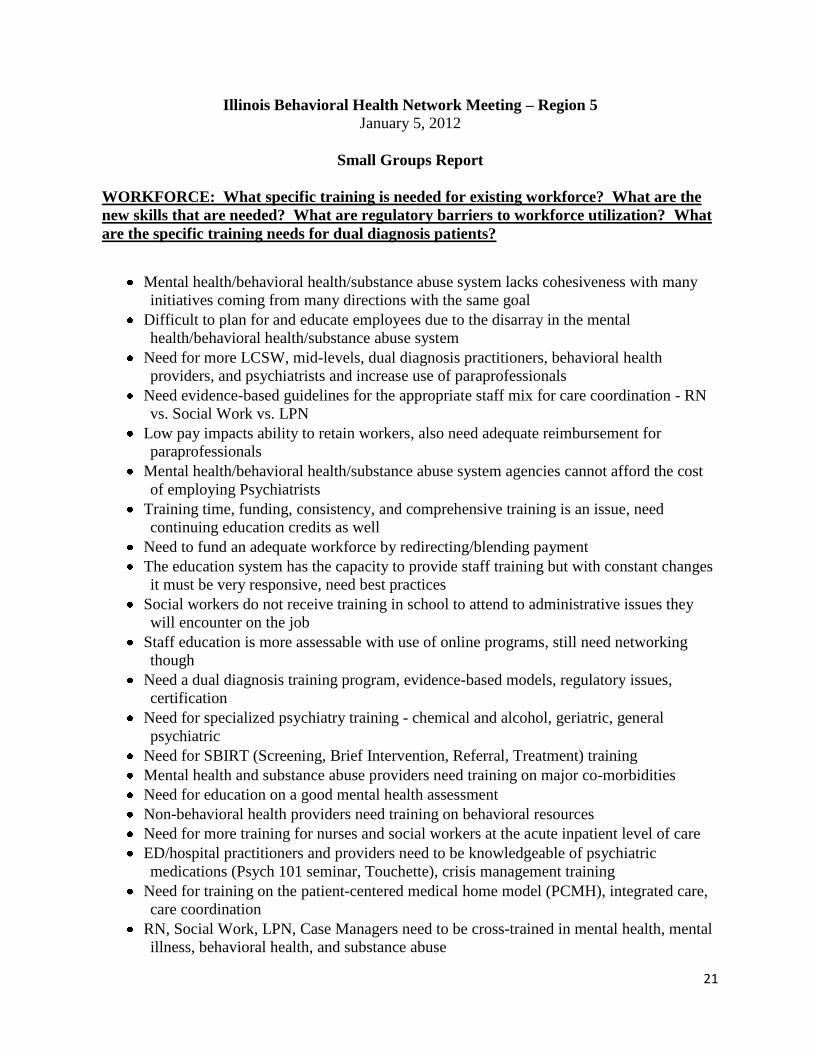
21
Illinois Behavioral Health Network Meeting – Region 5
January 5, 2012
Small Groups Report
WORKFORCE: What specific training is needed for existing workforce? What are the
new skills that are needed? What are regulatory barriers to workforce utilization? What
are the specific training needs for dual diagnosis patients?
Mental health/behavioral health/substance abuse system lacks cohesiveness with many
initiatives coming from many directions with the same goal
Difficult to plan for and educate employees due to the disarray in the mental
health/behavioral health/substance abuse system
Need for more LCSW, mid-levels, dual diagnosis practitioners, behavioral health
providers, and psychiatrists and increase use of paraprofessionals
Need evidence-based guidelines for the appropriate staff mix for care coordination - RN
vs. Social Work vs. LPN
Low pay impacts ability to retain workers, also need adequate reimbursement for
paraprofessionals
Mental health/behavioral health/substance abuse system agencies cannot afford the cost
of employing Psychiatrists
Training time, funding, consistency, and comprehensive training is an issue, need
continuing education credits as well
Need to fund an adequate workforce by redirecting/blending payment
The education system has the capacity to provide staff training but with constant changes
it must be very responsive, need best practices
Social workers do not receive training in school to attend to administrative issues they
will encounter on the job
Staff education is more assessable with use of online programs, still need networking
though
Need a dual diagnosis training program, evidence-based models, regulatory issues,
certification
Need for specialized psychiatry training - chemical and alcohol, geriatric, general
psychiatric
Need for SBIRT (Screening, Brief Intervention, Referral, Treatment) training
Mental health and substance abuse providers need training on major co-morbidities
Need for education on a good mental health assessment
Non-behavioral health providers need training on behavioral resources
Need for more training for nurses and social workers at the acute inpatient level of care
ED/hospital practitioners and providers need to be knowledgeable of psychiatric
medications (Psych 101 seminar, Touchette), crisis management training
Need for training on the patient-centered medical home model (PCMH), integrated care,
care coordination
RN, Social Work, LPN, Case Managers need to be cross-trained in mental health, mental
illness, behavioral health, and substance abuse

22
Behavioral health providers trained to team with health care providers
Need more assessment training for mid-level providers
Providers need education on roles and responsibilities, resources available, the referral
process, need for education on scope of practice/authority, system access , resident
patients, and outcome measures
Need for training on quality of life issues: housing, employment, nutrition, etc.
Need for telepsychology training, EHRs, HIE, and other data systems
Need education programs on drugs, including for law enforcement on psychiatric
medications
Need for law enforcement to be trained on mental health/mental illness/behavioral
health/substance abuse
Funding regulations must be changed to equate LCPC and LCSW and parity
Need to address scope of practice issues
Need for partnerships with SIU, U of I, or other universities for training/programs
Mid-level providers would benefit from more supervision from psychiatrists
Review mid-level regulations
Need recognition and services for domestic violence victims
PREVENTION: What are the current prevention services? What new prevention
services are needed?
Early intervention is needed for prevention, school/community partnerships important
Prevention currently provided by local mental health agencies, school and community-
based prevention, intensive outpatient programs, preventive medicine, public health
Private outreach programs are targeting prevention and working with communities
National Institute of Health (NIH) - child mental health prevention programs should
begin in the schools, need for more school based prevention program - project success
Primary care clinicians do not have time for prevention; are volunteers effective?
Current system focuses on episodic care not prevention, should also be for general
population and link to hospitals
Cycles of disparities (poverty/homelessness/low education level) limit implementation of
meaningful prevention, no mental health prevention, financial resources inadequate
SASS program cut
PCMH will strengthen prevention in primary care setting
Need for improved communication among health care providers - hospital/primary
care/community/schools for prevention
Hospitals are providing services to prevent readmissions, i.e. telephone calls
Utilize afterschool programs for prevention and DCFS parent and teen cafes
Competing needs inhibit effective preventive education in the schools
School counseling services need to be coordinated in new preventive system of care
focus, also school liability concerns limits referrals to mental health care
Use social media to promote prevention

23
Access to community mental health centers - past assessment to immediate services (four
to six-week program)
Need for more community follow-up preventive services, community awareness
Need for proactive case management, outpatient services
Need for post-partum prevention
Need links to alternative schools
Need to prevent patients from receiving drugs from multiple providers
Need to address over-the-counter designer drugs
DELIVERY SYSTEM: How would you recommend we fill the gaps in the service delivery
system? Are there new models that would be effective in this region?
Need to develop blended models for intensity of service delivery and a sustainable model
of care, regional administration of care coordination and payment design
Hospitals do not need to be the leaders for system redesign
Need community/agency support for new service delivery systems, break down silos
Need essential package of care services (housing excluded) - now directed by state vs.
federal
State needs to provide accurate, comprehensive cost/utilization data for planning delivery
system, assess bureaucratic inefficiencies in policy/procedure
Others groups must be brought into this discussion - law enforcement, FQHC, state
All entities in "new system" need to be healthy
Difficult to manage the utilization of available inpatient beds causing the supply not
meeting demand for inpatient beds, more inpatient beds in region
Models are available for alternatives to inpatient
Develop capacity for 23-48 hour hold/observation beds for patients in crisis, crisis center
Smaller hospitals must be compensated for providing the capacity for rapid access to care
for this population
Need holistic patient care: case mgmt., care coordination, timely access to behavioral
health/mental health services (esp. kids), primary care medical home, patient choice
Need for coordination among primary care and community providers
Integrate mental health within the health department
Integrate, co-locate, and change how mental health services are delivered/marketed
Need for accountable care organizations, care coordination, primary care medical home
Improved coordination with FQHC, community mental health centers and other
community primary care providers
Need to partner pharmacy and behavioral health professionals to manage dual diagnosis
patients.
Need for evaluations that align with outcomes
Explore Oklahoma, North Carolina, California, Kentucky, and Arizona telemedicine
programs
Implement new models - Recovery support model, shift of treatment, telepsych, case
management, PCMH, primary care/behavioral health integration, dental, and care
coordination

24
Explore Adams County model - groups going together to pay for services
Cherokee Health System in Knoxville, TN - model of care - system follows patient, not
funding streams, telepsych (and reimbursement), child and adolescent, assessment and
medication management
Outcome measures limit stays, resulting in too many short stays, patients discharged too
quickly, make time to get required follow-up
Disconnect between acute and community mental health/behavioral health/substance
abuse providers
Hospitals needing to provide "sitters" for acute patients
Lift Rule 132 DMH regulations - community support specialists
Need for address confidentiality laws to improve sharing of protected health information
Regulatory barriers with paperwork: private vs. public providers, assessment
requirements, H&P, state laws restricting sharing/access to mental health/behavioral
health/substance abuse information, federal regulations, accreditation process should
remove regulatory barriers, DMH - eligibility changes in mental health services,
duplicate paperwork
Need to allow hospitals to process involuntary patients
Working poor - need case management (IL Health Connect) and need to take
responsibility
Inmates released with no employment, housing, etc.; they need transition programs
Data: Population variance by provider type
TRANSPORTATION: Where are the transportation gaps (unfunded, Medicaid, others)?
What alternatives can you suggest in your community to provide transportation?
Lack of transportation providers; patients missing appointments and can’t apply for
entitlements
Transportation providers don’t want to accept Medicaid contracts; can’t build enough
volume to offer services at a fair price; want payment up front, and overcharge
Agencies looking for alternative providers - BART, sheriff department, churches, some
"pooling" funds
No payment for transit back to home
Medicaid does not reimburse for all patient transportation needs
Case managers are no longer reimbursed to provide patient's transportation
Lack of transportation prevents people from applying to entitlements
EMS won't transports patients with serious mental illness
Distance to available beds is lengthening
Burden is the paperwork and staff time to arrange transit
Regulations and liability for transportation services limits intake
Crisis - IPT works to state ops
Telemedicine would help with transportation issues
Jefferson County has a mobile detox program
Center for Rural Health and Social Service Development Rural Transportation Network
working on solutions

