imaging in family medicine
TRANSCRIPT
IMAGING IN FAMILY MEDICINE
Imaging Methods
• Ultrasonography (USG)
• X-ray
• Computed tomography (CT)
• Magnetic resonance imaging (MRI)
• Scintigraphy
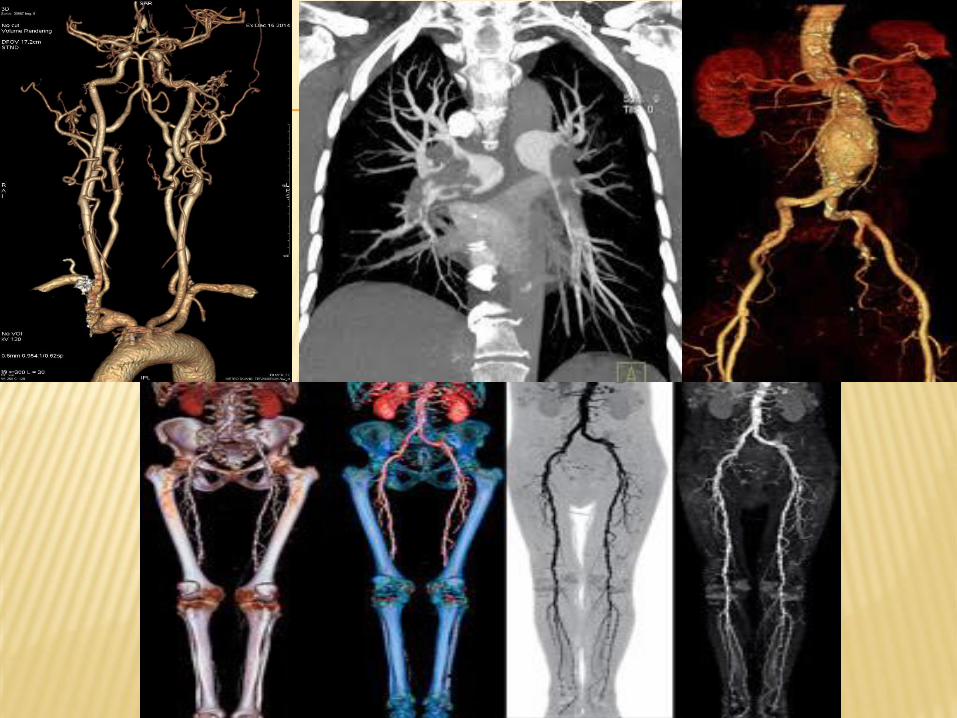
• Angiography
SNC
MEDIASTINUM
LUNGS
ABDOMEN
PELVIS
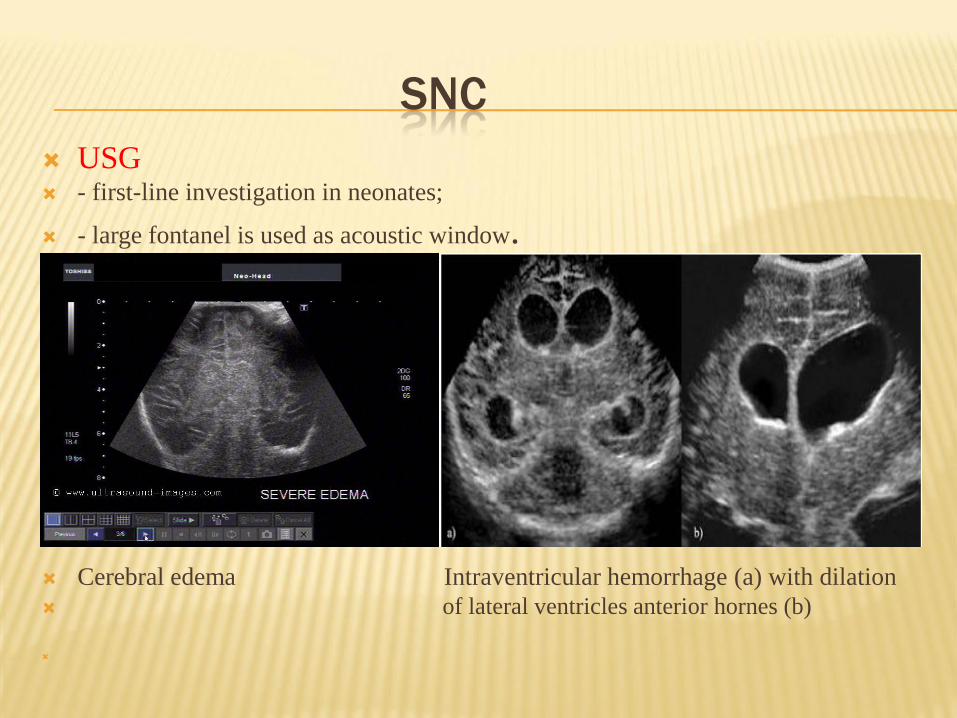
SNC
USG - first-line investigation in neonates;
- large fontanel is used as acoustic window.
Cerebral edema Intraventricular hemorrhage (a) with dilation
of lateral ventricles anterior hornes (b)
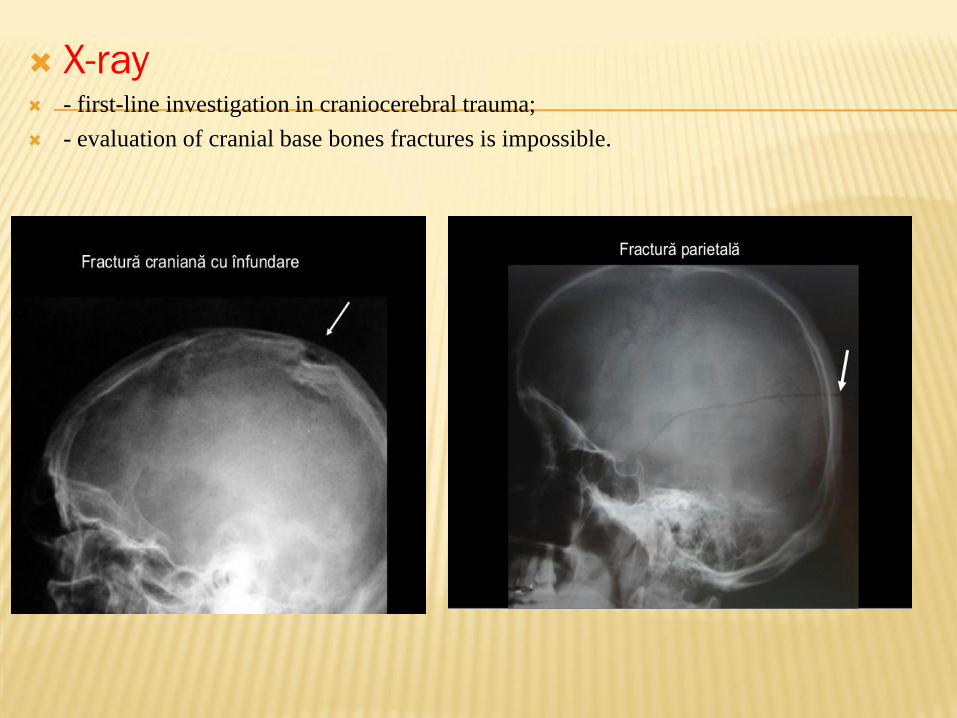
X-ray - first-line investigation in craniocerebral trauma;
- evaluation of cranial base bones fractures is impossible.
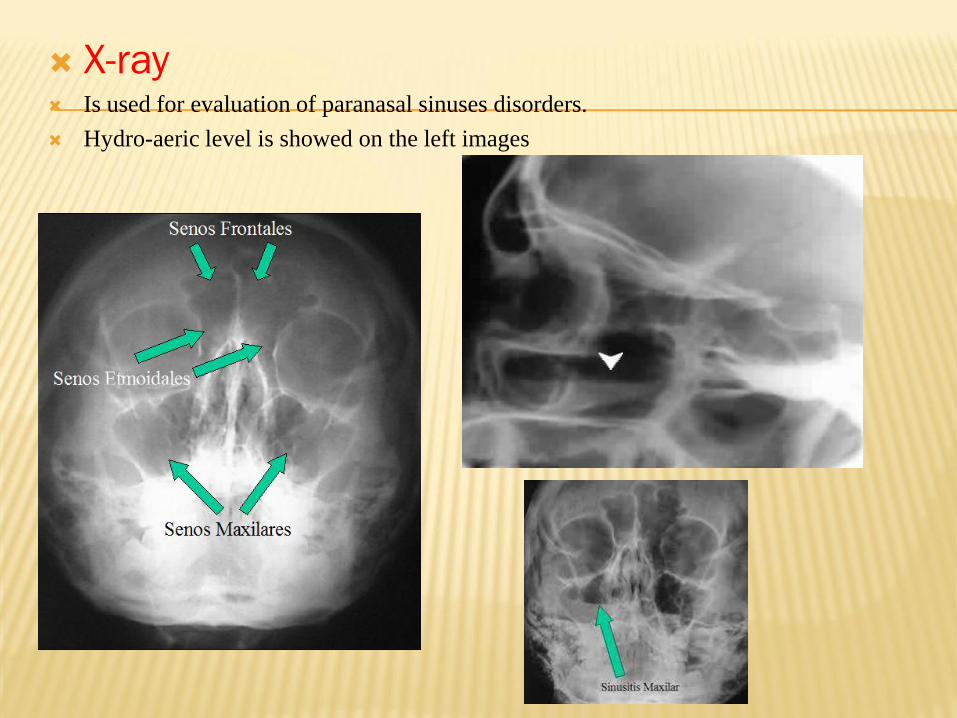
X-ray Is used for evaluation of paranasal sinuses disorders.
