ima 29 th march 2010
DESCRIPTION
Developing a Multi-Methodology Operating Theatre Scheduling Support System Marion Penn With: Prof. Chris Potts and Prof. Paul Harper. IMA 29 th March 2010. Outline. Introduction to topic and literature Soft OR - Understanding the problem Hard OR - Master Timetable Set Up Formulation - PowerPoint PPT PresentationTRANSCRIPT

Developing a Multi-Methodology Operating
Theatre Scheduling Support System
Marion PennWith: Prof. Chris Potts and Prof. Paul Harper
IMA 29th March 2010

Outline• Introduction to topic and literature
• Soft OR - Understanding the problem
• Hard OR - Master Timetable
– Set Up
– Formulation
– Results to date
– Future Work
Background Hospitals face the challenges of;
• Demanding Targets– Shorter waits for operations– Reduced cancellations
• Financial Constraints
• Resource Constraints
Theatre Scheduling
My Objective
• To develop a methodology that can be used in hospitals to produce efficient theatre schedules.

Literature • Over 100 papers
• Methods – LP, Simulation, Queuing …
• Whole system … narrow aspects
• Factors – Theatre Time– Staff– Beds

Gaps in the Literature
• Key Factors not brought together
• Lack of Implementation
• Addressing Stochastic Elements
Cognitive mapping
• Visual
• Brings together ideas
• Enables joint understanding
• Explores links
• Causal relationships
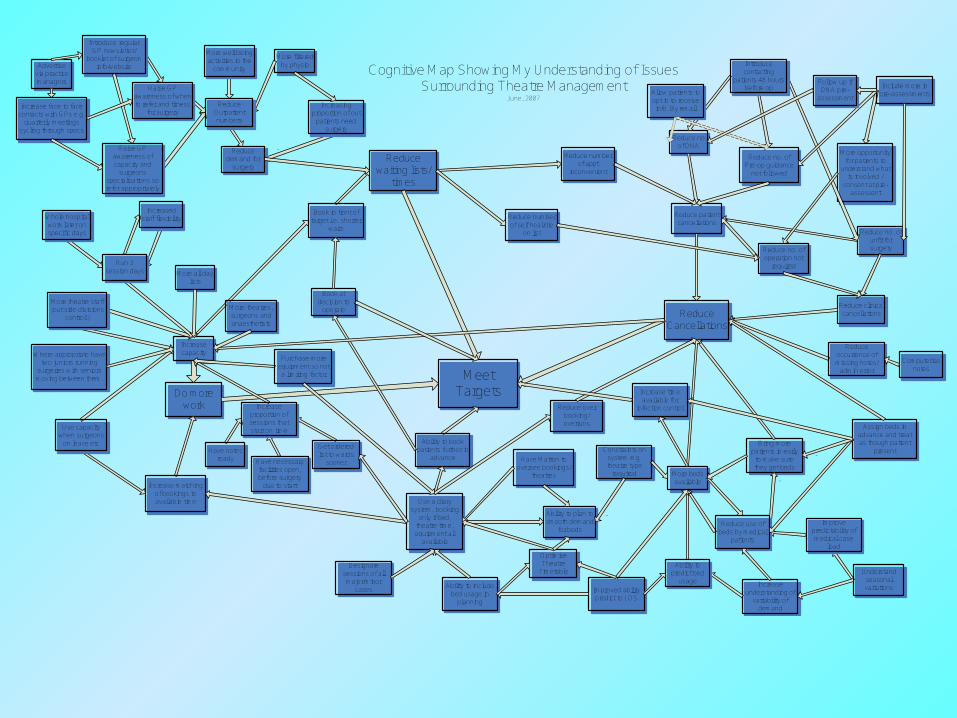
Meet Targets
Reduce Cancellations
Reduce waiting lists/
times
Do more work
Reduce clinical cancellations
Reduce patient cancellations
Reduce number of appt
inconvenient
Reduce no. of operation not
required
Reduce no. of unfit for surgery
Reduce no. of Pre-op guidance
not followed
Reduce no of DNA
Include more in pre-assessments
More opportunity for patients to
understand what is involved /
consent at pre-assessent
Introduce contacting
patients 48 hours before op
Reduce occurrence of missing notes/
admin error
More beds available
Bring more patients in early
to make sure they get beds
Reduce use of beds by medical
patients
-
-
Improve predictability of medical case
load
Understand seasonal variationsIncrease
understanding of variability of
demand
-
Ability to predict bed
usageImproved ability predict to LOS
Use a diary system, booking
only if bed, theatre time, equipment all
available
Ability to plan to smooth demand
for beds
Ability to book patients further in
advance
Ability to include bed usage in
planning
Have Matron to oversee bookings/
theatres
Reduce over booking/overruns
Increase capacity
Reduce demand for
surgery
Increasing proportion of out
patients need surgery
-
More filtered by physio
More well being activities in the
community
Reduce Outpatient numbers
Raise GP awareness of when to refer and fitness
for surgery
Raise GP awareness of capacity and
surgeons specialisations so refer appropriately
Introduce regular GP newsletter/
booklet of surgeon info/website
Increase face to face contacts with GPs e.g.
quarterly meetings cycling through specs
Advertise via practice managers
Increase proportion of sessions that start on time
Have notes ready Have necessary
facilities open, before surgery
due to start
Get ordered list to wards
sooner
Run 3 session days
Whole hospital work later on specific days
Increased staff flexibility
More theatre staff (out side divisions
control!)
Use capacity when surgeons
on leave etc
Increase matching of bookings to available time
Purchase more equipment so not a limiting factor
Book in front of target i.e. shorter
waits
Book at decision to
operate
Cognitive Map Showing My Understanding of IssuesSurrounding Theatre Management
June, 2007
Reduce number of self heal/die
on list
More theatres, surgeons and anaesthetists
Where appropriate have two juniors running
surgeries with seniors moving between them.
Designate sessions of all major/minor
cases
Allow patients to opt in to receive info. By email
Assign beds in advance and treat as though patient
present
More all day lists
-
Increase time available for
infection control
Computerise notes
Constraints on system e.g. theatre type
required
Follow up if DNA pre-
assessment
Optimise Theatre
Timetable
-