25
Use cell phones to help patients access transit
Needs: Case managers to assist mental health patients with transit arrangements
Need an 800 number to call and get transportation - Dial-a-ride, college
PAYMENT DESIGN: What services are not currently reimbursed that should be? How
should the payment system by redesigned to better meet the client’s needs?
Current system of reimbursement is dismantling the healthcare system, and state/grant
funding has eroded, and payment system is based on outdated models of care
Under current reimbursement system - unfunded or inadequate funding: preventive
services, medication assisted treatment, telemedicine, care management/coordination,
transportation, linkages to services, travel for case managers, consultative services,
administrative time for providing medical cards, utilization management, beds
Unable to be reimbursed for two provider visits in the same day; will only be reimbursed
for one visit and no reimbursement for mid-levels, just physicians
Does current funding reimburse for providing care in a "crisis center"?
Currently hospitals are absorbing the costs for providing direct service to the mental
illness/substance abuse population - i.e. care coordinator in emergency department,
transportation costs
Reality - reimbursement drives services offered
Providers unwilling to risk liability and use lower level of care
Hospitals/clinics etc. are hesitant to take financial risk for providing services to the
mental health/mental illness/substance abuse patient population
No health care provider will voluntarily join into an Accountable Care Organization
Utilize cost-based reimbursement
Load capacity
Need to move away from a "fee for service" model
Waivers are needed to adopt innovative models of care/delivery systems
Services bundled for reimbursement, care coordination fee is needed in addition to fee-
for-service, need for reimbursement to follow patients through new system of care
Must include reimbursement for transportation and various settings and care
coordination/case management
Reimbursement must be coordinated among organizations, allow providers to allocate
money to provide services by the patient’s needs
Provide reimbursement for quality, need for worker’s compensation
Funding differences need to be resolved – funding for FQHC, hospitals, providers needs
to look alike and community health center reimbursement must be on parity with FQHC/
Rural Health Clinics
Rule-16.6% of salary for benefits (limit) state dept. law (early 80's)
High users of mental health services are high cost; Uninsured need money to purchase
medications; as money for mental health declines, recidivism rates increase
Geriatric IOP - Senior Care Model, Medicare Part B, insurance, strictly medical fall
through cracks
26
Illinois Behavioral Health Network Meeting – Region 5
January 31, 2012, 10:00 a.m. – 1:00 p.m.
Centralia Recreation Complex
115 E. Second Street, Centralia, IL 62801
Agenda
I. WELCOME ........................................................10:00 ........................ Kim Sanders
II. SUMMARY OF SECOND MEETING ............10:20 ...................... ..Kim Sanders
III. REVIEW OF PLAN/PRIORITIES………… ..10:25 ............................ Ann Guild
IV. REGION INFORMATION...............................11:30 .............................. Everyone
V. NEXT STEPS ....................................................12:15 ............................ Ann Guild
VI. ADJOURNMENT ..............................................1:00 .......................... Kim Sanders

27
Illinois Behavioral Health Network Meeting – Region 5
January 31, 2012
Centralia Recreation Complex
115 E. Second Street, Centralia, IL 62801
Kevin Hutchison, St. Clair Public Health
Dana Rosenzweig, St. Clair County MHB
Orville Mercer, Chestnut Health System
Georgianne Broughton, Comm. Resource Center
Beverly Vokes, SIHF
Judy Wissel, Wabash Co. Health Dept.
Denise Daum, Community Resource Center
Ruth Heitkamp, SIU-Center for Rural Health
Kim Sanders, SIU-Center for Rural Health
Joann Emge, Sparta Community Hospital
Lori Clinton, Sparta Community Hospital
Sharon Szatkowski, SIHF
Angie Hampton, EHD
Loretta Stevens, SMGSMG
Katheryn McWhirter, WGH
Tamara Gould, Wabash General Hospital
Lyn Gartke, Center for Senior Renewal
Carole Hannan, Hardin County General Hospital
Bob Layman, Farm Resource Center
Ann Tyree, WellSpring Resources
Lorianne Schmider, Jeff. Co. Comp. Services
Lisa Tolbert, Delta Center
Julia Holland, Salem Counseling Center
John Cooley, Touchette Regional Hospital
Michele Sturm, Gateway Regional
Dana Shantel Taylor, Fairfield Memorial Hospital
Keith Suedemyer, St. Mary’s Good Samaritan
Stacia McGuire, EHD
Fred Bernstein, CHESI
John Markley, The H Group
Mickey Finch, The Fellowship House
Christopher Larrison, U of I
Gary L. Buatte, Human Service Center
Robert J. Cole, Human Support Services
Diane Duft, Bond Co. Health
Deborah Pape, The H Group
Patsy Jensen, Shawnee Health
Susan Grace, HMC
Jim Novelli, DMH
Vince Ashley, Harrisburg Medical Center
Woody Thorne, Southern Illinois Healthcare
Larry Mizell, Family Counseling Center
Gajef McNeill, IDHS/DASA
Rachael Belford, Massac Memorial Hospital
Kim Abell, Massac Memorial Hospital
Jeannie Johnson, Jasper Health
Ann Guild, IHA
Abby Radcliffe, IHA
I. Welcome & Introductions
Kim Sanders called the meeting to order at 10:00 a.m. and those in attendance introduced
themselves.
II. Summary of Second Meeting
Kim gave an overview of the last meeting. She thanked the group and the state for
participating in these meetings. The purpose of these three meetings is to outline a plan
for behavioral health services in this region. The goal is to develop a plan to improve
access to behavioral health services in the region and work with a state steering
committee to implement changes to the system.
28
III. Review of Plan/Priorities
Ann Guild noted that today’s meeting will take the priority issues that were identified in
the first two meetings and begin to craft recommendations to be part of this region’s plan.
Comments will be recorded and added to the plan. Ann went through each section of the
draft plan and the group made recommendations for any changes.
IV. Region Information
Some region specific data was collected. This was included in the packets and any
feedback on additional data needed would be appreciated.
V. Next Steps
The information collected at the meeting will be assembled by IHA. The updated draft
plan will be sent to the group for any other changes. This plan will then be submitted to
the State Steering Committee when they begin to meet.
VI. Adjournment
Kim adjourned the meeting at 1:00 p.m.

29
Appendix
Regional Integrated Behavioral Health Networks Act
Public Act 097-0381
An Act concerning health.
Be it enacted by the People of the State of Illinois, represented in the General Assembly:
Section 1. Short title.
This Act may be cited as the Regional Integrated Behavioral Health Networks Act.
Section 5. Legislative Findings.
The General Assembly recognizes that an estimated 25% of Illinoisans aged 18 years or older
have experienced a mental or substance use disorder, an estimated 700,000 Illinois adults aged
18 years or older have a serious mental illness and an estimated 240,000 Illinois children and
adolescents have a serious emotional disturbance. And on any given day, many go without
treatment because it is not available or accessible. Recent federal and State fiscal crises have
exacerbated an already deteriorating mental health and substance abuse (behavioral health)
treatment system that is characterized by fragmentation, geographic disparities, inadequate
funding, psychiatric and other mental health workforce shortages, lack of transportation, and
overuse of acute and emergency care by persons in crisis who are unable to obtain treatment
from less intensive community alternatives. The failure to treat mental and substance use
illnesses has human and financial consequences: human suffering and loss of function; increased
use of hospital emergency departments; increased use of all medical services; increased
unemployment, and lack of productivity; lack of meaningful engagement in family and
communities; school failure; homelessness; incarceration; and, in some instances, death. The
citizens of Illinois with mental and substance use illnesses need an organized and integrated
system of care that recognizes regional differences and is able to deliver the right care to the
right person at the right time.
Section 10. Purpose.
The purpose of this Act is to require the Department of Human Services to facilitate the creation
of Regional Integrated Behavioral Health Networks (hereinafter "Networks") for the purpose of
ensuring and improving access to appropriate mental health and substance abuse (hereinafter
"behavioral health") services throughout Illinois by providing a platform for the organization of
all relevant health, mental health, substance abuse, and other community entities, and by
providing a mechanism to use and channel financial and other resources efficiently and
effectively. Networks may be located in each of the Department of Human Services geographic
regions.
Section 15. Goals.
Goals shall include, but not be limited to, the following: enabling persons with mental and
substance use illnesses to access clinically appropriate, evidence-based services, regardless of
where they reside in the State and particularly in rural areas; improving access to mental health
and substance abuse services throughout Illinois, but especially in rural Illinois communities, by

30
fostering innovative financing and collaboration among a variety of health, behavioral health,
social service, and other community entities and by supporting the development of regional-
specific planning and strategies; facilitating the integration of behavioral health services with
primary and other medical services, advancing opportunities under federal health reform
initiatives; ensuring actual or technologically-assisted access to the entire continuum of
integrated care, including the provision of services in the areas of prevention, consumer or
patient assessment and diagnosis, psychiatric care, case coordination, crisis and emergency care,
acute inpatient and outpatient treatment in private hospitals and from other community providers,
support services, and community residential settings; identifying funding for persons who do not
have insurance and do not qualify for State and federal healthcare payment programs such as
Medicaid or Medicare; and improving access to transportation in rural areas.
Section 20. Steering Committee and Networks.
(a) To achieve these goals, the Department of Human Services shall convene a Regional
Integrated Behavioral Health Networks Steering Committee (hereinafter "Steering Committee")
comprised of State agencies involved in the provision, regulation, or financing of health, mental
health, substance abuse, rehabilitation, and other services. These include, but shall not be limited
to, the following agencies:
(1) The Department of Healthcare and Family Services.
(2) The Department of Human Services and its Divisions of Mental Illness and
Alcoholism and Substance Abuse Services.
(3) The Department of Public Health, including its Center for Rural Health.
The Steering Committee shall include a representative from each Network. The agencies of the
Steering Committee are directed to work collaboratively to provide consultation, advice, and
leadership to the Networks in facilitating communication within and across multiple agencies
and in removing regulatory barriers that may prevent Networks from accomplishing the goals.
The Steering Committee collectively or through one of its member Agencies shall also provide
technical assistance to the Networks.
(b) There also shall be convened Networks in each of the Department of Human Services'
regions comprised of representatives of community stakeholders represented in the Network,
including when available, but not limited to, relevant trade and professional associations
representing hospitals, community providers, public health care, hospice care, long term care,
law enforcement, emergency medical service, physicians trained in psychiatry; an organization
that advocates on behalf of federally qualified health centers, an organization that advocates on
behalf of persons suffering with mental illness and substance abuse disorders, an organization
that advocates on behalf of persons with disabilities, an organization that advocates on behalf of
persons who live in rural areas, an organization that advocates on behalf of persons who live in
medically underserved areas; and others designated by the Steering Committee or the Networks.
A member from each Network may choose a representative who may serve on the Steering
Committee.
Section 25. Development of Network Plans.
Each Network shall develop a plan for its respective region that addresses the following:

31
(a) Inventory of all mental health and substance abuse treatment services, primary health
care facilities and services, private hospitals, State-operated psychiatric hospitals, long
term care facilities, social services, transportation services, and any services available to
serve persons with mental and substance use illnesses.
(b) Identification of unmet community needs, including, but not limited to, the following:
(1) Waiting lists in community mental health and substance abuse services.
(2) Hospital emergency department use by persons with mental and substance use
illnesses, including volume, length of stay, and challenges associated with
obtaining psychiatric assessment.
(3) Difficulty obtaining admission to inpatient facilities, and reasons therefore.
(4) Availability of primary care providers in the community, including Federally
Qualified Health Centers and Rural Health Centers.
(5) Availability of psychiatrists and mental health professionals.
(6) Transportation issues.
(7) Other.
(c) Identification of opportunities to improve access to mental and substance abuse
services through the integration of specialty behavioral health services with primary care,
including, but not limited to, the following:
(1) Availability of Federally Qualified Health Centers in community with mental
health staff.
(2) Development of accountable care organizations or other primary care entities.
(3) Availability of acute care hospitals with specialized psychiatric capacity.
(4) Community providers with an interest in collaborating with acute care
providers.
(d) Development of a plan to address community needs, including a specific timeline for
implementation of specific objectives and establishment of evaluation measures. The
comprehensive plan should include the complete continuum of behavioral health
services, including, but not limited to, the following:
(1) Prevention.
(2) Client assessment and diagnosis.
(3) An array of outpatient behavioral health services.
(4) Case coordination.
(5) Crisis and emergency services.
(6) Treatment, including inpatient psychiatric services in public and private
hospitals.
(7) Long term care facilities.
(8) Community residential alternatives to institutional settings.
(9) Primary care services.
Section 30. Timeline.
The Network plans shall be prepared within 6 months of establishment of the Network. The
Steering Committee shall assist the Networks in the development of plans by providing technical
expertise and in facilitating funding support and opportunities for the development of services
identified under each of the plans.