Hydro-aeric level is showed on the left images
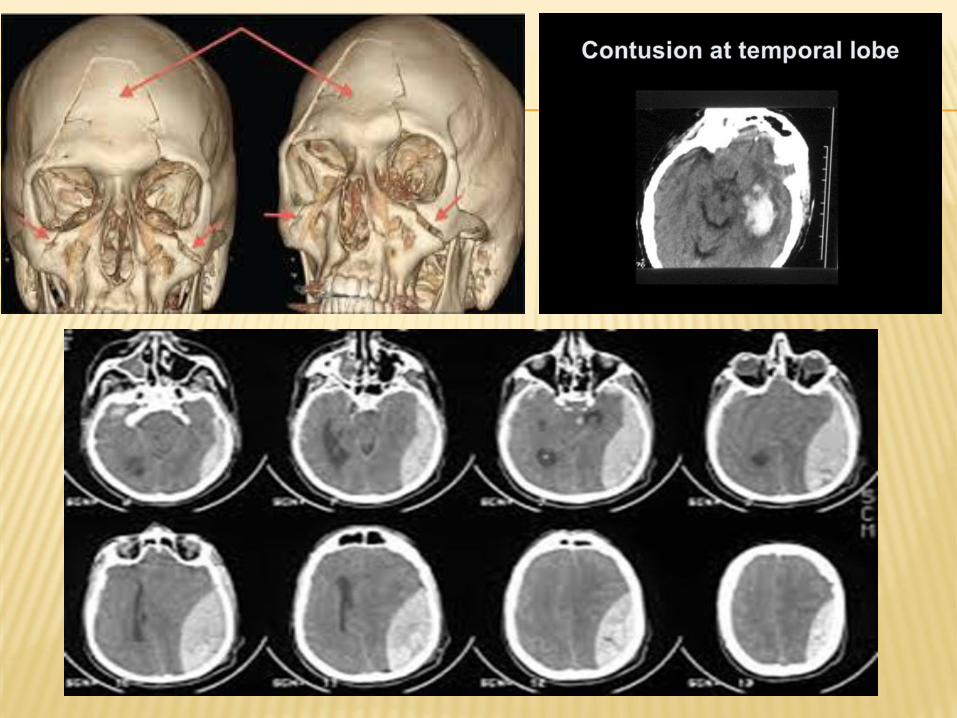
CT
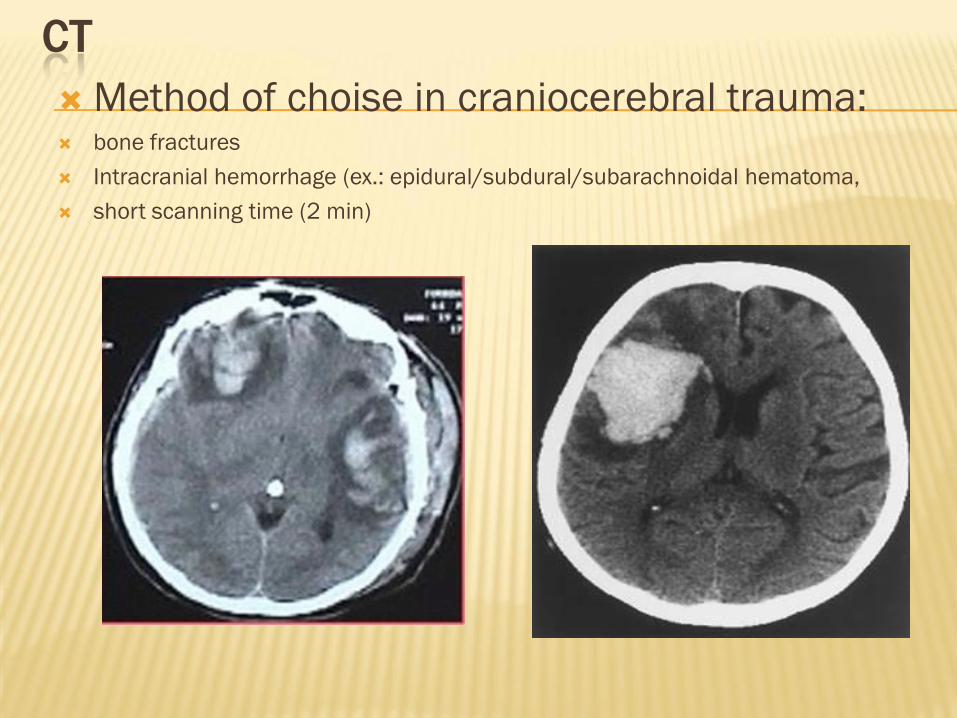
Method of choise in craniocerebral trauma: bone fractures
Intracranial hemorrhage (ex.: epidural/subdural/subarachnoidal hematoma,
short scanning time (2 min)
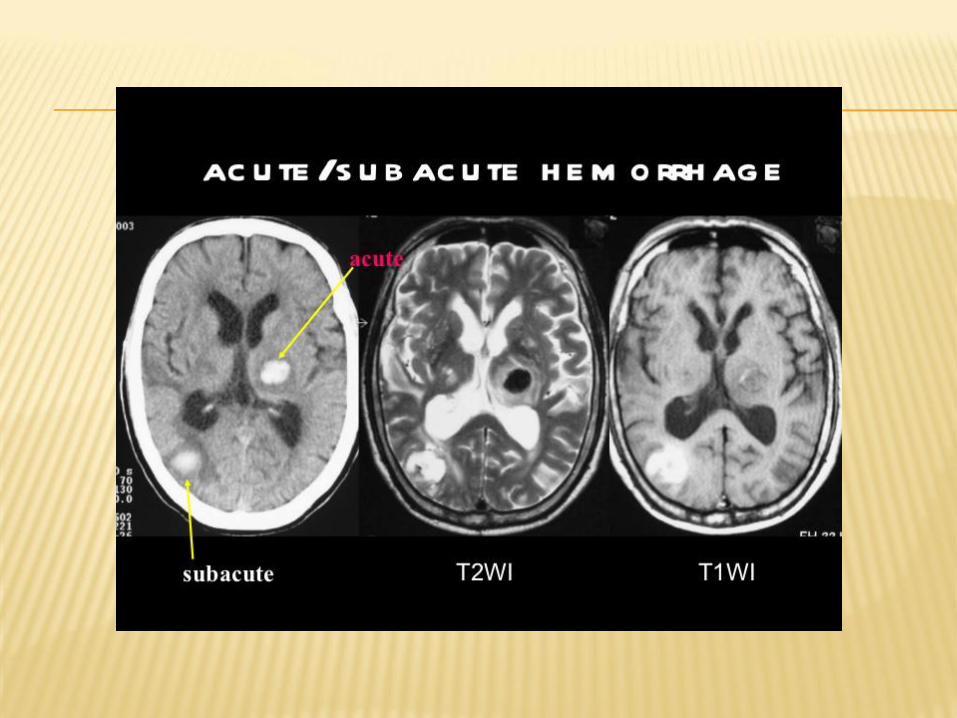
CT AND MRI STADIALIZATION OF INTRACRANIAL
HAEMORRHAGE
CT scan is almost always the first imaging modality used to
assess patients with suspected intracranial haemorrhage.
Fortunately acute blood is markedly hyperdense compared to
brain parenchyma (60-80 Hu)
The imaging characteristics of blood on MRI are variable and
change with the age of the blood:
- acute (1 to 2 days) - T2 signal intensity drops (T2 shortening),
T1 remains intermediate-to-low
- late subacute (7 to 14-28 days) - extracellular
methaemoglobin leads to an increase in T2 signal
- chronic (>14-28 days) – periphery low on both T1 and T2
center - isointense on T1, hyperintense on T2
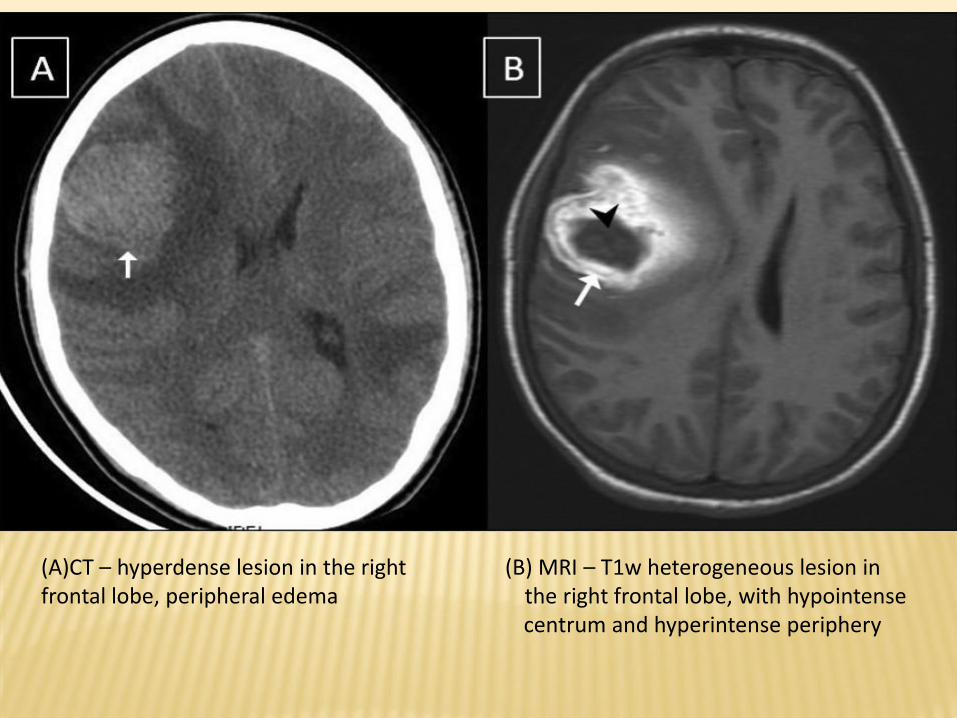
(A)CT – hyperdense lesion in the right (B) MRI – T1w heterogeneous lesion in frontal lobe, peripheral edema the right frontal lobe, with hypointense
centrum and hyperintense periphery
Chest imaging
X-ray, CT, MRI- Chest X-ray is made in PA and lateral projections for localising
lesions.