Hard OR – From Literature
• Strategic– Planning work load– Dividing theatre time
• Longer term tactical planning– Developing a Master Theatre Timetable
• Day to day scheduling of electives– Booking into slots– Live changes to the schedule
Master Timetable
• What– Assigns slots of theatre time to surgeons– Cyclic
• How– Linear / Goal Programming– Heuristics– Simulation– Column Generation
Inputs
• Theatre types and availability
• Numbers of theatre slots required
• Surgeon (and other staff) availability
• Surgeon preferences
• Expected bed usage (by ward)
• Equipment availability
• Bed availability and usage

Variables•Xi,t,d,s Assigns surgeons to slots.
•Yi,t,d,s If a slot has been assigned to a surgeon with a low preference score for it.
•Ui,t,d,s If surgeon in same theatre for consecutive slots.
•Vi,t,d,s If surgeon in different theatres for consec. slots.
•Wi,t,d,s If slot repeated weekly.
• Expected beds required each day. •Z Min difference between beds required and beds
available.X, Y, U, V and W are all binary variables.Index i represents an individual surgeon, t a theatre, d a dayin the cycle and s a daily theatre slot.
d
Significant Parameters
• Gh,t Types of theatres 1 if t is of type h, 0 otherwise
• Rh,t Number of slots of type h required by surgeon i
• Bi,t,j,w Expected number of patients in beds in ward k, j days after surgeon i
has a slot in theatre t• Dd,w Number of beds available on day d
in ward k

‘Straightforward’ Constraints
• Only use available slots
• Surgeons can only be in one place
• Surgeons availability
• Limit on surgeons no. slots per day
• Equipment constraint