32
Section 35. Report to Governor and General Assembly.
The Steering Committee shall report to the Governor and General Assembly the status of each
regional plan, including the recommendations of the Network Councils to accomplish their
goals and improve access to behavioral health services. The report shall also contain
performance measures, including changes to the behavioral health services capacity in the
region; any waiting lists for community services; volume and wait times in hospital emergency
departments for access to behavioral health services; development of primary care-behavioral
health partnerships or barriers to their formation; and funding challenges and opportunities. This
report shall be submitted on an annual basis.
Section 99. Effective date.
This Act takes effect January 1, 2012.
HB2982 Enrolled LRB097 10532 KTG 51304 b
Public Act 097-0381

33
Regional Behavioral Health Network – Region 5
Provider Questionnaire (14 Completed)
1. Wait Times
Over the past year, has your facility experienced longer wait times for patients to
receive services due to transportation, available placements, etc.? If so, what
primary factors contribute to the delays?
Available placements
No. Access is improving, as an FQHC, we are in
No, not at our facility
On a scale of 1-5 how big a problem are wait times for your facility? (1= very
important – 5 = not important at all)
#5 - 1
#4 - 4
#3 - 2
#2 - 2
#1 - 5
Have you documented these delays?
NO - 4
YES - 6
N/A - 2
If so, what data do you have?
Increased number of psych patients receiving care in ED, primary care,
etc. More paying for services to assess and place patients in psych
inpatient settings.
They are documented in the ER log book (length of stay), patient charts
The ECHO group, clinician’s desktop, provides a waitlist broken out by
services needed, wait time, location, etc. We have gone to a central intake
service delivery system that has reduced wait time, but the list continues to
grow due to an inability to expand capacity for financial and other logistic
reasons.
Our problem is for psychiatry. Counseling and assessments in mental
health or substance abuse are not a problem—less than one week wait
Crisis notes, referrals
2. Security Concerns
Have you had to utilize security to maintain patients who are at your facility
waiting for a transfer?
NO - 2
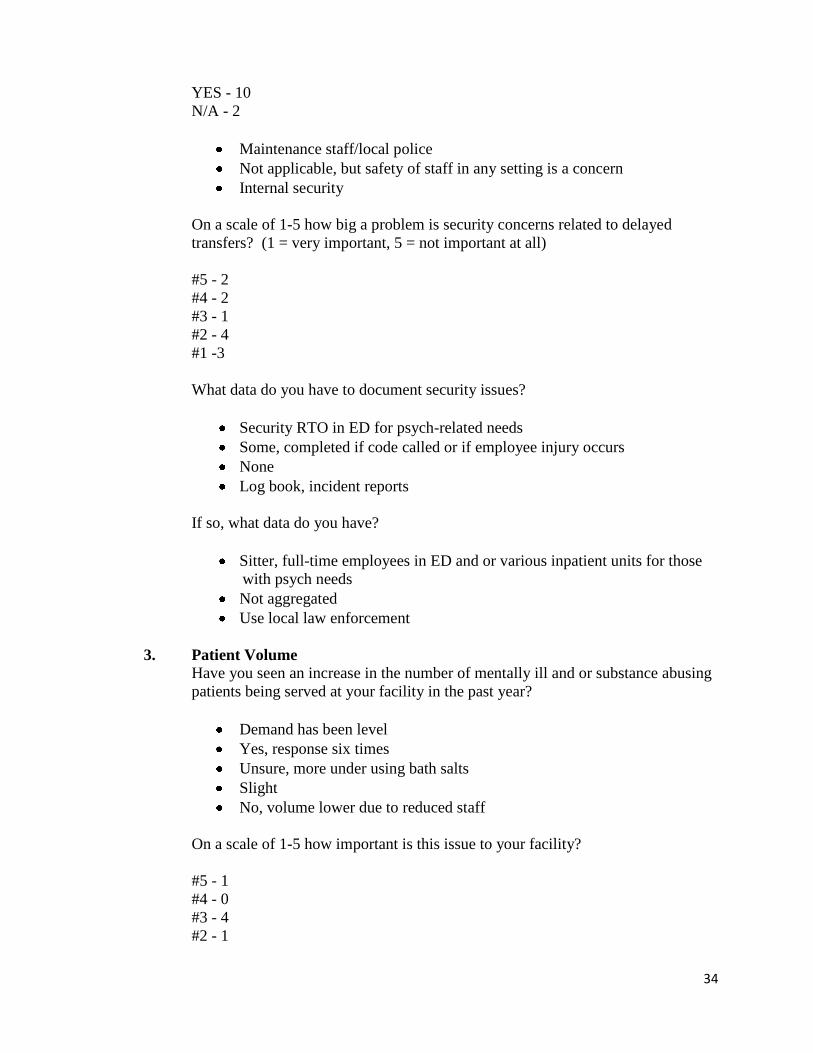
34
YES - 10
N/A - 2
Maintenance staff/local police
Not applicable, but safety of staff in any setting is a concern
Internal security
On a scale of 1-5 how big a problem is security concerns related to delayed
transfers? (1 = very important, 5 = not important at all)
#5 - 2
#4 - 2
#3 - 1
#2 - 4
#1 -3
What data do you have to document security issues?
Security RTO in ED for psych-related needs
Some, completed if code called or if employee injury occurs
None
Log book, incident reports
If so, what data do you have?
Sitter, full-time employees in ED and or various inpatient units for those
with psych needs
Not aggregated
Use local law enforcement
3. Patient Volume
Have you seen an increase in the number of mentally ill and or substance abusing
patients being served at your facility in the past year?
Demand has been level
Yes, response six times
Unsure, more under using bath salts
Slight
No, volume lower due to reduced staff
On a scale of 1-5 how important is this issue to your facility?
#5 - 1
#4 - 0
#3 - 4
#2 - 1
35
#1 - 5
What data do you have available to demonstrate these increases?
State of number of patients presenting with mental health diagnosis
Significant data with ongoing dashboard to assess the need being
established and ER logs, intake and census reports, dual diagnosis tracking
Wait list
Encounter data, not sure it is correct, seems under reported. I am willing to
share this data
If there had not been such severe reduction in non-Medicaid funding, we
would have definitely seen an increase in patients served
Percent of new patients is up
Not sure how to assess it
None
4. Transportation
Is transportation to appropriate care for unfunded patients a problem in your area?
NO - 1
YES - 6
On a scale of 1-5 how big a problem do you believe this is?
#5 - 2
#4 - 2
#3 - 2
#2 - 4
#1 - 4
What data is available to document this problem?
No shows
Number of transfers related to transportation, cost of transportation to
hospitals for voluntary or involuntary psych admits
Social service/crisis staffing notes calls to public transit for after-hours
transportation is unavailable
None, starting to collect, very limited
Non-reimbursed ambulance transports

36
5. Admissions
Over the past year have you had to admit more patients with mental illness or
substance abuse problems to non-behavior health units in your hospital because
you could not locate appropriate care elsewhere either inside or outside your
facility?
YES - 6
NO - 1
N/A - 5
Not a big problem. Admit because not medically stable. We leave them in the
emergency department while waiting for transfer.
On a scale of 1-5 how big a problem do you believe this is?
#5 - 0
#4 - 2
#3 - 3
#2 - 2
#1 - 1
What data do you have available to document this issue?
Patient encounters, length of stay, admission records, coding
documentation
We do assist individuals who need to be hospitalized. This volume has
been stable
6. Please add any additional issues or trends experienced at your facility over the
past year and what data you have to document the issue.
Lots of persons unable to get care/needs do to no funding. Referral
systems overwhelmed
No longer accept patients with no pay source, no documentation
Outpatient services are growing rapidly, more medically indigent
Medicaid reimbursement for two providers in the same day, medical and
psychiatric
As an FQHC, need to be able to bill for family practice MD/psychiatrist
same day
Patients come to the ED because they can’t afford medication, can’t find
anyone to prescribe psych medication and lack of care management. Also
lack data
Liability issue related to lack of ability to place individuals and then being
informed by mental health that it is permissible to discharge them home
Need to address co-morbidities of those with psych and medical needs
Timelines of response of mental health providers.
37
7. Would you be interested in continuing to dialogue with other behavioral health
providers in your region through meetings, trainings and workshops?
YES - 11
Maybe - 1
Yes, from a community mental health center perspective
We would be happy to assist and convene parties to seek solutions
8. Would you be interested in working with other providers in the region on
common network issues such as transportation, regulatory barriers and other
system design issues?
YES - 8
Please indicate which issues would be helpful to you.
Hospital ERs understanding how to treat mental illness or substance abuse
All
Patient care and coordination
System design and transportation
Regulatory, legislative
9. Any other items you would like to share about this planning process or materials
that are related to this effort?
In our situation, the issue is not that the patient is in the ER or that crisis
counselors are not available because this works, but that placing patients
in appropriate facilities is very difficult and takes days sometimes.
Share successes being implemented within the region

38
Region 5 Contact List
Organization Address Address 2 City & State Zip Contact Email
AAA DUI Services,
Inc.
828 Klein Ave. Edwardsville,
IL
62025 Linda Khan [email protected]
ABC DUI Services 1437 W. Whittaker Salem, IL 62881 Alta M. Allen [email protected]
Accurate Evaluations 951 Fairfax St. Carlyle, IL 62231 Jessica Daab [email protected]
Adapt 727 N. 17th St. Belleville, IL 62226 Cindy Janicak
Alcoholic
Rehabilitation
Community Home
1313 21st St. Granite City, IL 62040 Cary Green [email protected]
Alton Memorial
Hospital
One Memorial Drive Alton, IL 62002-
6755
David Braasch [email protected]
Anderson Hospital 6800 State Route
#162
Maryville, IL 62062-
1000
Keith Page, FACHE [email protected]
Association of
Community Mental
Health Authorities of
IL
P.O. Box
935
Aurora, IL 60507 Maureen Mulhall [email protected]
Association of
Community Mental
Health Authorities of
IL
P.O. Box
935
Aurora, IL 60507 Phyllis Russell [email protected]
Behavioral Health
Alternatives
337 E. Ferguson Ave. Wood River, IL 62095
Bond County Health
Dept.
1520 S. Fourth St. Greenville, IL 62246 Maxine Barth, RN,
MSN
Bond County Health
Dept.
1520 S. Fourth St. Greenville, IL 62246 Diane Duft
Call For Help, Inc. 9400 Lebanon Road Edgemont, IL 62203 Cheryl Compton