- Main indications for chest CT scanning:
Staging malignancy
Detecting pulmonary metastases
Far superior in assessing chest wall and pleural lesions, lung mass, the hilum and mediastinum
High value in the diagnosis of diffuse lung desease
Evaluation of bronchiectasis (surgery is undertaken without preoperative bronchography)
- MRI – helpful in the diagnosis of hilar masses, lymphadenopathy and mediastinal lesions
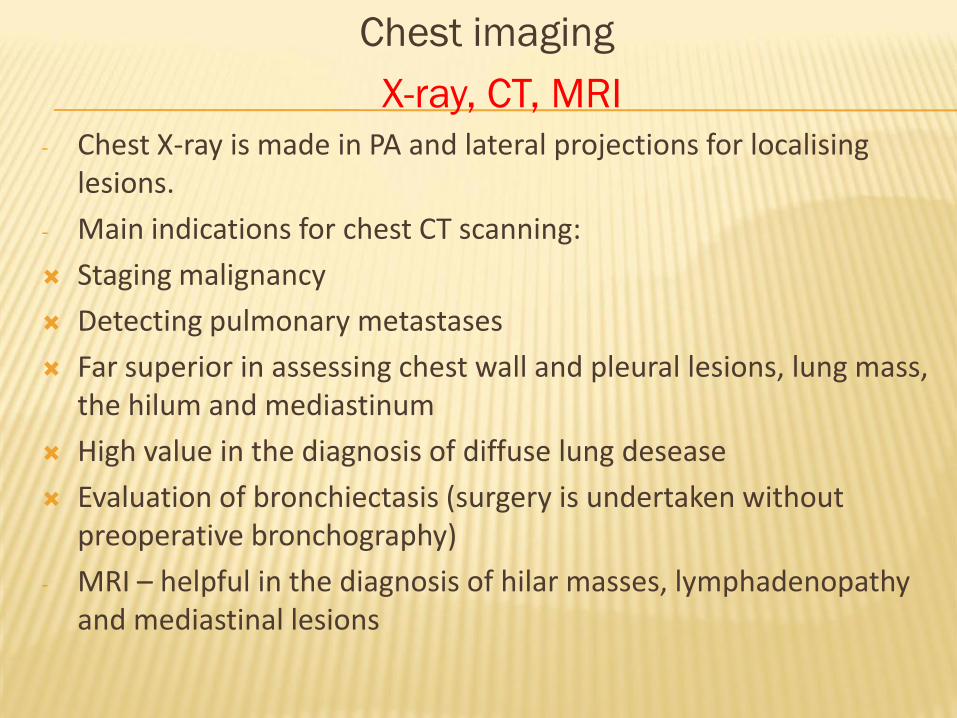
Hilul pulmonar
se vizualizeaza
prin formațiunea
de volum
Thymoma Anterior mediastinal lymphoma
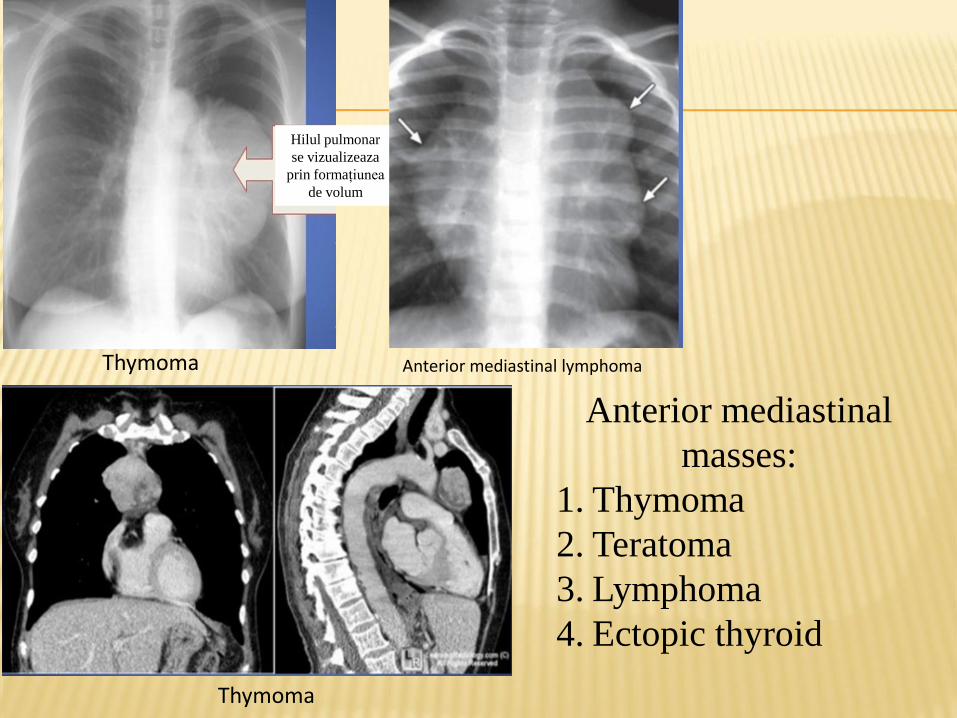
Thymoma
Anterior mediastinal
masses:
1. Thymoma
2. Teratoma
3. Lymphoma
4. Ectopic thyroid
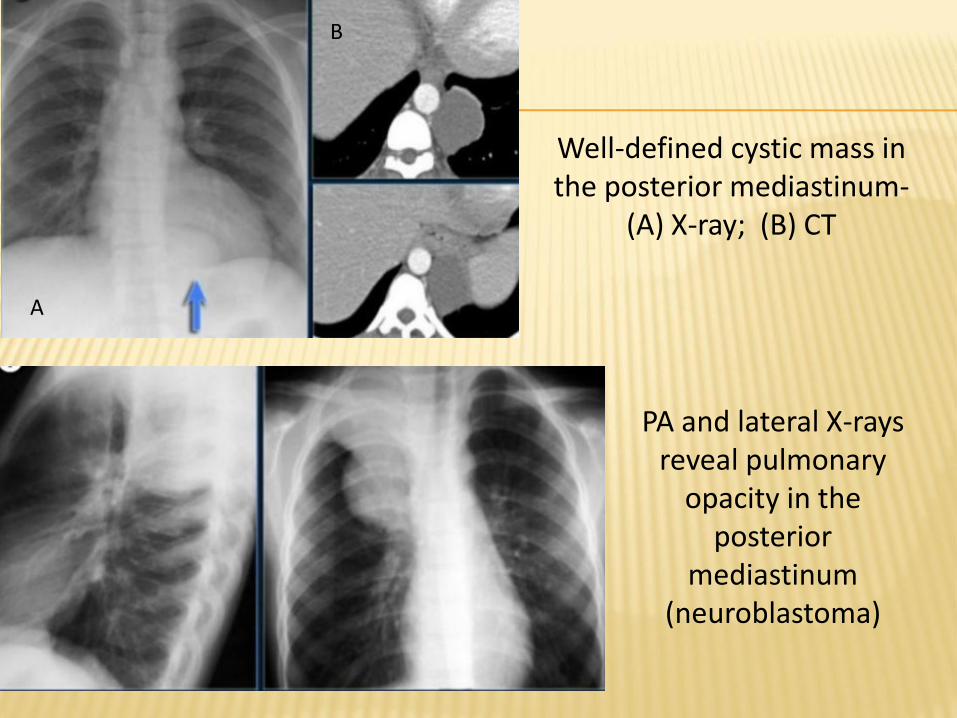
Well-defined cystic mass in the posterior mediastinum-
(A) X-ray; (B) CT
A
B
PA and lateral X-rays reveal pulmonary
opacity in the posterior
mediastinum (neuroblastoma)
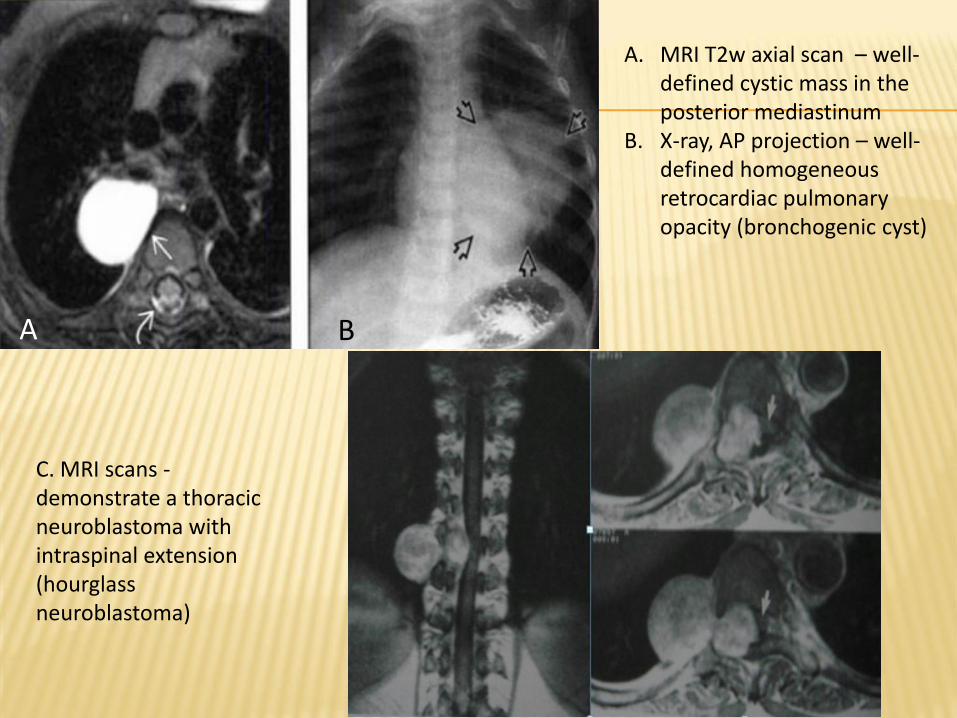
A. MRI T2w axial scan – well-defined cystic mass in the posterior mediastinum
B. X-ray, AP projection – well-defined homogeneous retrocardiac pulmonary opacity (bronchogenic cyst)
A B
C. MRI scans -demonstrate a thoracic neuroblastoma with intraspinal extension(hourglass neuroblastoma)
Abdominal imaging
USG, X-ray, CT, MRI
Ultrasound imaging of the abdomen uses sound waves to produce pictures of the structures within the upper abdomen. It is used to help diagnose pain or distention and evaluate the kidneys, liver, gallbladder, pancreas, spleen and abdominal aorta. .
Abdominal X-ray is helpful in detection of intestine obstruction, hollow organs perforation, abnormal calcifications, foreign radiopaque bodies.