Demand Constraints
•
Cover demand by theatre type
•
Meet each surgeon’s overall demand exactly
•
Surgeons don’t use any theatre more than
their total demand for its type(s)
ih, iht ds
sdtith RXG ,,
,,,,
i h
ihdst
sdti RX ,,,
,,,
ti, ds
sdtih
thih XGR,
,,,,,
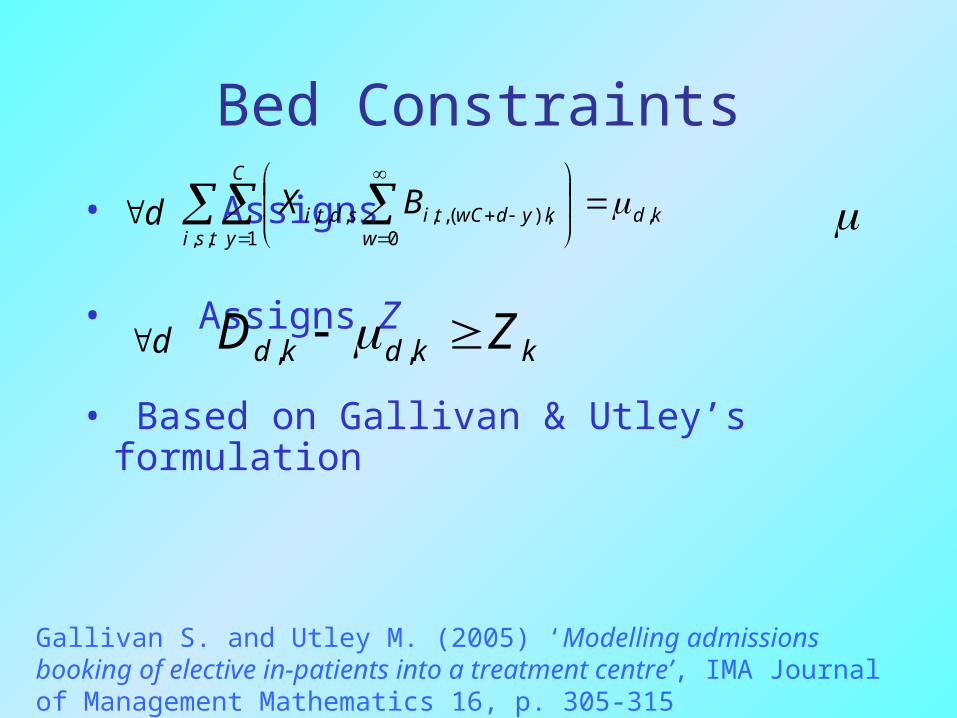
Bed Constraints
• Assigns
• Assigns Z
• Based on Gallivan & Utley’s formulation
d kdtsi
C
y wkydwCtisdti BX ,
,, 1 0),(,,,,,
d kkdkd ZD ,,
Gallivan S. and Utley M. (2005) ‘Modelling admissions booking of elective in-patients into a treatment centre’, IMA Journal of Management Mathematics 16, p. 305-315

Other Constraints
• Assign values to;– U– V– W– Y
• Based on the values in X
Objectives• Find a feasible timetable
• Smooth Bed usage
• Max surgeon pref. score
• Min low pref. scores
• Max all day slots
• Repeat slots weekly
• Avoid consecutive slots in
different theatres
k
kZ
sdti
sdtisdti XP,,,
,,,,,,
sdti
sdtiY,,,
,,,
sdti
sdtiU,,,
,,,
sdti
sdtiV,,,
,,,
sdti
sdtiW,,,
,,,
Output
• Weekly / Monthly Schedule– Slots for Surgeons
• Expected Bed Usage
• Ratings against objectives

Early Results
Indicator Original Timetable
LP Timetable
Max beds used 90 83
No. Surgeons changing theatres
0 0
No. of all day slots 30 55
Repeat weekly 166 178

Bed SmoothingComparing current and suggested timetables bed usage.
0
20
40
60
80
100
120
140
Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 8 Day 9 Day 10 Day 11 Day 12 Day 13 Day 14
Day of Cycle
Nu
mb
er
of
be
ds
Max. number of beds availableBeds required by current timetableMax. beds required by current timetableBeds required by suggested timetableMax. beds required by suggested timetable

Future Work
• Further Develop Master Timetable
• Day to day scheduling tool
• Warning systems
Questions/ Comments