39
Carbondale DUI and
Counseling Associates
2015 W. Main Carbondale, IL 62901 Colleen Anotnacci [email protected]
CEC/CIVIGENICS,
Inc.
3300 Honeybend
Ave.
Litchfield, IL 62056 Steven Bryant [email protected]
Center for Senior
Renewal
Lyn Gartke [email protected]
Changing Lives
Counseling Center, Inc.
307 Henry St. Alton, IL 62002 Ted Williams
Chesi Cedar Court
Clinic/Cedar Court
Specialty Clinic
1250 Cedar Court Carbondale, IL 62901-
5334
Fred Bernstein [email protected]
Chestnut Health
Systems
50 Northgate
Industrial Drive
Granite City, IL 62040 Russell J. Hagen [email protected]
Chestnut Health
Systems
50 Northgate
Industrial Drive
Granite City, IL 62040 Orville Mercer [email protected]
Chestnut Health
Systems
50 Northgate
Industrial Drive
Granite City, IL 62040 Dietra Kulicke [email protected]
Chestnut Health
Systems
50 Northgate
Industrial Drive
Granite City, IL 62040 Amy Gibbar [email protected]
Chestnut Health
Systems
50 Northgate
Industrial Drive
Granite City, IL 62040 Joan Hartman [email protected]
Children's Center for
Behavioral
Development
353 N. 88th St. Centreville, IL 62203
Choate Mental Health
& Dev Center
1000 N. Main St. Anna, IL 62906 Jim Novelli [email protected]
Christopher Rural
Health Planning
Corporation
201 Bailey Lane Benton, IL 62812
Christopher Rural
Health Planning
Corporation
4241 St. Highway 14
W.
Christopher, IL 62822

40
Christopher Rural
Health Planning
Corporation
27 Circle St. Zeigler, IL 62999
Christopher Rural
Health Planning
Corporation
Cisne, IL 62823
Christopher Rural
Health Planning
Corporation
201 E. North Ave. Flora, IL 62839
Christopher Rural
Health Planning
Corporation
3303 Logan Drive Herrin, IL 62948
Christopher Rural
Health Planning
Corporation
115 E. Franklin St. Sesser, IL 62884
Christopher Rural
Health Planning
Corporation
607 Fourth St/ Eldorado, IL 62930
Christopher Rural
Health Planning
Corporation
9525 Gold Hill Road Shawneetown,
IL
62984
Christopher Rural
Health Planning
Corporation
119 Gas Plant Road DuQuoin, IL 62832
Christopher Rural
Health Planning
Corporation
McLeansboro,
IL
62859
Christopher Rural
Health Planning
Corporation
300 S. Main Royalton, IL 62983
Christopher Rural
Health Planning
Corporation
2920 Veterans
Memorial Drive
Mount Vernon,
IL
62864

41
Christopher Rural
Health Planning
Corporation
14410 Route 37 Johnston City,
IL
62951
Clay County
Counseling Services
125 Broadway St. Louisville, IL 62858 Cara Rinehart [email protected]
Clay County Health
Department
601 E. 12th St. Flora, IL 62839
Clay County Hospital 911 Stacy Burk Drive P.O. Box
280
Flora, IL 62839-
0280
Robert Sellers [email protected]
Clinton County Health
Department
930-A Fairfax St. Carlyle, IL 62231
Community Behavioral
Healthcare Association
Sheryl Turpin [email protected]
Community Health &
Emergency Services,
Inc.
13245 Kessler Road Cairo, IL 62914-
3101
Frederick L. Bernstein [email protected]
Community Health &
Emergency Services,
Inc.
Elizabethtown,
IL
62931
Community Health &
Emergency Services,
Inc.
Pulaski, IL 62976
Community Health &
Emergency Services,
Inc.
217 S. Adams St. Golconda, IL 62938
Community Health &
Emergency Services,
Inc.
290 Railroad St. Tamms, IL 62988
Community Health &
Emergency Services,
Inc.
226 Main St. Rosiclare, IL 62982

42
Community Health &
Emergency Services,
Inc.
1340 Cedar Court Carbondale, IL 62901
Community Health &
Emergency Services,
Inc.
1250 Cedar Court Carbondale, IL 62901
Community Health &
Emergency Services,
Inc.
205 N. Main St. Harrisburg, IL 62946
Community Health &
Emergency Services,
Inc.
1400 W. Main Carmi, IL 62821
Community Resource
Center, Inc.
101 S. Locust Centralia, IL 62801 Denise Daum [email protected]
Community Resource
Center, Inc.
101 S. Locust Centralia, IL 62801 Georgianne
Broughton
Comprehensive
Behavioral Health
Center of St. Clair
County, Inc.
505 S. Eighth St. East St. Louis,
IL
62201 Marsha Johnson [email protected]
Crawford County
Health Department
202 N. Bline Blvd. Robinson, IL 62454
Crawford Memorial
Hospital
1000 N. Allen St. Robinson, IL 62454-
1114
Don Annis [email protected]
Crossroads Community
Hospital
#8 Doctors Park
Road
Mount Vernon,
IL
62864-
6224
M. Edward
Cunningham
Delta Center 1400 Commercial
Ave.
Cairo, IL 62914 Lisa Tolbert [email protected]
Delta Center 1400 Commercial
Ave.
Cairo, IL 62914 Kate Mays [email protected]
Delta Center 1400 Commercial
Ave.
Cairo, IL 62914 Wendy Ice [email protected]

43
Derouse Counseling &
DUI Services
100 W. Main St. Belleville, IL 62220 George Derousse [email protected]
om
DHS/DASA Gajef McNeill [email protected]
DHS/DMH Jim Novelli [email protected]
DHS/DMH Art Zaitz [email protected]
Egyptian Public &
Mental Health Dept.
1412 US 45 N. Eldorado, IL 62930 Angie Hamilton [email protected]
Egyptian Public &
Mental Health Dept.
1412 US 45 N. Eldorado, IL 62930 Stacia McGuire [email protected]
Egyptian Public &
Mental Health Dept.
1412 US 45 N. Eldorado, IL 62930 Wanda Scates [email protected]
Fairfield Memorial
Hospital
303 NW Eleventh St. Fairfield, IL 62837-
1298
Katherine Bunting [email protected]
Fairfield Memorial
Hospital
Dana Shantel Taylor [email protected]
Family Counseling
Center, Inc.
Washington &
Market Sts.
P.O. Box
759
Golconda, IL 62939 Larry W. Mizell [email protected]
Farm Resource Center 226 Main St. Mound City, IL 62963 Roger Hannan [email protected]
Farm Resource Center 226 Main St. Mound City, IL 62963 Bob Layman [email protected]
Fayette County Health
Department
416 W. Edwards Vandalia, IL 62471
Fayette County
Hospital
650 W. Taylor St. Vandalia, IL 62471-
1227
Lyn Gartke [email protected]
Fayette County
Hospital
650 W. Taylor St. Vandalia, IL 62471-
1227
Greg Starnes [email protected]
Ferrell Hospital 1201 Pine St. Eldorado, IL 62930-
1634
Mary Ellen Turner-
Groves
Ferrell Hospital 1201 Pine St. Eldorado, IL 62930-
1634
Thomas F. Barry [email protected]
First Choice DUI
Services & Evaluations
219 S. Illinois St. Belleville, IL 6220 Kevan Caliper [email protected]
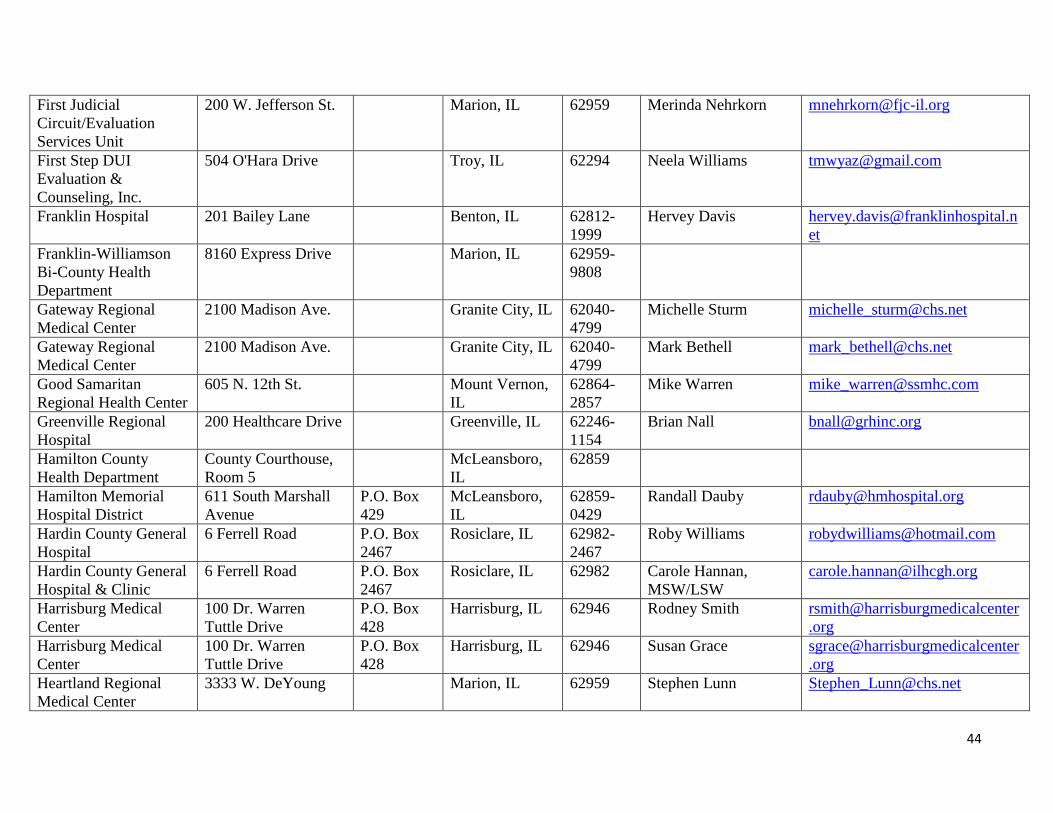
44
First Judicial
Circuit/Evaluation
Services Unit
200 W. Jefferson St. Marion, IL 62959 Merinda Nehrkorn [email protected]
First Step DUI
Evaluation &
Counseling, Inc.
504 O'Hara Drive Troy, IL 62294 Neela Williams [email protected]
Franklin Hospital 201 Bailey Lane Benton, IL 62812-
1999
Hervey Davis [email protected]
et
Franklin-Williamson
Bi-County Health
Department
8160 Express Drive Marion, IL 62959-
9808
Gateway Regional
Medical Center
2100 Madison Ave. Granite City, IL 62040-
4799
Michelle Sturm [email protected]
Gateway Regional
Medical Center
2100 Madison Ave. Granite City, IL 62040-
4799
Mark Bethell [email protected]
Good Samaritan
Regional Health Center
605 N. 12th St. Mount Vernon,
IL
62864-
2857
Mike Warren [email protected]
Greenville Regional
Hospital
200 Healthcare Drive Greenville, IL 62246-
1154
Brian Nall [email protected]
Hamilton County
Health Department
County Courthouse,
Room 5
McLeansboro,
IL
62859
Hamilton Memorial
Hospital District
611 South Marshall
Avenue
P.O. Box
429
McLeansboro,
IL
62859-
0429
Randall Dauby [email protected]
Hardin County General
Hospital
6 Ferrell Road P.O. Box
2467
Rosiclare, IL 62982-
2467
Roby Williams [email protected]
Hardin County General
Hospital & Clinic
6 Ferrell Road P.O. Box
2467
Rosiclare, IL 62982 Carole Hannan,
MSW/LSW
Harrisburg Medical
Center
100 Dr. Warren
Tuttle Drive
P.O. Box
428
Harrisburg, IL 62946 Rodney Smith rsmith@harrisburgmedicalcenter
.org
Harrisburg Medical
Center
100 Dr. Warren
Tuttle Drive
P.O. Box
428
Harrisburg, IL 62946 Susan Grace sgrace@harrisburgmedicalcenter
.org
Heartland Regional
Medical Center
3333 W. DeYoung Marion, IL 62959 Stephen Lunn [email protected]