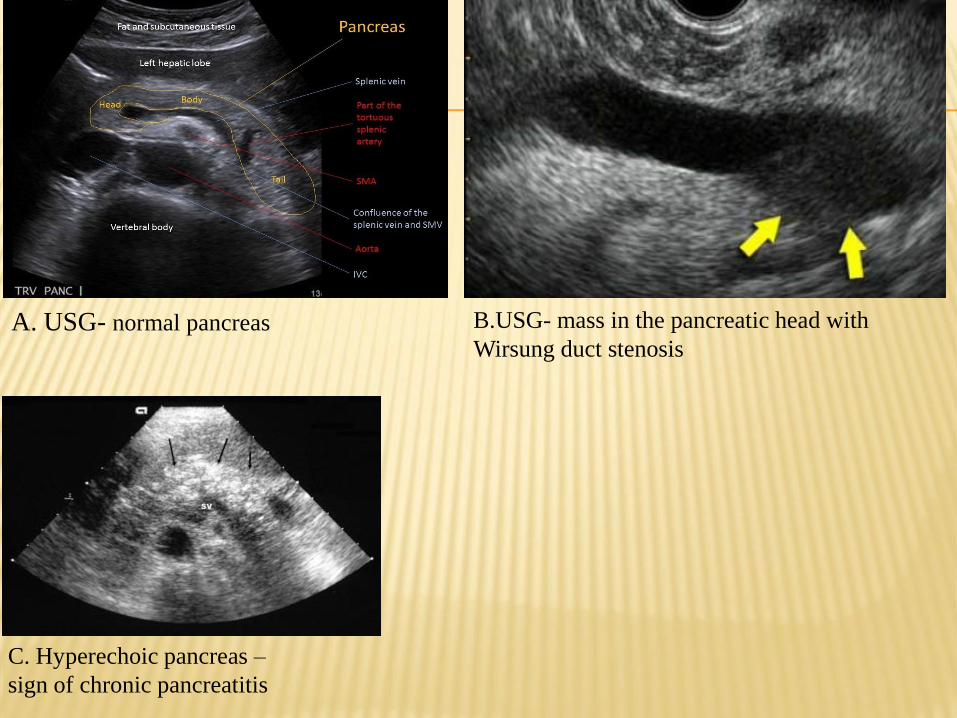
B.USG- mass in the pancreatic head with
Wirsung duct stenosis
C. Hyperechoic pancreas –
sign of chronic pancreatitis
A. USG- normal pancreas
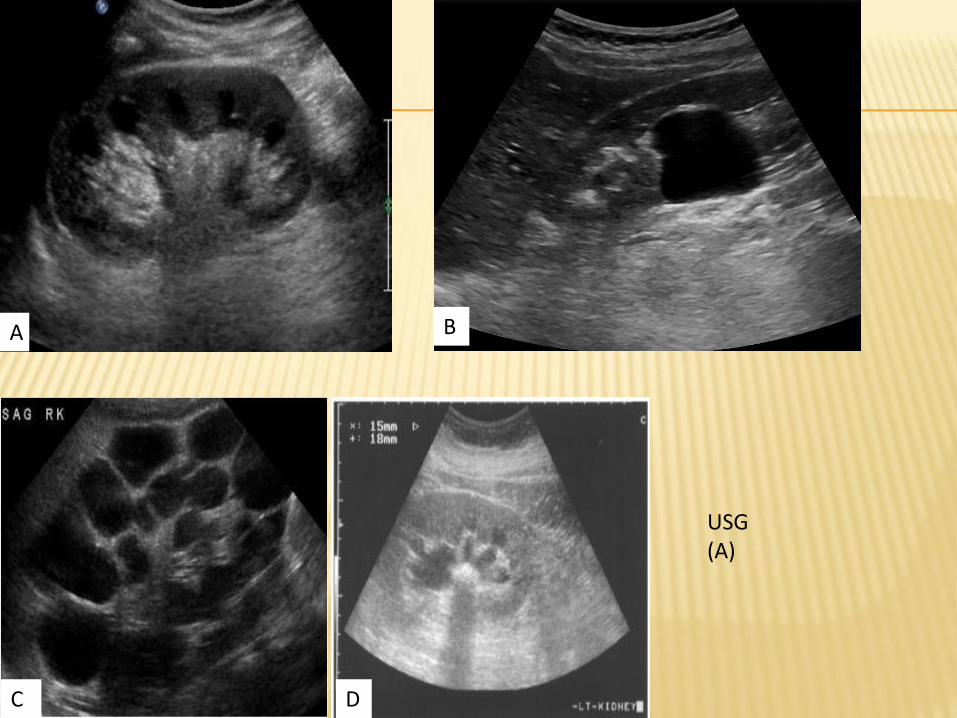
USG(A)
A B
C D
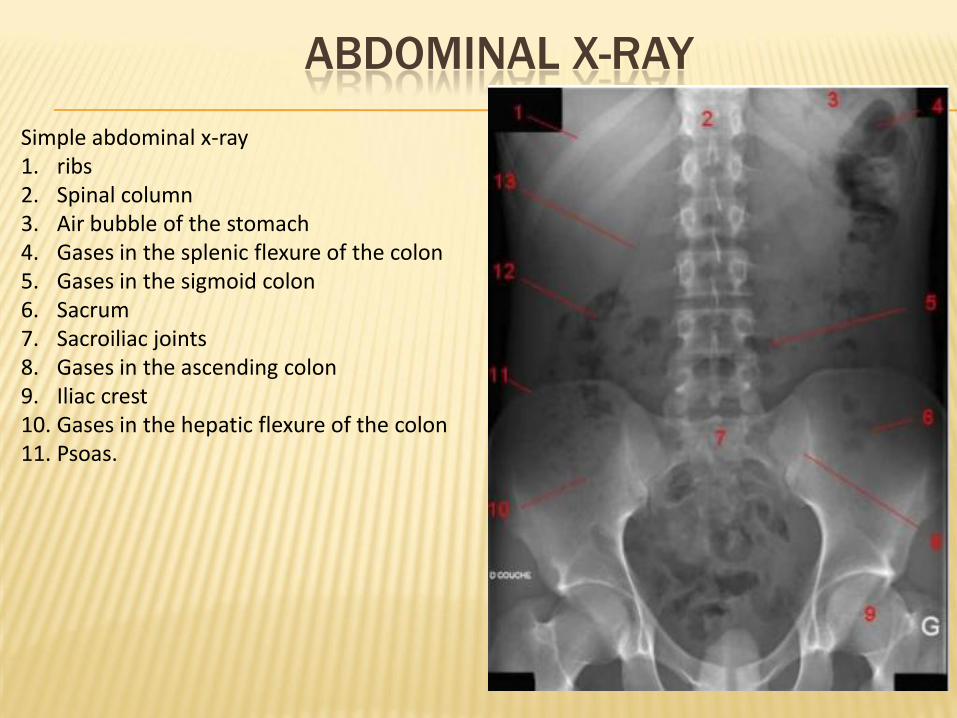
ABDOMINAL X-RAY
Simple abdominal x-ray1. ribs2. Spinal column3. Air bubble of the stomach4. Gases in the splenic flexure of the colon5. Gases in the sigmoid colon6. Sacrum7. Sacroiliac joints8. Gases in the ascending colon9. Iliac crest10. Gases in the hepatic flexure of the colon11. Psoas.
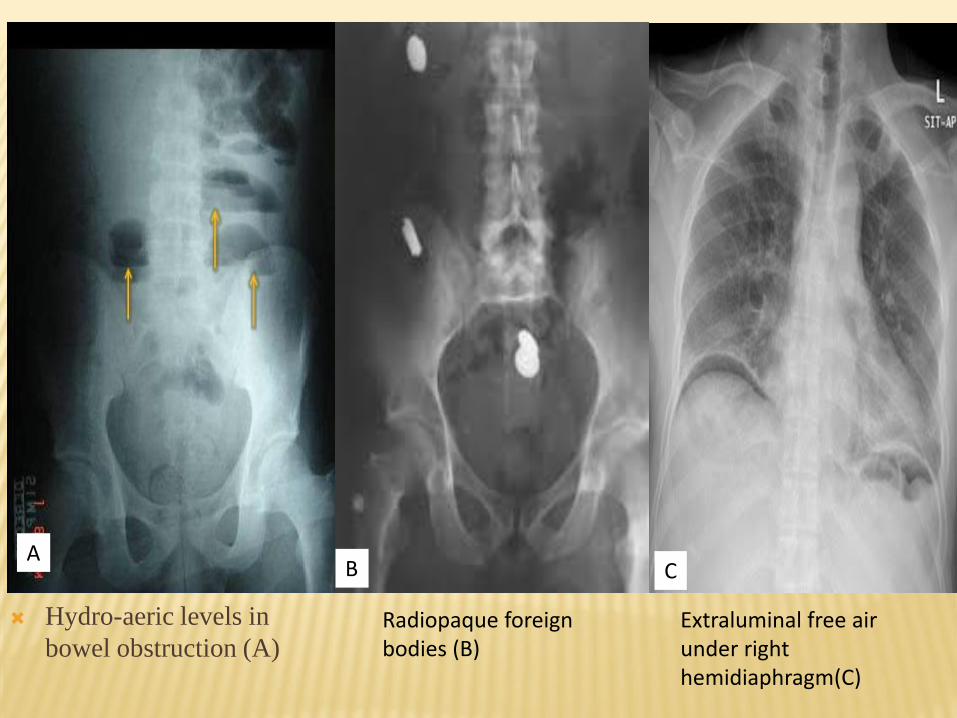
Hydro-aeric levels in
bowel obstruction (A)
BA
C
Radiopaque foreign bodies (B)
Extraluminal free air under right hemidiaphragm(C)

INTRAVENOUS UROGRAPHY
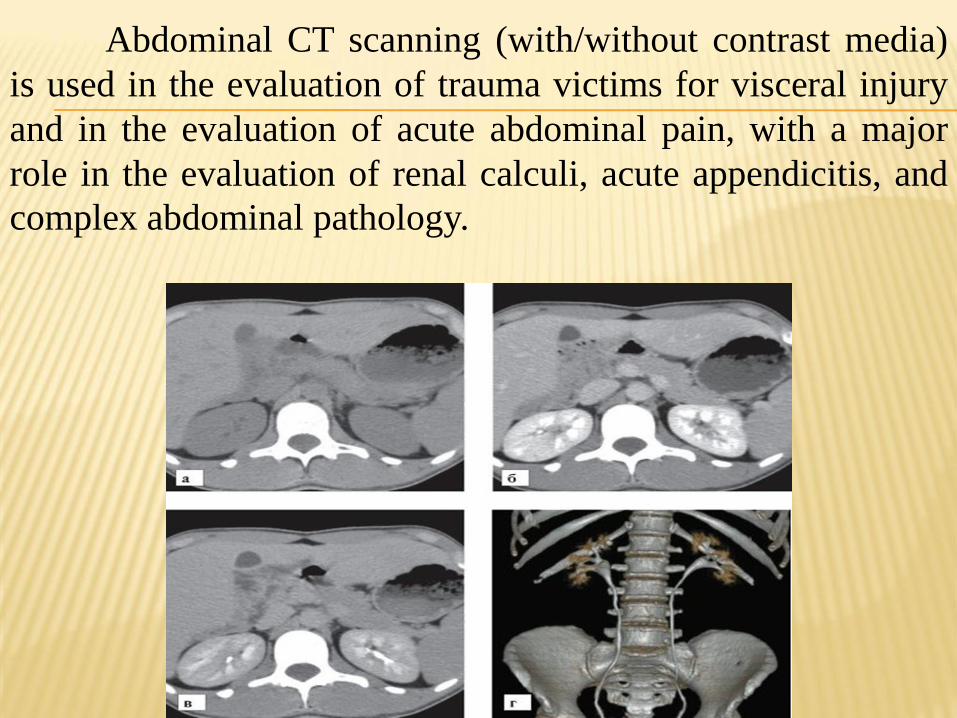
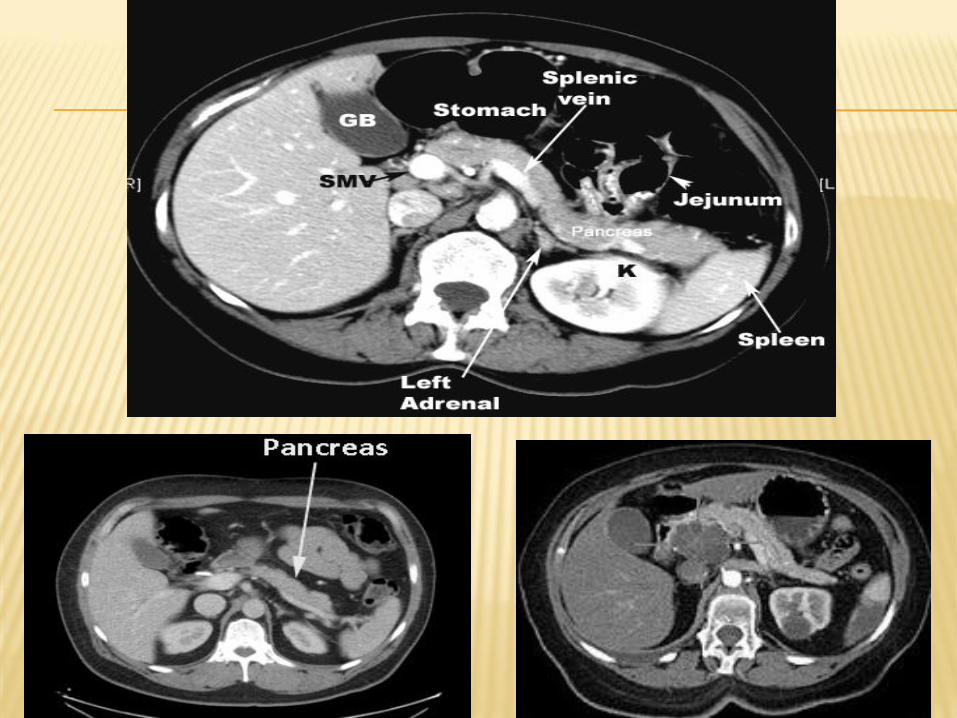
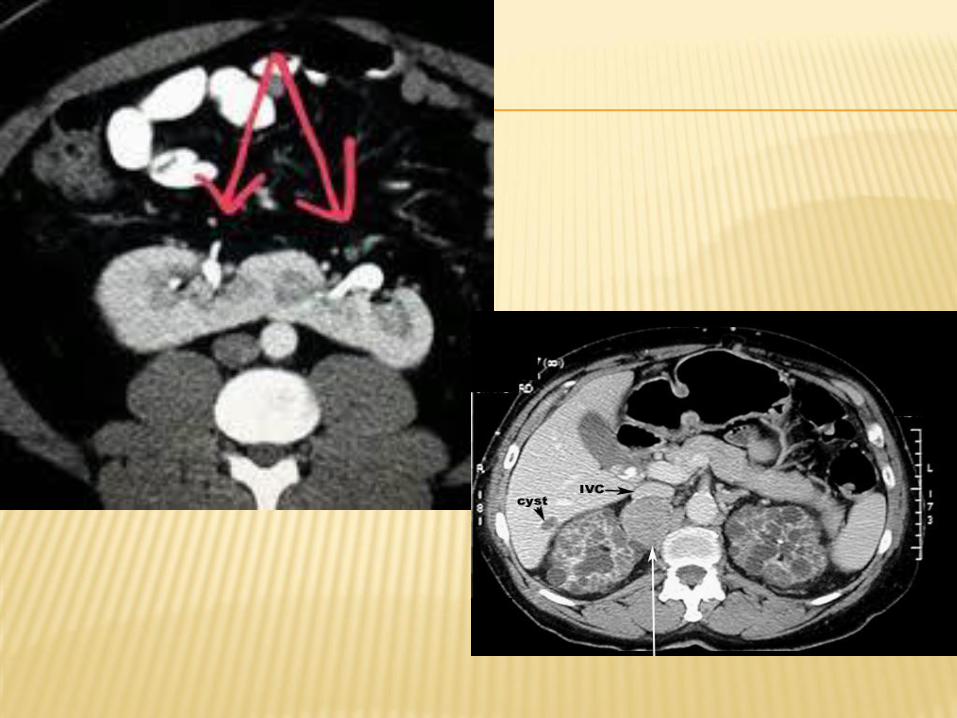
Abdominal CT scanning (with/without contrast media)
is used in the evaluation of trauma victims for visceral injury
and in the evaluation of acute abdominal pain, with a major
role in the evaluation of renal calculi, acute appendicitis, and
complex abdominal pathology.
Magnetic resonance imaging (MRI)
MRI ABDOMEN WITHOUT CM - Done to evaluate:
● Biliary tract, common bile duct
● Pancreatic duct
● Gall bladder stones
MRI ABDOMEN WITH CM - Done to evaluate:
● Liver pathology (hemangiomas, masses, etc)
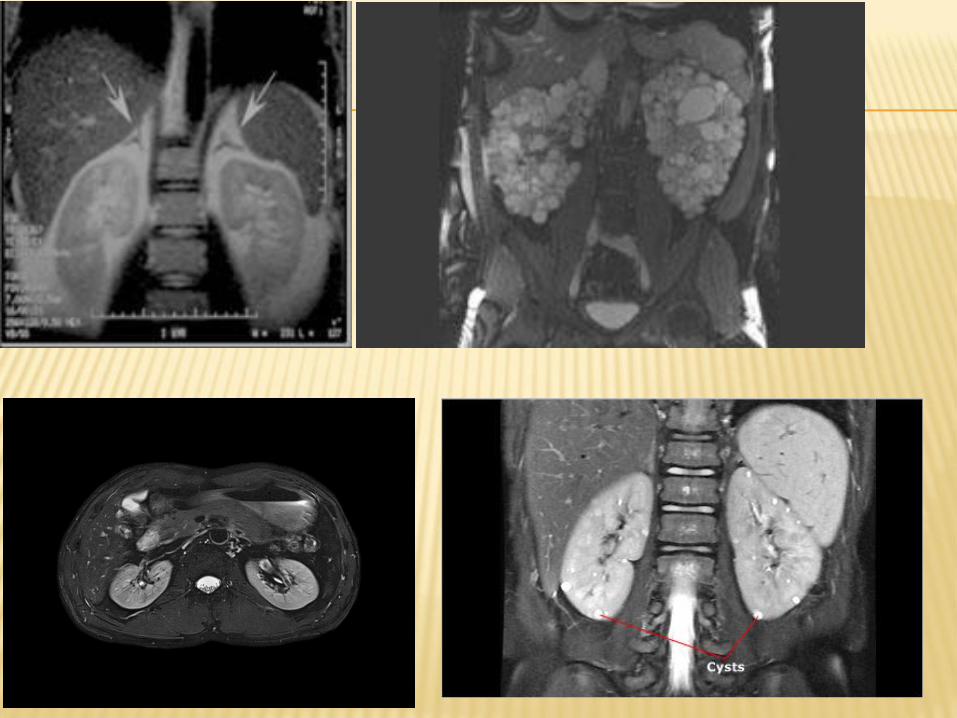
● Kidney pathology (cysts, tumors)
● Adrenal pathology (cysts, tumors)
● Pancreas pathology(cysts, tumors)
● Splenic pathology (cysts, tumors)
● Abd pain
MRI PELVIS− WITHOUT CM Done for:
● SI joint pain
● Pelvis fracture
● Sacral and/or coccyx disorders
MRI PELVIS− WITH/WITHOUT CM Done for:
● Ovarian or uterine pathology, fibroid tumors
● Bladder pathology
● Mass, Mets to bone
● CA of Prostate
● Plexus lesions

A B
C D
A
B
C
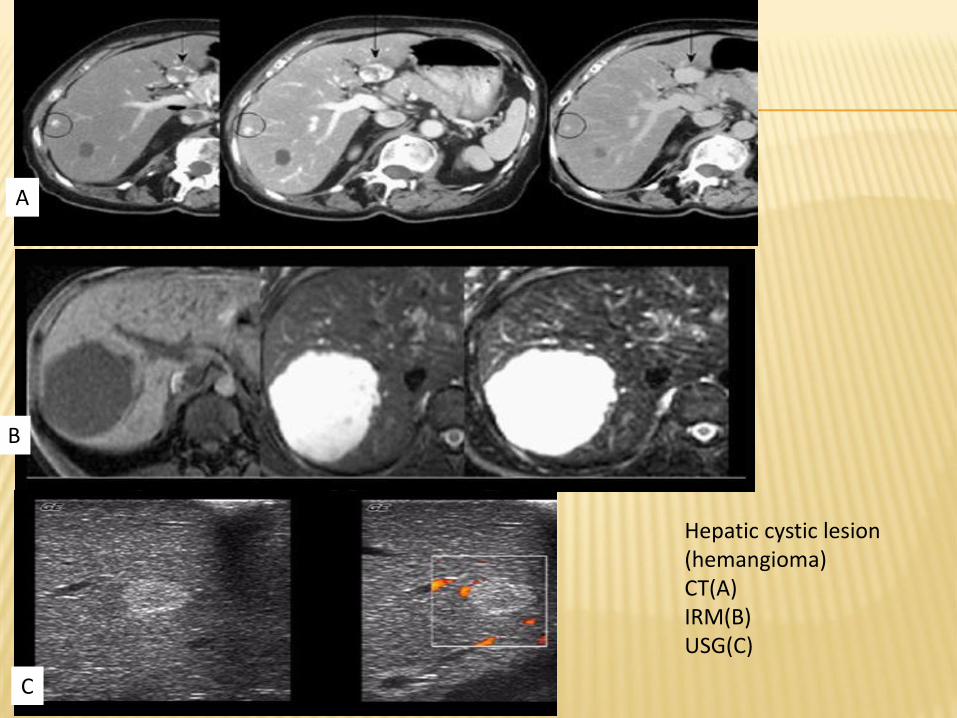
Hepatic cystic lesion (hemangioma) CT(A)IRM(B)USG(C)

B,C.MRI pelvis-axial T2,T1 : intrauterine gestational sac and uterine fibroid
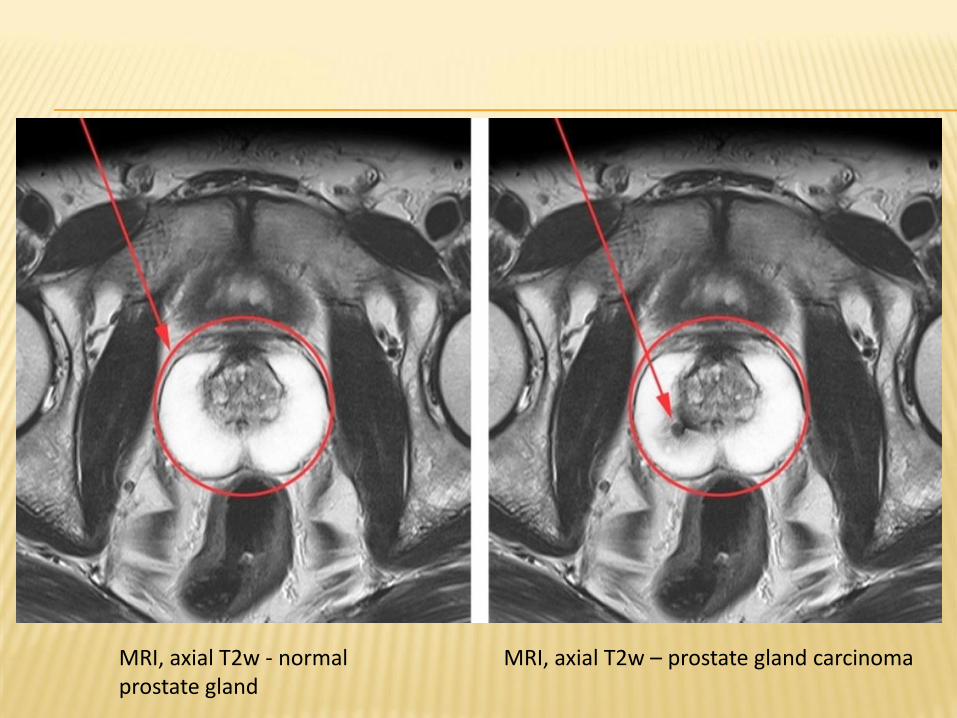
MRI, axial T2w - normal prostate gland
MRI, axial T2w – prostate gland carcinoma
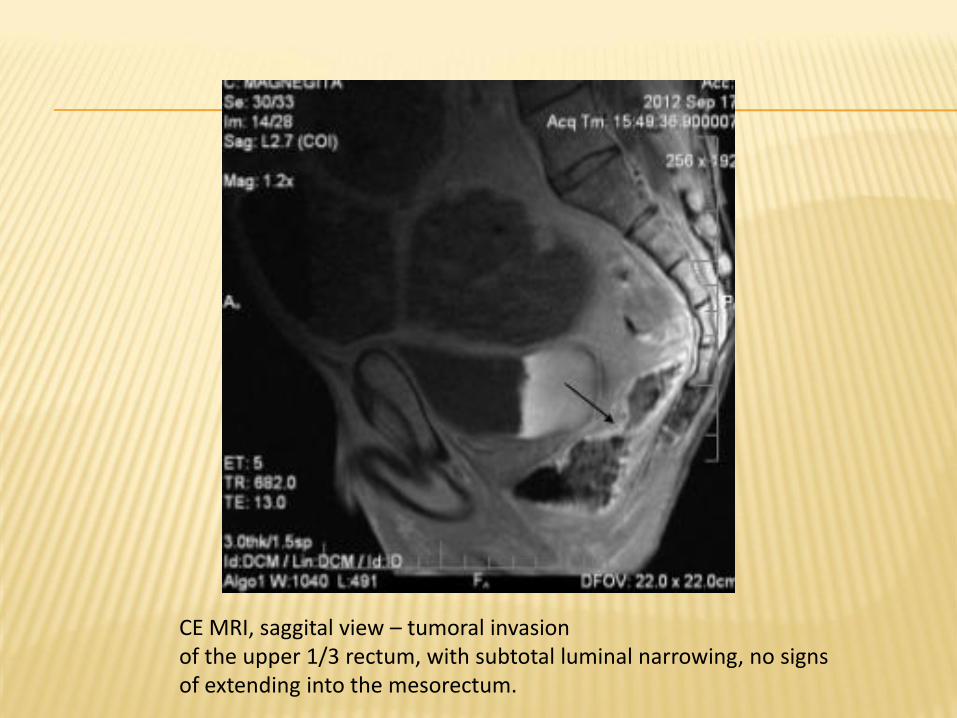
CE MRI, saggital view – tumoral invasion of the upper 1/3 rectum, with subtotal luminal narrowing, no signs of extending into the mesorectum.
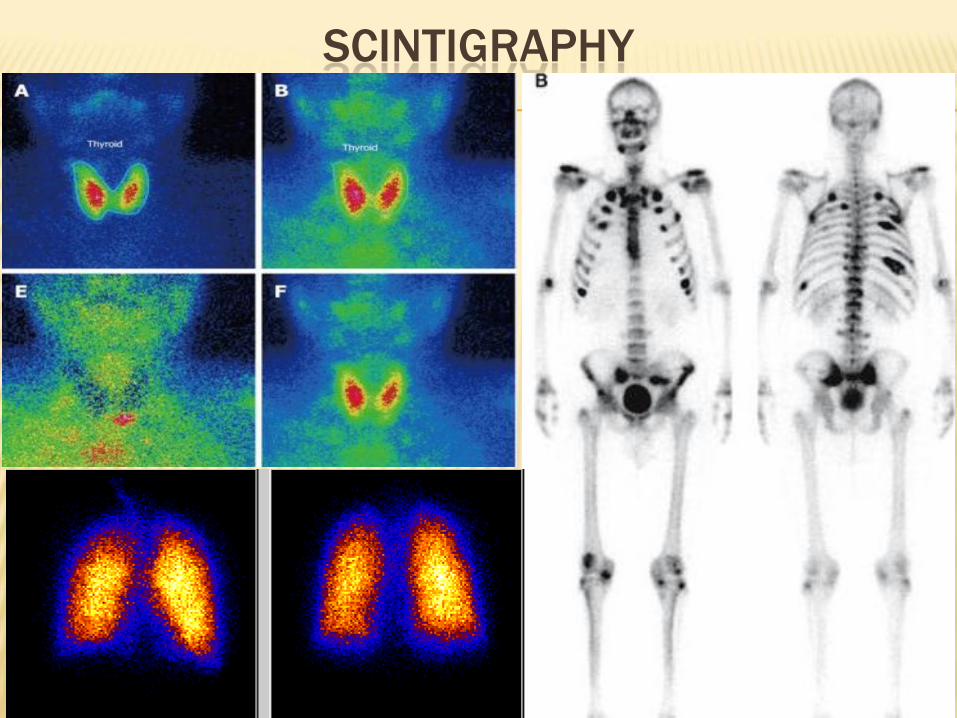
SCINTIGRAPHY
Recognizing Pneumonia
1) Pneumonia can be defined as consolidation of the lung produced by inflammatory exudate, usually as a result of an infectious agent.