45
Heartland Regional
Medical Center
3333 W. DeYoung Marion, IL Jim Flynn [email protected]
Heartland Regional
Medical Center
3333 W. DeYoung Marion, IL Melisa Adkins [email protected]
Helm DUI Services 716 School St. Vandalia, IL 62471 Brenda Duff [email protected]
Herrin Hospital 201 S. 14th St. Herrin, IL 62948-
3631
Terence Farrell,
FACHE
Holbrook &
Associates, LLC
6001 Old Collinsville
Road Ste. 4b
Fairview
Heights, IL
62208-
2937
Susan Holbrook [email protected]
Human Services Center 10257 State Route 3 Red Bud, IL 62278 Gary L. Buatte [email protected]
m
Human Support
Services
988 N. Illinois Route
3
P.O. Box
146
Waterloo, IL 62298 Robert Cole [email protected]
Illinois Association of
Rehab Facilities
206 S. Sixth St. Springfield, IL 62701 Janet Stover [email protected]
Illinois Association of
Rehab Facilities
206 S. Sixth St. Springfield, IL 62701 Josh Evans [email protected]
Intensive Outpatient
Care, Inc.
2 Club Centre Court Edwardsville,
IL
62025 Jennifer Manning [email protected]
Jackson County Health
Department
415 Health
Department Road
P.O. Box
307
Murphysboro,
IL
62966
Jasper County Health
Dept.
106 E Edwards Newton, IL 62448 Debbie Clark, B.S. [email protected]
Jasper County Health
Dept.
106 E Edwards Newton, IL 62448 Jeannie Johnson [email protected]
Jefferson County
Comprehensive Svcs.,
Inc.
Route 37 N. P.O. Box
428
Mt. Vernon, IL 62864 Lori Schmider [email protected]
Jefferson County
Comprehensive Svcs.,
Inc.
Route 37 N. P.O. Box
428
Mt. Vernon, IL 62864 Dan Boehmer
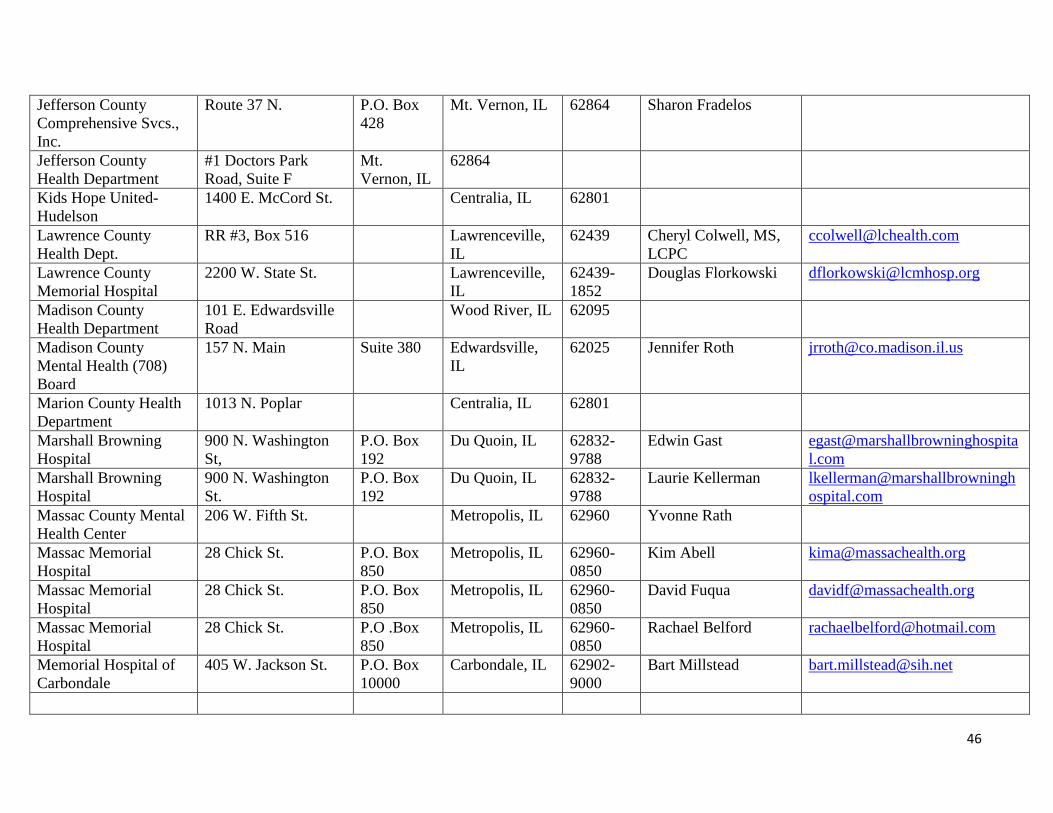
46
Jefferson County
Comprehensive Svcs.,
Inc.
Route 37 N. P.O. Box
428
Mt. Vernon, IL 62864 Sharon Fradelos
Jefferson County
Health Department
#1 Doctors Park
Road, Suite F
Mt.
Vernon, IL
62864
Kids Hope United-
Hudelson
1400 E. McCord St. Centralia, IL 62801
Lawrence County
Health Dept.
RR #3, Box 516 Lawrenceville,
IL
62439 Cheryl Colwell, MS,
LCPC
Lawrence County
Memorial Hospital
2200 W. State St. Lawrenceville,
IL
62439-
1852
Douglas Florkowski [email protected]
Madison County
Health Department
101 E. Edwardsville
Road
Wood River, IL 62095
Madison County
Mental Health (708)
Board
157 N. Main Suite 380 Edwardsville,
IL
62025 Jennifer Roth [email protected]
Marion County Health
Department
1013 N. Poplar Centralia, IL 62801
Marshall Browning
Hospital
900 N. Washington
St,
P.O. Box
192
Du Quoin, IL 62832-
9788
Edwin Gast egast@marshallbrowninghospita
l.com
Marshall Browning
Hospital
900 N. Washington
St.
P.O. Box
192
Du Quoin, IL 62832-
9788
Laurie Kellerman lkellerman@marshallbrowningh
ospital.com
Massac County Mental
Health Center
206 W. Fifth St. Metropolis, IL 62960 Yvonne Rath
Massac Memorial
Hospital
28 Chick St. P.O. Box
850
Metropolis, IL 62960-
0850
Kim Abell [email protected]
Massac Memorial
Hospital
28 Chick St. P.O. Box
850
Metropolis, IL 62960-
0850
David Fuqua [email protected]
Massac Memorial
Hospital
28 Chick St. P.O .Box
850
Metropolis, IL 62960-
0850
Rachael Belford [email protected]
Memorial Hospital of
Carbondale
405 W. Jackson St. P.O. Box
10000
Carbondale, IL 62902-
9000
Bart Millstead [email protected]

47
Memorial Hospital,
Belleville
4500 Memorial Drive Belleville, IL 62226-
5399
Mark Turner [email protected]
Memorial Hospital,
Chester
1900 State St. Chester, IL 62233-
0609
Steven Hayes [email protected]
Monroe County Health
Department
901 Illinois Avenue Waterloo, IL 62298
PAVE P.O. Box
342
Centralia, IL 62801
Perry County
Counseling Center, Inc.
1016 S. Madison St.
Ste. A
DuQuoin, IL 62832 Susan Engelhardt [email protected]
Perry County Health
Department
907 S. Main St. P.O. Box
49
Pinckneyville,
IL
62274
Perry County Health
Department
907 S. Main St. P.O. Box
49
Pinckneyville,
IL
62274 Jodi Schoen [email protected]
Pinckneyville
Community Hospital
101 N. Walnut St. Pinckneyville,
IL
62274-
1034
Thomas Hudgins,
FACHE
Pinckneyville
Community Hospital
101 N. Walnut St. Pinckneyville,
IL
62274-
1034
Nancy Keller [email protected]
Pinckneyville
Community Hospital
101 N. Walnut St. Pinckneyville,
IL
62274-
1034
Beth Inman [email protected]
Practical Rehab
Services
3550 College Ave. Alton, IL 62002 Sharon Johnson [email protected]
Randolph County
Health Department
2515 State St. Chester, IL 62233
Red Bud Regional
Hospital
325 Spring St. Red Bud, IL 62278-
1105
Shane Watson [email protected]
Residential Options,
Inc., Fosterberg
Terrace
4617 Wonderland
Drive
Alton, IL 62002
Richland Memorial
Hospital
800 E. Locust St. Olney, IL 62450-
2553
David Allen [email protected]
Rural Health Inc. 513 N. Main St. Anna, IL 62906 Cynthia K. Flamm [email protected]

48
Rural Health Inc. 318 N. Highway 51 Dongola, IL 62926
Rural Health Inc. 803 N. First St. Vienna, IL 62995
Rural Health Inc. 608 S. Main Anna, IL 62906
Rural Health Inc. Cobden, IL 62920
Rural Health Inc. 515 N. Main St. Anna, IL 62906
Saint Anthony's Health
Center
1 Saint Anthony's
Way
P.O .Box
340
Alton, IL 62002-
0340
E.J. Kuiper, FACHE [email protected]
Salem Counseling
Center, PC
220 E. Rodgers St. Salem, IL 62881 Julie Holland [email protected]
Salem Township
Hospital
1201 Ricker Drive Salem, IL 62881-
6250
Stephanie Hilton
Siebert
Shawnee Health
Service
6355 Brandhorst
Drive
Carterville, IL 62918 Patsy Jensen [email protected]
Shawnee Health
Service
101 S. Wall St. Carbondale, IL 62901
Shawnee Health
Service
1006 S. Division St, Carterville, IL 62918
Shawnee Health
Service
7 S. Hospital Drive Murphysboro,
IL
62966
Shawnee Health
Service
3111 Williamson
County Parkway
Marion, IL
62959
Shawnee Health
Service
202 W. Jackson St. Carbondale, IL 62901
Shawnee Health
Service
4 South Hospital
Drive
Murphysboro,
IL
62966
Shawnee Health
Service
1301 E. Walnut St. Carbondale, IL 62901
Shawnee Health
Service
1501 S. Carbon St. Marion, IL 62959
Shawnee Health
Service
1506 Sioux Drive Marion, IL 62959

49
Shawnee Health
Service
202 W. Jackson St. Carbondale, IL 62901
Shawnee Health
Service
3115 Williamson
County Parkway
Marion, IL 62959
Shawnee Health
Service
400 S. Lewis Lane Carbondale, IL 62901
Southeastern Illinois
Counseling Center
504 Micah Drive Olney, IL 62450 Glenn Jackson
Southern 7 Health
Department
37 Rustic Campus
Drive
Ullin, IL 62992
Southern Illinois
Behavioral Services
1016 S Madison St. Suite A DuQuoin, IL 62832
Southern Illinois
Healthcare
1239 E. Main St. P.O. Box
3988
Carbondale, IL 62902-
3988
Rex Budde [email protected]
Southern Illinois
Healthcare
1239 E. Main St. P.O. Box
3988
Carbondale, IL 62902-
3988
Woody Thorne [email protected]
Southern Illinois
Healthcare Foundation
Sharon Szatkowski [email protected]
Southern Illinois
Healthcare Foundation,
Inc.
7210 W. Main St. Belleville, IL 62223-
3038
Beverly Vokes [email protected]
Southern Illinois
Healthcare Foundation,
Inc.
80 Burlington Drive Collinsville, Il 62234
Southern Illinois
Healthcare Foundation,
Inc.
815 E. Fifth St. Alton, IL 62002
Southern Illinois
Healthcare Foundation,
Inc.
1820 Delmar Ave. Granite City, IL 62040
Southern Illinois
Healthcare Foundation,
Inc.
304 Madison Ave. Madison, IL 62060
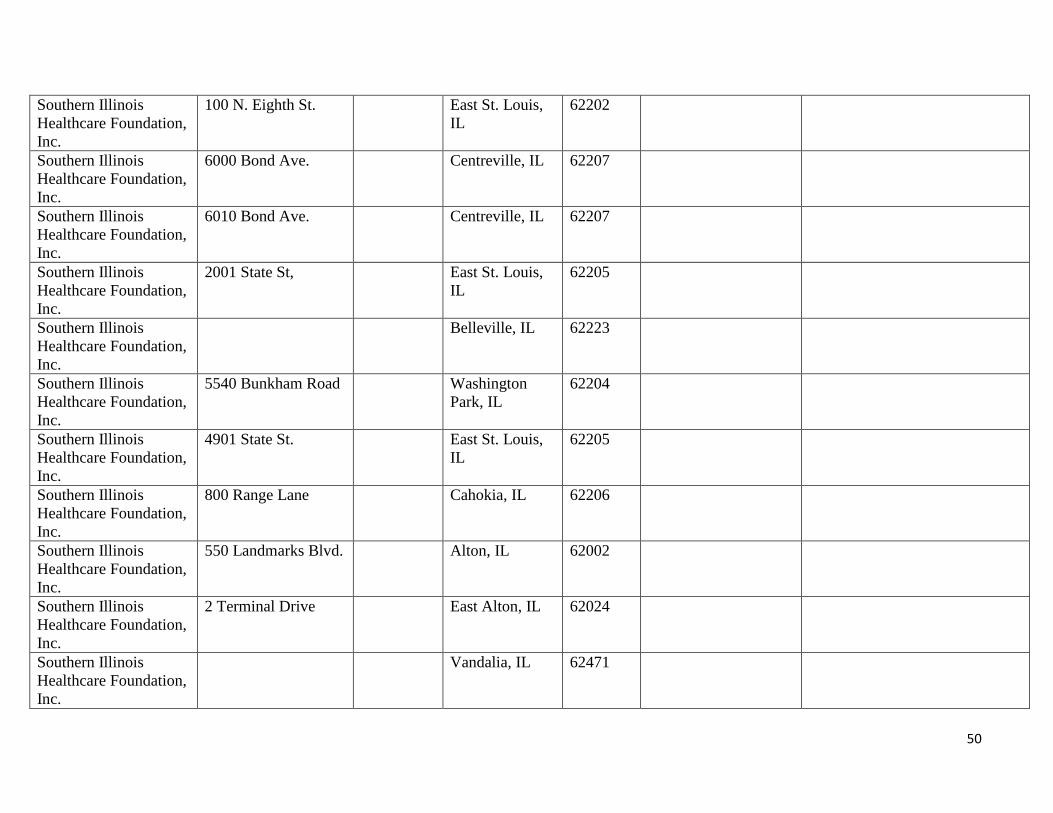
50
Southern Illinois
Healthcare Foundation,
Inc.
100 N. Eighth St. East St. Louis,
IL
62202
Southern Illinois
Healthcare Foundation,
Inc.
6000 Bond Ave. Centreville, IL 62207
Southern Illinois
Healthcare Foundation,
Inc.
6010 Bond Ave. Centreville, IL 62207
Southern Illinois
Healthcare Foundation,
Inc.
2001 State St, East St. Louis,
IL
62205
Southern Illinois
Healthcare Foundation,
Inc.
Belleville, IL 62223
Southern Illinois
Healthcare Foundation,
Inc.
5540 Bunkham Road Washington
Park, IL
62204
Southern Illinois
Healthcare Foundation,
Inc.
4901 State St. East St. Louis,
IL
62205
Southern Illinois
Healthcare Foundation,
Inc.
800 Range Lane Cahokia, IL 62206
Southern Illinois
Healthcare Foundation,
Inc.
550 Landmarks Blvd. Alton, IL 62002
Southern Illinois
Healthcare Foundation,
Inc.
2 Terminal Drive East Alton, IL 62024
Southern Illinois
Healthcare Foundation,
Inc.
Vandalia, IL 62471
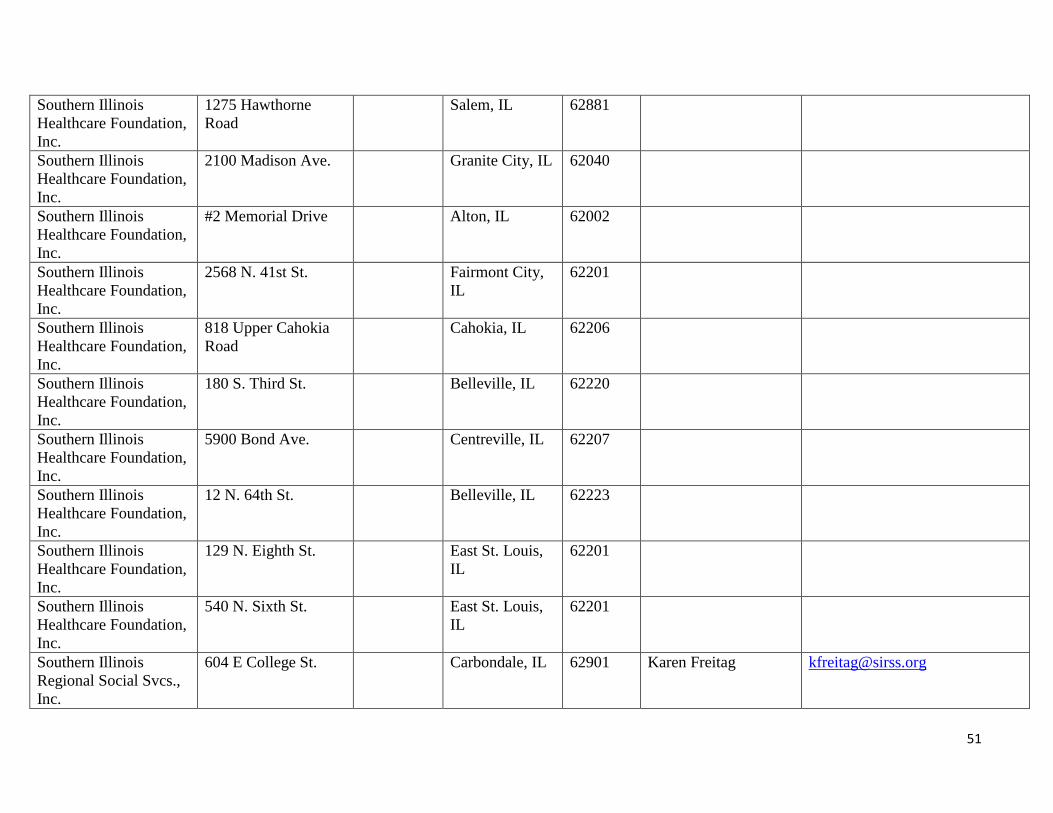
51
Southern Illinois
Healthcare Foundation,
Inc.
1275 Hawthorne
Road
Salem, IL 62881
Southern Illinois
Healthcare Foundation,
Inc.
2100 Madison Ave. Granite City, IL 62040
Southern Illinois
Healthcare Foundation,
Inc.
#2 Memorial Drive Alton, IL 62002
Southern Illinois
Healthcare Foundation,
Inc.
2568 N. 41st St. Fairmont City,
IL
62201
Southern Illinois
Healthcare Foundation,
Inc.
818 Upper Cahokia
Road
Cahokia, IL 62206
Southern Illinois
Healthcare Foundation,
Inc.
180 S. Third St. Belleville, IL 62220
Southern Illinois
Healthcare Foundation,
Inc.
5900 Bond Ave. Centreville, IL 62207
Southern Illinois
Healthcare Foundation,
Inc.
12 N. 64th St. Belleville, IL 62223
Southern Illinois
Healthcare Foundation,
Inc.
129 N. Eighth St. East St. Louis,
IL
62201
Southern Illinois
Healthcare Foundation,
Inc.
540 N. Sixth St. East St. Louis,
IL
62201
Southern Illinois
Regional Social Svcs.,
Inc.
604 E College St. Carbondale, IL 62901 Karen Freitag [email protected]

52
Southern Illinois
Regional Wellness
Center
100 N. Eighth St. East St. Louis,
IL
62201
Southern Illinois
Regional Wellness
Center
1835 Kingshighway Washington
Park, IL
62204
Southern Illinois
University, School of
Medicine
P.O. Box
19604
Springfield, IL 62794-
9604
Robert Wesley [email protected]
Southern Illinois
University-Center for
Rural Health
150 E. Pleasant Hill
Road
Suite 108 Carbondale, IL 62901 Kim Sanders [email protected]
Southern Illinois
University-Center for
Rural Health
150 E. Pleasant Hill
Road
Suite 108 Carbondale, IL 62901 Ruth Heitkamp [email protected]
Sparta Community
Hospital
818 E. Broadway P.O. Box
297
Sparta, IL 62286-
0297
Joann Emge [email protected]
Sparta Community
Hospital
818 E. Broadway P.O. box
297
Sparta, IL 62286-
0297
Lori Clinton [email protected]
SMGSMG Lisa Crouch [email protected]
SMGSMG Loretta Stevens [email protected]
SSMHC Keith Suedmeyer [email protected]
St. Clair County Health
Department
#19 Public Square-
Suite 150
Belleville, IL 62220 Kevin Hutchison [email protected]
St. Clair County
Mental Health Board
307 E. Washington
St.
Belleville, IL 62220 Dana Rosenzweig [email protected]
St. Elizabeth Hospital 211 S. Third St. Donna Meyers [email protected]
St. Elizabeth Hospital 211 S. Third St. Deborah Vogel [email protected]
St. Elizabeth's Hospital 211 S. Third St. Belleville, IL 62220-
1998
Michael Conley [email protected]
St. Elizabeth's Hospital 211 S. Third St. Belleville, IL 62220-
1998
Maryann Reese [email protected]