2) Most pneumonias produce airspace disease, either lobar or segmental. Other pneumonias demonstrate interstitial disease and others produce findings in both the airspaces and the interstitium
3)Most microorganisms that produce pneumonia are spread to the lungs via the tracheobronchial tree, either through inhalation or aspiration of the organisms.
4)In some instances, microorganisms are spread via the bloodstream and, in even fewer cases, by direct extension.
5)Because many different microorganisms can produce similar imaging findings in the lungs, it is difficult to identify with certainty the causative organism from the radiographic presentation alone. However, certain patterns of disease are very suggestive of a particular causative organism
6)Some use the term infiltrate synonymously with pneumonia, although many diseases, from amyloid to pulmonary fibrosis, can infiltrate the lung.
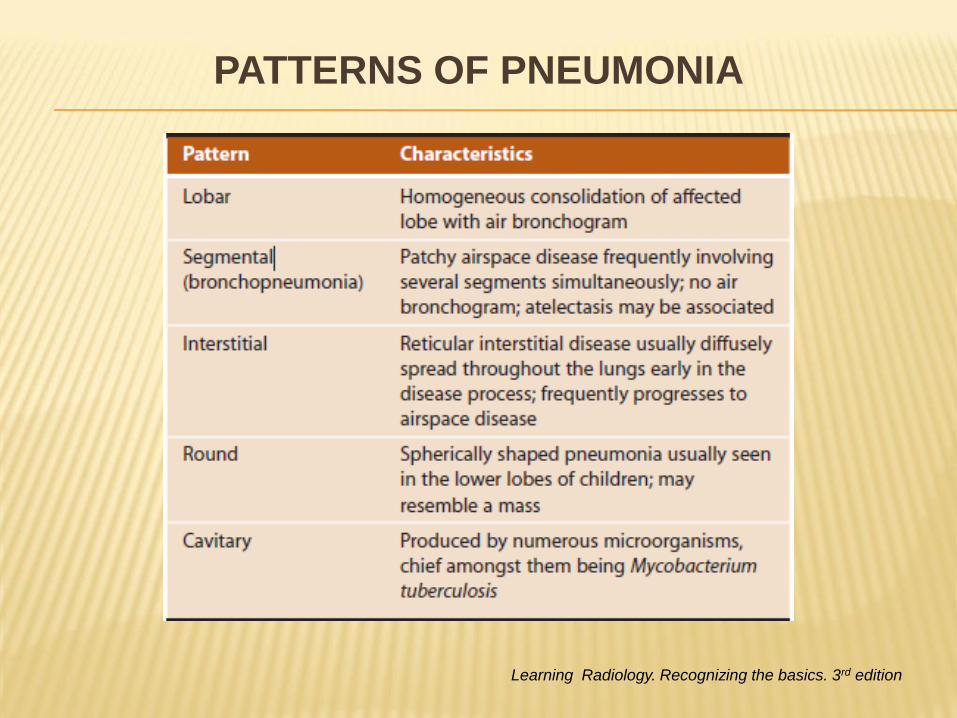
PATTERNS OF PNEUMONIA
Learning Radiology. Recognizing the basics. 3rd edition
PATTERNS OF PNEUMONIA
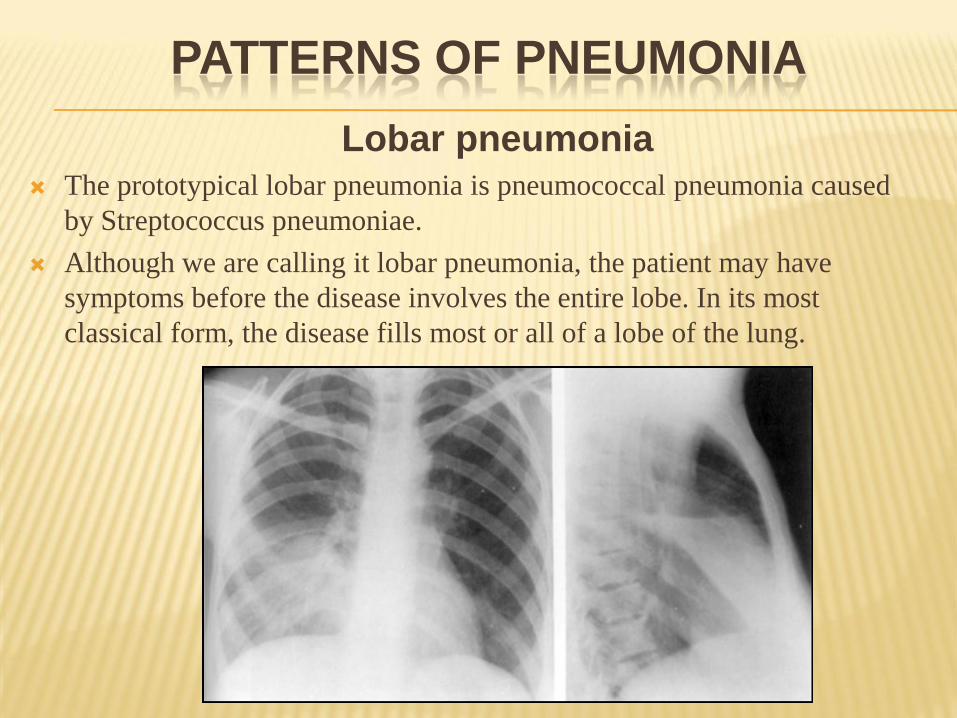
Lobar pneumonia
The prototypical lobar pneumonia is pneumococcal pneumonia caused
by Streptococcus pneumoniae.