53
St. Joseph Memorial
Hospital
2 S. Hospital Drive Murphysboro,
IL
62966-
0580
Scott Seaborn [email protected]
St. Joseph's Hospital,
Breese
9515 Holy Cross
Lane
P.O. Box
99
Breese, IL 62230-
0099
Mark Klosterman [email protected]
St. Joseph's Hospital,
Highland
1515 Main St. Highland, IL 62249-
1698
Peggy Sebastian [email protected]
St. Mary's Hospital,
Centralia
400 N. Pleasant Ave. Centralia, IL 62801-
3091
Virginia Telford [email protected]
St. Mary's Hospital,
Centralia
400 N. Pleasant Ave. Centralia, IL 62801-
3091
Amy Whipple [email protected]
St. Mary's Hospital,
Centralia
400 N. Pleasant Ave. Centralia, IL 62801-
3091
Bruce Merrell [email protected]
St. Mary's Hospital,
Centralia
400 N. Pleasant Ave. Centralia, IL 62801-
3091
Greg Sims [email protected]
Starting Point
Counseling Program
801 W. Main,
Columbian Complex
Collinsville, IL 62234 Robert Dellamano
Suburban Clinical, Inc. 2217 W. Main Belleville, IL 62226 Ronald Vitale [email protected]
The Fellowship House P.O. Box
682
Anna, IL 62906 Mickey Finch [email protected]
m
The H Group 902 W Main P.O. Box
637
West Frankfort,
IL
62896 John G. Markley,
MBA
The H Group 902 W. Main P.O. Box
637
West Frankfort,
IL
62896 Wendy Bailie [email protected]
The H Group 902 W. Main P.O. Box
637
West Frankfort,
IL
62896 Debby Pape [email protected]
The H Group 902 W. Main P.O. Box
637
West Frankfort,
IL
62896 Sharon Adams [email protected]
Thompson Counseling
Services
4230 Lincolnshire Suite E Mt. Vernon, IL 62864 Michael Thompson [email protected]
Touchette Regional
Hospital
5900 Bond Ave. Centreville, IL 62207-
2326
Sulbrena Day [email protected]
Touchette Regional
Hospital
5900 Bond Ave. Centreville, IL 62207-
2326
Larry McCulley [email protected]
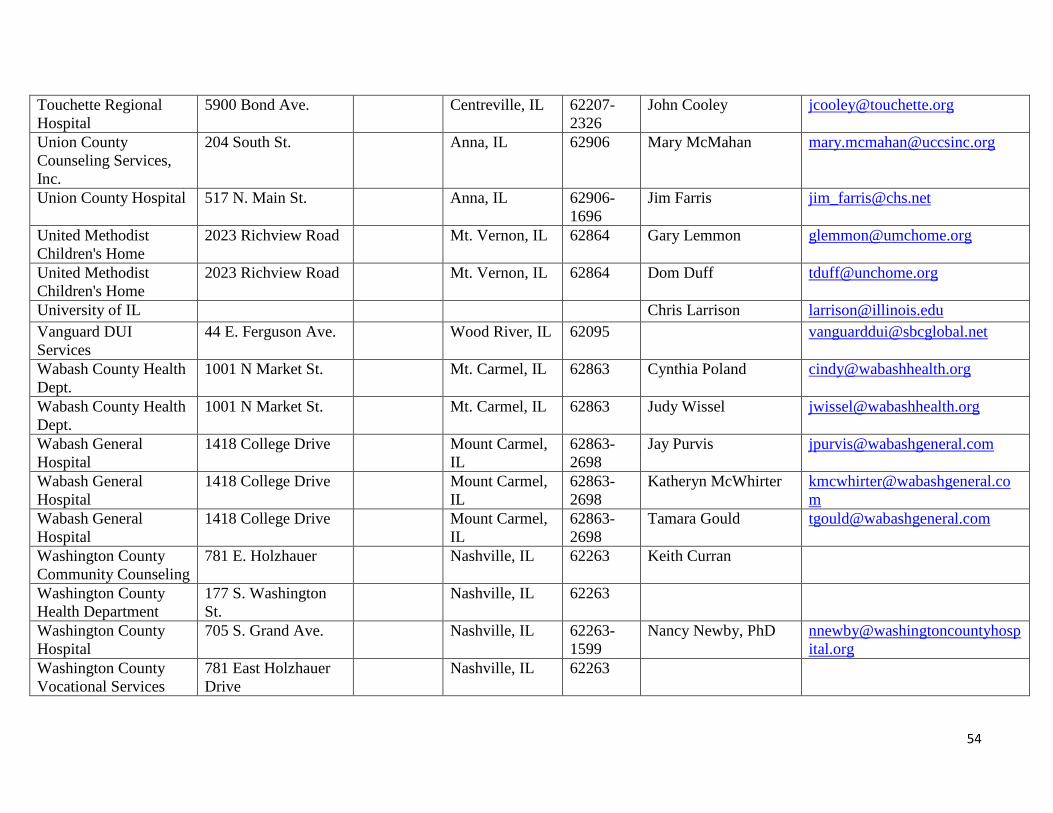
54
Touchette Regional
Hospital
5900 Bond Ave. Centreville, IL 62207-
2326
John Cooley [email protected]
Union County
Counseling Services,
Inc.
204 South St. Anna, IL 62906 Mary McMahan [email protected]
Union County Hospital 517 N. Main St. Anna, IL 62906-
1696
Jim Farris [email protected]
United Methodist
Children's Home
2023 Richview Road Mt. Vernon, IL 62864 Gary Lemmon [email protected]
United Methodist
Children's Home
2023 Richview Road Mt. Vernon, IL 62864 Dom Duff [email protected]
University of IL Chris Larrison [email protected]
Vanguard DUI
Services
44 E. Ferguson Ave. Wood River, IL 62095 [email protected]
Wabash County Health
Dept.
1001 N Market St. Mt. Carmel, IL 62863 Cynthia Poland [email protected]
Wabash County Health
Dept.
1001 N Market St. Mt. Carmel, IL 62863 Judy Wissel [email protected]
Wabash General
Hospital
1418 College Drive Mount Carmel,
IL
62863-
2698
Jay Purvis [email protected]
Wabash General
Hospital
1418 College Drive Mount Carmel,
IL
62863-
2698
Katheryn McWhirter [email protected]
m
Wabash General
Hospital
1418 College Drive Mount Carmel,
IL
62863-
2698
Tamara Gould [email protected]
Washington County
Community Counseling
781 E. Holzhauer Nashville, IL 62263 Keith Curran
Washington County
Health Department
177 S. Washington
St.
Nashville, IL 62263
Washington County
Hospital
705 S. Grand Ave. Nashville, IL 62263-
1599
Nancy Newby, PhD nnewby@washingtoncountyhosp
ital.org
Washington County
Vocational Services
781 East Holzhauer
Drive
Nashville, IL 62263

55
Wayne County Health
Department
405 N. Basin Road Fairfield, IL 62837
WellSpring Resources 2615 E. Edwards St. Alton, IL 62002 Karen Sopronyi-
Tompkins
ksopronyi@wellspringresources.
co
WellSpring Resources 2615 E. Edwards St. Alton, IL 62002 Kelly Medlin [email protected]
o
WellSpring Resources 2615 E. Edwards St. Alton, IL 62002 Ann Tyree [email protected]

56
Region 5 Acute Care Hospitals
with Psychiatric Beds
Hospital Name City
Psychiatric
Licensed Beds
Staffed Psych
Beds Oct 1,
2009
Alton Memorial Hospital Alton 20 5
Alton Mental Health Center Alton
Anderson Hospital Maryville 0 0
Chester Mental Health Center Chester
Choate Mental Hlth & Dev Ctr Anna
Clay County Hospital Flora 0 0
Crawford Memorial Hospital Robinson 0 0
Crossroads Community Hospital Mount Vernon 0 0
Fairfield Memorial Hospital Fairfield 0 0
Fayette County Hospital & LTC Vandalia 0 0
Ferrell Hospital Eldorado 0 0
Franklin Hospital Benton 0 0
Gateway Regional Medical Center Granite City 100 100
Good Samaritan Region Hlth Ctr Mount Vernon 0 0
Greenville Regional Hospital Greenville 10 10
Hamilton Memorial Hosp District McLeansboro 0 0
Hardin County General Hospital Rosiclare 0 0
Harrisburg Medical Center Harrisburg 27 27
Heartland Regional Medical Ctr Marion 0 0
Herrin Hospital Herrin 0 0
Lawrence County Memorial Hosp Lawrenceville 0 0
Marshall Browning Hospital Du Quoin 0 0
Massac Memorial Hospital Metropolis 0 0
Memorial Hosp of Carbondale Carbondale 0 0
Memorial Hospital Belleville 0 0
Memorial Hospital Chester 0 0
Pinckneyville Community Hosp Pinckneyville 0 0
Red Bud Regional Hospital Red Bud 0 0
Richland Memorial Hospital Olney 16 16
Saint Anthony's Health Center Alton 0 0
Salem Township Hospital Salem 0 0
Scott Medical Center Scott AFB
Sparta Community Hospital Sparta 0 0

57
St Elizabeth's Hospital Belleville 35 36
St Joseph Memorial Hospital Murphysboro 0 0
St Joseph's Hospital Breese 0 0
St Joseph's Hospital Highland 0 0
St Mary's Hospital Centralia 12 8
Touchette Regional Hospital Centreville 12 0
Union County Hospital Anna 0 0
Veterans Affairs Medical Ctr Marion
Wabash General Hospital Mount Carmel 0 0
Washington County Hospital Nashville 0 0
Region Total: 232 202
Source: Licensed Beds-IDPH Addendum to Inventory of Health Care Facilities
Staffed Beds-IDPH Annual Hospital Questionnaire, 2009.