Although we are calling it lobar pneumonia, the patient may have
symptoms before the disease involves the entire lobe. In its most
classical form, the disease fills most or all of a lobe of the lung.
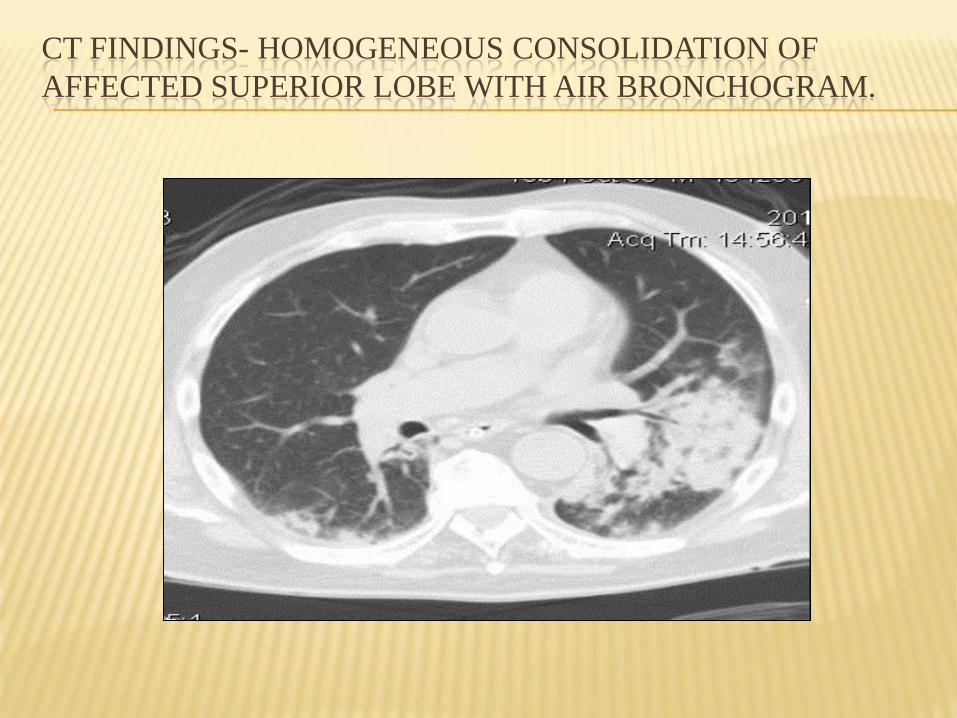
CT FINDINGS- HOMOGENEOUS CONSOLIDATION OF
AFFECTED SUPERIOR LOBE WITH AIR BRONCHOGRAM.
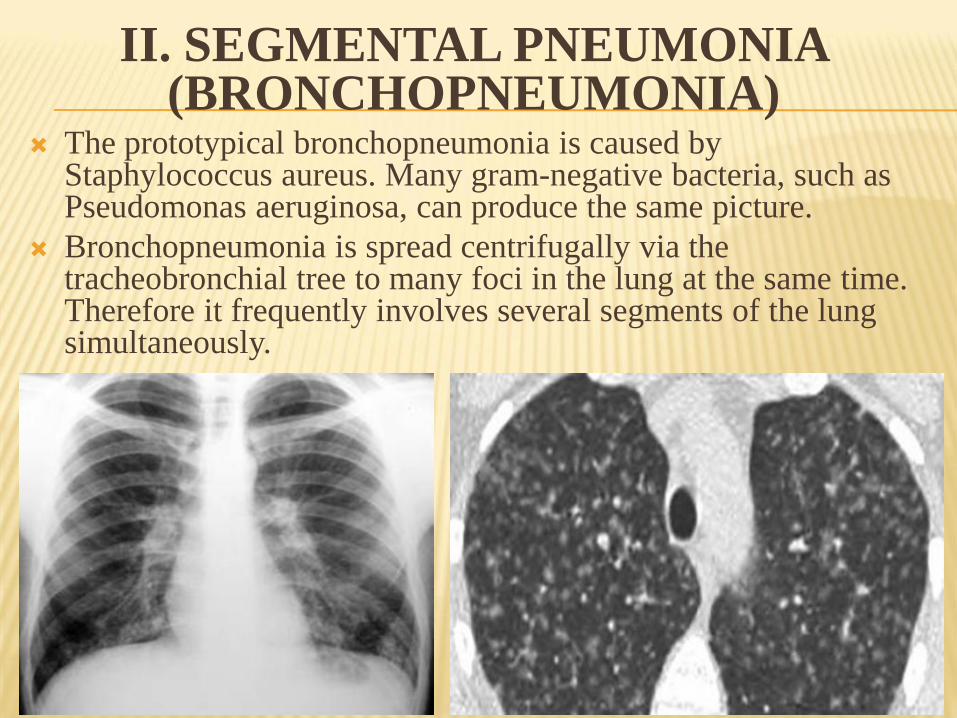
II. SEGMENTAL PNEUMONIA(BRONCHOPNEUMONIA)
The prototypical bronchopneumonia is caused by Staphylococcus aureus. Many gram-negative bacteria, such as Pseudomonas aeruginosa, can produce the same picture.
Bronchopneumonia is spread centrifugally via the tracheobronchial tree to many foci in the lung at the same time. Therefore it frequently involves several segments of the lung simultaneously.

Pseudolobar pneumonia
Micro- and macronodular pattern
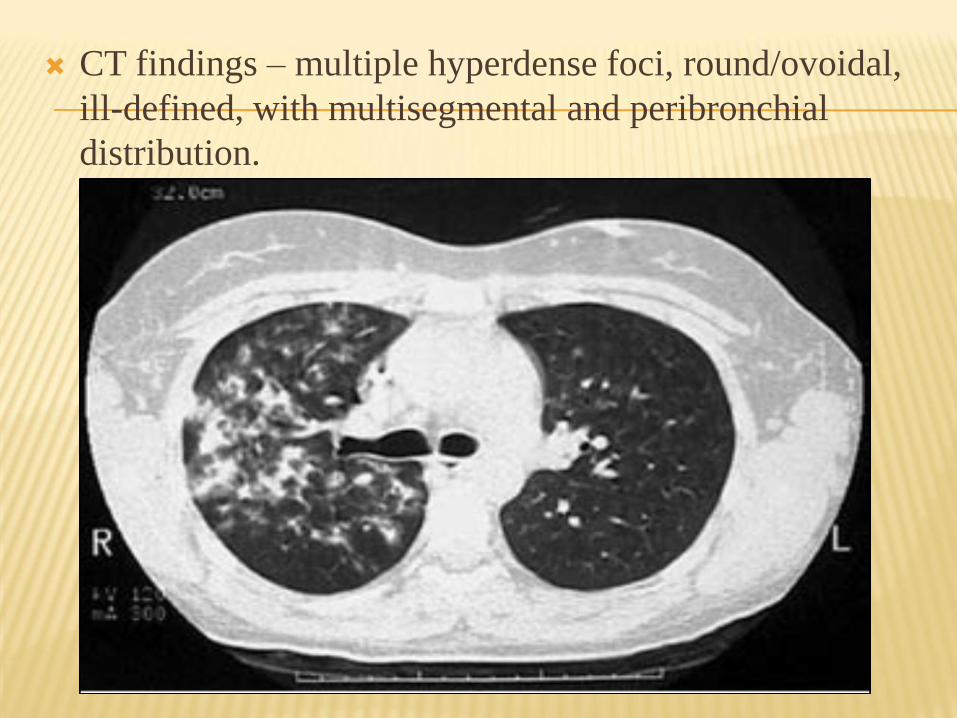
CT findings – multiple hyperdense foci, round/ovoidal,
ill-defined, with multisegmental and peribronchial
distribution.
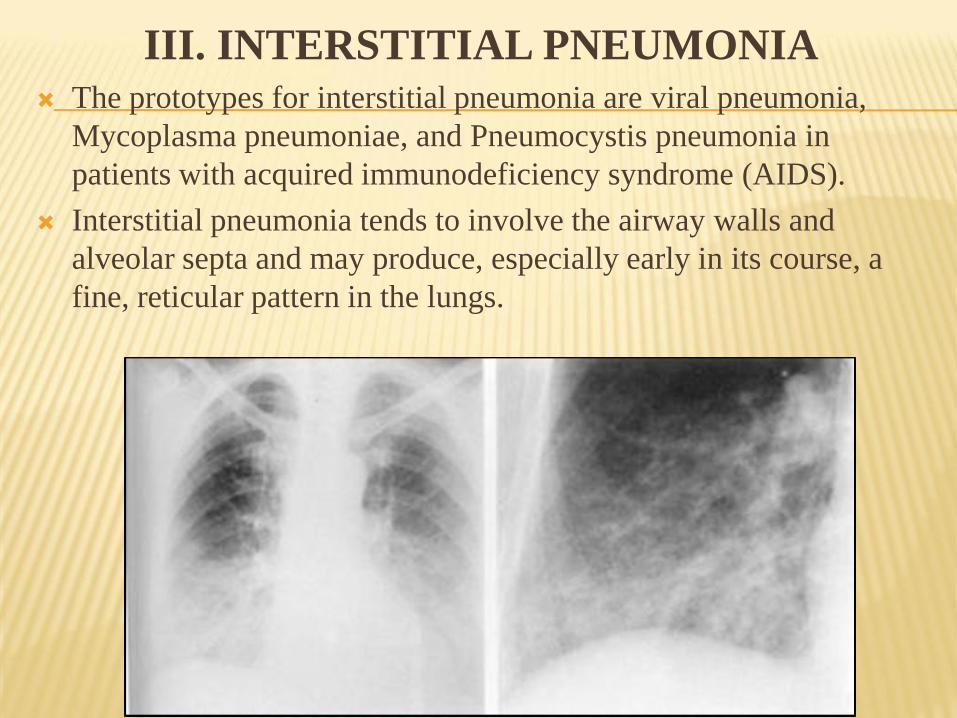
III. INTERSTITIAL PNEUMONIA The prototypes for interstitial pneumonia are viral pneumonia,
Mycoplasma pneumoniae, and Pneumocystis pneumonia in
patients with acquired immunodeficiency syndrome (AIDS).