Inpatient Discharges Cumulative % Change
SFY 2005 SFY 2006 SFY 2007 SFY 2008 SFY 2009 SFY 2010 From SFY 2005 to SFY 2010
Statewide 1,723,215 1,714,661 1,724,116 1,715,750 1,677,926 1,651,967 -4.1%
Region 5 9,728 9,954 9,661 10,422 10,455 10,297 5.8%
Source: COMPdata

59
SOH Inpatient Inpatient Discharges
Peds
Adults
Total
REGION FACILITY SFY 2007
SFY 2008
SFY 2009
SFY 2010
SFY 2007
SFY 2008
SFY 2009
SFY 2010
SFY 2007
SFY 2008
SFY 2009
SFY 2010
1C Madden MHC 0 0 0 0
4,242 4,151 3,654 3,674
4,242 4,151 3,654 3,674
1N Chic-Read MHC 0 0 0 0
1,913 1,788 1,848 1,829
1,913 1,788 1,848 1,829
1S Tinley Park MHC 0 0 0 0
1,721 1,473 1,784 1,823
1,721 1,473 1,784 1,823
Region 1 TOTAL 0 0 0 0
7,876 7,412 7,286 7,326
7,876 7,412 7,286 7,326
2 Elgin MHC 0 0 0 0 1,032 1,031 1,137 1,204 1,032 1,031 1,137 1,204
Singer MH/Dev Ctr 0 0 0 0 728 706 852 850 728 706 852 850
Treatment & Deten 0 0 0 0 4 9 9 6 4 9 9 6
Region 2 TOTAL 0 0 0 0
1,764 1,746 1,998 2,060
1,764 1,746 1,998 2,060
4 McFarland MHC 22 13 13 16
696 728 623 717
718 741 636 733
Region 4 TOTAL 22 13 13 16
696 728 623 717
718 741 636 733
5
Alton MH/Dev Ctr 0 0 0 0 197 198 191 188 197 198 191 188
Chester MHC 0 0 0 0 107 119 150 115 107 119 150 115
Choate MH and Dev 78 84 60 65 460 400 364 233 538 484 424 298
Region 5 TOTAL 78 84 60 65 764 717 705 536 842 801 765 601
TOTAL
100 97 73 81
11,100 10,603 10,612 10,639
11,200 10,700 10,685 10,720
No State Operated Inpatient Facilities in Region 3.
Mental Health and Substance Abuse Cases.
Source: Illinois Department of Human Services
Illinois Statistics
Office of Mental Health and Development Disabilities

60
*The Illinois Health Facilities Planning Board discontinued licensing substance abuse beds as a category of service on April 17, 2000.
this category was converted to medical/surgical beds.
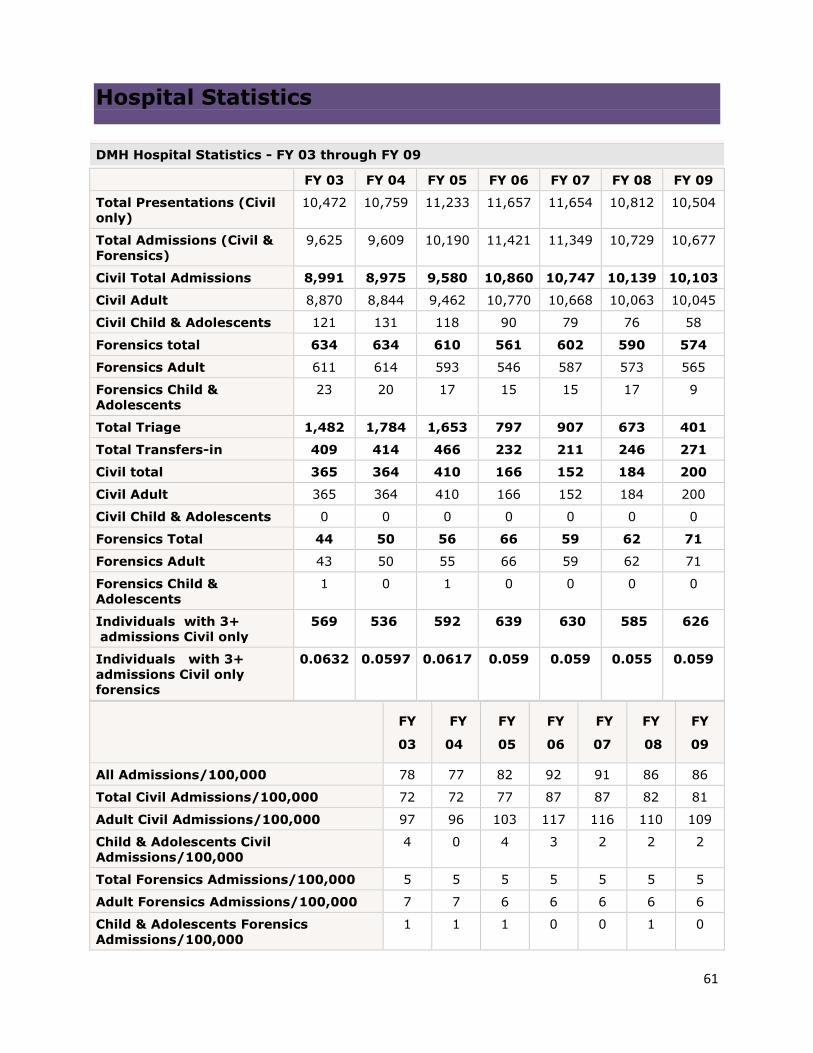
61
Hospital Statistics
DMH Hospital Statistics - FY 03 through FY 09
FY 03 FY 04 FY 05 FY 06 FY 07 FY 08 FY 09
Total Presentations (Civil
only)
10,472 10,759 11,233 11,657 11,654 10,812 10,504
Total Admissions (Civil &
Forensics)
9,625 9,609 10,190 11,421 11,349 10,729 10,677
Civil Total Admissions 8,991 8,975 9,580 10,860 10,747 10,139 10,103
Civil Adult 8,870 8,844 9,462 10,770 10,668 10,063 10,045
Civil Child & Adolescents 121 131 118 90 79 76 58
Forensics total 634 634 610 561 602 590 574
Forensics Adult 611 614 593 546 587 573 565
Forensics Child &
Adolescents
23 20 17 15 15 17 9
Total Triage 1,482 1,784 1,653 797 907 673 401
Total Transfers-in 409 414 466 232 211 246 271
Civil total 365 364 410 166 152 184 200
Civil Adult 365 364 410 166 152 184 200
Civil Child & Adolescents 0 0 0 0 0 0 0
Forensics Total 44 50 56 66 59 62 71
Forensics Adult 43 50 55 66 59 62 71
Forensics Child &
Adolescents
1 0 1 0 0 0 0
Individuals with 3+
admissions Civil only
569 536 592 639 630 585 626
Individuals with 3+
admissions Civil only
forensics
0.0632 0.0597 0.0617 0.059 0.059 0.055 0.059
FY
03
FY
04
FY
05
FY
06
FY
07
FY
08
FY
09
All Admissions/100,000 78 77 82 92 91 86 86
Total Civil Admissions/100,000 72 72 77 87 87 82 81
Adult Civil Admissions/100,000 97 96 103 117 116 110 109
Child & Adolescents Civil
Admissions/100,000
4 0 4 3 2 2 2
Total Forensics Admissions/100,000 5 5 5 5 5 5 5
Adult Forensics Admissions/100,000 7 7 6 6 6 6 6
Child & Adolescents Forensics
Admissions/100,000
1 1 1 0 0 1 0

62
FY
03
FY
04
FY
05
FY
06
FY
07
FY
08
FY
09
Co-Occurring Disorders 4,613 5,389 5,417 4,916 4,991 4,569 4,491
Percent of Co-Occurring
Disorders Admissions
0.48 0.56 0.51 0.43 0.44 0.43 0.42
Numbers shown do not include individuals considered developmentally disabled based upon legal
status at time of episode. Calculation for Admissions 100,000: population
count/100,000=multiplier: number of admissions/multiplier = Admissions/100,000.
Report Date: 07/09/2009 Population Served: 12,419,293 - FY 03 thru FY 09
Utilization of Illinois State Psychiatric Hospitals
FY03 FY04 FY05 FY06 FY07 FY08 FY09
Length of Stay (All) Average 158 196 211 199 200 221 229
Length of Stay (All) Median 16 17 15 13 12 13 13
Length of Stay (Civil ALL) Average 100 119 125 113 104 111 108
Length of Stay (Civil ALL) Median 14 14 13 11 10 11 11
Length of Stay (Civil Adult)
Average
101 120 126 113 104 112 108
Length of Stay (Civil Adult) Median 14 14 13 11 10 11 11
Length of Stay (Civil Child &
Adolescents) Average
23 20 26 33 25 39 22
Length of Stay (Civil Child &
Adolescents) Median
170 210 394 402 411 426 433
Length of Stay (Forensic Adults)
Average
678 737 841 889 926 1,005 1,077
Length of Stay (Forensic Adults)
Median
171 212 394 403 416 427 436
Length of Stay (Forensic Child &
Adolescents) Average
144 180 334 339 338 283 274
Length of Stay (Forensic Child &
Adolescents) Median
127 127 280 353 214 150 282
Average Daily Census (All) 1,512 1,481 1,466 1,440 1,413 1,400 1,377
Average Daily Census (Civil) 942 882 866 844 806 800 778
Average Daily Census (Civil Adult) 935 874 861 840 802 796 775
Average Daily Census (Civil Child &
Adolescents)
8 7 6 5 4 5 4
Average Daily Census (Forensics) 570 599 600 596 607 600 598
Average Daily Census (Forensics
Adult)
561 588 585 582 597 590 593

63
FY03 FY04 FY05 FY06 FY07 FY08 FY09
Average Daily Census (Forensics
Child & Adolescents)
9 11 15 13 10 9 6
Total Number of Residents & Home
Visits on 7/09/09.
1,410 1,369 1,402 1,322 1,373 1,353 1,319
Total Number of Civil Residents and
Home Visits on 7/09/09.
799 760 791 706 762 742 709
Total Number of Civil Adult
Residents and Home Visits on
7/09/09.
797 757 786 705 757 742 707
Total Number of Civil Child &
Adolescents Residents and Home
Visits on 7/09/09.
2 3 5 1 5 0 2
Total Number for Residential and
Home Visits on 7/09/09
611 609 611 616 611 611 610
Total Number for Adult Residential
and Home Visits on 7/09/09
601 593 595 601 603 601 605
Total Number for Child
& Adolescents Residential and
Home Visits on 7/09/09
10 16 16 15 8 10 5
Utilization of Illinois State Psychiatric Hospitals
FY 03 FY 04 FY 05 FY 06 FY 07 FY 08 FY 09
Total Separations 10,190 10,058 10,625 11,731 11,496 10,988 10,979
Total Discharges (Civil &
Forensics)
9,772 9,641 10,150 11,498 11,286 10,739 10,708
Civil Total Discharge 9,255 9,052 9,584 10,981 10,729 10,211 10,171
Civil Adult 9,122 8,922 9,468 10,888 10,654 10,131 10,115
Civil Child & Adolescents 133 130 116 93 75 80 56
Forensics Total 517 589 566 517 557 528 537
Forensic Adults 502 578 553 506 538 517 525
Forensic Child &
Adolescents
15 11 13 11 19 11 12
Total Transfers-Out (Civil
& Forensic)
418 417 475 233 210 249 271
Civil Total 368 359 408 161 138 173 200
Civil Adult 368 359 408 161 138 173 200
Civil Child & Adolescents 0 2 0 0 0 0 0
Forensics Total 50 58 67 72 72 76 71
Forensics Adult 49 58 65 72 72 76 71
Forensics Child &
Adolescents
1 0 2 0 0 0 0

64
Report date 07/09/2009 Population Served 12,419,293 http://www.dhs.state.il.us/page.aspx?item=33869