Interstitial pneumonia tends to involve the airway walls and
alveolar septa and may produce, especially early in its course, a
fine, reticular pattern in the lungs.
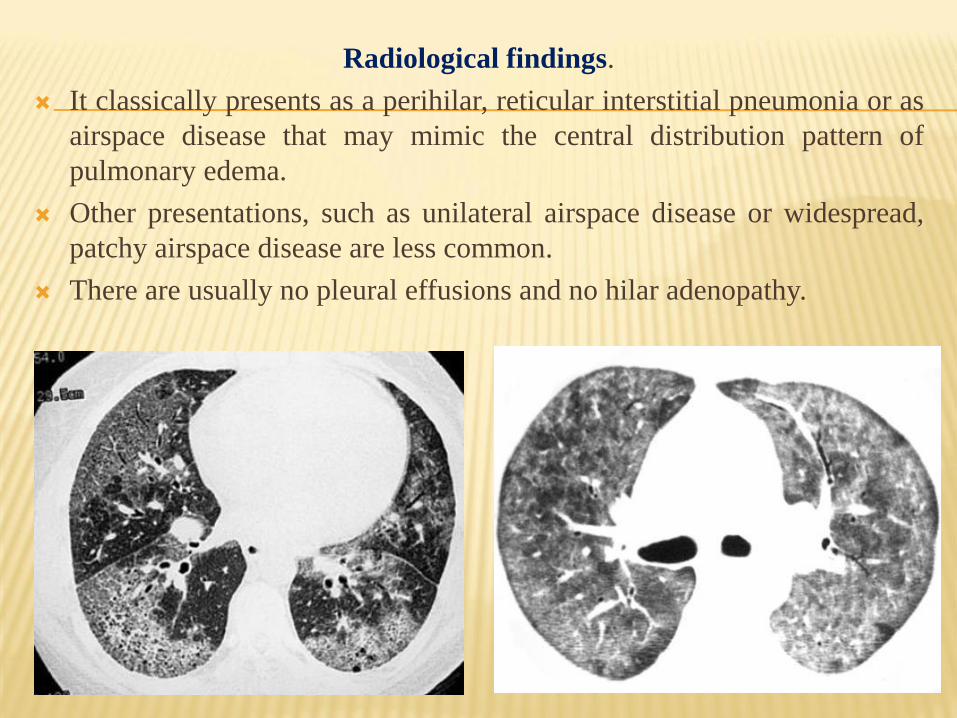
Radiological findings.
It classically presents as a perihilar, reticular interstitial pneumonia or as
airspace disease that may mimic the central distribution pattern of
pulmonary edema.
Other presentations, such as unilateral airspace disease or widespread,
patchy airspace disease are less common.
There are usually no pleural effusions and no hilar adenopathy.
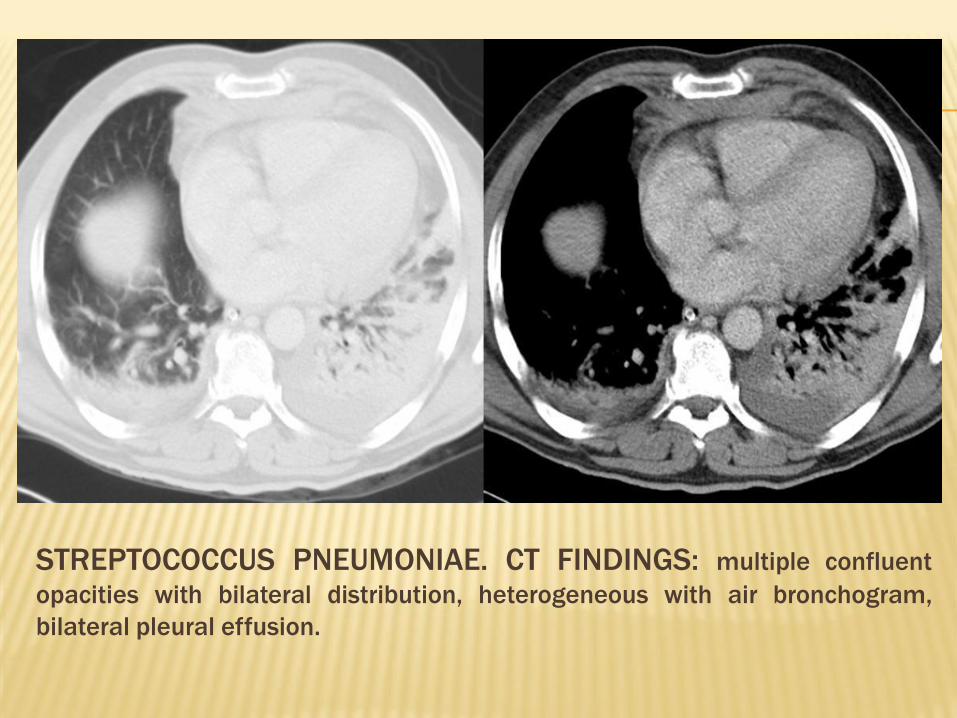
STREPTOCOCCUS PNEUMONIAE. CT FINDINGS: multiple confluent
opacities with bilateral distribution, heterogeneous with air bronchogram,
bilateral pleural effusion.
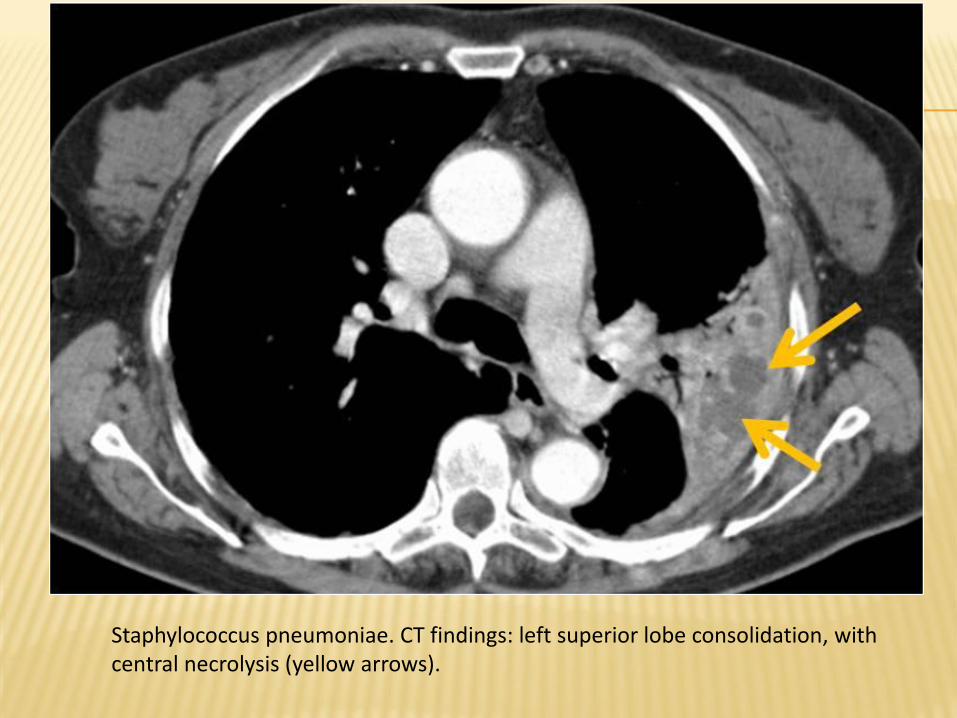
Staphylococcus pneumoniae. CT findings: left superior lobe consolidation, with central necrolysis (yellow arrows).
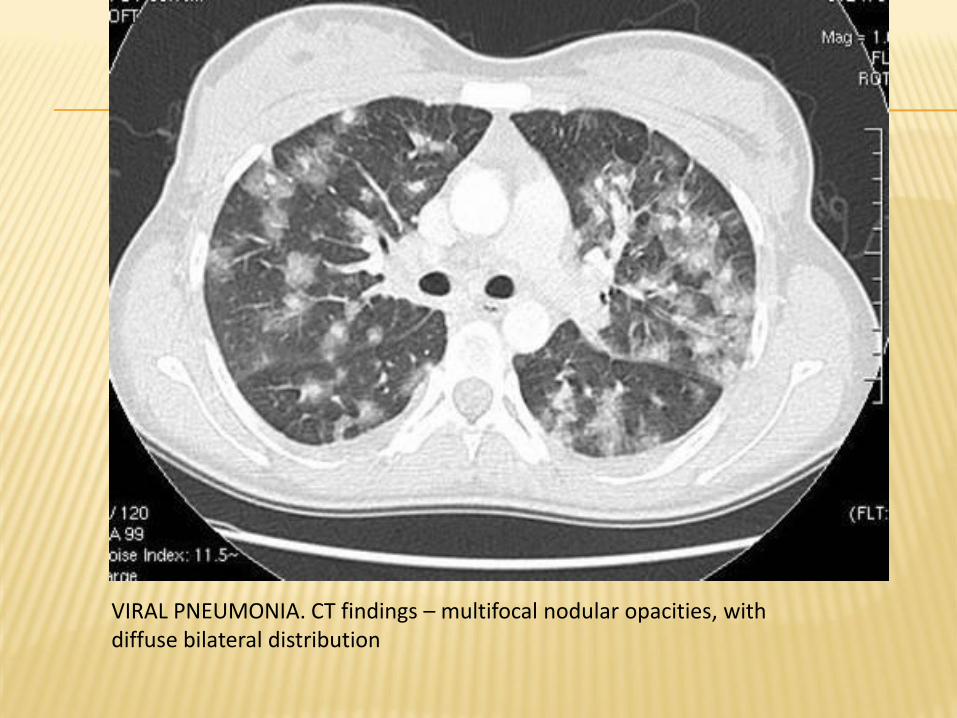
VIRAL PNEUMONIA. CT findings – multifocal nodular opacities, with diffuse bilateral distribution